treatment
DESCRIPTION
TREATMENT. General Principles of Treatment. Obtain a complete historical record of prior therapies, including all over-the-counter products Most common and important cause of failure of treatment is lack of compliance - PowerPoint PPT PresentationTRANSCRIPT

TREATMENT

General Principles of Treatment
• Obtain a complete historical record of prior therapies, including all over-the-counter products
• Most common and important cause of failure of treatment is lack of compliance
• Topical application to the entire affected area rather than to specific lesions should be emphasized
• Oral and topical medications should be used daily as the treatment is preventive in nature
General Principles of Treatment
• Avoidance of specific foods is not necessary
• Scrubbing of the face will not only increase irritation but may worsen acne due to friction
• Non-comedogenic cosmetics are recommended and pressed powders and oil-based products should be avoided
• Preventive• Long term usage is the rule
A. Topical RetinoidsB. Benzoyl PeroxideC. Topical AntibacterialsD. Sulfur, Sodium Sulfacetamide, Resorcin, and
Salicylic AcidE. Azeleic Acid

Topical Retinoids
• Effective in promoting normal desquamation of the follicular epithelium
• Have marked anti-inflammatory effect
• Help in penetration of other active agents
• Preferred agents in maintenance therapy
• Use of moisturizers may lessen their irritancy
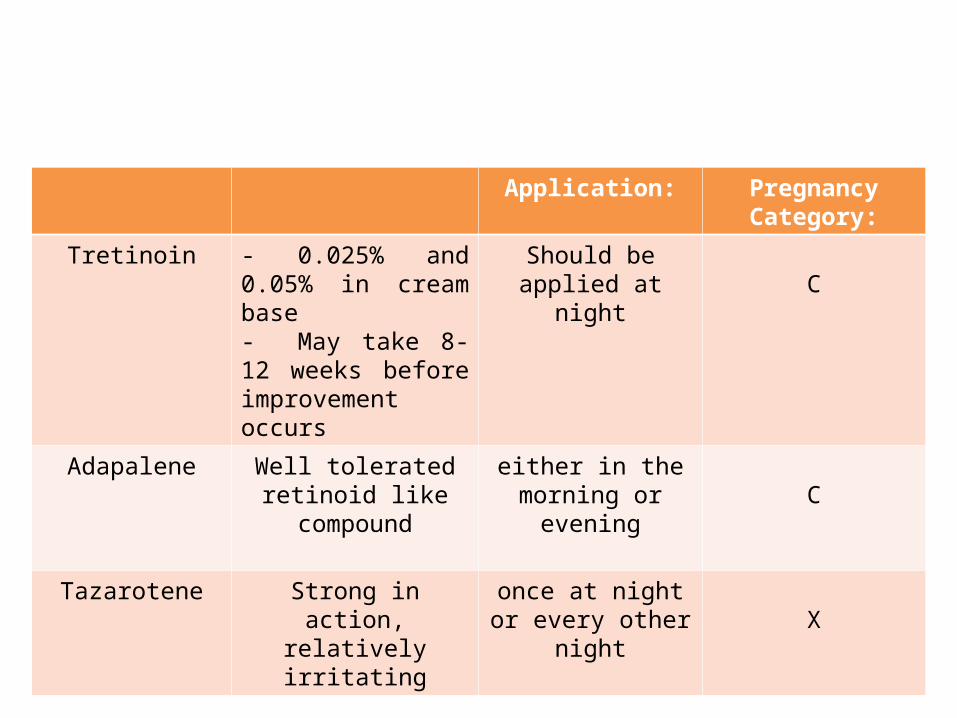
Application: Pregnancy Category:
Tretinoin - 0.025% and 0.05% in cream base- May take 8-12 weeks before improvement occurs
Should be applied at night C
Adapalene Well tolerated retinoid like compound
either in the morning or evening C
Tazarotene Strong in action, relatively irritating
once at night or every other night X

Benzoyl Peroxide
• Has a potent antibacterial effect; P. acne resistance doesn’t develop during use
• Concomitant use during antibiotic treatment will limit the development of resistance
• Wash formulations may be utilized for mild trunkal acne
• Usually used once or twice a day• May irritate skin and produce peeling• Pregnancy Category: C
Topical Antibacterials
• Clindamycin & Erythromycin
• Well tolerated; effective in mild-to-moderate inflammatory acne
• Pregnancy category: B
• Use of topical antibiotics alone is not recommended because of increasing resistance
Sulfur, Sodium Sulfacetamide, Resorcin, Salicyclic Acid
• Useful and helpful if newer medications are not tolerated
• Sulfacetamide-sulfur combination– Mildly effective in both acne and rosacea

Azeleic Acid
• Dicarboxylic acid
• Remarkably free from adverse actions and has mild efficacy in both inflammatory and comedonal acne
• Help to lighten post inflammatory hyperpigmentation
• Pregnancy Category: B

• Indications:– Moderate to severe acne– Patients with inflammatory disease in
whom topical combinations have failed/ not tolerated
– Treatment for chest, back or shoulder acne– Patients in whom absolute control is
deemed essential
• Takes 6-8 weeks to judge efficacy
• Safest and cheapest• Given usually at an initial dose of 250-
500mg, once to four time a day; best taken on an empty stomach
• Side effects:– Vaginitis or perianal itching– Nausea– Staining of growing teeth (not used in
pregnant women and children < 9 years of age)
• Avoided if renal function is impaired
Tetracycline

Dosage Side effects
Doxycycline 50-100 mg od or bid
Photosensitivity reactions
Minocycline Most effective oral antibiotic in treating acne vulgaris; absorption is less affected by food or milk
50-100 mg od or bid
Vertigo; pigmentation; lupus-like syndromes; serum sickness; pneumonitis; hepatitis

Erythromycin
• For those who cannot take tetracycline
• Low efficacy
• Side effects: gastrointestinal upset; vaginal itching (rare)
• Initial dosage: 250-500 mg bid or qid, reduced gradually after control is achieved

Clindamycin
• Initial dose is 150 mg tid, reduced gradually as control is achieved
• Excellent response in treatment of acne but the potential for development of pseudomembranous colitis and availability of retinoids has limited its use
Other Antibiotics
• Sulfonamides• Trimethoprim-sulfamethoxazole• Trimethoprim• Dapsone

• Good candidates for hormonal therapy:– Women with PCOS, adrenal hyperplasia– Women with late onset acne, severe acne,
acne that has not responded to other oral & topical therapies or acne that has relapsed quickly after isotretinoin treatment
– Women with acne primarily on the lower face and neck, deep seated nodules that are painful and lasting
• Oral Contraceptives– Block adrenal and ovarian androgens– Orthro Tri-Cyclin, Estrostep, Alesse, Yasmin– Adverse reactions: nausea, vomiting, abnormal
menses, melasma, weight gain, breast tenderness, thrombophlebitis, pulmonary embolism, HPN
• Spironolactone– Effective dose: 25-200 mg/day– Usually prescribed in combination w/ OC– Side effects: breast tenderness, headache,
dizziness, light headedness, irregular menses, diuresis

• Dexamethasone– Doses of 0.125-0.5 mg once at night reduced
androgen excess and alleviated cystic acne
• Prednisone– Generally only given to patients with severe
inflammatory acne during first few weeks of treatment w/ isotretinoin, for initial reduction of inflammation, and to reduce isotretinoin-induced flares.
• Others:– Finasteride, flutamide, GRH agonists,
estrogen, metformin

• Indications:– For severe acne
– Poorly responsive acne that improves by < 50% after 6 mos of therapy with combined oral and topical antibiotics
– Acne that relapses off oral treatment
– Scars or acne that induces psychological distress
– Gram negative folliculitis, inflammatory rosacea, pyoderma faciale, acne fulminans, hidradenitis suppurativa

• Dose: 0.5-1 mg/kg/day in one or two doses
• Major advantage: it is the only acne therapy that is not open ended
• Adverse effects: – Risk of severe damage to the fetus when given
during pregnancy
– Psychological effects
• Other side effects:– Dry skin, lips, eyes and nasal mucosa
– Arthralgias
– hypertriglyceridemia

Summary of Acne Treatment
Mild Moderate Severe
1. Comedonal- Topical retinoid +/-
physical extraction (first line)
- Alternate retinoid, salicylic acid, azelaic acid (2nd line)
2. Papular/pustular- Topical antimicrobial
combination + topical retinoid, benzoyl peroxide wash if mild trunkal lesions (1st line)
- Alternate antimicrobials + alternate topical retinoids, azelaic acid, sodium sulfacetamide-sulfur, salacylic acid (2nd line)
Papular/Pustular-Oral antibiotic + topical retinoid + benzoyl peroxide (1st line)- Alternate antibiotic, alternate topical retinoid, alternate benzoyl peroxide (2nd line)-In women, spirinolactone + OCP + topical retinoids +/- topical antibiotic and/or benzoyl peroxide-Isotretinoin if relapses quickly off oral antibiotics, does not clear or scars
Nodular/conglobate-Isotretinoin-Oral antibiotic + topical retinoid + benzoyl peroxide-In women, spironolactone + oral birth control pill + topical retinoid, +/- topical or oral antibiotics and/or benzoyl peroxide
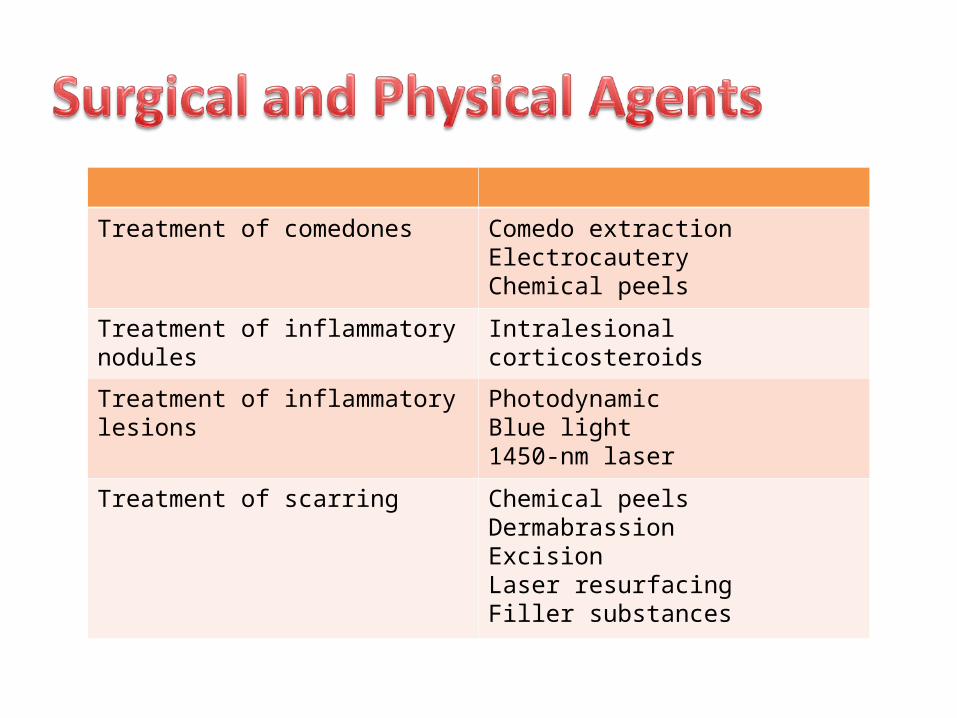
Treatment of comedones Comedo extractionElectrocauteryChemical peels
Treatment of inflammatory nodules Intralesional corticosteroids
Treatment of inflammatory lesions PhotodynamicBlue light1450-nm laser
Treatment of scarring Chemical peelsDermabrassionExcisionLaser resurfacingFiller substances

• Pitted scarring and wide-mouthed depression and keloids
• Maybe prominent and often results from cystic type of acne
• Prominent residual hyperpigmentation, especially in darker-skinned patients
• Pyogenic granuloma formation – more common in acne fulminans and in patients treated with high-dose isotretinoin
• Osteoma cutis – small, firm papules resulting from long-standing acne vulgaris
• Facial edema - uncommon