tracheostomy care bundle guidelinesnwcriticalcare.com/wp-content/uploads/2016/05/... ·...
TRANSCRIPT

EirianEdwards(SeniorStaffNurse,CriticalCare,BCUHBWest)(September,2013.UpdatedMay,2015)
TRACHEOSTOMY
CAREBUNDLE
GUIDELINES
Author:EirianEdwards(SeniorStaffNurse,CriticalCare,BCUHBWest)
ContributionsfromAshaMetharam-Jones(SeniorPhysiotherapist,BCUHBWest)
(September,2013.UpdatedMay,2015)
1
CONTENTS
• Aims• Definition• Indicationsfortemporarytracheostomy• Tracheostomytubes• CareBundleElement
1. Tracheostomytubecare2. Suction3. Humidification4. Tracheostomydressingsandstomacare5. Safety6. Communication7. Swallowing
• Referencesandfurtherreading• Appendix1–Tracheostomy/LaryngectomyEmergencyalgorithm
&bedsigns• Appendix2–Dischargeform&Bedareachecklist• Appendix3–
a) Swallowingassessmentforcuffedtracheostomyb) Swanseaswallowscreenforuncuffed/deflatedcuffed
tracheostomyc) SwanseaTrackingsheet

2
AIMS
Theaimofthetracheostomycarebundleistostandardisethecareofadultpatientswithtemporarytracheostomiesinacriticalcareenvironment.
ThetracheostomycarebundlefollowstherecommendationsontracheostomycarefromtheNCEPOD(2014)report“OntheRightTrach”providingguidanceonhumidification,cuffpressure,monitoringandcleaningofinnercannula.
Thecarebundlehasbeendevelopedutilisingthe‘IntensiveCareSocietyStandardsandGuidelinesforthecareofadultpatientswithatemporarytracheostomy’(Mackenzieetal,2008&2014),‘StGeorge’shealthcareNHSTrust,Guidelinesforthecareofpatientswithtracheostomytubes’(Laws-Chapmanetal,2000),‘theRoyalMarsdenHospital’smanualofclinicalnursingprocedures’(DoughertyandLister,2011),andevidenceobtainedfromrelevantliteraturesupportingbestclinicalpracticefortracheostomymanagement.Imagesareusedforillustrationonly,andtubesmaydiffertoimagesshowndependingonthemanufactures.
DEFINITION
Atracheostomyisthesurgicalopening(stoma)intothetracheathroughtheneck,andiskeptpatentwithatracheostomytube(DoughertyandLister,2011).Tracheostomiescaneitherbetemporaryorpermanent.Permanenttracheostomyisformedfollowingatotallaryngectomy.
Atracheostomymaybeperformedsurgicallyorpercutaneously,andasanemergencyorelectiveprocedure.
INDICATIONSFORTEMPORARYTRACHEOSTOMY
• Airwayprotectione.g.bulbarpalsy• Tomaintaintheairwaye.g.reducedlevelofconsciousness,upper-airwayobstruction,
intubationdifficulties• Toenabletheaspirationoftracheobronchialsecretionse.g.excessivesecretions,inadequate
cough• Long-termmechanicalventilatione.g.weaningfromIPPV,patientcomfort,reductionof
sedation
TheinsertionofaTracheostomywhereverperformedisidentifiedasasurgicalprocedure.TheNCEPOD(2014)recommendsthataWHOstylechecklistisusedinrelationtotracheosotomyproceduresinCriticalCareunits.

3
TRACHEOSTOMYTUBES
Tracheostomytubesshouldbechosentakingintoaccountthepatientandtubecharacteristicsandnotjusttheeaseofinsertion(ICS,2014).Itisrecommendedthattheentiretubeshouldbechangedatleastevery30daysoraspermanufacturer’srecommendations.
Itisrecommendedthatallpatientshaveadualcannulatracheostomyinserted.Atracheostomywithaninnercannulaaresafer,theinnercannulacanprovideimmediatereliefoflife-threateningairwayobstructionintheeventofablockedtracheostomytube.Manytracheostomytubesarenowmanufacturedwithaninnercannula.
SINGLELUMEN
Thesinglelumenhasalargerinnerdiameterthanadoublelumentube,anddoesnothavearemovableinnercannula.DOUBLELUMEN(INNERCANNULA)Theinnercannulahasastandard15mmattachmenttoconnecttothebreathingcircuitofamechanicalventilator.Whilstsomeinnercannulasaredisposableforsingleuse,otherscanbecleanedandre-used.Theadvantageofaninnercannulaisthatitallowstheimmediatereliefoflife-threateningairwayobstructionintheeventofablockedtracheostomytube.Thesedualcannulatubesmayeitherbecuffedofuncuffedandfenestratedorunfenestrated.Thedoublelumenhasalargerexternaldiameterthanthesinglelumen.CUFFEDTRACHEOSTOMYTUBESIntheIntensiveCaresetting,mostpatientswillrequireacuffedtracheostomytubeinitially,bothtofacilitateeffectivemechanicalventilationandalsotoprotectthelowerrespiratorytractagainstaspiration.
UNCUFFEDTRACHEOSTOMYTUBES
Thistypeoftracheostomytubedoesnothaveacuffthatcanbeinflatedinsidethetrachea.Anuncuffedtubeissuitableforapatientnotrequiringpositiveventilation,butrequiredforsecretionclearanceandairwaymaintenance.
FENESTRATEDTRACHEOSTOMYTUBEAfenestratedtracheostomytubemaybeusedtoassistindirectingairflowtopassthepatient’soral/nasalpharynx(mouth,noseandvocalcords)aswellastheirtrachealstomawhenbreathing.Itdoescreateariskfororalandstomachcontentstoenterthelungsthroughthefenestrations.

4
Manufacturesdonotrecommendtheuseofsuchtubesatthetimeofpercutaneoustracheostomy,andgenerallytheyshouldnotbeusedwhilstapatientstillrequiresmechanicalventilationbecauseofsignificantriskofsurgicalemphysema(ICS,2014).PatientswhoareatriskofaspirationorareonIPPVshouldnothaveafenestratedtubeunlessanon-fenestratedinnercannulaisusedtoblockoffthefenestration.TheICS(2014)recommendsthatafenestratedtracheostomytubeshouldbeusedwithcautioninmechanicallyventilatedpatients,andonlywithpatientswhoareweaningfromventilation.Afenestratedtubeisthemostsuitableforweaningpatientsfromtheirtemporarytracheostomytube.Itismostusefulforpatientswhorequirebothperiodsofcuffinflation(toprotecttheairway)andcuffdeflation(toenableaspeakingvalvetobeused)(DoughertyandLister,2011).
ADJUSTABLEFLANGETracheostomytubeswithadjustableflangearespecificallydesignedforpatientswhohave‘deepsettracheas’,suchasthosewhoareobeseorhavedistortedanatomywithintheneckduetoinflammationandoedema.Patientswithspinalabnormalitiesmayalsobenefitfromthistypeoftube.

5
CAREELEMENT
1. TRACHEOSTOMYTUBECAREINNERCANNULAMANAGEMENTTheinnercannula(ifadoublelumentube)shouldberemoved,inspectedandwhennecessarychanged(ifdisposable)orcleaned(non-disposable)ifneeded.TheICS(2014)recommendsthatinanon-ventilatedpatienttheinnercannulashouldberegularlyremoved,cleanedorchangedatamaximumintervalof4hourlyinapatientwithaproductivechest,andatleast8hourlyinallcases,beingconsiderateofthepatient’sneedforsleepandrest.However,Laws-Chapmanetal(2000)recommendedthattheinnertubeshouldbeinspectedatleast4hourly,ormorefrequentlyifindicated.Ifthepatientappearstobeinrespiratorydistress,theinnercannulaneedstoberemovedandinspectedforencrustationimmediately.Therecommendationsof4-8hourlyinspectionoftheinnertubewillbeusedforthecarebundleincriticalcare.
Forapatientundergoingmechanicalventilation,itmaynotbesafetorepeatedlydisconnecttheventilatorcircuitandchange/cleantheinnertuberoutinely.Cleaningorchanginganinnertubeshouldalwaysrepresentthebestbalanceofrisktopatient.Ifaninnertubeisnotchanged/clean,thenitshouldbeclearlydocumentedandcommunicatedalongwiththerational(NationalTracheostomySafetyProject,2010).
GUIDELINESFORCHANGING/CLEANINGINNERCANNULAESSENTIALEQUIPMENT:
• Steriledressingpack• 0.9%sodiumchlorideorsterilewaterforcleaning• Disposableplasticapron,powder-freeglovesandeyeprotection• Bactericidalalcoholhandrub• TemporaryInnercannulaofthesamesizeasthetracheostomytubethatisinsitu(donot
useaninnercannulafromanewset,asallsetsareevidentlyhandfinished).Preprocedure,preoxygenatepatientifknowntodesaturate,andclearanysecretions.ACTION RATIONALEPerformprocedureusingacleantechnique. Tominimisetheriskofcontamination.
Positionpatientwithneckslightlyextended. Extendingtheneckwillmakeremovaland
insertionofthetubeeasier.Removethedressingpackfromitsouterwrappings.
Putonadisposableapronandeyeprotection.
Minimisecontaminationofsecretionsontonurse.
Cleanhandswithbactericidalhandrub.
Minimisetheriskofinfection.
Putoncleandisposablegloves.
Removetheinnercannulaandifdisposable,disposeinclinicalwaste.Ifnon-disposable,cleancannulawithsterile0.9%sodiumchlorideorsterilewateranddrythoroughly.Donotleavetheinnercannulatosoak.Atemporaryreplacementinnertube(ofthesamesize)canbeinsertedwhilstcleaningtakesplace.Trachy
Soakingtubescouldresultinabsorptionofthesolutionintothematerial,causingirritationtothetrachea,aswellasbacterialcolonizationinstagnantcleaningsolution.Placingatemporaryinnertubereducestheriskoftheoutertracheostomytubeobstructingwhilstcleaningisbeingundertaken.

6
cleaningspongescanbeusedtohelpcleaninsideinnertubeifneededReplacethecleaninnertubeandensureitissecuredina‘locked’position.
Documentthetimewheninnercannulawaschanged/cleaned,andthetypeofsecretionsthepatienthas.
Toensurestaffareawareoftheneedforandfrequencyofinnercannulachanges.
DougheryandLister(2011)
CUFFMANAGEMENTThetracheostomycuffprovidesasealtoenablepositivepressureventilationandalsoprovidessomeprotectionagainstaspirationofsecretions.Overinflatedcuffmaycauseischaemiaofthetrachealmucosaandtherebyleadtotrachealstenosis.Toolittlepressuremaymeanthatthecufffailstomakeanadequatesealagainstthetrachealmucosaandthepatientisatriskofaspiration.Thepressurewithinthecuffshouldbecheckedregularlywithahandheldpressuremonometerandshouldnotexceed25cmH₂O(ICS,2014).Cuffpressureneedstobecheckedeachnursingshiftor2-3timesdaily,andfollowinganytracheostomyrelatedintervention,anddocumentedonthechart.Ifanairleakoccurswiththecuffpressureatthemaximumrecommended,thetracheostomymayhavebecomedisplacedormayrequirechangingorresizing,askanaesthetiststoreviewpatient.
2. SUCTIONAneffectivecoughrequirestheclosureoftheglottis,thenthereopeningoftheglottisonceanadequateintrathoracicpressureisachieved.Whenatracheostomyisinsituthemechanismofclosingtheglottisiscompromised,sothepatient’sabilitytoremovesecretionsisreducedastheyareunabletogeneratethehighflowsrequiredforcoughing.Trachealsuctionisanessentialcomponentofmanagingsecretions,maintainingrespiratoryfunctionandapatientairway,DoughertyandLister(2011).However,suctioningmaybebothpainfulanddistressingforthepatient,andcanalsobecomplicatedbyhypoxemia,bradycardia(particularlyinpatientswithautonomicdysfunctionsuchasspinalinjuries),trachealmucosaldamage,bleeding,andintroductionofinfection(ICS,2014).Therefore,thesuctionrequirementsofanindividualpatientshouldbereassessedeachshiftanddocumented(ICS,2008).INDICATIONSFORSUCTIONING
• Coarsebreathsounds(crackles)onauscultation• Noisybreathing• Stridor• Increasedordecreasedrateofrespiration• Decreasedoxygensaturation(Sp0₂)• Copioussecretions• Patientattemptingtocough/clearsecretions• Distress• Poororabsentcough• Deterioratingskincolour
Edgtton-WinnandWright(2005),ChoateandBarbetti(2003).

7
SUCTIONCATHETERSIZEChoosingthecorrectsuctioncathetersizedependsonthesizeofthetracheostomytube.Thefollowingformulacanbeusedtodeterminethecorrectsizecatheter:Suctioncathetersize(Fg)=2x(sizeoftracheostomytube–2)Forexample,8.00mmIDtube:2x(8–2)=12Fg(ICS,2008)
SUCTIONPRESSURE
Excessivelyhighsuctionpressuremayleadtomucosaltrauma.Thelowestpossiblevacuumpressureshouldbeused,≤100–120mmHg(13-16kPa),tominimiseatelectasisandmucosaldamage(ICS,2008).
CLOSED-CIRCUITSUCTIONCATHETER
Closed-circuitsuctioncatheteristhepreferredwayofsuctioningamechanicallyventilatedpatientwithinthecriticalcareenvironment.Itisimportantthataclosedsuctiontracheostomycatheterisused,andnotanendotrachealcatheter,sincethesevaryinlength.Usinganendotrachealcatheterwithatracheostomytubecouldleadtodamageofthetrachealmucosaandtrauma.However,ifthepatienthasanadjustableflangedtracheostomytube,thenitmaybenecessarytouseanendotrachealsuctioncatheterduetothelengthoftheflangedtube.Theuseoftheclosed-circuitcatheterreducesthenumberoftimesthepatientisdisconnectedfromtheventilator,avoidingcross-infection,hypoxia,andlossofPEEP.
CLOSED-CIRCUITSUCTIONINGGUIDELINES
ACTION RATIONALEWashhandswithbactericidalsoapandwaterorbactericidalalcoholhandrub,andputonadisposableplasticapron,disposableglovesandeyeprotection.
Tominimisetheriskofcross-infection,incaseofaccidentaldisconnection.
Preoxygenatepatientpriortosuctioningifpatientisknowntodesaturatewithsuctioning.
Toreducetheriskofhypoxiaandarrhythmias.
Turnonthesuctionandcheckthesuctionpressure(≤100-120mmHg,13-16kPa).
Tominimiseatelectasis.
Passtheclosed-circuittracheostomysuctioncatheterintothetracheostomytube,whenthepatientcoughsorthepassageofthecatheterisobstructed,withdrawtipofthecatheterby0.5-1cm
Theclosed-circuitcatheterisinsertedwiththesuctionofftoavoidtrauma.Toreducetheriskoftraumatothetrachealmucosaandcarina.
Takeholdofthetracheostomytubeandclosed-circuitcatheter,applysuctionandwithdrawcatheter,takingnomorethan10seconds.
Tosupporttubeandminimisetheriskofdisconnection.Toreducetheriskofhypoxia.
Repeatthisactionasnecessary,allowingpatienttimetorecoverbetweeneachsuctioning.
Toensuregeneralconditionisstable.
Whensuctioniscomplete,ensureclosed-circuitcatheteriswithdrawnfully,andflushwith0.9%sodiumchloridebyapplyingsuctionwhileflushingviatheinstallationportontheclosed-circuitcatheter.
Toreducetheriskofany0.9%sodiumchloridepassingintopatient’sairways.Toflushsuctioncatheterandtubingafteruseassuringcontinuedpatency.
Laws-Chapmanetal(2000).

8
OPENSUCTIONGUIDELINESESSENTIALEQUIPMENT:
• Suctionsource(wallorportable),collectioncontainerandtubing• Disposableplasticapron,eyeprotection,selectionofnon-sterile,powder-free,cleanboxed
gloves• Bactericidalalcoholhandrub• Sterilesuctioncatheters(assortedsizesaccordingtotubesize)• Sterilebottledwater(labelled‘suction’withopeningdate),changedevery24hoursto
preventthegrowthofbacteria
ACTION RATIONALEIfapatienthasafenestratedoutertube,ensurethatanon-fenestratedinnercannulaisinsituforsuctioning.
Suctionviaafenestratedtubeallowsacathetertopassthroughthefenestrationandcausetraumatothetrachealwall.
Washhandswithbactericidalsoapandwaterorbactericidalalcoholhandrub,andputonadisposableplasticapron,disposableglovesandeyeprotection.
Tominimisetheriskofcross-infection.
Ifpatientisoxygendependentpreoxygenatepatient
Minimiseriskofhypoxia.
Ensurethesuctionpressureissetattheappropriatelevel.
Recommendedsuctionpressureis≤100-120mmHg(13-16kPa)tominimiseatelectasis.
Selectthecorrectcathetersize(seeaboveformula)
Incorrectchoiceofcathetersizecancausemucosaldamage.
Opentheendofthesuctioncatheterpackandusethepacktoattachthecathetertothesuctiontubing.Keeptherestofthecatheterinthesterilepacket.Useanasepticnon-touchtechniquethroughout.
Toreducetheriskoftransferringinfectionfromhandstothecatheterandtokeepthecatheterascleanaspossible.
Anadditionalclean,disposableglovecanbeusedonthedominanthandatthisstage.
Tofacilitateeasydisposalofthesuctioncatheteraftersuction.
Removethecatheterfromthesleeveandintroducethecathetertoaboutone-thirdofitslengthorapproximately10-15cmoruntilthepatientcoughs.Ifresistantisfelt,withdrawcatheterapproximately1cmbeforeapplyingsuctionbyplacingthethumboverthesuctionportcontrolandslowlywithdrawtheremainderofthecatheter.
Thecathetershouldgonofurtherthanthecarinatopreventtrauma.Thecatheterisinsertedwiththesuctionofftoreducetheriskoftrauma.
Donotsuctionthepatientformorethan10seconds.
Prolongedsuctioningmayresultinacutehypoxia,cardiacarrhythmias,mucosaltrauma,infectionandthepatientexperiencingafeelingofchoking.
Wrapcatheterarounddominanthand,thenpullbackgloveoversoiledcatheter,thuscontainingcatheteringlove,thendiscard.
Cathetersareusedonlyoncetoreducetheriskofintroducinginfection.
Ifthepatientisoxygendependent,reapplyoxygenimmediately.
Topreventhypoxia.
Rinsethesuctiontubingbydippingitsendintothesterilewaterbottleandapplyingsuctionuntilthesolutionhasrinsedthetubingthrough.
Toloosensecretionsthathaveadheredtotheinsideofthetube.
Ifthepatientrequiresfurthersuction,repeatthe Toensuregeneralconditionisstable.

9
aboveactionsusingnewglovesandanewcatheter,andallowthepatientsufficienttimetorecoverbetweensuction.DoughertyandLister(2011).
Anydifficultyinpassingthesuctioncathetershouldleadtoconsiderationthattheinnercannulamaybepartiallyblockedandthereforerequirechanging(ICS,2014).
3. HUMIDIFICATION
Innormalbreathing,inspiredairiswarmed,filteredandmoistenedbyciliatedepithelialcellsinthenoseandupperairway.Cellsintheepithelialliningproducemucus.Atracheostomytubewillby-passthesenaturalmechanismsforwarmingandmoisteninginspiredairandadministrationofdrygascausesphysiologicalchanges.Therefore,humidificationmustbeartificiallysupplementedtoassistnormalfunctionandfacilitatesecretionremoval,Laws-Chapmanetal(2000).Inadequatehumidificationmayleadtolife-threateningblockageofthetracheostomywithtenacioussputum,ulcerationofthetrachealmucosa,sputumretention,atelectasisandimpairedgasexchangeICS(2008).
HumidificationisessentialforALLhospitalisedpatientswithtracheostomies(andlaryngectomies).TheICS(2014)providesausefulHumidificationladderguide:
• Self-ventilatingpatients(nooxygen)–HME(Buchanonbib,Swedishnose)• Self-ventilatingpatientsonoxygen–coldwaterhumidification• Self-ventilatingpatientsonoxygenwiththicksecretions–heatedwaterhumidification• Ventilatedpatient/CPAPcircuit–heatedwaterhumidification(wetcircuit)
Patientswiththicksecretions,orwhorequirehighflowoxygentherapywillrequireheatedwaterhumidification(e.g.FisherandPaykel),andmayrequiresalinenebulisersprescribing.WetcircuitshouldbeusedifCPAPorPositivePressureVentilationisappliedviaatracheostomy.
Whenusingaheatedwaterhumidifier,monitoranddocumenttemperature2hourly,checkwaterlevel,andchangesterilewaterPRN.
HumidificationofinspiredgascanbeachievedinpatientswithminimalorlowoxygenrequirementsusingacoldwaterventurihumidifiersystemconnectedtoaT-pieceortracheostomymask.However,ifwarmedhumidificationisrequired,thiscanbeachievedusingtheAIRVOhumidifier.
4. TRACHEOSTOMYDRESSINGSANDSTOMACARE
Atracheostomyisasurgicalopeningintothetracheaandhenceapotentialrouteofinfection,sotheareashouldbekeptclean.Damagecanalsobecausedtothesurroundingtissuesthroughpressureandthepresenceofirritantsecretions,DoughertyandLister(2011).ICS(2008)recommendsthatthesiteshouldbeassessedandstomacleanedatleastoncein24hoursusingacleantechnique.Whenassessingthewound,ifinfectionissuspected,i.e.theareaisreddened,excoriated,painful,discolouredorexudateispresent,amicrobiologyswabshouldbesentforculture.Toprotectthesurroundingskinfrombecomingredandexcoriated,aCavilonwandcanbeused(Hampton,1998).

10
Contraindication:occasionallyasurgicalteammayrequestthattheoriginaldressingremainintactforaperiodoftime.Theremaybeanincreasedriskofbleedingassociatedwiththestomaformationandinthisinstancethedressingshouldnotbechangeduntilconsultationwiththesurgeonhasoccurred(DoughertyandLister,2011).
TRACHEOSTOMYDRESSINGCHANGEGUIDELINES
ESSENTIALEQUIPMENT:• Steriledressingpack• Tracheostomydressingandholder• Cleaningsolution,suchas0.9%sodiumchloride• Bactericidalalcoholhandrub
Thisprocedurerequirestwonurses.Oneisrequiredtoholdthetracheostomyinplace,andtheothertochangethedressing.ACTION RATIONALEWashhandsusingbactericidalsoapandwaterorbactericidalalcoholhandrub,andpreparethedressingtrolley.
Tominimisetheriskofinfection.
Performtheprocedureusingaseptictechnique. Removethesoileddressingfromaroundthetube,cleanaroundthestomawith0.9%sodiumchlorideusinggauze.
Toremovesecretionsandanycrusts.
Replacewithatracheostomydressing. Toavoidpressurefromthetube.Renewtracheostomytapes,checkingthat1–2fingerscanbeplacedbetweenthetapesandneck.
Tosecurethetube.Tominimisetheriskofreducedcerebralbloodflowfromthecarotidarteriesduetoexcessiveexternalpressure.
DoughertyandLister(2011).
5. SAFETY
Thefollowingequipmentshouldbeimmediatelyavailableatalltimesforapatientwithatracheostomy,bothbythebedsideaswellasduringtransfers.SomeequipmentmaybeavailableontheDifficultAirwayTrolley(see*).TheICS(2014)suggeststhata‘tracheostomybox’shouldbeusedtokeepequipmentthatgoeswiththepatientfromcriticalcaretotheward,’includingtransfer.
• Operationalsuctionunit,whichshouldbecheckedatleastdaily,withsuctiontubingattached
• Appropriatesizedsuctioncathetersandyankeurs• Non-powderedlatexfreegloves,apronsandeyeprotection• Sparetracheostomytubesofthesametypeasinserted:oneofthesamesizeandoneasize
smaller• Trachealdilators(availableatthebedsideorimmediatelyavailableontheDifficultyAirway
Trolley,tobeagreedlocally)• Watercircuitandfilter• Cathetermountorconnection• Tracheostomydisconnectionwedge

11
• Tracheostomytubeholderanddressing• 10mlsyringe(iftubecuffed)• ScissorsorStitchcutter(iftracheostomytubeissutured)• Oxygentubingandmask• Re-intubationequipment/resuscitationequipment• Trachealhook(seenotebelow)• Intubationdrugsfortransfer• Tracheostomy/Laryngectomyemergencyalgorithm• Tracheostomy/Laryngectomybedsign• Humidificationequipment• Cleanpotforspareinnercannula• Sterilewaterforcleaningthesuctiontubing(labelledanddated,changeevery24hours)• Watersolublelubricatingjelly• Steriledressingpack• Nursecallbell(whereavailable):thepatientmaybeunabletocallforhelpverbally• Communicationaids:thepatientmaynotbeabletoverbalise• Bedsideequipmentchecklist
ICS(2014)
Trachealhookshouldbeavailableonallcriticalcareunit(toanchoranteriortrachealwallduringtubechangesrecommendedbyENTsurgeonsforopenproceduresbutunfamiliartomanyotherstaff).TrachealhooktobeavailableontheDifficultAirwayTrolley.
Anemergencymanagementalgorithmshouldbeavailableatthepatientbedside,atracheostomymanagementalgorithmforatracheostomypatient,andaLaryngectomymanagementalgorithmforalaryngectomypatient.Thetracheostomy/laryngectomybedheadsignshouldcontainkeyinformationregardingthenatureanddateofthetracheostomy,includingemergencycontactdetails,seeappendix1.
Atthebeginningofeachshiftthenurseisresponsibleforcheckingthatallequipmentisavailableandinworkingorderincaseofanycomplicationsarising.
Atransfer/dischargechecklistneedstobecompletedwhentransferringapatientwithatracheostomytoanotherward/hospital,andplacedinthenursingnotesofthereceivingward(appendix2).
6. COMMUNICATION
Whenapatienthasatracheostomy,majorityoftheairisnolongerdirectedthroughthelarynx,sopatientsmaybeunabletocommunicateverbally,especiallywhenthecuffisinflated.EverypatientwithatracheostomyneedstobereferredtoSpeechandLanguagetherapy.
NON-VERBALCOMMUNCIATION
Itisimportantthatnon-verbalcommunicationisfacilitatedfromthebeginning:
• YES/NOquestions• Penandpaper
12
• Communicationchart:pictures,alphabetchart
VERBALCOMMUNICATION
PASSYMUIRVALVE(VENTILATORDEPENDENT)/SPEAKINGVALVE(SELFVENTILATINGPATIENT)
Ifapatientisventilatordependent,andfitsthefollowingcriteria,followinganagreementwithasenioranaesthetistandaseniorphysiotherapistaPassymuirvalvecouldbeusedtoaidcommunication(cuffmustbedeflated).Foraself-ventilatingpatient,consideraspeakingvalve.Speakingvalveshouldonlybeusedwithanuncuffedtube,acuffedtubewithcuffdeflatedorafenestratedtracheostomytubewithcuffdeflated,ICS(2014).Priortofittingaspeakingvalve,cuffmustbefullydeflatedandpatientassessedtoensurethereisasignificantleak.
ThePassy-Muirvalveisaone-wayvalvethatallowsventilatedpatienttovocalise.Theairpassesthroughthevalveintothelungsasnormalbuttheone-wayvalveredirectstheexpirationupthroughthevocalcords.ThePassy-MuirvalveshouldonlybeusedwithpatientsonCPAPASBwithaPEEP<10andASB<15andFi0₂<60%.However,theseareonlyguidelines,andthedecisionoftryingthePassy-Muirvalveshouldbedoneonanindividualbasisfollowingdiscussionswithasenioranaesthetistandseniorphysiotherapist.WhenthepatientisusingaPassy-Muirvalvetheventilatoralarmswillkeepalarmingbecausetheventilatorisnotabletodetectanoutbreath,thereforealarmsettingswillneedadjustingtocompensatethis.WhenthePassy-Muirvalveisremovedtheventilatorsettingsandalarmneedtoberesetasbefore.
CONTRAINDICATIONSFORUSINGPASSYMUIRVALVE/SPEAKINGVALVE:
• Unconsciousand/orcomatosepatients• Inflatedtracheostomytubecuff• Severeairwayobstructionwhichmaypreventsufficientexhalation• Verythickandtenacioussecretions• Severelyreducedlungelasticity• Severeaspiration• Notforusewithendotrachealtubes• Lessthan48-72hoursposttracheostomy• Postlaryngectomy• Postheadandnecksurgery
PRIORTOFITTINGPASSYMUIRVALVE/SPEAKINGVALVE:
• Patientisalert• Tracheostomytubewasinsertedatleast48-72hoursago• Allcontraindicationshavebeenoutruled• Thepatient’spulmonarystatusisstable(vitalsigns,O₂saturation>92,respiratoryrate<30,
airwaypatency)• Abletotoleratecuffdeflation• Ventilatorsettingsassessedbyanaesthetist(Ifventilated)• TracheostomytubecuffmustbefullydeflatedbeforeplacingthePassyMuirvalveor
speakingvalve• Iffenestratedtubeinsitu,ensuretheinnertubeisfenestratedforusewithspeakingvalve

13
Ifalloftheabovecriteriacannotbemet,donotfitaPassyMuirvalve/speakingvalveatthepresenttime.
Iftheabovecriteriaareallmetyoucanproceedwithcaution,followingagreementwithsenioranaesthetistandseniorphysiotherapist.
WHENFITTINGASPEAKINGVALVE:• MonitorOxygensaturations• Explainproceduretopatient• Suction• Deflatecuff(ifpresent),suction,changeinnertubetofenestrated(ifafenestrated
tracheostomyisinsitu),• Attachspeakingvalveandcontinuetomonitorpatient• Removeifpatientnottolerating
7. SWALLOWING
Patientswithtracheostomiesmayexperienceproblemswithswallowing.Thepresenceofaninflatedcuffcompressestheoesophagus,andmakesswallowingdifficultforsomepatients,increasingtheriskofaspiration.Theriskisgreatestinthosepatientswithassociatedneurologicalormechanicalcauseofdysphagia,orthosewithsignificanton-goingrespiratoryfailures,ICS(2014).Thedecisiontoallowfeedingwithcuffinflatedshouldbemadeonanindividualbasisafteraswallowingassessment.
Ifthepatienthasacuffedtracheostomytubewithcuffinflated,swallowingassessmentshouldbeperformedusingtheBCUHBguidelinesonassessingfordysphagiawithtracheostomytube(seeappendix3a),alongsidetheSwanseatrackingsheet(appendix3c)andresultdocumentedclearlyontheBCUHBassessmentform(appendix3a).Donotattemptaswallowingassessmentifthepatientisdrowsy,semi-consciousordoesnotopeneyestospeech.Ensurepatientisinanupright,supportedpositionpriortocommencingaswallowingassessment.Swallowingshouldbereassessedifcuffisdeflated.
Ifthepatienthasanuncuffedtubeoracuffedtubewithcuffdeflated,thentheswallowingassessmentshouldbedoneusingtheSwanseaSwallowingscreenguidelines(appendix3b)andmonitorusingtheSwanseatrackingsheet(appendix3c).DocumentassessmentandresultontheBCUHBassessmentform(appendix3a).Seeflowchartbelow.
Ifapatientshowssignsofaspirationwhennoneurologicalcomponentpresent,thenitisextremelyprobablethattheywillcontinuetoaspiratewhilethetracheostomytubeisinsituunlessthereisasignificantchangesuchaschangingtoadifferenttypeoftubeordeflatingthecuffifitwasinflated.

14
FlowchartforassessingswallowingwithTracheostomypatients:
Ifthepatientfailstoswalloweffectively,thenassessmentbyaspeechandlanguagetherapistisrecommended.Ifneurologicaldysphagiaissuspected,refertoSpeechandLanguageTherapyearly.
TheICS(2014)providedifferentriskfactorsforswallowingproblemsinpatientswithatracheostomy:
• Neurologicalinjury• Disuseatrophy• Headandnecksurgery• Evidenceofaspirationofenteralfeedororalsecretionsontrachealsuctioning• Increasedsecretionload,orpersistentwet/weakvoice,whencuffisdeflated• Coughingand/ordesaturationfollowingoralintake• Patientanxietyordistressduringoralintake• HighFiO₂
SWALLOWINGASSESSMENTFORTRACHEOSTOMYPATIENTINCRITICALCARE
CUFFEDTRACHEOSTOMYTUBEWITHINFLATEDCUFF
UNCUFFEDTRACHEOSTOMYTUBEorCUFFEDTUBEWITHDEFLATEDCUFF
• ASSESSSWALLOWINGUSINGBCUHBASSESSMENTFORDYSPHAGIAWITHTRACHEOSTOMYTUBE(appendix3a)
• RECORDSUCTIONONTHESWANSEATRACKINGSHEET(appendix3c)
• CLEARLYDOCUMENTRESULTONTHEBCUHBASSESSMENTFORDYSPHAGIAWITHTRACHEOSTOMYTUBE(appendix3a)
• ASSESSSWALLOWINGUSINGTHESWANSEASWALLOWSCREENGUIDELINES(appendix3b)
• RECORDSUCTIONONTHESWANSEATRACKINGSHEET(appendix3c)
• CLEARLYDOCUMENTASSESSMENTANDRESULTONTHEBCUHBASSESSMENTFORDYSPHAGIAWITHTRACHEOSTOMYTUBE(appendix3a)

15
REFERENCES.
Dougherty,L.andLister,S.(2011)TheRoyalMarsdenHospitalManualofClinicalNursingProcedures,8thed,Wiley-Blackwell,Chichester.
Choate,K.andBarbetti,J.(2003)Tracheostomy:Yourquestionsanswered.AustralianNursingJournal,10(11),1CU-4CU.
Edgtton-Winn,M.andWright,K.(2005)Tracheostomy:aguidetonursingcare.AustralianNursingJournal,13(5),17-20.
Hampton,S.(1998)Filmsubjectswintheday.NursingTimes,94(24),80-82.
ICS(2008)StandardsfortheCareofAdultPatientswithaTemporaryTracheostomy.IntensiveCareSociety,London.www.ics.ac.uk/intensive_care_professional/standards_and_guidelines/care_of_the_adult_patient_with_a_temporary_tracheostomy_2008
ICS(2014)StandardsfortheCareofAdultPatientswithaTemporaryTracheostomy;STANDARDSANDGUIDELINES.IntensiveCareSociety,London.http://www.ics.ac.uk/ics-homepage/guidelines-and-standards
Laws-Chapman,C.etal(2000)StGeorge’sHealthcareNHSTrust,CareofPatientswithTracheostomyTubes.London:SIMSPortexLtd.
NationalTracheostomySafetyProject(2010)Informationresourceforthesafermanagementofpatientswithtracheostomiesandlaryngectomies.www.tracheostomy.org.uk
PassyMuir(2008)PassyMuirTracheostomyandVentilatorSwallowingandSpeakingValvesInstructionBooklet.
FURTHERREADING
Bernhard,W.N.andCothalis,S.(1985)Intracuffpressuresinendotrachealandtracheostomytubes.Chest,87(6),720-725.
Burglass,E.(1999)Tracheostomycare:trachealsuctioningandhumidification.BritishJournalofNursing,8(8),500-504.
Day,T.,Haynes,S.,Waimwright,S.andWilson-Barnett,J.(2002)Trachealsuctioning:anexplorationofnurses’knowledgeandcompetenceinacuteandhighdependencywardareas.JournalofAdvancedNursing,3991),35-45.
Harkin,H.andRussell,C.(2001)Tracheostomypatientcare.NursingTimes,97(25),34-36.
Hettige,R.,Arora,A.,Ifeacho,S.&Narula,A.(2008)Improvingtracheostomymanagementthroughdesign,implementationandprospectiveauditofcarebundle:howwedoit.ClinicalOtolarynology,33(5),488-491.
McGrath,B.A.,Bates,L.,Atkinson,D.andMoore,J.A.(2012)Multidisciplinaryguidelinesforthemanagementoftracheostomyandlaryngectomyairwayemergencies.Anaesthesia,67(9),1025-1041.

16
Ontherighttrach?Areviewofthecarereceivedbypatientswhounderwentatracheostomy(2014)http://www.ncepod.org.uk/2014report1/downloads/On%20the%20Right%20Trach_FullReport.pdf
Russell,C.(2005)Providingthenursewithaguidetotracheostomycareandmanagement.BritishJournalofNursing,14(8),428-433.

17
Appendix1.
ReproducedfromMcGrathBA,BatesL,AtkinsonD,MooreJA.Multidisciplinaryguidelinesforthemanagementoftracheostomyandlaryngectomyairwayemergencies.Anaesthesia.2012Jun26.doi:10.1111/j.1365-2044.2012.07217,withpermissionfromtheAssociationofAnaesthetistsofGreatBritain&Ireland/BlackwellPublishingLtd."

18
ReproducedfromMcGrathBA,BatesL,AtkinsonD,MooreJA.Multidisciplinaryguidelinesforthemanagementoftracheostomyandlaryngectomyairwayemergencies.Anaesthesia.2012Jun26.doi:10.1111/j.1365-2044.2012.07217,withpermissionfromtheAssociationofAnaesthetistsofGreatBritain&Ireland/BlackwellPublishingLtd."
19
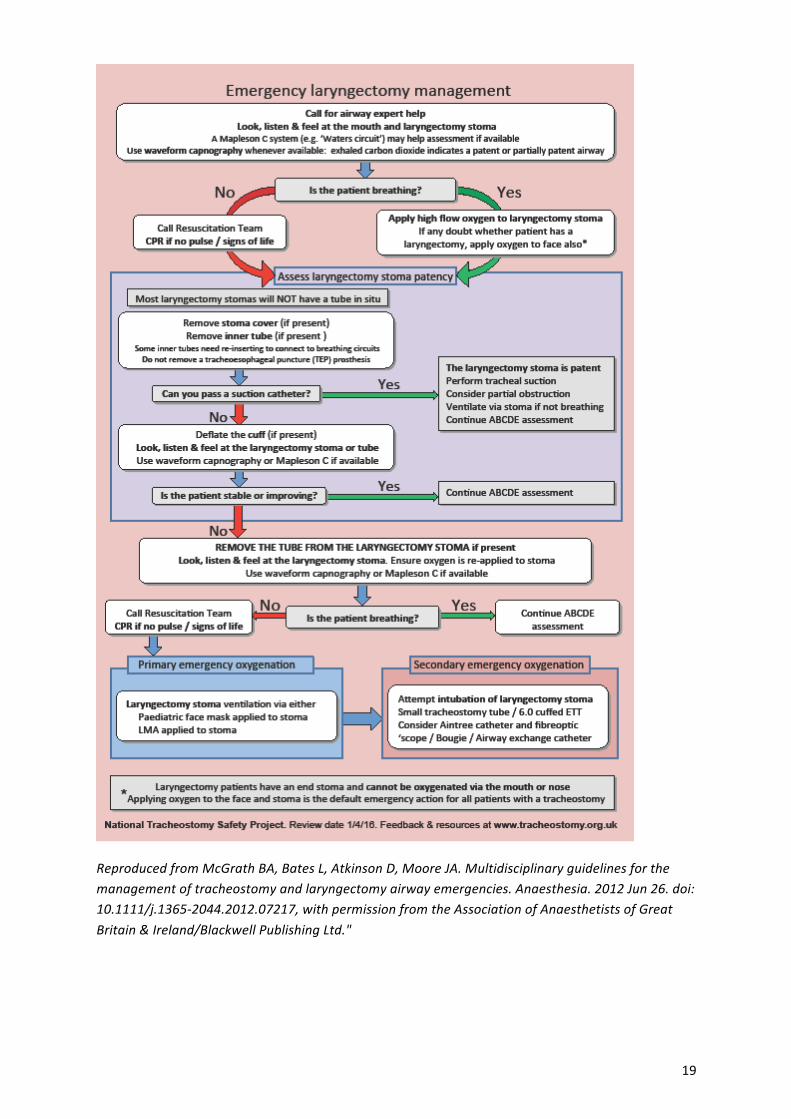
ReproducedfromMcGrathBA,BatesL,AtkinsonD,MooreJA.Multidisciplinaryguidelinesforthemanagementoftracheostomyandlaryngectomyairwayemergencies.Anaesthesia.2012Jun26.doi:10.1111/j.1365-2044.2012.07217,withpermissionfromtheAssociationofAnaesthetistsofGreatBritain&Ireland/BlackwellPublishingLtd."

20
ReproducedfromMcGrathBA,BatesL,AtkinsonD,MooreJA.Multidisciplinaryguidelinesforthemanagementoftracheostomyandlaryngectomyairwayemergencies.Anaesthesia.2012Jun26.doi:10.1111/j.1365-2044.2012.07217,withpermissionfromtheAssociationofAnaesthetistsofGreatBritain&Ireland/BlackwellPublishingLtd."

21
Transfer/DischargeFormforTracheostomyPatient Appendix2.Tobecompletedbythetransferringnurseandtoaccompanythepatientontransfer/discharge.
Tobeplacedinthenursingnotesofthereceivingward/hospital.Name:
Addressographlabel
Dateoftransfer:
Date:
Time:
Transferfrom: Wardreceiving:
Dateoftracheostomy:
Typeoftracheostomy:
Reasonfortracheostomy:
Tubechanged: YesDate: No
Dateofnextchange:
Staysuturestotrachealwall: Yes No
Make/Typeoftube:
Innertube: Yes No
Cuffstatus:inflated? Yes No
Size:
Frequencyrequiredforcleaninginnertube:
Reasonforcuffinflation:
Reasonforcuffdeflation(e.g.uncuffed):
Swallowscreen: YesDate: No
Ifno,why?
Referraltospeechtherapyforformalswallowassessment:
YesDate: No
Typeofhumidification:
PrescribedO2therapy:
Sparetube: Yes
Suction: Yes
Patientmustnotbeleftwithouttheseitems.
Trachealdilators: Yes
Disconnectionwedge: Yes
PleaseseeoverleafforequipmentlistasperICSGuidance
Stomasite:Pleasetick Dry Inflammation Excoriation
Secretions:Type:Amount:
Comments:Signaturetransferringnurse:
Signaturereceivingnurse:
Printname:
Printname:

22
Bedsideequipmentforalltracheostomypatients(Ref:ICS2014)Thefollowingequipmentshouldbeimmediatelyavailableatalltimesforapatientwithatracheostomy,bothbythebedsideaswellasduringtransfers.SomeequipmentmaybeavailableontheDifficultAirwayTrolley(see*):
Operationalsuctionunit,whichshouldbecheckedatleastdaily,withsuctiontubingattachedandYankeursucker
Appropriatelysizedsuctioncatheters Non-powderedlatexfreegloves,apronsandeyeprotection Sparetracheostomytubesofthesametypeasinserted:onethesamesizeandone
asizesmaller Trachealdilators Rebreathingbagandtubing Cathetermountorconnection Tracheostomydisconnectionwedge* Tracheostomytubeholderanddressing 10mlsyringe(iftubecuffed) Resuscitationequipment Trachealhook*(toanchoranteriortrachealwallduringtubechanges
recommendedbyENTsurgeonsforopenproceduresbutunfamiliartomanyotherstaff).
Humidificationequipment Cleanpotforspareinnercannula Sterilewaterforcleaningthesuctiontube Scissorsorstitchcutteriftracheostomytubeissutured) Watersolublelubricatingjelly Steriledressingpack Nursecallbell(whereavailable):thepatientmaybeunabletocallforhelpverbally Communicationaids:thepatientmaynotbeabletoverbalise Bedsideequipmentlist

23
Appendix3a.
Assessed by:
Patient's Label
Date:
Consultant: Medical consent for assessment: YES MDT discussion: YES
Ward:
Type of tracheostomy tube and is it cuffed? Percutaneous or surgically performed
Type:_________ Size:______
cuffed: Yes No Date:_______
Percutaneous o surgical o Is the patient confused?
Yes
No Yes o No o
Any neurological problems, head & neck surgery, Wet/weak voice or drooling?
Yes
No
**If yes then likely to aspirate ** - Refer to SALT for neurological swallowing assessment
Does the patient have any respiratory secretions? What colour and how much?
Yes
No
Secretions thick o looseo Colour………… min / mod / large
Does the patient have pain on dry swallow
Yes
No
**If yes then likely to aspirate **
Does the patient have an ineffective cough?
Yes
No
IF YES TO ANY OF THE ABOVE THEN NEEDS FULL MDT AGREEMENT TO PROCEED NB: Do not assess swallow if patient on ventilator or CPAP with cuff deflated without full MDT agreement. Cuff Inflated - Using water coloured with blue food dye please follow steps 1- 5 over page and record outcome below.FordeflatedcuffpleasefollowSwanseascreenguidelinesandrecordoutcomebelow
Is patient obviously aspirating? Yes No coughing o choking o stridor o hoarseness o wet/gurgly voice o
Evidence of aspiration on suction Yes No Large amt o Mod o Min o
PLEASE RECORD OUTCOME OF SWALLOW ASSESSMENT HERE CUFF INFLATED CUFF DEFLATED
PASS FAIL PASS FAIL • Trial of blue water for 24 hrs • Stop if blue dye on suction. • Record suction on tracking sheet
• Evidence of aspiration • KEEP PATIENT
NIL BY MOUTH • MDT Discussion
• Trial with blue
water for 24 hrs • Stop trial if blue dye
on suction • Record suction on
tracking sheet
• Evidence of aspiration • KEEP PATIENT NIL BY
MOUTH • MDT Discussion
Adapted by Asha Metharam-Jones, Band 7 Respiratory Physiotherapy Clinical Specialist, from the swallowing screening form developed by the Speech and Language Therapy Department from an original idea by Sister Carol Shamas RGN, Ysbyty Gwynedd, Bangor. Combined with The Swansea Tracking Sheet. Version 5.1 - 07/05/15
ASSESSMENT FOR DYSPHAGIA WITH
TRACHEOSTOMY TUBE.
Do not attempt the assessment if the patient is drowsy, semi-conscious or does not open eyes to speech.
Remember to fill in ALL SECTIONS.
Post 24 Hrs Monitoring with trial blue water PASS FAIL
Post 24 Hrs Monitoring with trial blue water PASS FAIL

24
COMMENTSANDADVICE
Signature:
Advice on Conducting Swallow Assessments with Cuff Inflated
1. Obtain medical consent for swallow assessment. 2. Ensure the patient is in an upright position as possible 3. Give the patient 3 teaspoonful of blue water 4. Ensure the patient swallows each mouthful several times before taking the next mouthful. 5. If evidence of aspiration is not immediate wait 5 minutes before suctioning as sometimes
secretions pool at back of throat and it takes a few minutes for aspirant to become evident.
6. If no evidence of aspiration then allow small sips of blue water via cup not straw and
monitor closely for 24 hours 7. Record the monitoring on the Swansea tracking sheet. Stop oral fluids if evidence of blue
dye on suction and refer back to MDT. 8. If they have a speaking tube in situ have the suction tube in place for the initial
assessment so you can suction. If they pass then monitor swallow with speaking valve in situ.
9. Advise the patient not to try to talk while eating and drinking Adapted by Asha Metharam-Jones, Band 7 Respiratory Physiotherapy Clinical Specialist, from the swallowing screening form developed by the Speech and Language Therapy Department from an original idea by Sister Carol Shamas RGN, Ysbyty Gwynedd, Bangor. Combined with The Swansea Tracking Sheet. Version 5.1 - 07/05/15

25
Appendix 3b. Swansea NHS trust. Swallow Screen for Patients with Tracheostomy
(Uncuffed tube or Deflated cuff) (Prior to the commencement of oral feeding)
To be performed by nurses who have attended a dysphagia training session.
1. YES NO 2. Does the patient have any of the following?
YES NO 3. Ensure patient is sitting upright and as straight as possible
4. Deflate the cuff and suction via Tracheostomy tube
YES NO 5. YES
NO
6. If patient is using a fenestrated inner cannula and a speaking valve, put fenestrated tube and valve in place and go to Step 7.
NB – ensure cuff is deflated
Istheremedicalconsentforfullcuffdeflation?
ProceedDeferswallowscreenuntilmedicalconsentobtained
• Headandnecksurgery• Neurologicalsymptoms• Weak/absentcough• Drooling
• Beawarethesepatientsareathighriskofaspirating.Proceedwithcaution
• IfnecessaryrefertoSALT
GotoStep3IsPatient:
Desaturating?Coughing?WetVoice?Distressed?
• Ceasetest• Reinflatecuff.Check
pressureusingpressuregauge
• Resumepreviousrespiratorysupport
• Re-testin24hoursorwhenrequired
Gotostep5CanPatientswallowtheirsaliva?
GotoStep6Proceedwithcaution–thismayindicateaswallowingproblem

26
7.Oral Trial
Give patient 1 teaspoon of sterile H₂0 coloured with blue food colouring
Observe for ϴ indicators:-
YES
NO
8.Give patient a further 3 teaspoons of H₂0 coloured blue and observe the above
YES
NO
9.Give patient small sips of H₂0 coloured blue from a cup (no straws or spouted beakers).
YES
NO
10. Trial with teaspoons of yoghurt consistency, dyed blue.
YES
NO
ϴIndicators
• Immediateordelayedcoughing
• Desaturation• H₂0lostfromorheldinthe
mouth• Bluedyefromstomasiteor
suctioning–immediateordelayed(usetrackingsheettoobservecolourofsecretions)
• Ceasetestandinformmedicalteam
• Repeatin24hours• ConsiderSALTreferral
GotoStep8Areϴindicatorspresent?(Seestep7)
CeasetestasStep7GotoStep9Aresecretionsclear(notblue)over24hoursofsuctioningusingtrackingsheet?
GotoStep10ConsiderreferraltoSALTAresecretionsclear(notblue)over24hoursofsuctioningusingtrackingsheet?
• Consideroralintake• Cautiouslyincreasing
quantityandobservingforϴindicatorsasinStep7
• Refertodietitian
• ConsiderreferraltoSALT• ContinuewithH₂0trials

27
Appendix 3c. Swansea NHS Trust
Blue Dye Tracking Sheet
A speech and language therapist or a nurse who has attended a dysphagia training session should perform the Modified Evans Blue Dye Test.
Name:
Hospital Number:
Ward:
Date of Test:
Trialled with:
Consistency:
Amount:
SUCTION
Blue Dye Presence at Suction
Date Time None Minimal Intermittent trace
Moderate Consistently tinged blue
Significant Consistently concentrated
Signature
28