treatment for pad: can we turn humans into · pdf file« every 30 seconds a lower limb...
TRANSCRIPT

Inserm
Joseph EMMERICH
Dept of Vascular Medicine
University Paris Descartes - INSERM U765
Treatment for PAD: can we turn humans
into salamanders ?

Prevalence of intermittent claudication (IC). Edinburgh Artery Study. Int J Epidemiol 1991;20:384-92
Prevalence of IC was 4.5% and incidence 15.5 per 1000 person-years.
In individuals who were initially symptomatic :
- 28.8% continued to have IC after 5 years
- 8.2% underwent revascularization or amputation
- 1.4% developed ischemic ulcers
Mean prevalence of IC in large population studies (From the TASC consensus)
0
1
2
3
4
5
6
7
30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74
Age group

Critical leg ischemia
a) persistently recurring ischemic rest pain requiring
regular adequate analgesia for more than 2 weeks, with
an ankle systolic pressure of < 50 mmHg and/or a toe
systolic pressure of < 30 mmHg, or
b) ulceration or gangrene of the foot or toes, with an
ankle systolic pressure of < 50 mmHg or a toe systolic
systolic pressure of < 30 mmHg.
CLI, in both diabetic and nondiabetic patients, is
defined by either of the following two criteria :
Incidence of CLI is around 500 per million per year
Inserm

Hiatt WR. N Engl J Med 2001;344:1608
Ankle Brachial Index (ABI)
Higher ankle pressure
Higher humeral pressure
Below 0.4 severe PAD

« Every 30 seconds a lower limb
is lost somewhere in the world
as a consequence of diabetes »
Boulton, Vol 366 November 12, 2005


Stage I Stage IIa Stage IIb Stage III or IV
Asymptomatic Mild claudication Moderate claudication Critical leg ischemia
(rest pain, ulcer or gangrene)

Bypass
Percutaneous angioplasty

Treatment strategy of Critical Limb Ischemia
To control pain and infection
Rapid evaluation of the arterial lesions (arteriography)
and rapid revascularization (surgery or angioplasty). In some cases (gangrene or septicemia), poor general condition,
a major amputtion is initially preferred.
Revascularization No possibility of
revascularization
Success
• Medical treatment
• Amputation Failure
Inserm

Tibioperoneal (outflow lesion) angioplasty can be used as primary
treatment in 235 patients with CLI (5-year follow-up)
Dorros G et al. Circulation 2001;104:2057-62.
Actuarial analysis of CLI patients
Fontaine
Inserm

Recommendation 100 : Spinal cord stimulation in CLI.
On current evidence, spinal cord stimulation cannot be
recommended in the treatment of CLI.
Recommendation 101 : Chelation therapy in CLI.
There is no scientific basis for the use of chelation therapy
in the treatment of peripheral arterial disease.
Recommendation 102 : Lumbar sympathectomy in CLI.
There is currently insufficient scientific evidence for the
selection of patients likely to benefit from lumbar
sympathectomy for the treatment of CLI.
Useless treatment
TASC. J Vasc Surg 2000;31(Suppl).
Inserm

ICAI study : Ann Intern Med 1999;130:412-21
Total patients
(n = 1334)
12.6%
11.2%
30.4%
0.9%
55.1%
Alprostadil
(n = 661)
10.9%
11.0%
29.3%
1.2%
52.6%
Controls
(n = 673)
14.3%
11.3%
31.4%
0.6%
57.5%
0.064
> 0.2
> 0.2
> 0.2
0.074
Death
Amputation
Persistant CLI
MI, stroke
Combined events
Events at 6 months
Inserm

Superficial femoral occlusion - Collateral vessels
Arteriogenesis: remodeling of newly formed
or preexisting vascular vessels
Angiogenesis: sprouting of new capillaries from preexisting vessels
Vasculogenesis: formation of blood vessels from endothelial progenitor cells

Ramsauer M. JCI 2002;110:1615
Angiogenesis
Vascular lesion
Tumor
Ischemic tissue Inserm Moore M.A.S.
JCI 2002.
Vasculogenesis

Drawing by M. Malphighi (1661), showing the vascular network of arteries, capillaries
and veins in a developing chicken embryo.
From Carmeliet P, Nature 2005
Inserm
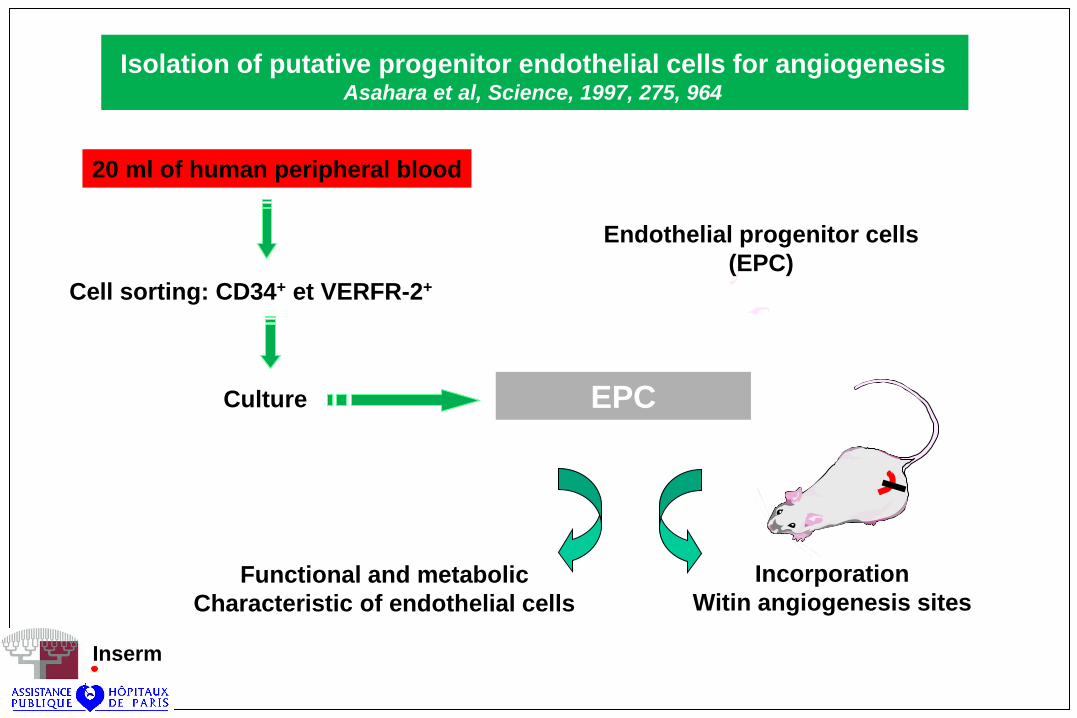
Isolation of putative progenitor endothelial cells for angiogenesis Asahara et al, Science, 1997, 275, 964
20 ml of human peripheral blood
Culture
Cell sorting: CD34+ et VERFR-2+
EPC
Functional and metabolic
Characteristic of endothelial cells
Incorporation
Witin angiogenesis sites
Endothelial progenitor cells
(EPC)
Inserm

CLI
Pro-angiogenic GF
Anti-angiogenic GF
of PEC
VEGF
PlGF
FGF1,2
Angiopoietin 1,2
HGF
IGF
EPO
G-CSF,GM-CSF
MCP-1
HIF-1
TSP-1
Inserm

Circulating Endothelial Progenitor Cells, Vascular Function and CV risk.
Hill JM et al. N Engl J Med 2003;348:593-600
Circulating Endothelial Progenitor Cells and Cardiovascular Outcome.
Werner N et al. N Engl J Med 2005;353:999-1007
Inserm

Critical overexpression of thrombospondin 1 in chronic leg ischaemia.
J. Favier et al. J Pathol. 2005;207:358-66.
mRNA
Western-blot Overexpression of TSP1 in macrophages
and endothelial cells of ischemic tissues Inserm

EPCs C-EPCs
ischemia
VEGF-A
PLGF
Mobilisation
CD 34 +
CD 133+
VEGFR2+
VE-cadherin+
CD 146+
CXCR4 +
vWF +
CD 31 +
GM-CSF
EPO
Statins
Inserm

From Carmeliet P, Nature Med 2003
Participate directly
or indirectly

What are able to do the salamanders ?


The stages of newt limb regeneration. One day: a wound epithelium covers the
amputation site. One to four weeks: dedifferentiation, migration, and proliferation of cells
leads to the formation of a regeneration blastema. Three to six weeks: the limb flattens out
and cartilage begins to form. Four to ten weeks: the new digits develop and regeneration
of the limb is completed (From Odeberg SJ, 2005).


From Whited & Tabin, 2009
and Odelberg, 2005
Msx1, BMP, Notch 1, MMPs pathways

GENE
and / or
CELL THERAPY

Gene therapy of PAD

From : Losordo DW, Dimmeler S. Circulation 2004;109:2487-91

Clinical evidence of angiogenesis after arterial
gene transfer of phVEGF165 in patient with
ischaemic limb.
Isner JM. Lancet 1996;348:370.
Constitutive expression of phVEGF165 after
intramuscular gene transfer promotes collateral
vessel development in patients with critical limb
ischemia.
Baumgartner I. Circulation 1998;97:1114-23.
Inserm

Baumgartner I.
Circulation 1998;97:1114-23.

Intramuscular vascular endothelial growth factor gene therapy in patients with
chronic critical leg ischemia. Shyu KG. Am J Med 2003;114:85-92
21 patients with CLI – 24 legs treated (5 Buerger).
Naked plasmid coding for VEGF (same plasmid as J. Isner)
(dose 400 to 2000 mg – 2 injections IM/calf after 1 month)
Increase circulating VEGF from 26 to 63 pg/mL (p<0.005) 2 weeks
after the injection.
Transient edema in 25% of the patients.
Follow-up : 6 months.
- Disappearance of rest pain : 83%
- Improvement or healing of ischemic ulcer : 75%
ABI : 0.58±0.24 -> 0.72±0.28 (p<0.001) 4 weeks after second injection
Perfusion scoring of the leg (ARM) : 0.37±0.10 -> 0.47±0.11 (p<0.01)

Naked plasmid DNA encoding fibroblast growth factor type 1 for the treatment
of end-stage unreconstructible lower extremity ischemia : preliminary results of
a phase I trial. Comerota AJ et al. J Vasc Surg 2002;35:930-6
51 patients.
Tolerance and dose finding (dose max. 2x8000 mg)
Biodistribution of plasmid was limited and transient in plasma ;
absent in urine.
No increase of FGF-1 was detected.
Significant reduction of pain and ulcer size was seen, as well
as increase in ABI (P<0.01).
Absence of control group.
Inserm

Increased vascularity detected by digital subtraction angiography after VEGF
gene transfer to human lower limb artery: a randomized, placebo-controlled,
Double-blinded phase II study.Mäkinen K, et al. Mol Therapy 2002;6:127-133
3 groups – 19 Controls - 17 VEGF Plasmid/liposome – 18 VEGF adenovirus
Intra-arterial administration after peripheral angioplasty.
40 IC and 14 CLI patients.
Digital subtraction angiography revealed increased vascularity in the
VEGF-treated groups distally to the gene transfer site .
Mean Rutherford class and ABI showed statistically significant
improvements in the VEGF-Ad and VEGF-P/L groups, but similar
improvements were also seen in the control patients.
Anti-adenovirus antibodies increased in 61% of the patients treated
with VEGF-Ad.
Inserm
Phase 2 study

Regional angiogenesis with vascular endothelial growth factor in peripheral arterial
disease. A phase II randomized, double-blind, controlled study of adenoviral
delivery of VEGF 121 in patients with disabling intermittent claudication.
Rajagopolan S, et al. Circulation 2003;108:1933-38
101 patients, randomized in 3 groups.
Patients were randomized to low-dose (4x109 PU) AdVEGF121, high-dose
(4x1010 PU) AdVEGF121, or placebo, administered as 20 intramuscular
injections to the index leg in a single session.
A single unilateral intramuscular administration of AdVEGF121
was not associated with improved exercise performance or quality
of life in this study.
This study does not support local delivery of single-dose VEGF121
as a treatment strategy in patients with unilateral PAD and IC.
Inserm
Phase 2 study

Permanent ischemia as seen
in CLI, but not in IC, is probably
required to induce significant
angiogenesis.

Treatment with intramuscular vascular endothelial growth factor gene
compared with placebo for patients with diabetes mellitus and critical limb
ischemia: a double-blind randomized trial. . Kusumanto YH, et al. Human Gene Therapy 2006;17:683-91.
A double-blind, placebo-controlled study was performed in 54 adult
diabetic patients with CLI.
Patients were randomized to receive phVEGF165 or placebo (0.9% NaCl).
A single unilateral intramuscular administration of AdVEGF121
was not associated with improved exercise performance or quality
of life in this study.
This study failed to meet the primary objective of significant amputation
reduction (3 amputations vs 6; NS).
Overall, 3 versus 14 responding patients (p=0.003). Mainly decreased in
pain and ABO improvement.
Inserm

Inserm
Treatment with Intramuscular VEGF Gene Compared with Placebo for
Patients with Diabetes Mellitus and Critical Limb Ischemia:
A Double-Blind Randomized Trial. Kusumanto YH et al. Hum Gene Ther, 2006
In this small randomized study gene therapy failed to meet the primary
objective of significant amputation reduction.
However, significant and meaningful improvement was found in patients
treated with a VEGF165-containing plasmid.
There were no substantial adverse events.

125 patients. Multicenter study (37 sites).
Randomized, double blind study : FGF-1 vs Placebo.
CLI with non healing ulcers were randomized to receive
eight intramuscular injections of placebo or 2.5 ml of
NV1FGF at 0.2 mg/ml on days 1, 15, 30, and 45 (total
16 mg: 4 × 4 mg).
The primary end point was occurrence of complete
healing of at least one ulcer in the treated limb at week 25.
Secondary end points included ankle brachial index (ABI),
amputation, and death.
125 patients included – 107 eligible for evaluation Inserm
Therapeutic angiogenesis with intramuscular NV1FGF improves
amputation-free survival in patients with CLI. TALISMAN study.
Nikol S et al. Molecular Therapy 2008;16:972-8.

Therapeutic angiogenesis with intramuscular NV1FGF improves
amputation-free survival in patients with CLI. TALISMAN study.
Nikol S et al. Molecular Therapy 2008;16:972-8.
Amputation rate (week 52)
All
Major
Death rate (week 52)
Combined major
Amputation + deaths
Complete healing of > 1 ulcer
Mean change
ABI
TBI
TcPO2
Placebo
(N=56)
31 (55.4%)
19 (33.9%)
13 (23.2%)
29 (51.8%)
8 (14.3%)
0.01 ± 0.04
0.03 ± 0.02
9.81 ± 3.15
NV1FGF
(N=51)
19 (37.3%)
8 (15.7%)
6 (11.8%)
14 (27.4%)
10 (19.6%)
0.05 ± 0.04
0.04 ± 0.02
8.55 ± 3.41
p value
0.013
0.019
0.111
0.011
0.514
NS
NS
NS
Endpoints at week 25

Intramuscular Fibroblast Growth Factor-1 gene transfer in patients with CLI :
A double-blind, placebo-controlled study. Etude TALISMAN (Mol Ther 2008)
Major amputations Deaths

All
Serious
Severe
Possibly related to study drug
Leading to discontinuation
Neoplasm
Cardiovascular
Retinopathy
Death
Placebo
(N=61)
91.8%
80.3%
68.9%
21.3%
16.4%
8.2%
11.5%
0
24.6%
NV1FGF
(N=57)
93%
70.2%
47.4%
26.3%
7.0%
8.8%
24.6%
1.8%
17.5%
Adverse events at week 25
Total
(N=118)
92.4%
75.4%
58.5%
23.7%
11.9%
8.5%
17.8%
0.8%
21.2%
Therapeutic angiogenesis with intramuscular NV1FGF improves
amputation-free survival in patients with CLI. TALISMAN study.
Nikol S et al. Molecular Therapy 2008;16:972-8.

Inserm

Interestingly, the benefit relating to the amputation rate
observed with angiogenic therapy in the present study
was not associated with a benefit in respect of
hemodynamic end points (ABI, TBI), and no significant
differences in these were observed between the two
groups.
These data indicate that ABI and TBI, as well as ulcer
healing and ulcer size, may not be useful markers
of NV1FGF efficacy in patients with CLI,
Inserm

Isner
(1996)
Baumgartner
(1998)
Makinen
(2002)
Comerota
(2002)
Shyu
(2003)
Rajagopalan
(2003)
Motyas L
(2005)
Kusumanto
(2006)
Rajagopalan
(2007)
Nikol
(2008)
Powell
(2008)
IA VEGF165 plasmid
IM VEGF165 plasmid
IA VEGF adenovirus
IA VEGF plasmid/lipo
IM FGF1 plasmid
IM VEGF 165 plasmid
IM VEGF121 adenovirus
IM FGF-4 adenovirus
IM VEGF 165 plasmid
IM HIF-1a adenovirus
IM FGF1 plasmid
IM HGF plasmid
1 -
9 -
18 19
17 19
51 -
24 -
72 33
10 3
27 27
34 7
51 56
78 26
12 wks
6 mths
2 yrs
6 mths
6 mths
6 mths
6 mths
3 mths
1 yr
6 mths
6 mths
Increased collaterals (angio). Spider angioma.
Transient oedema.
Increased collaterals (angio) and increased ABI.
Increased collaterals. No change in ABI.
Increased collaterals. No change in ABI.
Reduction in pain and ulcer size.
Increased ABI and TcPO2.
Increased collaterals and improved ABI.
Reduced rest pain and ulcer healing.
Patients without CLI, but IC.
No improvement of peak walking time, ABI or IC.
Increased collaterals (angiography)
Reduction in pain and ulcer healing
No change in amputatioin rate
Safety of the treatment. No correlation between
ABI and outcomes
Decrease in minor and major amputations
Similar improvement in ulcer healing
No difference between treated and placebo groups
Author
(Year)
Treatment N° of patients
Active Control
FU Results
Summary of gene therapy trials in PAD
Total number of treated patients > 500

TAMARIS study Sanofi-Aventis
NV1-FGF
Confirmation of theTalisman study
Inserm

• METHODE:
TAMARIS est donc une étude internationale de phase III multicentrique.
Elle a inclus 525 malades présentant une ischémie critique des membres inférieurs avec ulcères
cutanés, non accessible à la revascularisation. Ils ont été randomisés, en double aveugle, pour être soit
traités par transfert de gène sous la forme de 4 injections intramusculaires multiples réalisées à 2
semaines d’intervalle, soit par injection de placebo.
• RESULTATS:
Pas d’impact sur les amputations et les décès
A 12 mois de la première injection de la thérapie à visée angiogénique, le taux d’amputation majeure et
de décès qui constituait le critère principal de l’étude a été identique dans les 2 groupes avec 37% dans
le groupe actif contre 33% dans le groupe placebo (RR = 1,11 ; p = 0,48).
Le taux d’amputation majeure seul a été de 25,9% contre 21% dans le groupe placebo
(RR = 1,2 ; p = 0,31).
• TOLERANCES
un cancer ou une rétinopathie proliférative avait été exclus de l’étude, aucun effet secondaire de ce type
n’a été observé à 1 an. Le taux de cancer, de rétinopathie, d’infarctus et d’insuffisance rénale a été
identique dans les 2 groupes. Une surveillance prolongée jusqu’à 3 ans sur ces critères est prévue.
Etude TAMARIS
AHA NOVEMBRE 2010,CHICAGO
HIATT W et al. AHA 2010

Amputation et décès à 1 an dans TAMARIS
Hiatt WR. NV1FGF gene therapy on amputation-free survival in
critical limb ischemia: phase 3 randomised, double-blind placebo-
controlled trial (TAMARIS). AHA 2010
Placebo (n = 259)
Th. Gèn. (n = 266)
RR p
Amputation majeure ou décès
86 (33,2 %) 96 (37,07 %) 1,11 0,48
Amputation majeure
55 (21,24 %) 67 (25,87 %) 1,20 0,31
Décès 39 (15,06 %) 46 (17,76 %) 1,15 0,53

Angiogenic synergism by the
combination of PDGF-BB and
FGF-2. Cao R. et al.
Nature Med 2003;9:604.

Use of a constituvely active HIF-1a transgene as a therapeutic strategy
in no-option critical limb ischemia patients.
Rajagopolan S, et al. Circulation 2007;115:1234-43
34 patients.
Escalation dose from 1x108 to 2x1011 viral particles.
HIF-1a therapy in patients with CLI was well tolerated, supporting further,
larger, randomized efficacy trials.
Inserm

Cell therapy of PAD

Therapeutic angiogenesis for patients
with limb ischaemia by autologous
transplantation of bone-marrow cells :
a pilot study and a randomised
controlled trial. Tateishi-Yuyama E et al.
Lancet 2002;360:427-35
General anesthesia.
Bone marrow cells (500 ml)
Mononuclear cells (95% purity)
Concentrated in 30 ml.
Cells implanted within 3 hours, by IM
injection in gastrocnemius (40 sites,
1.5 cm deep).

ABI 0.34 --> 0.47
Increase in ABI in 17 of 25
No change in the leg treated
with saline
ABI 0.37 --> 0.46
Increase in ABI in 13 of 20
No change in the leg treated
with PBMNCs
TcPO2 28.8 --> 46.3
Pain resolved in 16 of 20 legs
treated with mononuclear cells
but in only 3 of 20 legs treated
by peripheral blood monon. cells
Group B
Group A Groupe A
Groupe B

Therapeutic angiogenesis for patients
with limb ischaemia by autologous
transplantation of bone-marrow cells :
a pilot study and a randomised
controlled trial. Tateishi-Yuyama E et al.
Lancet 2002;360:427-35

Autologous transplantation of peripheral blood stem cells as an effective
therapeutic approach for severe arteriosclerosis obliterans of lower extremities.
Huang PP, et al. Thromb Haemost 2004;91:606-9
5 patients with CLI.
CD34+ mobilsation by G-CSF (600 mg/JD) injection during 5 days.
Cell therapy product defined as « peripheral blood stem cells »
containing 0,35% of CD34+ (concentration 1 x108 cell / mL).
Injection of 30 mL of this cell therapy product (40 injections
of 0.75 mL).
Inserm
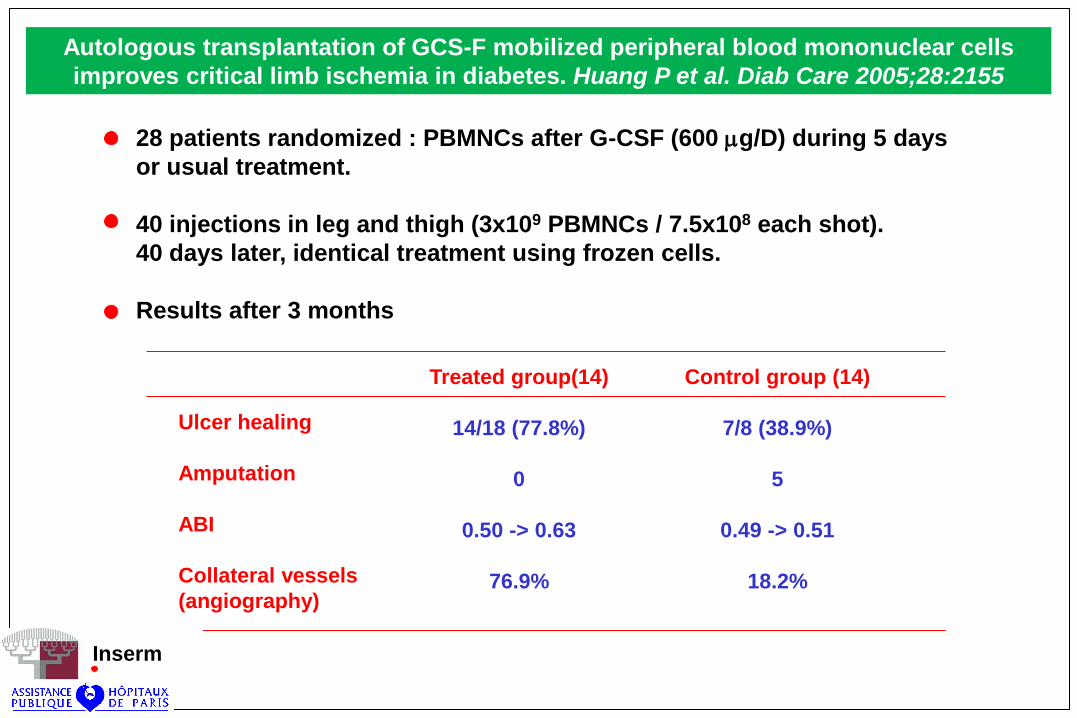
Autologous transplantation of GCS-F mobilized peripheral blood mononuclear cells
improves critical limb ischemia in diabetes. Huang P et al. Diab Care 2005;28:2155
28 patients randomized : PBMNCs after G-CSF (600 mg/D) during 5 days
or usual treatment.
40 injections in leg and thigh (3x109 PBMNCs / 7.5x108 each shot).
40 days later, identical treatment using frozen cells.
Results after 3 months
Treated group(14)
14/18 (77.8%)
0
0.50 -> 0.63
76.9%
Control group (14)
7/8 (38.9%)
5
0.49 -> 0.51
18.2%
Ulcer healing
Amputation
ABI
Collateral vessels
(angiography)
Inserm

Author
(year)
Tateishi-Yuyama
(2003)
Higashi
(2004)
Huang
(2004)
Saigawa
(2004)
Huang
(2005)
Lenk K
(2005)
Yang
(2005)
…..
Treatment
(N of cells)
BMMNCs
(0.7 ± 2.9x109)
BMMNCs
(1.6 ± 0.3x109)
PBMNCs
(3x109)
BMMNCs
(6.04 ± 1.58x107/kg)
PBMNCs
(3x109)
PBMNCs
(39x106)
PBMNCs
…..
Injection
IM, calf
40 x 0.75 ml
IM, calf
40 x 0.75 ml
IM, thigh, leg
and foot
IM
IM, calf, thigh
40 x 0.75 ml
Intra-arterial
4 days of cell cult
IM
calf and foot
…..
N of
patients
45
7
5
8
14 treated
14 controls
(randomized)
7
62
……
FU
(weeks)
24
24
12
4
12
Results
Collaterals, ABI, TcPO2
Collaterals, ABI, TcPO2
Endothel-dependent VD
ABI and laser-Doppler
Correlation between CD34+
and in ABI
ABI and laser-Doppler
78% of ulcers healed vs
39% in controls ABI, TcPO2
Endothel-dependent VD
Decrease pain
ABI, TcPO2, ulcer healing
…..
Review of the trials of cell therapy in CLI
Since 2002, a steady rise in the number of clinçical reports, currently accumulating to at least
39 reports, including more than 750 patients.

Autologous stem cell therapy for PAD. Meta-analysis and systematic
review of the literature. Fadini et al. Atherosclerosis 2010;209:10-17.

Autologous stem cell therapy for PAD. Meta-analysis and systematic
review of the literature. Fadini et al. Atherosclerosis 2010;209:10-17.

Walter D H et al. Circ Cardiovasc Interv 2011;4:26-37
Study flow chart of the PROVASA study.

ABI during the randomized-start phase and until 6 months follow-up (open-label phase).
Walter D H et al. Circ Cardiovasc Interv 2011;4:26-37

ABI during the randomized-start phase and until 6 months follow-up (open-label phase).
Walter D H et al. Circ Cardiovasc Interv 2011;4:26-37
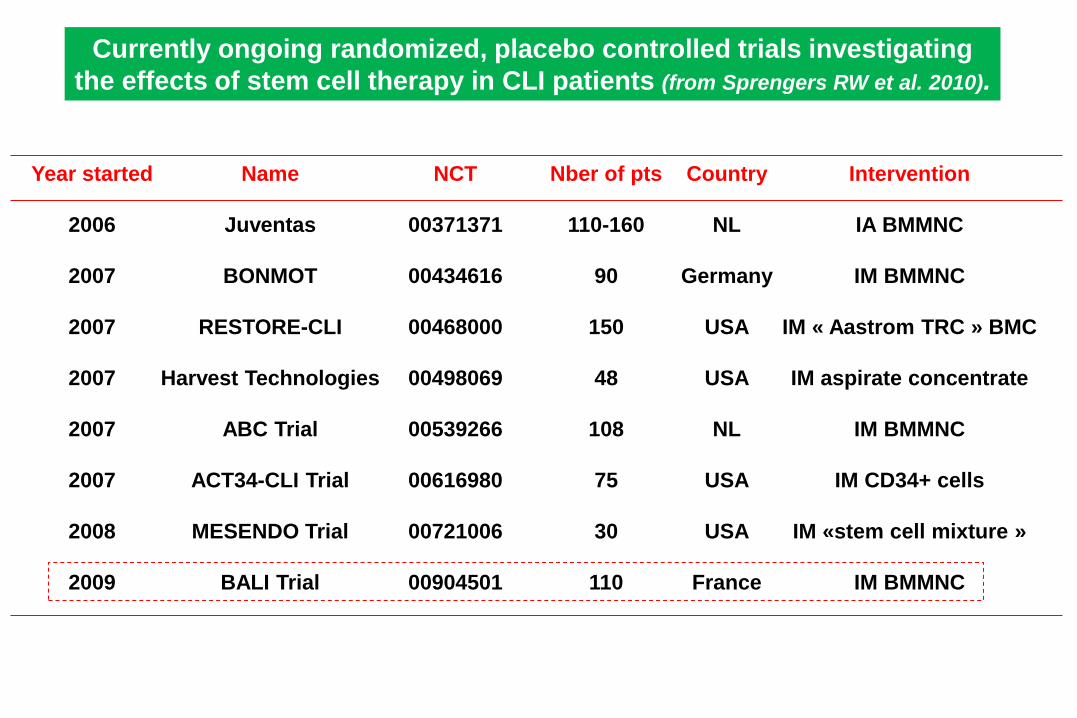
Currently ongoing randomized, placebo controlled trials investigating
the effects of stem cell therapy in CLI patients (from Sprengers RW et al. 2010).
Year started
2006
2007
2007
2007
2007
2007
2008
2009
Name
Juventas
BONMOT
RESTORE-CLI
Harvest Technologies
ABC Trial
ACT34-CLI Trial
MESENDO Trial
BALI Trial
NCT
00371371
00434616
00468000
00498069
00539266
00616980
00721006
00904501
Nber of pts
110-160
90
150
48
108
75
30
110
Country
NL
Germany
USA
USA
NL
USA
USA
France
Intervention
IA BMMNC
IM BMMNC
IM « Aastrom TRC » BMC
IM aspirate concentrate
IM BMMNC
IM CD34+ cells
IM «stem cell mixture »
IM BMMNC

OPTIPEC trial
« Optimisation d'un produit de thérapie
cellulaire autologue par cellules mononucléées
médullaires dans l’ischémie critique des membres
inférieurs liée à l’athérosclérose. »
Promoter : AP-HP (PHRC national 2003 - AOM 03 034)
CCPPRB de Paris-Broussais-HEGP : 3/12/2004
Inserm

No side effects within 30 days after the treatment.
No side effects in the follow-up due to the teatment :
- 1 sudden death
- 1 GI K
No retinal side effect
50% clinical improvement ; ulcer healing or minor amputation
healing.
4 major amputations in 15 treated patients.

All the amputation specimens were submitted to a standardized
dissection protocol.
When the limb was amputated below the knee, a large sample of gastrocnemius
was sampled, around the site of cell injection and along the tibial arteries.
The forefoot tissues and arteries (plantar and toe arteries) were also sampled in
each case.
Between 15 and 20 paraffin blocks were prepared in each case and were stained
with hematoxylin and eosin (H&E).
Immunihistochemistry :
Tissue sampling
- anti-CD31, anti-CD34, and anti-von Willebrand factor : endothelial cell markers
- anti-podoplanin : lymphatic endothelial cell marker
- anti-a-smooth muscle actin : vascular smooth muscle cell marker
- anti-Ki67 antibody : proliferation cell marker
- anti-CD117 (c-kit) : precursor endothelial cell marker
- anti-Glut-1 : endothelial cells of some angiomas and angiosarcomas.

Modern Pathology, 2008

Inserm
Modern Pathology, 2008

Inserm
Modern Pathology, 2008

Magnitude of incorporation of bone-marrow derived cells into
vasculature varies : 50% to occasional cells.
Other mechanisms apart from cell incorporation contribute to
collateral remodeling observed after BM cell therapy in various
models of ischemia.
Numerous arteriogenic cytokines are released by marrow stromal
cells.
Local delivery of marrow-derived stromal cells augments collateral perfusion
through paracrine mechanisms. Kinnaird T, et al. Circulation, 2004.
Marrow-derived stromal cells express genes encoding a broad spectrum of
arteriogenic cytokines and promote in vitro and in vivo arteriogenesis through
paracrine mechanisms. Kinnaird T, et al. Circ Res 2004
Bone marrow-derived progenitor cells can improve tissue ischemia
at least in part through paracrine mechanisms.

Perivascular
incorporation
Differentiation
to an endothelial
phenotype
Production of
paracrine factors
Improvement of neovascularization
Inserm

Progenitor endothelial cells

endothelial cell
Inserm

From Aranguren et al. J Mol Med 2009

Late EPC culture from cord blood
Day 0
Cord blood
mononuclear cells
adhesion
colonies
Day 1 Day 7/14
CD34+ isolation
Day 18 Day 25 Day 48 …
Expansion
In EGM-2 medium during
5 weeks
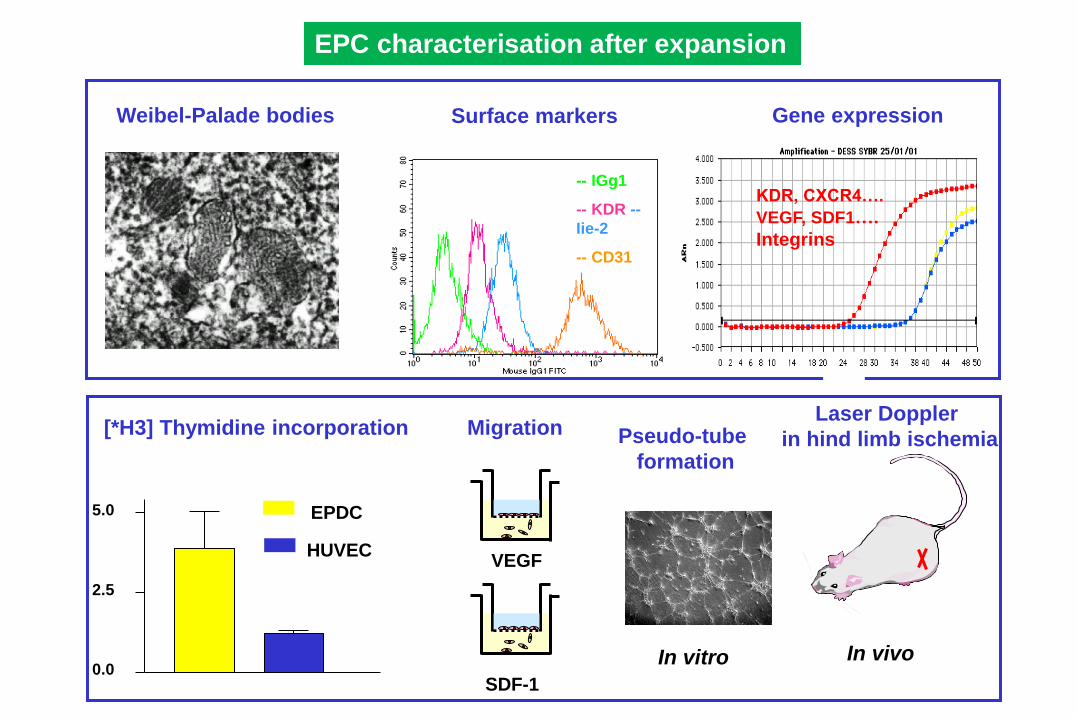
EPC characterisation after expansion
Weibel-Palade bodies
-- IGg1
-- KDR --
Iie-2
-- CD31
Surface markers Gene expression
KDR, CXCR4….
VEGF, SDF1….
Integrins
0.0
2.5
5.0 EPDC
HUVEC
[*H3] Thymidine incorporation
VEGF
SDF-1
Migration Pseudo-tube
formation
In vitro In vivo
Laser Doppler
in hind limb ischemia

Early EPC Late EPC
• Circulating angiogenic cells (CAC)
• CFU-Hill
• Culture modified mononuclear
cells (CMMC)
• Endothelial colonies forming
cells (ECFC)
• Endothelial progenitor derived
cells (EPDC)
• Outgrowth endothelial cells (OECs)
• Blood outgrowth endothelial cells (BOECs)
• LPP-HPP endothelial cells
• Appear in culture after 4-7 days
• Monocytic and endothelial cell markers
• High levels of growth factors secretion
• Appear in culture after 7-20 days
• Cobblestone appearance
• Endothelial cell markers
• High proliferative potential

Early EPC Late EPC
KDR, VE-Cadherin,
VWF, Flt-1, CD14+, CD45+
Positive
No
VEGF, SDF-1, IL-8, HGF
Low
No
Cathepsin L
Good
KDR, VE-Cadherin,
VWF, Flt-1, CD14-, CD45-
Positive
Yes
Low
High
Yes
u-PA
Good
Inserm
Surface Ag expression
AcLDL and lectin binding
Tube formation
Cytokines secretion
NO production
BMP 2/4
Proteolytic capacity
Angiogenic potential

Inserm

The 2 types of EPCs showed comparable angiogenic potentials when each
type was transplanted alone.
Early EPCs may contribute to neovascularization by secretion of cytokines
and MMP-9,
whereas OECs participate by providing building blocks and secreting MMP-2.
Improved perfusion to the ischemic limb and subsequent improved limb salvage
in mice receiving mixed EPC transplantation through cross-talk between
2 types of EPCs, with a synergistic effect.
Synergistic neovascularization by mixed transplantation of early
endothelial progenitor cells and late outgrowth endothelial cells.
The role of angiogenic cytokines and matrix metalloproteinases.
Yoon CH, et al. Circulation 2005;112:1618-27.
Inserm

Inserm
Pleiotropic role of PAR-1 stimulation on EPCs
SFLLRN SFLLRN SFLLRN
Pseudotube
formation Migration Proliferation Inflammatory cells
recruitment
Smadja et al. J Thromb Haemost 2006.
Smadja et al. J Cell Mol Med 2007.
Smadja et al. J Cell Mol Med 2008.
Smadja et al. J Cell Mol Med 2009.
Stimulation of EPCs by PAR-1 activation does not influence significantly
VEGF/VEGFR2 pathway.

BMPs increase late EPC proangiogenic potential
Hindlimb ischemia (nude mice)
Late EPC Late EPC-
pretreated with BMP4
Late EPC-
pretreated with BMP2
Smadja et al, 2008, ATVB
Expression of BMP 2/4 characterized late EPC compared to early EPC

Newly Formed vessels after BM-MNC injection in CLI
are positive for BMP
CD34 vWF
CD45 a-SMA
Ki-67 BMP2/4
Smadja et al, 2008, ATVB
Newly Formed
vessels
originate from
LATE EPC
LINEAGE

CD34
Tie-2
CD34 Commitment Expansion
VEGF, Angiopoïétin-1 BMP 2/4
VEGF, Angiopoïétin-2 BMP 2/4, SDF-1, Thrombin, E-selectin, Fc-ephrin B2…
VEGFR2

mouse embryonic cell line
10T1/2
served as the perivascular
component of the vascular
networks
Vessel density with adult PB-EPC
Vessel density with adult PB-EPC

Autologuous cells
Expansion Transfection (Oct3/4, Sox2, Klf4, c-Myc)
iPS
Embryonic stem cells
Late EPC
ECFC
Ethical and immunological
problems
?
Endo-iPS Endo-
ES
Very rare cells in
peripheral adult
blood of pts with CLI
and low angiogenic
property ?

Mobilisation of progenitor cells in-vivo
GM-CSF
G-CSF
VEGF
SDF-1
EPO
Angiopoietin-1
Statins
Exercise
Estrogen
(PPARg agonists)
Eff
icie
ncy
Infl
am
mati
on
From Aicher A. et al. Hypertension 2005;45:1-5 Inserm

START Trial. A pilot study on Stimulation of ARTeriogenesis
susingsubcutaneousapplication of GM-CSF as a new treatment of PAD
Van Royen N et al. Circulation 2005;112:1040-46
A double-blinded, randomized, placebo-controlled study was performed in 40 patients with
moderate or severe intermittent claudication
Placebo or subcutaneously applied GM-CSF (10 mg/kg) for a period of 14 days (total of 7 injections)
PWT day 14 PWT day 90

START Trial. A pilot study on Stimulation of ARTeriogenesis
susingsubcutaneousapplication of GM-CSF as a new treatment of PAD
Van Royen N et al. Circulation 2005;112:1040-46
Stem cell mobilization induced by granulocyte colony-stimulating factor to
Improve cardiac regeneration after acute ST-elevation MI.
STEMMI trial
Ripa RS et al. Circulation 2006;113:1983-92
Stem cell mobilization by G-CSF therapy in patients with acute
myocardial infarction and successful mechanical reperfusion has no
influence on infarct size, left ventricular function, or coronary restenosis.
Stem cell mobilization by granulocyte colony-stimulating factor in
patients with acute myocardial infarction: a randomized controlled trial.
Zohlnhofer D et al. JAMA 2006;295:1058-60 (REVIVAL-2)
Inserm

Iwaguro H, Yamaguchi J, Kalka C, et al. Endothelial progenitor cell
vascular endothelial growth factor gene transfer for vascular regeneration.
Circulation. 2002;105:732–738.
VEGF
Murasawa S, Llevadot J, Silver M, et al. Constitutive human telomerase
reverse transcriptase expression enhances regenerative properties of
Endothelial progenitor cells. Circulation. 2002;106:1133–1139.
Telomerase
Kong D, et al. Enhanced inhibition of neointimal hyperplasia by genetically
Engineered EPCs. Circulation 2004;109:1769-75.
eNOS.
Combination of gene and cell therapy ?
Inserm

Potential side effects of the stimulation of angiogenesis

Heistad, D. D. N Engl J Med 2003;349:2285-2287
Intraplaque hemorrhage and progression of coronary atherosclerosis. Kolodgie FD et al. N Engl J Med 2003;349:2316-25

Increase risk of cancer on the long term
by promoting the angiogenic switch

Cancer without disease. Do inhibitors of blood-vessel growth found naturally in our bodies defend most
of us against progression of cancer to a lethal stage ?
Judah Folkman and Raghu Kalluri. Nature 2004;427:787.
Systematic autopies after traumatic deaths:
- Women 40-50 y.o.: 30% in situ breast K, but only 1%
of breast cancer diagnosed at this age.
- Similar pattern for men concerning prostate K.
- Between 50 and 70 years , in situ thyroid K in almost 100%
of subjects, but incidence of clinical cancer in only 0.1%.
Two critical steps in cancerogenesis:
1. Cell mutations due to genetic instability that will trigger cell
transformation (stable if cell divisions compensated by cell deaths)
2. Angiogenic switch, converts in-situ tumors that are non-fatal to
grow up and generates metastasis.
(In trisomia 21, few solid tumors due to elevated levels of endostatin
and conversely increase rate of K prostate associated with endostatin SNPs)

Another approach of
cell therapy in CLI

Fibroblast cells, which form the
structural backbone of blood
vessels, are extracted from a
small dermal biopsy (the size of
a postage stamp) and
expanded in culture. Part of
Cytograft’s core technology
includes techniques to grow
these cells into robust sheets
that can be manipulated into
three-dimensional structures.
Cytograft is currently applying
this technology to create the
world's first clinically available
completely autologous tissue
engineered vascular grafts:
Lifeline™

Tissue-Engineered Blood Vessel for Adult Arterial Revascularization.
L’Heureux N, Mac Allister T. N Engl J Med 2007;356:1451-2

From Kumar & Caplice, ATVB 2010
Emerging and future clinical trials of adult vascular progenitor therapy.

Need for new treatment of PAD (CLI)
Clinical need High
Comorbidity High
Patients homogenicity Low
Endpoints Pain
Ulcer healing
Gangrene
Limb loss
Death
Effective therapy Revascularisation (if possible)
Inserm

1) Which patient population should be considered for stem cell
or gene-therapy ?
2) What type of stem cell / gene therapy should be used ?
3) What is the best route for cell / gene delivery ?
4) What is the optimum number of cells / plasmid that should be
used to achieve functional effects ?
5) Is stem cell / gene therapy safer and more effective than
conventional therapies ?
Inserm

INSERM U765 : David Smadja
Pascale Gaussem
Anne-Marie Fischer
Catherine Boisson-Vidal
Blandine Dizier
Gabrielle Sarlon
Isabelle Martinez
Saul Azouelos
Laetitia Mauge
Clément d’Audigier
Centre de Thérapie Cellulaire
de Necker : M. Cavazzana-Calvo
L. Dal Cortivo
F. Lefrère
Inserm
« Nutrisco et extinguo »
François 1er’ motto

What is the relationship between the war
in Iraq and regenerative limb medicine ?


Do you believe in miracles ?
Durand (1997) Fra Angelico (1440)
Deacon Justinian’s recovery.
by transplantation of a black’s leg by St Côme and St Damien)


Clinical Application Cell and Source
Therapeutic application and source of adult vascular progenitor cells
used in clinical trials.
From Kumar & Caplice, ATVB 2010

http://www.cbsnews.com/stories/2008/03/22/sunday/main3960219.shtml