treatment challenges in transplant patients
TRANSCRIPT

Treatment Challenges inTransplant Patients
Gregory T Everson, MDProfessor of MedicineDirector of Hepatology
University of Colorado Denver

DisclosuresAdvisory Boards: Roche/Genentech, Vertex, GlobeImmune,
BMS, Abbvie, Eisai, HGS/Novartis, Pfizer, Gilead, Janssen/Tibotec, Abbvie/Abbott
Consulting: Roche‐Genentech, HGS/Novartis, BMS,Three Rivers/Kadmon, Vertex, Abbvie, BioTest, Boehringer‐Ingelheim
DSMB: Merck, Centocor, Galectin
Stock/Ownership: Source, HepQuant LLCManagement: HepQuant LLC
Research Grants: Roche/Genentech, Schering/Merck, Vertex,GlobeImmune, Gilead, HGS/Novartis, BMS,Pfizer, Source, Eisai, GSK, Pharmassett,Ortho Biotech, Janssen/Tibotec, Abbvie

Key Questions
1. Should we treat HCV pre‐ or post‐transplant?
2. What are the current antiviral choices?
3. What are the potential future choices?

Pre‐Transplant



1. SVR: Avoid LTx
2. SVR: Prevent Recurrence of HCV
3. On Rx at LTx: Suppress HCV toPrevent Recurrence (pTVR)
Treatment Goals

Pan‐GT: PEG/RBVSOF/PEG/RBVSOF/RBV**LDV/SOF ± RBV
GT 1 only: TT (SMV, TPV, or BOC)SMV/SOF ± RBV3D+r ± RBV
Possible Options
** Only FDA‐recommended Pre‐transplant treatment option.Otherwise, treatment of clinically decompensated cirrhosis is considered “off‐label”.

PEG/RBV
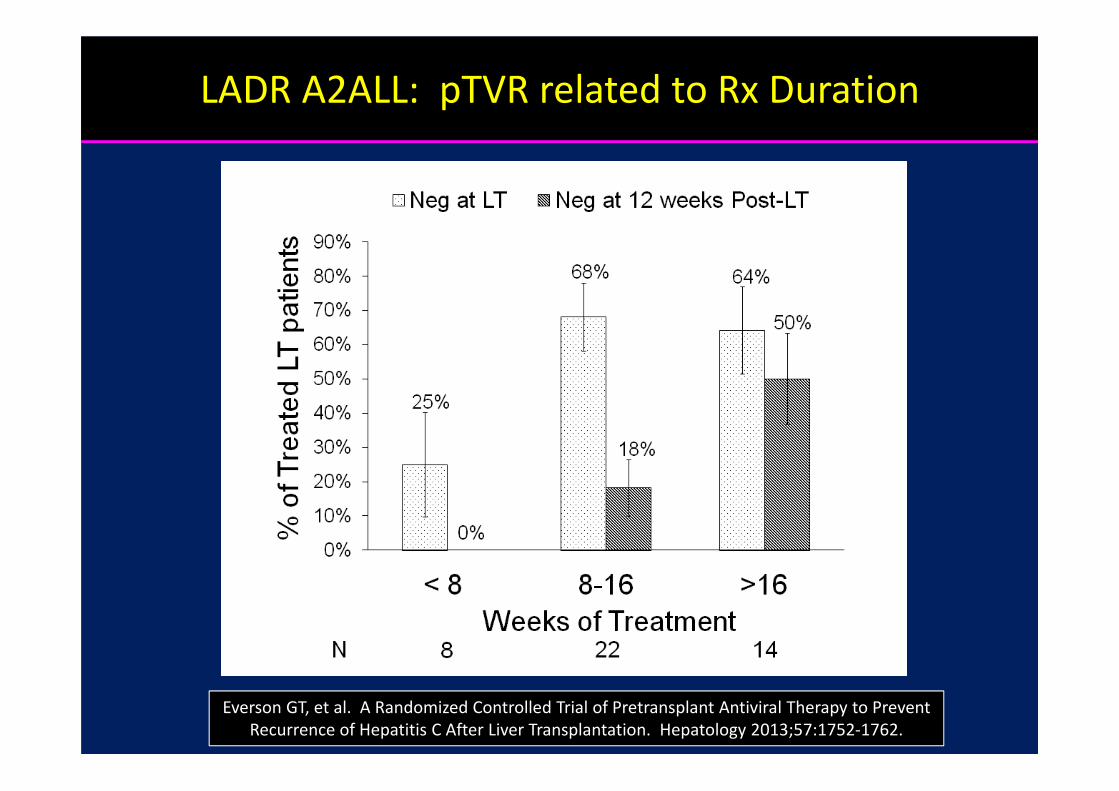
Everson GT, et al. A Randomized Controlled Trial of Pretransplant Antiviral Therapy to PreventRecurrence of Hepatitis C After Liver Transplantation. Hepatology 2013;57:1752‐1762.
LADR A2ALL: pTVR related to Rx Duration

PEG/RBV + BOC or TPV(no data with SIM or SOF)

AlbuminPlatelet Count µL-1
> 100,000 ≤ 100,000
≥ 3.5 g/dLN 306 74
% SVR 55% 37%
% SAE/Death 6% 12%
< 3.5 g/dLN 31 37
% SVR 29% 27%
% SAE/Death 16% 51%
Impact of Disease SeverityCUPIC French open‐access Study
Hezode C, et al. Effectiveness of Telaprevir or Boceprevir in Treatment‐experienced Patients with HCV Genotype 1 Infection and Cirrhosis. Gastroenterology 2014. doi: 10.1053/j.gastro.2014.03.051.

Albumin: < 3.5 g/dL
Platelet Count: < 100,000 µL
CUPIC Caveat
These laboratory features indicate high‐risk for treatment‐related SAEs with PEG/RBV plus BOC or TPV.

PEG/RBV/TPV: pTVR
50
7180
67
0
20
40
60
80
100
Week 4 of TT Week 8 of TT Week 12 of TT pTVR
% HCV RNA negative
Verna EC, et al. Columbia and Georgetown. Hepatology 2012;56:218A. Submitted.High Rates of SAEs, ANEMIA – EPO + Transfusions of pRBCs. One pt underwent LTx at Week 3 of Rx, RNA negative post‐LTx.

Pan‐GT: PEG/RBVSOF/PEG/RBVSOF/RBVLDV/SOF ± RBV#
GT 1 only: TT (SMV, TPV, or BOC)SMV/SOF ± RBV3D+r ± RBV
Acceptable Options
# Daclatasvir (DAC) may substitute for ledipasvir (LDV) for GT 2 and 3.

SOF/RBV
Afdahl N, Everson GT, et al. Sofosbuvir and Ribavirin for the Treatment of Chronic HCV with Cirrhosis and Portal Hypertension with and without Decompensation: Early Virologic Response and Safety. EASL 2014.

56
100 100 100 100
44
75
94 94 93
0
20
40
60
80
100
Week 2 Week 4 Week 8 Week 12 Week 24
CTP A CTP B
% with undetectable HCV RNA
SOF/RBV in Cirrhosis with Portal Hypertension(N=50, 1:1 Rx:No Rx Cntrl for 24 Wks, 48 Wks Rx, HVPG 16 (7-29), CTP<10)
Rx extended to 48 weeks. SVR in most. HVPG improved in a subset. EASL 2015.

pTVR
25
67 65
0
20
40
60
80
100
PEG/RBV TT‐TPV SOF/RBV
% Achieving pTVR
Center Multi Single Multi N 11/44 8/12 24/37%HCC 62% 39% 100%MELD 12 8 8* No SAE was attributed to SOF. Rate of SAEs was similar to rate of SAEs in Controls in LADR‐A2ALL.
Curry MP, et al. Pretransplant Sofosbuvir and Ribavirin to Prevent Recurrence of HCV Infection after Liver Transplantation. Hepatology 2013;58:3134A.
SAE 46%Death 15%
SAE 31%Death 3%
SAE 18%*Death 0%

36
96
0
20
40
60
80
100
<30 Days >30 Days
% Achieving pTVR
Curry MP, et al. Pretransplant Sofosbuvir and Ribavirin to Prevent Recurrence of HCV Infection after Liver Transplantation. Hepatology 2013;58:3134A.
SOF/RBV: pTVR is related toDuration of undetectable HCV RNA

SMV/SOF
1. SMV: FDA‐approved 2013
2. SOF: FDA‐approved 2013
3. SMV/SOF: FDA‐approved 12/2014
AASLD/IDSA Guidelines: “Daily sofosbuvir (400 mg) plus simeprevir (150 mg), with or without weight‐based RBV (1000 mg [<75kg] to 1200 mg [≥75 kg) for 12 weeks is recommended for IFN‐ineligible patients
with HCV genotype 1infection, regardless of subtype.” “……..is recommended for retreatment of HCV genotype 1 infection,regardless of subtype or IFN eligibility.” The basis for these recommendations were an average SVR of 72% in 211 Rx‐Naïve GT1 patients treated with 24 Wks SOF/RBV. SIM/SOF, 12 Wks,
might be a more effective regimen in these patients.
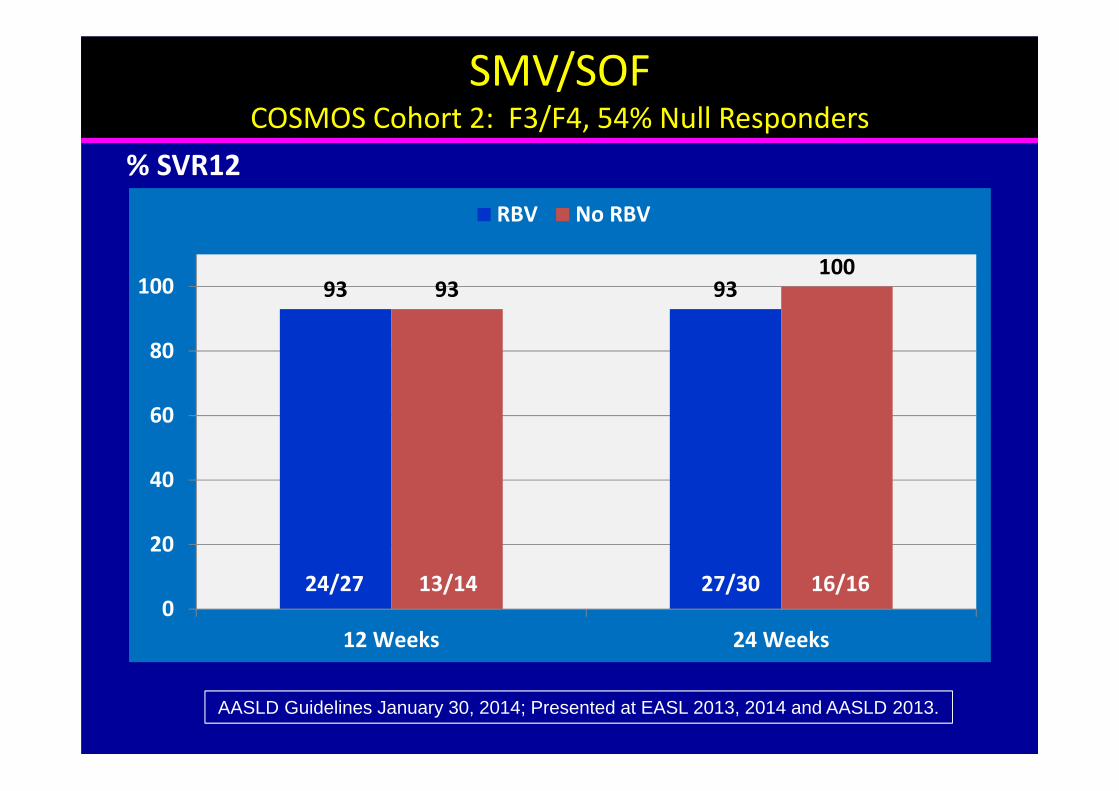
SMV/SOFCOSMOS Cohort 2: F3/F4, 54% Null Responders
93 9393100
0
20
40
60
80
100
12 Weeks 24 Weeks
RBV No RBV
% SVR12
AASLD Guidelines January 30, 2014; Presented at EASL 2013, 2014 and AASLD 2013.
13/1424/27 27/30 16/16

HCV TARGET1012 Treated with SMV/SOF ± RBV (303 evaluable for SVR4)
9287
7585
79
0
20
40
60
80
100
No Cirrhosis Cirrhosis Decomp
All PI Failures% SVR4
Presented at AASLD 2014. RBV did not improve SVR overall or in any subpopulation.Lower SVR4: Low albumin, GT1a, Prior Decomp, TT failure. AEs: Anemia - RBV. SAEs 5 to 6%.
12 Deaths – 9 in patients with cirrhosis.
17/20113/123 27/34 61/81156/180

LDV/SOF
1. SOF: FDA‐approved 2013
2. LDV/SOF: FDA‐approved 12/2014
FDA approved without RBV. Addition of RBV may allow shortening 24 week course to 12 weeks.

LDV/SOF in >500 Patients with GT1 Cirrhosis
96 98 97 10090
96 98 100
0
20
40
60
80
100
12 Wk 12 Wk + RBV 24 Wk 24 Wk + RBV
Rx‐Naïve Rx‐Experienced% SVR 12
Bourliere M, et al. AASLD 2014.

Results: SVR12GT 1 and 4, CTP Class B and C
6 subjects (2 CPT B/24 Wk, 1 CPT C/12 Wk and 3 CPT C/24 Wk) excluded (transplant on study); 3 subjects CPT C/24 Wk have not reached SVR12.Error bars represent 90% confidence intervals.
87 87 8689 89 90
0
20
40
60
80
100
CPT B CPT C
SV
R12
(%)
26/30 19/22 18/20
Overall
24/2745/52 42/47
LDV/SOF + RBV 12 Weeks LDV/SOF + RBV 24 Weeks

Laboratory Results: Change in MELD Score From Baseline Through Follow-up Week 4
26
-6
-4
-2
0
2
4
-6
-4
-2
0
2
4
n=5 n=5 n=2 n=3
(-8)
(+10)
CPT B CPT C
12 wk (n=30)* 24 wk (n=29)* 12 wk (n=23)* 24 wk (n=26)*
*Missing FU-4: n=2 CPT B 12 wks; n=4 CPT B 24 wks; n=2 CPT C 12 wk; n=7 CPT C 24 wk.

3D/r + RBV(Paritaprevir/r + Ombitasvir + Dasabuvir + RBV)
1. 3D/r ± RBV: FDA‐approved 12/2014

Integrated Efficacy Analysis of 4 Phase 3 Studies in HCV Genotype 1a‐Infected Patients Treated With ABT450/r/Ombitasvir and Dasabuvir With and Without Ribavirin|AASLD| November 711, 2014 28
126/142
61/66
14/15
11/11
40/50
115/121
53/56
13/13
10/10
39/42
High SVR12 Rates with 3D + RBV in GT1a Treatment‐Naïve and ‐Experienced Patients With Cirrhosis
12 weeks24 weeks
3D + RBV
p values from Fisher’s exact test

Normalization of liver –related laboratory parameters in HCV GT1‐infected patients with cirrhosis | ACG 2014 | 20 October 2014 29
Improvement from baseline in conjugated bilirubin at PTW12
12‐week arm 24‐week arm
BL mean (mg/dL)
0.30 0.31
PTW12 mean(mg/dL)
0.19 0.17
Mean from BL at PTW12(95% CI)
‐0.10(‐0.12, ‐0.09)
‐0.13(‐0.15, ‐0.11)
3D + RBV

Normalization of liver –related laboratory parameters in HCV GT1‐infected patients with cirrhosis | ACG 2014 | 20 October 2014 30
Improvement from baseline in albumin levels at PTW12
12‐week arm 24‐week arm
BL mean (g/dL)
3.9 3.9
PTW12 mean (g/dL)
4.1 4.2
Mean from BL at PTW12(95% CI)
0.2(0.17, 0.24)
0.3(0.21, 0.31)
3D + RBV

Others

Multi‐DAA in HCV GT1 Cirrhosis
96 92 93 94
0
20
40
60
80
100
LDV/SOF (Gilead) 3D r (Abbvie) 3D (BMS) 2D (Merck)
% SVR 12
RBV ± + ± ±Duration 12 vs 24 12 vs 24 12 12 vs 18Genotype 1a/1b 1a 1a/1b 1a/1bPhase 3 3 3 2
493/513 241/263 187/201 115/123

Genotypes 2 and 3

SOFOSBUVIR
RIBAVIRIN
Cirrhosis, Rx-Experienced12 Wks
Cirrhosis, Rx-Naive12 Wks
No Cirrhosis, Rx-Naive12 Wks
ExpectedSVR
TreatmentDuration
Genotype 2
95%1
94%1
60%2,*
Cirrhosis, Rx-Experienced16 Wks 78%2
1 Data from FISSION and POSITRON and 2 FUSION.*In VALENCE, an SVR of 78% (7/9) was achieved with 12 weeks SOF/RBV. Given the
discordancy in results, optimal duration of SOF/RBV for Rx‐experienced cirrhosis is unknown.
No Cirrhosis, Rx-Experienced12 or 16 Wks 97%2

SOFOSBUVIR
RIBAVIRIN*
No Cirrhosis, Rx-Experienced24 Wks (85/98)
Cirrhosis, Rx-Naive24 Wks (12/13)
No Cirrhosis, Rx-Naive24 Wks (87/92)
ExpectedSVR
TreatmentDuration
95%
92%
87%Cirrhosis, Rx-Exp
24 Wks (29/47) 62%
Genotype 3 (based on VALENCE* study)
An alternative for IFN‐eligible patients could be SOF/PEG/RBV for 12 weeks.In PROTON and ELECTRON studies (Rx‐Naïve) 38/39 patients (97%) achieved SVR.
In LONESTAR‐2 (Rx‐Experienced), 83% (10/12) achieved SVR.* Zeuzem, et al. NEJM 2014;370:1993‐2001.

Pan‐GT: SOF/RBVLDV/SOF ± RBV#
GT 1 only: SMV/SOF ± RBV3D+r ± RBV
Pre‐Transplant Options
# Daclatasvir (DAC) may substitute for ledipasvir (LDV) for GT 2 and 3.

Post‐Transplant

1. SVR
2. Improve Graft and Patient Survival
Treatment Goals

Pan‐GT: PEG/RBVSOF/PEG/RBVSOF/RBV**LDV/SOF ± RBV
GT 1 only: TT (SMV, TPV, or BOC)SMV/SOF ± RBV3D+r ± RBV
Possible Options
** None of these post‐transplant treatment options are FDA‐approved.Treatment of post‐transplant patients is considered “off‐label”.

PEG/RBV

Gane EJ, Agarwal K. Am J Transplant 2014;14:994‐1002.
PEG/RBV: SVR

PEG/RBV + BOC or TPV(no data with SIM or SOF)

CRUSH C and French Multicenter Studies
Adverse Events• 20% Early discontinuation• 25‐59% Hospitalizations• 56% Blood transfusions• 14‐40% Renal insufficiency• 3‐17% Rejection• 7‐8% Liver‐related deathCRUSH-C French
%S
VR
12
100
80
60
40
20
59
53/90 36/79
Stravitz, et al. AASLD 2013. Abstract 416. Coilly A, et al. AASLD 2013. Abstract 216.
46

Pan‐GT: PEG/RBVSOF/PEG/RBVSOF/RBVLDV/SOF ± RBV#
GT 1 only: TT (SMV, TPV, or BOC)SMV/SOF ± RBV3D+r ± RBV
Acceptable Options
# Daclatasvir (DAC) may substitute for ledipasvir (LDV) for GT 2 and 3.
SOF/RBV ± PEG
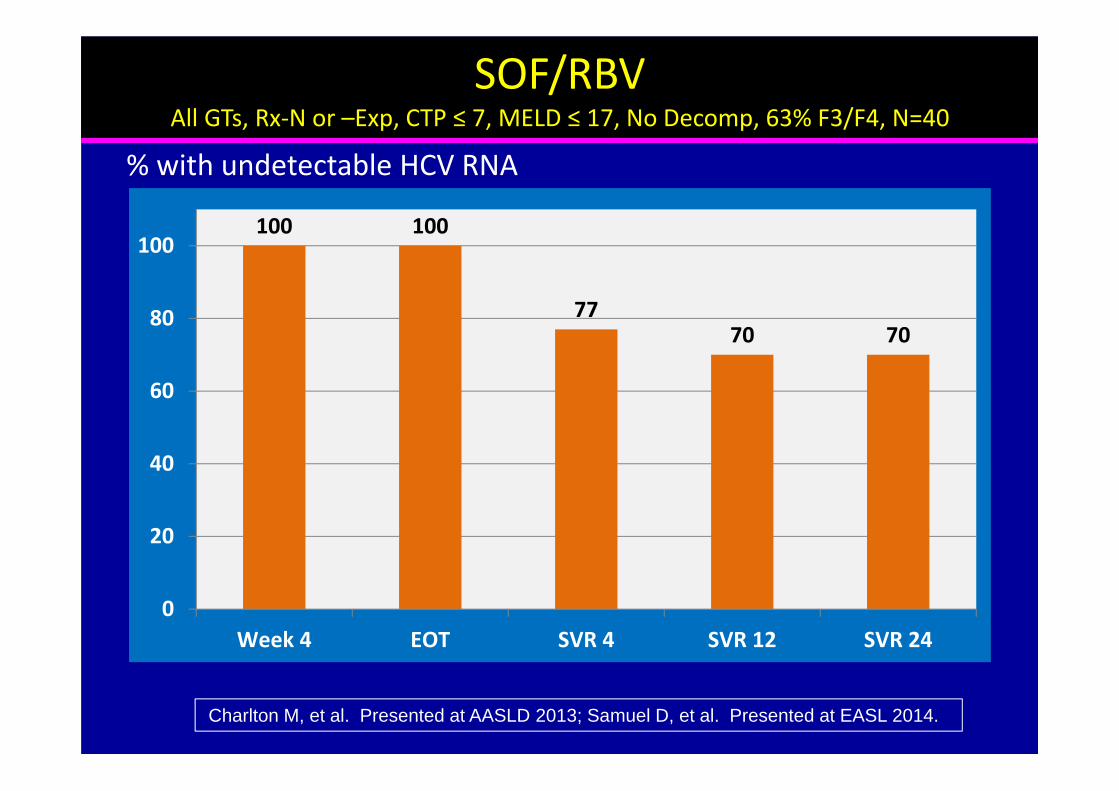
SOF/RBVAll GTs, Rx‐N or –Exp, CTP ≤ 7, MELD ≤ 17, No Decomp, 63% F3/F4, N=40
100 100
7770 70
0
20
40
60
80
100
Week 4 EOT SVR 4 SVR 12 SVR 24
% with undetectable HCV RNA
Charlton M, et al. Presented at AASLD 2013; Samuel D, et al. Presented at EASL 2014.

SOF/RBV ± PEGPost‐LT Compassionate Use for Severe HCV Recurrence, N=104
87
62 62
21 21
0
20
40
60
80
100
EOT SVR12 Improved Stabilized Worse/Died
% of Patients
Forns X, et al. Presented at AASLD 2013 and EASL 2014. Wide range of disease severity,some very sick. Improved Bili, INR, Alb, and MELD.

SMV/SOF

HCV TARGET143 Treated with SMV/SOF ± RBV (68 evaluable for SVR4)
9486
0
20
40
60
80
100
No Cirrhosis Cirrhosis
All% SVR4
Presented at AASLD 2014. Anemia from RBV was a common AE.8.5% had an SAE.
29/3127/34
32/37156/180

3D/r + RBV(Paritaprevir/r + Ombitasvir + Dasabuvir + RBV)

ABT450/r/Ombitasvir/Dasabuvir/RBVGT1, Rx‐N, <F3, No Decomp, N=34
100 100 97 96
0
20
40
60
80
100
Week 4 EOT SVR 4 SVR 12
% with undetectable HCV RNA
Kwo P, et al. Presented at EASL 2014.

LDV/SOF

96 96
85
60
98 96
83
67
0
20
40
60
80
100
F0–F3
SV
R12
(%)
53
53/55 22/26 15/18
CPT B
55/56 25/26 24/25 2/3
CPT A
Results: SVR12GT 1 or 4: Post-Transplant F0–F3, CPT A, B, C
Error bars represent 2-sided 90% exact confidence intervals.8 CPT B 24 Week and 1 CPT C 24 Week subjects have not reached the Week 12 post treatment visit.
LDV/SOF + RBV 12 Weeks LDV/SOF + RBV 24 Weeks
3/5
CPT C

Laboratory Results: Change in MELD Score From Baseline Through Follow-up Week 4
54
CPT A Patients (n=48)
-8
-6
-4
-2
0
2
4
CPT B Patients (n=41)
n=4 n=1
-8
-6
-4
-2
0
2
4
n=9 n=4
(-11)
12 Wk (n=23) 24 Wk (n=25) 12 Wk (n=21) 24 Wk (n=20)

Pan‐GT: SOF/RBVLDV/SOF ± RBV#
GT 1 only: SMV/SOF ± RBV3D+r ± RBV
Post‐transplant Options
# Daclatasvir (DAC) may substitute for ledipasvir (LDV) for GT 2 and 3.
Longer duration of 24 weeks and addition of RBV may be required,particularly for liver recipients with cirrhosis.

1. From IFN‐based Treatment• Low efficacy (both pre‐ and post‐LT)• High Toxicity (especially in cirrhosis)• Limited Applicability
2. To IFN‐free Treatments• Improved efficacy (both pre‐ and post‐LT)• Limited Toxicity (both pre‐ and post‐LT)• Treat either pre‐ or post‐LT
Paradigm Shift

“Anybody can jump a motorcycle. The trouble begins when you try to land it.” Evel Kneivel

Drug‐Drug Interactions
Clinical Pharmacist

Resources for DDIs• Outstanding – University of Liverpool (David Back, Editorial Board, EASL reps); sponsored by Janssen, MSD, Roche, Vertex:– http://www.hep‐druginteractions.org
• FDA:– http://www.fda.gov/Drugs/DrugSafety/
• Other Online Resources –– http://www.drugs.com/drug‐interactions/html– http://www.merckmedicus.com/pp/us/hep– Epocrates– Micromedex, Lexicomp and Others

Can Hepatitis C Virus be Cured?
Yes
But, someone has to pay for it!
Panic: 5 x 106 cases @ 105 $/case
= $500,000,000,000

• Study of economic burden of chronic hepatitis C in the US, stratified by disease severity, based upon a large health insurance claims database.
• Based on data from 53,796 patients with chronic hepatitis C – 78% without cirrhosis, 7% with compensated cirrhosis, 15% with ESLD
• Overall Annual Healthcare Costs per Patient: $24,176
• Annual Costs per Patient Without Cirrhosis: $17,277
• Annual Costs per Patient With Compensated Cirrhosis: $22,752
• Annual Costs per Patient With ESLD: $59,995
• Estimated US Average Charges per LTx in 2011: $577,100
The Price of NOT Treating Chronic Hepatitis C
Reau N, Jensen D. Review/Editorial HEPATOLOGY 2014;59:1246‐1249.Gordon SC, et al. Disease Burden in Patients with chronic hepatitis C in US …….2003 to 2010. Presented at AASLD 2011.
http://digestive.niddk.nih.gov/ddiseases/pubs/livertransplant/http://digestive.niddk.nih.gov/before‐the‐transplant/financing‐a‐transplant/the‐costs/

1. MELD “Purgatory”?• MELD decreases with SVR• Portal hypertension and clinical
complications persist
2. HCV+ Donor?• HCV+ recipient – wait to treat?• HCV‐ recipient – accept liver?• Renal transplantation – wait to treat?• Renal candidate HCV+ or ‐ ‐ accept kidney?
Intriguing Questions