toxicity of amphotericin b deox ycholate-based in...
TRANSCRIPT

1
Toxicity of Amphotericin B deoxycholate-based induction therapy 1
in patients with HIV-associated cryptococcal meningitis 2
3
Tihana Bicanic1♯, Christian Bottomley2, Angela Loyse1, Annemarie E Brouwer3, 4
Conrad Muzoora4, Kabanda Taseera4, Arthur Jackson5, Jacob Phulusa5, Mina C 5
Hosseinipour5, Charles van der Horst5, Direk Limmathurotsakul6, Nicholas J 6
White6,7, Douglas Wilson8, Robin Wood9, Graeme Meintjes10,11, Thomas S 7
Harrison1, Joseph N Jarvis12-14 8
9
1. Institute of Infection and Immunity, St. George’s University of London, 10
UK 11
2. Faculty of Epidemiology and Population Health, London School of 12
Hygiene & Tropical Medicine, UK. 13
3. Elisabeth Hospital, Tilburg, the Netherlands 14
4. Mbarara University of Science and Technology, Uganda 15
5. University of North Carolina (UNC) Project, Lilongwe, Malawi 16
6. Mahidol-Oxford Research Unit, Faculty of Tropical Medicine, Mahidol 17
University, Bangkok, Thailand 18
7. Centre for Tropical Medicine and Global Health, Nuffield Department of 19
Clinical Medicine, University of Oxford 20
8. Edendale Hospital, Pietermaritzburg, South Africa 21
9. Desmond Tutu HIV Centre, Institute of Infectious Disease and Molecular 22
Medicine, University of Cape Town, South Africa 23
AAC Accepted Manuscript Posted Online 8 September 2015Antimicrob. Agents Chemother. doi:10.1128/AAC.01698-15Copyright © 2015, American Society for Microbiology. All Rights Reserved.
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

2
10. Division of Infectious Diseases and HIV Medicine, Department of 24
Medicine, University of Cape Town, South Africa 25
11. Institute of Infectious Disease and Molecular Medicine, University of 26
Cape Town, South Africa 27
12. Department of Clinical Research, Faculty of Infectious and Tropical 28
Diseases London School of Hygiene and Tropical Medicine, UK 29
13. Botswana-UPenn Partnership, Gaborone, Botswana 30
14. Division of Infectious Diseases, Department of Medicine, Perelman 31
School of Medicine, University of Pennsylvania, USA 32
33
Running title: AmB toxicity cryptococcal meningitis HIV 34
35
♯ Address correspondence to Tihana Bicanic [email protected] 36
Senior Lecturer and Consultant in Infectious Diseases 37
Institute of Infection and Immunity, St George’s University of London 38
Cranmer Terrace, London, SW17 0RE, UK 39
40
41
Key words: amphotericin B; amphotericin B deoxycholate; cryptococcal 42
meningitis; drug therapy; drug toxicity; antifungal 43
44
Word count 2536 45
46
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from


4
Abstract 51
Amphotericin B deoxycholate (AmBd) is the recommended induction treatment 52
for HIV-associated cryptococcal meningitis (CM). Use is hampered by toxicities 53
that include electrolyte abnormalities, nephrotoxicity and anaemia. Protocols to 54
minimise toxicity are applied inconsistently. In a clinical trial cohort of AmBd-55
based CM induction treatment, a standardised protocol of pre-emptive 56
hydration and electrolyte supplementation was applied. Changes in blood 57
counts, electrolytes, and creatinine over 14 days were analysed in relation to 58
AmBd dose, treatment duration (short course, 5-7 days or standard, 14 days), 59
addition of flucytosine, and outcome. In the 368 patients studied, haemoglobin 60
dropped by a mean(95% CI) of 1.5(1.0-1.9) g/dL following 7 days of AmBd, and 61
2.3(1.1-3.6) g/dL after 14 days. Serum creatinine increased by 37(30-45) μmol/L 62
by day 7 and 49(35-64) μmol/L by day 14 of AmBd. Overall 33% of patients 63
developed grade III/IV anaemia, 5.6% developed grade III hypokalaemia, in 64
9.5% creatinine exceeded 220μmol and 6% discontinued AmBd prematurely. 65
Addition of 5FC was associated with a slight increase in anaemia but not 66
neutropenia. Laboratory abnormalities stabilised or reversed during the second 67
week in patients on short course induction. Grade III/IV anaemia(aOR 2.2, 95% 68
CI 1.1-4.3, p= 0.028); and nephrotoxicity(aOR 4.5, 95% CI 1.8-11, p=0.001) were 69
risk factors for 10-week mortality. In summary, routine intravenous saline 70
hydration and pre-emptive electrolyte replacement during AmBd-based 71
induction regimens for HIV-associated CM minimised incidence of 72
hypokalaemia and nephrotoxicity. Anaemia remained a concerning adverse 73
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

5
effect. Addition of flucytosine was not associated with increased neutropenia. 74
Shorter AmBd courses were less toxic, with rapid reversibility. 75
76
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

6
Introduction 77
Amphotericin B deoxycholate(AmBd) is a polyene antifungal that binds to 78
ergosterol in the fungal cell membrane, resulting in increased permeability and 79
cell death(1), as well as to cholesterol in mammalian cell membranes, partly 80
explaining its adverse effects of nephrotoxicity, electrolyte imbalance and 81
anaemia(1). 82
83
Less toxic lipid formulations of AmB, developed in the 1990s, have now largely 84
supplanted the use of the AmBd preparation for the treatment of systemic 85
mycoses in high-resource settings. AmBd has been used to treat cryptococcal 86
meningitis(CM) since the pre-HIV era(2, 3). AmB exhibits concentration-87
dependent killing(4), and successive randomised controlled trials used 88
progressively increasing doses as induction therapy for HIV-associated CM, 89
+/- flucytosine(5FC) or fluconazole as second agents(5-9). AmBd 1mg/kg/d 90
plus 5FC provided the best fungal clearance and 10-week survival in a recent 91
phase III trial(10) and remains the ‘gold standard’ for treatment of HIV-92
associated CM in IDSA and WHO guidelines(11, 12). 93
94
AmBd nephrotoxicity results from decreased renal blood flow resulting in 95
reduced glomerular filtration rate and direct renal tubular toxicity, causing 96
potassium and magnesium loss(1). Nephrotoxicity is cumulative and dose-97
dependent, though reversible(13, 14), and is reduced by pre-loading with saline, 98
adequate hydration and electrolyte replacement(15-19). Anaemia results 99
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

7
primarily from inhibition of renal erythropoietin production, though 100
haemolysis has been reported(20). 101
102
In resource-poor settings, facilities to prevent, monitor and manage AmBd 103
toxicity are lacking. Fear of toxicities deters clinicians from using AmBd to treat 104
CM. Instead, less effective but widely available fluconazole monotherapy is 105
used(21). 106
107
Since 2000, we have implemented a standardised protocol of pre-hydration and 108
pre-emptive electrolyte supplementation in clinical trials of AmBd-based CM 109
induction treatment in Asia and Africa(14, 22-27), which is now included in 110
WHO guidelines(12). We present the toxicity analyses of AmBd dosed at the 111
currently recommended dose range (0.7-1mg/kg/d), for treatment durations of 112
5-14 days, alone or combined with a second antifungal, in a large combined 113
cohort of patients with HIV-associated CM managed in resource-limited 114
settings. Our aims were to characterise the association of AmBd dose and 115
duration, and addition of 5FC, with the development of its common toxicities, 116
and determine the relationship between toxicity and mortality. 117
118
119
120
121
122
123
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from


9
Materials and Methods 127
Participants and procedures 128
The cohort consisted of adult HIV-infected, antiretroviral therapy(ART)-naïve 129
patients with first episode of CM enrolled in six phase II clinical trials carried 130
out from 2002-10 in Asia and Africa(14, 23-27)(Supplementary Table 1). 131
In trials 1-4 patients received standard (14-day) courses of AmBd, and in 132
studies 5-6 received shorter courses (< 7 days). Induction therapy differed in 133
terms of AmB dose (0.7 or 1mg/kg/d, dosed according to actual body weight), 134
choice of second+/- third drug and adjunctive interferon-γ. All patients on 5FC 135
received 5FC orally, except for 32 patients in the Thai study who received 136
intravenous 5FC as part of a pharmacokinetic sub-study(28). 137
138
Management of toxicity 139
Laboratory monitoring 140
During the first 14 days, all patients had alternate day measurements of 141
complete blood counts, urea, creatinine and electrolytes (magnesium 142
measurement was only available in South Africa). 143
144
Electrolytes and renal impairment 145
Patients received daily pre-hydration with 1L 0.9% (normal) saline with 146
20mmol potassium chloride(KCl) before AmBd administration. Additional IV-147
fluids were at study physicians’ discretion. Nephrotoxic drugs such as 148
aminoglycosides and NSAIDS were avoided (pre-medication with paracetamol 149
or chlorpheniramine was allowed in case of infusion reactions). If creatinine 150
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

10
rose to 220μmol/L (2.5mg/dL), equivalent to grade III nephrotoxicity on 151
Division of AIDS (DAIDS) criteria (creatinine rise 1.9-3.4X ULN), the next 152
AmBd dose was omitted and the patient was given additional IV-fluids. The 153
following day, if creatinine was stable or improving, alternate daily dosing was 154
instituted at the same AmBd dose, with return to daily dosing once creatinine 155
had normalised. If creatinine was still increasing, AmBd was stopped and the 156
patient switched early to fluconazole, adjusting dose according to renal 157
function (50% for creatinine clearance 20-40ml/min, 25% if <20ml/min). 158
Flucytosine dose interval was extended to 12-hourly if creatinine clearance 159
decreased to 20-40ml/min, and once daily if creatinine clearance <20ml/min. In 160
all South African trials, patients received oral electrolyte supplementation with 161
2 tablets twice daily of potassium chloride (Slow-K, 600mg, 8mmol K/tab) and 162
2 tablets once daily of magnesium chloride (Slow-Mag 535mg, 5.33mmol 163
Mg/tab), with additional IV or oral supplementation as required. At other sites, 164
additional IV or oral potassium was administered according to laboratory 165
results. 166
167
Bone marrow toxicity 168
Due to limited blood product availability, there was no haemoglobin threshold 169
for transfusion: this was done at study sites’ discretion. Flucytosine was 170
stopped if platelets dropped to <50x109/ml or neutrophils to <0.5x109/L. 171
172
Statistical analyses 173
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

11
We explored changes in haemoglobin(Hb), neutrophil and platelet count, 174
creatinine, potassium(K), and magnesium(Mg) over a 14-day period following 175
start of AmBd-based treatment. For each measure we used LOESS (locally 176
weighted scatterplot smoothing) to estimate the mean value as a function of the 177
number of days post-treatment initiation. 178
179
Linear regression models were constructed examining the effects of AmB dose 180
(0.7 or 1mg/kg/d) and duration (5-7 days or 14 days) on Hb, K and creatinine 181
change from baseline to days 7 and 14, peak creatinine and Hb nadir. Sex and 182
treatment with 5FC were included as potential confounders in the Hb analyses. 183
Baseline imbalances between groups were accounted for by using a ‘change 184
from baseline’ analysis rather than adjusting for baseline (with the exception of 185
peak and nadir values). 186
Logistic regression models examined associations between protocol pre-defined 187
nephrotoxicity, DAIDS grade III hypokalaemia (K+ 2-2.4 mmol/L or mEq/L), 188
grade III (Hb 6.5-7.4 g/dL) and IV anaemia (Hb<6.5g/dL) and mortality at 2 189
and 10 weeks, adjusting for baseline value (Hb, creatinine, K); patient weight in 190
the nephrotoxicity analysis, and established prognostic markers baseline fungal 191
burden, altered mental status and CD4-cell count(29). 192
193
Given the pooling of data across studies, clustering by study in both the linear 194
and logistic regression models was accounted for by including ‘study’ as a 195
random effect term. 196
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

12
197
Data were analyzed using Stata, v12.0 (StataCorp TX77845 USA). 198
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

13
Results 199
368 (52% male) patients were included; 64 (17%) were Thai, 298 (81%) Black 200
African and 3(<1%) of mixed race. Median (IQR) age was 33 (29-38) years and 201
CD4 count 25 (10-55) cells/μL. Changes from baseline (pre-treatment) are 202
shown in Table 1 and LOESS curves (Figures 1 and 2). 203
204
From a mean baseline of 11g/dL, mean overall(%) drop in haemoglobin was 205
1.5g/dL(12%) by day 7 and 2.3g/dL(20%) by day 14. With pre-emptive 206
supplementation, potassium values remained stable over time (Supplementary 207
Figure 1a). Mean(95%CI) creatinine change from baseline was +37(30-45) 208
μmol/L at day 7 and +49(35-64) μmol/L at day 14. 209
210
Incidence of serious toxicity 211
Grade III/IV anaemia (Hb<7.5g/dL) developed in 112 patients(33%). 212
Fifty-nine patients(18%) developed grade IV anaemia (Hb<6.5g/dL). Women 213
had a higher incidence of Grade III (54% vs 14%) and grade IV anaemia (31% vs 214
5%, p<0.001) due to sex differences in baseline, rather than differences in on-215
treatment change (d14 Hb drop 2.14g/dL males vs 2.21g/dL females, p=0.92) 216
(Fig 1c). In the South African trials, which collected transfusion data, 12 of 304 217
patients (4%) received blood transfusions, constituting only 20% of patients 218
with grade IV anaemia. 219
220
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

14
Sixteen of 284 patients(5.6%) developed grade III hypokalaemia(K+<2.5 221
mmol/L), 5 in the first week of treatment, of whom three patients(1.1% of 222
cohort) developed grade IV hypokalaemia (K+<2mmol/L), two on d11 and one 223
on d12 of treatment. In the South African trials using pre-emptive oral in 224
addition to IV K+ supplementation, potassium change from baseline differed 225
significantly from trials not using oral K (mean(95%CI) d7 K change +0.39(0.24, 226
0.54) vs -0.17(-0.47, +0.12), p<0.001 t-test), with a lower incidence of grade III 227
hypokalaemia (4.2% vs 9.7%, p=0.08). 228
229
Thirty-three patients(9.5%) exceeded the protocol-defined nephrotoxicity 230
threshold(Creat>220μmol/L). In the South African trials using standard-course 231
AmBd(n=234), 15 patients(6.4%) discontinued AmBd early due to 232
nephrotoxicity, at a median(range) of 11(5-13)d. In the short-course trials 233
(n=70), 4 patients(5.7%) stopped early (all in the 7-day study), three of whom 234
omitted the final day only. 235
236
Toxicity by AmB dose and duration 237
There was a greater absolute drop in Hb at days 7 and 14 in patients receiving 238
the higher AmBd dose and for those receiving standard vs short-course 239
treatment, though differences were non-significant (supplementary Table 2). 240
Patients receiving shorter courses had a higher nadir Hb (mean 9.5 v 8.3g/dL), 241
even after adjustment for sex and 5FC (p=0.033). 242
243
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

15
There was less renal impairment in those receiving the 0.7mg/kg AmBd dose: 244
mean creatinine rise 28 vs 41μmol/L at d7 (p=0.02); 42 vs 53μmol/L at d14 245
(p=0.09). Mean creatinine peaked at 127 vs 145μmol/L (p=0.04), remaining 246
significant on multivariable analysis (adjusted mean difference 13μmol/L, 247
p=0.04). Despite similarities in peak creatinine, creatinine change to d14 was 248
less in patients receiving short-course versus standard treatment (mean rise 17 249
vs 49μmol/L, p<0.001, supplementary Table 2). 250
251
Reversibility 252
Hb stabilised and started to increase in the second week in the short-course 253
group after stopping AmBd, whilst continuing to decline in the standard 254
group(mean week 2 change -0.12 vs -0.93 g/dL, p=0.01, Figure 1b). 255
256
Renal impairment in the short-course group resolved in week 2 following 257
cessation of AmBd, with creatinine continuing to rise in the standard group 258
(mean week 2 change: -28 vs +14μmol/L, p<0.001, Figure 2c). 259
260
Potassium 261
There was no significant association of AmB dose or duration with potassium 262
change (data not shown). The Loess curves of potassium change 263
(Supplementary figure 1) show a dip in K+ during days 8-10 in the short-course 264
trials, after stopping AmBd and K+ supplementation, supportive of ongoing 265
potassium wasting(30). 266
267
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

16
Incidence of grade III/IV hypomagnesemia, neutropenia and 268
thrombocytopenia and associations with use of 5FC are shown in the 269
Supplementary Results. 270
271
Association of toxicity with 2 and 10-week outcome 272
Development of nephrotoxicity (Creat>220μmol/L) was associated with 2-week 273
mortality (Table 2), however this was no longer significant in the adjusted 274
model (2-week aOR 2.9, 95% CI 0.6-12.7, p= 0.17). The association between 275
nephrotoxicity and 10-week mortality remained significant following 276
adjustment for baseline creatinine, weight, CD4 count, fungal burden, altered 277
mental status and study (10-week aOR 4.5, 95% CI 1.8-11, p=0.001, Table 2). 278
279
Severe anaemia (grade III/IV) was a significant risk factor for 10-week 280
mortality following adjustment for baseline Hb, CD4 count, fungal burden, 281
altered mental status and study (aOR 2.2, 95% CI 1.1-4.3, p= 0.028, Table 3). 282
283
Development of grade III hypokalaemia (K+<2.5mmol/L) was not associated 284
with mortality (Table 2). 285
286
287
288
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

17
Discussion 289
290
This analysis of 368 patients treated with AmBd-based induction regimens in 291
resource-poor settings represents the largest reported toxicity analysis of HIV-292
associated CM treatment. 293
294
Published trials reporting toxicity of AmBd at recommended 0.7-1mg/kg/d 295
doses for HIV-associated CM include 6 trials from high-income settings(6, 8, 31-296
34) and 8 trials from low-income settings in Asia and Africa(9, 10, 35-297
40)(Supplementary Table 3). Six trials reported routine use of saline pre-loading 298
and one reported pre-emptive electrolyte replacement(41). Definitions of 299
nephrotoxicity varied. Incidence of grade III nephrotoxicity (or equivalent) was 300
20-33% in older trials without routine fluid pre-loading(8, 32, 36), compared to 301
2-11% in our data and more recent trials using saline pre-loading(10, 39). 6% of 302
our patients discontinued treatment early, usually 1-2 days before completion, 303
in comparison to up to 53% in published trials. 304
305
AmBd nephroxicity is cumulative(42): in our patients, creatinine rose by a mean 306
of 52% by day 7 and 73% by day 14. Although nephrotoxicity was greater using 307
the 1mg/kg/d dose, this translated into a mean difference in peak creatinine of 308
13μmol/L, which is of minor clinical significance and should not deter 309
clinicians from using the more fungicidal higher dose. 310
311
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

18
The long terminal half-life of AmBd(up to 2 weeks)(4) provides ongoing 312
fungicidal activity after stopping drug administration(25, 27). These data 313
demonstrate better tolerability of 5-7 day regimens, with less nephrotoxicity 314
and reversibility, with creatinine almost returning to baseline one week after 315
stopping short-course AmBd. Ongoing electrolyte losses following AmBd 316
discontinuation mean supplementation and monitoring are needed for several 317
more days: an important implementation issue, as stable patients are usually 318
discharged following discontinuation of intravenous therapy. Short-course 319
regimens minimise toxicity whilst potentially maintaining efficacy, as well as 320
reducing costs of hospitalisation, intravenous administration and laboratory 321
monitoring. A phase III trial comparing short-course to standard AmBd 322
regimens is underway in Africa (ACTA, ISRCTN 45035509). Administration of 323
fewer, higher doses of liposomal preparations may be an alternative (AmBition-324
CM, ISRCTN 10248064). 325
326
Reported incidence of hypokalaemia (7 studies, variable definitions, 327
Supplementary Table 3) ranges from <1 to 56%. In this cohort, with routine pre-328
emptive supplementation with 20mmol KCl (and supplemental oral potassium 329
in South Africa), potassium levels changed little over 14 days. In the recent 330
large Vietnamese trial(10) 18% developed grade III hypokalaemia, as opposed 331
to only 6% in our cohort and 9% in a Ugandan cohort using pre-emptive 332
replacement(41). These data support WHO recommendations for pre-emptive 333
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

19
daily supplementation with 20mmol KCl IV, with additional oral 334
supplementation(12). 335
336
Despite oral supplementation, hypomagnesaemia was much more common 337
than hypokalemia in our cohort. Unfortunately, magnesium was not measured 338
at study sites where routine supplementation was not given, for comparison. 339
Lack of availability of magnesium monitoring or oral replacement preparations 340
(magnesium chloride or glycerophosphate) is a problem. IV magnesium 341
(usually stocked for pre-eclampsia) can be considered for patients with severe 342
deficiency or those remaining hypokalaemic despite potassium replacement(12). 343
344
Rates of anaemia reported in 8 studies (variable definitions, Supplementary 345
Table 3) were 37-44%. Two trials reported an average Hb drop of 1.5-2.5g/dL: 346
in one, 59% of patients were transfused (34, 38). Despite development of grade 347
IV anaemia (Hb<6.5g/dL) in 16% of our cohort, with a mean decrease in 348
haemoglobin of 2.3g/dL over 14 days, only 4% of patients received 349
transfusions, reflecting the scarcity of blood for transfusion in Africa. Severe 350
AmBd-induced anaemia is potentially life-threatening in such settings, given 351
the low baseline Hb and current lack of validated preventative interventions. 352
353
Addition of oral 5FC to AmBd did not result in clinically significant excess 354
toxicity in our cohort, with slightly greater drop in haemoglobin, but no 355
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

20
increase in rates of neutropenia or thrombocytopenia, an important observation 356
given this combination remains the recommended CM induction regimen. 357
358
Development of nephrotoxicity and severe anaemia were independent risk 359
factors for mortality, with odds of dying at 10 weeks increased two-fold in 360
patients with a haemoglobin decrease below 7.5g/dL and more than four-fold 361
in those with a creatinine increase above 220μmol/L. Using these cut-offs, 362
anaemia was more than 3 times more common than nephrotoxicity. The lack of 363
association between hypokalaemia and mortality is likely related to routine pre-364
emptive potassium replacement. 365
366
A limitation of this study is the pooling of data from multiple cohorts treated 367
with different AmBd-based combination regimens from four countries on two 368
continents over an 8-year period. Although toxicity management was uniform 369
across trial sites, there may have been heterogeneities in clinical management. 370
To address this, we adjusted for potential variable-specific and outcome-related 371
confounders in the multivariate analyses, as well as including an additional 372
‘study’ variable to try to account for any residual confounding due to 373
unmeasured effects related to temporal or site-specific differences. 374
375
Findings from this large cohort of patients treated in resource-poor settings 376
demonstrate that, with appropriate laboratory monitoring, it is possible to 377
implement the most fungicidal AmBd-based induction-treatment regimens for 378
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

21
HIV-associated CM using a standardised protocol for pre-emptive toxicity 379
management. Hypokalaemia was minimised and nephrotoxicity occurred in 380
<10% of patients. Anaemia remains a concerning side effect. Shorter courses of 381
AmBd are less toxic, with rapid reversibility. The implementation of 382
standardised protocols for pre-emptive toxicity management is a priority in 383
high HIV prevalence countries to maximise the benefits of a drug that is likely 384
to remain a cornerstone of CM treatment for many years to come. 385
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

22
Acknowledgements 386
Conflicts of interest: TB has attended an Advisory Board and received sponsorship 387
for conference attendance from Gilead Sciences Ltd and Astellas Pharma Inc. JNJ 388
and TSH are principal investigators in an investigator-led trial funded by Gilead. 389
For the remaining authors no conflicts were declared. 390
391
Source of Funding: This work was supported by a Wellcome Trust Intermediate 392
Clinical Fellowship (WT 089966 to TB) and a Wellcome Trust Training Fellowship 393
(WT 081794 to JNJ). 394
Other authors’ funding sources include Medical Research Council (UK) to TSH 395
(G0501476), UNC Center for AIDS Research P30-AI50410 and the NIH Fogarty 396
AIDS International Training and Research Program (DHHS/NIH/FIC 2-D43 397
TW01039 to CvDH, MH). Studies in Thailand were part of the Wellcome Trust 398
Mahidol University Oxford Tropical Medicine Research programme funded by the 399
Wellcome Trust. GM is supported by a Wellcome Trust fellowship (098316) and 400
the National Research Foundation (NRF) of South Africa (UID 85858). GM 401
acknowledges that opinions, findings and conclusions or recommendations 402
expressed in any publication generated by the NRF supported research are that of 403
the author(s), and that the NRF accepts no liability whatsoever in this regard. 404
405
406
407
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
23
References 408
1. Gallis, HA, Drew, RH, Pickard, WW. 1990. Amphotericin B: 30 years of clinical experience. 409 Review of Infectious Diseases. 12:308-329. 410
2. Dismukes, WE, Cloud, G, Gallis, HA, Kerkering, TM, Medoff, G, Craven, PC, Kaplowitz, LG, 411 Fisher, JF, Gregg, CR, Bowles, CA. 1987. Treatment of cryptococcal meningitis with combination 412 amphotericin B and flucytosine for four as compared with six weeks. N. Engl. J. Med. 317:334-341. 413 doi: 10.1056/NEJM198708063170602. 414
3. Bennett, JE, Dismukes, WE, Duma, RJ, Medoff, G, Sande, MA, Gallis, H, Leonard, J, Fields, 415 BT, Bradshaw, M, Haywood, H. 1979. A comparison of amphotericin B alone and combined with 416 flucytosine in the treatment of cryptoccal meningitis. N. Engl. J. Med. 301:126. 417
4. Atkinson, AJ, Bennett, JE. 1978. Amphotericin B pharmacokinetics in humans. Antimicrob. 418 Agents Chemother. 13:271-276. 419
5. Larsen, RA, Leal, MAE, Chan, LS. 1990. Fluconazole Compared with Amphotericin B plus 420 Flucytosine for Cryptococcal Meningitis in AIDSA Randomized Trial. Ann. Intern. Med. 113:183-421 187. 422
6. van der Horst, Charles M, Saag, MS, Cloud, GA, Hamill, RJ, Graybill, JR, Sobel, JD, Johnson, 423 PC, Tuazon, CU, Kerkering, T, Moskovitz, BL. 1997. Treatment of cryptococcal meningitis 424 associated with the acquired immunodeficiency syndrome. N. Engl. J. Med. 337:15-21. 425
7. Saag, MS, Powderly, WG, Cloud, GA, Robinson, P, Grieco, MH, Sharkey, PK, Thompson, SE, 426 Sugar, AM, Tuazon, CU, Fisher, JF. 1992. Comparison of amphotericin B with fluconazole in the 427 treatment of acute AIDS-associated cryptococcal meningitis. N. Engl. J. Med. 326:83-89. 428
8. de Lalla, F, Pellizzer, G, Vaglia, A, Manfrin, V, Franzetti, M, Fabris, P, Stecca, C. 1995. 429 Amphotericin B as primary therapy for cryptococcosis in patients with AIDS: reliability of relatively 430 high doses administered over a relatively short period. Clinical Infectious Diseases. 20:263-266. 431
9. Pappas, PG, Chetchotisakd, P, Larsen, RA, Manosuthi, W, Morris, MI, Anekthananon, T, 432 Sungkanuparph, S, Supparatpinyo, K, Nolen, TL, Zimmer, LO. 2009. A phase II randomized trial 433 of amphotericin B alone or combined with fluconazole in the treatment of HIV-associated 434 cryptococcal meningitis. Clinical Infectious Diseases. 48:1775-1783. 435
10. Day, JN, Chau, TT, Wolbers, M, Mai, PP, Dung, NT, Mai, NH, Phu, NH, Nghia, HD, Phong, 436 ND, Thai, CQ. 2013. Combination antifungal therapy for cryptococcal meningitis. N. Engl. J. Med. 437 368:1291-1302. 438
11. Perfect, JR, Dismukes, WE, Dromer, F, Goldman, DL, Graybill, JR, Hamill, RJ, Harrison, TS, 439 Larsen, RA, Lortholary, O, Nguyen, MH. 2010. Clinical practice guidelines for the management of 440 cryptococcal disease: 2010 update by the Infectious Diseases Society of America. Clinical Infectious 441 Diseases. 50:291-322. 442
12. World Health Organisation Rapid advice: Diagnosis, prevention and management of 443 cryptococcal disease in HIV-infected adults, adolescents and children. Geneva, Switzerland 2011. 444
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

24
13. Deray, G. 2002. Amphotericin B nephrotoxicity. J. Antimicrob. Chemother. 49:37-41. 445
14. Bicanic, T, Wood, R, Meintjes, G, Rebe, K, Brouwer, A, Loyse, A, Bekker, LG, Jaffar, S, 446 Harrison, T. 2008. High-dose amphotericin B with flucytosine for the treatment of cryptococcal 447 meningitis in HIV-infected patients: a randomized trial. Clinical Infectious Diseases. 47:123-130. 448
15. Llanos, A, Cieza, J, Bernardo, J, Echevarria, J, Biaggioni, I, Sabra, R, Branch, RA. 1991. Effect of 449 salt supplementation on amphotericin B nephrotoxicity. Kidney Int. 40:302-308. 450
16. Stein, R, Alexander, J. 1989. Sodium protects against nephrotoxicity in patients receiving 451 amphotericin B. Am. J. Med. Sci. 298:299-304. 452
17. Mayer, J, Doubek, M, Doubek, J, Horký, D, Scheer, P, Štěpánek, M. 2002. Reduced 453 nephrotoxicity of conventional amphotericin B therapy after minimal nephroprotective measures: 454 animal experiments and clinical study. J. Infect. Dis. 186:379-388. 455
18. Branch, RA. 1988. Prevention of Amphotericin B--Induced Renal Impairment: A Review on the 456 Use of Sodium Supplementation. Arch. Intern. Med. 148:2389. 457
19. Girmenia, C, Cimino, G, Di Cristofano, F, Micozzi, A, Gentile, G, Martino, P. 2005. Effects of 458 hydration with salt repletion on renal toxicity of conventional amphotericin B empirical therapy: a 459 prospective study in patients with hematological malignancies. Supportive Care in Cancer. 13:987-460 992. 461
20. Yeo, E, Ryu, J, Cho, Y, Chun, Y, Huang, LE, Kim, M, Park, J. 2006. Amphotericin B blunts 462 erythropoietin response to hypoxia by reinforcing FIH-mediated repression of HIF-1. Blood. 463 107:916-923. 464
21. Loyse, A, Thangaraj, H, Easterbrook, P, Ford, N, Roy, M, Chiller, T, Govender, N, Harrison, 465 TS, Bicanic, T. 2013. Cryptococcal meningitis: improving access to essential antifungal medicines in 466 resource-poor countries. The Lancet Infectious Diseases. 13:629-637. 467
22. Bicanic, T, Meintjes, G, Wood, R, Hayes, M, Rebe, K, Bekker, LG, Harrison, T. 2007. Fungal 468 burden, early fungicidal activity, and outcome in cryptococcal meningitis in antiretroviral-naive or 469 antiretroviral-experienced patients treated with amphotericin B or fluconazole. Clinical Infectious 470 Diseases. 45:76-80. 471
23. Brouwer, AE, Rajanuwong, A, Chierakul, W, Griffin, GE, Larsen, RA, White, NJ, Harrison, 472 TS. 2004. Combination antifungal therapies for HIV-associated cryptococcal meningitis: a 473 randomised trial. Lancet. 363:1764-1767. 474
24. Jarvis, JN, Meintjes, G, Rebe, K, Williams, GN, Bicanic, T, Williams, A, Schutz, C, Bekker, L-, 475 Wood, R, Harrison, TS. 2012. Adjunctive interferon- immunotherapy for the treatment of HIV-476 associated cryptococcal meningitis: A randomized controlled trial. AIDS. 26:1105-1113. 477
25. Muzoora, CK, Kabanda, T, Ortu, G, Ssentamu, J, Hearn, P, Mwesigye, J, Longley, N, Jarvis, 478 JN, Jaffar, S, Harrison, TS. 2012. Short course amphotericin B with high dose fluconazole for HIV-479 associated cryptococcal meningitis. J. Infect. 64:76-81. 480
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

25
26. Loyse, A, Wilson, D, Meintjes, G, Jarvis, JN, Bicanic, T, Bishop, L, Rebe, K, Williams, A, 481 Jaffar, S, Bekker, L-, Wood, R, Harrison, TS. 2012. Comparison of the early fungicidal activity of 482 high-dose fluconazole, voriconazole, and flucytosine as second-line drugs given in combination 483 with amphotericin B for the treatment of HIV-associated cryptococcal meningitis. Clinical Infectious 484 Diseases. 54:121-128. 485
27. Jackson, AT, Nussbaum, JC, Phulusa, J, Namarika, D, Chikasema, M, Kanyemba, C, Jarvis, 486 JN, Jaffar, S, Hosseinipour, MC, van der Horst, C. 2012. A phase II randomized controlled trial 487 adding oral flucytosine to high-dose fluconazole, with short-course amphotericin B, for 488 cryptococcal meningitis. AIDS. 26:1363-1370. 489
28. Brouwer, AE, van Kan, HJ, Johnson, E, Rajanuwong, A, Teparrukkul, P, Wuthiekanun, V, 490 Chierakul, W, Day, N, Harrison, TS. 2007. Oral versus intravenous flucytosine in patients with 491 human immunodeficiency virus-associated cryptococcal meningitis. Antimicrob. Agents 492 Chemother. 51:1038-1042. 493
29. Jarvis, J, Bicanic, T, Loyse, A, Namarika, D, , J, A, Nussbaum, J, Longley, N, Muzoora, C, 494 Phulusa, J, Taseera, K, Kanyembe, C, Wilson, D, Hosseinipour, M, Brouwer, A, 495 Limmathurotsakul, D, White, N, van der Horst, C, Wood, R, Meintjes, G, Bradley, J, Jaffar, S, 496 Harrison, TS. Determinants of mortality in a combined cohort of 501 patients with HIV-associated 497 Cryptococcal meningitis: implications for improving outcomes. - Clin Infect Dis.2014 Mar;58(5):736-498 45.Doi: 10.1093/Cid/cit794.Epub 2013 Dec 6. . 499
30. Sawaya, BP, Briggs, JP, Schnermann, J. 1995. Amphotericin B nephrotoxicity: the adverse 500 consequences of altered membrane properties. J. Am. Soc. Nephrol. 6:154-164. 501
31. Robinson, PA, Bauer, M, Leal, MAE, Evans, SG, Holtom, PD, Diamond, DM, Leedom, JM, 502 Larsen, RA. 1999. Early mycological treatment failure in AIDS-associated cryptococcal meningitis. 503 Clinical Infectious Diseases. 28:82-92. 504
32. Hamill, RJ, Sobel, JD, El-Sadr, W, Johnson, PC, Graybill, JR, Javaly, K, Barker, DE. 2010. 505 Comparison of 2 doses of liposomal amphotericin b and conventional amphotericin B deoxycholate 506 for treatment of AIDS-associated acute cryptococcal meningitis: A randomized, double-blind 507 clinical trial of efficacy and safety. Clinical Infectious Diseases. 51:225-232. 508
33. Leenders, AC, Daenen, S, Jansen, RL, Hop, WC, Lowenberg, B, Wijermans, PW, Cornelissen, 509 J, Herbrecht, R, Lelie, HVD, Hoogsteden, HC. 1998. Liposomal amphotericin B compared with 510 amphotericin B deoxycholate in the treatment of documented and suspected neutropenia‐511 associated invasive fungal infections. Br. J. Haematol. 103:205-212. 512
34. Sharkey, PK, Graybill, JR, Johnson, ES, Hausrath, SG, Pollard, RB, Kolokathis, A, Mildvan, 513 D, Fan-Havard, P, Eng, RH, Patterson, TF. 1996. Amphotericin B lipid complex compared with 514 amphotericin B in the treatment of cryptococcal meningitis in patients with AIDS. Clinical 515 Infectious Diseases. 22:308-314. 516
35. Tansuphaswadikul, S, Maek-a-Nantawat, W, Phonrat, B, Boonpokbn, L, Mctm, AG, 517 Pitisuttithum, P. 2006. Comparison of one week with two week regimens of amphotericin B both 518 followed by fluconazole in the treatment of cryptococcal meningitis among AIDS patients. J. Med. 519 Assoc. Thai. 89:1677-1685. 520
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

26
36. Pitisuttithum, P, Tansuphasawadikul, S, Simpson, A, Howe, P, White, N. 2001. A prospective 521 study of AIDS-associated cryptococcal meningitis in Thailand treated with high-dose amphotericin 522 B. J. Infect. 43:226-233. 523
37. Kambugu, A, Meya, DB, Rhein, J, O'Brien, M, Janoff, EN, Ronald, AR, Kamya, MR, Mayanja-524 Kizza, H, Sande, MA, Bohjanen, PR. 2008. Outcomes of cryptococcal meningitis in Uganda before 525 and after the availability of highly active antiretroviral therapy. Clinical Infectious Diseases. 526 46:1694-1701. 527
38. Joly, V, Aubry, P, Ndayiragide, A, Carrière, I, Kawa, E, Mlika-Cabanne, N, Aboulker, J, 528 Coulaud, J, Larouze, B, Yeni, P. 1996. Randomized comparison of amphotericin B deoxycholate 529 dissolved in dextrose or Intralipid for the treatment of AIDS-associated cryptococcal meningitis. 530 Clinical Infectious Diseases. 23:556-562. 531
39. Lightowler, JV, Cooke, GS, Mutevedzi, P, Lessells, RJ, Newell, M, Dedicoat, M. 2010. 532 Treatment of cryptococcal meningitis in KwaZulu-Natal, South Africa. PloS One. 5:e8630. 533
40. Boulware DR, Meya DB, Muzoora C, Rolfes MA, Huppler Hullsiek K, Musubire A, Taseera 534 K, Nabeta HW, Schutz C, Williams DA, Rajasingham R, Rhein J, Thienemann F, Lo MW, 535 Nielsen K, Bergemann TL, Kambugu A, Manabe YC, Janoff EN, Bohjanen PR, Meintjes G. 2014. 536 Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. New Engl J Med. 537 370(26):2487-98. 538
41. Bahr, NC, Rolfes, MA, Musubire, A, Nabeta, H, Williams, DA, Rhein, J, Kambugu, A, Meya, 539 DB, Boulware, DR. 2014. Standardized electrolyte supplementation and fluid management 540 improves survival during amphotericin therapy for Cryptococcal meningitis in resource-limited 541 settings. Open Forum Infectious Diseases 1 (2), ofu070 542
42. Luber, AD, Maa, L, Lam, M, Guglielmo, BJ. 1999. Risk factors for amphotericin B-induced 543 nephrotoxicity. J. Antimicrob. Chemother. 43:267-271. 544
545
546
547
548
549
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

27
Figure legends 550
Figure 1. Individual data points and fitted Loess curves for haemoglobin values 551
over the first 14 days of antifungal therapy 552
1a. All patients receiving 14 days’ AmB-based induction therapy 1b. Plot by AmB 553
duration short-course vs standard 1c. Plot by sex 554
Broken line indicates DAIDS grade IV adverse event threshold of 6.5 g/dL. 555
556
Figure 2. Individual data points and fitted Loess curves for creatinine values over 557
the first 14 days of antifungal therapy 558
2a. All patients receiving 14 days’ AmB-based induction therapy 2b. Plot by AmB 559
dose, 0.7 vs 1mg/kg/d. 2c. Plot by AmB duration short-course vs standard 560
Broken line indicates threshold of 220μmol/L (protocol definition of 561
nephrotoxicity). 562
563
564
565
566
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

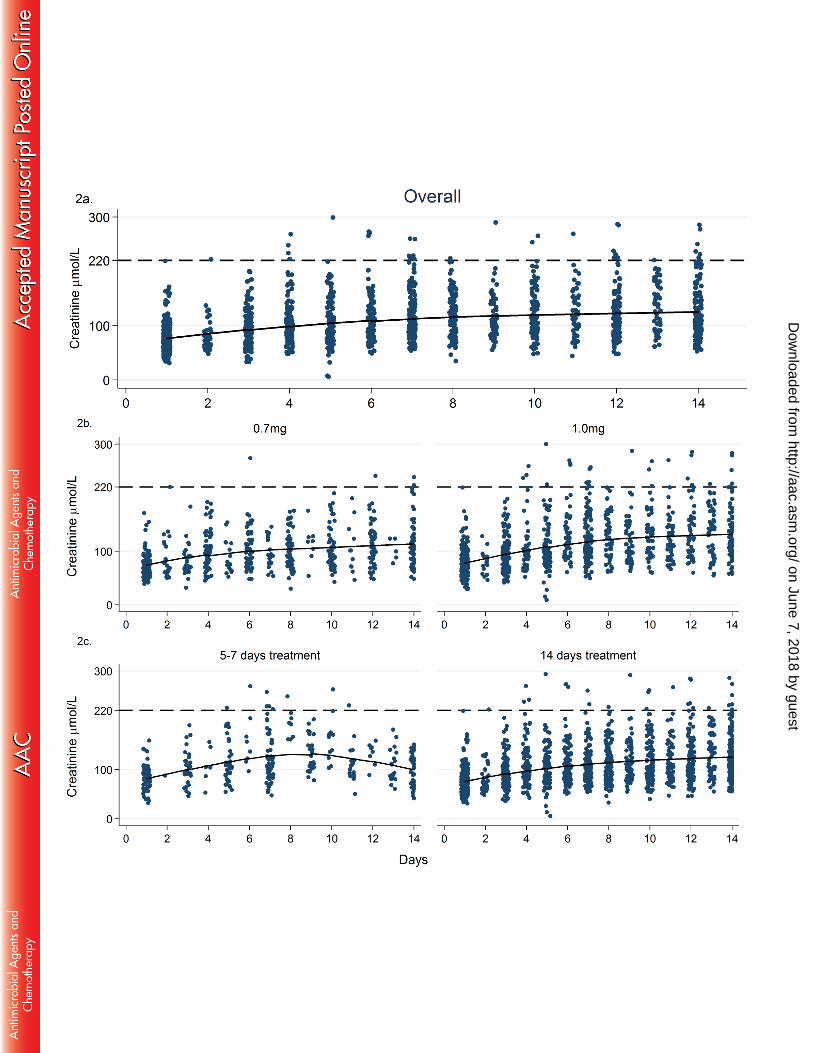

Table 1. Changes in laboratory parameters from baseline over 1 and 2 weeks’ AmBd treatment
Laboratory parameter Baseline value absolute change to day 7 % change to day 7 absolute change to day 14a % change to day 14a
Haemoglobin (g/dL) 11 (10.4, 11.6) -1.5 (-1.9, -1) -12 (-16, -9) -2.3 (-3.6, -1.1) -20 (-32, -8)
Creatinine (umol/L) 77 (68,87) +37 (30, 45) +52 (43, 62) +49 (35, 64) +73 (53, 93)
Potassium (mmol/L) 3.9 (3.8, 4.0) +0.2 (-0.0, 0.5) +9 (3,15) +0.1 (-0.1, 0.3) +6 (-1, 11)
Magnesium (mmol/L) 0.7 (0.6,, 0.8) -0.07 (-0.12, -0.02) -1(-7, 5) -0.15 (-0.2, -0.1) -10 (-33, -13)
Neutrophils (x10^9/L) 3.5 (2.2, 4.9) -0.1 (-0.4, 0.0.1) +8 (0.9, 14) -0.3 (-0.5, 0.0) +8 (-3, 20)
Values shown are means with 95% CI adjusted for study-level clustering
a. changes from baseline to day 14 are calculated only for patients enrolled in studies of standard course AmBd (1-4).
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

Table 2. Association between development of toxicities and 2- and 10-week mortality
Toxicity variable Category 2-wk
mortality
OR (95%CI)
univariable
P aOR (95% CI)
multivariable
P 10-wk
mortality
OR (95%CI)
univariable
P aOR (95% CI)
multivariable
P
2-week mortality
Nephrotoxicitya Creat peak >220umol/L 21% 3.1 (1.2-7.8) 0.018 2.8 (0.6-12.7) 0.17 53% 4.2 (2-8.8) <0.00
1
4.5(1.8-11) 0.001
<220umol/L 8% 1 1 21% 1 1
Anaemia
Grade III/ IV
Hb nadir <7.5g/dL 6% 0.8 (0.33-2) 0.65 - 31% 2.1 (1.2-3.5) 0.008 2.2 (1.1-4.3) 0.028
>7.5g/dL 8% 1 18% 1 1
Hypokalaemia
Grade III
K nadir <2.5 mmol/L 6% 0.77 (0.1-
6.1)
0.81 - 25% 0.99 (0.3-
3.2)
0.99 -
>2.5 mmol/L 8% 1 25% 1
Adjusted for the baseline variable (Hb1, Creat1, K1), baseline fungal burden, mental status, CD4 count and study.
a. Because of the association of weight with nephrotoxicity as well as outcome, weight was additionally adjusted for in the nephrotoxicity analysis
on June 7, 2018 by guesthttp://aac.asm
.org/D
ownloaded from