treatment of non-hodgkin's lymphoma with radiolabeled...
TRANSCRIPT

CANCER RESEARCH(SUPPL.)55, 5899s-5907s, December 1, 1995J
Abstract
LL2 is a murine IgG2a anti-CD22 monoclonal antibody found to reactwith virtually all non-Hodgkin's lymphomas (NHLs). Twenty-one patientswith chemotherapy-resistant NHL received nonmyeloablative doses of‘311-labeledLL2 IgG and F(ab')2 ranging from 15 to 343 mCi given incycles of 15—50 mCi, for up to seven treatment cycles. The cumulative
protein dose ranged from 1.1 mg IgG to 157 mg F(ab')2. Seventeenpatients were assessable for treatment response, and antitumor effectswere seen in five (one complete remission, two partial remissions, and twominor or mixed responses). In addition, one complete response was seen ina patient who received only “diagnostic―doses of ‘311-LL2IgG. Thus, atotal of six patients had responses according to the defmed response
criteria. Three additional patients have been treated with potentiallymyeloablative doses of ‘311-LL2IgG at a starting dose level of 90 mCi/m2(100 mg). Two patients were evaluable, and both had partial remissionslasting 8 and 3 months, respectively. Chimeric and complementaritydetermining region-grafted LL2 have been developed. Initial clinical studies have shown that these agents have targeting properties similar to the
murine LL2 and, therefore, may be suitable alternatives to murine LL2 in
the treatment of NHL. LL2 is a promising agent for the treatment oflymphoma, particularly when the maximum tolerated dose is given eitherwith or without autologous bone marrow transplantation.
Introduction
Despite the availability of several effective chemotherapeuticagents for the treatment of NHL,3 this disease remains the seventhleading cause of cancer deaths in the United States (1). High-dosechemoradiotherapy combined with ABMT has been a promisingadvance in the treatment of NHL; however, this mode of treatment hasserious toxicity and is still associated with a high relapse rate (2—4).Therefore, there is a continuous search for more effective and lesstoxic treatment modalities.
NHLs have been identified as attractive targets for RAIT because oftheir remarkable radiosensitivity (5—11). Moreover, it has been foundin animal studies that the low-dose-rate irradiation associated withRAff may be more effective than similar radiation doses delivered byfractionated external beam radiation (12, 13). This inverse-dose-rateeffect is related presumably to apoptosis in lymphoma cell lines andto cell cycle redistribution with cell accumulation in radiosensitiveG2-M (13, 14).
Several MAbs directed against different antigens on the surface ofB-lymphoma cells have been used in the treatment of NHL (5—11).
1 Presented at the “Fifth Conference on Radioimmunodetection and Radioimmuno
therapy of Cancer,―October 6—8,1994, Princeton, NJ. Supported in part by OutstandingInvestigator Grant CA39841 from the National Cancer Institute, NIH, Bethesda, MD(D. M. G.).
2 To whom requests for reprints should be addressed, at the Garden State Cancer
Center, Center for Molecular Medicine and Immunology, 1 Bruce Street, Newark, NJ07103.
3 The abbreviations used are: NHL, non-Hodgkin's lymphoma; ABMT, autologous
bone marrow transplantation; CDR, complementarity-determining region; cLL2, chimericLL2; mLL2, murine LL2; hLL2, humanized LL2; CT, computed tomography; HAHA,human antihuman antibody; HAMA, human antimouse antibody; HPLC, high performance liquid chromatography; MAb, monoclonal antibody; RAff, radioimmunotherapy;ROt, region of interest; RT, residence time.
Our group has developed a murine anti-CD22 MAb (originally designated EPB-2 and now called LL2) for imaging and treatment ofNHL or chronic lymphatic leukemia. Immunohistological studiesrevealed that LL2 is reactive with virtually all cases of NHL, including diffuse and nodular, poorly differentiated lymphocytic lymphomas, and histiocytic large cell lymphomas. LL2 has a highly restrictedspecificity, being reactive with only the B-cell population of the
germinal center of normal lymph nodes and the white pulp of thespleen, but not with megakaryocytes, myeloid, or erythroid cells in thebone marrow (15). Moreover, LL2 is not reactive with any peripheralblood cells, including the blood's normal B cells, or with any othernormal tissue. LL2 also has other unique features related to its targetantigen, differentiating it from other anti-B-cell lymphoma antibodies.In vitro studies have demonstrated clearly that LL2 is internalized
after binding to its CD22 target antigen on Raji cells, and that theantigen is reexpressed rapidly on the cell surface (15—17).The internalizing ability of LL2 already has been exploited successfully forimmunotoxin therapy. Kreitman et a!. (18) conjugated LL2 to theirmodified Pseudomonas endotoxin and showed exquisite antitumoreffects in vitro and in vivo. LL2-PE38KDEL (a derivative of Pseudomonas exotoxin), but not the control immunotoxins, led to completeregressions of measurable s.c. CA-46 tumors in nude mice when givenat 50% and 35% of the LD50 (18). Initial clinical studies using131I-labeled LL2 IgG or F(ab')2 also have shown promising results inthe treatment of advanced and chemotherapy-refractive NHL. Thefirst patient to receive LL2 IgG for imaging purposes had a clinicalresponse after the infusion of only 6.2 mCi (0.2 mg) ‘311-LL2IgG (7).This surprising response to low doses of ‘31I-LL2prompted theinitiation of a RAIT trial to test the safety and efficacy of repeatedinfusions of low levels (<30 mCi) of ‘311-LL2IgG or F(ab')2. The
infusion of radioactive doses of <30 mCi allowed the treatment to beconducted as an outpatient procedure. Goldenberg et a!. (7) havereported the initial results of this trial previously, finding two partialremissions and two mixed or minor responses in five assessable of a
total of seven NHL patients treated (7).
Since this initial report, we have treated a total of 21 patients on anoutpatient basis, using repeated injections of low doses (<30 mCi) of‘311-LL2.In addition, a Phase I trial of single high-dose RAIT withmurine ‘311-LL2IgG combined with ABMT has been initiated. Threepatients have been treated thus far at a starting dose level of 90mCi/m2. More recently, we also have developed the chimeric and aCDR-grafted (humanized) form of LL2, and initial clinical studieshave been conducted to investigate the pharmacokinetics, dosimetry,and targeting capabilities of these agents.
In this report, we describe the results of the completed outpatienttreatment program, the initial results of the high-dose therapy approach, and our initial clinical experience with the chimeric andhumanized forms of LL2 in the targeting and treatment of NHL.
Materials and Methods
Development and Characterization of mLL2 Anti-B-cell LymphomaMAb. LL2 is one of two anti-B-cell lymphoma MAbs developed in our
5899s
Treatment of Non-Hodgkin's Lymphoma with Radiolabeled Murine, Chimeric,or Humanized LL2, an Anti-CD22 Monoclonal Antibody'
Malik Juweid, Robert M. Sharkey, Adeline Markowitz, Thomas Behr, Lawrence C. Swayne, Robert Dunn,Hans J. Hansen, Jerry Shevitz, Shui-On Leung, Arnold D. Rubin, Thomas Herskovic, Debra Hanley, andDavid M. Goldenbere
Garden State Cancer Center at the Center for Molecular Medicine and Immunology, Newark, New Jersey 07103 (M. J.. R. M. S.. A. M., T. B., L C. S., R. D., D. M. G.];Immunomedics, Inc., Morris Plains, New Jersey (H. J. H. J. S.. 5-0. LI; and St. Joseph ‘sHospital and Medical (‘enter,Paterson, New Jersey 07503 (A. D. R., 1'. H., D. H.]
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

TREATMENT OF NHL WITH ‘311-LL2ANTI-CD22 MAb
laboratories (I 5). Both antibodies were generated by fusion of mouse myelomaSP2/0-Ag 14 cells with splenocytes of BALB/c mice immunized with membrane preparations from the Raji cell line (a human Burkitt lymphoma). Theantigen identified by LL2 is Mr 140,000, and blocking studies have characterized LL2 reactivity with the @3-epitopegroup of the CD22 antigen (12).CD22 is expressed in the cytoplasm of early pre-B and progenitor cells,appears on the surface of only mature B cells and on the majority of NHL cells,and is then lost during terminal differentiation prior to the plasma cell stagefrom both the surface and cytoplasm (16).
Development of Chimeric and Humanized LL2. As part of our programof developing less immunogenic MAbs, we prepared initially a chimerized
version of the LL2 MAb. The cLL2 was shown to have an equivalent affinity
to the mLL2 and was shown additionally to internalize as quickly as the murineMAb (17). The framework sequences and the CDR sequences of both theheavy- and light-chain variable regions of the mLL2 antibody were identified.
The human EU heavy-chain framework (subgroup 1) served as the base onwhich CDRs from the mLL2 heavy chain were grafted, whereas for the light
chain, the human REI light-chain framework from the human . chain subgroupI was selected. The human framework sequence, except in regions that are inclose vicinities to the CDRs, was conserved as much as possible. Computermodeling was used to assist in identifying important framework amino acids
that might have interaction with the binding pocket. Once identified, theoriginal murine amino acid in that particular position was kept. The version of
the hLL2 constructed had seven retained murine framework residues on the
heavy chain. For the light chain, a total of five murine framework residueswere retained. Residues that were retained were those considered essential inmaintaining the antigen-binding site. The hLL2 was shown to bind to Raji cellswith an equivalent affinity to the chimeric MAb. After adapting the hLL2 forgrowth in serum-free media, cells were grown in a bioreactor for 1 month, after
which 2 g purified hLL2 were produced.
Preparation and Radiolabeling of LL2 Antibody. mLL2 IgG was isolated from ascites-grown hybridoma cells. The F(ab')2 fragment was preparedby pepsin digestion with separation from undigested IgG by protein A andS-200 (2.6 X 95-cm columns; Pharmacia, Piscataway, NJ) chromatography.
All final reagents were analyzed for purity by size-exclusion chromatography(HPLC; GF-250; DuPont, Wilmington, DE) and SDS-PAGE under reducingand nonreducing conditions. The preparations were sterile, pyrogen free, anddevoid of adventitious viruses, and they passed general safety testing. Radio
iodination was performed using the chloramine-T or iodogen method (19). The
specific activity was 12—16mCi/mg. Unbound iodine was removed by eitherion-exchange or size-exclusion chromatography using PD-b (Pharmacia).
More than 95% of radioactivity eluted with the native-size product, as assessedby HPLC. Immunoreactivity was determined by a live-cell RIA with Raji cells.Immunoreactivity of the radiolabeled products ranged from 50 to 75%.
Therapeutic Infusions. Two clinical RAIT studies in patients with B-celllymphomas have been conducted at our institution. One pilot study wasdesigned to test the safety and efficacy of repeated injections of low levels
(<30 mCi) of ‘31I-LL2IgG or F(ab')2. The study was of an exploratory nature
and did not attempt to determine the maximum tolerated dose of the antibodyconstructs used. The patients first received 30 mCi ‘311-LL2,followed by 20mCi ‘‘‘l-LL2I week later to complete one cycle of therapy, enabling the entiretreatment program to be carried out as an outpatient procedure. If patients didnot experience severe dose-limiting myelotoxicity (i.e., grade 3 or higher),they were eligible to receive additional treatment cycles when toxicity from the
preceding treatment had resolved. Twenty-one patients were treated on this
regimen. Six patients received ‘311-mLL2IgG, 14 others received ‘311-mLL2F(ab')2, and 1 patient received the chimeric IgG LL2. All patients received alow-protein dose of 2 mg LL2 in at least one of their therapeutic infusions.However, we also have examined the effect of protein dose on antibodypharmacokinetics and targeting in six patients. Five patients received alternat
ing protein doses of 2 or 20 mg (one patient received 50 mg) in theirtherapeutic infusions given one week apart. In all of these five patients, 18 mgadditional unlabeled protein (one patient received 48 mg) were coinjected with
the 2 mg labeled MAb. The sixth patient was given 20 mg unlabeled protein20 mm before the infusion of 2 mg labeled antibody.
The other clinical RAIT study was a Phase I trial with escalation of a singlehigh dose of radioactivity resulting potentially in bone marrow ablation.
Therefore, this trial was combined with ABMT. Starting doses were 90mCi/rn2, increasing in increments of 40 mCi/m2. The radiation dose to the
lungs was limited to no more than 2400 cGy, based on a pretherapy diagnosticstudy. The patients first received a diagnostic injection of 10 mCi (10 mg)‘311-LL2antibody. If targeting was seen, the patient then received a therapeuticdose with a constant protein amount of 100 mg. The protein amount was keptconstant between patients to assess the therapeutic effects of escalating radiation doses and not varying amounts of unlabeled protein.
Patient Selection. Patientseligible for eitherstudywere adultswith B-celllymphomas who had not responded to conventional systemic therapy, had
normal renal and hepatic function, had not been treated for 4 weeks, had noother active medical problems, and had expected survival of 3 months or more.
The patient had to have a WBC count 3,000/mm3 or a granulocyte count1,500/mm3and a platelet count 100,000/mm3.Patients who entered under
the bone marrow transplantation program must have had tumor-free bonemarrow by bilateral bone marrow biopsy. The patients entered under thelow-dose protocol were allowed to have bone marrow involvement. Initially,no limits were put on the degree of bone marrow disease. However, bonemarrow involvement with lymphoma cells was limited later to no more than
25% of the hematopoietic marrow elements. Both protocols were approved bythe appropriate institutional review committees, and all patients gave writteninformed consent.
Pharmacokinetic Analysis. Blood clearance rates were determined bycounting samples of whole blood at various time points after the end of the
infusion; for example, at 5 mm and 1, 2, 4, 24, 48, and 72 h after the infusion.The data were first fit manually to obtain estimates of the slopes of thedistribution (a) and elimination (@3)phases and their respective intercepts.These estimates were then used in a nonlinear, least-squares, curve-fittingprogram to generate both monophasic and biphasic clearance curves. If the
biphasic result improved the sum of the squares significantly, then it was
selected as the best fit; otherwise, the monophasic curve was used to define theblood clearance. Total-body clearance rates were determined by either wholebody external scintigraphy taken at three separate times or by daily measurements with a rate meter at 1 m from the patient. All body clearance rates fit a
monoexponential curve. The biological clearance data are expressed in the
following fashion: tv2,h taken to clear 50% of the initial radioactivity from theblood; t½-a,distribution phase; tv@-f3,elimination phase; and the RT, theintegration of the blood clearance curve with normalization to the mCi dose
injected.
Imaging. Scans were acquired using a Sophy-DS-7 or DS-X camera(Sopha Medical Systems, Columbia, MD). In patients who received radioactive doses of <30 mCi, imaging could be started immediately after antibody
infusion. Anterior and posterior planar images of the head, neck, chest,abdomen, and pelvis were obtained 3 h after the injection and then on a dailybasis (minimum of 3 days) for up to 1 week after injection. In patients whoreceived higher doses, imaging could be started only after the radiation
exposure was <5 millirems/h. This was usually 7—10days after infusion of thehigher, potentially myeloablative, doses. A high-energy collimator and a 15%energy window centered on the 1311energy peak of 364 keV were used;500,000 counts were collected using a 128 X 128 matrix. Single photonemission CT images of the chest, abdomen, and pelvis were obtained routinely
in all patients on at least two occasions, usually on days 2 and 3, with a 64 X
64 matrix and 64 projections in a 360° circular orbit. A total of 50,000 counts
were collected for each projection. Reconstruction was performed using aHamming-Hann filter. The images were interpreted by at least two reviewers.
Dosimetry. The red marrow dose was estimated both based on bloodactivity and sacral scintigraphy (20, 21). The blood clearance data were usedto estimate the red marrow dose by using the conservative assumption of equalactivity concentrations of blood and red marrow (20). The whole-blood time
activity curve was used to obtain the cumulated activity concentration in theblood. The cumulated activity in the red marrow then was calculated from theblood data by multiplying this concentration by 1500, the weight in g of themarrow in the average adult. The mean dose in cGy to the red marrow then wascalculated according to the Medical Internal Radiation Dose schema with
correction of the remainder of the body activity (22). The method for determining the red marrow dose by sacral scintigraphy has been described previously (21). The sacrum was chosen for the scintigraphic method, because itcontains a known fraction of red marrow and is easily identifiable on nuclearmedicine images of the pelvis. The sacrum was not used in patients whoexhibit focal sacral uptake, a photopenic sacral region, or lower pelvic masses
obscuring the sacral ROl. In these cases, ROIs of other marrow-containing
5900s
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

Table 1 Blood and whole.body pharmacokinetics of ‘@IgG andF(ab')2BloodWholebodyti,2
(hy't112-a (h)t1@-@ (h)RTp1/2(h)RTIgG
(n = 6)F(ab')2 (n = 14)20.7
±4.88.5±7.02.2
±0.73.0± 1.738.9
±10.330.2±8.37.0
±3.73.3± 1.842.0
±13.346.6± 15.960.6
±19.167.2±23.0‘a
mean ±SD.
TREATMENT OF NHL WITH ‘311-LL2ANTI-CD22 MAb
areas were used. ROIs around the sacrum were used to quantitate activityuptake as a function of time, using the conjugate view counting method (23).The anterior and posterior planar images of the pelvis obtained at multiple timepoints during imaging with the radiolabeled LL2 antibody were used fordrawing the sacral ROI. An inverted triangular ROI encompassing the area
between the internal iliac vessels, with exclusion of the bladder, was used to
identify the sacrum to minimize the count contribution from the blood vessels
and ureters within the ROl to the sacral counts. A bone marrow scan with
@“Tc-sulfurcolloid (Syncor, Fairfield, NJ) or a bone scan with @“Tc
methylene diphosphonate (Syncor) was used sometimes to delineate the sacrum in patients without discernable uptake on the antibody scan. A computer
generated gray scale was used in the selection of the background for thesacrum. This minimizes the possibility of choosing areas with increased
radiolabeled antibody uptake. The background ROIs usually were drawnlateral to the sacrum. Cumulated activity in red marrow was determined by
curve integration and division by 0.099, because it has been determined that9.9% of the total red marrow is contained in the adult sacrum. Red marrowdoses were then obtained by multiplying the cumulated activities by theappropriate S factor.
The radiation doses to other organs and to tumors were calculated using theconjugate view techniques by drawing ROIs around the organs of interest onthe pairs of planar anterior and posterior images for all imaging sessions.Appropriate background ROIs also were drawn for each organ and tumor. Theabsolute activity concentration in mCi in each ROl at all imaging times was
calculated using the build-up factor methodology for Compton scatter compensation, as described previously (24). The organ and tumor time-activitydata were then fit to either a monoexponential or biexponential function by a
nonlinear least-squares, curve-fitting routine and then integrated to obtain the
various cumulated activities needed for the dosimetry calculations. The meandose in cGy to the various target organs, with the exception of the tumors, was
then obtained according to Medical Internal Radiation Dose schema withcorrection for the remainder of the body activity. The mean dose in cGy totumors was obtained using the method reported previously (25).
Toxicity and Tumor Response. All patientswere followed for toxicitywith weekly complete peripheral blood counts and blood urea nitrogen, crc
atinine, and liver enzyme determinations on days 7 and 28 after RAIT.
Pulmonary and cardiac functions also were determined 1 and 3 months after
high-dose RAIT combined with ABMT. One month after therapy, thyroid
stimulating hormone was measured to evaluate thyroid function. HAMA wasmeasured at baseline and at 1, 4, 12, and, where possible, 24 weeks aftertherapy. Bone marrow toxicity and other critical organ toxicities were evalu
ated according to standard Radiation Oncology Therapy Group grading. Tumor
responses were assessed at 1—3months after treatment and every 3 months
thereafter, up to I year. If disease progression occurred after 3 months, no
further follow-up was obtained. Physical exams, chest-X-ray, CT, and magnetic resonance imaging were used to assess tumor response. A completeremission was defined as the complete disappearance of all detectable disease
for a minimum of 4 weeks, a partial response as a reduction of at least 50% inthe sum of the products of the longest perpendicular diameters of all measurable lesions for a minimum of 4 weeks, and disease progression as an increase
of at least 25% in diameter or the appearance of new lesions. Minor responseswere considered when the reduction in disease was between 25 and 50%. Amixed response was considered when there was a >50% regression of at leastone lesion and stable disease in other lesions.
HAMA or HAHA Assays. HAMA titers were determined using theELISA described previously (26). In some cases, a commercial HAMA enzyme-linked immunoassay (ImmuSTRIP HAMA enzyme-linked immunoassay; Immunomedics, Inc., Morris Plains, NJ) was used. Values less than 74ng/ml were considered normal. HAHA responses were assessed by HPLC,combining plasma with labeled hLL2 or cLL2. Antibody complexation in
plasma that was higher than 10% was considered consistent with a HAHAresponse. The cutoff of 10% was based on experience with the maximumamount of aggregation in the labeled product (—5%)and the reproducibility ofHPLC determinations in our laboratory.
Results
Pharmacokinetics. HPLC size-exclusion chromatographic analy
sis showed that less than 10% of the radiolabeled MAb was complexed after 1 h, suggesting that the LL2-CD22-reactive epitope is not
present in the plasma of most patients. Furthermore, the HPLC sizeanalysis of the radiolabeled F(ab')2 indicated that the fragment did notdissociate to Fab' fragments after injection. Table 1 shows the phar
macokinetic data for the whole IgG and F(ab')2 forms of LL2. Theaverage blood and whole-body clearance for either antibody form arereported for protein dose infusions of only 2—3mg. The t112sin theblood and total body for the whole IgG were 20.7 ±4.8 h and 42.0±13.3 h, respectively. The blood and total body t112sfor the F(ab')2form were 8.5 ±7.0 and 46.6 ±15.9, respectively. The difference inthe blood half-lives of the IgG and F(ab')2 forms was statisticallysignificant (P < 0.01). There was a considerable interpatient variabil
ity in the blood clearance for either antibody form. This variabilitywas manifested particularly in the a phase of antibody clearance. Theeffect of protein dose on antibody clearance was studied in fivepatients who received alternating doses of 2 and 20 mg (one patientreceived 50 mg) LL2-F(ab')2 given 1 week apart. The blood t1,@withthe 2-mg-protein dose was 12.7 ±5.1 versus 21.0 ±3.2 (P < 0.02)with the higher-protein dose (five patients, 10 injections). Interestingly, the red marrow dose based on blood was also lower with thelow-protein dose compared with the higher-protein dose (1.7 ±0.9versus 2.3 ±0.5 cOy/mCi). However, this difference did not reach
statistical significance in this small number of patients. In the onepatient who received 20 mg unlabeled cLL2 20 mm prior to thelabeled antibody infusion, the blood t,,@was 52.5 h, compared with26.0 h for 2 mg labeled antibody alone.
Therapeutic Results with Nonmyeloablative Doses of ‘311-LL2.Table 2 summarizes the characteristics of the patients who receivednonmyeloablative doses of ‘311-LL2IgG or F(ab')2. These include thehistological types of their tumors, the stages of their disease, and theRAIT treatments they received. The corresponding total-body redmarrow doses (based on blood) and hematopoietic toxicity are alsoshown. A total of 21 patients were treated with variable doses of‘311-LL2IgG or F(ab')2. Six patients received ‘311-mLL2IgG, 14others received ‘311-mLL2F(ab')2, and 1 patient received the cLL2IgG. The cumulative radioactive dose ranged from 15.1 mCi ‘31I-LL2IgG to 343 mCi ‘311-LL2F(ab')2. The cumulative protein dose rangedfrom 1.1 mg IgG to 157 mg LL2-F(ab')2. One patient (patient 1273)received up to seven treatment cycles (14 injections), with each cycledelivering approximately 50 mCi “Iradioactivity.
Sixteen patients received at least one treatment cycle of@@ ‘I-LL2IgG or F(ab')2. Five patients (patients 1113, 1206, 1218, 1404, and1469) received only one of the two injections required to complete thefirst treatment cycle. These patients had been entered on a compassionate approval and, after the first injection, were judged too advanced to receive the full treatment cycle. Four of them died due to
5901s
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

Table 2 Patient characteristicsRadiation
doseStageToxicity(cGy)PatientHistology(Ann
Arbor)Age/SexDates of InjectionAbFormmCigradeTBRM1002
1062Large
cell, noncleaved
SmallroundcellIV IV6OIMa 22/M1
1/88—10/8912/4—12/10/905/15—5/24/89IgG
F(ab')2IgG24.1
55.149.00
046
II3214
27
941077Diffuselarge cell,noncleavedIII49/M7/18—7/25/89IgG47.41291319/19/8946.415271084Poorly
differentiatedIV73/F8/8—8/15/89IgG46.6322651092
1102Nodular,
mixed
Nodular, poorly differentiatedIV III70/F 481M8129/899/26/89
10/17—10/24/89lgG IgG29.958.2
52.3NA 41754
1584228
68II 13Nodular, diffuse largecellIII61/F12/12/89IgG30.7NA68149I153Follicular and diffuse large cellIV73/F4/9/90
5/8/906/4/90F(ab')218.5
32.351.02 312
203225
631401206Poorly
differentiatedIV581M11/6/90F(ab').,30.4NA20471218HistiocyticnodularIV70/F1/2/91F(ab')229.82+14231220Diffuse,
well-differentiatedIII691M1/15—1/22/915/28—6/3/91
7/8/91F(ab'),51.249.729.80
0019
17534
43151225Diffuse,well-differentiatedIV691M418-4/16/91F(ab').,46.8420421226Nodular,
mixedIII55/F2/19—2/25/917/9—7/16/91F(ab').,52.5 50.1265 332491281
248CLLIV56/F4/30—5/7/9 1F(ab')240.1422341273CLLIV58/F8/5—8/13/91
9/16—9/24/91ll/12—ll/19/911/06—1/13/92
3/2—3/9/92
5/12—5/18/927/13—7/20/92F(ab')248.3
48.546.549.449.8
51.448.60
0001
2433
33283334
363370
1061068095
98831291Diffuse
large cell, noncleavedIV651M10/28—I1/04/91F(ab')249.23+1211501404Follicularsmall cell,cleavedIV4/8/93F(ab')229.0ND27.442.6(nodular,
poorlydifferentiated)1448Diffusesmall cell,cleavedIV701M9/1—9/14/93F(ab').,49.4424.461.51469Follicular
lymphomaIV6OIM12/20/93F(ab')215.1310.227.01476Nodularsmall cell, cleavedIV52/M1/19—1/26/94ChimericIgG24.6316.374.91478Large
cell, diffuse,B-cellIV66/F2/22—2/28/94F(ab')748.8422.690.4phenotype.highgradea
NI, male;F, female.
TREATMENT OF NHL WiTH ‘311-LL2ANTI-CD22 MAb
their advanced disease within 2—3weeks. The fifth patient, whoreceived a reduced dose of only 15 mCi ‘31I-LL2F(ab')2, had stabledisease for 6 months. Four patients who received at least one completecycle of treatment were not assessable for treatment response; one(patient 1448) received external radiation 1 week after our treatment,and follow-up studies were not done on another patient (patient 1478)who was sent into hospice care. The third patient (patient 1248)presented with massive splenomegaly. A splenectomy was performed,and the patient left the study. The fourth patient (patient 1273)received 13 injections of ‘31I-LL2F(ab')2 over more than 1 yearwithout developing HAMA. This patient experienced severe swellingof her lymph nodes after the first injection of labeled LL2, promptingher primary physician to place her on prednisone, which reduced theswelling and permitted us to administer the second injection and tocomplete the first treatment cycle. Although the patient was notassessable for response at this time, her advancing disease (axillaryadenopathy and retroperitoneal mass, 2.9 X 1.3 cm) stabilized suddenly, and her primary physician requested that we resume RAIT,although he continued to treat the patient with prednisone. Becausethe patient had been refractive to several forms of treatment, includingextensive steroid (prednisone) therapy, the primary physician believedthat the disease stabilization was due to RAIT. Indeed, the prednisonetreatment may, in part, explain this patient's lack of HAMA. Thispatient was able to tolerate a total of 638 cGy to her red marrow beforedose-limiting myelotoxicity occurred. She has recovered from themyelotoxicity, and her disease remained stable for 9 months.
Of the assessable 17 patients treated with the low-dose RAffregimen (6 with murine IgG, 10 with murine F(ab')2, and one withchimeric IgG), 5 have had responses, ranging from a short-term (1
month) mixed response to one complete response lasting 5 months. Ofthis series, 12 had a complete cycle of LL2 therapy (-“50mCi),resulting in 5 patients showing objective responses. In addition, onepatient (patient 1002), who received only “diagnostic―doses of‘31I-LL2IgG, experienced a complete remission of disease lasting 1year. However, this patient relapsed again and was referred to ourprogram 2 months later, at which time she received one cycle (55.1mCi) of treatment with ‘311-LL2F(ab')2. No antitumor response wasseen after this treatment. A summary of these treatment responses andtheir duration can be found in Table 3.
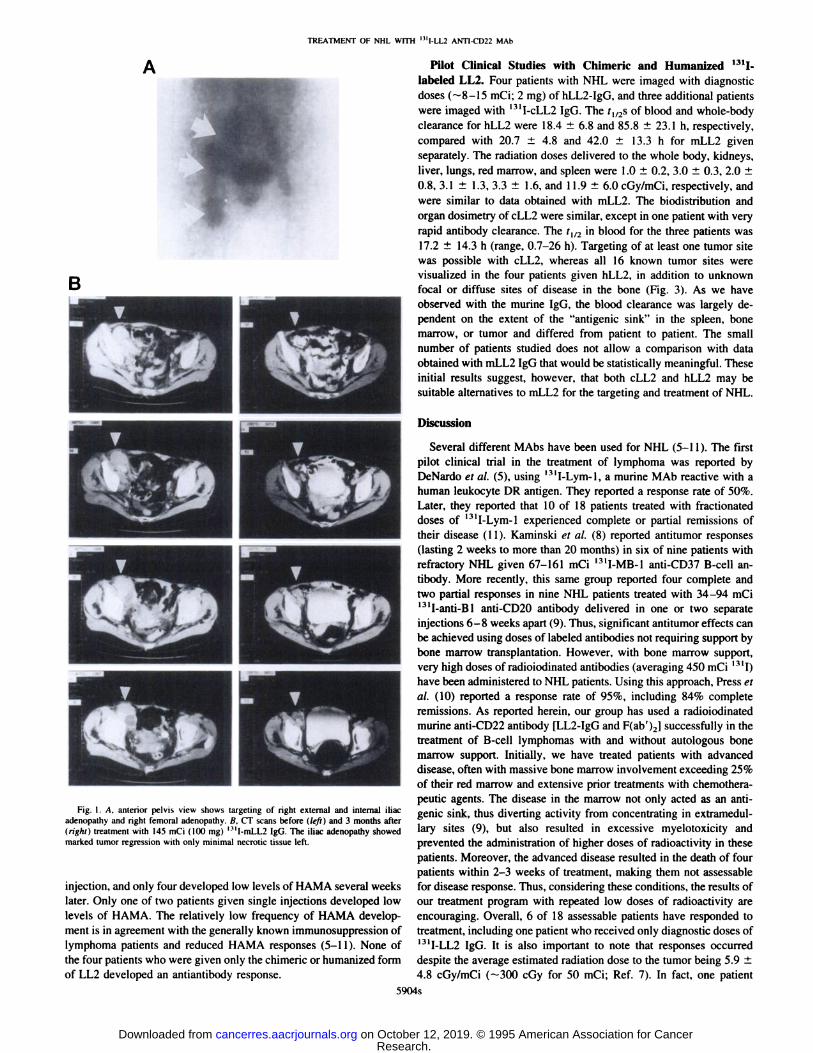
Initial Therapeutic Results with Myeloablative Doses of‘311-LL2IgG. Three additional patients received high, potentiallymyeloablative doses of ‘311-LL2IgG, starting at 90 mCiJm2, and all ofthese patients were reinfused with previously harvested bone marrow.Two of the three patients treated with the high-dose ‘31I-LL2IgGRAIT regimen combined with ABMT were assessable. One patient
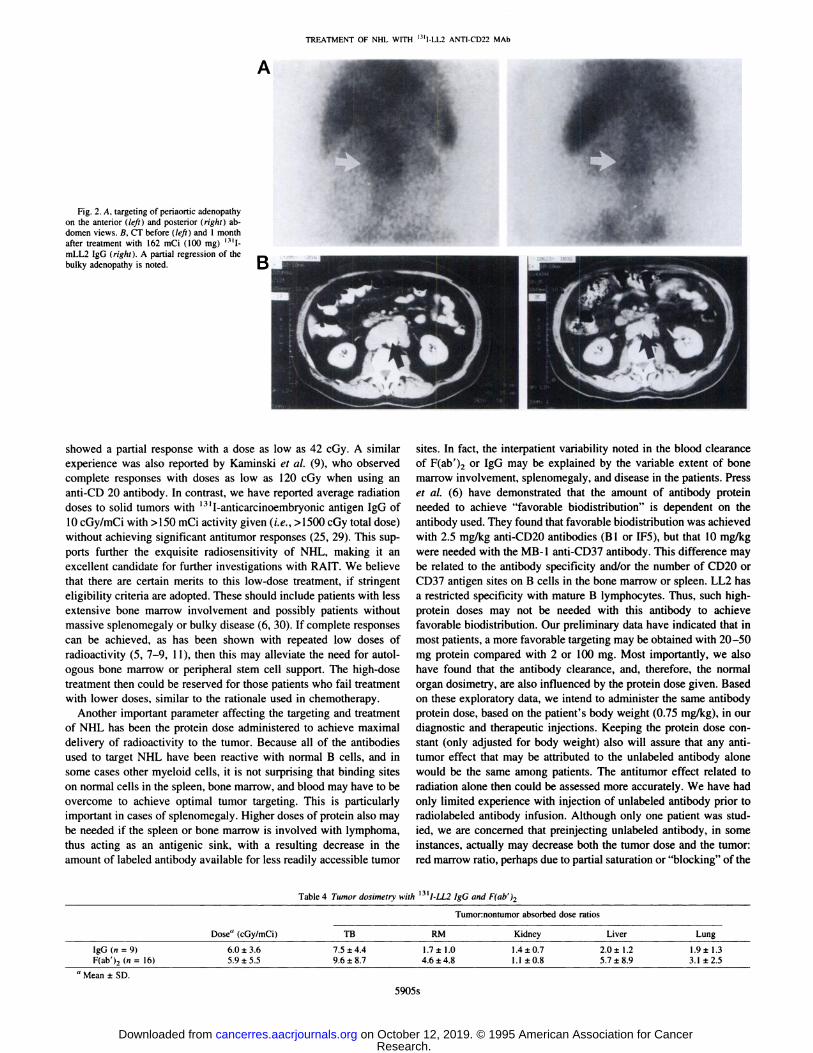
had a partial response by CT for 8 months (Fig. 1). She then developed meningeal lymphoma. However, there was no evidence ofdisease progression in the peripheral nodes, based on a CT scanperformed at that time. The patient was treated subsequently withintrathecal chemotherapy (methotrexate, l-j3-D-arabinofuranosylcytosine, and hydrocortisone). Unfortunately, the patient died 1 monthlater of her central nervous system disease. The other patient haddemonstrated a partial response on his 1-month follow-up scan (Fig.2). However, the patient's disease progressed 2 months later, and a CT
scan performed at that time showed enlargement of the intraabdominal adenopathy, which responded previously to RAIT. He then wenton to receive an EPOCH chemotherapeutic regimen (a combination ofetoposide, prednisone, vincristine, cytoxan, and doxorubicin hydro
5902s
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

Table 3 Antitumor responses with ‘3114fl fgG andF(ab')2Antibody
infusionPatient(totaldose, mCi; antibody form)Response,duration10023
injections (24.1, all diagnostic; IgG)After RAID I: complete response, 2 moAfter RAID 2 and 3: complete response, Iyr10773
injections (93.8; IgG)Mixed, Imo10922injections (88.1; lgG)Partial response, 2.5moI
1022 injections (52.3; IgG)Minor response, 2.5moI1533 injections [101.8; F(ab')2jComplete response, 5mo12205
injections [130.7; F(ab')2]Partial response, 4mo14901injection (145.0; IgG) with ABMTPartial response, 8moI
5081 injection (I 83.0; IgG) with ABMTPartial response, 3 mo
TREATMENT OF NHL WITh ‘311-LL2ANTI-CD22 MAb
evaluated for toxicity. Two of the 3 evaluable patients who receivedthe IgG form had grade 3 or 4 myelotoxicity, and 5 of 10 who receivedthe F(ab')2 form had grade 3 or 4 thrombocytopenia or leukopenia.The average red marrow dose (based on blood) in the patients whoreceived the IgG form was not statistically different from that of thepatients who received the F(ab')2 form. Neither the red marrow dosebased on blood nor the total-body radiation-absorbed dose couldpredict toxicity for either antibody form used. For example, grade 3and 4 toxicity with IgG occurred at red marrow doses of 65 and 94cGy, respectively. However, only grade 1 toxicity was noted inanother patient who received a red marrow dose of 131 cOy. In the 5patients with F(ab')2 who had grade 3 or 4 myelotoxicity, the averagered marrow dose was 75.6 ±46.9 versus 93.6 ±84.1 cGy (P ns)for those who had grade 2 toxicity or less. However, patients withbone marrow metastases or hyperproliferating red marrow were farmore likely to develop dose-limiting toxicity than patients withoutbone marrow disease. A similar experience was reported by DeNardoet a!. (27) in NHL patients treated with ‘31I-Lym-l antibody. Both
conditions, diffuse disease or red marrow proliferation, resulted inelevated red marrow uptake of radiolabeled LL2, increased radiationto the red marrow, and enhanced myelotoxicity. Based on this finding,the utility of using an imaging-based method, particularly sacralscintigraphy, as a better estimate of the red marrow dose and potentially a better predictor of toxicity was investigated. In patients withuniformly increased bone marrow uptake, the red marrow dose based
on sacral scintigraphy was significantly higher than that based onblood, regardless of the antibody form used. Five of seven of thesepatients who could be evaluated for myelotoxicity developed grade 3or 4 toxicity after only 50 mCi ‘31I-LL2F(ab')2. On the other hand,patients with tumor-negative marrow biopsies and without increasedbone marrow uptake had equal or lower estimates of the red marrowdose when based on sacral scintigraphy than when estimated by bloodactivity. All three patients with this finding developed grade 2 toxicityor less when given the same radioactive dose of ‘311-LL2F(ab')2. Thesame trend was found in the limited number of patients who weregiven the IgG form of LL2. These data suggest that sacral scintigraphymay provide a better estimate of the red marrow dose and, therefore,may be a better predictor of myelotoxicity in patients treated withradiolabeled antibodies. A more detailed description of the results ofthis investigation is published elsewhere in this supplement (28).
llAMA Response. HAMA development was followed adequatelyin 19 patients given the murine forms of LL2 antibody. One patientreceived 13 injections of ‘31I-LL2F(ab')2 without developing HAMAover more than 1 year. However, as described earlier, this patient wasreceiving prednisone treatment, and this, in part, may explain the lackof HAMA. One patient received five injections of IgG before developing HAMA, and two patients received three injections before developing HAMA. One of the latter had received an unknown scmtherapy previously in Europe and, thus, was believed to bepresensitized to mouse protein. Twelve patients received two antibodyinjections. Ten of these patients were followed after the second
5903s
chloride), to which he responded well. Both responses are included inTable 3.
Dosimetry. Table 4 gives the average tumor dose estimates andtumor:normal organ dose ratios determined in 12 patients infused with
‘3t1-labeledwhole IgG (n = 4) or F(ab')2 (n 8) of LL2. Tumorweights ranged from 2 1 to 3 12 g. The biological half-life of the MAbsin the tumors ranged from 19 to 467 h (median, 58 h), with noappreciable difference between the IgG and the fragment. Tumordoses were calculated in 25 lesions and ranged from 0.5 to 25cGy/mCi (average, 5.9 ±4.8 cGy/mCi). The differences between theaverage tumor doses and tumor:nontumor ratios obtained with the IgGor F(ab'), forms were not statistically significant.
Protein Dose. As mentioned earlier, the effect of increasing theprotein dose was examined in six patients. Four patients had beeninjected with doses of 2 or 20 mg protein within a 1-week period.Another patient had 2- and 50-mg injections within 1 week. In allthese five patients, the additional unlabeled protein was coinjectedwith 2 mg labeled antibody. The sixth patient was given 20 mgunlabeled antibody 20 mm before the injection of 2 mg labeledantibody.
One common observation was that the higher protein dose reducedthe rate of clearance from the blood, resulting in higher radiationdoses to the red marrow, based on blood clearance data. In addition,there was a decrease in percent uptake and radiation dose to the spleenor involved bone marrow. The effect of increasing MAb protein ontumor dose and the ratio of the tumor:red marrow dose was assessedin three patients. Two patients showed clearly higher tumor:red marrow ratios with the injection of 20 mg (32% higher) or 50 mg (38%higher) than with the injection of 2 mg. However, one patient showeda 25% lower tumor:red marrow dose ratio with the 20-mg dosecompared with the 2-mg dose. In the one patient in whom 20 mgunlabeled antibody was injected before the labeled antibody, the doseto two relatively small tumors (42 and 113 g) decreased by 49% and24%, respectively. Tumor and red marrow doses also decreased 54%
and 34%, respectively, with the preinfusion of the unlabeled antibody.A larger tumor (558 g), however, showed a 32% increase in the tumordose and a 16% increase in the tumor:red marrow ratio. A comparisonof the 10-mg diagnostic protein dose given in patients who thenunderwent high-dose RAIT with 100 mg given in the therapeuticinfusion was made difficult by early therapeutic responses (tumorregression) that were observed very early after the therapeutic infusion (within 1 week in one patient). However, in one patient, in whomthere was little immediate change in tumor size, the tumor doses were25—60%lower, and the tumor:organ dose ratios were 20—70%lowerwith the 100-mg dose compared with the 10-mg dose.
Myelotoxicity. Patients who were treated with repeated low dosesof ‘@ ‘I-LL2received variable numbers of treatment cycles and, thus,different amounts of radioactivity. Therefore, we have evaluated myelotoxicity in patients after they have received only one full cycle ofRAIT [50 mCi ‘311-LL2IgG or F(ab')2]. Three patients who receivedthe IgG form and 10 patients who received the F(ab')2 form could be
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from
‘:4Fa@@IE@4@..@:;:i@@s‘-@@:..•@.kP@
TREATMENT OF NHL WITH ‘311-LL2ANTI-CD22 MAt,
A Pilot Clinical Studies with Chimeric and Humanized ‘@‘Ilabeled LL2. Four patients with NHL were imaged with diagnosticdoses (—8—15mCi; 2 mg) of hLL2-IgG, and three additional patientswere imaged with ‘311..cLL2IgG. The t1125of blood and whole-bodyclearance for hLL2 were 18.4 ±6.8 and 85.8 ±23.1 h, respectively,compared with 20.7 ±4.8 and 42.0 ± 13.3 h for mLL2 givenseparately. The radiation doses delivered to the whole body, kidneys,liver, lungs, red marrow, and spleen were 1.0 ±0.2, 3.0 ±0.3, 2.0 ±0.8, 3.1 ±1.3, 3.3 ±1.6, and 11.9 ±6.0 cGy/mCi, respectively, andwere similar to data obtained with mLL2. The biodistribution andorgan dosimetry of cLL2 were similar, except in one patient with veryrapid antibody clearance. The t112in blood for the three patients was17.2 ±14.3 h (range, 0.7—26h). Targeting of at least one tumor sitewas possible with cLL2, whereas all 16 known tumor sites werevisualized in the four patients given hLL2, in addition to unknown
focal or diffuse sites of disease in the bone (Fig. 3). As we haveobserved with the murine IgG, the blood clearance was largely dependent on the extent of the “antigenicsink―in the spleen, bonemarrow, or tumor and differed from patient to patient. The small
number of patients studied does not allow a comparison with dataobtained with mLL2 IgG that would be statistically meaningful. Theseinitial results suggest, however, that both cLL2 and hLL2 may besuitable alternatives to mLL2 for the targeting and treatment of NHL.
Discussion
Several different MAbs have been used for NHL (5—I1). The firstpilot clinical trial in the treatment of lymphoma was reported byDeNardo et a!. (5), using ‘31I-Lym-l, a murine MAb reactive with a
human leukocyte DR antigen. They reported a response rate of 50%.Later, they reported that 10 of 18 patients treated with fractionateddoses of ‘311-Lym-lexperienced complete or partial remissions oftheir disease (1 1). Kaminski et al. (8) reported antitumor responses(lasting 2 weeks to more than 20 months) in six of nine patients withrefractory N}IL given 67—161mCi ‘31I-MB-lanti-CD37 B-cell antibody. More recently, this same group reported four complete andtwo partial responses in nine NHL patients treated with 34—94mCi‘311-anti-Bl anti-CD2O antibody delivered in one or two separate
injections 6—8weeks apart (9). Thus, significant antitumor effects can
be achieved using doses oflabeled antibodies not requiring support bybone marrow transplantation. However, with bone marrow support,very high doses of radioiodinated antibodies (averaging 450 mCi ‘@‘I)have been administered to NHL patients. Using this approach, Press eta!. (10) reported a response rate of 95%, including 84% complete
remissions. As reported herein, our group has used a radioiodinatedmurine anti-CD22 antibody [LL2-IgG and F(ab')2] successfully in thetreatment of B-cell lymphomas with and without autologous bonemarrow support. Initially, we have treated patients with advanceddisease, often with massive bone marrow involvement exceeding 25%
of their red marrow and extensive prior treatments with chemotherapeutic agents. The disease in the marrow not only acted as an antigenic sink, thus diverting activity from concentrating in extramedullazy sites (9), but also resulted in excessive myelotoxicity andprevented the administration of higher doses of radioactivity in thesepatients. Moreover, the advanced disease resulted in the death of fourpatients within 2—3weeks of treatment, making them not assessablefor disease response. Thus, considering these conditions, the results ofour treatment program with repeated low doses of radioactivity areencouraging. Overall, 6 of 18 assessable patients have responded totreatment, including one patient who received only diagnostic doses of
‘311-LL2IgG. It is also important to note that responses occurreddespite the average estimated radiation dose to the tumor being 5.9 ±4.8 cGy/mCi (-‘-300cGy for 50 mCi; Ref. 7). In fact, one patient
59045
B
Fig. 1. A, anterior pelvis view shows targeting of right external and internal iliacadenopathy and right femoral adenopathy. B, CT scans before (left) and 3 months after(right) treatment with 145 mCi (100 mg) ‘31I-mLL2IgG. The iliac adenopathy showedmarked tumor regression with only minimal necrotic tissue left.
injection, and only four developed low levels of HAMA several weekslater. Only one of two patients given single injections developed lowlevels of HAMA. The relatively low frequency of HAMA development is in agreement with the generally known immunosuppression oflymphoma patients and reduced HAMA responses (5—11). None ofthe four patients who were given only the chimeric or humanized formof LL2 developed an antiantibody response.
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from
l―@―@4'
.@-@,,@..4
@ ‘: “@
@o@D.,-
Table 4 Tumor dosimetrywith I3I@@ IgG andF(ab')2Dose'@
(cGy/mCi)Tumor:nontumor
absorbed doseratiosTBRM
KidneyLiverLungIgG
(n = 9)F(ab')2 (n = 16)6.0
±3.65.9±5.57.5
±4.49.6±8.71
.7 ±I .0 1.4 ±0.74.6±4.8 1.1 ±0.82.0
±I .25.7±8.91
.9 ±1.33.1±2.5a
Mean ±SD.
TREATMENT OF NHL WITH ‘311-LL2ANTI-CD22 MAb
A
?. @.@
-@ r@-@@
Fig. 2. A, targeting of periaortic adenopathy
on the anterior (left) and posterior (right) abdomen views. B, CT before (left) and 1 monthafter treatment with 162 mCi (100 mg)@@ ‘I-mLL2 IgG (right). A partial regression of thebulky adenopathy is noted.
showed a partial response with a dose as low as 42 cGy. A similarexperience was also reported by Kaminski et a!. (9), who observed
complete responses with doses as low as 120 cGy when using ananti-CD 20 antibody. In contrast, we have reported average radiationdoses to solid tumors with ‘@@ I-anticarcinoembryonic antigen IgG of10 cGy/mCi with >150 mCi activity given (i.e., >1500 cGy total dose)without achieving significant antitumor responses (25, 29). This supports further the exquisite radiosensitivity of NHL, making it anexcellent candidate for further investigations with RAIT. We believethat there are certain merits to this low-dose treatment, if stringenteligibility criteria are adopted. These should include patients with lessextensive bone marrow involvement and possibly patients withoutmassive splenomegaly or bulky disease (6, 30). If complete responses
can be achieved, as has been shown with repeated low doses of
radioactivity (5, 7—9,11), then this may alleviate the need for autologous bone marrow or peripheral stem cell support. The high-dosetreatment then could be reserved for those patients who fail treatment
with lower doses, similar to the rationale used in chemotherapy.Another important parameter affecting the targeting and treatment
of NHL has been the protein dose administered to achieve maximaldelivery of radioactivity to the tumor. Because all of the antibodies
used to target NHL have been reactive with normal B cells, and insome cases other myeloid cells, it is not surprising that binding siteson normal cells in the spleen, bone marrow, and blood may have to beovercome to achieve optimal tumor targeting. This is particularlyimportant in cases of splenomegaly. Higher doses of protein also maybe needed if the spleen or bone marrow is involved with lymphoma,thus acting as an antigenic sink, with a resulting decrease in theamount of labeled antibody available for less readily accessible tumor
sites. In fact, the interpatient variability noted in the blood clearanceof F(ab')2 or IgG may be explained by the variable extent of bonemarrow involvement, splenomegaly, and disease in the patients. Presset a!. (6) have demonstrated that the amount of antibody protein
needed to achieve “favorablebiodistribution― is dependent on theantibody used. They found that favorable biodistribution was achieved
with 2.5 mgfkg anti-CD2O antibodies (B 1 or IFS), but that 10 mg/kgwere needed with the MB-l anti-CD37 antibody. This difference maybe related to the antibody specificity and/or the number of CD2O orCD37 antigen sites on B cells in the bone marrow or spleen. LL2 hasa restricted specificity with mature B lymphocytes. Thus, such highprotein doses may not be needed with this antibody to achievefavorable biodistribution. Our preliminary data have indicated that inmost patients, a more favorable targeting may be obtained with 20—50mg protein compared with 2 or 100 mg. Most importantly, we alsohave found that the antibody clearance, and, therefore, the normalorgan dosimetry, are also influenced by the protein dose given. Basedon these exploratory data, we intend to administer the same antibodyprotein dose, based on the patient's body weight (0.75 mg/kg), in ourdiagnostic and therapeutic injections. Keeping the protein dose constant (only adjusted for body weight) also will assure that any antitumor effect that may be attributed to the unlabeled antibody alonewould be the same among patients. The antitumor effect related toradiation alone then could be assessed more accurately. We have hadonly limited experience with injection of unlabeled antibody prior toradiolabeled antibody infusion. Although only one patient was studied, we are concerned that preinjecting unlabeled antibody, in someinstances, actually may decrease both the tumor dose and the tumor:
red marrow ratio, perhaps due to partial saturation or “blocking―of the
59055
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

TREATMENT OF NHL WITH ‘31l-LL2ANTI-CD22 MAb
Fig. 3. Targeting of focal bone and bone marrowdisease with ‘311-hLL2.Anterior and posterior viewsof the chest (upper row) and pelvis (lower row) showthoracic spine involvement and focal involvement ofthe pelvic bones.
accretion and longer retention with ‘‘‘Inand @°Y-labeledLL2 thanwith ‘311-LL2,yielding a 2—3-foldimprovement in radiation dose totumor (32). Although this may enhance the therapeutic activity of
@°Y-LL2in comparison with ‘31I-LL2, the higher retention of @°Yin
the bone, combined with its higher energy, also may result in highermyelotoxicity of @°Y-labeledantibody (14—15). Thus, a clear thera
peutic advantage of @°Y-labeledLL2 has to be established empirically. Clinical trials, therefore, are planned to determine whether@°Y-LL2may be a more effective therapeutic agent.
Another important issue is the possible role for chimeric or human
ized anti-B-cell lymphoma antibodies in the diagnosis and treatmentof lymphoma, considering the low incidence of antiglobulin responsein lymphoma patients. Both Press et a!. (10) and Kaminski et a!. (9)have administered up to three infusions of antibodies in the samepatients at approximately 1-week intervals, at even higher proteindoses, without HAMA occurring in this period. HAMA also has notbeen a major problem in patients who have received diagnostic or
therapeutic doses of ‘31ImLL2IgG. Most patients could receive atleast two antibody infusions given within a 1-week period. HAMAdoes develop, however, after frequent injections. Fourteen (33%) ofthe 43 patients treated at the University of Washington with antiCD2O antibodies developed HAMA response 2—76weeks (median, 5weeks) after exposure to murine antibodies (10). Four of 10 patientsgiven two injections of mLL2 also developed low levels of HAMA,and only one of three patients who were given more than threeinjections of LL2 failed to develop HAMA. Thus, there is a rationalefor the development of chimeric and humanized LL2, particularly ifmultiple treatments with radiolabeled antibodies are planned. In thisregard, we are encouraged with the similar tumor targeting betweenthe murine and the humanized or chimeric forms of LL2 in NHLpatients.
Radiolabeled LL2 has shown promise in the treatment of advanced,chemotherapy-refractive NHL. The chimeric and humanized formsshow a similar targeting and biodistribution behavior to the murineform and are expected to result in less immunogenicity. The therapeutic efficacy of LL2, a rapidly internalizing antibody, may be
5906s
antigenic sites on lymphoma cells, combined with the slower bloodclearance. The different effects between variable-size tumors may berelated to their different vascularization, thus resulting in a variabledegree of antigenic saturation caused by the preinfused unlabeledantibody. Based on these initial results, we have chosen to coinfuse
the unlabeled antibody with the radiolabeled material.Our initial experience with the high-dose RAff schedule has been
encouraging. Two partial responses have been seen in the first twopatients who could be assessed. The third patient, who died within 1month of treatment, had extensive disease involving the liver andstomach and, thus, could not be evaluated for response. Higher tumorradiation doses should be possible to achieve when the dose escalationproceeds beyond our starting dose of 90 mCi/m2 (156 mCi in a 70-kgpatient). More durable and complete responses may then be achieved.
Myelotoxicity has been dose limiting and difficult to predict. Theradioactive dose administered, the red marrow dose based on blood,
and the total body dose all failed to predict myelotoxicity. Oneimportant finding was that the red marrow dose based on imaging
(sacral scintigraphy) may provide a better estimate of the red marrowdose and a better predictor of myelotoxicity. Diffuse bone marrowuptake (either due to red marrow involvement or uptake by hyperproliferative normal B cells) will result in increasing the radiationdose to the red marrow through spillover radiation from targeted cells.There is, therefore, a rationale for using antibody imaging to providea better estimate of the radiation dose to the red marrow in thesepatients than that obtained with conventionally used methods, such asblood or whole-body measurements.
The choice of the ideal radioisotope is an important issue in RAIT.LL2 is internalized rapidly when bound to lymphoma cells in vitro,and 50% of the antigen is reexpressed within 5 h (15—17).Internalization and rapid reexpression of the antigen may be exploited for LL2if radiometals, such as ‘‘tIn or @°Y,which have a higher intracellularretention than iodine after radioantibody degradation (31), are used fortumor targeting. ‘‘‘InLL2is retained by lymphoma cells in vitro,whereas ‘31ILL2is processed quickly, with liberation of @Iinto themedia (32). Tumor-bearing nude mice have shown a higher tumor
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

TREATMENT OF NHL WITH ‘311-LL2ANTI-CD22 MAb
improved by using a therapeutic radiometal, such as 90Y. Therefore,clinical trials are underway to test these suppositions.
References
1. Meagher, K. J., Giffen, C. A., Barrett, M. J., Brooks, E. M., Helsel, w. E., andSmucker, R. C. Cancer Statistics Review 1973—1986.in: L. A. Gloeckler Ries (ed),NIH Publication No. 89—2789.Bethesda, MD: NIH, Public Health Services, 1989.
2. Appelbaum, F. R., Sullivan, K. M., Bucker, C. D., Clift, R. A., Deeg, H. J., Fefer, A.,
Hill, R., Mortimer, J., Neiman, P. E., Sanders, J. E., Singer, J., Stewart, P., Storb, R.,and Thomas, D. E. Treatment of malignant lymphoma in 100 patients with chemotherapy, total body irradiation, and marrow transplantation. J. Clin. Oncol., 5: 1340—1347,1987.
3. Freedman,A. S., Takvorian,T., Anderson,K. C., Mauch,P., Rabinowe,S. N., Blake,K.,Yeap, B., Soiffer, P., Coral, F., Heflin, L, Ritz, J., and Nadler, L. M. Autologous bonemarrow transplantationin B-cell non-Hodgkin's lymphoma:very low treatment-relatedmortalityin 100patients in sensitiverelapse. J. Clin. Oncol., 8: 784—791,1990.
4. Armitage, J. 0. Bone marrow transplantation in the treatment of patients with
lymphoma. Blood, 73: 1749—1758, 1989.5. DeNardo, S. J., DeNardo, G. L., O'Grady, L. F., Levy, N. B., Mills, S. L., Macey,
D. J., McGahan, J. P., Miller, C. H., and Epstein, A. L. Pilot studies of radioimmunotherapy of B cell lymphoma and leukemia using 1-131 Lym-l monoclonal antibody.AntibodyImmunoconj.Radiopharm..I: 17-33,1988.
6. Press, 0. W., Eaty, J. F., Badger, C. C., Martin, P. J., Applebaum, F. R., Levy, R., Miller,R., Brown, S., NeIp, W. B., Krohn, K. A., Fisher, D., DeSantes, K., Porter, B., I(idd, P.,Thomas, E. D., and Bemstein, I. D. Treatmentof refractorynon-Hodgkin's lymphomawith radiolabeled MB-I (anti-CD37) antibody. J. Clin. Oncol., 7: 1027—1038,1989.
7. Goldenberg, D. M., Horowitz, J. A., Sharkey, R. M., Hall, T. C., Murthy, S.,
Goldenberg, H., Lee, R. E., Stein, R., Siegel, J. A., Izon, D. 0., Burger, K., Swayne,L. C., Belisle, E., Hansen, H. J., and Pinsky, C. M. Targeting, dosimetry, andradioimmunotherapy of B-cell lymphomas with iodine-l31-labeled LL2 monoclonalantibody. J. Clin. Oncol., 9: 548—564, 1991.
8. Kaminski, M. S., Fig, L. M., Zasadny, K. R., Koral, K. F., DelRosario, R. B., Francis,
I. R., Hanson, C. A., Normolle, D. P., Mudgett, E., Liu, C. P., Moon, S., Scott, P.,Miller, R. A., and WahI, R. L. Imaging, dosimetry, and radioimmunotherapy withiodine 131-labeled anti-CD37 antibody in B-cell lymphoma. J. Clin. Oncol., 10:1696—1711,1992.
9. Kaminski, M. S., Zasadny, K. R., Francis, I. R., Milik, A. W., Ross, C. W., Moon,S. D., Crawford, S. M., Burgess, J. M., Petry, N. A., Butchko, G. M., Glenn, S. D.,and Wahl, R. L. Radioimmunotherapy of B-cell lymphoma with @3I‘I]anti-Bl(antiCD2O)antibody. N. EngI. J. Med., 329: 459—465,1993.
10. Press, 0. W., Eary, J. F., Appelbaum, F. R., Martin, P. J., Badger, C. C., Nelp, W. B.,Glenn, S. G., Butchko, G., Fisher, D., Porter, B., Matthews, D. C., Fisher, L. D., andBernstein, I. D. Radiolabeled-antibody therapy of B-cell lymphoma with autologousbone marrow support. N. Engl. J. Med., 329: 1219—1224, 1993.
I I . DeNardo, G. L., DeNardo, S. J., O'Grady, L. F., Levy, N. B., Adams, G. P., and Mills,S. L. Fractionated radioimmunotherapy of B-cell malignancies with ‘311-Lym-l.Cancer Res., 50: 1014—1016,1990.
12. Buchsbaum, D. J., ten Haken, R. K., Heidom, D. B., Lawerence, T. S., Glatfelter,A. A., Terry, V. H., Guilbault, D. M., Steplewski, Z., and Lichter, A. S. A comparisonof ‘@‘Imonoclonal antibody 17—lAtreatment to external beam radiation on thegrowth of LS174T human colon carcinoma xenografts. tnt. J. Radiat. Oncol. Biol.Phys., 18: 1033—1041,1990.
13. Mackiis,R. M., Beresford,B.A., andHumm,J.L. Radiobiologicstudiesof low-doserate Y-90-lymphoma therapy. Cancer (Phila.), 73: 966—973, 1994.
14. O'Donoghue, J. A. The impact of tumor cell proliferation in radioimmunotherapy.Cancer (Phila.), 73: 974—980, 1994.
15. Stein, R., Belisle, E., Hansen, H. J., and Goldenberg, D. M. Epitope specificity of theanti-B-cell lymphoma monoclonal antibody, LL2. Cancer Immunol. Immunother.,37:293—298,1993.
16. Pawlak-Byczkowska, E., Hansen, H. J., Dion, A. S., and Goldenberg, D. M. Two newmonoclonal antibodies, EPB-1 and EPB-2, reactive with human lymphoma. CancerRes., 49: 4568—4577,1989.
17. Shih, L. B., Lu, H. H-Z., Xuan, H., and Goldenberg, D. M. Internalization andintracellular processing of an anti-B-cell lymphoma monoclonal antibody, LL2. tnt. J.Cancer, 56: 538—545, 1994.
18. Kreitman, R. J., Hansen, H. J., Jones, A. L., FitzGerald, D. J. P., Goldenberg, D. M.,and Pastan, I. Pseudomonas exotoxin-based immunotoxins containing the antibodyLL2 or LL2-Fab' induce regression of subcutaneous human B-cell lymphoma inmice. Cancer Res., 53: 819—825,1993.
19. Weadock, K. S., Sharkey, R. M., Varga, D. C., and Goldenberg, D. M. Evaluation ofa remote radioiodination system for radioimmunotherapy. J. Nucl. Med., 31: 508—511, 1990.
20. Bigler, R., Zanzonico, P. B., Leonard, R., Cosma, M., Primus, F. J., Alger, E.,
DeJager, R., Stowe, S., Ford, E., Brennan, K., and Goldenberg, D. M. Bonemarrow dosimetry for monoclonal antibody therapy. in: Proceedings of the 4thInternational Radiopharmaceutical Dosimetry Symposium, pp. 535—544. OakRidge, TN: Oak Ridge National Laboratory, 1985.
21. Siegel, J. A., Lee, R. E., Pawlyk, D., Horowitz, J. A., Sharkey, R. M., andGoldenberg, D. M. Sacral scintigraphy for bone marrow dosimetry in radioirnmunotherapy. mt. J. AppI. Radiat. Instrum., 16: Part B, 553—559,1989.
22. Loevinger, R., and Berman, M. A revised scheme for calculating the absorbed dosefrom biologically distributed radionuclide. In: Medical Internal Radiation Dose,Pamphlet 1, revised. New York: Society of Nuclear Medicine, Inc., 1976.
23. van Rensburg, A. J., Latter, M. G., Heyns, A. P., and Minnear, P. C. An evaluationof four methods of In-l 11 planar image quantification. Med. Phys. (NY), 15:853—861,1988.
24. Siegel, J. A., Wu, R. K., and Maurer, A. H. The buildup factor@effect of scatter onabsolute volume determination. J. Nucl. Med., 25: 390—394, 1985.
25. Siegel, J. A., Goldenberg, D. M., Sharkey, R. M., Hall, T. C., Murthy, S., Lee. R. E.,Pawlyk, D. A., and Swayne, L. C. Tumor and organ dosimetry for 1-131-labeled LL2(EPB2) monoclonal antibody in patients with B-cell lymphomas. Antibody Immunoconj. Radiopharm., 4: 649—654,1991.
26. Primus, F. J., Kelley, E. A., Hansen, H. J., and Goldenberg, D. M. “Sandwich―-typeimmunoassay for carcinoembryonic antigen in patients receiving murine monoclonalantibodies for diagnosis and therapy. Clin. Chem., 34: 261—264,1988.
27. DeNardo, G. L., DeNardo, S. J., Macey, D. J., Shen, S., and Kroger, L. A. Overview
of radiation myelotoxicity secondary to radioimmunotherapy using ‘31Lym-las amodel. Cancer, 73: l038s—l048s,1994.
28. Juweid, M., Sharkey, R. M., Dunlop, D., Dunn, R., Siegel, J. A., and Goldenberg, D.M. Estimates of red marrow dose by sacral scintigraphy in radioimmunotherapypatients with non-Hodgkin's lymphoma and diffuse bone marrow uptake. CancerRes.,55 (Suppl.):5827—5831,1995.
29. Sharkey, R. M., Goldenberg, D. M., Murthy, S., Pinsky, H., Vagg, R., Pawlyk, D.,Lee, R. E., Siegel, J. A., Wong, G. Y., Gascon, P., Izon, D. 0., Vezza, M., Burger,K., Swayne, L. C., Pinsky, C. M., and Hansen, H. J. Clinical evaluation of tumortargeting with a high-affinity, anticarcinoembryonic-antigen-specific, murine monoclonal antibody, MN-14. Cancer (Phila.), 71: 2082—2096, 1993.
30. Scheinberg, D. A., Straus, D. J., Yeh, S. D., Divgi, C., Garin-Chesa, P., Graham, M.,Pentlow, K., Coit, D., Oeugen, H., and Old, L. J. A Phase I toxicity, pharmacology,and dosimetry trial of monoclonal antibody OKB7 in patients with non-Hodgkin'slyrnphoma: effects of tumor burden and antigen expression. J. Clin. Oncol., 8:792—803, 1990.
31. Duncan, J. R., and Welch, M. J. Intracellular metabolism of indium-I 1l-DTPAlabeled receptor targeted proteins. J. NucI. Med., 34: 1728—1738,1993.
32. Behr, T. M., Sharkey, R. M., Juweid, M., Aninipot, R., Mattes, M. J., Stein, R.,Griffiths, G. L., and Goldenberg, D. M. Residualizing (indium, yttrium) versusreleased (iodine) isotopes in radioimmunodetection and therapy with internalizingantibodies (Abstract). J. NucI. Med., 36: 20, 1995.
59075
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from
1995;55:5899s-5907s. Cancer Res Malik Juweid, Robert M. Sharkey, Adeline Markowitz, et al. AntibodyMurine, Chimeric, or Humanized LL2, an Anti-CD22 Monoclonal Treatment of Non-Hodgkin's Lymphoma with Radiolabeled
Updated version
http://cancerres.aacrjournals.org/content/55/23_Supplement/5899s
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/55/23_Supplement/5899sTo request permission to re-use all or part of this article, use this link
Research. on October 12, 2019. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from