training report
TRANSCRIPT

A
PROJECT REPORT
ON
“GENE IDENTIFICATION AND TARGET VALIDATION OF GENE(BRCA1) WITH THE COMPARATIVE STUDY THROUGH GENOMIC AND PORTEOMIC ANALYSIS USING BIOINFORMATICS TECHNIQUES.”
SUBMITTED BY:
PRIYA YADAV
B.Sc. (H) Biotech
Session-2012-15
JNU, JAIPUR

DECLARATION
I Priya Yadav, Enrollment no:- jnujaipur/2012/01591 hereby declare that the dissertation entitled submitted to the Director, School Of Life Science, Jaipur National University, Jaipur, in the partial fulfilment for the degree of Bachelor Of Science in Biotechnology and the dissertation represents independent and original work.
Place……….
Date………..
Signature of student

CERTIFICATE: 1
This is to certify that Priya Yadav has successfully completed her summer training at Rapture Biotech. , Noida on the topic “GENE IDENTIFICATION AND TARGET VALIDATION OF GENE (BRCA1) WITH THE COMPARATIVE STUDY THROUGH GENOMIC AND PORTEOMIC ANALYSIS USING BIOINFORMATICS TECHNIQUES.”
Her training report is satisfactory for the submission in the partial fulfillment of the required B.Sc. (Hons.) Biotechnology of JAIPUR NATIONAL UNIVERSITY.
Date:
Supervisor:
Mr. Vaibhav Kumar Sharma

CERTIFICATE: 2
This is to certify that the one month project training report entitled “GENE IDENTIFICATION AND TARGET VALIDATION OF GENE (BRCA1) WITH THE COMPARATIVE STUDY THROUGH GENOMIC AND PORTEOMIC ANALYSIS USING BIOINFORMATICS TECHNIQUES”submitted by Priya Yadav to JAIPUR NATIONAL UNIVERSITY, JAIPUR in partial fulfillment of requirements of the degree of B.Sc. (Hons.) Biotechnology has been approved by the committee after an oral examination of the same in the collaboration with an External Examiner.
Mr. Vaibhav Kumar Sharma External Examiner
Supervisor.
Prof. D.S. Bhatia
Director, SIILAS

ACKNOWLEDGMENT
The success and the final outcome of this project required a lot of guidance and assistance from countless persons. I am extremely fortunate to have so many people to guide me all along the completion of this project work. Whatever I have been able to do is only due to such guidance and assistance and I would never forget to thank them.
I deeply respect and thank my mentor, teacher Mr. Vaibhav Kumar Sharma, Assistant Professor, School Of Life Science, SIILAS Campus, Jaipur National University, Jaipur for encouraging me and putting emphasis on this opportunity to do a project work and getting exposure to various research tools and techniques. I am thankful to him which made me complete the project work on time. I am greatly indebted to him for providing such a nice support and guidance though he had busy schedule managing the academic affairs.
I owe my profound gratitude to my project guide Er Mayank Bahrdwaj, who took interest on my project work entitled “Gene Identification and Target Validation of the Gene (BRCA1) with the comparative study through Genomic and Proteomic Analysis Using Bioinformatics Techniques” and guided me all along, till the completion of my project work by providing all the necessary information required for a good scholarly output.
I would not forget to remember whole team of RAPTURE BIOTECH for their unlisted encouragement and more over for their timely support and guidance till the completion of my project work. I heartily wish to thank my internal projectguide Mr. Mayank Raj Bhardawaj, Dean, RAPTURE BIOTECH, for his guidance and suggestions during this project work.
I am appreciative to and fortunate enough to get constant encouragement, support and guidance from all the teaching staff of RAPTURE BIOTECH and Jaipur National University, Jaipur. I would also like to thank my project partner Nitesh Tripura of NIMS University, Jaipur. Also, I would like to extend my sincere regards to all the non-teaching staff of the RAPTURE BIOTECH for their timely support. In the last, I would like to thank my family members and friends who assisted me with this project.
30.06.2014 PRIYA YADAV

CONTENTS
- ABSTRACT- OBJECTIVES OF THE STUDY- INTRODUCTION TO CANCER- REVIEW OF THE LITREATURE- AVAILABLE TREATMENTS AND DIAGNOSTIC METHODS FOR
CANCER AND THEIR SIDE EFFECTS- AVAILABLE DRUGS USED FOR CANCER TREATMENT- INTRODUCTION TO BREAST CANCER- SIGNS AND SYMPTOMS OF BREAST CANCER- AVAILABLE DRUGS FOR BREAST CANCER - ALTERED GENES THAT GENERALLY RESULT IN BREAST
CANCER- TYPES OF GENES INNOVLVED IN BREAST CANCER- INTRODUCTION TO THE BRCA1 GENE- INTRODUCTION TO BIOINFORMATICS- BRIEF INTRODUCTION OF THE USED BIOINFORMATICS
TOOLS AND TECHNIQUES- METHODOLOGY- RESULTS AND DISCUSSION- CONCLUSION- REFERENCE

ABSTRACT
Cancer medically known as a Malignant Neoplasm, is defined as a group of more than 100 disease which are characterized by the uncontrolled proliferation of the cells. A number of mutations to the DNA base composition sequence of the concerned genes are responsible for the diseased condition. This project is focused majorly on the studies about BRCA1 (tumor suppressor gene) mutations and its role in the breast cancer through various bioinformaticstechniques by performing comparative genomic and proteomic analysis and the phylogenetic analysis. The project work also includes the mechanism behind breast cancer, available treatments, diagnosis and the available drugs for the treatment.
Objectives of the Study:
1) Comparative Analysis of the genetic information of the gene BRCA1 using Bioinformatics tools and software.
2) Study of the application of bioinformatics tools in order to determine whether the DNA contain mutations or not responsible for the breast cancer.
3) To navigate NCBI in order to align sequences using different tools and software and finally to validate the model.
4) To analyze the reference sequence, known to be free of cancer causing mutations are used to determine whether the DNA or peotein sequence carry mutations or not.
(1) Introduction to Cancer-1.1 Definition:
Any of a group of more than 100 distinct diseases that are characterized by the uncontrolled multiplication of abnormal cells. Cancerous cells and tissues have abnormal growth rates, shapes, size and functioning. Cancer may progress the stages from a localized tumor (confined to the site of origin) to direct the extension (spread into nearby tissues or lymph nodes) and metastasis (spread to more distant sites via the blood or lymphatic nodes). This malignant growth pattern distinguishes cancerous tumors from benign ones. Cancer is also classified by the grade, the extent to which cell characteristics remain specific to their tissue of origin. Both stage and grade affect the chances of survival. Genetic factors and immune status affect the susceptibility. Triggers include hormones, viruses, smoking, diet, and radiation. Cancer can initiate in almost any of the tissue as well as in the blood and the lymph. When it metastasizes, it remains a cancer of tissue of origin. Early diagnosis and

treatment increases the chance of cure. Treatments may include chemotherapy, Surgery, Radiation therapy.
Fig;1- Different levels of mutations are required to turn out a normal cell into cancerous cell.
Review of Literature:-
1) J. Mandelblatt (2007) Descriptive Review Of The Literature on Breast Cancer Outcomes. There is increasing interest in the incorporation of non- biomedical outcomes in cancer research. The goal was to review the use of non biomedical outcomes in research on breast cancer care. Conducted a MEDLINE search of all studies on breast cancer care, quality of life, preferences, satisfaction and economics that were published during the period from January 1, 1990 to December 31,2000. Also searched for bibliographies of the published articles. Included original primary research and excluded reviews, methods, papers, studies conducted outside the US and Western Europe, or the studies with fewer than 100 subjects. Data were abstracted by using a structured tool. There were 1089 articles identified; out of which 230 were included. The greatest proportion of research focused on survivorship followed by the screening. The most frequently reported outcomes were health-related quality of life (54%) followed by the economic analysis (38%) and patient satisfaction (14%); only 9% measured patient preferences. Few studies included more than 10% of the studies, and many authors developed de novo tools for use in their studies. The most general health outcome measure is the survival. For breast and other cancers, 5- year survival or the interval of disease-free survival has customarily been used to evaluate the success of the treatment. Clinical events, such as severity of the illness, tumor response, or stage shifts have served as intermediate measures of
outcome, principally, because they are believed to be associated with the differences in survival. For instance, therapeutic strategies may be associated with similar survival but varied toxic effects. Alternatively, one therapy may yield better survival but more severe side effects, while another may offer poorer survival but better quality of life during the patients remaining months or years. Even when the cures are possible, the costs of treatment may exceed an individual’s or society’s willingness to pray.
2) New Zealand Health Technology Assessment (NZHTA). Department of Public health and general practice.The following conclusions are based on the current evidence available from this report’s critical appraisal of literature published on the risk factors for breast cancer in women. Factors with a higher level of risk (RR.2.0) included: past history of breast cancer, selected precursor lesions of breast cancer, including a typical ductal carcinoma, lobular carcinoma and ductal carcinoma in situ increased the breast cancer density. Other factors appeared to have a moderate level of increased risk (RR 1.5-2.0): include alcohol intake. Some risk factors appeared to have modest level of increased risk of breast cancer (RR 1.0-1.5): nulliparity post menopausal obesity hormone replacement therapy, current use of oral contraceptives or recent use of oral contraceptves high total energy intake. Finally, for some risk factors the level of increased risk factors, the level of increased risk was difficult to determine.
3) Bettencourt BA. Department of Physiological Sciences. University of Mssouri, Columbia, USA.This report is a review of the studies that focus on rural breast cancer survivorship. It includes a total of 14 studies using large databases and 27 other studies using quantitative and qualitative methods. In this review, four broad themes were identified, including the access to treatment and treatment type, medical providers and health information, psychosocial adjustments and the social support services. The findings of the rural breast cancer survivorship studies within each of these broad themes. A few of the findings of the review include that rural and urban women receive different primary treatments for breast cancer.
4) Hereditary breast and ovarian cancer syndrome (HBOC), caused by a germline mutation in BRCA1 or BRCA2, is characterized by an increased risk for breast cancer, ovarian cancer, prostate cancer, and pancreatic cancer. The lifetime risk for these cancers in individuals with a mutation in BRCA1 or BRCA2:
40%-80% for breast cancer 11%-40% for ovarian cancer 1%-10% for male breast cancer Up to 39% for prostate cancer 1%-7% for pancreatic cancer
Individuals with BRCA2 mutations may also be at an increased risk for melanoma. Prognosis for BRCA1/2-related cancer depends on the stage at which the cancer is diagnosed; however, studies

on survival have revealed conflicting results for individuals with germline BRCA1 or BRCA2mutations when compared to controls. An increased likelihood of a BRCA1 or BRCA2 mutationis suspected on the basis of certain personal and family history characteristics and various clinical criteria. A diagnosis of HBOC is made following molecular genetic testing in an individual or family with a germline BRCA1 or BRCA2 mutation. No currently available technique can guarantee the identification of all cancer-predisposing mutations in BRCA1 or BRCA2. Furthermore, mutations of uncertain clinical significance may be identified.
Treatment of manifestations: Treatment of breast and ovarian cancer in individuals with BRCA1-or BRCA2-related tumors is similar to that for sporadic forms of these cancers; however, new classes of drugs that specifically target the BRCA1/2 signaling pathways are being studied.
1.2 Signs and Symptoms:
A cancer may cause symptoms like fever, extreme tiredness (fatigue) or weight loss. This may be because cancer cells use up much of the body’s energy supply, or they may release substances that change the way that body derives the energy from the food. Cancer may also cause the immune system to react in ways that produce these signs and symptoms. Sometimes, cancer cells release substances into the bloodstream that cause symptoms which are not usually linked to cancer. For example, some cancers of the pancreas can release substances that cause blood clots in veins of the legs. Some lung cancers make hormone- like substances that raise the blood calcium levels, affecting nerves and muscles, making the person fell weak and dizzy.

Fig;2- Immunity and the Abnormal Cancerous Cells.
1.3 Causes of Cancer- Smoking- Bad eating habits- Viruses- Radiations- Alcohols and several other Carcinogenic agents
Fig; 3- Contributing factors of Cancer.
1.4 Types Of Cancer:
Mainly there are two types of cancer on the basis of their behavior with the neighboring cells as written below:
A Benign tumor: A benign tumor is basically defined as a type of tumor that doesn’t come back and doesn’t spread to other parts of the body. A tumor is a mass of tissue that serves no useful purpose and generally exists at the expense of the healthy tissues.
B Malignant Tumor: A malignant tumor most commonly refers to any growth or the tumor which is cancerous. Malignant growths have the ability to spread to other areas of the body. By definition, any cancer is considered as malignant.
1.5 Classification on the basis of cell:

a) Carcinoma cancer: Any of the various cancerous tumors that are derived from the epithelial tissue of the skin, blood vessels, or other organs and that tend to metastasize to other parts of the body; like Lung Cancer, Kidney Cancer, Brain Cancer, Skin Cancer etc.
b) Sarcoma cancer: A tumor, often highly malignant, composed of the cells derived from the connective tissue such as bone, cartilage, muscle, blood vessel, or lymphoid tissue; sarcomas usually develop rapidly and metastasize through the lymph channels. Different types are named for the specific tissue they affect: Fibrosarcoma in fibrous connective tissue, Lymphosarcoma in lymphoid tissue, Osteosracoma in bone, Chondrosarcoma in cartilage, Rhabdosarcoma in muscle and Liposarcoma in fat cells.
c) Myeloma (Leukemia) Cancer: A tumor of the bone marrow( usually) malignant, composed of the cells normally found in the bone marrow. Like;
-Acute Lymphoblastic Leukemia-Acute Myeloid Leukemia (Acute Myelogenous Leukemia)-Chronic Lymphoid Leukemia (Chronic Lymphocytic Leukemia)-Chronic Myeloid Leukemia (Chronic Myelogenous Leukemia)
d) Lymphoma Cancer: Any of various usually malignant tumors that arise in the lymph nodes or in other lymphoid tissue, like;
- Hodgkin Lymphoma
- Non- Hodgkin Lymphoma
- Burkett’s Lymphoma
1.6 Diagnosis of Cancer
The most common diagnostic methods include:
a) BIOPSY: This is a test where a small sample of tissue is taken from the suspected cancer with the help of a fine tipped needle (Fine Needle Aspiration- FNA), or with a thicker hollow needle (Core biopsy) or by surgical excision. The tissues are then examined under a microscope for the presence of cancer cells.
b) Sentinel Node Biopsy: This is a procedure where the closest and most important nodes near the cancer are surgically excised and examined. Since sentinel nodes are the first location that cancer is likely to spread, only these lymph nodes that likely contain cancer cells.
c) Endoscopy: In this imaging technique, a thin, flexible tube with a tiny camera on the end is inserted into the body cavities. This allows the doctors to view the suspicious area. There are many types of scopes, each designed to view particular areas of the body. For example; a colonoscope looks at the colon and large intestine and a laparoscope is used to look within the abdomen etc.

d) Blood Tests: Blood tests can be performed to detect the normal blood cells as well as for specific tumor markers. Some tumors release substances called tumor markers, which can be detected in the blood. A blood test for prostate cancer determines the amount of prostate specific antigen (PSA). Higher than the normal PSA levels can indicate cancer. Similarly, in ovarian cancer a tumor CA-125 is released.
e) Pap test: Pap test( Pap smear) is a routine test where a sample of cells from a women’s cervix is examined under the microscope. This helps to identify the changes in the cells that could indicate cervical cancer or other conditions.
f) Sputum analysis and bronchial washing analysis: The cells of the sputum and bronchial secretions are analyzed under the microscope for signs of lung and other respiratory cancers.
g) Imaging studies: There are several imaging techniques including X-rays, CT scans, MRI scans of various parts of the body. X-rays: are the most common imaging techniques and they may be made more
specific by using a Barious Enema. This is used for detection of stomach and small intestinal growths and cancers. Mammogram is an X-ray of the breasts used to screen for and/or detect breast lumps and growths.
A CAT scan uses radiographic beams to create detailed computerized pictures. It is more precise than a standard X-ray.
A Magnetic Resonance Imaging uses a powerful magnetic field to create detailed computer images of the body’s soft tissue, large blood vessels and major organs. Both CT scan and MRI scans can also be used with the contrast radio-labelled dyes to obtain a more clear and specific picture of the cancer.
An ultrasound uses high- frequency sound waves to determine if a suspicious lump is solid or liquid. These sound waves are transmitted into the body and converted into a computerized image.
Bone scan is usually used to identify and locate new areas of cancer spread to the bone. Normally a Positron Imaging Test (PET Tests) is used. A gallium scan is another nuclear medicine test in which a special camera takes a picture of the tissues of the body after a special radioactive tracer is injected into a vein. The cancerous areas light up under the scanner.
h) Genetic Analysis: Cytogenetic analysis involves analysis of blood or bone marrow cells for organizations of chromosomes. This shows up any genetic mutations.
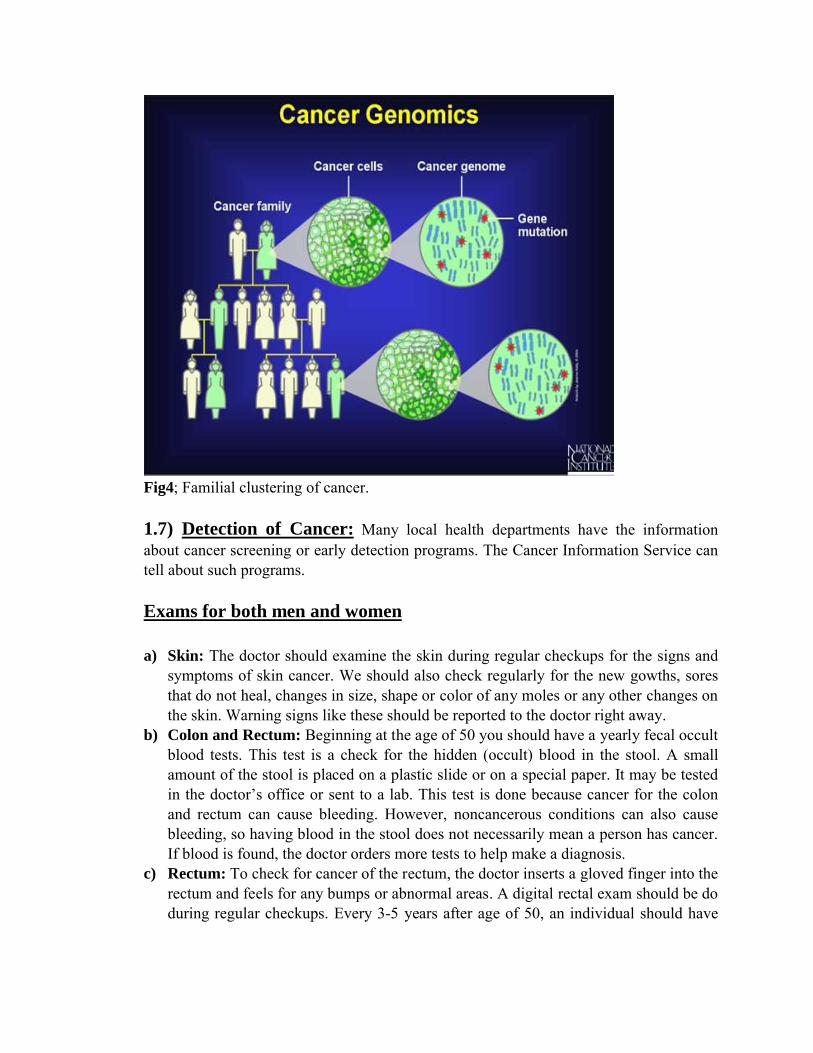
Fig4; Familial clustering of cancer.
1.7) Detection of Cancer: Many local health departments have the information about cancer screening or early detection programs. The Cancer Information Service can tell about such programs.
Exams for both men and women
a) Skin: The doctor should examine the skin during regular checkups for the signs and symptoms of skin cancer. We should also check regularly for the new gowths, sores that do not heal, changes in size, shape or color of any moles or any other changes on the skin. Warning signs like these should be reported to the doctor right away.
b) Colon and Rectum: Beginning at the age of 50 you should have a yearly fecal occult blood tests. This test is a check for the hidden (occult) blood in the stool. A small amount of the stool is placed on a plastic slide or on a special paper. It may be tested in the doctor’s office or sent to a lab. This test is done because cancer for the colon and rectum can cause bleeding. However, noncancerous conditions can also cause bleeding, so having blood in the stool does not necessarily mean a person has cancer. If blood is found, the doctor orders more tests to help make a diagnosis.
c) Rectum: To check for cancer of the rectum, the doctor inserts a gloved finger into the rectum and feels for any bumps or abnormal areas. A digital rectal exam should be do during regular checkups. Every 3-5 years after age of 50, an individual should have

sigmoidoscopy in this exam; the doctor uses a thin, flexible tube with a light to look inside the rectum and colon for the abnormal areas.
d) Mouth: Your doctor and dentist should examine our mouth at a regular basis. Also, by looking in a mirror, you can check inside your mouth for the changes in the color of the lips, gums, tongue or inner cheeks and for scabs, cracks, sores, white patches, swelling or bleeding. It is often possible to see or feel changes in the mouth that might be cancer or a condition that might lead to cancer. Any symptoms in your mouth should be checked by a doctor or the dentist. Oral exams are especially important for the people who intake alcohol or tobacco products and for anyone over the age of 50.
(A)Exams for Men:
1) Prostate:- Men over age 40 should have a yearly digital rectal exam to check the prostate gland for hard or lumpy areas. The doctor feels the prostate through the wall of the rectum.
2) Testicles:- Testicular Cancer occurs mostly between the age of 15-34. Most of these cancers are found by men themselves, often by doing a testicular self-exam. If you find a lump or notice another change, such as heaviness, swelling, unusual tenderness, or pain, you should see your doctor. Also, the doctor should examine the testicles as part of regular medical checkups.
(B) Exams for Women:
1) Breast:- When breast cancer is found early, a woman has more treatment choices and good chances of a complete recovery. It is therefore, important that breast cancer be detected as early as possible. The National Cancer Institute encourages women to take an active part in early detection. They should talk to their doctor about this diseases, the symptoms to watch for, and an appropriate schedule of checkups. Women should ask their doctors about:
Mammograms (X-rays of the breast) Breast exams by a doctor or a nurse Breast self-examination
A mammogram can often show tumors or changes in the breast before they can be felt or cause symptoms. However, we know mammograms cannot find every abnormal area in the breast. This is especially true in the breasts of young women. Another important step in early detection is for women to have their breasts examined regularly by a doctor or a nurse. More breast lumps are not cancer, but can make a diagnosis.
2) Cervix:- For the Pap test, a sample of cells is collected from the early cervix cancer. In a pelvic exam, the doctor feels the uterus, vagina, ovaries, fallopian tubes, bladder and rectum for any change in shape or size, upper vagina and cervix with a small brush or a flat wooden stick. The sample is placed on a glass slide. Women should start having a Pap test every year after they turn 18

or become sexually active. If the results are normal for 3 or more years in a row, a woman may have this test less often, based on the doctor’s advice.
1.8) Treatment of Cancer: There are many types of treatment but specific are Chemotherapy, Radiotherapy, Target Therapy, Transplantation.
a) Chemotherapy:- is the use of chemicals to treat the disease more specifically, it usually refers to the destruction of cancer cells. However, chemotherapy may also include the use of antibiotics or other medications to treat any illness or infection.Chemotherapy drugs work in the following ways:
Impairing Mitosis- they are known as cytotoxic drugs. Stopping the growth of new blood vessels that supply a tumor. In a study, researchers
at the Johns Hopkins University, School of Medicine discovered how a whole class of commonly used chemotherapy drugs destroy cancer by blocking the blood vessel growth.
Triggering suicide of cancer cells.
b) Radiation Therapy:- uses high-energy radiations to shrink tumors and kill cancer cells. X-rays, Gamma-rays and charged particles are the types of radiation used for cancer treatment. The radiation may be delivered by a machine outside the body (external beam radiotherapy) or it may come from radioactive material placed in the body near cancer cells (internal radiation therapy).
Side – effects of radiotherapy:- There are actually two kinds of side-effects from radiotherapy—Early and Late.
Early side effects such as nausea or fatigue are usually temporary. They develop during or right after the treatment and last for several weeks after treatment ends, but then improve.
Late side effects, such as lung or heart problems, may take years to develop and are often permanent when they do.
c) Target Therapy:- Target therapy or Molecularly targeted therapy is a type of medication that blocks the growth of cancer cells by interfering with the specific targeted molecules needed for carcinogenesis and tumor growth, rather than by simply interfering with all rapidly dividing cells. Targeted cancer therapy is expected to be more effective than the current treatments and less harmful to the normal cells. There are targeted therapies for breast cancer, multiple myeloma, lymphoma, prostate cancer, melanoma and other cancers.
d) Drugs for Cancer:- There are some drugs which affect cancer directly or help to breakdown the cancer pain.
Abraxane for the treatment of non-small cell lung cancer

Abstral for the treatment of breakthrough cancer pain 1 opoid-tolerant patients. Actic treatment for cancer pain. Adcretris (brentuximab vedotin) for the treatment of Hodgkin Lymphoma ana
anaplastics large cell lymphoma. Afinitor (everolimus) for the treatment of hormone receptor- positive, HER2-
negative breast cancer. Alimta ( permetexed for injection) for the treatment of malignant pleural
mesothelioma.
1.9) Mechanism of Cancer:
1) Cells start to grow and multiply overtime, some more changes may also take place.
2) Eventually cell and its descendants become immortal, escape destruction by the body’s natural defences.
3) Then these abnormal cells secret some specific enzymes to break the lymph vessels. This way they enter the lymphatic system developing their own blood supply and invade rest of the body.
In cancer cells, the signals to grow are altered or the growth termination signals are missing. These abnormal cells have uncontrolled proliferation owing to change in the growth factors and their products, altered signaling pathways, particularly those controlling cell cycle and the apoptosis, telomerase expression and tumor related angiogenesis.
Fig5; Different stages of cancer and metastasis.
Types of Cancer:- Cancer is generally defined as a malignant neoplasm which comprises of about 100 different diseases. Some common types of cancers are listed under:
1) Bladder Cancer

2) Breast Cancer
3) Kidney Cancer
4) Lung Cancer
5) Colon and Rectal Cancer
6) Endometrial Cancer
7) Leukemia
8) Melanoma
9) Non- Hodgkin Lymphoma
10) Pancreatic Cancer
11) Prostate Cancer
12) Thyroid Cancer
13) Ovarian Cancer
14) Cervical Cancer
Introduction to Breast Cancer:-
Breast cancer is defined as malignant tumor that initiates into the breast cells. A malignant tumor is a group of cancer cells that can grow to invade the surrounding tissues or spread to the distant areas in body. The disease occurs almost entirely in females, but men can get it too. To understand breast cancer, it is important to understand the normal breast structure and functioning.
The Normal Breast:
The female breast is mostly made up of a collection of fat cells called adipose tissue. This tissue extends from the collarbone down to the underarm and across to the middle of the ribcage. A healthy female breast is made up of 12–20 sections called lobes. Each of these lobes is made up of many smaller lobules, the gland that produces milk in nursing women. Both the lobes and lobules are connected by milk ducts, which act as stems or tubes to carry the milk to the nipple. These breast structures are generally where the cancer begins to form.
Within the adipose tissue is a network of ligaments, fibrous connective tissue, nerves, lymph vessels, lymph nodes, and blood vessels. The lymph system, which is part of the immune system, is a network of lymph vessels and lymph nodes running throughout the entire body. Similar to how the blood circulatory system distributes elements throughout the body, the lymph system transports disease-fighting cells and fluids. Clusters of bean-shaped lymph nodes are fixed in areas throughout the lymph system and act as filters by carrying abnormal cells away from healthy tissue. The type of breast cancer is generally determined by the origin of the growth of cancer cells, which is almost always in the lobes, lobules, or ducts. When cancer is found in the nearby lymph nodes, it helps doctors identify just how far the cancer has spread. If the nearest

nodes contain cancer, additional nodes are usually examined for the presence or absence of cancer cells to understand how far the disease has progressed.
Fig6;- Normal breast anatomy and anatomical location of common breast lesions.
Signs and Symptoms of the Breast Cancer:-
1) A lump in the breast2) Any pain in the armpits or breast that does not seem to be related to the women’s
menstrual periods.3) Pitting or redness of the skin of the breast4) A rash around or one of the nipples5) A swelling in one of the or both the armpits6) An area of the thickened tissue in a breast7) One of the nipples has a discharge, sometimes it may also contain blood.8) Nipple changes in the appearance, it may become sunken or inverted9) Size or shape of the breast changes10) Nipple skin or breast skin may start to peel, scale or flake.
Some major drugs approved by FDA for breast cancer:
1) Abitrexate (Methotrexate)2) Abraxane (Pactitaxel Albumin- stabilized nanoparticles formulation)3) Ado- trastuzumab tntansine

4) Adriamycin PFS (Doxorubicin Hydrochloride)5) Adriamycin RDF (Doxorubicin Hydrochloride)6) Adrucil (Fluorouracil)7) Afinitor (Everolimus)8) Anastrogol9) Aredio (Pamidromate Disodium)10) Arimidex (anastrozole)
Some combinatorial drugs used for the treatment of breast cancer:
1) Doxorubicin Hydrochloride Cyclophosphamide2) Doxorubicin Hydrochloride Cyclophosphamide Paclitaxel3) Cyclophosphamide Doxorubicin Hydrochloride Fluorouracil4) Cyclophosphamide Methotexate Fluorouracil5) Fluorouracil Epirubicin Hydrochloride Cyclophosphamide6) Docetaxel Doxorubicin Hydrochloride Cyclophosphamide
Epidemiology of the Breast Cancer:
Worldwide breast cancer is the most common invasive cancer in women. Breast cancer comprises 22.9% of invasive cancer in female in female and 16% of all familial cancer. In 2010, breast cancer caused 458-503 deaths worldwide (13.7% of cancer deaths in women and 6% of all cancer deaths for all men and women together). The number of cases worldwide has significantly since 1970. Breast cancer is strong related to age, with only % of all breast cancer occurring in women under years old. The incidence of breast cancer varies greatly around the world. It is lowest in less- developed countries and greatest in the more developed countries. Breast cancer in less developed countries such as those of South America is a major public health issue. It is a leading cause of cancer related deaths among the women in countries like Argentina, Uruguay and Brazil.
Types of the faulty genes causing cancer:- Variations of the following genes increases the risk of developing breast cancer:
BRCA1 BRCA2 CHD1 SET11 TP53
Genes listed below are associated with breast cancer:-
AR ATM

BARD1 BRIP1 CHEK2 DIRAS3 ERBB2 NBN PALB2 RAD50 RAD51
Introduction to BRCA1 Gene:
Fig;7- Cytogenetic location of the BRCA1 gene.
The BRCA1 gene belong to a class of the genes known to have tumor suppressor function and is hence called as the tumor suppressor gene. The protein pBRCA1 in normal conditions help prevent cells from growing and dividing rapidly and uncontrollably.
The BRCA1 gene provides instructions for making protein that is directly involved in the repairing DNA damage.interacts with several other proteins including the proteins produced from the RAD5 and BRAD1 genes. Some midor other environmental factors and also may occur whenevthe genetic materials in the preparation for cell division. By helping repairmnet of DNA, BRCA1 plays a role in maintaining stability of the genetic information. Researches suggests that BRCA1 protein also regulates the activitycritical role in the embryonic development.
Introduction to BRCA1 Gene:
Cytogenetic location of the BRCA1 gene.
The BRCA1 gene belong to a class of the genes known to have tumor suppressor function and is hence called as the tumor suppressor gene. The protein pBRCA1 in normal conditions help prevent cells from growing and dividing rapidly and
The BRCA1 gene provides instructions for making protein that is directly involved in the In the nucleus of many types of normal cells, BRCA1 protein
interacts with several other proteins including the proteins produced from the RAD5 and BRAD1 genes. Some mid- breaks in the DNA can be caused by any natural and chemical or other environmental factors and also may occur whenever the chromosomes exchange the genetic materials in the preparation for cell division. By helping repairmnet of DNA, BRCA1 plays a role in maintaining stability of the genetic information. Researches suggests that BRCA1 protein also regulates the activity of some other genes and plays a critical role in the embryonic development.
The BRCA1 gene belong to a class of the genes known to have tumor suppressor function and is hence called as the tumor suppressor gene. The protein production of BRCA1 in normal conditions help prevent cells from growing and dividing rapidly and
The BRCA1 gene provides instructions for making protein that is directly involved in the normal cells, BRCA1 protein
interacts with several other proteins including the proteins produced from the RAD5 and breaks in the DNA can be caused by any natural and chemical
er the chromosomes exchange the genetic materials in the preparation for cell division. By helping repairmnet of DNA, BRCA1 plays a role in maintaining stability of the genetic information. Researches
of some other genes and plays a

Fig;8- Mutations in the BRCA1 gene.
The BRCA1 gene belong to a family of genes called RNF (Ring-Type Zinc finger Protein). It is located on the long (q) arm of the chromosome no 17 at position 21. More precisely, BRCA1 gene is located from base pair 43,044,294 to the base pairs 43,125,482 on the chromosome no 17.
Researchers have identified that more than 1000 mutations in the BRCA1 gene may be associated with an increased risk of cancer. Most of the mutations lead to the production of an abnormal short version of BRCA1 protein from being made up of from one copy of the gene. Other BRCA1 mutations change single amino acid in the protein or delete large segment of the DNA from the BRCA1 gene.
Fig;9- Increased Risk of Cancer because of BRCA Mutations.

A defective or missing BRCA1 protein is unable to help repair the damaged DNA or fix the mutations that occur in other genes. As these defects accumulate, they can allow the cell to grow and divide uncontrollably and form a tumor. In addition to female breast cancer, mutations in the BRCA1 gene also increases the risk of several other cancers like Ovarian Cancer, Fallopian Tube Cancer, Male breast cancer, Pancreatic cancer. Many of these mutations change one amino acid used to make BRCA1 protein which results in a protein that cannot perform its normal functions of DNA repair.
Fig;10- Increased risk of developing breast cancer due to BRCA1 mutations.
Introduction to Bioinformatics:-
Bioinformatics has become an important part of many areas of biology. In experimental molecular biology, bioinformatics techniques such as image and signal processing allow extraction of useful results from large amounts of raw data. In the field of genetics and genomics, it aids in sequencing and annotating genomes and their observed mutations. It plays a role in the text mining of biological literature and the development of biological and gene ontologies to organize and query biological data. It also plays a role in the analysis of gene and protein expression and regulation. Bioinformatics tools aid in the comparison of genetic and genomic data and more generally in the understanding of evolutionary aspects of molecular biology. At a more integrative level, it helps analyze and catalogue the biological pathways and networks that are an important part of systems biology. In structural biology, it aids in the simulation and modeling of DNA, RNA, and protein structures as well as molecular interactions.
Paulien Hogeweg and Ben Hesper coined the term bioinformatics in 1970 to refer to the study of information processes in biotic systems. This definition placed bioinformatics as a field parallel

to biophysics (the study of physical processes in biological systems) or biochemistry (the study of chemical processes in biological systems). Computers became essential in molecular biology when protein sequences became available after Frederick Sanger determined the sequence of insulin in the early 1950s. Comparing multiple sequences manually turned out to be impractical. A pioneer in the field was Margaret Oakley Dayhoff, who has been hailed by David Lipman, director of the National Center for Biotechnology Information, as the "mother and father of bioinformatics. Dayhoff compiled one of the first protein sequence databases, initially published as books and pioneered methods of sequence alignment and molecular evolution. Another early contributor to bioinformatics was Elvin A. Kabat, who pioneered biological sequence analysis in 1970 with his comprehensive volumes of antibody sequences released with Tai Te Wu between 1980 and 1991.
BRIEF INTRODUCTION OF THE USED BIOINFORMATICS TOOLS AND TECHNIQUES:-
S.No. Tool/ Software URL Significance1 pBLAST http://blast.ncbi.nlm.nih.gov/Blast.cgi This program, given
a protein query, returns the most similar protein sequences from the protein database that the user specifies.
2 nBLAST http://blast.ncbi.nlm.nih.gov/Blast.cgi This program, given a DNA query, returns the most similar DNA sequences from the DNA database that the user specifies.
3 Protpram http://www.expasy.org/tools/protparam.html It is used for calculating various physiochemical parameters of a provided protein. The protein sequence is the only input provided to calculate such parameters.
4 GOR http://abs.cit.nih.gov/gor/ (Garnier-

Osguthorpe-Robson) is an information theory-based method for the prediction of secondary structures in proteins. GOR method takes into account not only the propensities of individual amino acids to form particular secondary structures, but also the conditional probability of the amino acid to form a secondary structure given that its immediate neighbors have already formed that structure.
5 GENO 3D http://geno3d-pbil.ibcp.fr Automatic web server for protein molecular modelling. Starting with a query protein sequence, the server performs the homology modelling in six successive steps.
6 SPDBV spdbv.vital-it.ch/ Used to generate Ramachandran Plot.
7 UCLA Server(ERRAT, Verify 3D)
nihserver.mbi.ucla.edu/SAVES Determines the compatibility of an atomic model (3D) with its own amino acid sequence (1D) by assigning a structural class based on its location and environment (alpha, beta, loop, polar, nonpolar etc) and comparing the results to good structures.

Methodolgy:
Navigation to the NCBI website → Retrieval of FASTA seq. of BRCA1 gene → nBLAST → Retrieval of FASTA seq. of BRCA1 protein → pBLAST → Protein Primary Structure Analysis using Protpram → Secondary structure Prediction using GOR → Protein Model Building with the help of Swissmodel → Generation of Ramachandran Plot using SPDBV → Model Validation sing UCLA server.
Results:
The normal and the mutant protein, their amino acid composition, nucleotide composition, base pair repeats was identified and studied. The protein’s ligand binding sites, 3D structure and also the phylogenetic relationships with various families with the help of Genomic and Proteomic studies were also studied. With the help of comparative proteomics, the normal and abnormal protein and that with the help of comparative genomics, the signaling sites in the disease, were identified and studied easily.
1) Nucleotide BLAST of the gene BRCA1:


2) Protein BLAST of BRCA1 :

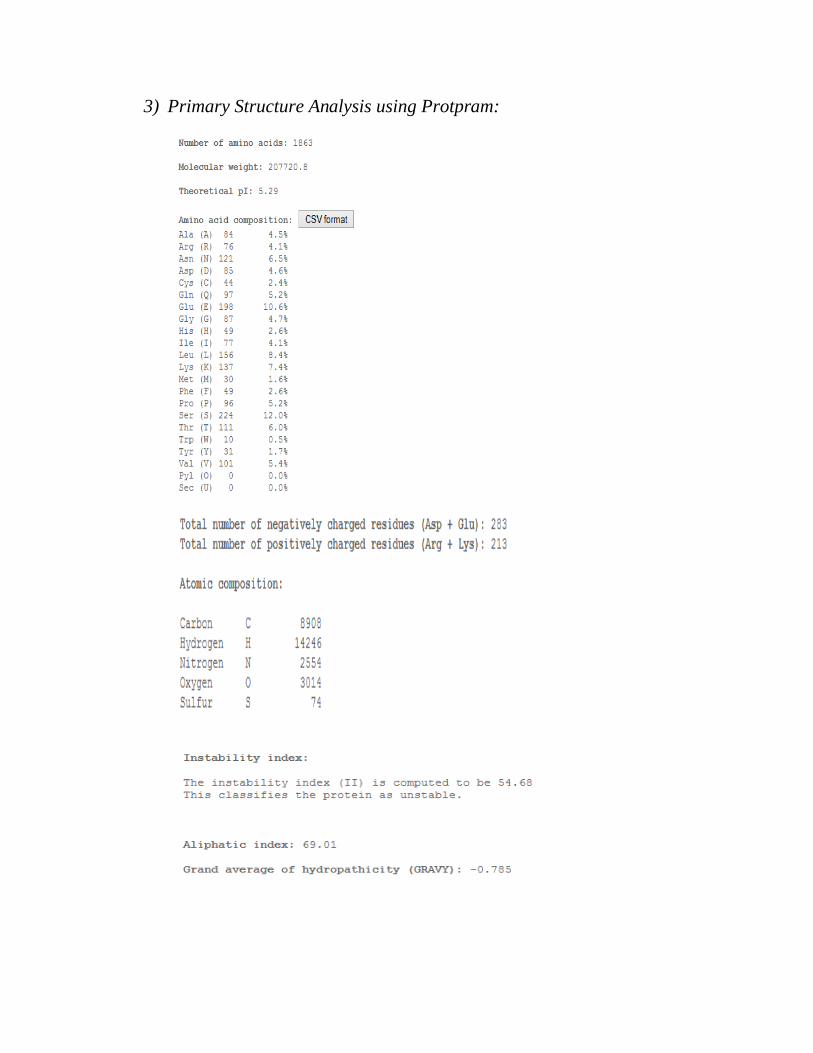
3) Primary Structure Analysis using Protpram:

4) Secondary Structure Analysis using GOR:

5) Protein Model Building Using Swissmodel

6) Ramachandran Plot of Normal BRCA1 protein using SPDBV software:

7) -Model Verification using Verify 3D:
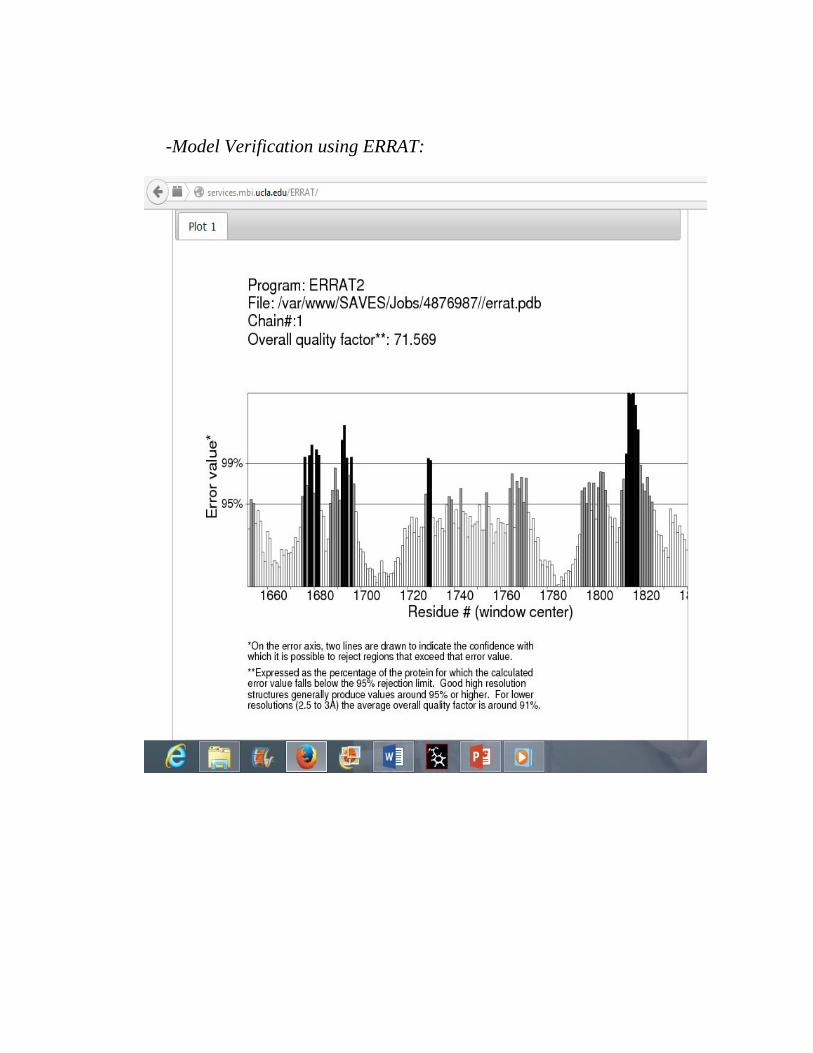
-Model Verification using ERRAT:

8) Phylogenetic Analysis using ClustalW alignmet, TPhylogeny.fr phylogenetic tree:
Phylogenetic tree using ClustalW alignment
Phylogenetic tree using T
Phylogenetic Analysis using ClustalW alignmet, T-Coffee Alignment and phylogenetic tree:
hylogenetic tree using ClustalW alignment
hylogenetic tree using T-COFFEE alignment
Coffee Alignment and

Phylogeny.fr phylogenetic tree
Phylogenetic Analysis
To get a broader understanding of the evolutionary trajectory path of the complete BRCA1 gene sequences from the 7 primate species was analyzed. It showed that the specific amino acid sites have been experiencing a repeated selection for the amino acid replacement over the primate evolution. This selection has been focused specifically on Homo sapiens and the closest living relatives, i.e; Chimpanzees (Bonobos (Pan paniscus).
After analyzing BRCA1(Macaca mulatta) individuals, considerable variation within each of these species and evidence for recent selection in
Phylogeny.fr phylogenetic tree
Phylogenetic Analysis-
To get a broader understanding of the evolutionary trajectory path of the gene sequences from the 7 primate species was analyzed. It showed that
the specific amino acid sites have been experiencing a repeated selection for the amino cid replacement over the primate evolution. This selection has been focused specifically
and the closest living relatives, i.e; Chimpanzees (Pan troglodytes).
polymorphisms in Bonobo, Chimpanzee and Rhesus macaque ) individuals, considerable variation within each of these species and
evidence for recent selection in Homo sapiens populations was studied.
To get a broader understanding of the evolutionary trajectory path of the BRCA1, gene sequences from the 7 primate species was analyzed. It showed that
the specific amino acid sites have been experiencing a repeated selection for the amino cid replacement over the primate evolution. This selection has been focused specifically
Pan troglodytes) and
nzee and Rhesus macaque ) individuals, considerable variation within each of these species and

Conclusion:
The mutant gene BRCA1 in breast cancer is responsible for the disease. The comparative study between normal and mutant gene using various types of tools, i.e; BLAST, Protpram, GOR, Swissmodel, Ramachandran Plot, Geno 3D and UCLA server, was analyzed. After using these software and tools it is predicted that there are various positions of the gene and also between normal and mutant gene which indicates of the project as a result the binding of available drug molecules in respect to cure the diseaseare studied, various signaling sites, and the feasibility of finding the new drug molecules for better treatment and cure can also be studied. The normal BRCA1 gene’s position is on the long (q) arm of the chromosome no. 17.
In normal conditions, the BRCA1 gene act as tumor suppressor, producing a protein that prevents cells from multiplying too quickly. When abnormalities in the protective BRCA1 gene are inherited or acquired, cells can grow and divide uncontrollably and tumors may form. BRCA1 and BRCA2 appear to share similarities: both abnormalities translate to a higher-than-average cancer risk and can be inherited by men or women from either parent. While much more research is needed to explore differences between the mutations, experts have already identified a few distinctions.
The maintenance of chromosomal integrity is an essential task of every living organism and cellular repair mechanisms exist to guard against insults to DNA. Given the importance of this process, it is expected that DNA repair proteins would be evolutionarily conserved, exhibiting very minimal sequence change over time. BRCA1; an essentially important gene involved in DNA repair, and is a tumor suppressor gene, is reported to be evolving rapidly despite of the fact that many protein-altering mutations within the mentioned gene convey a significantly elevated risk for breast and ovarian cancers.
Some more phylogenetic studies and the molecular characterization of the above mentioned gene- BRCA1, and another member of the family BRCA2; may prove helpful in the process for better drug development solutions for the cure of disease and a better understanding of the molecular mechanism and the altered cell signaling pathways leading to Cancer.

Discussion:
Almost all known and well studied cases of recurrent positive selection in the genomes involve the genes in any of three categories: (a) immunity (b) environmental perception (3) sexual selection and mate-choice. This is because of the reason that ever-changing external stimuli drive the selection of new allelic variants.
But this is quite unobvious to find that BRCA1 gene does not fit into any of the above 3 categories and are evolving in a similar manner to the highly adaptive immunity genes. Additional to the gene BRCA1, other DNA repair genes have also been shown to evolve under positive selection, but the driver behind this unusual finding remains to be identified.
The BRCA1 protein play key roles in the repairing of damage to chromosomal the DNA. The analysis of the evolution of the BRCA1 gene, shows that the mentioned gene has been a subject to recurrent positive selection during simian primate speciation. Although the forces driving the diversifying selection of the gene is still unknown, the result is that the sequence of this protein has been altered in humans and the closest living relatives.
It still remains to be analyzed that whether this is an instance of antagonistic pleiotropy; where positive selection driven by one force causes functional consequences in another context, potentially leading to the formation of cancers.
Refrences:
Antoniou A, Pharoah PD, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: A combined analysis of 22 studies. American Journal of Human Genetics 2003; 72(5):1117–1130.
Brose MS, Rebbeck TR, Calzone KA, et al. Cancer risk estimates for BRCA1 mutation carriers identified in a risk evaluation program. Journal of the National Cancer Institute2002; 94(18):1365–1372.
Burk-Herrick A, Scally M, Amrine-Madsen H, Stanhope MJ, Springer MS: Natural selection and mammalian BRCA1 sequences: elucidating functionally important sites relevant to breast cancer susceptibility in humans. Mamm Genome 2006, 17:257-270.
Campeau PM, Foulkes WD, Tischkowitz MD. Hereditary breast cancer: New genetic developments, new therapeutic avenues. Human Genetics 2008; 124(1):31–42.
Chen S, Parmigiani G. Meta-analysis of BRCA1 and BRCA2 penetrance. Journal of * Clinical Oncology 2007; 25(11):1329–1333.

Easton DF. How many more breast cancer predisposition genes are there? Breast Cancer Research 1999; 1(1):14–17.
Finch A, Beiner M, Lubinski J, et al. Salpingo-oophorectomy and the risk of ovarian, fallopian tube, and peritoneal cancers in women with a BRCA1 or BRCA2 mutation. JAMA2006; 296(2):185–192.
Fleming MA, Potter JD, Ramirez CJ, Ostrander GK, Ostrander EA: Understanding missense mutations in the BRCA1 gene: an evolutionary approach. Proc Natl Acad Sci U
S A 2003, 100:1151-1156. Hemel D, Domchek SM: Breast Cancer Predisposition Syndromes. Hematol Oncol Clin
North Am 2010, 24:799-814. Howlader N, Noone AM, Krapcho M, et al. (eds). SEER Cancer Statistics Review, 1975-
2011, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2011/ , based on November 2013 SEER data submission, posted to the SEER web site, April 2014.
Hurst LD, Pál C: Evidence for purifying selection acting on silent sites in BRCA1. Trends
Genet 2001, 17:62-65. Huttley GA, Easteal S, Southey MC, Tesoriero A, Giles GG, McCredie MR, Hopper JL,
Venter DJ: Adaptive evolution of the tumour suppressor BRCA1 in humans and
chimpanzees. Australian Breast Cancer Family Study. Nat Genet 2000, 25:410-413. Ludwig T, Chapman DL, Papaioannou VE, Efstratiadis A: Targeted mutations of breast
cancer susceptibility gene homologs in mice: lethal phenotypes of Brca1, Brca2, Brca1/Brca2, Brca1/p53, and Brca2/p53 nullizygous embryos. Genes Dev 1997, 11:1226-
1241. Meyerson NR, Sawyer SL: Two-stepping through time: mammals and viruses. Trends
Microbiol 2011, 19:286-294. Mullen P, Miller WR, Mackay J, Fitzpatrick DR, Langdon SP, Warner JP: BRCA1
5382insC mutation in sporadic and familial breast and ovarian carcinoma in Scotland.
Br J Cancer 1997, 75:1377-1380. O’Connell MJ: Selection and the Cell Cycle: Positive Darwinian Selection in a W O’Donovan PJ, Livingston DM: BRCA1 and BRCA2: breast/ovarian cancer
susceptibility gene products and participants in DNA double-strand break repair.
Carcinogenesis 2010, 31:961-967. Pal T, Permuth-Wey J, Betts JA, et al. BRCA1 and BRCA2 mutations account for a large
proportion of ovarian carcinoma cases. Cancer 2005; 104(12):2807–16. Pavlicek A, Noskov V, Kouprina N, Barrett JC, Jurka J, Larionov V: Evolution of the tumor
suppressor BRCA1 locus in primates: implications for cancer predisposition. Hum Mol
Genet 2004, 13:2737-2751.
Well-Known DNA Damage Response Pathway. J Mol Evol 2010, 71:444-457.

Yang Z, Nielsen R: Codon-substitution models for detecting molecular adaptation at
individual sites along specific lineages. Mol Biol Evol 2002, 19:908-917.