treatment of an intrabony defect combined
TRANSCRIPT

Treatment of an intrabony defect combined
with an endodontic lesion: a case report
Geetha Ari, Anil Kumar K, Thyagarajan Ramakrishnan
ENDO (Lond Engl) 2010;4(3):215–222
DR.AMITHBABU.C.BM.Sc.D-ENDO

Introduction
• Periodontal therapy is mainly aimed at removal of local factors, which leads to resolution of inflammation in the supporting structures of the tooth.• This therapy predominantly involves scaling and
root planing as the main therapy, combined with hard and soft tissue surgery. • With proper postoperative maintenance care,
resolution of inflammation occurs, leading to arrest of disease progression

• Combined periodontal–endodontic therapy is widely used because of the close proximity of the pulp and periodontal structures and their mutual involvement in disease. • The prognosis of the combined periodontal–
endodontic diseases depends upon the severity of the periodontal disease and the response of the perio dontal treatment.• Yamasaki et al4 have reported that periradicular
lesions may initially expand horizontally through cancellous bone and then proceed vertically

• The periodontal–endodontic lesion is used to describe lesions due to inflammatory products found in varying degrees in both the periodontium and the pulpal tissues.• Platelet-rich plasma (PRP) has become a valuable
adjunct in wound healing in dentistry. • Post-surgically, blood clots initiate the healing
and regeneration of hard and soft tissues. • PRP is a platelet concentrate that has been used
widely to accelerate soft and hard tissue healing.

• Platelet-rich fibrin (PRF) belongs to a new generation of platelet concentrates, with simplified processing and without biochemical blood sampling. • The use of platelet gel to improve bone
regeneration is a recent technique in implantology and periodontology.• PRF was first developed in France by Choukroun
et al5 for specific use in oral and maxillofacial surgery.
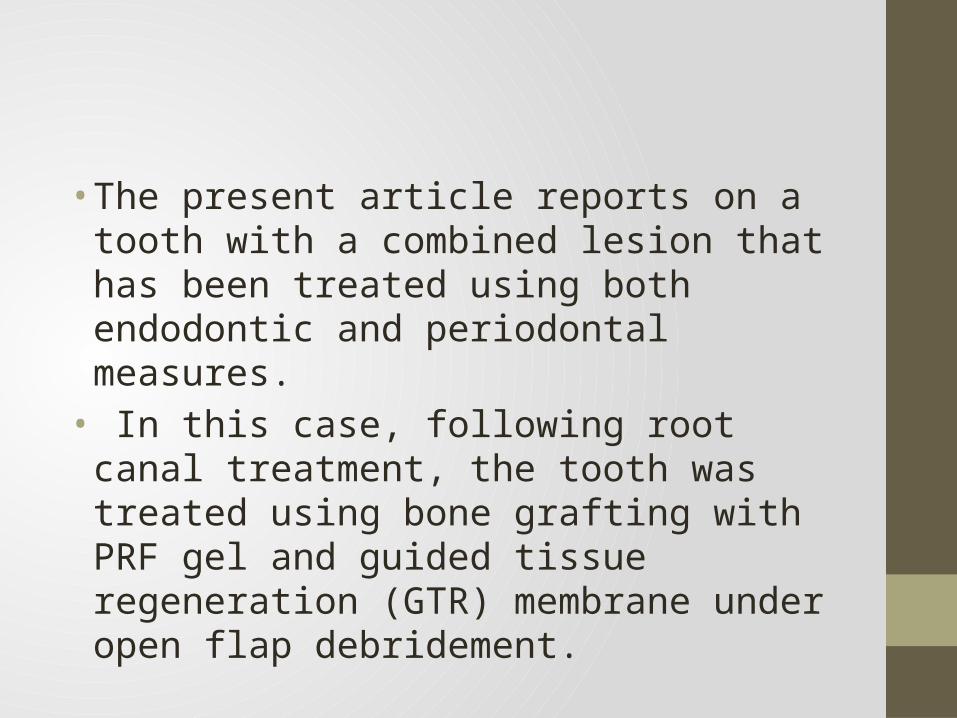
• The present article reports on a tooth with a combined lesion that has been treated using both endodontic and periodontal measures.• In this case, following root canal treatment, the
tooth was treated using bone grafting with PRF gel and guided tissue regeneration (GTR) membrane under open flap debridement.

CASE REPORT
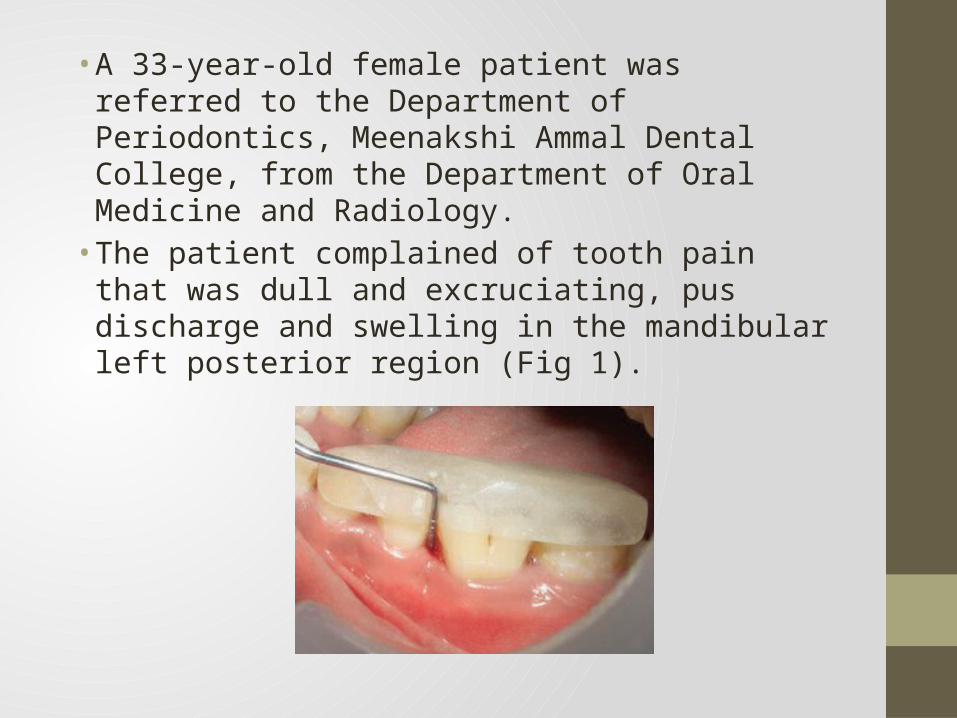
• A 33-year-old female patient was referred to the Department of Periodontics, Meenakshi Ammal Dental College, from the Department of Oral Medicine and Radiology. • The patient complained of tooth pain that was
dull and excruciating, pus discharge and swelling in the mandibular left posterior region (Fig 1).

• On examination, inflammation of the attached gingiva and pain on percussion were present. • An abnormal painful response to percussion on
tooth 36 indicated that inflammation of the periodontal ligament could be of pulpal or periodontal origin. • The tooth showed attrition and presented with
plaque and calculus.• Pulp sensitivity testing was performed using hot
and cold and the results were confirmed using a pulse oximeter8, which indicated no response, hence the pulp of tooth 36 swas considered to be non-vital.

• Periodontal probing revealed a pocket depth of 8 mm and clinical attachment loss of 10 mm in relation to tooth 36. There were no other periodontally involved teeth in the remaining dentition. • Radiographic examination demonstrated severe
bone loss around the mesial aspect of tooth 36 (Fig 2).

• The initial phase of treatment included complete scaling and root planing. • After drainage of the abscess, antibiotics (amoxicillin
500 mg, 3 times a day for 5 days) and analgesics (ibuprofen 400 mg, 3 times a day for 3 days) were prescribed. • The patient was referred to the Department of
Endodontics for root canal treatment of tooth 36.• After 3 months, the patient was recalled and surgical
treatment was planned for the treatment of the intrabony defect with bone graft, PRF and GTR membrane.

Presurgical therapy• The initial phase of treatment included complete
scaling and root planing. • Periodontal parameters (probing depth, mobility and
radiographic evidence of bone loss) were assessed before and after surgery.

Management• Root canal therapy• The first step in the treatment plan after phase 1therapy
was to deal with the endodontic procedure
Working length Master cone
obturation
3 months Follow up

Periodontal therapy• After 3 months, the patient was recalled for management
of the intrabony defect.• After proper isolation of the surgical field, the operative
sites were anaesthetised using 2% xylocaine hydrochloride with adrenaline (1:200000).• Crevicular incisions were made using a Bard–Parker
No.15 blade (BD, Franklin Lakes, NJ, USA) on the facial and lingual surfaces of each tooth, with segment or area involved.• A full-thickness mucoperiosteal flap was reflected using a
periosteal elevator, taking care to preserve the maximum amount of gingival connective tissue in the flap.

• The defect was thoroughly debrided and the root surface was then planed and the flap trimmed to remove granulation tissue tags and minimise bleeding (Figs 7 and 8).• This was followed by irrigation with Betadine®
(Purdue Products, Stamford, CT, USA) and sterile saline solution.

PRF preparation
• The advantages of PRF over PRP are its simplified preparation and lack of biochemical handling of the blood. • A blood sample of the patient was drawn in 10
mL test tubes without an anticoagulant and centrifuged immediately. • Blood was centrifuged using a tabletop
centrifuge (REMY Laboratories, Chennai, Tamilnadu, India) for 12 min at 2500 rpm.
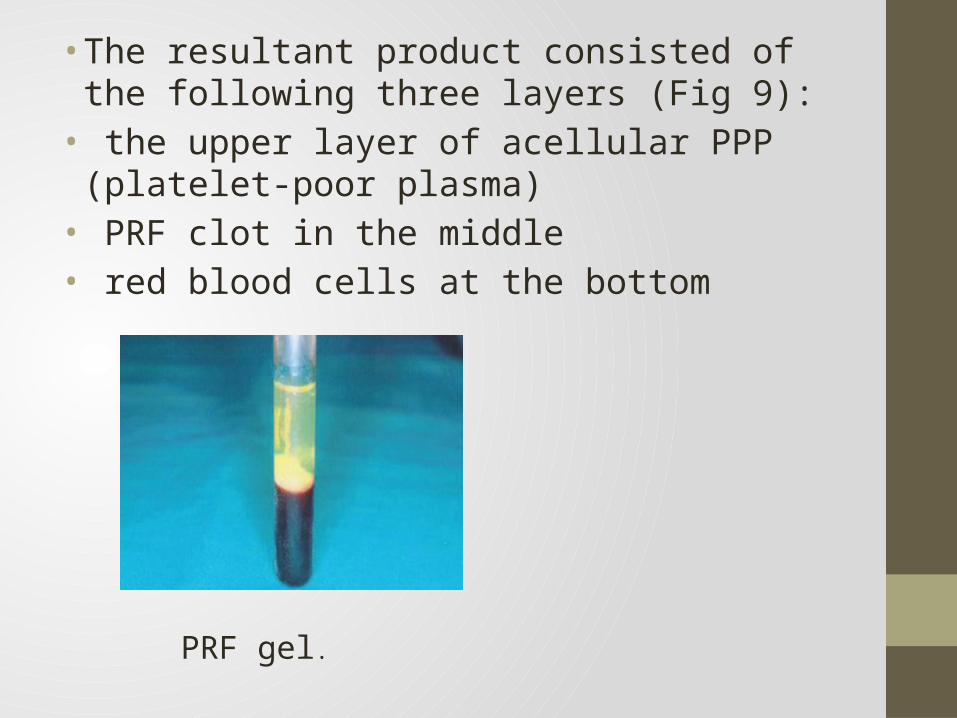
• The resultant product consisted of the following three layers (Fig 9):• the upper layer of acellular PPP (platelet-poor
plasma)• PRF clot in the middle• red blood cells at the bottom
PRF gel.

• Because of the absence of an anticoagulant, blood begins to coagulate as soon as it comes in contact with the glass surface. • Therefore, for successful preparation of PRF,
speedy blood collection and immediate centrifugation, before the clotting cascade is initiated, is absolutely essential. • PRF can be obtained in the form of a membrane
by squeezing out the fluids in the fibrin clot.
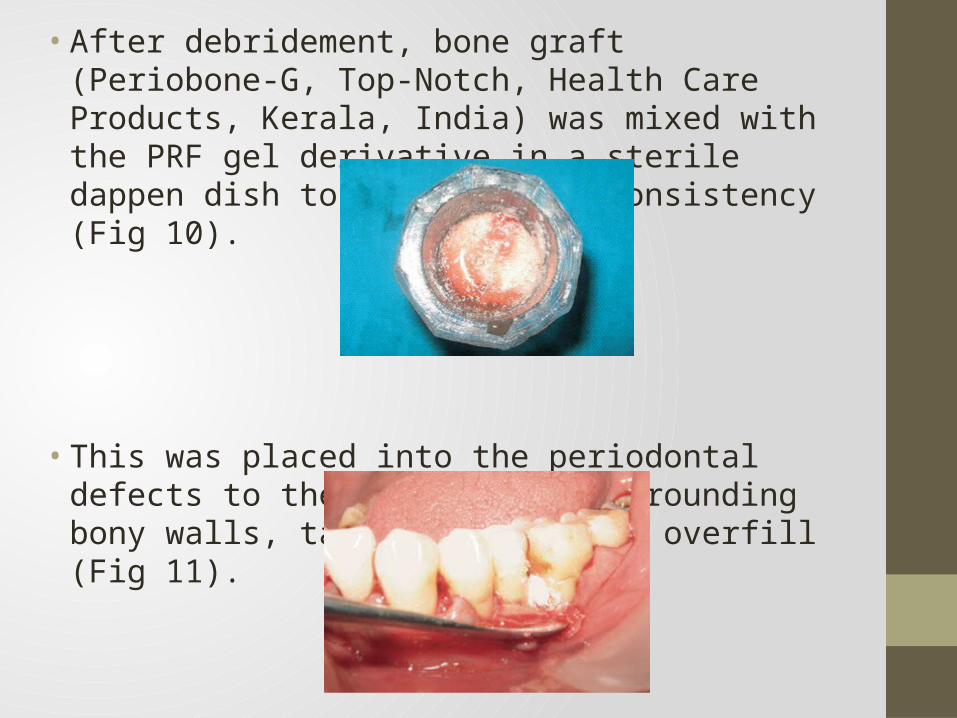
• After debridement, bone graft (Periobone-G, Top-Notch, Health Care Products, Kerala, India) was mixed with the PRF gel derivative in a sterile dappen dish to a paste-like consistency (Fig 10).
• This was placed into the periodontal defects to the level of thesurrounding bony walls, taking care not to overfill (Fig 11).

• It has been suggested that under-filling or overfilling may be counter productive because it may preclude proper flap closure, thereby retarding healing and possibly resulting in loss of the graft material. • This was followed by placement of a GTR
membrane over the defect (Fig 12).

• The mucoperiosteal flap was replaced and primary wound closure was achieved by means of black silk 4-0 sutures (Fig 13) and Coe-PakTM (GC America, Alsip, IL, USA) was placed (Fig 14).• After a period of 7 to 10 days the sutures were
removed.
Placement of sutures. Placement of Coe-Pak

Post operative care• Following surgery, the patient was instructed to avoid
chewing in the surgical area during the first post operative day.• Systemic antibiotics (amoxicillin 500 mg, 3 times a
day for 5 days) and analgesics (ibuprofen 400 mg, 3 times a day for 3 days) were prescribed.
• After 10 days, the sutures were removed and healing was found to be adequate. • Re-evaluation of the patient after 9 and 12 months
revealed satisfactory bone fill and complete soft tissue healing.
Healing

• Periapical radiographs taken at the 9- and 12-month follow up appointments indicated radiographic bone fill in relation to tooth 36 and healing of the periapical lesion (Fig 15). • The probing depth reduced from 8 mm to 3 mm
(Fig 16).
Twelve-month follow-up radiographTwelve-month post-operative view showing reducedpocket depth

Discussion• Periodontal–endodontic lesions develop by either
periodontal destruction combining apically with an existing periapical lesion, or an endodontic lesion combining with an existing periodontal lesion. • It has long been recognised that an intimate
relationship exists between the pulp of a tooth and its surrounding periodontium. • Seltzer et al12 concluded that an established
endodontic lesion could progress through the main or accessory canals to produce periodontal breakdown.

• The regeneration of a new attachment apparatus is one of the most challenging aspects of periodontal therapy. • Periodontal regeneration is now understood in the
treatment of many periodontal defects, and is at the forefront of periodontal research.• The goal is to regenerate the components of the
periodontium that have been lost through periodontitis. The use of bone grafts and bone substitutes, guided tissue regeneration and, more recently, the application of polypeptide growth factors to the surgical wound are some commonly used techniques to promote periodontal regeneration.
• The case presented was more amenable to regenerative therapy than root resection as there was complete bone support on the buccal side when the flap was raised.• Clinically, the tooth showed no mobility. Anderegg
et al18 showed that the vertical component of the defect can predict the extent of osseous repair following regenerative surgery.• Although the vertical component in this case was
extensive, the lack of mobility and the presence of good bone support on the buccal side were factors that favoured the use of regenerative procedures instead of root resection.

• Diagnosis of primary endodontic disease and primary periodontal disease usually presents no clinical difficulty. • In primary endodontic disease the pulp is
infected and non-vital. • In primary periodontal disease the pulp is vital
and responds to sensitivity testing.• Treatment results should be evaluated in 2 to 3
months and only then should periodontal treatment be considered.

• Within the limit of the present report, a combination of bone graft with PRF gel and GTR led to a favourable clinical improvement in periodontal intrabony defects. • Further studies are necessary to assess the long-
term effectiveness of this combined therapy in the treatment of intrabony defects.

THANK YOU