treatment of hyperuricemia in gout: current therapeutic options,...
TRANSCRIPT

Ther Adv Musculoskel Dis
2016, Vol. 8(4) 145 –159
DOI: 10.1177/ 1759720X16646703
© The Author(s), 2016. Reprints and permissions: http://www.sagepub.co.uk/journalsPermissions.nav
Therapeutic Advances in Musculoskeletal Disease
http://tab.sagepub.com 145
IntroductionGout is the most common type of inflammatory arthritis in adults in the United States [Lawrence et al. 2008; Zhu et al. 2011]. In the UK, gout has an incidence of approximately 2.68 per 1000 per-son-years and increases significantly with age [Cea Soriano et al. 2011]. Besides its significant frequency, gout has also been associated with poor quality of life and increased healthcare utili-zation. In addition, poor gout management can result in recurrent hospital admissions and disa-bility [Singh and Strand, 2008; Becker et al. 2009; Hutton et al. 2009; Garg et al. 2013]. Despite this, management of gout is usually overlooked or suboptimal because of different barriers, which include patient and physician misbeliefs, along with lack of knowledge about guideline and evi-dence-based gout management [Doherty et al. 2012; Spencer et al. 2012].
Hyperuricemia, defined as a serum urate (SU) concentration higher or equal to 6.8 mg/dl (0.408
mmol/l), is the biochemical abnormality underly-ing the development of gout. Hyperuricemia usu-ally occurs due to overproduction or under excretion of urate, the latter being causative of hyperuricemia in 90% of gout patients [Choi et al. 2005]. The risk of developing gout is strongly associated with the degree of hyperuricemia [Campion et al. 1987]. However, hyperuricemia is not a sufficient causative factor for the develop-ment of gout, as demonstrated by multiple stud-ies including the 2007–2008 National Health and Nutrition Examination Survey in the US in which the prevalence of hyperuricemia was 21%, com-pared with a gout prevalence of only 3.9% [Zhu et al. 2011].
Because of the established association between hyperuricemia, gout development, and the effec-tiveness of SU reduction in its chronic manage-ment, urate-lowering therapy (ULT) represents the main pillar in the chronic management of gout. An insufficient amount of ULT agents has
Treatment of hyperuricemia in gout: current therapeutic options, latest developments and clinical implicationsSebastian E. Sattui and Angelo L. Gaffo
Abstract: Despite being the most common type of inflammatory arthritis, gout is often poorly managed. Except for febuxostat and pegloticase, research in new therapeutic agents for the management of hyperuricemia in gout remained insufficient for several decades. With emerging evidence of possible roles of hyperuricemia in cardiometabolic comorbidities, as well as more convincing evidence regarding poor outcomes (e.g. disability, recurrent hospital admissions) in patients with uncontrolled gout, several agents are current under development. Increasing knowledge regarding renal urate transporters has resulted in the development of new generation uricosurics such as lesinurad and arhalofenate. This review aims at discussing current therapeutic strategies for gout, as well as their limitations and the possible role of emerging agents in the chronic management of hyperuricemia in gout. Drugs in phases I and II of development will be discussed, along with new agents and therapeutic classes, such as purine nucleoside phosphorylase inhibitors and dual-action drugs. These new developments are encouraging, and will hopefully contribute to a more adequate management of hyperuricemia in gout.
Keywords: arhalofenate, gout, hyperuricemia, lesinurad, ulodesine, URAT1, urate-lowering therapy
Correspondence to: Angelo L. Gaffo, MD, MsPH University of Alabama, School of Medicine, Division of Clinical Immunology and Rheumatology, Department of Medicine, Shelby Building 201, 1825 University Boulevard, Birmingham, AL 35294, USA [email protected]
Sebastian E Sattui, MD Tinsley Harrison Internal Medicine Residency Program, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
646703 TAB0010.1177/1759720X16646703Therapeutic Advances in Musculoskeletal DiseaseSE Sattui and AL Gafforesearch-article2016
Review

Therapeutic Advances in Musculoskeletal Disease 8(4)
146 http://tab.sagepub.com
led to many decades of unmet needs in the treat-ment of hyperuricemia of gout. Besides, emerging evidence about an association between hyper-uricemia with cardiovascular and metabolic comorbidities has raised further interest in the development of the novel ULTs [Kim et al. 2009, 2010; Grayson et al. 2011].
This review will provide an overview of current practice and agents available for ULT in gout as well as data on new agents currently in the devel-opment pipeline in different clinical trial phases, including the recently FDA-approved lesinurad. Repercussion of current therapies on other medi-cal comorbidities will also be discussed.
Current treatment for hyperuricemia in gout
General principlesBased on 2012 American College of Rheumatology (ACR) guidelines, ULT is recommended in the established diagnosis of gout with two or more acute gout attacks per year, presence of tophi, chronic kidney disease (CKD) stage 2 or more, or presence of renal stones [Khanna et al. 2012]. These are consistent with recommendations from other guidelines. SU goal is less than 6 mg/dl (0.36 mmol/l), based on ACR and European League Against Rheumatism (EULAR) recommendations, in comparison to a lower target of less than 5 mg/dl (0.3 mmol/l) recommended by the British Society
for Rheumatology (BSR) [Zhang et al. 2006; Jordan et al. 2007; Khanna et al. 2012]. The goal of less than 5 mg/dl is supported by ACR and EULAR in severe cases of gout, defined as patients with tophi, chronic arthropathy, or frequent attacks.
Xanthine oxidase inhibitors (XOIs) still remain the first line of treatment as recommended by all guidelines. Among these, allopurinol is the first-line agent in all but the ACR guidelines, which recommend allopurinol or febuxostat inter-changeably. Uricosurics are still second-line or alternative agents, and all recent guidelines also support the combination of agents (e.g. XOIs and uricosurics) when monotherapy is not effective [Zhang et al. 2006; Khanna et al. 2012]. Benefits of management of asymptomatic hyperuricemia are still unclear, but the Japanese guidelines do recommend treatment in nongout patients with SU above 8 mg/dl (0.44 mmol/l) under the con-cern of increased risk of development of gout or development of other comorbidities such as CKD [Yamanaka, 2011].
XOIsXOIs are the oldest agents, and still first-line for the treatment of hyperuricemia in gout (see Figure 1). Allopurinol and febuxostat are the two agents available in this category; the former being still the more established and commonly used medication for ULT.
Figure 1. Uric acid pathway and action site of urate-lowering therapies. *Drugs in italics are agents still under development or still not approved. **Dashed arrow representing lack of metabolic step in humans, due to evolutionary loss of uricase enzyme.PNP, purine nucleoside phosphorylase; XO, xanthine oxidase.

SE Sattui and AL Gaffo
http://tab.sagepub.com 147
AllopurinolAllopurinol remains as first-line agent for ULT due to its efficacy, availability, and low cost. It is a nonspecific competitive XOI that is later converted to oxypurinol for its renal excretion. Starting dose, as recommended by ACR guidelines, is usually 100 mg with slow-up titration of the dose every 2–4 weeks until target SU is achieved [Khanna et al. 2012]. Doses up to 800 mg/day are approved in the US, in comparison with up to 900 mg/day in Europe [Jordan et al. 2007].
Despite the wide availability of allopurinol, target SU concentrations are not always achieved due to multiple factors, including failure to monitor SU, low adherence to medication, and inade-quate dosing [Horsburgh et al. 2014; Stamp et al. 2014]. A study that randomized patients to fixed doses of 100 and 300 mg of daily allopurinol based on renal function, showed that only 39–41% achieved a target SU of 6 mg/dl [Schumacher et al. 2008]. Another trial that titrated allopurinol up to 300 daily mg showed that only 56% of patients reached a target SU of 6 mg/dl [Reinders et al. 2009].
Inadequate up-titration and dosing is partly influ-enced by lack of knowledge by physicians, but to some extent by the concern of possible side effects. Besides gastrointestinal side effects, the main concern is development of rashes, Steven–Johnson’s syndrome, and allopurinol hypersensi-tivity syndrome (AHS) [Arellano and Sacristan, 1993]. AHS is a rare side effect that carries a mor-tality rate of approximately 27% and is more common in individuals of Thai or Han Chinese descent who carry the HLA-B*5801 haplotype [Hung et al. 2005; Ryu et al. 2013; Yun et al. 2014]. Under the concern that high allopurinol doses increased the risk of AHS, allopurinol titra-tion was guided by dosing recommendations given by Hande and colleagues [Hande et al. 1984] Recent evidence however, has showed that risk of AHS is mostly related to allopurinol start-ing dose rather than the maintenance dose [Stamp et al. 2012]. In this case-control study, those who developed AHS were more likely to be started on a higher than creatinine clearance-based allopurinol dose, Odds Ratio (OR) 16.7 (95% CI 5.7–47.6). Moreover, in patients who tolerated allopurinol initiation uneventfully, no association between AHS risk and allopurinol maintenance dose was observed. Safety and efficacy of allopu-rinol dose escalation in combination with educa-tion and lifestyle advice was subsequently proved
in a trial of 106 participants in which 92% of participants reached a SU target of 6 mg/dl [Rees et al. 2013]. Allopurinol starting dosing needs to be adjusted in CKD patients. Despite previous concerns about the risk of AHS in this popula-tion, a recent investigation has described effective and safe up-titration of allopurinol with 88% of patients reaching a goal SU of 6 mg/dl and no events of AHS [Stamp et al. 2011].
FebuxostatFebuxostat is a nonpurine-specific XOI that is primarily metabolized in the liver. It is currently approved in the US at doses of 40–80 mg/day and up to 120mg/day in Europe. In a 52-week phase III trial that compared febuxostat 80 and 120 mg to allopurinol 300 mg in 762 patients with esti-mated glomerular filtration rate (eGFR) > 50 ml/min, 53%, 62%, and 21%, respectively, achieved a SU of 6 mg/dl [Becker et al. 2005a]. Another large phase III trial compared febuxostat 80, 120, and 240 mg to fixed doses of allopurinol, 300 and 100 mg based on renal function, in patients with normal and impaired renal function [Schumacher et al. 2008]. Among patients with normal kidney function, the primary end point of SU less than 6 mg/dl was achieved in 48%, 65% and 69% of the 80, 120 and 240 mg of febuxostat compared to only 22% in the allopurinol arm. Results were similar in the groups with renal impairment. An important observation for all studies comparing febuxostat with allopurinol, and claiming a higher potency for febuxostat, is that allopurinol com-parator doses are fixed and not titrated as recom-mended in most practice guidelines. This places allopurinol at a relative disadvantage, and should call for a word of caution about simplistic state-ments of comparative efficacy.
Diarrhea, nausea and elevation of liver enzymes are the most common side effects reported for febuxostat [Becker et al. 2005a, 2005b; Schumacher et al. 2008]. Also, increased gout flare rates have been reported with higher febux-ostat doses when compared to allopurinol [Becker et al. 2005]. This was, nevertheless, expected as rapid and pronounced reductions in SU are known to commonly induce flares. A nonstatisti-cally significant increase in the frequency of car-diovascular events in the febuxostat arms of a subsequent clinical trial was noted. This is of unclear clinical relevance and is currently care-fully followed in postmarketing analyses [Becker et al. 2010; White et al. 2012]. It would be

Therapeutic Advances in Musculoskeletal Disease 8(4)
148 http://tab.sagepub.com
expected that any cardioprotective effect of allopurinol mediated by reduction in oxidative stress should also be observed with febuxostat [De Abajo et al. 2015; Grimaldi-Bensouda et al. 2015; MacIsaac et al. 2016] Although an adverse cardiovascular profile for febuxostat is far from confirmed, the clinical concern for this has led to the development of a comparative cardiovascular outcomes trial [MacDonald et al. 2014].
Cost remains the biggest limitation in febuxostat use; a reason why cost-analysis studies describe it as a second option after allopurinol has shown to be ineffective, not tolerated or contraindicated [Beard et al. 2014; Jutkowitz et al. 2014].
UricosuricsUricosurics are the second class of ULT currently available, which act by increasing renal urate excre-tion (see Figure 1). This is mediated by selective inhibition of organic anion transporters (OATs) present in the proximal tubular cells (see Figure 2). All uricosurics carry with them the increased risk of precipitation of urate stones; a reason why under-elevated urinary urate is a contraindication to the use of these agents [Khanna et al. 2012]. Benzbromarone and probenecid are the two main agents available in this class. Sulfinpyrazone, although still available in few countries, has been
very restricted in its use for gout and therefore will not be discussed.
ProbenecidProbenecid acts by inhibiting URAT 1 and GLUT 9 transporters (see Figure 2), and is the prototypical uricosuric drug. In a small case series of 30 patients on probenecid monotherapy and 27 patients on probenecid and allopurinol, 33% and 37% reached a target SU of 6 mg/dl, respec-tively [Pui et al. 2013]. Another trial of probene-cid at a dose of 1000 mg twice a day added to allopurinol 300 mg daily resulted in 65% of patients reaching a target SU of 5 mg/dl [Reinders et al. 2007]. Probenecid is still reserved as an option for those who cannot tolerate allopurinol or cannot reach target SU on monotherapy with xanthine-oxidase inhibitors.
Although the efficacy of uricosurics is believed to be impaired with decreasing glomerular filtration rate (GFR), a recent study showed no difference in the percentage of patients achieving target SU when comparing patients with GFR below or above 50 ml/min/1.73m2 [Pui et al. 2013]. Probenecid also has multiple significant drug interactions with commonly used drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs), beta-lactams, and heparin, which limit its use.
Figure 2. Renal anion transporters involved in urate reabsorption in the proximal tubule and action sites of existing and novel uricosuric agents. *Drugs in italics are agents still under development or still not approved.GLUT, glucose transporter; OAT, organic anion transporter; URAT, urate transporter. Adapted from Rees, F. et al. (2014) Nat Rev Rheumatol 10: 271–283.

SE Sattui and AL Gaffo
http://tab.sagepub.com 149
BenzbromaroneBenzbromarone is a potent uricosuric that acts via inhibition of URAT 1 and GLUT 9 transport-ers. Benzbromarone was shown to be more potent than probenecid when used as an add-on to 300 daily mg of allopurinol, with 92% of participants reaching a target SU of 5 mg/dl [Reinders et al. 2007]. Two different studies that compared ben-zbromarone to allopurinol showed higher potency of benzbromarone compared to the standard dose (300 mg) of allopurinol, but almost equal effec-tiveness after up-titration of allopurinol [Perez-Ruiz et al. 1998; Reinders et al. 2009]. A systematic review of available evidence concluded that there is no difference in urate-lowering potency between benzbromarone and allopuri-nol. The same review concluded that benzbro-marone is more potent than probenecid at achieving SU goals [Kydd et al. 2014].
Efficacy in benzbromarone has been seen even in patients with an estimated GFR of 20 ml/min [Lee et al. 2008]. Despite its high efficacy, benz-bromarone was withdrawn from the market in several countries due to postmarketing reports of abnormal liver function and deaths from hepatic failure. This risk was especially high in patients taking high doses of 300 mg daily [Hautekeete et al. 1995]. Interestingly, the systematic review by Kydd and colleagues concluded that when compared with probenecid, benzbromarone resulted in fewer withdrawals due to adverse events (AE) and fewer incidence of AE [Kydd et al. 2014].
Uricases (pegloticase)Uricase, the enzyme responsible for the breaking down of urate to the more water-soluble allantoin (see Figure 1) was somehow lost during the evo-lution of man [Orowan, 1955]. This vital step in the final product of purine metabolism became a viable therapeutic target with the development of recombinant uricases.
Pegloticase, a porcine recombinant polyethylene-glucol conjugated uricase was FDA approved in 2014, is currently indicated for gout, refractory to conventional ULT or patients with severe disease burden (e.g. deforming tophaceous gout) [Khanna et al. 2012]. However, this indication was not supported by the United Kingdom’s National Institute for Health and Care Excellence (NICE) based on its high cost and adverse reac-tions [NIOHCA, 2013].
Two phase III trials compared two different pegloticase infusions strategies (8 mg intrave-nously every 2 and 4 weeks) with placebo for a primary outcome of achieving a SU of less than 6 mg/dl for at least 80% of the time between months 3 and 6 [Sundy et al. 2011]. Based on combined results from both trials, 42% and 35% of respond-ers were observed in the every 2 weeks and every 4 weeks groups, respectively. Another analysis that evaluated the same regimens in their response on tophi reduction, reported that the proportion of patients who, after 6 months had complete resolution of at least one tophus without the development of new tophi or enlargement of another tophus, was 45%, 26% and 8% in the every 2 weeks, every 4 weeks, and placebo groups, respectively [Baraf et al. 2013]. Due to its rapid urate-reduction effect, use of pegloticase can cause a significant amount of acute flares even with the concomitant use of prophylactic therapy [Sundy et al. 2011].
Infusion reactions (IRs), which mainly consist of chest discomfort, flushing, and dyspnea have been reported in 20–40% of patients and occur more commonly with less frequent infusions [Baraf et al. 2014]. IRs occur most commonly in patients who developed high-titer antipegloticase antibodies, with formation of these occurring in approximately 40% of patients. The titer of these antibodies cor-relates with loss of the urate-lowering effect, with up to 91% and 71% of patients (in the every 2 and 4 weeks dosing, respectively) losing efficacy in the achievement of goal SU before the development of an IR [Lipsky et al. 2014]. However, a study that included organ transplant recipients on immuno-suppressive agents such as tacrolimus, mycophe-nolate mofetil, cyclosporine A, or azathioprine showed a decreased risk for the formation of anti-pegloticase antibodies and this has generated inter-est for further research about a potential role of immunosuppression to prevent the formation of antipegloticase antibodies [Hershfield et al. 2014]. Current research is also ongoing due to some post-marketing concerns about higher frequency on cardiovascular events in patients receiving pegloti-case [Gentry et al. 2014].
New therapies in developmentDespite available therapies, gout is inadequately managed. This fact, in addition to emerging evi-dence of the possible role of hyperuricemia and gout in cardiovascular and metabolic comorbidi-ties have led to the development of newer agents.

Therapeutic Advances in Musculoskeletal Disease 8(4)
150 http://tab.sagepub.com
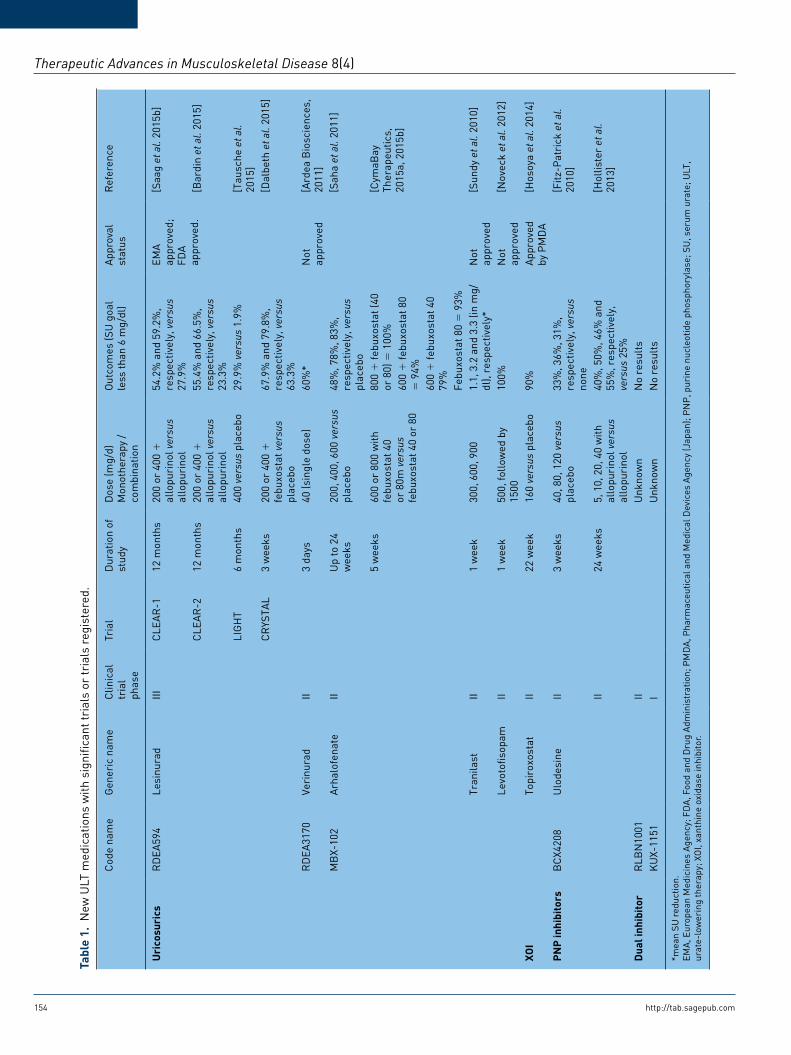
Most of them, including lesinurad which has been recently approved by the US FDA, are uricosuric agents developed based on the increasing knowl-edge of renal urate transporters (see Figure 1 and 2). Here we will discuss some of the new drugs currently under study, including phase I and II trials (see Table 1).
UricosuricsLesinurad (RDEA594). Lesinurad is a URAT1 and OAT4 inhibitor, which increases proximal renal tubule urate excretion. RDEA806, which is the prodrug for lesinurad, is a nonnucleoside reverse transcriptase inhibitor in trials for HIV treatment that was found to have significant hypouricemic properties. An initial phase II trial of 208 patients with gout with SU over 6 mg/dl and a creatinine clearance (CrCl) over 60 ml/min despite allopuri-nol, were randomized to combination therapy by adding 200, 400 and 600 mg of lesinurad daily or placebo [Perez-Ruiz et al. 2010]. After 28 days, 79%, 74%, and 63% of patients achieved SU reduction below 6 mg/dl in to 600, 400 and 200 mg lesinurad groups compared to only 25% in the placebo group. This study was followed by a phase IIb extension that enrolled 126 patients to assess the ongoing efficacy of the combination strategy with a 44-week follow up [Perez-Ruiz et al. 2011] Approximately 78% of the patients receiving lesinurad maintained SU levels below 6 mg/dl by week 44, compared to only 56% of patients in the placebo group. Allopurinol was adequately titrated in this follow-up study. Even more, 59% of the patients in the lesinurad group achieved a SU of less than 5 mg/dl. No significant differences in AEs were noted between groups in any of the two studies.
With promising results in the phase II trials, recent phase III trials have been done showing the effi-cacy and safety of lesinurad. The CLEAR-1 study was 12 month randomized, double-blind trial that compared lesinurad, 200 or 400 mg daily, in combination with allopurinol to allopurinol with placebo [Saag et al. 2015b]. This study included 603 patients who were inadequate responders, meaning not reaching SU less than 6 mg/dl, already on adequate allopurinol dosing. SU less than 6 mg/dl at 6 months, which was the study’s main outcome, was reached in 59.2% and 54.2% in the lesinurad 400 and 200 mg, respectively, compared to only 27.9% in the placebo group. Goal SU of less than 5 mg/dl was also achieved in twice as many patients in the lesinurad 200 mg
group compared to placebo, and up to four times as much in the lesinurad 400 mg. The main AEs observed were elevations of serum creatinine (SCr) readings two times above the baseline level. This was mostly observed in the lesinurad 400 mg group, where 6% of patients presented this AE. However, all patients in the lesinurad 200 mg group presented resolution of the increased SCr by the end of the study without need to discon-tinue medication, as well as 85% of patients in the higher dose group. Other AEs were not signifi-cantly different between the groups. Similar results were observed from the international CLEAR-2 study [Bardin et al. 2015]. A recent combined analysis of both CLEAR-1 and CLEAR-2 studies, that pooled 1208 patients and divided them into groups based on estimated CrCl (<60, <90 or ⩾90 ml/min) [Saag et al. 2015a]. Efficacy, measured as a proportion of patients achieving SU goal of less than 6 mg/dl was con-sistently greater (p < 0.05) across all groups com-pared to placebo. No significant difference in incident of AEs was noted between different groups. Elevation in SCr occurred more fre-quently among the lesinurad groups, particularly in the 400 mg groups, however most of these patients presented resolution in SCr levels by the end of the study. The LIGHT study, which evalu-ated lesinurad 400 mg as monotherapy as an option for patients intolerant or with contraindica-tions to XOIs, showed a significant reduction in SU compared to placebo [Tausche et al. 2015]. However, only 29.9% achieved SU below 6 mg/dl, and effectiveness was not as encouraging as those observed in the combination trials. In this trial, there was a higher frequency of SCr elevations in individuals receiving lesinurad (8.4%) and almost half of them did not present resolution of SCr elevation by the end of the trial. A final study that focused on patients with chronic tophaceous gout, the CRYSTAL study, evaluated the combi-nation of lesinurad and febuxostat with SU goals of 5 and 6 mg/dl [Dalbeth et al. 2015]. At 6 months, approximately 76% of patients on the lesinurad 400 mg group achieved the goal SU of less than 5 mg/dl. A higher proportion of patients achieving SU goal of 5 mg/dl was also seen in patients in the lesinurad 200 mg group, and this was clearly observed amongst all different SU goal levels. Improvement in the resolution of one or more tophus and decrease in tophus area was reported in the lesinurad 200 and 400 mg groups compared to placebo. The safety profile was over-all consistent with previous studies, with more individuals with elevations in SCr being observed

SE Sattui and AL Gaffo
http://tab.sagepub.com 151
in the lesinurad 400 mg group and most of the individuals returning to baseline SCr by the study’s final visit. The importance of maintained SU lowering by ULT was clearly shown by a pooled analysis of the CLEAR-1, CLEAR-2 and CRYSTAL studies, where a lower SU goal was clearly correlated with improvement in tophi bur-den (measure by total tophus area) and incidence of gout flares requiring therapy [Terkeltaub et al. 2015]. The safety of lesinurad in patients with CKD and other comorbidities is still unknown. The drug has been recently approved by the US FDA for the management, in association with a XOI, of hyperuricemia in gout [FDA, 2015]. The European Medicines Agency has also recently approved the 200 mg dose of lesinurad for the management of hyperuricemia in chronic gout [EMA, 2015].
Arhalofenate (MBX-102). Arhalofenate is a long-acting dual action medication whose main urico-suric effect comes from the selective inhibition of URAT1 and OAT4 [Choi et al. 2012]. It is also a peroxisome proliferator-activated receptor-ligand (PPAR)-γ modulator, and through this mecha-nism, is capable of reducing IL-1β levels with a potential added benefit of reducing gout flares.
While being initially intended as a type 2 diabetes mellitus drug, an analysis of four global double-blinded phase II randomized controlled trials (RCTs) including 955 patients analyzed the effect of different doses of arhalofenate on SU [Saha et al. 2011]. Statistically significant dose-depend-ent reductions from baseline SU were observed in 13%, 22%, and 29% of the patients receiving arh-alofenate 200, 400, and 600 daily mg respectively. When analyzing patients whose baseline SU was above 6 mg/dl, 48%, 78%, and 83% of patients receiving 200, 400, and 600 mg of arhalofenate achieved a SU below 6 mg/dl compared to only 25% in the placebo group. The safety profile was overall good, with significant reductions in fasting glucose, hemoglobin A1c and triglycerides were seen in all treatment arms.
A phase II study evaluated a sequential combina-tion strategy using arhalofenate and febuxostat [CymaBay Therapeutics, 2015a, 2015b]. One arm used 600 daily mg of arhalofenate for 2 weeks, followed by sequential weekly coadminis-tration of febuxostat at 80 mg and 40 mg daily, with 2 final weeks of febuxostat as monotherapy at 40 mg daily. A second analogous arm used an arhalofenate dose of 800 daily mg with a final
febuxostat monotherapy phase of 80 mg daily. The combination therapy showed a significant effectiveness in the reduction of SU, with the highest dose combination (arhalofenate 800 mg and febuxostat 80 mg) showing 100%, 93% and 79% of patients reaching a SU of less than 6, 5 and 4 mg/dl, respectively. Treatment was well tolerated, with no serious AEs reported. No patients presented any significant elevations in SCr and only one patient presented an elevation in liver transaminases. Another phase II trial was designed not only for evaluation of arhalofenate’s urate lowering effect, but also to evaluate its abil-ity to prevent flares. This 12-week RCT used arh-alofenate, in 600 or 800 mg daily doses, when compared to placebo, allopurinol 300 mg daily, and allopurinol 300 mg daily in combination with colchicine 0.6 mg daily [Steinberg et al. 2015]. Participants receiving the arhalofenate 800 mg dose presented a flare rate reduction of 46% and 41% when compared to allopurinol monotherapy and placebo, respectively. These flare rate reduc-tions, although statistically significant, were not as effective as the ones achieved by the allopurinol and colchicine combination arm. By the end of the study, the mean percentage change in SU was 12% and 16% in the arhalofenate 600 and 800 mg when compared to placebo and did not result in a statistically significant number of participants reaching a target SU of less than 6 mg/dl. The only serious AE reported was nephrolithiasis in a patient in the allopurinol group, and no signifi-cant differences regarding the need for manage-ment of AE was noticed between the different groups. Again, no changes in SCr where noticed among the patients receiving arhalofenate.
Tranilast. Tranilast, which was initially devel-oped as medication for asthma and other allergic conditions in Japan, was shown to reduce SU lev-els in healthy volunteers. This is achieved through inhibition of GLUT9 and URAT1 transporters and promotion of renal excretion of urate [Mandal et al. 2010]. Two phase II clinical trials evaluated the effect of tranilast, one by using a single dose of tranilast with doses ranging from 100 to 900 mg, and the second study using total daily doses of 300, 600 or 900 mg daily during 7 days [Sundy and Kitt, 2010]. The first study reported mean SU decrease of 0.17 and 0.24 mg/dl at 4 and 24 hours, respectively. In the second study, mean SU reductions of 1.1, 3.2 and 3.3 mg/dl were reported in the tranilast 300, 600 and 900 mg groups, respectively. Besides its urate lowering effect, tranilast has also been reported

Therapeutic Advances in Musculoskeletal Disease 8(4)
152 http://tab.sagepub.com
to reduce inflammation induced by monosodium urate (MSU) crystals in vivo, by suppressing leu-kocyte infiltration and plasma extravasation in a similar magnitude to colchicine and indometha-cin [Serafini and Emerling, 2010]. This would represent an added benefit to ULT therapy offered with the possibility of flare prevention. A phase II clinical trial using tranilast in combina-tion with allopurinol was carried out, however no results have been published yet.
Levotofisopam. Levotofisopam is the S-enantiomer of a 2,3-benzodiazepine, tofisopam, which is approved in several countries outside the US for the management of anxiety. Two phase I trials showed a reduction of SU levels in healthy indi-viduals, and although the mechanism is not known precisely, it is thought to be through enhancement of urate excretion. In a phase II trial with 13 patients with hyperuricemia with gout, one day of levotofisopam 500 mg daily fol-lowed by TID doses and one final single dose on day 7 showed a mean absolute SU reduction of 3.9 mg/dl (range 2.3–5.3) [Noveck et al. 2012]. All patients achieved the SU goal below 6 mg/dl, with a mean treated SU of 4.1 mg/dl. No serious AEs were reported, with 23% of patients experi-encing a gout flare. Further investigations on levotofisopam are pending.
Verinurad (RDEA3170). RDEA3170 is a URAT1 inhibitor that has shown to be three times more potent that benzbromarone and 100 times more potent that probenecid is currently in phase II trials [Miner and Tan, 2013]. In a phase I trial, a 36-hour sustained decrease of over 60% in SU concentrations was reported in healthy individuals after a single dose of RDEA3170 40 mg [Ardea Biosciences, 2011]. Currently, phase II trials comparing monother-apy and combination therapy with allopurinol and febuxostat are ongoing. No results are avail-able at the moment.
UR-1102. UR-1102 is a novel, URAT1, OAT1 and OAT3 inhibitor, that has shown a higher potency that benzbromarone in in vitro studies [Ahn et al. 2013]. At the moment, no further studies or results have been reported regarding the development of this agent.
XOIsTopiroxostat. Topiroxostat (FYX-501) is a selective XOI that acts by structure and mechanism-based
inhibition (competitive versus noncompetitive enzymatic inhibition), combining allopurinol and febuxostat’s XOI mechanisms, respectively. This medication is currently approved in Japan by the Pharmaceuticals and Medical Devices Agency (PMDA) in doses from 20 to 80 mg twice daily [PMDA, 2013]. The half-life for topiroxostat is 20 h, and even after the dissociation of the topiroxo-stat–XO complex, the enzyme does not recover complete activity. A Japanese phase III study showed that the percentage decrease in SU obtained by topiroxostat 120 mg/day was compa-rable to allopurinol 200 mg/day, with 72.4% of patients achieving the goal SU of less than 6 mg/dl. AEs were similar overall when compared with allopurinol and placebo, except for elevation of transaminases.
Regarding indication of patients with baseline renal impairment, a 22-week RCT randomized patients with a baseline eGFR between 30–60 ml/min/1.72m2 to topiroxostat 160 mg daily or placebo and evaluated the SU reduction [Hosoya et al. 2014]. Percent decrease in SU in patients in the treatment group and placebo were 45.38% and 0.08%, respectively, with 90% of patients receiving topiroxostat achieving a SU less than 6 mg/dl. There were no significant changes in renal function between groups, with the added effect of a decrease in the urinary albumin-to-creatinine ratio. Increases in liver enzymes were reported, but these were not considered statistically sig-nificant and no serious AEs were reported.
Purine nucleoside phosphorylase inhibitorUlodesine. Ulodesine (BCX4208) is a novel and unique agent in its class which acts by inhibiting purine nucleoside phosphorylase (PNP), an enzyme which is one step before XO in the pro-duction of urate (see Figure 1). Ulodesine admin-istration has shown a dose-dependent effect on the reduction of xanthine and hypoxanthine [Bantia et al. 2013]. Urate production is inhibited in this way, therefore representing an exciting agent for the management of hyperuricemia in gout. An initial randomized placebo-controlled trial compared oral doses of 40, 80, 120 mg daily in 60 gout patients with a baseline SU over 8 mg/dl [Fitz-Patrick et al. 2010]. SU was reduced by 2.7, 3.3 and 4.4 mg/dl in the 40, 80 and 120 mg groups, respectively. No placebo-treated subjects achieved the SU goal of less than 6 mg/dl, com-pared to 33%, 36% and 31% of the subjects receiving the 40, 80 and 120 mg daily doses by

SE Sattui and AL Gaffo
http://tab.sagepub.com 153
the end of 3 weeks. A higher proportion of patients in each respective dose achieved the goal SU at least once during the whole 3 week period. All lymphocyte subsets were decreased by 30–70% with all ulodesine doses, however none of the sub-jects had to stop treatment due to lymphocyte reduction. No other significant AEs were reported.
An initial 12-week RCT comparing four different doses of ulodesine (5, 10, 20 and 40 mg/day) with allopurinol 300 mg/day to allopurinol monother-apy showed a significantly greater proportion of patients achieving the SU goal, with a safe profile and adequate tolerance to the combination [Becker et al. 2013]. The 24-week extension which included 160 patients from the original study showed that by the end of trial, 40%, 50%, 46% and 55% of the patients receiving the 5, 10, 20 and 40 mg/day of ulodesine, respectively, achieved a goal SU less than 6 mg/dl [Hollister et al. 2013]. This compared to only 25% of patient in the allopurinol–placebo group. AE frequency and severity, including infectious AEs, were similar among ulodesine groups and placebo. Protocol-specified withdrawals due to CD4+ less than 350 cells/ml occurred in 4 and 11 patients in the ulodesine 20 and 40 mg/day groups, respectively. All subjects were tested for response to Tetanus Toxoid and Pneumococcal Polysaccharide Vaccine, showing no significant difference in response between the ulodesine-treated and pla-cebo subjects. Although initial concerns of inhibi-tion of PNP was raised, due to absence of PNP in immunodeficiency and autoimmune disorders, evidence so far seems encouraging. Ulodesine has also shown a well tolerated drug-interaction pro-file, which is an important factor in the manage-ment of gout patients who usually have a high comorbidity-burden [Bantia et al. 2013].
Dual inhibitors of xanthine oxidase and urate renal transportersRLBN1001 was a prototype cancer drug that induced marked urate reduction in human patients [Warrell et al. 2014]. Hypouricemia was induced by an increase in urate urinary excretion and modest inhibition of XO. Urate urinary excretion was observed to be due to inhibition of URAT1 but not GLUT9, although upon produc-tion of diverse analogs, one of them was shown to potently inhibit GLUT9.
KUX-1151 is another potential ULT currently undergoing phase II trials [Kissei Pharmaceutical
Co., 2013]. The urate-lowering effect by KUX-1151 is thought to be through the inhibition of XO and URAT1. No results are available at the moment.
ConclusionDespite its high prevalence and a significant impact in productivity and quality of life associ-ated with its inadequate management, gout has mirrored other orphan diseases when considering the paucity of therapeutic options. This, associ-ated with socio-economical and educational bar-riers described in the management of gout, has led to a suboptimal patient care and poor health outcomes.
Treatment failure is sometimes related to poor tolerance and side effects to available therapeutic options, even including serious AEs such as AHS. Although febuxostat has emerged as an option, wide availability is still limited because of cost and health insurance coverage considera-tions. Availability of newer drugs, especially the emerging uricosurics such as lesinurad, will allow for the introduction into clinical practice of com-bination regimens that have shown promising results in several studies. The high efficacy seen in these combination studies could also represent an alternative for management of tophaceous gout when pegloticase use is limited by IRs, high cost, or the formation of neutralizing antipegloti-case antibodies. In addition, the development of novel therapeutic classes targeting dual and com-plementary targets for gout is encouraging. Combined action as XOI/URAT1 inhibitors and ULT/IL-1β antagonists hold a promise for a more comprehensive and simplistic approach to gout therapy in the future.
Much of the renewed interest in hyperuricemia and gout arises from emerging evidence about the impact of hyperuricemia in cardiovascular and metabolic conditions. Although still incon-clusive, the potential benefits of ULT in early hypertension or CKD outcomes could be easier to implement in practice with new generation drugs having safer side effect profiles [Feig et al. 2008; Kanji et al. 2015]. Some of these drugs such as arhalofenate and topiroxostat have shown promising improvements in metabolic disease markers such as hemoglobin A1c reduc-tions, improvement in lipid profiles, and reduc-tions in microalbuminuria. More specific pathways targeted by this new generation of
Therapeutic Advances in Musculoskeletal Disease 8(4)
154 http://tab.sagepub.com
Tabl
e 1.
New
ULT
med
icat
ions
with
sig
nific
ant t
rial
s or
tria
ls r
egis
tere
d.
Cod
e na
me
Gen
eric
nam
eC
linic
al
tria
l ph
ase
Tria
lD
urat
ion
of
stud
yD
ose
(mg/
d)
Mon
othe
rapy
/co
mbi
natio
n
Out
com
es (S
U g
oal
less
than
6 m
g/dl
)A
ppro
val
stat
usR
efer
ence
Uri
cosu
rics
RD
EA59
4Le
sinu
rad
IIIC
LEA
R-1
12 m
onth
s20
0 or
400
+
allo
puri
nol v
ersu
s al
lopu
rino
l
54.2
% a
nd 5
9.2%
, re
spec
tivel
y, v
ersu
s 27
.9%
EMA
ap
prov
ed;
FDA
ap
prov
ed.
[Saa
g et
al.
2015
b]
CLE
AR
-212
mon
ths
200
or 4
00 +
al
lopu
rino
l ver
sus
allo
puri
nol
55.4
% a
nd 6
6.5%
, re
spec
tivel
y, v
ersu
s 23
.3%
[Bar
din
et a
l. 20
15]
LIG
HT
6 m
onth
s40
0 ve
rsus
pla
cebo
29.9
% v
ersu
s 1.
9%[T
ausc
he e
t al.
2015
]C
RYS
TAL
3 w
eeks
200
or 4
00 +
fe
buxo
stat
ver
sus
plac
ebo
67.9
% a
nd 7
9.8%
, re
spec
tivel
y, v
ersu
s 63
.3%
[Dal
beth
et a
l. 20
15]
RD
EA31
70Ve
rinu
rad
II3
days
40 (s
ingl
e do
se)
60%
*N
ot
appr
oved
[Ard
ea B
iosc
ienc
es,
2011
]M
BX-
102
Arh
alof
enat
eII
Up
to 2
4 w
eeks
200,
400
, 600
ver
sus
plac
ebo
48%
, 78%
, 83%
, re
spec
tivel
y, v
ersu
s pl
aceb
o
[Sah
a et
al.
2011
]
5
wee
ks60
0 or
800
with
fe
buxo
stat
40
or 8
0m v
ersu
s fe
buxo
stat
40
or 8
0
800 +
febu
xost
at (4
0 or
80)
= 1
00%
[Cym
aBay
Th
erap
eutic
s,
2015
a, 2
015b
]
60
0 +
febu
xost
at 8
0 =
94%
60
0 +
febu
xost
at 4
0 79
%
Febu
xost
at 8
0 =
93%
Tr
anila
stII
1 w
eek
300,
600
, 900
1.1,
3.2
and
3.3
(in
mg/
dl),
resp
ectiv
ely*
Not
ap
prov
ed[S
undy
et a
l. 20
10]
Le
voto
fisop
amII
1 w
eek
500,
follo
wed
by
1500
100%
Not
ap
prov
ed[N
ovec
k et
al.
2012
]
XOI
Topi
roxo
stat
II22
wee
k16
0 ve
rsus
pla
cebo
90%
App
rove
d by
PM
DA
[Hos
oya
et a
l. 20
14]
PN
P in
hibi
tors
BC
X420
8U
lode
sine
II3
wee
ks40
, 80,
120
ver
sus
plac
ebo
33%
, 36%
, 31%
, re
spec
tivel
y, v
ersu
s no
ne
[Fitz
-Pat
rick
et a
l. 20
10]
II
24 w
eeks
5, 1
0, 2
0, 4
0 w
ith
allo
puri
nol v
ersu
s al
lopu
rino
l
40%
, 50%
, 46%
and
55
%, r
espe
ctiv
ely,
ve
rsus
25%
[Hol
liste
r et
al.
2013
]
Dua
l inh
ibit
orR
LBN
1001
IIU
nkno
wn
No
resu
lts
K
UX-
1151
IU
nkno
wn
No
resu
lts
*mea
n SU
red
uctio
n.EM
A, E
urop
ean
Med
icin
es A
genc
y; F
DA
, Foo
d an
d D
rug
Adm
inis
trat
ion;
PM
DA
, Pha
rmac
eutic
al a
nd M
edic
al D
evic
es A
genc
y (J
apan
); P
NP
, pur
ine
nucl
eotid
e ph
osph
oryl
ase;
SU
, ser
um u
rate
; ULT
, ur
ate-
low
erin
g th
erap
y; X
OI,
xant
hine
oxi
dase
inhi
bito
r.

SE Sattui and AL Gaffo
http://tab.sagepub.com 155
drugs would also represent better drug-interaction profiles, which has been an important limiting factor in the management of gout patients with high comorbidity burden.
The approval of febuxostat, pegloticase, and the more recent availability of lesinurad, start filling a decades-long gap in the management of gout. Encouraging results in the upcoming trials could lead to further development of new therapeutic agents. Hopefully, this will translate into improve-ments in clinical outcomes, quality of life, pro-ductivity, and even cardiometabolic profiles in patients with gout.
FundingThis research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statementThe authors declare that there is no conflict of interest.
ReferencesAhn, S., Horiba, N., Ohtomo, S., Lee, K., Kim, K., Kim, B. et al. (2013) The therapeutic efficacy of the novel uricosuric agent UR-1102 for hyperuricemia and gout. Ann Rheum Dis 72: A704.
Ardea Biosciences (2011) Ardea’s Next-Generation Urat1 Inhibitor, Shows Promising Phase 1 Clinical Results, vol. 2015. Ardea Biosciences.
Arellano, F. and Sacristan, J. (1993) Allopurinol hypersensitivity syndrome: a review. Ann Pharmacother 27: 337–343.
Bantia, S., Harman, L., Hollister, A. and Pearson, P. (2013) BCX4208, a novel enzyme inhibitor for chronic management of gout, shows a low risk of potential drug–drug interactions. Annals of the Rheumatic Diseases 71: 450.
Baraf, H., Becker, M., Gutierrez-Urena, S., Treadwell, E., Vazquez-Mellado, J., Rehrig, C. et al. (2013) Tophus burden reduction with pegloticase: results from phase 3 randomized trials and open-label extension in patients with chronic gout refractory to conventional therapy. Arthritis Res Ther 15: R137.
Baraf, H., Yood, R., Ottery, F., Sundy, J. and Becker, M. (2014) Infusion-related reactions with pegloticase, a recombinant uricase for the treatment of chronic gout refractory to conventional therapy. J Clin Rheumatol 20: 427–432.
Bardin, T., Keenan, R., Khanna, P., Kopicko, J., Fung, M., Bhakta, N. et al. (2015) Lesinurad, a selective uric acid reabsorption inhibitor, in combination with allopurinol: results from a phase III study in gout patients having an inadequate response to standard of care (clear 2). Annals of the Rheumatic Diseases 74: 545.
Beard, S., Von Scheele, B., Nuki, G. and Pearson, I. (2014) Cost-effectiveness of febuxostat in chronic gout. Eur J Health Econ 15: 453–463.
Becker, M., Hollister, A., Terkeltaub, R., Waugh, A., Flynt, A., Fitz-Patrick, D. et al. (2013) BCX4208 added to allopurinol increases response rates in patients with gout who fail to reach goal range serum uric acid on allopurinol alone: a randomized, double-blind, placebo-controlled trial. Annals of the Rheumatic Diseases 71: 438.
Becker, M., Schumacher, H., Benjamin, K., Gorevic, P., Greenwald, M., Fessel, J. et al. (2009) Quality of life and disability in patients with treatment-failure gout. J Rheumatol 36: 1041–1048.
Becker, M., Schumacher, H., Espinoza, L., Wells, A., Macdonald, P., Lloyd, E. et al. (2010) The urate-lowering efficacy and safety of febuxostat in the treatment of the hyperuricemia of gout: the CONFIRMS trial. Arthritis Res Ther 12: R63.
Becker, M., Schumacher, H., Wortmann, R., Macdonald, P., Eustace, D., Palo, W. et al. (2005a) Febuxostat compared with allopurinol in patients with hyperuricemia and gout. N Engl J Med 353: 2450–2461.
Becker, M., Schumacher, H., Wortmann, R., Macdonald, P., Palo, W., Eustace, D. et al. (2005b) Febuxostat, a novel nonpurine selective inhibitor of xanthine oxidase: a twenty-eight-day, multicenter, phase II, randomized, double-blind, placebo-controlled, dose-response clinical trial examining safety and efficacy in patients with gout. Arthritis Rheum 52: 916–923.
Campion, E., Glynn, R. and Delabry, L. (1987) Asymptomatic hyperuricemia. Risks and consequences in the normative aging study. Am J Med 82: 421–426.
Cea Soriano, L., Rothenbacher, D., Choi, H. and Garcia Rodriguez, L. (2011) Contemporary epidemiology of gout in the UK general population. Arthritis Res Ther 13: R39.
Choi, H., Mount, D. and Reginato, A. (2005) Pathogenesis of gout. Ann Intern Med 143: 499–516.
Choi, Y., Larroca, V., Lucman, A., Vicena, V., Abarca, N., Rantz, T. et al. (2012) Arhalofenate is a novel dual-acting agent with uricosuric and anti-inflammatory properties. Arthritis Rheum 64: 1632.

Therapeutic Advances in Musculoskeletal Disease 8(4)
156 http://tab.sagepub.com
CymaBay Therapeutics (2015a) CymaBay Therapeutic Announces Positive Results from Its Phase 2 Clinical Study of Arhalofenate in Combination with Febuxostat, vol. 2015. CymaBay Therapeutics: http://ir.cymabay.com/press-releases/detail/234.
CymaBay Therapeutics (2015b) CymaBay Therapeutics to Present Results from Two Arhalofenate Phase 2 Studies at the American College of Rheumatology (ACR) Annual Meeting, November 6–11, Vol. 2015. CymaBay Therapeutics: http://ir.cymabay.com/press-releases/detail/353.
Dalbeth, N., Jones, G., Terkeltaub, R., Khanna, D., Kopicko, J., Bhakta, N. et al. (2015) Lesinurad, a novel selective uric acid reabsorption inhibitor, in combination with febuxostat, in patients with tophaceous gout: the crystal phase III clinical trial. Ann Rheum Dis 74: 778.
De Abajo, F., Gil, M., Rodriguez, A., Garcia-Poza, P., Alvarez, A., Bryant, V. et al. (2015) Allopurinol use and risk of non-fatal acute myocardial infarction. Heart 101: 679–685.
Doherty, M., Jansen, T., Nuki, G., Pascual, E., Perez-Ruiz, F., Punzi, L. et al. (2012) Gout: why is this curable disease so seldom cured? Ann Rheum Dis 71: 1765–1770.
EMA (2015) Zurampic, vol. 2015. European Medicines Agency: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/003932/smops/Positive/human_smop_000913.jsp&mid=WC0b01ac058001d127web.
FDA (2015) FDA Approves Zurampic to Treath High Blood Uric Acid Levels Associated with Gout, vol. 2015. U.S. Food and Drug Administration: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm478791.htm.
Feig, D., Soletsky, B. and Johnson, R. (2008) Effect of allopurinol on blood pressure of adolescents with newly diagnosed essential hypertension: a randomized trial. JAMA 300: 924–932.
Fitz-Patrick, D., Drummond, W., Pappas, J. and Hollister, A. (2010) Effects of a purine nucleoside phosphorylase inhibitor, BCX4208, on the serum uric acid concentrations in patients with gout. Arthritis Rheum 62: 150.
Garg, R., Sayles, H., Yu, F., Michaud, K., Singh, J., Saag, K. et al. (2013) Gout-related health care utilization in us emergency departments, 2006 through 2008. Arthritis Care Res (Hoboken) 65: 571–577.
Gentry, W., Dotson, M., Williams, B., Hartley, M., Stafford, K., Bottorff, M. et al. (2014) Investigation of pegloticase-associated adverse events from a
nationwide reporting system database. Am J Health Syst Pharm 71: 722–727.
Grayson, P., Kim, S., Lavalley, M. and Choi, H. (2011) Hyperuricemia and incident hypertension: a systematic review and meta-analysis. Arthritis Care Res (Hoboken) 63: 102–110.
Grimaldi-Bensouda, L., Alperovitch, A., Aubrun, E., Danchin, N., Rossignol, M., Abenhaim, L. et al. (2015) Impact of allopurinol on risk of myocardial infarction. Ann Rheum Dis 74: 836–842.
Hande, K., Noone, R. and Stone, W. (1984) Severe allopurinol toxicity. description and guidelines for prevention in patients with renal insufficiency. Am J Med 76: 47–56.
Hautekeete, M., Henrion, J., Naegels, S., Deneve, A., Adler, M., Deprez, C. et al. (1995) Severe hepatotoxicity related to benzarone: a report of three cases with two fatalities. Liver 15: 25–29.
Hershfield, M., Ganson, N., Kelly, S., Scarlett, E., Jaggers, D. and Sundy, J. (2014) Induced and pre-existing anti-polyethylene glycol antibody in a trial of every 3-week dosing of pegloticase for refractory gout, including in organ transplant recipients. Arthritis Res Ther 16: R63.
Hollister, A., Dobo, S., Maetzel, A., Becker, M., Terkeltaub, R., Fitz-Patrick, D. et al. (2013) Long-term safety of BCX4208 added to allopurinol in the chronic management of gout: results of a phase 2 24-week blinded safety extension and vaccine challenge study. Ann Rheum Dis 71: 442–443.
Horsburgh, S., Norris, P., Becket, G., Arroll, B., Crampton, P., Cumming, J. et al. (2014) Allopurinol use in a New Zealand population: prevalence and adherence. Rheumatol Int 34: 963–970.
Hosoya, T., Ohno, I., Nomura, S., Hisatome, I., Uchida, S., Fujimori, S. et al. (2014) Effects of Topiroxostat on the serum urate levels and urinary albumin excretion in hyperuricemic stage 3 chronic kidney disease patients with or without gout. Clin Exp Nephrol 18: 876–884.
Hung, S., Chung, W., Liou, L., Chu, C., Lin, M., Huang, H. et al. (2005) HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Natl Acad Sci USA 102: 4134–4139.
Hutton, I., Gamble, G., Gow, P. and Dalbeth, N. (2009) Factors associated with recurrent hospital admissions for gout: a case-control study. J Clin Rheumatol 15: 271–274.
Jordan, K., Cameron, J., Snaith, M., Zhang, W., Doherty, M., Seckl, J. et al. (2007) British Society for Rheumatology and British health professionals in

SE Sattui and AL Gaffo
http://tab.sagepub.com 157
rheumatology guideline for the management of gout. Rheumatology (Oxford) 46: 1372–1374.
Jutkowitz, E., Choi, H., Pizzi, L. and Kuntz, K. (2014) Cost-effectiveness of allopurinol and febuxostat for the management of gout. Ann Intern Med 161: 617–626.
Kanji, T., Gandhi, M., Clase, C. and Yang, R. (2015) Urate lowering therapy to improve renal outcomes in patients with chronic kidney disease: systematic review and meta-analysis. BMC Nephrol 16: 58.
Khanna, D., Fitzgerald, J., Khanna, P., Bae, S., Singh, M., Neogi, T. et al. (2012) 2012 American College of Rheumatology Guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res (Hoboken) 64: 1431–1446.
Kim, S., Guevara, J., Kim, K., Choi, H., Heitjan, D. and Albert, D. (2009) Hyperuricemia and risk of stroke: a systematic review and meta-analysis. Arthritis Rheum 61: 885–892.
Kim, S., Guevara, J., Kim, K., Choi, H., Heitjan, D. and Albert, D. (2010) Hyperuricemia and coronary heart disease: a systematic review and meta-analysis. Arthritis Care Res (Hoboken) 62: 170–180.
Kissei Pharmaceutical Co. (2013) Kissei announces licensing agreement with Pfizer Inc. for KUX-1151, a novel investigational therapy for gout, vol. 2015. Kissei Pharmaceutical Co., Ltd. https://www.kissei.co.jp/e_contents/relation/l4/Vcms4_00000741.html.
Kydd, A., Seth, R., Buchbinder, R., Edwards, C. and Bombardier, C. (2014) Uricosuric medications for chronic gout. Cochrane Database Syst Rev 11: CD010457.
Lawrence, R., Felson, D., Helmick, C., Arnold, L., Choi, H., Deyo, R. et al. (2008) Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum 58: 26–35.
Lee, M., Graham, G., Williams, K. and Day, R. (2008) A benefit-risk assessment of benzbromarone in the treatment of gout. Was its withdrawal from the market in the best interest of patients? Drug Saf 31: 643–665.
Lipsky, P., Calabrese, L., Kavanaugh, A., Sundy, J., Wright, D., Wolfson, M. et al. (2014) Pegloticase immunogenicity: the relationship between efficacy and antibody development in patients treated for refractory chronic gout. Arthritis Res Ther 16: R60.
MacDonald, T., Ford, I., Nuki, G., Mackenzie, I., De Caterina, R., Findlay, E. et al. (2014) Protocol of the febuxostat versus allopurinol streamlined trial (fast): a large prospective, randomised, open, blinded
endpoint study comparing the cardiovascular safety of allopurinol and febuxostat in the management of symptomatic hyperuricemia. BMJ Open 4: e005354.
MacIsaac, R., Salatzki, J., Higgins, P., Walters, M., Padmanabhan, S., Dominiczak, A. et al. (2016) Allopurinol and cardiovascular outcomes in adults with hypertension. Hypertension 67: 535–540.
Mandal, A., Emerling, D., Serafini, T. and Mount, D. (2010) Tranilast Inhibits urate transport medicated by URAT1 and GLUT9. Arthritis Rheum 62: 164.
Miner, J. and Tan, P. (2013) RDEA3170, a novel, high affinity URAT1 inhibitor binds to a central domain within URAT1. Ann Rheum Dis 71: 446.
NIOHCA (2013) Pegloticase for Treating Severe Debilitating Chronic Tophaceous Gout. Nice Technology Appraisal Guidance (TA291), vol. 2013. National Institute for Health and Care Excellence.
Noveck, R., Wang, Z., Forsthoefel, A., Sigmon, K., Hall, P. and Keogh, J. (2012) Levotofisopam has uricosuric activity and reduces serum urate levels in patients with gout. Arthritis Rheum 64: 818.
Orowan, E. (1955) The origin of man. Nature 175: 683–684.
Perez-Ruiz, F., Alonso-Ruiz, A., Calabozo, M., Herrero-Beites, A., Garcia-Erauskin, G. and Ruiz-Lucea, E. (1998) Efficacy of allopurinol and benzbromarone for the control of hyperuricemia. A pathogenic approach to the treatment of primary chronic gout. Ann Rheum Dis 57: 545–549.
Perez-Ruiz, F., Sundy, J., Krishnan, E., Hingorani, V., Welp, J., Suster, M. et al. (2011) Efficacy and safety of lesinurad (RDEA594), a novel uricosuric agent, given in combination with allopurinol in allopurinol-refractory gout patients: randomized, double-blind, placebo-controlled, phase 2b study. Ann Rheum Dis 70: 104.
Perez-Ruiz, F., Hingorani, V., Welp, J., Sheedy, B., Manhard, K., Shen, Z. et al. (2010) Efficacy and safety of a range of doses of rdea594, a novel uricosuric agent, as a single agent in hyperuricemic gout patients: multicentre, randomized, double-blind, placebo controlled, phase 2 experience. Ann Rheum Dis 69: 121.
PMDA (2013) Report on the Deliberations Results, vol. 2015. Pharmaceuticals and Medical Devices Agency: https://www.pmda.go.jp/files/000153624.pdf.
Pui, K., Gow, P. and Dalbeth, N. (2013) Efficacy and tolerability of probenecid as urate-lowering therapy in gout; clinical experience in high-prevalence population. J Rheumatol 40: 872–876.
Rees, F., Jenkins, W. and Doherty, M. (2013) Patients with gout adhere to curative treatment

Therapeutic Advances in Musculoskeletal Disease 8(4)
158 http://tab.sagepub.com
if informed appropriately: proof-of-concept observational study. Ann Rheum Dis 72: 826–830.
Reinders, M., Haagsma, C., Jansen, T., Van Roon, E., Delsing, J., Van De Laar, M. et al. (2009) A randomised controlled trial on the efficacy and tolerability with dose escalation of allopurinol 300–600 mg/day versus benzbromarone 100–200 mg/day in patients with gout. Ann Rheum Dis 68: 892–897.
Reinders, M., Van Roon, E., Houtman, P., Brouwers, J. and Jansen, T. (2007) Biochemical effectiveness of allopurinol and allopurinol-probenecid in previously benzbromarone-treated gout patients. Clin Rheumatol 26: 1459–1465.
Ryu, H., Song, R., Kim, H., Kim, J., Lee, E., Lee, Y. et al. (2013) Clinical risk factors for adverse events in allopurinol users. J Clin Pharmacol 53: 211–216.
Saag, K., Bardin, T., So, A., Khanna, P., Storgard, C., Baumgartner, S. et al. (2015a) Analysis of gout subjects receiving lesinurad and allopurinol combination therapy by baseline renal function. Arthritis Rheum 67(Suppl. 10).
Saag, K., Fitz-Patrick, D., Kopicko, J., Fung, M., Bhakta, N., Adler, S. et al. (2015b) Lesinurad, a selective uric acid reabsorption inhibitor, in combination with allopurinol: results from a phase III study in gout patients having an inadequate response to standard of care (clear 1). Annals of the Rheumatic Diseases 74: 540.
Saha, G., Karpf, D., Choi, Y. and Roberts, B. (2011) Arhalofenate, a potential novel treatment for hyperuricemia, with or without metabolic co-morbidities, in patients with gout: meta-analysis of urate lowering in four phase 2 studies in type 2 diabetes. Arthritis Rheum 63(Suppl. 10): 2584.
Schumacher, H., Becker, M., Wortmann, R., Macdonald, P., Hunt, B., Streit, J. et al. (2008) Effects of febuxostat versus allopurinol and placebo in reducing serum urate in subjects with hyperuricemia and gout: a 28-week, phase III, randomized, double-blind, parallel-group trial. Arthritis Rheum 59: 1540–1548.
Serafini, T. and Emerling, D. (2010) Tranilast suppresses inflammation induced by monosodium urate crystals in vivo. Ann Rheum Dis 69: 664.
Singh, J. and Strand, V. (2008) Gout is associated with more comorbidities, poorer health-related quality of life and higher healthcare utilisation in US veterans. Ann Rheum Dis 67: 1310–1316.
Spencer, K., Carr, A. and Doherty, M. (2012) Patient and provider barriers to effective management of gout in general practice: a qualitative study. Ann Rheum Dis 71: 1490–1495.
Stamp, L., Merriman, T., Barclay, M., Singh, J., Roberts, R., Wright, D. et al. (2014) Impaired response or insufficient dosage? Examining the potential causes of 'inadequate response' to allopurinol in the treatment of gout. Semin Arthritis Rheum 44: 170–174.
Stamp, L., O’Donnell, J., Zhang, M., James, J., Frampton, C., Barclay, M. et al. (2011) Using allopurinol above the dose based on creatinine clearance is effective and safe in patients with chronic gout, including those with renal impairment. Arthritis Rheum 63: 412–421.
Stamp, L., Taylor, W., Jones, P., Dockerty, J., Drake, J., Frampton, C. et al. (2012) Starting dose is a risk factor for allopurinol hypersensitivity syndrome: a proposed safe starting dose of allopurinol. Arthritis Rheum 64: 2529–2536.
Steinberg, A., Chera, H., Choi, Y., Martin, R., Mcwherter, C., Zhang, Y. et al. (2015) A study to evaluate the efficacy and safety of arhalofenate for preventing flares and reducing serum uric acid in gout patients. Arthritis Rheum 67(Suppl. 10).
Sundy, J., Baraf, H., Yood, R., Edwards, N., Gutierrez-Urena, S., Treadwell, E. et al. (2011) Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: two randomized controlled trials. JAMA 306: 711–720.
Sundy, J. and Kitt, M. (2010) Tranilast, a novel, potential treatment for the chronic management of hyperuricemia in patients with gout, reduces serum uric acid in healthy subjects. Ann Rheum Dis 69: 607.
Tausche, A., Alten, R., Dalbeth, N., Kopicko, J., Bhakta, N., Storgard, C. et al. (2015) Lesinurad monotherapy in gout patients intolerant to xanthine oxidase inhibitors (light): a randomized, double-blind, placebo-controlled, 6-month phase III clinical trial. Ann Rheum Diseases 74: 769.
Terkeltaub, R., Perez-Ruiz, F., Storgard, C., Fung, M., Kopicko, J. and Dalbeth, N. (2015) Relationship between sustained lowering of serum urate levels and improvements in gout flares and tophus area: pooled exploratory analysis of gout subjects receiving lesinurad and xanthine oxidase inhibitor combination therapy. Ann Rheum Dis 74: 771–772.
Warrell, R., Klukovits, A., Barnes, K., Satyanarayana, C., Cheeseman, C. and Piwinski, J. (2014) Novel bifunctional inhibitors of xanthine oxidase and urat1 induce profound hypouricemia in human subjects. Ann Rheum Dis 73: 786.
White, W., Chohan, S., Dabholkar, A., Hunt, B. and Jackson, R. (2012) Cardiovascular safety of febuxostat and allopurinol in patients with gout

SE Sattui and AL Gaffo
http://tab.sagepub.com 159
and cardiovascular comorbidities. Am Heart J 164: 14–20.
Yamanaka, H. (2011) Japanese guideline for the management of hyperuricemia and gout: second edition. Nucleosides Nucleotides Nucleic Acids 30: 1018–1029.
Yun, J., Marcaida, M., Eriksson, K., Jamin, H., Fontana, S., Pichler, W. et al. (2014) Oxypurinol directly and immediately activates the drug-specific T cells via the preferential use of HLA-B*58:01. J Immunol 192: 2984–2993.
Zhang, W., Doherty, M., Bardin, T., Pascual, E., Barskova, V., Conaghan, P. et al. (2006) EULAR evidence based recommendations for gout. Part II: management. report of a task force of the EULAR standing committee for international clinical studies including therapeutics (ESCISIT). Ann Rheum Dis 65: 1312–1324.
Zhu, Y., Pandya, B. and Choi, H. (2011) Prevalence of gout and hyperuricemia in the US general population: the national health and nutrition examination survey 2007–2008. Arthritis Rheum 63: 3136–3141.
Visit SAGE journals online http://tab.sagepub.com
SAGE journals