traumatic brain injury update naccsgbi asm, 2017 · traumatic brain injury update naccsgbi asm,...
TRANSCRIPT

Traumatic Brain Injury UpdateNACCSGBI ASM, 2017
Matt Wiles
Sheffield Teaching Hospital NHS Foundation Trusthttp://sthjournalclub.wordpress.com @STHJournalClub
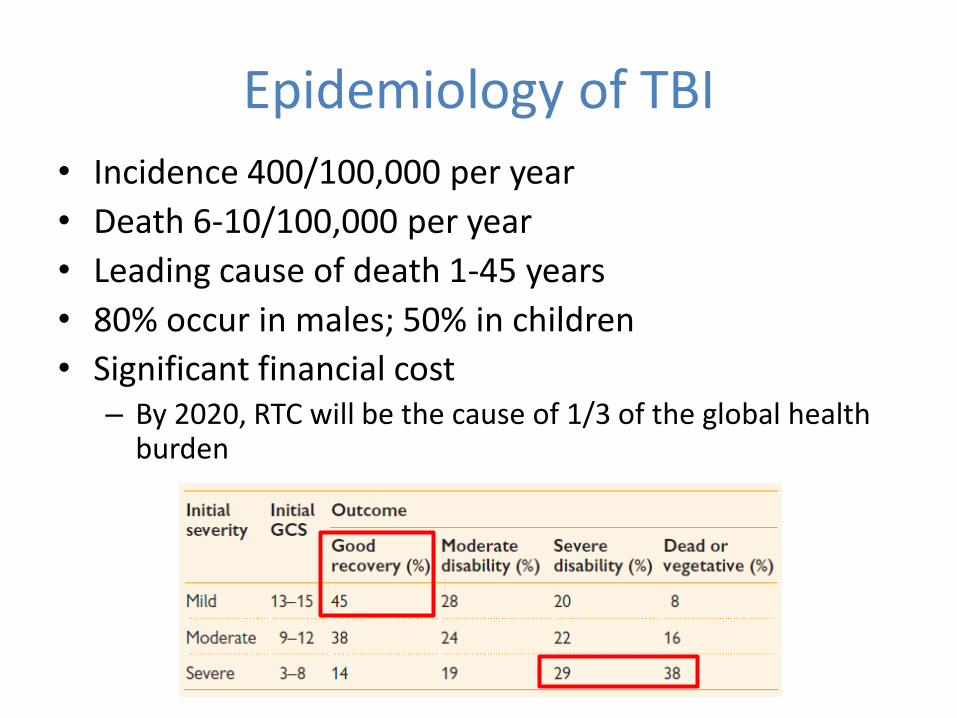
Epidemiology of TBI
• Incidence 400/100,000 per year
• Death 6-10/100,000 per year
• Leading cause of death 1-45 years
• 80% occur in males; 50% in children
• Significant financial cost– By 2020, RTC will be the cause of 1/3 of the global health
burden
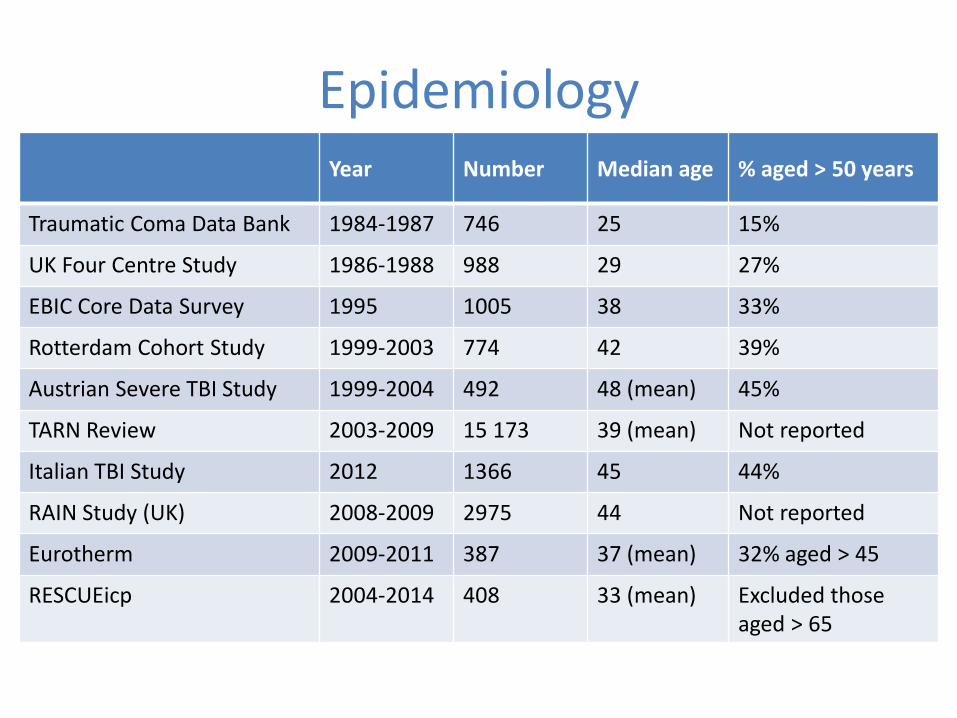
EpidemiologyYear Number Median age % aged > 50 years
Traumatic Coma Data Bank 1984-1987 746 25 15%
UK Four Centre Study 1986-1988 988 29 27%
EBIC Core Data Survey 1995 1005 38 33%
Rotterdam Cohort Study 1999-2003 774 42 39%
Austrian Severe TBI Study 1999-2004 492 48 (mean) 45%
TARN Review 2003-2009 15 173 39 (mean) Not reported
Italian TBI Study 2012 1366 45 44%
RAIN Study (UK) 2008-2009 2975 44 Not reported
Eurotherm 2009-2011 387 37 (mean) 32% aged > 45
RESCUEicp 2004-2014 408 33 (mean) Excluded those aged > 65
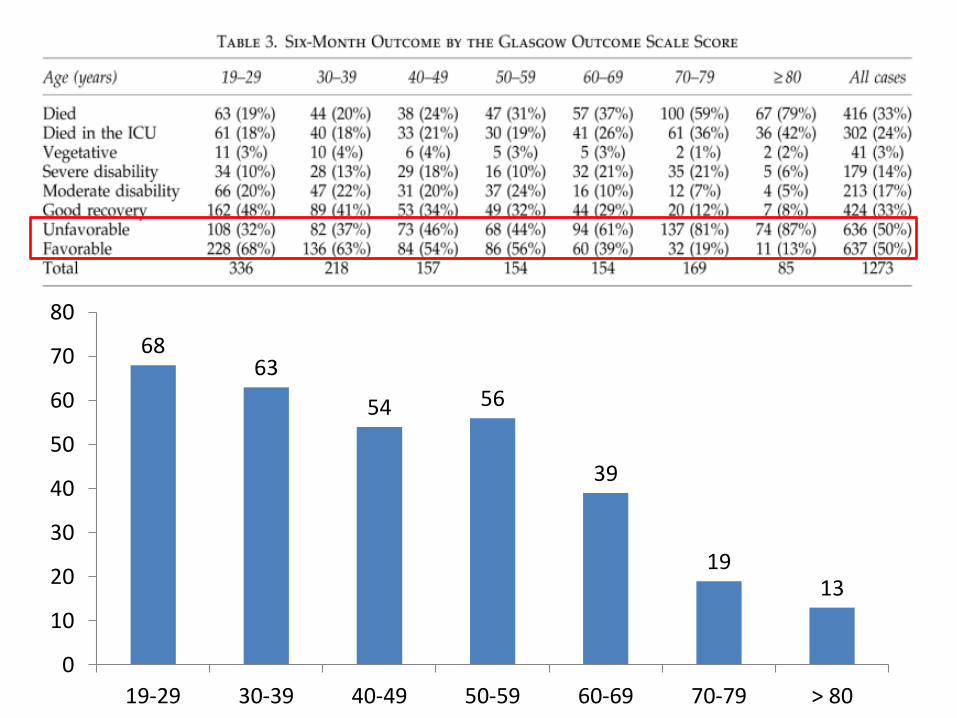
6863
54 56
39
1913
0
10
20
30
40
50
60
70
80
19-29 30-39 40-49 50-59 60-69 70-79 > 80
Series 1
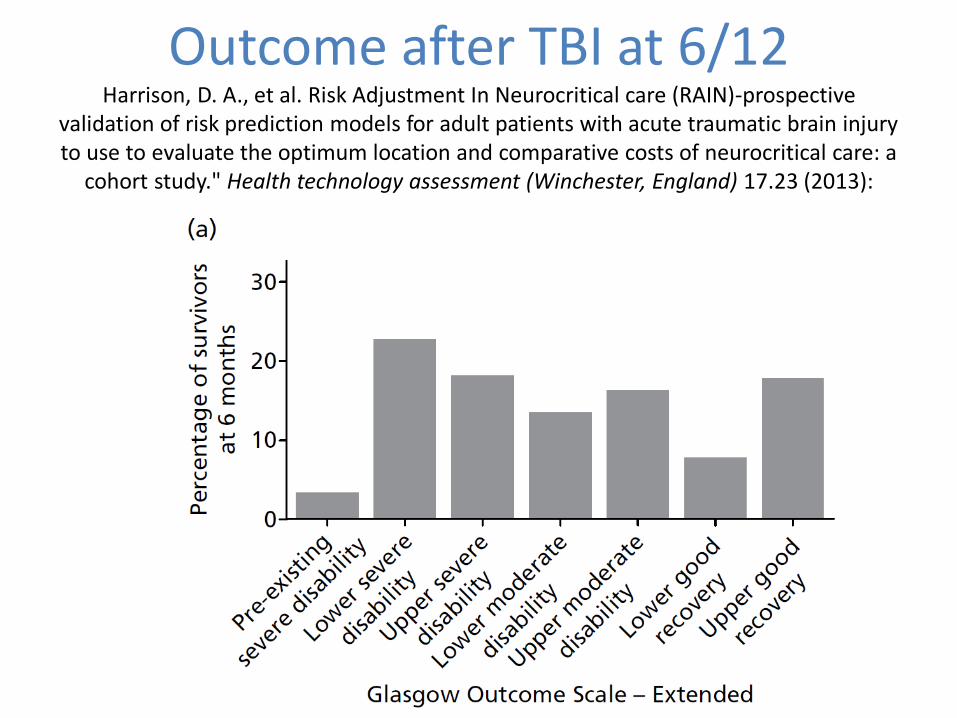
Outcome after TBI at 6/12Harrison, D. A., et al. Risk Adjustment In Neurocritical care (RAIN)-prospective
validation of risk prediction models for adult patients with acute traumatic brain injury to use to evaluate the optimum location and comparative costs of neurocritical care: a
cohort study." Health technology assessment (Winchester, England) 17.23 (2013):

Tracheal Intubation• The stress response to laryngoscopy must be attenuated

Tracheal Intubation• The stress response to laryngoscopy must be attenuated
• Alfentanil 10 µg kg-1 is as effective as remifentanil

Tracheal Intubation• The stress response to laryngoscopy must be attenuated
• Alfentanil 10 µg kg-1 is as effective as remifentanil
• Ketamine is my first choice in trauma
– Propofol and thiopentone are alternatives
– Etomidate is contraindicated in head injury
• Most patients will require a RSI: suxamethonium and rocuronium are both safe in brain injury



Ketamine
• Ketamine increases ICP/CBF in spontaneously breathing volunteers (III)
• No effect on ICP with controlled ventilation and sedation (III)
• Greater CPP maintained with ketamine and lower vasopressor requirements (II)
• No effect on cerebral autoregulation (III)

Breathing
• Hypoxia associated with worse outcome
• Marked hypo- and hypercapnia similarly bad
– Must calibrate PaCO2 with ETCO2

Breathing
• Hypoxia associated with worse outcome
• Marked hypo- and hypercapnia similarly bad
– Must calibrate PaCO2 with ETCO2

Breathing
• Hypoxia associated with worse outcome
• Marked hypo- and hypercapnia simliarly bad
• What about PEEP?

CirculationChesnut et al. J Trauma 1993
• A single episode of hypotension doubles mortality

• A single episode of hypotension doubles mortality
• Head injury alone rarely causes hypotension
• Treatment of cardiovascular instability takes precedence over direct head injury intervention
• No evidence for any one vasopressor
• Trials with permissive hypotension excluded those with TBI
CirculationChesnut et al. J Trauma 1993

Permissive HypotensionMaas AI et al. Advancing care for traumatic brain injury: findings from the IMPACT studies
and perspectives on future research. Lancet Neurol 2013; 12: 1200-10
• Hypotension increases mortality & poor outcomes
Permissive HypotensionWiles MD. Blood pressure management in trauma: from feast to famine? Anaesthesia
2013; 68: 445–452
• “Trials” of permissive hypotension excluded patients with TBI
• Evidence of reduction in haemorrhage with permissive hypotension is lacking in clinical studies
• Much (all) is extrapolated from animal models

Bickell et al Turner et al Dutton et al Schreiber et al Carrick et alNumber 598 1309 110 191 168Years 1989-1992 1996-1997 1996-1999 2012-2013 2007-2013Age; years 31 (mean) 80% aged ≤ 64 31 (mean) 42 (mean) 31 (median)Sex; male 89% 64% 80% 76% 90%Penetrating trauma 100% 1.8% 51% 34% 100%Inclusion criteria Gunshot/stab wounds
with SBP < 90mmHgSignificant trauma injury as determined by admission destination, length of stay and death
Evidence of haemorrhage after trauma and SBP < 90 mmHg at least once in the first 60 min
Traumatic injury with an out-of-hospital SBP ≤ of 90 mm Hg.
Age ≤ 45; penetrating trauma with SBP ≤ 90 mmHg requiring laparotomy/thoracotomy.
Exclusion criteria Revised Trauma Score 0; fatal gunshot wound to head; minor injuries not requiring surgery
Burns; hangings; pregnancy; drowning; isolated traumatic injury
CNS injury; age > 55; coronary artery disease; diabetes mellitus
Severe head injury; GCS ≤ 8; burns; hangings; pregnancy; drowning; 250 ml fluid administered prior to randomisation; ground level falls.
Known or suspected head injury; pregnancy.
Brain injury included Unclear Yes; 24.4% some degree of head injury
No No No
Intervention arm Delayed resuscitation:minimal i.v. fluid until arrival in theatre (mean 375 ml)
Delayed resuscitation:i.v. fluids withheld for the first hour of prehospital care.
Target SBP 70 mmHg Controlled resuscitation: maintain SBP 70 mmHg/radial pulse with 250 ml fluid bolus as necessary.
Intra-operative minimal MAP 50 mmHg
Control arm Immediate resuscitation: if SBP < 100 mmHg then given i.v. crystalloid (mean 2478 ml)
Immediate resuscitation: i.v. fluids administered following primary patientassessment.
Target SBP > 100 mmHg with fluids/PRC.
Standard resuscitation: 2000 ml fluid bolus and further fluids to maintain SBP 110 mmHg.
Intra-operative minimal MAP 65 mmHg
Primary outcome Survival to hospital discharge. 70% in delayed resuscitation group vs. 64% in immediate resuscitation group (p=0.04)
Composite of mortality and morbidity.Mortality 9.8%% in delayed resuscitation group vs.10.4% in immediate resuscitation group (Adjusted OR 0.93 (0.58 to 1.49)).
Mortality.93 % survival in both groups.
Feasibility study. Primary safety end-point 24 h mortality.Mortality at 24 hours was 5.2% vs. 14.7% in controlled and standard groups respectively (adjusted OR 0.3995% CI 0.12-1.25).
30-day mortality
Coagulation measured
Coagulopathy (not defined) similar incidence in both groups.
Coagulopathy (not defined) similar incidence in both groups.
No. Yes; PT, APTT and platelet counts similar in both groups.
Coagulopathy (not defined) similar incidence in both groups.
Coagulation factors used
FFP (≈ 300ml) given with PRC (≈ 1800 ml).
No Not stated Yes. In the first 2 h total blood products (including PRC) 400 ml vs. 1050 ml in controlled and standard groups respectively.
Yes. Similar between groups: median 1125-1500 ml PRC, with PRC:FFP ratios of 2.2-2.3.
Weaknesses Randomisation by day of week; immortality bias.
Poor compliance with protocol. Only 30.9% of patients in the immediate resuscitation groups received i.v. fluids.Randomisation by treating paramedic rather than patient.
Target not achieved in hypotensive group (mean SBP 100).
Not powered for mortality outcomes. Only 35% of patients had ISS > 15.
Early termination or study due to because of clinical equipoise and futility (168 of planned 271 patients recruited).Little difference between groups in terms of MAP (intra-operative MAP was66 mmHg in the intervention group and 69 mmHg in the control group_
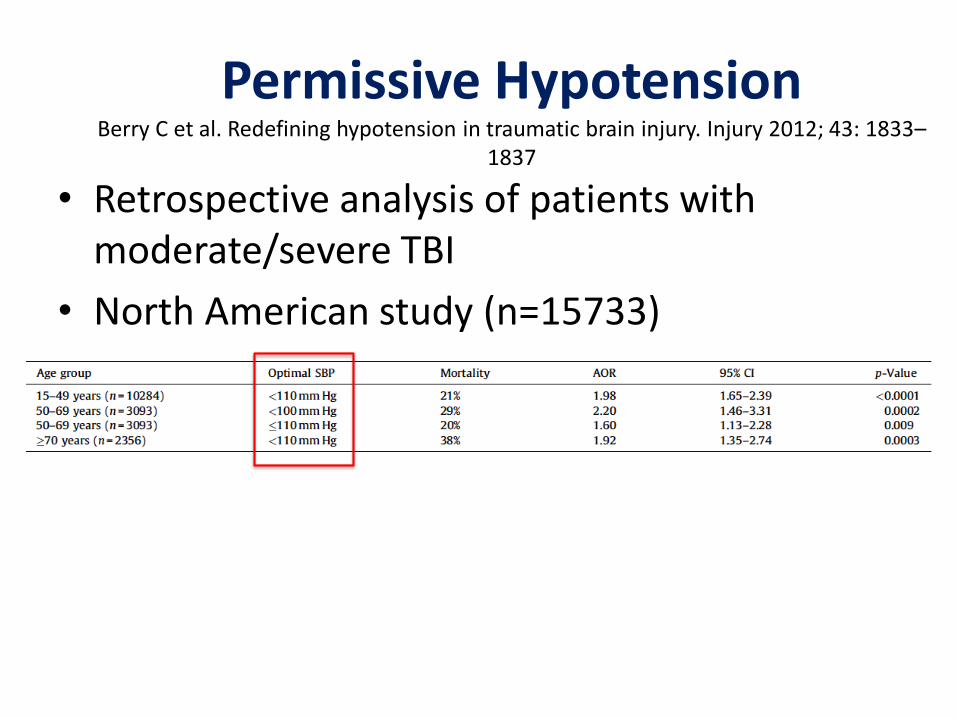
Permissive HypotensionBerry C et al. Redefining hypotension in traumatic brain injury. Injury 2012; 43: 1833–
1837
• Retrospective analysis of patients with moderate/severe TBI
• North American study (n=15733)

Permissive HypotensionHassler RM et al. Systolic blood pressure below 110 mmHg is associated with
increased mortality in penetrating major trauma patients: Multicentre cohort study. Resuscitation 2012; 83: 476-81
• 3444 patients with penetrating trauma (TARN)
1
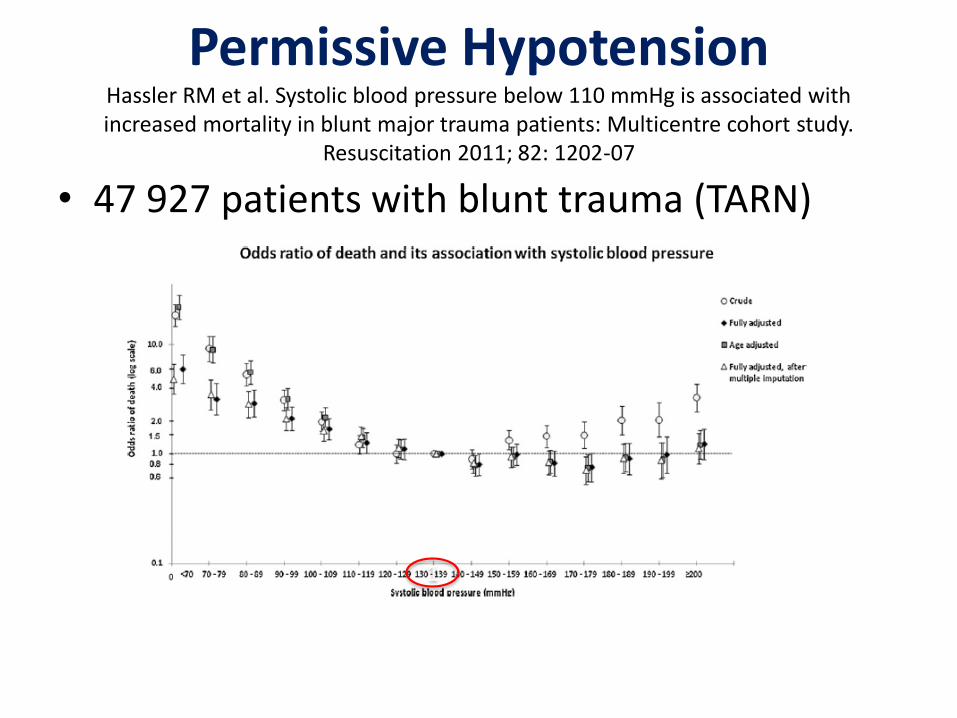
Permissive HypotensionHassler RM et al. Systolic blood pressure below 110 mmHg is associated with increased mortality in blunt major trauma patients: Multicentre cohort study.
Resuscitation 2011; 82: 1202-07
• 47 927 patients with blunt trauma (TARN)
1


Fluid TherapyCooper DJ et al. Albumin Resuscitation for Traumatic Brain Injury: Is Intracranial
Hypertension the Cause of Increased Mortality? Journal of Neurotrauma 2013; 30: 512-8.
• Post hoc analyses of SAFE study (n=321)

Glucose ControlFinfer et al. Intensive versus Conventional Glucose Control in Critically Ill Patients with Traumatic Brain Injury: Long term follow up of a subgroup of patients from the NICE
SUGAR Study Intensive Care Medicine 2015; 41: 1037-47
• Planned sub-group analyses of NICE-SUGAR study (n=391 with TBI)
– 183 “Conventional” Glucose < 10 mmol L-1
– 201 “Intensive” Glucose 4.5 to 6 mmol L-1
• No difference in mortality or eGOS at 2 years
• Significantly more moderate/severe hypoglycaemic episodes in intensive group

Parameter BTF EBIC AAGBI
Respiratory AVOIDPaCO2 <3.3 kPa
TARGETSpO2 >95%PaO2 >10 kPaPaCO2 4.0-4.5 kPa
TARGET
PaO2 >13 kPaPaCO2 4.5-5.0 kPa
Cardiovascular TARGETSBP > 100 mmHg if aged 50-69 or SBP > 110 mmHg if aged < 49 or > 70.
TARGETMAP >90 mmHgSBP >120 mmHg
TARGETMAP >80 mmHg
Neurological Treat if ICP >22CPP 60-70
ICP <20-25CPP 60-70
ICP <20-25CPP 60-70

OsmotherapyWakai A et al. Mannitol for acute traumatic brain injury. Cochrane Database
Syst Rev. 2013; 8: CD001049.
• Mannitol - no effect on mortality
• Both hypertonic saline (HTS) and mannitol reduce ICP in the short term to similar degrees
• Both associated with morbidity if given in excess
• HTS may have a role in low-volume resuscitation in trauma
– Highly irritant; best delivered centrally
– Potential for error is huge

Osmotherapy: MannitolWakai A et al. Mannitol for acute traumatic brain injury. Cochrane Database Syst Rev.
2013; 8: CD001049.
• Only able to identify 4 trials (n=197)
• Insufficient reliable evidence to make recommendations for its use in TBI
• Further high-quality RCTs needed despite the widespread use of mannitol
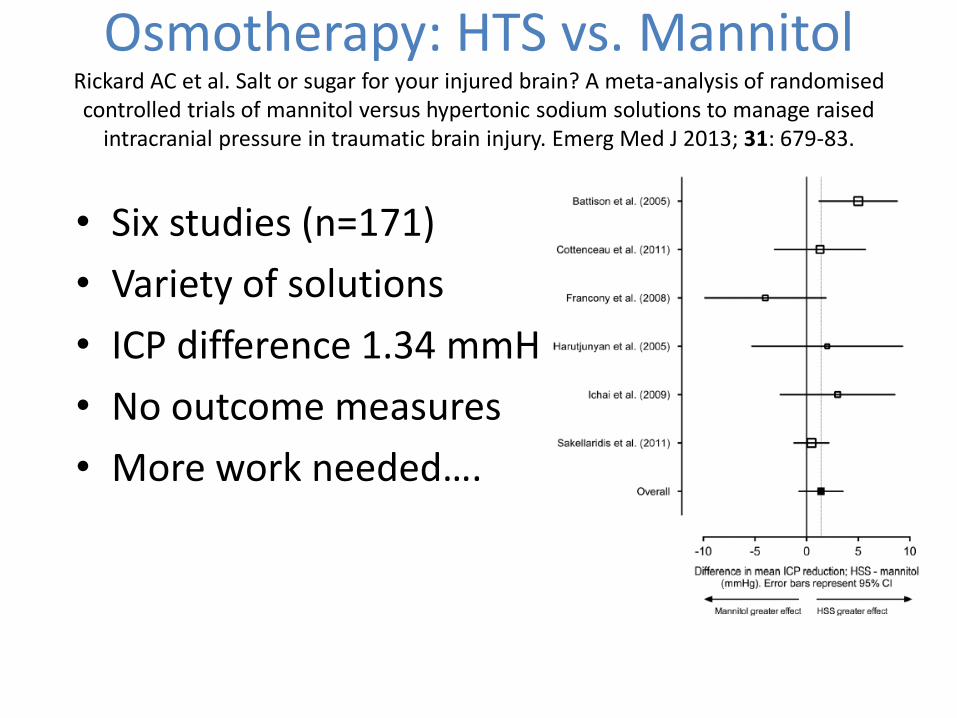
Osmotherapy: HTS vs. MannitolRickard AC et al. Salt or sugar for your injured brain? A meta-analysis of randomisedcontrolled trials of mannitol versus hypertonic sodium solutions to manage raised
intracranial pressure in traumatic brain injury. Emerg Med J 2013; 31: 679-83.
• Six studies (n=171)
• Variety of solutions
• ICP difference 1.34 mmHg
• No outcome measures
• More work needed….

Intracranial Pressure MonitoringChesnut RM et al. A trial of intracranial-pressure monitoring in traumatic brain injury.
New England Journal of Medicine 2012; 367: 2471-81.
• 6/12 Mortality 39% (ICP care) vs. 41% (Clinical) [P=0.60]
– < 25% in hospital within 60 min & only 45% came by ambulance
– ICP target similar to DECRA (ICP >20mmHg for 15 min)
– ICP bolts sited on the basis of GCS alone
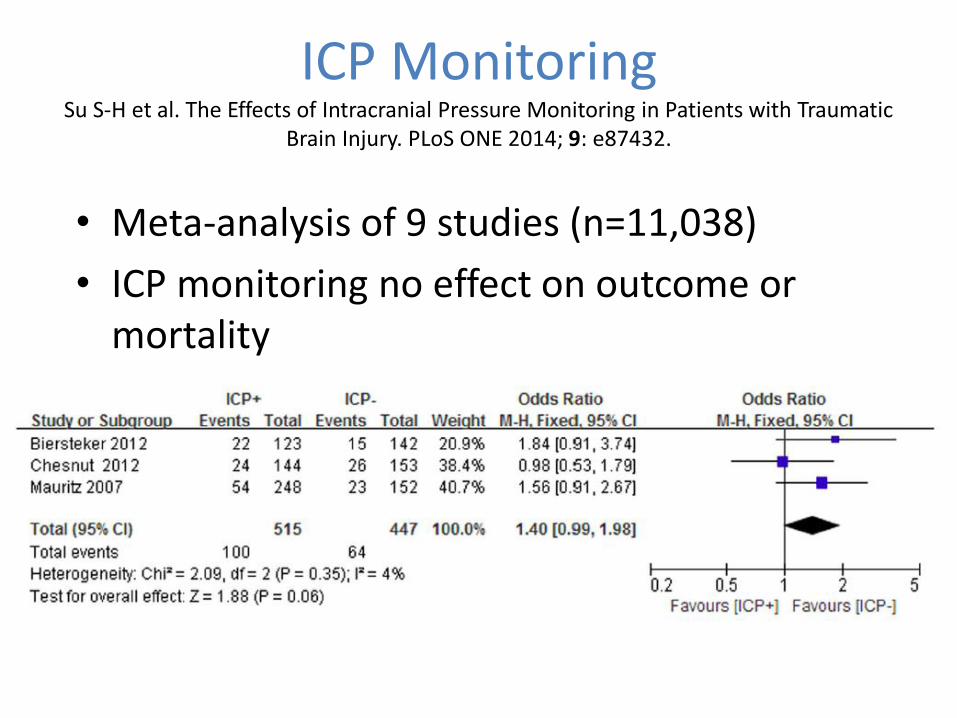
ICP MonitoringSu S-H et al. The Effects of Intracranial Pressure Monitoring in Patients with Traumatic
Brain Injury. PLoS ONE 2014; 9: e87432.
• Meta-analysis of 9 studies (n=11,038)
• ICP monitoring no effect on outcome or mortality
• Significant heterogeneity in papers
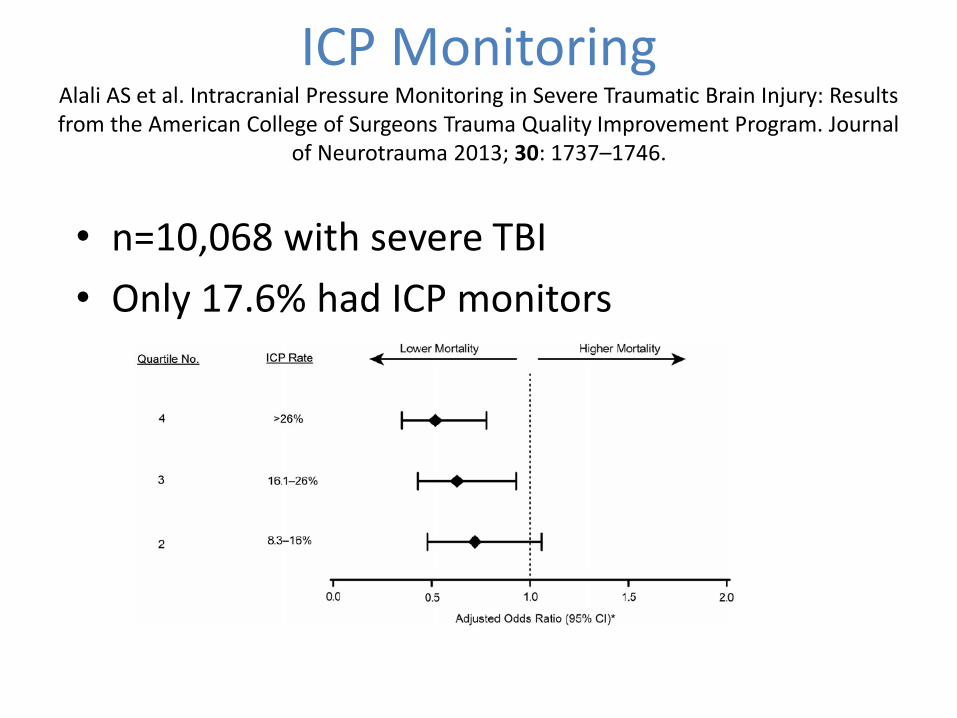
ICP MonitoringAlali AS et al. Intracranial Pressure Monitoring in Severe Traumatic Brain Injury: Results from the American College of Surgeons Trauma Quality Improvement Program. Journal
of Neurotrauma 2013; 30: 1737–1746.
• n=10,068 with severe TBI
• Only 17.6% had ICP monitors

ICP MonitoringGerber LM et al. Marked reduction in mortality in patients with severe traumatic brain
injury. J Neurosurg 2013; 119: 1583–1590.
• Retrospective analysis of severe TBI (2001-2009)
• Primarily Level 1

ICP MonitoringStocchetti N et al. Clinical applications of intracranial pressure monitoring in traumatic
brain injury. Acta Neurochir 2014; 156: 1615–1622
• No ICP bolt:
– Normal CT brain
• ICP bolt:
– Cerebral contusions and remained sedated
– After decompressive craniectomy
– After evacuation of supratentorial haematoma and at risk of raised ICP
• GCS ≤ 5, midline shift > 5mm, abnormal pupils etc..
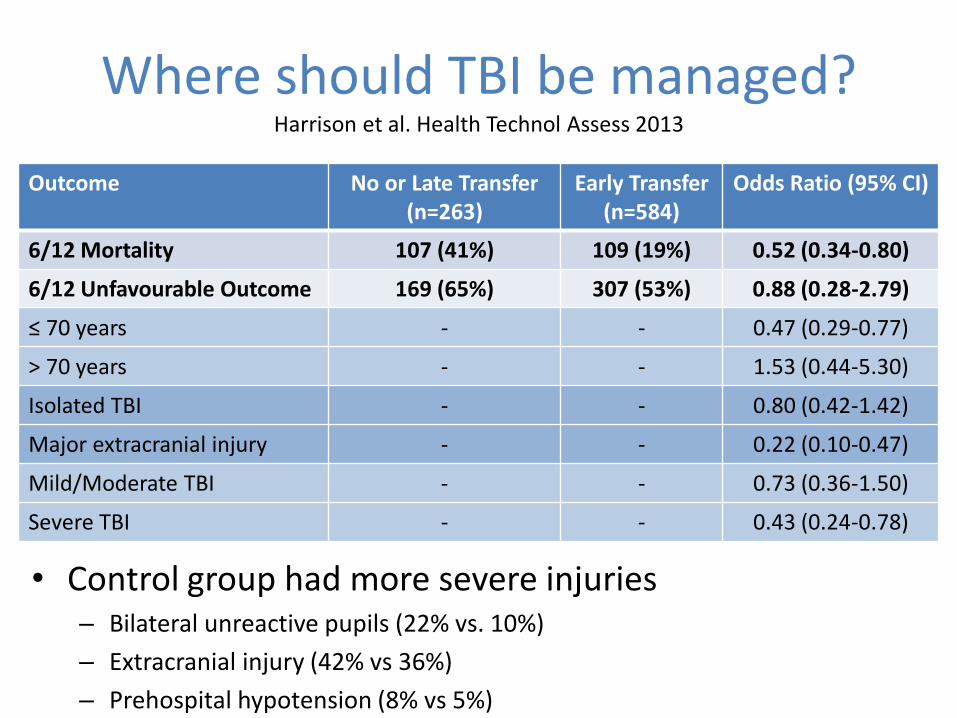
Where should TBI be managed?Harrison et al. Health Technol Assess 2013
Outcome No or Late Transfer(n=263)
Early Transfer(n=584)
Odds Ratio (95% CI)
6/12 Mortality 107 (41%) 109 (19%) 0.52 (0.34-0.80)
6/12 Unfavourable Outcome 169 (65%) 307 (53%) 0.88 (0.28-2.79)
≤ 70 years - - 0.47 (0.29-0.77)
> 70 years - - 1.53 (0.44-5.30)
Isolated TBI - - 0.80 (0.42-1.42)
Major extracranial injury - - 0.22 (0.10-0.47)
Mild/Moderate TBI - - 0.73 (0.36-1.50)
Severe TBI - - 0.43 (0.24-0.78)
• Control group had more severe injuries– Bilateral unreactive pupils (22% vs. 10%)
– Extracranial injury (42% vs 36%)
– Prehospital hypotension (8% vs 5%)

“The lack of improvement in head injured patients is typified by the apparent overall lack of progress in head injury care, which is suggested by the failure to identify a single therapy to improve outcome despite over 250 randomised controlled trials.
However, several studies have shown that the institution of packages of specialist neurosurgical or neurocritical care is associated with improved outcomes.”

Outcome PredictionRoe C et al. Severe traumatic brain injury in Norway: impact of age on outcome. J
Rehabil Med 2103; 45: 734-40.
16-64 years(n=156)
≥ 65 years(n=22)
90-day mortality 24% 67%
Returned to own home @ 90 days 53% 68%

Outcome PredictionStevens RD, Sutter R. Prognosis in severe brain injury. Crit Care Med 2013; 41: 1104-23.

Outcome PredictionMercier E et al. Predictive value of S-100β protein for prognosis in patients with moderate
and severe traumatic brain injury: systematic review and meta-analysis. BMJ 2013; 346: f1757
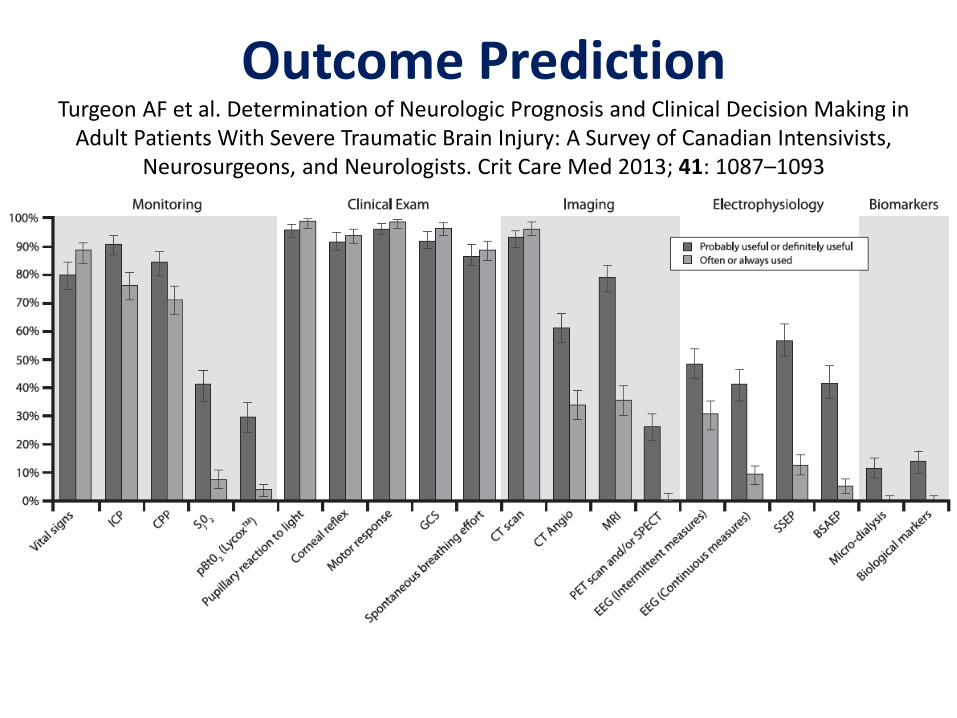
Outcome PredictionTurgeon AF et al. Determination of Neurologic Prognosis and Clinical Decision Making in
Adult Patients With Severe Traumatic Brain Injury: A Survey of Canadian Intensivists, Neurosurgeons, and Neurologists. Crit Care Med 2013; 41: 1087–1093
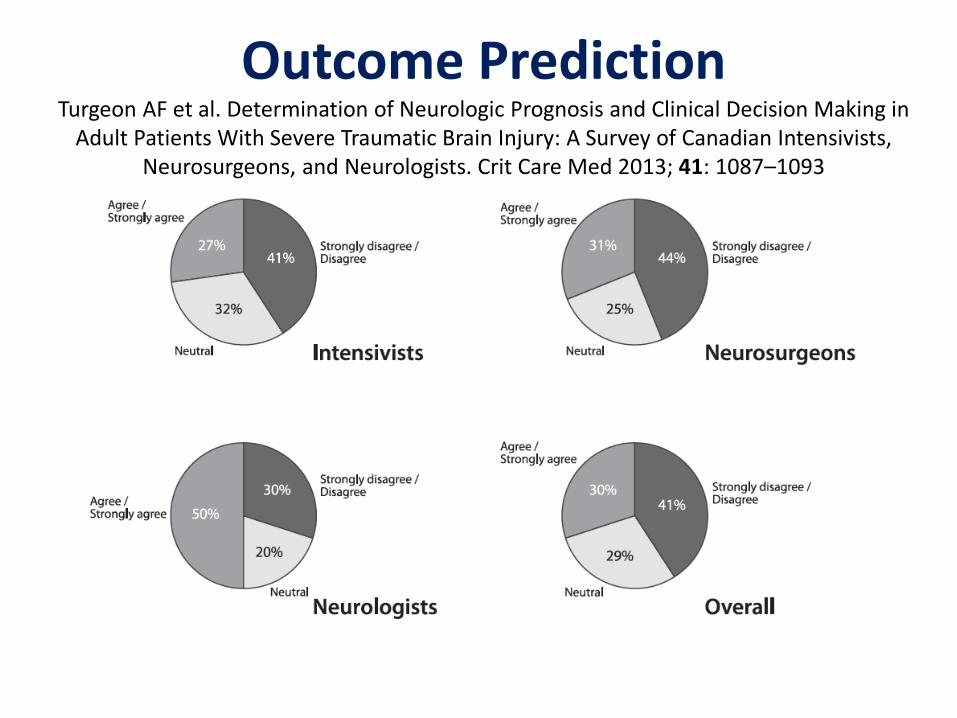
Outcome PredictionTurgeon AF et al. Determination of Neurologic Prognosis and Clinical Decision Making in
Adult Patients With Severe Traumatic Brain Injury: A Survey of Canadian Intensivists, Neurosurgeons, and Neurologists. Crit Care Med 2013; 41: 1087–1093

Summary (TBI)
• Hypoxia & hypotension are bad for the brain
– Permissive hypotension has no place in TBI
– MAP > 80 mmHg and/or SBP >110 mmHg
• Anything we can do to avoid these are good (including ketamine, PEEP & calibration ETCO2)
• ICP monitors are of no value in Bolivia or Ecuador
• TBI should be managed in a neurosurgical centre
– If GCS 3-8 and aged < 70
References1. Finfer SR, Cohen J. Severe traumatic brain injury. Resuscitation 2001; 48: 77–90.2. Foulkes AM, Eisenberg MH, Jane AJ. The Traumatic Coma Data Bank; design, methods and baseline
characteristics. J Neurosurg1991; 75: S1–15.3. Murray LS, Teasdale GM, Murray GD, Miller DJ, Pickard JD,Shaw MD. Head injuries in four British
neurosurgical centres. Br J Neurosurg 1999; 13: 564–69.4. Murray GD, Teasdale GM, Braakman R et al. The European Brain Consortium survey of head injuries. Acta
Neurochir (Wien) 1999; 141: 223–36.5. Stocchetti N, Paternò R, Citerio G, Beretta L, Colombo A. Traumatic Brain Injury in an Aging Population.
Journal of Neurotrauma 2012; 29: 1119-1125.6. Thornhill S, Teasdale GM, Murray GD, McEwen J, Roy CW, Penny KI. Disability in young people and adults
one year after head injury: prospective cohort study. Br Med J 2000; 320: 1631–5.7. Chesnut RM, Marshall LF, Klauber MR et al. The role of secondary brain injury in determining outcome
from severe head injury. J Trauma 1993; 34: 216–22.8. IK Moppett. Traumatic brain injury: assessment, resuscitation and early management. Br J Anaesth 2007;
99: 18-31.9. Brain Trauma Foundation. Guidelines for Prehospital Management of Traumatic Brain Injury. New York:
Brain Trauma Foundation, 2000.10. Brain Trauma Foundation, American Association of Neurological Surgeons (AANS), Congress of
Neurological Surgeons (CNS), AANS/CNS Joint Section on Neurotrauma and Critical Care. Guidelines for the management of severe traumatic brain injury, 3rd edition. J Neurotrauma 2007; 24: S1–106.
11. Maas AI, Dearden M, Teasdale GM et al. EBIC-guidelines for management of severe head injury in adults. European Brain Injury Consortium. Acta Neurochir (Wien) 1997; 139: 286–94.
12. Schierhout G, Roberts I. Anti-epileptic drugs for preventing seizures following acute traumatic brain injury. Cochrane Database Syst Rev 2001; 4: doi:10.1002/14651858. CD000173
13. Tennant A. The epidemiology of head injury. In: Chamberlain MA, Neumann V, Tennant A, eds. Traumatic Brain Injury Rehabilitation: Services, Treatments and Outcomes. London: Chapman Hall, 1996.
14. Wakai A, Roberts I, Schierhout G. Mannitol for acute traumatic brain injury. Cochrane Database Syst Rev2007; 1: doi:10.1002/14651858. CD001049.pub4

References15. Schwedler M, Miletich DJ, Albrecht RF. Cerebral Blood Flow and Metabolism Following Ketamine
Administration. Can Anaesth Soc J 1982; 29: 222-6.16. Himmelseher S, Durieux ME. Revising a Dogma: Ketamine for Patients with Neurological Injury? Anesth
Analg 2005;101:524–34.17. Pfenninger E, Griinert A, Bowdler I, Kilian J. The Effect of Ketamine on Intracranial Pressure During
Haemorrhagic Shock Under the Conditions of Both Spontaneous Breathing and Controlled Ventilation. Acta Neurochirurgica 1985; 78: 113-8.
18. Huynh T, Messer M, Sing RF, Miles W, Jacobs DG, Thomason MH. Positive End-Expiratory Pressure Alters Intracranial and Cerebral Perfusion Pressure in Severe Traumatic Brain Injury. J Trauma 2002; 53: 488-93.
19. Hasler RM et al. Systolic blood pressure below 110mmHg is associated with increased mortality in penetrating major trauma patients: Multicentre cohort study. Resuscitation 2011; 83: 476-81.
20. Hasler, RM et al. (2011). Systolic blood pressure below 110mmHg is associated with increased mortality in blunt major trauma patients: Multicentre cohort study. Resuscitation 2011; 82: 1202-1207.
21. Ryken TC, Hurlbert RJ, Hadley MN et al. The Acute Cardiopulmonary Management of Patients With Cervical Spinal Cord Injuries. Neurosurgery 2013; 72: 84-92.
22. Fehlings MG, Vaccaro A, Wilson JR et al. Early versus delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PloS one 2012 7: e32037.
23. Panczykowski DM, Tomycz ND & Okonkwo DO. Comparative effectiveness of using computed tomography alone to exclude cervical spine injuries in obtunded or intubated patients: meta-analysis of 14,327 patients with blunt trauma: A review. Journal of neurosurgery 2011; 115: 541-549.
24. Bracken MB, Shepard MJ, Collins WF et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury: results of the Second National Acute Spinal Cord Injury Study. New England Journal of Medicine 1990; 322: 1405-1411.
25. Sundstrøm T, Asbjørnsen H, Habiba S, Sunde GA & Wester K. Prehospital Use of Cervical Collars in Trauma Patients: A Critical Review. Journal of neurotrauma 2014; 31: 531-40.
26. Rosso A, Brazinova A, Janciak I et al. Severe traumatic brain injury in Austria II: epidemiology of hospital admissions. Wiener Klinische Wochenschrift 2007; 119: 29-34.

References27. Chesnut, RM, Temkin N, Carney N et al. A trial of intracranial-pressure monitoring in traumatic brain injury.
New England Journal of Medicine 2012; 367: 2471-2481.28. Harrison D, Prabhu G, Grieve R et al. Risk Adjustment In Neurocritical care (RAIN)-prospective validation of
risk prediction models for adult patients with acute traumatic brain injury to use to evaluate the optimum location and comparative costs of neurocritical care: a cohort study. Health Technol Assess 2013; 17: 1-350.
29. Burney RG & Winn R. Increased cerebrospinal fluid pressure during laryngoscopy and intubation for induction of anesthesia. Anesthesia & Analgesia 1975; 54: 687-690.
30. Warner DS, Hindman BJ, Todd MM et al. Intracranial pressure and hemodynamic effects of remifentanilversus alfentanil in patients undergoing supratentorial craniotomy. Anesthesia & Analgesia 1996; 83: 348-353.
31. Prause G. Hetz H, Lauda P et al. A comparison of the end-tidal-CO2 documented by capnometry and the arterial pCO2 in emergency patients. Resuscitation 1997; 35: 145-148.
32. Huynh T, Messer M, Sing RF et al. Positive end-expiratory pressure alters intracranial and cerebral perfusion pressure in severe traumatic brain injury. Journal of Trauma and Acute Care Surgery 2002; 53:488-493.
33. Wiles MD. Blood pressure management in trauma: from feast to famine? Anaesthesia 2013; 68: 445-449.34. Berry C, Ley EJ, Bukur M et al. Redefining hypotension in traumatic brain injury. Injury 2012; 43: 1833–7.35. Fattah S, Ekås GR, Hyldmo PK & Wisborg T. The lateral trauma position: What do we know about it and
how do we use it? A cross-sectional survey of all Norwegian emergency medical services. Scandinavian journal of trauma, resuscitation and emergency medicine 2011; 19: 1-5.
36. Andrews PJD, Sinclair HL, Rodriguez A, et al. Hypothermia for Intracranial Hypertension after Traumatic Brain Injury. New England Journal of Medicine 2015; 373: 2403-12.
37. Cooper DJ, Myburgh J, Heritier S, et al. Albumin resuscitation for traumatic brain injury: is intracranial hypertension the cause of increased mortality? J Neurotrauma 2013; 30: 512-8.
38. Hutchinson PJ, Kolias AG, Timofeev IS, et al. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension. New England Journal of Medicine 2016; 0: null.
References39. Robertson CS, Hannay HJ, Yamal JM, et al. Effect of erythropoietin and transfusion threshold on
neurological recovery after traumatic brain injury: a randomized clinical trial. Jama 2014; 312: 36-47.40. Skolnick BE, Maas AI, Narayan RK, et al. A Clinical Trial of Progesterone for Severe Traumatic Brain Injury.
New England Journal of Medicine 2014; 371: 2467-76.41. Wright DW, Yeatts SD, Silbergleit R, et al. Very Early Administration of Progesterone for Acute Traumatic
Brain Injury. New England Journal of Medicine 2014; 371: 2457-66.