tramadol
DESCRIPTION
TRANSCRIPT

Optimizing postoperative pain con-trol is an important aspect in peri-
operative patient care. Wound infiltrationwith local anesthetics has been the pre-ferred analgesic method since the early20th century.1 Local anesthetic effects ofopioids have been demonstrated in sev-eral studies; tramadol is an analgesicwith different spectrums of activity.2 Itcauses the activation of both opioid andnonopioid (descending monoaminergic)systems, which are mainly involved inthe inhibition of pain. The effect of thenonopioid component of tramadol is me-diated through α2 agonistic and seroton-ergic activities by inhibiting the reuptakeof the norepinephrine and 5-hydroxy-tryptamine, and possibly by displacingstored 5-hydroxytryptamine from nerveendings.3,4 Moreover, as a weak opioid,tramadol is a centrally acting analgesicselective for µ-receptors, with local anes-thetic actions on peripheral nerves.5
The postoperative analgesic effects ofsubcutaneous wound infiltration withtramadol have not been extensively stud-ied and compared with those of intra-venous administration; therefore, the aim
The Annals of Pharmacotherapy n 2009 March, Volume 43 n
Subcutaneous Tramadol Infiltration at the Wound Site Versus
Intravenous Administration after Pyelolithotomy
Mohammad Reza Khajavi, Seyed Babak Mojaver Aghili, Reza Shariat Moharari, Atabak Najafi,
Robab Mohtaram, Patricia Khashayar, and Mojtaba Mojtahedzade
www.theannals.com
Pain Management
Author information provided at the end of thetext.
RESEARCH REPORTS
BACKGROUND: Recently, the peripheral anesthetic effect of tramadol has beenthe theme of many studies. The postoperative analgesic effects of subcutaneouswound infiltration with tramadol have not been extensively studied and comparedwith those of intravenous administration.
OBJECTIVE: To compare the therapeutic effects and complications of intravenousversus local wound infiltration of using tramadol following pyelolithotomy.
METHODS: This double-blind study was carried out on 60 patients (age 18–60 y)of American Society of Anesthesiologists physical status I–II who were awaitingpyelolithotomy in Sina Hospital, Tehran, Iran, during 2006 and 2007. They wererandomly assigned to receive intravenous or subcutaneous wound infiltration withtramadol. Vital signs, the intensity of pain (visual analog scale), and the level ofconsciousness (Ramsey Sedation Scale [RSS]), as well as the frequency ofnausea and vomiting were recorded during 30 minutes to 1 hour after the patiententered the recovery room. Vital signs were also recorded every hour until 6hours postoperatively and then on the day after the patient was transferred to theward.
RESULTS: The RSS was lower in patients who had received subcutaneousinfiltration of tramadol (p < 0.001). A significant difference was noted in theseverity of pain between the groups; it was higher in the group that receivedintravenous tramadol. The average time for the first meperidine requirement was45.2 ± 8.4 min (mean ± SD) in the subcutaneous group and 21.6 ± 12.4 min inthe intravenous group. Total meperidine consumption was lower in patients whohad received subcutaneous wound infiltration with tramadol compared with thosewho had received intravenous tramadol (p < 0.001). Nausea and vomiting weremore frequent during the first hour of recovery; the complication, however, wasless frequent in the subcutaneous group.
CONCLUSIONS: Subcutaneous wound infiltration with tramadol reduces post-operative opioid consumption and produces less nausea and vomiting than doesintravenous administration.
KEY WORDS: meperidine, postoperative analgesia, tramadol, wound infiltration.
Ann Pharmacother 2009;43:xxxx.
Published Online, 3 Mar 2009, www.theannals.com, DOI 10.1345/aph.1L494

of this study was to compare the therapeutic effects andpossible complications of intravenous versus local woundinfiltration of tramadol following pyelolithotomy.
Methods
Following the approval of the institutional ethics com-mittee, a double-blind randomized clinical trial was carriedout in the urology unit of Sina Hospital. Informed consentwas obtained from the patients. All 18- to 60-year-old pa-tients of the American Society of Anesthesiologists physi-cal status I–II who underwent pyelolithotomy during 2006and 2007 were enrolled in the study. A pyelolithotomy isan operation in which renal stones are extracted via a 15-cm incision in the flank. Patients with definite liver disease(eg, acute and chronic hepatitis, cirrhosis, hemochromato-sis); renal impairment (acute and chronic renal failure,glomerulonephritis); history of opium addiction and aller-gy to tramadol; history of seizure disorder; or administra-tion of monoamine oxidase inhibitors, naloxone, yohim-bine, cimetidine, carbamazepine, and ondansetron wereexcluded.
Midazolam 0.04 mg/kg and fentanyl 2 µg/kg were usedas premedication for all patients. Anesthesia induction wasachieved using atracurium 0.5 mg/kg, thiopental sodium 5mg/kg, and lidocaine 1.5 mg/kg. Isoflurane with 1 mini-mum alveolar concentration and O2/N2O 50% was main-tained during the anesthesia period. After acceptable anes-thesia was achieved, a Foley catheter was inserted.
Patients were placed in a flank position during surgery.Bispectral index was maintained between 40 and 50. Until30 minutes before the termination of the operation, fen-tanyl 0.7 µg/kg was injected in patients who experienced a20% increase in blood pressure or heart rate (comparedwith baseline values measured in the ward). Patients whorequired higher doses of opioids were excluded from thestudy.
Isoflurane was discontinued and N2O was increased to70% at the end of the surgery and at the time of suturing.At this time, the patients were randomly assigned to 1 of 2groups, using a computer random number generator: 1group consisted of patients who received subcutaneouswound infiltration with tramadol, and intravenous tra-madol 2 mg/kg was prescribed for the other group. Thecontent of a microset filled with tramadol 2 mg/kg (mini-mum dose 100 mg) plus NaCl 0.9% to a volume of 50 mLwas infused slowly in the intravenous group within 20minutes. Subcutaneous wound infiltration contained tra-madol 2 mg/kg titrated with NaCl 0.9% based on the pa-tient’s weight for a total of 20 mL. Intravenous administra-tion and subcutaneous wound infiltration with tramadolwere performed by the anesthesiologist and the surgeon,respectively. Train of Four (TOF) was assessed with anerve stimulator at the end of the operation by a resident
unaware of the study objectives; N2O was discontinuedand O2 100% was administered if TOF was documented tobe 3 or 4. Muscular relaxation was reversed by neostig-mine 50 µg/kg and atropine 20 µg/kg. The patients’ vitalsigns, including blood pressure and heart rate, were moni-tored at the time of injection.
Vital signs, the intensity of pain as measured by a 10-mm visual analog scale (VAS), the level of consciousnessas measured by Ramsey Sedation Scale (RSS), and com-plications such as nausea and vomiting were recorded by aresident of anesthesiology, unaware of the type of drug ad-ministered to each patient, 30 and 60 minutes after the pa-tient had entered the recovery room.
Patients were transferred to the ward if there were nosigns of complication. Vital signs, pain, nausea, and vomit-ing were recorded every hour until 6 hours postoperativelyand then on the day after they entered the ward. Meperi-dine 0.5 mg/kg was administered intravenously if pain in-tensity was greater than 4 and intravenous metoclopramide10 mg/dose was prescribed if nausea and vomiting werepresent.
STATISTICAL ANALYSIS
Based on a pilot study, the difference between the meanVAS and the mean RSS of the 2 groups was calculated(2.7 ± 3.8 vs 3.2 ± 1.3) and, considering the findings, therequired sample size for each group was calculated to be30. For data analysis, we used independent sample t-tests,Fisher’s exact test, and repeated measures analysis of vari-ance with post hoc tests in SPSS software V. 15.
Results
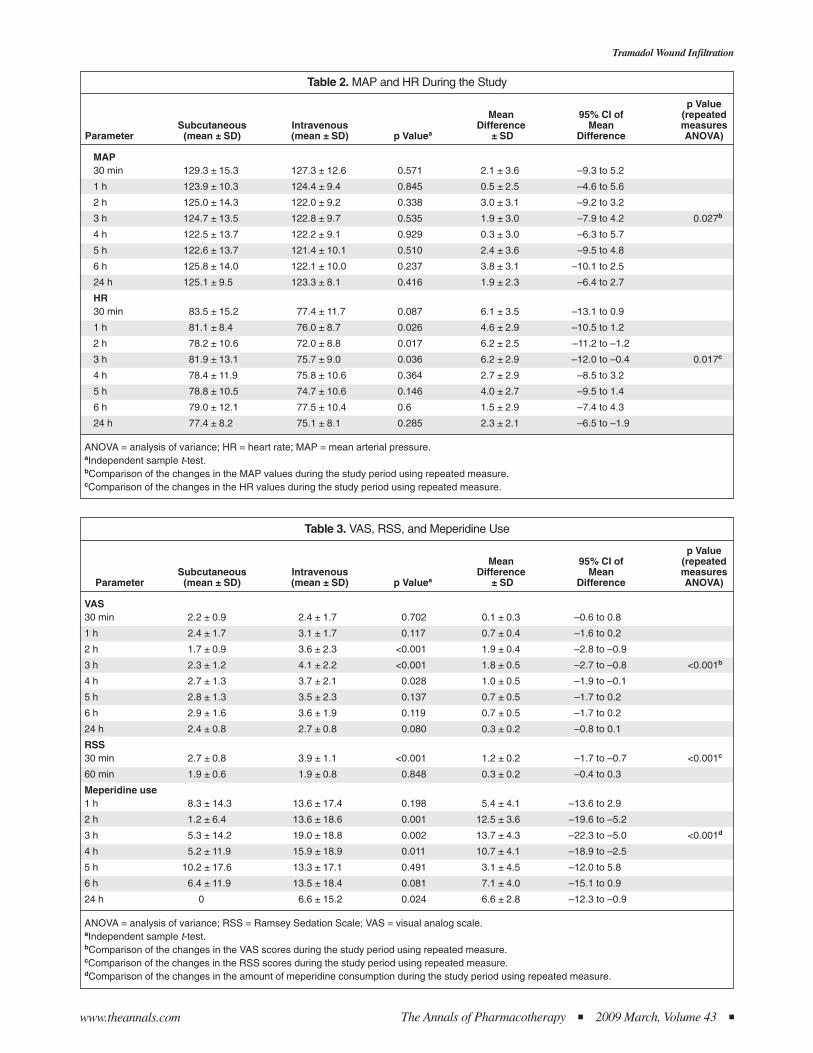
The 60 patients enrolled in the study were divided into 2groups. There were no significant differences in the demo-graphic data of the participants (Table 1). Hemodynamicchanges (mean arterial pressure, heart rate) during thestudy period are listed in Table 2. The mean differences inRSS, VAS, and meperidine consumption in each group
n The Annals of Pharmacotherapy n 2009 March, Volume 43 www.theannals.com
MR Khajavi et al.
Table 1. Patient Characteristicsa
Characteristic Subcutaneous Intravenous p Value
Age (y) 35 ± 2.4 33.8 ± 4.1 0.65b
Male/female 17/13 13/17 0.439c
MAP 122.44 ± 2.5 124.21 ± 1.9 0.170b
HR 71.09 ± 3.27 68.66 ± 2.71 0.431b
Operation time (min) 120 ± 15 110 ± 25 0.284b
HR = heart rate; MAP = mean arterial pressure.aMean ± SD. bIndependent sample t-test.cFisher’s exact test.
Tramadol Wound Infiltration
The Annals of Pharmacotherapy n 2009 March, Volume 43 nwww.theannals.com
Table 3. VAS, RSS, and Meperidine Use
p ValueMean 95% CI of (repeated
Subcutaneous Intravenous Difference Mean measuresParameter (mean ± SD) (mean ± SD) p Valuea ± SD Difference ANOVA)
VAS30 min 2.2 ± 0.9 2.4 ± 1.7 0.702 0.1 ± 0.3 –0.6 to 0.8
1 h 2.4 ± 1.7 3.1 ± 1.7 0.117 0.7 ± 0.4 –1.6 to 0.2
2 h 1.7 ± 0.9 3.6 ± 2.3 <0.001 1.9 ± 0.4 –2.8 to –0.9
3 h 2.3 ± 1.2 4.1 ± 2.2 <0.001 1.8 ± 0.5 –2.7 to –0.8 <0.001b
4 h 2.7 ± 1.3 3.7 ± 2.1 0.028 1.0 ± 0.5 –1.9 to –0.1
5 h 2.8 ± 1.3 3.5 ± 2.3 0.137 0.7 ± 0.5 –1.7 to 0.2
6 h 2.9 ± 1.6 3.6 ± 1.9 0.119 0.7 ± 0.5 –1.7 to 0.2
24 h 2.4 ± 0.8 2.7 ± 0.8 0.080 0.3 ± 0.2 –0.8 to 0.1
RSS30 min 2.7 ± 0.8 3.9 ± 1.1 <0.001 1.2 ± 0.2 –1.7 to –0.7 <0.001c
60 min 1.9 ± 0.6 1.9 ± 0.8 0.848 0.3 ± 0.2 –0.4 to 0.3
Meperidine use1 h 8.3 ± 14.3 13.6 ± 17.4 0.198 5.4 ± 4.1 –13.6 to 2.9
2 h 1.2 ± 6.4 13.6 ± 18.6 0.001 12.5 ± 3.6 –19.6 to –5.2
3 h 5.3 ± 14.2 19.0 ± 18.8 0.002 13.7 ± 4.3 –22.3 to –5.0 <0.001d
4 h 5.2 ± 11.9 15.9 ± 18.9 0.011 10.7 ± 4.1 –18.9 to –2.5
5 h 10.2 ± 17.6 13.3 ± 17.1 0.491 3.1 ± 4.5 –12.0 to 5.8
6 h 6.4 ± 11.9 13.5 ± 18.4 0.081 7.1 ± 4.0 –15.1 to 0.9
24 h 0 6.6 ± 15.2 0.024 6.6 ± 2.8 –12.3 to –0.9
ANOVA = analysis of variance; RSS = Ramsey Sedation Scale; VAS = visual analog scale.aIndependent sample t-test.bComparison of the changes in the VAS scores during the study period using repeated measure.cComparison of the changes in the RSS scores during the study period using repeated measure.dComparison of the changes in the amount of meperidine consumption during the study period using repeated measure.
Table 2. MAP and HR During the Study
p ValueMean 95% CI of (repeated
Subcutaneous Intravenous Difference Mean measuresParameter (mean ± SD) (mean ± SD) p Valuea ± SD Difference ANOVA)
MAP30 min 129.3 ± 15.3 127.3 ± 12.6 0.571 2.1 ± 3.6 –9.3 to 5.2
1 h 123.9 ± 10.3 124.4 ± 9.4 0.845 0.5 ± 2.5 –4.6 to 5.6
2 h 125.0 ± 14.3 122.0 ± 9.2 0.338 3.0 ± 3.1 –9.2 to 3.2
3 h 124.7 ± 13.5 122.8 ± 9.7 0.535 1.9 ± 3.0 –7.9 to 4.2 0.027b
4 h 122.5 ± 13.7 122.2 ± 9.1 0.929 0.3 ± 3.0 –6.3 to 5.7
5 h 122.6 ± 13.7 121.4 ± 10.1 0.510 2.4 ± 3.6 –9.5 to 4.8
6 h 125.8 ± 14.0 122.1 ± 10.0 0.237 3.8 ± 3.1 –10.1 to 2.5
24 h 125.1 ± 9.5 123.3 ± 8.1 0.416 1.9 ± 2.3 –6.4 to 2.7
HR30 min 83.5 ± 15.2 77.4 ± 11.7 0.087 6.1 ± 3.5 –13.1 to 0.9
1 h 81.1 ± 8.4 76.0 ± 8.7 0.026 4.6 ± 2.9 –10.5 to 1.2
2 h 78.2 ± 10.6 72.0 ± 8.8 0.017 6.2 ± 2.5 –11.2 to –1.2
3 h 81.9 ± 13.1 75.7 ± 9.0 0.036 6.2 ± 2.9 –12.0 to –0.4 0.017c
4 h 78.4 ± 11.9 75.8 ± 10.6 0.364 2.7 ± 2.9 –8.5 to 3.2
5 h 78.8 ± 10.5 74.7 ± 10.6 0.146 4.0 ± 2.7 –9.5 to 1.4
6 h 79.0 ± 12.1 77.5 ± 10.4 0.6 1.5 ± 2.9 –7.4 to 4.3
24 h 77.4 ± 8.2 75.1 ± 8.1 0.285 2.3 ± 2.1 –6.5 to –1.9
ANOVA = analysis of variance; HR = heart rate; MAP = mean arterial pressure.aIndependent sample t-test.bComparison of the changes in the MAP values during the study period using repeated measure.cComparison of the changes in the HR values during the study period using repeated measure.

during the study period are outlined in Table 3. RSS wasreported to be lower in the group that received subcuta-neous versus intravenous wound infiltration with tramadol(2.7 ± 0.8 vs 3.9 ± 1.1, respectively); a significant differ-ence was found between the 2 groups within the first 30minutes (p = 0.006).
The VAS score in the first 30 minutes following the op-eration was 2.2 ± 0.9 in the subcutaneous group and 2.4 ±1.7 in the intravenous group. The VAS score was reportedto be higher in the group that received intravenous tra-madol throughout the study (Figure 1). These scores werefound to be significant at 2 (p < 0.001), 3 (p < 0001), and 4(p = 0.028) hours.
The average time for the first meperidine requirementwas 45.2 ± 8.4 minutes in the subcutaneous group and 21.6± 12.4 minutes in the intravenous group (p < 0.001). Totalmeperidine consumption was lower in the group that re-ceived subcutaneous wound infiltration with tramadol.This difference was statistically significant in the fourthhour and a day following the operation (4 h 5.2 ± 11.9 mg[subcutaneous] vs 15.9 ± 18.9 mg [intravenous]; 24 h [sub-cutaneous] vs 6.6 ± 15.2 mg [intravenous]).
Considering both groups, nausea and vomiting were fre-quently reported during the first hours of recovery(31.7%); the complication, however, was less frequent 6hours after the operation (Table 4). Nausea and vomitingoccurred less frequently in the subcutaneous group
throughout the study period. None of the subjects com-plained about peri-incisional allodynia or hyperalgesia dur-ing the study period.
Discussion
Opioids have long been the mainstay for postoperativepain relief; however, the high rates of adverse effects pro-vide an impetus to investigate alternatives. Recent studieshave shown that localized use of these drugs can overcomethe associated problems.6-8
Many studies have shown that the peripheral local anes-thetic effects of tramadol are related to those of codeine.2,9,10
According to these studies, the suggested sites of action forthis drug are the nerve endings as well as a possible associat-ed central effect. In this study, we demonstrated that subcu-taneous wound infiltration with tramadol followingpyelolithotomy is associated with a lower incidence ofnausea and vomiting, reduced need for meperidine, de-crease in VAS scores, and lower RSS level.
There was no significant difference between the finalmean arterial pressure and heart rate of the 2 groups; thiscould be due to complete absorption of tramadol after it isinfiltrated into the wound, along with good pain control inthe 2 groups. However, a significant change in mean arteri-al pressure was reported over time in each group; this wasnot related to the method by which tramadol was adminis-
n The Annals of Pharmacotherapy n 2009 March, Volume 43 www.theannals.com
MR Khajavi et al.
Figure 1. Mean pain severity (VAS) in each group (repeated measures analysis with comparing factor, p < 0.001). IV = intravenous administration;SC = subcutaneous wound infiltration; VAS = visual analog scale.

tered. These findings were similar to the results of thestudy conducted by Pang et al.6 In that study, they showedthat there was no significant difference in arterial bloodpressure, heart rate, and respiratory depression followingintramuscular and intravenous injection of the analgesic.
Several studies have noted that use of analgesic agentssuch as tramadol during surgery lowers a patient’s postop-erative need for morphine. Unlugenc et al.11 found a con-siderable decrease in morphine consumption following tra-madol administration after major abdominal surgery. Al-tunkaya et al.12 showed that the duration of postoperativeanalgesia provided by subcutaneous wound infiltrationwith tramadol was significantly longer compared with thelength achieved with lidocaine. Similarly, in our study,there was a significant decrease in the postoperative de-mand for analgesia in the group that received subcuta-neous wound infiltration with tramadol. This fact demon-strates the higher effectiveness of subcutaneous wound in-filtration with tramadol, possibly due to its concurrent localand systemic effects.
Immer et al.13 could not identify any significant differ-ences in VAS, morphine consumption, or antiemetic re-quirement following tramadol administration; this wascontrary to the findings of our study. Nausea and vomitingare the major adverse effects of tramadol.14,15 The rate oftitration of the tramadol dose, rather than the target dose, isthe major determinant of a patient’s tolerability; therefore,our patients experienced less nausea and vomiting whenreceiving tramadol via subcutaneous wound infiltration.16
Yet, there is no report of such complications followingsubcutaneous wound infiltration with tramadol.6 Anotherstudy demonstrated skin rash due to histamine release aftertramadol injection17; however, such a complication was ab-sent in our study.
Similar to other studies, our study concluded that intra-venous administration of tramadol is accompanied by
more complications, as well as a longer recovery time(higher RSS), compared with localized subcutaneous infil-tration.18
We did not evaluate the link between tramadol’s bloodconcentrations and the resulting analgesic effects. We rec-ommend that the serum concentration of tramadol and thekey pharmacokinetic parameters be determined to estab-lish a dose–response relationship and the reliability for thismethod of drug administration.
In conclusion, following subcutaneous wound infiltra-tion with tramadol, postoperative analgesia was prolongedand the need for more opioid was reduced considerably.However, administration of tramadol at the operation siterequires further studies.
Mohammad Reza Khajavi MD, Associate Professor of Anesthe-siology, Tehran University of Medical Sciences, Sina Hospital, Tehran,Iran Seyed Babak Mojaver Aghili MD, Resident of Anesthesiology,Tehran University of Medical Sciences, Sina HospitalReza Shariat Moharari MD, Assistant Professor of Anesthesiology,Tehran University of Medical Sciences, Sina Hospital Atabak Najafi MD, Associate Professor of Anesthesiology, TehranUniversity of Medical Sciences, Sina HospitalRobab Mohtaram MD, Assistant Professor of Anesthesiology,Tehran University of Medical Sciences, Farabi Hospital, Tehran, SinaHospital Patricia Khashayar MD, General Practitioner, Research and De-velopment Center, Tehran University of Medical Sciences, Sina Hos-pital Mojtaba Mojtahedzade PharmD, Professor of Pharmacotherapy,Tehran University of Medical Sciences, Sina Hospital Reprints: Dr. Reza Shariat Moharari, Tehran University of MedicalSciences, Sina Hospital, Hassan Abad Square, Tehran, Iran, fax 98-2188276654, [email protected], [email protected]
We are indebted to the Research and Development Center of Sina Hospital for theirsupport. We acknowledge Gazelle Shariat Moharari, biology student, for her reviewand helpful comments on this article. We also thank Mohsen Rezaii MD for his sup-port and comments regarding the statistics of the study.
References
1. Brower MC, Johnson ME. Adverse effects of local anesthetic infiltrationon wound healing. Reg Anaesth Pain Med 2003;28:233-40.
2. Altunkaya H, Ozer Y, Kargi E, Babuccu O. Comparison of local anaes-thetic effects of tramadol with prilocaine for minor surgical procedures.Br J Anaesth 2003;90:320-2.
3. Desmeules JA, Piguet V, Collart L, Dayer P. Contribution of monoamin-ergic modulation to the analgesic effect of tramadol. Br J Clin Pharmacol1996;41:7-12.
4. Mert T, Gunes Y, Guven M, Gunay I, Ozcengiz D. Comparison of nerveconduction blocks by an opioid and a local anesthetic. Eur J Pharmacol2002;439:77-81.
5. Altunkaya H, Ozer Y, Kargi E, Babuccu O. Comparison of local anaes-thetic effects of tramadol with prilocaine for minor surgical procedures.Br J Anaesth 2003;90:320-2.
6. Pang WW, Huang PY, Chang DP, Huang MH. The peripheral analgesiceffect of tramadol in reducing propofol injection pain: a comparison withlidocaine. Reg Anaesth Pain Med 1999;24:246-9.
7. Raffa RB, Friderich E, Reimann W, Shank RP, Codd EE, Vaught JL.Opioid and non opioid components independently contribute to themechanism of action of tramadol, an atypical opioid analgesic. J Phar-macol Exp Ther 1992;260:257-85.
Tramadol Wound Infiltration
The Annals of Pharmacotherapy n 2009 March, Volume 43 nwww.theannals.com
Table 4. Frequency of Nausea and Vomiting in Each Group During the Study
Subcutaneous IntravenousTime (%) (%) p Valuea p Valueb
30 min 1 (3.3) 10 (33.3) 0.006
1 h 3 (10) 16 (53.3) <0.001
2 h 0 13 (43.3) <0.001
3 h 2 (6.7) 12 (40) 0.002 <0.001c
4 h 1 (3.3) 9 (30) <0.001
5 h 0 8 (26.7) 0.002
6 h 2 (6.7) 6 (20) 0.254
aFisher’s exact testbRepeated measure analysis of variance.cComparison of the incidence of nausea and vomiting during the studyperiod using repeated measure.

8. Pang WW, Mok MS, Chang DP, Huang MH. Local anesthetic effects oftramadol, metoclopramide and lidocaine following intradermal injection.Reg Anesth Pain Med 1998;23:580-3.
9. Tsai YC, Chang PJ, Jou IM. Direct tramadol application on sciatic nerveinhibits spinal somatosensory evoked potentials in rats. Anesth Analg2001;92:1547-51.
10. Kapral S, Gollmann G, Waltl B, et al. Tramadol added to mepivacaineprolongs the duration of an axillary brachial plexus blockade. AnesthAnalg 1999;88:853-6.
11. Unlugenc H, Ozalevli M, Gunes Y. Pre-emptive analgesic efficacy of tra-madol compared with morphine after major abdominal surgery. Br JAnaesth 2003;91:209-13.
12. Altunkaya H, Ozer Y, Kargi E, et al. The postoperative analgesic effectof tramadol when used as subcutaneous local anesthetic. Anesth Analg2004;99:1461-4.
13. Immer FF, Immer Bansi AS, Trachsel N, et al. Pain treatment with aCOX-2 inhibitor after coronary artery bypass. Ann Thoracic Surg 2003;75:490-5.
14. Demiraran Y, Ilce Z, Kocaman B, Bozkurt P. Does tramadol wound in-filtration offer an advantage over bupivacaine for postoperative analgesiain children following herniotomy? Pediatr Anesth 2006;16:1047-50.
15. Shipton EA. Tramadol: present and future. Anesth Intensive Care 2000;28:363-74.
16. Petrone D, Kamin M, Olson W. Slowing the titration rate of tramadolHCl reduces the incidence of discontinuation due to nausea and/or vom-iting: a double-blind randomized trial. J Clin Pharm Ther 1999;24:115-23.
17. Acalovschi I, Cristea T, Margarit S, Gavrus R. Tramadol added to lido-caine for intravenous regional anesthesia. Anesth Analg 2001;92:209-14.
18. But AK, Erdil F, Yucel A, Gedik E, Durmus M, Ersoy MO. The effect ofsingle dose tramadol on post operative pain and morphine requirementsafter coronary artery bypass. Acta Anaesthesiol Scand 2007;51:601-6.
La Infiltración Subcutánea de Tramadol en el Lugar de la Herida enComparación con la Administración Intravenosa Después de unaPielolitotomía
MR Khajavi, SBM Aghili, RS Moharari, A Najafi, R Mohtaram, PKhashayar, y M Mojtahedzade
Ann Pharmacother 2009;43:xxxx.
EXTRACTO
TRASFONDO: Recientemente, el efecto anestésico periférico del tramadolha sido el tema de muchos estudios. Los efectos analgésicos postoperatori-os de la infiltración subcutánea del tramadol en la herida no han sidoampliamente estudiados ni comparados con los de la administraciónintravenosa.
OBJETIVOS: El propósito de este estudio fue comparar los efectos terapéuti-cos y las complicaciones de la administración intravenosa en comparacióncon la infiltración local en la herida al usar el tramadol después de unapielolitotomía.
MÉTODOS: Este estudio doble ciego fue llevado a cabo en 60 pacientes, conun estado físico I-II según la ASA en un grupo de edad de 18 a 60 añosen espera de una pielolitotomía en el Hospital de Sina durante 2006 y2007. Los pacientes fueron asignados al azar a recibir tramadolintravenoso o mediante infiltración subcutánea en la herida.
Se registraron los signos vitales, la intensidad del dolor (VAS) y el nivelde consciencia (Escala de Sedación de Ramsey [RSS]) al igual que lafrecuencia de las náuseas y los vómitos durante 30 minutos a una horadespués de que el paciente entrara a la sala de recuperación. También, seregistraron cada hora durante 6 horas y luego el día después de entrar ala habitación.
RESULTADOS: La RSS fue menor en los que habían recibido la infiltraciónsubcutánea de tramadol (p < 0.001). Se observó una diferencia significativaen cuanto a la severidad del dolor entre los grupos. Ésta fue mayor en elgrupo que recibió el tramadol intravenoso. El tiempo promedio para
requerir la primera dosis de la meperidina fue 45.2 ± 8.4 minutos en elgrupo SC y 21.6 ± 12.4 minutos en el grupo IV. El uso total de lameperidina fue menor en el grupo que había recibido la infiltraciónsubcutánea de tramadol en la herida en comparación con los que habíanrecibido el tramadol intravenoso (p < 0.001). La náusea y el vómito fueronmás frecuentes durante la primera hora de la recuperación; sin embargo,la complicación fue menos frecuente en el grupo SC.
CONCLUSIONES: La infiltración subcutánea de tramadol en la herida reduceel uso postoperatorio de opiodes y se produce menos náusea y vómitoque con el uso IV.
Traducido por Rafaela Mena
n The Annals of Pharmacotherapy n 2009 March, Volume 43 www.theannals.com
MR Khajavi et al.