transitioning to icd-10 - sohn nursesohnnurse.com/wp-content/uploads/pdf/313 pollock... ·...
TRANSCRIPT

Transitioning to ICD-10
Sponsored by:
Society of Otorhinolaryngology and
Head-Neck Nurses
Vancouver, Canada
September 29, 2013 Presented by:
Kim Pollock, RN, MBA, CPC

Here’s How To Reach Us…
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
2 CPT only © 2012 American Medical Association. All Rights Reserved
Be sure to visit our website for useful practice management ideas and course information!
www.karenzupko.com
KZA Disclaimer
This manual is not intended to provide legal advice to physicians and their staffs. If you have specific questions regarding the permissibility of your billing or other practices, we recommend that you consult legal counsel directly for assistance in evaluating any legal, regulatory or compliance issues regarding these matters. In the event that you choose to consult with outside legal counsel, KZA is available to work with such counsel, as appropriate, to meet your needs.
CPT five digit codes, nomenclature and other data are copyright 2012 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values or related listings are included in CPT. The AMA assumes no liability for the data contained herein.
Kim Pollock, RN, MBA, CPC
Consultant and Speaker
For almost twenty years, Kim Pollock has been nationally recognized as an otolaryngology coding expert including all subspecialties. Additionally, she has demonstrated expertise in improving collections, decreasing expense, minimizing risk and enhancing efficiencies in large group practices, as well as academic and solo practices. She knows how to apply reimbursement principles to ensure otolaryngologists are paid accurately. She has over thirty years of healthcare experience working for and with otolaryngologists.
Ms. Pollock understands the complexity of coding and reimbursement issues specific to otolaryngologists – both from a clinical perspective and from a payor side. She is a nationally recognized authority in coding and analyzing chart documentation.
She presents seminars and workshops for physicians and their staff on behalf of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNSF), the American Association of Neurological Surgeons and the American Society of Plastic Surgeons. Ms. Pollock has also conducted programs for the American Academy of Professional Coders, the North American Spine Society, the American Neurotology Society and the Congress of Neurological Surgeons.
Based on her previous years of administrative experience, Ms. Pollock has a unique understanding of the challenges facing academic medicine both clinically and organizationally. She has served as the Administrator of the Department of Otorhinolaryngology, where she was a member of the Association of Otolaryngology Administrators, as well as Associate Vice President of Cancer Programs at the University of Texas Southwestern Medical Center in Dallas.
Ms. Pollock was the representative for the AAO-HNS on the clinical practice expert panel-technical group (CPEP-TEG) convened by CMS (formerly HCFA) to redetermine the practice expense portion of RBRVS. She served two terms on the Board of Directors for the Society of Otorhinolaryngology and Head-Neck Nurses, Inc. (SOHN) and has served on the Board for the Ear, Nose and Throat Nursing Foundation.
Ms. Pollock is the recipient of the prestigious Presidential Citation Award from the SOHN as well as an Honor Award from the AAO-HNSF.

What’s ICD-10?
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
3 CPT only © 2012 American Medical Association. All Rights Reserved
International Classification of Diseases, 10th Revision, Clinical Modification
We are currently using ICD-9-CM
Codes are used to calculate MS-DRG payments
Compile statistics
Already being used in 138 countries for mortality reporting, 99 countries for morbidity. US implemented for mortality on 1/1/99.
Other countries use ICD-10 for reimbursement or case mix: UK, Denmark, Finland, Iceland, Norway, Sweden, France, Australia, Belgium, Germany, Canada
Why Are We Changing?
ICD-9 is out of date and running out of space for new codes
ICD-10 is the international standard to report and monitor disease and mortality – USA must adopt for reporting and surveillance
ICD codes are core elements of many health information technology systems making the conversion to ICD-10-CM necessary to fully realize benefits of HIT adoption
FIRM ICD-10 DEADLINE
OCT 1, 2014

Dirty Dozen ICD-10
Action Agenda
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
4 CPT only © 2012 American Medical Association. All Rights Reserved
1. Run an ICD-9 frequency report from your practice management system for
each doctor or provider for the last 12 months. Focus on the top 25
diagnosis codes.
10-25 Top Most Used Frequency Codes
Diagnosis Code
Description Number of Charges
380.4 Impacted cerumen 460
472.0 Chronic rhinitis 256
382.1
Chronic tubotympanic suppurative otitis media, Benign chronic suppurative otitis media (with anterior perforation of ear drum), Chronic tubotympanic disease (with anterior perforation of ear drum)
253
478.0 Hypertrophy of nasal turbinates 244
476.0 Chronic laryngitis 205
780.4 Dizziness and giddiness, Lightheadedness, Vertigo 152
784.7 Epistaxis 152
389.10 Sensorineural hearing loss, unspecified 133
474.00 Chronic tonsillitis 124
470 Deviated nasal septum 124
See if you can run this valuable data!
Diagnosis Diagnosis Description Charges
Total Insurance Payments
Patient Payments
Total Payments
Charge Flag
715.16 OSTEOARTHRITIS KNEE DJD 465,292.78 149,858.59 22,201.08 172,059.67 1,059
726.10 TENDINITIS/BURSITIS SHOULDER
94,311.00 32,864.94 7,383.28 40,248.22 526
719.46 PAIN KNEE /PATELLOFEMORAL SYNDROME
53,831.00 18,899.07 8,740.03 27,639.10 370
836.0 TEAR OF MEDIAL CARTILAGE OR MENISCUS OF KNEE, CURR
144,250.01 43,335.61 12,188.79 55,524.40 360
847.2 LUMBAR SPRAIN AND STRAIN 45,440.00 18,622.16 4,352.74 22,974.90 275
726.5 BURSITISITEND-HIP,TROCHANTERIC,LEG
31,848.00 9,744.27 2,287.40 12,031.67 216
715.35 LOCALIZED OSTEOARTHROSIS NOT SPECIFIED WHETHER PRI
91,979.00 30,839.96 6,065.04 36,905.00 171
845.02 SPRAIN AND STRAIN OF CALCANEOFIBULAR (LIGAMENT)
23,544.00 8,231.70 3,742.62 11,974.32 159
845.00 UNSPECIFIED SITE OF ANKLE SPRAIN AND STRAIN
15,685.00 5,512.86 3,007.57 8,520.43 117
842.00 SPRAIN/TEAR RUPTURE- WRIST.LIG.,AVN,MUSCLE
15,343.00 6,145.57 1,654.46 7,800.03 112

Dirty Dozen ICD-10
Action Agenda
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
5 CPT only © 2012 American Medical Association. All Rights Reserved
Compare ICD-9 to ICD-10: Dr. A Top Codes
ICD-9 ICD-9 Description ICD-10 ICD-10 Description
380.4 Impacted cerumen H61.2Ø Impacted cerumen, unspecified ear
H61.21 Impacted cerumen, right ear
H62.22 Impacted cerumen, left ear
H62.23 Impacted cerumen, bilateral
780.4 Dizziness and giddiness, Lightheadedness, Vertigo
R42 Dizziness and giddiness, Lightheadedness, Vertigo
Compare ICD-9 to ICD-10: Dr. B Top Codes
ICD-9 ICD-9 Description ICD-10 ICD-10 Description
V50.1 Elective surgery plastic surgery unacceptable cosmetic appearance
Z411 Encounter for cosmetic surgery
216.3 Benign neoplasm skin face other unspecified part
D22.3Ø Melanocytic nevi of unspecified part of the face
D22.39 Melanocytic nevi of other parts of the face
D23.3Ø Other benign neoplasm of skin of unspecified part of face
D23.39 Other benign neoplasm of skin of other parts of face
873.41 Open wound cheek, without mention of complication
SØ1.4Ø1A Unspecified open wound of right cheek and temporomandibular area, initial encounter
SØ1.4Ø2A Unspecified open wound of left cheek and temporomandibular area, initial encounter
SØ1.4Ø9A Unspecified open wound of unspecified cheek and temporomandibular area, initial encounter
SØ1.411A Laceration without foreign body of right cheek and temporomandibular area, initial encounter
SØ1.412A Laceration without foreign body of left cheek and temporomandibular area, initial encounter
SØ1.419A Laceration without foreign body of unspecified cheek and temporomandibular area, initial encounter
SØ1.431A Puncture wound without foreign body of right cheek and temporomandibular area, initial encounter
SØ1.432A Puncture wound without foreign body of left cheek and temporomandibular area, initial encounter
SØ1.439A Puncture wound without foreign body of unspecified cheek and temporomandibular area, initial encounter
SØ1.451A Open bite of right cheek and temporomandibular area, initial encounter
SØ1.452A Open bite of left cheek and temporomandibular area, initial encounter
SØ1.459A Open bite of unspecified cheek and temporomandibular area, initial encounter
*The appropriate 7th character needs to be added to each code:
A = Initial encounter D = Subsequent encounter S = Sequela

Dirty Dozen ICD-10
Action Agenda
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
6 CPT only © 2012 American Medical Association. All Rights Reserved
2. Now, pull operative reports for the top FIVE procedures you do.
See if using your present level of documentation staff can find an ICD-10 code. If
they can’t—have them write a memo of what’s missing for you. Budget two weeks
for the five procedures.
This is a retrospective gap analysis. It is based on YOUR practice reality. No one
else’s.
Pay special attention to laterality, late effects and sequelae.
Improve your dictation or documentation templates accordingly.
Now do the next five conditions and corresponding reports. You should be done
with your top 25 by the end of Q1 or early Q2.
3. Armed with good technology, well educated staff should begin by the end of the
first quarter coding at least 50% of your cases in both diagnosis coding
systems. Practice makes perfect.
4. Check what your software vendor has to offer in terms of resources and
support. Check what the clearinghouse offers.
Discuss at a partner’s meeting or one-on-one sessions with each physician.
Who will lead this effort?
Anatomy + Terminology + Physiology Training Helps in Accurate Coding!

Dirty Dozen ICD-10
Action Agenda
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
7 CPT only © 2012 American Medical Association. All Rights Reserved
5. Estimate what the transition is going to cost your practice.
6. Investigate revised, changed medical necessity guidelines for top five diagnoses for
three payors.
7. http://www.anthem.com/medicalpolicies/policies/mp_pw_a053311.htm
ICD-10 Coding (Effective October 1, 2014)
In preparation for the implementation of ICD-10 CM and ICD-10 PCS, we are updating
medical policies and clinical UM guidelines on a quarterly basis to include proposed
ICD-10 coding. The ICD-10 coding is available through either a hyperlinked Appendix or
a listing of applicable ICD-10 codes within the Coding section. Please note that at this
time, the ICD-10 code list may not be all inclusive and is subject to change as Position
Statements may be updated. Feel free to send comments regarding the ICD-10 coding
using the Contact Us link below.

Dirty Dozen ICD-10
Action Agenda
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
8 CPT only © 2012 American Medical Association. All Rights Reserved
Source: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNMattersArticles/Downloads/MM8348.pdf
8. At the first available opportunity (6 to 9 months out) run some tests with your
software and clearinghouse and biggest payers to see if it is all working correctly
enough to generate payments.
Whose job?

Dirty Dozen ICD-10
Action Agenda
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
9 CPT only © 2012 American Medical Association. All Rights Reserved
9. Take advantage of resources for ICD-10.
AAOHNS: http://entnet.org/Practice/International-Classification-of-Diseases-ICD.cfm
KZA: Take advantage of webinars that are planned. www.karenzupko.com
10. Sharpen practice collection skills. All sources are predicting cash flow
slowdowns. If you are collecting at 87% functionality, that’s not good enough and
work now to improve.
11. Delay bonuses! Reserve money, “just in case.”
12. Obtain a LOC. Shoot for 1st quarter.
This is serious!
ALERT
Plan your schedule! To extent possible, schedule as much surgery and as many patients as possible in September as possible (unfortunately a historically low period for otolaryngologists!). Get those claims in ASAP so your cash flow is high.

Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
10 CPT only © 2012 American Medical Association. All Rights Reserved
New!
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
11 CPT only © 2012 American Medical Association. All Rights Reserved
NUCC recommends April 1 implementation of new 1500 claim form
The National Uniform Claim Committee (NUCC) approved a transition timeline
for the version 02/12 1500 Health Insurance Claim Form (1500 claim form). The
updated form accommodates ICD-10 reporting and aligns with additional
requirements identified by the industry. MGMA serves on the NUCC.
Changes incorporated into the new 1500 claim form include:
An indicator in Item Number 21 to identify the version of the diagnosis
code set being reported (i.e., ICD-9 or ICD-10). This indicator will be
important during the implementation period for ICD-10.
Expansion of the number of diagnosis codes that can be reported in Item
Number 21, which was increased from 4 to 12.
The ability to identify the role of the provider reported in Item Number 17
and the specific dates reported in Item Number 14.
The NUCC approved the following 2014 transition timeline:
Jan. 6: Payers begin receiving and processing paper claims submitted on
the revised 1500 claim form (version 02/12).
Jan. 6 through March 31: Dual use period during which payers continue to
receive and process paper claims submitted on the old 1500 claim form
(version 08/05).
April 1: Payers receive and process paper claims submitted only on the
revised 1500 claim form (version 02/12).
Although the NUCC timeline is not binding on commercial health plans, it does
align with Medicare's announced transition timeline. Medicare has indicated it will
reject claims submitted on the old claim form after April 1.

ICD-9 vs. ICD-10
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
12 CPT only © 2012 American Medical Association. All Rights Reserved
ICD-9-CM
3-5 characters in length
1st digit may be alpha, but is usually numeric; 2nd-5th is numeric
Approximately 14,000 codes
Limited space for adding new codes
Lacks detail
Lacks laterality
Difficult to analyze data due to non-specific codes
Codes are non-specific and do not adequately define diagnosis needed
for medical reesearch
Does not support interoperatbility because it's not used by other
countries
ICD-10-CM
3-7 characters in length
Character 1 is alpha; character s 2 & 3 are numeric; characters 4-6 can be
either alpha or numeric
Approximately 69,000 codes
Flexible for adding new codes
Very specific
Has laterality
Specificity improves coding accuracy and richness of data for analysis
Detail improves the accuracy of data used for medical research
Supports interoperability and the exchange of health data between
other countries & the U.S.

ICD-9 vs. ICD-10
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
13 CPT only © 2012 American Medical Association. All Rights Reserved
ICD-10 CM Examples
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
14 CPT only © 2012 American Medical Association. All Rights Reserved
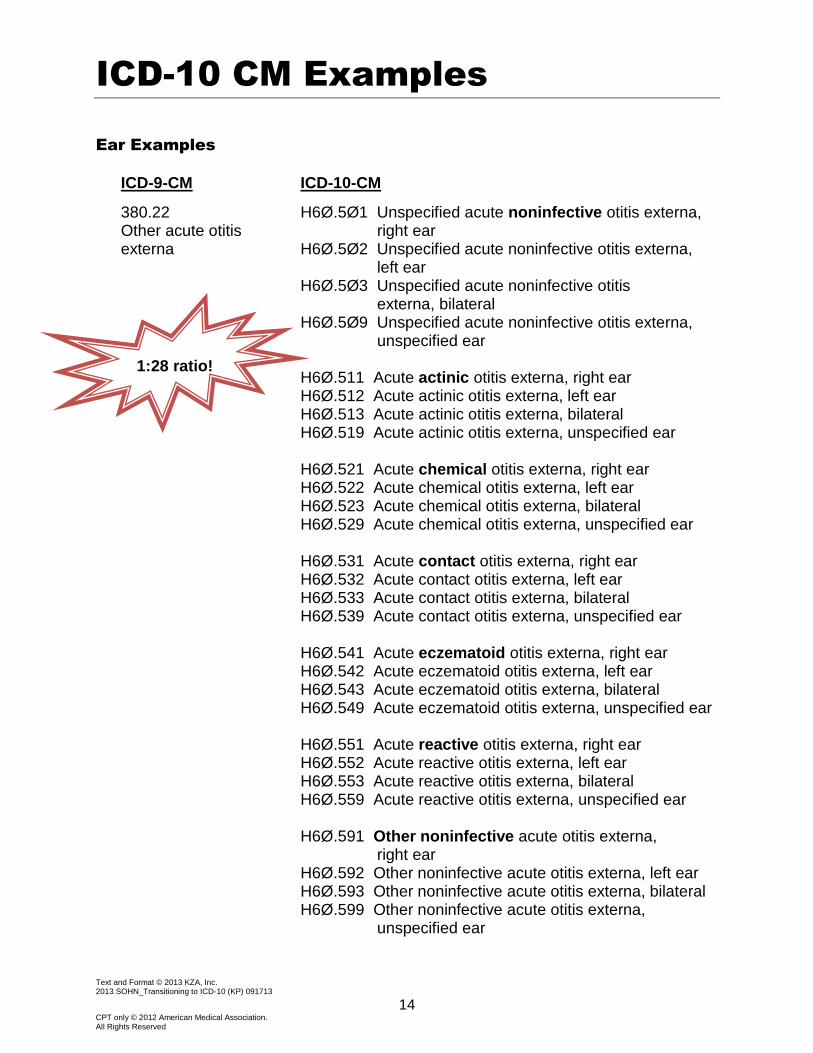
Ear Examples
ICD-9-CM ICD-10-CM
380.22 Other acute otitis externa
H6Ø.5Ø1 Unspecified acute noninfective otitis externa, right ear
H6Ø.5Ø2 Unspecified acute noninfective otitis externa, left ear
H6Ø.5Ø3 Unspecified acute noninfective otitis externa, bilateral
H6Ø.5Ø9 Unspecified acute noninfective otitis externa, unspecified ear
H6Ø.511 Acute actinic otitis externa, right ear
H6Ø.512 Acute actinic otitis externa, left ear H6Ø.513 Acute actinic otitis externa, bilateral H6Ø.519 Acute actinic otitis externa, unspecified ear
H6Ø.521 Acute chemical otitis externa, right ear
H6Ø.522 Acute chemical otitis externa, left ear H6Ø.523 Acute chemical otitis externa, bilateral H6Ø.529 Acute chemical otitis externa, unspecified ear
H6Ø.531 Acute contact otitis externa, right ear
H6Ø.532 Acute contact otitis externa, left ear H6Ø.533 Acute contact otitis externa, bilateral H6Ø.539 Acute contact otitis externa, unspecified ear
H6Ø.541 Acute eczematoid otitis externa, right ear
H6Ø.542 Acute eczematoid otitis externa, left ear H6Ø.543 Acute eczematoid otitis externa, bilateral H6Ø.549 Acute eczematoid otitis externa, unspecified ear
H6Ø.551 Acute reactive otitis externa, right ear
H6Ø.552 Acute reactive otitis externa, left ear H6Ø.553 Acute reactive otitis externa, bilateral H6Ø.559 Acute reactive otitis externa, unspecified ear
H6Ø.591 Other noninfective acute otitis externa,
right ear H6Ø.592 Other noninfective acute otitis externa, left ear H6Ø.593 Other noninfective acute otitis externa, bilateral H6Ø.599 Other noninfective acute otitis externa,
unspecified ear
1:28 ratio!

ICD-10 CM Examples
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
15 CPT only © 2012 American Medical Association. All Rights Reserved
Ear Examples (continued)
ICD-9-CM ICD-10-CM
380.12 Acute swimmers ear
H6Ø.331 Swimmer's ear, right ear H6Ø.332 Swimmer's ear, left ear H6Ø.333 Swimmer's ear, bilateral H6Ø.339 Swimmer's ear, unspecified ear
ICD-10-CM*
H65.ØØ Acute serous otitis media, unspecified ear H65.Ø1 Acute serous otitis media, right ear H65.Ø2 Acute serous otitis media, left ear H65.Ø3 Acute serous otitis media, bilateral H65.Ø4 Acute serous otitis media, recurrent, right ear H65.Ø5 Acute serous otitis media, recurrent, left ear H65.Ø6 Acute serous otitis media, recurrent, bilateral H65.Ø7 Acute serous otitis media, recurrent, unspecified ear
*For H65- and H66- codes: -Use additional code for any associated perforated tympanic membrane (H72-) -Use additional code to identify: exposure to environmental tobacco smoke (Z77.22) exposure to tobacco smoke in the perinatal period (P96.81) history of tobacco use (Z87.891) occupational exposure to environmental tobacco smoke (Z57.31) tobacco dependence (F17-) tobacco use (Z72.Ø)
Nose
ICD-9-CM ICD-10-CM
478.19 Nasal airway obstruction J34.89 Nasal airway obstruction
473.0 Chronic maxillary sinusitis J32.Ø Chronic maxillary sinusitis 473.1 Chronic frontal sinusitis J32.1 Chronic frontal sinusitis 473.2 Chronic ethmoidal sinusitis J32.2 Chronic ethmoidal sinusitis 473.3 Chronic sphenoidal sinusitis J32.3 Chronic sphenoidal sinusitis 473.8 Other chronic sinusitis (pansinusitis, chronic)
J32.4 Chronic pansinusitis J32.8 Other chronic sinusitis – sinusitis (chronic) involving more than one sinus but not pansinusitis
1:4 ratio!
ICD-10 CM Examples
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
16 CPT only © 2012 American Medical Association. All Rights Reserved
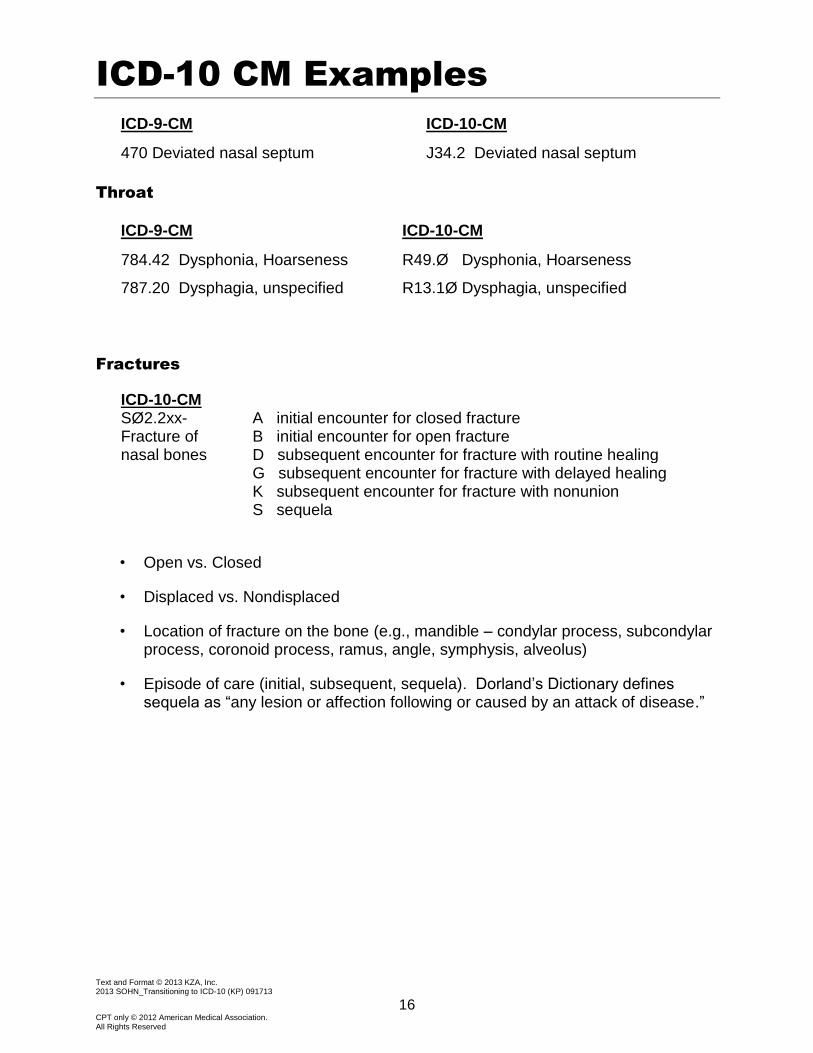
ICD-9-CM ICD-10-CM
470 Deviated nasal septum J34.2 Deviated nasal septum
Throat
ICD-9-CM ICD-10-CM
784.42 Dysphonia, Hoarseness R49.Ø Dysphonia, Hoarseness
787.20 Dysphagia, unspecified R13.1Ø Dysphagia, unspecified
Fractures
ICD-10-CM SØ2.2xx- Fracture of nasal bones
A initial encounter for closed fracture B initial encounter for open fracture D subsequent encounter for fracture with routine healing G subsequent encounter for fracture with delayed healing K subsequent encounter for fracture with nonunion S sequela
• Open vs. Closed
• Displaced vs. Nondisplaced
• Location of fracture on the bone (e.g., mandible – condylar process, subcondylar process, coronoid process, ramus, angle, symphysis, alveolus)
• Episode of care (initial, subsequent, sequela). Dorland’s Dictionary defines sequela as “any lesion or affection following or caused by an attack of disease.”

More on Fracture/Injuries
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
17 CPT only © 2012 American Medical Association. All Rights Reserved
Chapter 19 Chapter 20
Injury, Poisoning and Certain Other Consequences of External Cause
External Causes of Morbidity
SØØ-T88 VØ1-Y98
Injuries, fractures, burns and corrosions, adverse effects, poisoning, underdosing and toxic effects
Required: Vxx.xxxx (How it happened)
Example: VØØ.211A Fall from ice-skates
7th character required:
A Initial encounter
D Subsequent encounter
S Sequela
Example: SØ2.2xxA Fracture of nasal bones, initial encounter for close fracture
Required: Y92.xxx (Place it happened) Place of occurrence of the external cause
Example: Y92.331 Ice skating rink (indoor) (outdoor)
Fractures of skull and facial bones Required: Y93.xx (Activity performed) Activity codes
7th character required:
A Initial encounter for closed fracture
B Initial encounter for open fracture
D Subsequent encounter for fracture with routine healing
Example: Y93.21 Activity, ice skating
G Subsequent encounter for fracture with delayed healing
K Subsequent encounter for fracture with nonunion
S Sequela
Required: Y99.x (Who patient is) External cause status
External cause status
Y99.Ø Civilian activity done for income or pay
Y99.1 Military activity
Y99.2 Volunteer activity
Y99.8 Other external cause status
Y99.9 Unspecified external cause status

Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
18 CPT only © 2012 American Medical Association. All Rights Reserved
Clarification on the Use of External Cause and Unspecified Codes in ICD-10-CM
Approved by the four Cooperating Parties for ICD-10-CM/PCS and ICD-9-CM Coding, which
includes American Health Information Management Association, American Hospital Association,
Centers for Medicare & Medicaid Services, and National Center for Health Statistics
External Cause Codes
Just as with ICD-9-CM, there is no national requirement for mandatory ICD-10-CM external
cause code reporting. Unless a provider is subject to a state-based external cause code
reporting mandate or these codes are required by a particular payer, reporting of ICD-10-CM
codes in Chapter 20, External Causes of Morbidity, is not required. If a provider has not been
reporting ICD-9-CM external cause codes, the provider will not be required to report ICD-10-CM
codes in Chapter 20, unless a new state or payer-based requirement regarding the reporting of
these codes is instituted. Such a requirement would be independent of ICD-10-CM
implementation. In the absence of a mandatory reporting requirement, providers are
encouraged to voluntarily report external cause codes, as they provide valuable data for injury
research and evaluation of injury prevention strategies.
If a definitive diagnosis has not been established by the end of the encounter, it is appropriate to
report codes for sign(s) and/or symptom(s) in lieu of a definitive diagnosis. When sufficient
clinical information isn’t known or available about a particular health condition to assign a more
specific code, it is acceptable to report the appropriate “unspecified” code (e.g., a diagnosis of
pneumonia has been determined, but not the specific type). In fact, unspecified codes should be
reported when they are the codes that most accurately reflects what is known about the
patient’s condition at the time of that particular encounter. It would be inappropriate to select a
specific code that is not supported by the medical record documentation or conduct medically
unnecessary diagnostic testing in order to determine a more specific code.
Source: Cooperating Parties for ICD-10-CM/PCS and ICD-9-CM Coding, May 2013.
http://library.ahima.org/xpedio/groups/public/documents/government/bok1_050189.hcsp?dDocName=bok1_050189
Sign/Symptom/Unspecified Codes
In both ICD-9-CM and ICD-10-CM, sign/symptom and “unspecified” codes have acceptable,
even necessary, uses. While specific diagnosis codes should be reported when they are
supported by the available medical record documentation and clinical knowledge of the patient’s
health condition, there are instances when signs/symptoms or unspecified codes are the best
choices for accurately reflecting the healthcare encounter. Each healthcare encounter should be
coded to the level of certainty known for that encounter.

Notes
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
19 CPT only © 2012 American Medical Association. All Rights Reserved

Course Evaluation
Text and Format © 2013 KZA, Inc. 2013 SOHN_Transitioning to ICD-10 (KP) 091713
20 CPT only © 2012 American Medical Association. All Rights Reserved
Please submit to the course instructor at the conclusion of the program. We appreciate your feedback!
Strongly Agree
Agree Neutral Disagree Strongly Disagree
Overall, the program met my expectations.
The speaker was knowledgeable and presented in a clear, concise manner.
The workbook will be a useful reference.
This program answered my questions.
I would attend another course by this speaker.
I would recommend this course to a colleague.
General comments about the course:
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
I am an:
MD NPP Administrator Office Manager Staff
DO RN CPC PA Billing Manager Other
Please sign me up for KZAlert e-mails for useful, practical, updated information and tips on practice management and coding. ___________________________________________________________________________________
(Print your e-mail address clearly.)
Please send me more information about the following KZA services:
Practice Management Consultation Onsite Workshops
Accounts Receivable Help Contract Review
Coding and Documentation Review Strategic Planning
Name ______________________________________________________________________
Practice Name ______________________________________________________________________
Address ______________________________________________________________________
______________________________________________________________________
Phone ______________________________________________________________________
Website ______________________________________________________________________
KP/SOHN_ICD-10 /092913