treatment thyrotoxicosis - postgraduate medical...
TRANSCRIPT

282
¥THE TREATMENT OF THYROTOXICOSIS
By VICTOR RIDDELL, M.D., F.R.C.S.Surgeon, St. George's Hospital
~~~~~~~~~~~~..........i:!:'iizl~,~ i: :i ;,ii~~% j ~~ ....
TET *::l*... ... I*
. .:..: ..:: .::?~;?5.;?:~7~?~?:~·iii·:ii. .'...
-. .. .. ··
....... ................... .. .....iii
...... .. ..
.... .. ...... .. ..... ...-
-... ........::.... "'.................
L.
FIG. I.-Primary thyrotoxicosis: Grave's disease (exoph-thalmic goitre). Treated with thiouracil but re-lapsed. Stabilized following sub-total thyroidec-tomy.
Toxic GoitreIt is convenient to retain the terms primary
toxic goitre and secondary toxic goitre or toxicnodular goitre, although the one merges im-perceptibly into the other, if for no other reasonthan that the extreme examples of these twovarieties (Figs. i and 2) usually require different
management. Secondary toxic goitre is bettercalled toxic nodular goitre because it is the nodularelement when this is marked, rather than the toxicelement, which differentiates this group from theprimary toxic goitres and is responsible for thespecial treatment (usually surgical) which they mayrequire. In toxic goitre the particular clinical
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

N4ne I953 RIDDELL: The Preatment of Thyrotoxicosts
-1S|i,-12".
.ii?i~!';i!?
..,..........
·:.l`....u.
..·i
'-?:~ii!i:;~ii;i,:i,:,J.::;' ::',...,., ··
- q: '-
.) A. .. ':..'":.'.' ... .
......:...........-;.
FIG. 2.-Secondary thyrotoxicosis (toxic nodular goitre).
picture produced is the result of the interplay oftwo factors-the thyroid gland on the one handand the tissues on the other. The gland can reacttotally if normal or only partially if nodular to theprovoking stimuli. The tissues can resist the re-sulting toxaemia vigorously or feebly. Age is thecatalyst in the reaction. The most unfavourablecircumstances will be achieved when the gland re-acts maximally and the tissues resist minimally.Fortunately the conditions most likely to producethis state of affairs do not commonly go together,for they imply a young gland and old tissues.
The Presenting Symptom. If the presentingsymptom is associated with goitre or exophthalmos,the diagnosis is straightforward, but it is not im-possible to miss a case of hyperthyroidism if thereis no goitre and there are no eye changes-so-calledmasked hyperthyroidism, e.g. one patient maycomplain only of loss of weight, another only ofswelling of the ankles and another only of sterilityor amenorrhoea.
Anti-Thyroid AgentsThe whole trend of therapy in thyrotoxicosis
has been transformed in recent years by the dis-covery and introduction of the anti-thyroid sub-stances. They have ushered in a new era of safetyin thyroid surgery and they have rendered obsoletein all but the most exceptional cases the need forindividual ligation of arteries and multiple stageoperations.By their agency a small group of patients with
thyrotoxicosis can be cured or at least controlledwithout resort to surgery. For the remainder,surgery following upon a course of one of the anti-thyroid agents may be necessary, but by enablingus for the first time to fulfil our main pre-operativeobjective-the conversion of a toxic into a non-toxic goitre-they have removed much of thehazard and increased the accuracy of the operation.When we speak today of the surgical treatment
of thyrotoxicosis we infer treatment by combinedmedicine and surgery. Surgery is only the cul-minating act in the final phase of a combinedmethod. In comparing the merits of the purelymedical and the combined procedures it is im-portant to bear in mind the altered circumstancesin which thyroid surgery is conducted today. The
B2
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

28·POSTGRADU~ATE MEDICA;L jOURNA L jtune x951
:i84'
FIG. 3.-Thiouracil therapy. A patient suffering fromthiouracil overdosage which has produced athiouracil goitre and myxoedema with thickeningof the vocal cords.
adverse conditions which existed prior to 1943,when surgery so often had to be undertaken underthe unfavourable conditions of uncontrolledtoxicity, no longer exist, as a direct result of theintroduction of the anti-thyroid substances.
This event has had its effect upon both patientand surgeon. It is now in our power to make thepatient safe for surgery to a degree unknown priorto the thiouracil era. It is also in our power tomake surgery safer for the patient, since there is nolonger the same necessity for speed in operating asthere was in the constitutionally ill and toxicsubject. One great advantage which an unhurriedoperation affords is that it allows time for the de-liberate identification of the parathyroid glands andrecurrent laryngeal nerves so that the incidence ofdamage to these important structures has fallen.Equally important, a more accurate assessment ofthe amount of gland to be resected can be made-a key decision in the operation, for nothing brings
thyroidectomy for toxic goitre into such disreputeas inadequate procedures.While the present satisfactory position is in part
due to modern anaesthetic agents and methods it isin greater measure due to the thiouracils. It isincumbent therefore upon all surgeons using theantithyroid drugs for the pre-operative stabiliza-tion of their patients to be familiar with theirpotentialities. In addition it is essential to see thepatients with their physician in their originalthyrotoxic state before therapy is initiated. If seenfor the first time when a thiouracil effect has beenobtained, an entirely false assessment of theseverity of the disease may be made and a wrongdecision come to as to the need or time forsurgical intervention.
The ThiouracilsAction. The anti-thyroid agents most com-
monly employed are methyl and propyl thiouracil.
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from
June 1953 RIDDELL: The Treatment of Thyrotoxicosis 285
~~~~~~'"':!11i~11ii
-':·::i.~%IIaet~PS~s IM
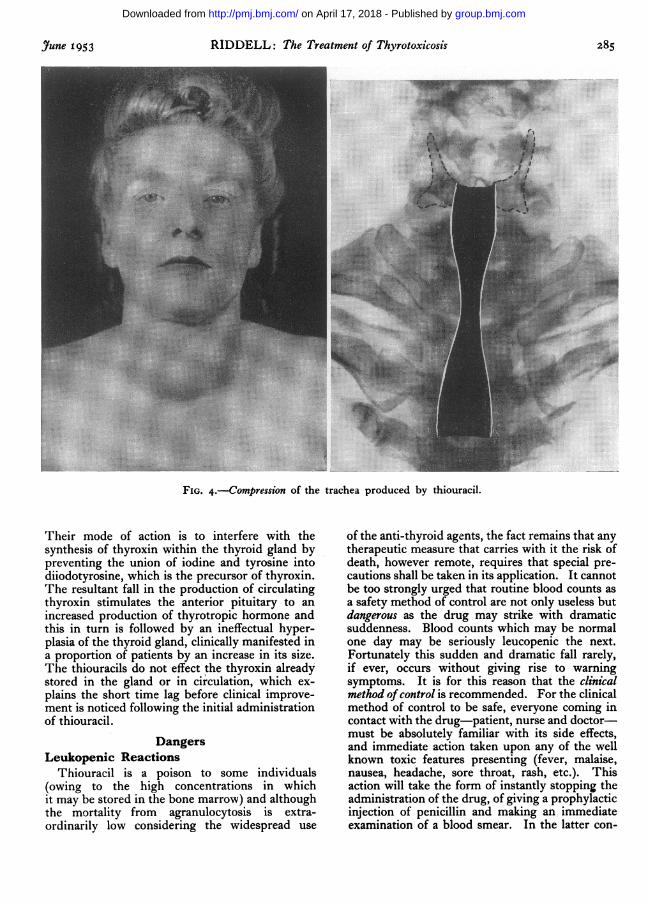
FIG. 4.-Compression of the trachea produced by thiouracil.
Their mode of action is to interfere with thesynthesis of thyroxin within the thyroid gland bypreventing the union of iodine and tyrosine intodiiodotyrosine, which is the precursor of thyroxin.The resultant fall in the production of circulatingthyroxin stimulates the anterior pituitary to anincreased production of thyrotropic hormone andthis in turn is followed by an ineffectual hyper-plasia of the thyroid gland, clinically manifested ina proportion of patients by an increase in its size.The thiouracils do not effect the thyroxin alreadystored in the gland or in circulation, which ex-plains the short time lag before clinical improve-ment is noticed following the initial administrationof thiouracil.
DangersLeukopenic Reactions
Thiouracil is a poison to some individuals(owing to the high concentrations in whichit may be stored in the bone marrow) and althoughthe mortality from agranulocytosis is extra-ordinarily low considering the widespread use
of the anti-thyroid agents, the fact remains that anytherapeutic measure that carries with it the risk ofdeath, however remote, requires that special pre-cautions shall be taken in its application. It cannotbe too strongly urged that routine blood counts asa safety method of control are not only useless butdangerous as the drug may strike with dramaticsuddenness. Blood counts which may be normalone day may be seriously leucopenic the next.Fortunately this sudden and dramatic fall rarely,if ever, occurs without giving rise to warningsymptoms. It is for this reason that the clinicalmethod of control is recommended. For the clinicalmethod of control to be safe, everyone coming incontact with the drug-patient, nurse and doctor-must be absolutely familiar with its side effects,and immediate action taken upon any of the wellknown toxic features presenting (fever, malaise,nausea, headache, sore throat, rash, etc.). Thisaction will take the form of instantly stopping theadministration of the drug, of giving a prophylacticinjection of penicillin and making an immediateexamination of a blood smear. In the latter con-
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from
286 POSTGRADUATE MEDICAL JOURMAL Yune I953
..IODINE.20oz(56 9)
..: ..:.. .............
;"d-. A~
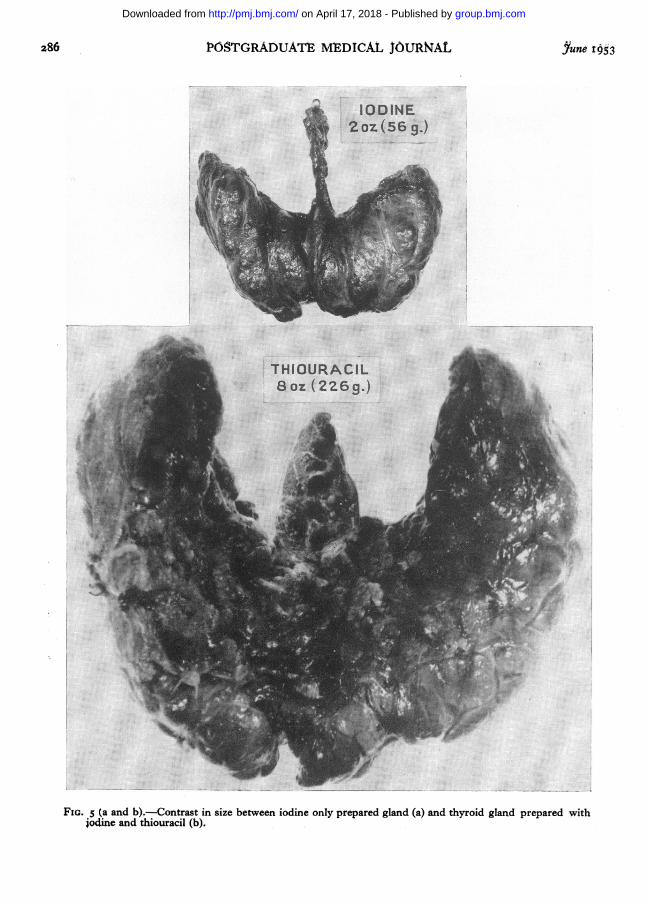
FIG. 5 (a and b).-Contrast in size between iodine only prepared gland (a) and thyroid gland prepared withjodine and thiouracil (b).
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

June 1953 RIDDELL: The Treatment of Thyrotoxicosis 287
nection a formal differential count-unless thepolymorphs are alarmingly scanty-is unnecessaryand time consuming. It is a simple matter for anexperienced pathologist to tell from a smear, almostat a glance, whether the granulocytes are plentifulor not. If the granulocytes are scanty it will bewise to abandon thiouracil therapy altogether;after the blood count returns to normal the patientshould be put on to iodine and followed up with athyroidectomy. If the granulocytes are plentifulafter a toxic reaction, it is sufficient to wait a weekand then to switch to another anti-thyroid agent-for example from methyl to propyl thiouracil.Toxic effects-once they have subsided-with theexception of persistent leucopenia, do not contra-indicate the continuation of treatment. In usingthe term leucopenia it should be borne in mindthat an absolute polymorphonuclear count whichis a neutropenia for one person is not necessarily aneutropenia for another. The interpretation of theterm must be related to the pretherapy normalcount-hence the importance of this count for pur-poses of comparison subsequently. Thus, apatient with a normal high count of, say, 5,000polymorphs which drops to I,500 polymorphs isto be regarded more seriously than a patient witha low normal of, say, 3,000 polymorphs whichdrops to I,5oo, the first representing a drop of70 per cent. and the second a drop of 50 per cent.
Thiouracil Goitre and MyxoedemaHigh dosage-if prolonged-will produce
a thiouracil goitre (Fig. 3).It is very undesirable that overdosage with
antithyroid agent should occur. The resultantthiouracil goitre ' may cause pressure symptoms
and force surgery while the gland is still enlargedand vascular and so greatly increase the tech-nical difficulties of the operation (Fig. 4). Thethickening of the vocal cords which takes placein the myxoedematous phase also constitutesa very real post-operative danger from oedema ofthe glottis. Tracheotomy was required in threepatients operated upon at the Lahey Clinic duringthe myxoedematous phase (Cattell, I949).
Furthermore in spite of what has been writtento the contrary my experience is that an irreversi-ble state may be set up if myxoedema is producedby anti-thyroid agents or at least a state whichtakes a long time to adjust itself. In addition itcomplicates the surgeon's decision as to how muchthyroid to remove at operation and post-operativelyseriously retards the patient's return to normalhealth and thyroid function.
BleedingThiouracil produces effects upon the gland of
primary toxic goitre which only occur minimally
or not at all in the nodular thyroid of the olderpatient. It increase3 the size of the gland, rendersits consistency hard and rigid and so restricts itsmobility at operation and increases its vascularitymany times (Fig. 5a, b).
It is important to be aware of these effects,and so prepared for the very severe bleedingwhich can occur at operation. If this comesas a surprise it may well extend the most ex-perienced surgeon. Much can be done to diminishthe technical difficulties associated with the alteredphysical state of the gland (i) by careful preparationwith iodine, (ii) by avoiding pre-operative over-dosage with thiouracil and (iii) by a sense of timingin the choice of the optimum moment for theoperation, but despite observing these precautionsthere will still be occasional cases calling for allthe operator's skill if bleeding is to be controlled,an adequate amount of gland removed and nodamage inflicted upon either of the recurrentlaryngeal nerves.
DosageGrowing experience shows that there is little
to choose between methyl and propylthiouracil.They both produce the same effect in the samedosage, in the same time and with much thesame reaction rate. It seems probable that theearlier doses used were too high-the maximuminitial dosage should not exceed 200 mgm. twicea day and in many cases an excellent response willbe obtained from half this dose (Figs. 6 and 7).Because of its availability methyl thiouracil hasbeen used in this country more than the propylcompound and perhaps for this reason acquired areputation for having a higher toxic reaction rate;in practice there is little difference in the respectivereaction rates, approximately one in five patientsshowing some toxic manifestation. It is, however,worth bearing in mind that a patient who is sen-sitive to one form of anti-thyroid agent may re-spond normally to another, for example to Mer-cazole (i methyl: 2 mercaptomidazole-averagecomparable dosage, 2 to 4 mgm. b.d.), so thatafter a brief interruption treatment may becontinued with safety.
Administration-General ManagementThiouracil can be used in combination with
surgery as a pre-operative agent with a view tobringing the patient to a safe operative level, or itsadministration can be prolonged with a view toobtaining stabilization without operation-chemi-cal thyroidectomy so to say.
In-patient treatment is advisable for all cases atthe outset but this can give way to treatment as anout-patient as soon as the patient seems well andstrong enough to make the necessary journeys to
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

288 POSTGRADUATE MEDICAL JOURNAL June 1953
aa"" ::' ....... .... ..
:............
FIG. 6.-Thiouracil therapy. A patient with severeprimary thyrotoxicosis who was brought to a safeoperative level with thiouracil and iodine (see con-secutive photograph).
attend regularly, i.e. at weekly intervals at first,though this period can be lengthened as the courseproceeds.To Medical Cases-Thiouracil as a PermanentStabilising AgentThe initial management of all patients is the
same; the patient is admitted for a period ofobservation during which, apart from a generalexamination, a pre-therapy B.M.R. and a 'base-line' differential W.B.C. are done, the weighttaken, the neck measured and X-rayed to excludedeviation or compression of the trachea andretro-sternal goitre, and cardiological and otheropinions obtained when in doubt. All toxicpatients should, in addition, be interviewed by amature and sympathetic almoner, and in excep-tional cases by a psychiatrist, so that we may befamiliar with the home housing conditions andother relevant social and personal factors. After
the first few days of the resting phase mostpatients should be allowed to go to the bathroomand to get up for a short time each evening.Having weighed all the available data the
selected anti-thyroid agent is started and continuedin its initial dosage until the patient is symptomfree. Progress is assessed by observing an im-provement in the patient's general clinical con-dition-usually first noticed at the end of tendays-by a fall in the B.M.R. and pulse rate, andby an increase in weight. When symptom freethe dosage is halved and gradually reduced duringthe course of the next three months, after which asmaller or maintenance dose is substituted andmaintained for a minimum period of six months. Ifat the end of this time the patient remains symptomfree the thiouracil is stopped and the patient pro-visionally discharged with instructions to reportfor reassessment in three months' time or beforeif there is a recurrence of the thyrotoxic symptoms.If this regime is followed, few patients will or
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

yune I953 RIDDELL: The Treatment of Thyrotoxicosis 289
~·a
.?j
::..:
.. .... .::
I.....:... .:
===......;.........;:;.::'.···
:'.':.:.. ·`"l'I; ::::8 ...
.tl(. ". :·· ...:.::..''·· ?;::':..'...·... . : ::::::::....
'.."~~~~~~··;':~: '"J :il'::':"
·*-::,.. . . . ' . . . . :r.:.:~,.;:.:.
FIG. 7.-Thiouracil therapy. The same patient aftersix weeks on methyl thiouracil to show the optimumresponse to this anti-thyroid agent.
should be free from supervision and therapy inless than one year.While thiouracil treatment is continuing it is
usual, although not essential, to have a white cellcount at fortnightly intervals. A second B.M.R.estimation during the course of therapy may alsobe a useful guide to the duration of therapy andoccasionally may give valuable warning of im-pending hypothyroidism.An initial pre-therapy white cell count below
3,000 associated with neutropenia contra-indicatestreatment with thiouracil.
RelapsesSo far as it is possible to judge, approximately
half the patients on thiouracil alone relapsefollowing the first full course of thiouracil anda substantial number of those that relapse, re-lapse again following a second course. The in-ference is that the relapser goes on being a relapserwith repeated courses, but it is only fair to saythat of those that relapse a proportion only arethiouracil failures and others relapse because of the
persistence of the original precipitating factor suchas domestic or financial worry.
Relapses, if they are going to occur, tend tohappen quickly, i.e. within two to four months ofstopping treatment. Short courses of thiouracilare followed by a high relapse rate, so that treat-ment with anti-thyroid agents must be continuedfor a substantial period-not less than six monthsafter the patient has become symptom free.The permanency of the remission induced by
thiouracil is not yet known, as thiouracil therapyhas only been available since 1943, nor is it knownif its carcinogenic properties in certain animals willever produce cancer in man. Time alone willdecide these points for us.
To Surgical Cases-Thiouracil as a TemporaryStabilising AgentThe initial procedure when using thiouracil
as a pre-operative agent is the same as for medicalcases. Administration continues until the patientis symptom free, or ideally, just short of thispoint when the drug is stopped altogether.
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

290 POSTGRADUATE MEDICAL JOURNAL June I 953
..:.·-·.' ...·X· iii
"":·i:' ...: ::*':
"":ji: ·-·
I..
Medica!treamen fig. 8 I
FIG. 8.-Mild thyrotoxicosis. Full and lasting recoverywith sedation, rest and change of occupation.
FIG. io.-Recurrent thyrotoxicosis with nerve lesion onopposite side.
In cases of primary thyrotoxicosis, if the thiouraciltherapy before operation has been prolonged,iodine (minims x, t.d.s. in milk) should be givenfor a period of at least three, and sometimesfour, weeks-the first two of which can over-lap with the last two weeks of the thiouraciltherapy. The usual short course of Io to I2 days issufficient in cases of toxic nodular goitre as theyhave not the same tendency to bleed. Thosepatients who have been receiving the terminal partof their ihiouracil course as out-patients may withadvantage begin their pre-oFerative iodine beforethey return to hospital, which should be not lessthan three days before the anticipated day of opera-tion.
Delayed thiouracil reactions have been reportedso that it is wise to wait a week after the termina-tion of thiouracil therapy before operating and thisinterval has also the advantage of enabling theiodine to produce its full devascularizing effect,which cannot be achieved in ten days. Finally,a post therapy pre-operative white cell countshould be carried out on the day before operationto exclude a delayed leucopenic reaction. In cal-culating the optimum day for operation it is im-portant not to forget to take into consideration thedate of onset of the next menstrual period.
Differences in Response-Clinical Improvement.Clinical improvement, which occurs more rapidlyin primary than in secondary toxic goitres, ismanifested by an abatement of the symptoms, anincrease in weight and a fall in the sleeping pulserate. The B.M.R. averages a drop of a point a dayin primary and a point every other day in secondarytoxic goitres, so that a patient with primary thyro-toxicosis and a B.M.R. of plus 42 who is to have athyroidectomy can be told that it will take aboutsix weeks to prepare her for operation.
THE THREE GROUPSDefinitive TreatmentWhen faced with a thyrotoxic patient, who may
be young or old, who may be with or without en-largement of the thyroid gland and with or with-out the classical features of the disease, it can beperplexing to make up one's mind as to the mostsuitable definitive line of treatment.
In practice it will be found that the majority ofthyrotoxic patients when first seen can be dividedinto three groups:A medical group in whom there is present a
special indication for medical treatment.A surgical group in whom there is present a
special indication for surgical treatment.
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

June I953 RIDDELL: The Treatment of Thyrotoxicosis 29I
w-o
:. ... .... !!
I'Z ,.': .:....
.. .......;.
............
......... ..';L R1X···7'p'X'S |
'~~ : ·· ' .:,t':.1 (.';::~.
.: .· :i·.·· ···.:.... :. :: ..nB
;:.:
·:·' :::. .:
;e2w=,g'k,I:i·9ili$0ls;s(g%$ ;I; ··t~
FIG. 9.-Recurrent thyrotoxicosis following sub-total thyroidectomy.
A residual group in whom the method of treat-ment can only be decided after a period of trialwith the anti-thyroid agents.
In arriving at a decision as to the appropriateline of treatment in an individual case it is helpfulfirst to exclude those patients who for purposes oftherapy fall naturally into a medical or surgicalcategory. Let us consider first those in whommedical treatment is indicated.
Group i. Medical Treatment-The Indications(i) Mild Thyrotoxicosis (Fig. 8). Medical treat-
ment is indicated in all patients with mild thyro-toxicosis, that is to say, those with a B.M.R. ofplus o2 and a pulse rate of not more than go. Theusual methods of rest and sedation will suffice forthe majority; a few will require thiouracil; surgeryis absolutely contra-indicated.
(ii) Recurrent Thyrotoxicosis. Recurrent thyro-toxicosis might be regarded as the cardinal indica-tion for the use of thiouracil although radio-iodineis now available for the same purpose. Re-operation on these patients is always hazardousbecause of the risk of damaging either or both
inferior laryngeal nerves (Fig. 9). Thiouracil isalso of particular value in treating patients with aunilateral recurrence associated with a recurrentlaryngeal nerve palsy on the side opposite to therecurrence (Fig. io). If the recurrence takes placeon the side of the nerve lesion re-operation can beconsidered with less anxiety as the underlyingnerve has already been damaged.
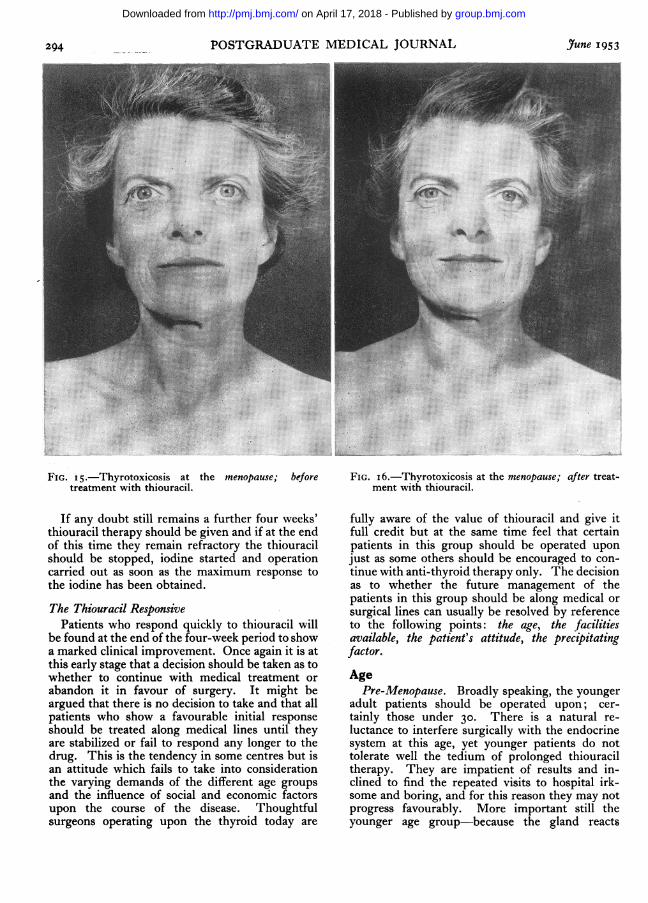
(iii) Age-Stress and Other Factors. Medicaltreatment should be employed whenever possiblein young children (Fig. 1) and in the elderly(Fig. I2) and at times of exceptional physiologicalstress such as puberty (Fig. I3), pregnancy (Fig. 14)and the menopause (Figs. 15 and I6), whenthiouracil cover will generally be all that is neces-sary. In the case of thyrotoxicosis associated withpregnancy it should be stated that it is unnecessaryto interrupt the pregnancy. The danger of pro-ducing sub-thyroid babies as a result of thiouraciltherapy during pregnancy appears to have beengreatly exaggerated, but iodine should replace thethiouracil for the last four weeks before delivery.In those few cases in which the prospectivemother does not tolerate the anti-thyroid agent,
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

292 POSTGRADUATE MEDICAL JOURNAL June 1953.
*M~~e - -
.. -
::
FIG. I I.-Thyrotoxicosis in a child of three; treated withthiouracil; now aged eight and symptom free.
r::.··.'::I·"
:a ··'····:.·i;
..*;-·.er.,;· .:!in'·:H
:··'·:
1·..··a*Jrr ·:·
8'.ii,.Pi:.·;··:·: :.i.':!".··ii!·iii;"i
·/L:'
·.::·
II1;
:··. ·:*:
:"'"'.:i·:;iaas·i:: .!ii.· ·iiLS!i[j..::8iii·i '"·i::i'i::·;·::··'' ·:::··:· ····
:: ·saaiss:iiI·····*:··.i::·I!B;iii:iit?li;i'ii:*-;I·;;;·;;···;::··: ··;:·;·:-·-·:*.
FIG. I2.-Thyrotoxicosis in the elderly; no auricularfibrillation; stabilized on thiouracil.
thyroidectomy during pregnancy after iodine pre-paration may have to be carried out. Thethiouracils are secreted in the milk so that it iswise either to wean the child after birth or to con-tinue with only very small doses to avoid cretinism.
Medical treatment will also be the electiveinitial method in patients in whom thyrotoxicosis iscomplicated by an anxiety state; in patients inwhom a precipitating causal agent is discoveredand can be removed, whether it be physical suchas a septic tooth or tonsil or even a carcinoma ofthe breast, or mental, for example financial worryor housing difficulties; in post-menopausal patientsin whom the thyrotoxicosis is unassociated withpressure symptoms, undule nodularity or cardio-vascular effects; in certain cases of malignantexophthalmos; in poor operative risks and whenexpert surgery is unavailable or refused.Group 2. Surgical Treatment-The Indications
Surgery, as the primary definitive line of treat-ment, is indicated when pressure symptoms arepresent as shown by displacement or compressionof the trachea, or when symptoms of pressuremight be precipitated by the use of thiouracil as ina retrosternal or intrathoracic goitre (Fig. 17).
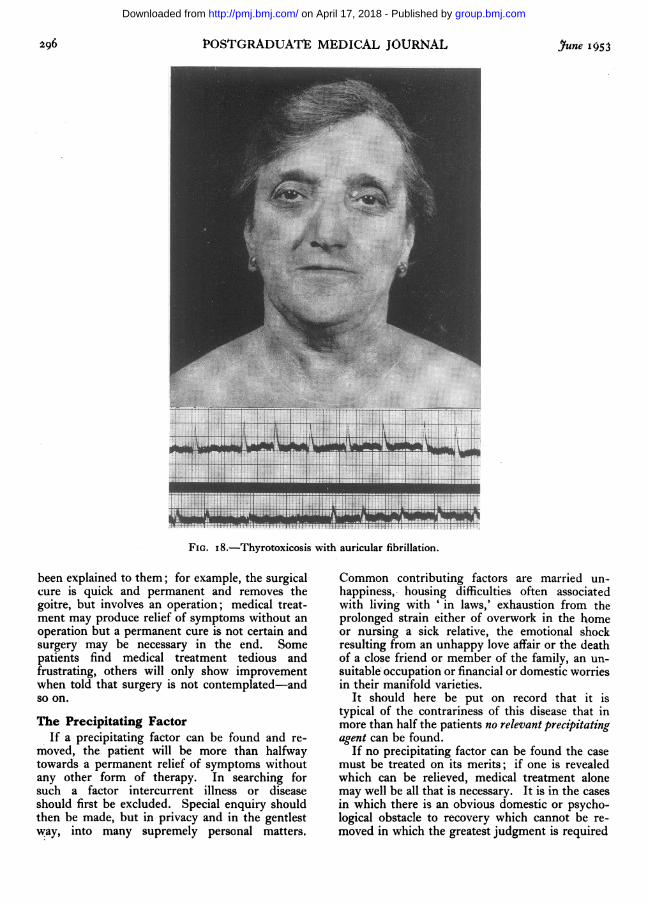
It is also generally agreed that surgery is advis-able in patients with auricular fibrillation or othercardiovascular disturbance attributable to thethyrotoxicosis (Fig. i8). Surgery may also be themost desirable method of treatment in those whoare unable or unwilling to attend regularly, in theunreliable and unco-operative, for social oreconomic reasons and for reasons of size or nodu-larity or because malignancy cannot be excluded.By a process of elimination it also becomes theonly effective expedient in those patients in whommedical treatment has failed, i.e. the thiouracilsensitive, the thiouracil relapses and the thiouracilresistant. There is no reason to withhold anti-thyroid agent in the pre-operative preparation oftoxic patients in the surgical group provided thatit is administered under close supervision andfollowed by iodine in the usual way. In manyinstances there may be a very satisfactory responseto anti-thyroid agents and in approximately one-third of the cases of auricular fibrillation of thyro-toxic origin normal rhythm will be restored.
Group 3. Residual GroupThe exclusion of patients in the two previous
groups leaves us with a large residual group, all of
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

June 1953 RIDDELL: The Treatment of Thyrotoxicosis293
... ......:·::::
E...
ci :..
FIG. 13.-Thyrotoxicosis in puberty and adolescence(age I7). Undergoing treatment with thiouracil.
: -
m }si S.. X......
FIG. 14.-Thyrotoxicosis in pregnancy; thiouracilcover during pregnancy. Post-partum relapseon withholding anti-thyroid agent; sub-totalthyroidectomy after weaning baby.
whom have moderately severe thyrotoxicosis (pulserate 90 to 120) or severe thyrotoxicosis (pulse rateabove 120). This is a group of mixed thyrotoxics,some primary, some secondary, in whom there isno clear-cut indication as to whether they would bebest treated by medical or surgical methods. Ifwe treat all patients in this group surgically, thenwe shall automatically operate upon a number whomight have been cured medically. If we treat allpatients in this group medically for an indefiniteperiod of time we are going to submit a consider-able proportion to a prolonged and eventuallyfruitless course of therapy.The difficulty is that at the first examination we
have no way of predicting which patients will bestabilized by anti-thyroid agents and thereforecould be excluded from surgery, and whichpatients will relapse after medical treatment andwould therefore be better prepared for surgeryfrom the outset. Accordingly all patients withsevere or moderately severe thyrotoxicosis who donot naturally fall into the medical or surgicalcategories mentioned should be submitted to acourse of anti-thyroid agents in order to determinetheir response to the drug.
Therapeutic TrialThe procedure recommended is as follows: Give
to all patients in the residual group a therapeutictest course of thiouracil for a period not exceedingone month or until symptom free, whichever isthe earlier. The situation should then be re-assessed. It is at this early stage that the positionof all these patients should be reviewed and notafter months of thiouracil treatment. Exclud-ing those who fall out because they are thiouracilsensitive two groups will be found to emerge forreassessment-a small group which respondsindifferently and a large group which respondswell to thiouracil.
The Thiouracil Resistant or Dilatory. Thisgroup consists of patients who respond slowly tothiouracil and are dilatory in showing clinical im-provement at the end of the trial period. Ex-perience suggests that the majority of these re-fractory patients will never become completelysymptom free on the anti-thyroid agents atpresent available, however prolonged the use ofthese drugs may be.
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from
294 POSTGRADUATE MEDICAL JOURNAL June 1953
'>s¢
:X: Se
At...: .
*..:..:..
FIG. 15.-Thyrotoxicosis at the menopause; beforetreatment with thiouracil.
.i :i!i!,!! ,,. :~?:^:::::.:.:':i:. ^....
i::'.....r?. <<. : ^' ' . .
.. .;
5~i jci ··: I,iiii
FIG. i6.-Thyrotoxicosis at the menopause; after treat-ment with thiouracil.
If any doubt still remains a further four weeks'thiouracil therapy should be given and if at the endof this time they remain refractory the thiouracilshould be stopped, iodine started and operationcarried out as soon as the maximum response tothe iodine has been obtained.
The Thiouracil ResponsivePatients who respond quickly to thiouracil will
be found at the end of the four-week period to showa marked clinical improvement. Once again it is atthis early stage that a decision should be taken as towhether to continue with medical treatment orabandon it in favour of surgery. It might beargued that there is no decision to take and that allpatients who show a favourable initial responseshould be treated along medical lines until theyare stabilized or fail to respond any longer to thedrug. This is the tendency in some centres but isan attitude which fails to take into considerationthe varying demands of the different age groupsand the influence of social and economic factorsupon the course of the disease. Thoughtfulsurgeons operating upon the thyroid today are
fully aware of the value of thiouracil and give itfull credit but at the same time feel that certainpatients in this group should be operated uponjust as some others should be encouraged to con-tinue with anti-thyroid therapy only. The decisionas to whether the future management of thepatients in this group should be along medical orsurgical lines can usually be resolved by referenceto the following points: the age, the facilitiesavailable, the patient's attitude, the precipitatingfactor.Age
Pre-Menopause. Broadly speaking, the youngeradult patients should be operated upon; cer-tainly those under 30. There is a natural re-luctance to interfere surgically with the endocrinesystem at this age, yet younger patients do nottolerate well the tedium of prolonged thiouraciltherapy. They are impatient of results and in-clined to find the repeated visits to hospital irk-some and boring, and for this reason they may notprogress favourably. More important still theyounger age group-because the gland reacts
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

1yune Ir 953 fDDELL: the treatment of Thyrotoxicosls
''....
:);' -- -^-}
Surgical treatment figs. 17-18FIG. I7.-Retrosternal goitre; thiouracil dangerous.
maximally to the anti-thyroid agent-are moreliable to develop a thiouracil goitre and quitesuddenly to slip over into myxoedema unless veryfrequent and time consuming visits are made to athyroid clinic.
Menopausal and Post-Menopausal. In meno-pausal and post-menopausal patients who areresponding well it is wise to avoid thyroidectomyand to persist rather with anti-thyroid agents ifthese are well tolerated. Commonly a thyrotoxicflare-up during the menopause is a transientmanifestation of the disease and will die down asthe climacteric comes naturally to its end.
Post-menopausal patients, even if the gland isnodular, respond in my experience in a more satis-factory and lasting manner to anti-thyroid agentsthan patients in the younger age groups. Opera-tion will be advisable in those showing displace-ment of the trachea, a retrosternal goitre, or withassociated cardiovascular disease or if there is anysuspicion of malignancy, although coincidence ofthe latter with thyrotoxicosis is exceedingly rare.Post-menopausal patients without these complica-tions should be encouraged to persist with the full
course of anti-thyroid agent and the subsequentmaintenance dose for some months after they havebecome symptom free.
Facilities'availableIf the surgical facilities available are poor;,
as they can be, it will be prudent to continuewith medical treatment. Only if they are gooddoes surgery become an alternative to medicalmethods and it should then be carried out im-mediately the patient has had her pre-operativecourse of thiouracil and iodine. The medicalfacilities available can also be poor-by this Imean the time and care the physician concerned isprepared or able to give to the patient. Con-tinued supervision by one man is essential in thesemixed diseases of psyche and soma and this de-mands both time and patience.The Patient
Patients with thyrotoxicosis are usually in-telligent and their own wishes in regard totreatment must be consulted after the advan-tages and disadvantages of both methods have
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from
296 POSTGRADUATE MEDICAL JOURNAL , une 1953
f!,,:':C
-.... - *
.:i,..-....:.....: ! . ..:!..
*'i,X... l..,-: . . '-:: -
-' . - - - :-"-"t--'...:?'::': e 1
...
FIG. I8.-Thyrotoxicosis with auricular fibrillation.
been explained to them; for example, the surgicalcure is quick and permanent and removes thegoitre, but involves an operation; medical treat-ment may produce relief of symptoms without anoperation but a permanent cure is not certain andsurgery may be necessary in the end. Somepatients find medical treatment tedious andfrustrating, others will only show improvementwhen told that surgery is not contemplated-andso on.
The Precipitating FactorIf a precipitating factor can be found and re-
moved, the patient will be more than halfwaytowards a permanent relief of symptoms withoutany other form of therapy. In searching forsuch a factor intercurrent illness or diseaseshould first be excluded. Special enquiry shouldthen be made, but in privacy and in the gentlestway, into many supremely personal matters.
Common contributing factors are married un-happiness, housing difficulties often associatedwith living with ' in laws,' exhaustion from theprolonged strain either of overwork in the homeor nursing a sick relative, the emotional shockresulting from an unhappy love affair or the deathof a close friend or member of the family, an un-suitable occupation or financial or domestic worriesin their manifold varieties.
It should here be put on record that it istypical of the contrariness of this disease that inmore than half the patients no relevant precipitatingagent can be found.
If no precipitating factor can be found the casemust be treated on its merits; if one is revealedwhich can be relieved, medical treatment alonemay well be all that is necessary. It is in the casesin which there is an obvious domestic or psycho-logical obstacle to recovery which cannot be re-moved in which the greatest judgment is required
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

june f953 RIDDELL: The Treatment of Thyrotoxicosis
:.r*.n.;···li·., :'*
1;·
Ai.ii'i::te:··:i:
: rr.9.a
eiii'"t: .,ai.i·''··::':·a;*.
:..::*.:
i:i.
r.i:··:
;::·:: ··:
i·
·:'··
:':::·iQ.i·i'i .::i..·*i.·i
FIG. I9.-Three previous thyroid operations. Symp-tomless palsy on right side.
e;S
8.~ ~ ~ ~ ..:::j.:t3:,.::...:.::::.::'e
·Ss''. ^ ke 1:1S
FIG. 20.-Carcinoma of the thyroid with paralysis ofthe right vocal cord.
::.: ..::i
w:. .:
*;SwWS-SF .. ... r .. iiFh"
'. ::;. . . ...''..;
FIG. 2 .-Hashimoto's disease with paralysis of onevocal cord.
in determining the most suitable form of treat-ment. Such patients will almost certainly relapseif treated with thiouracil alone. In the same wayoperation is likely to be only partly successful.Sub-total thyroidectomy in these circumstancesshould, I think, be reserved for the severelythyrotoxic in whom the measure of improvementproduced may be sufficiently significant to enablethe patients to review and assess their own prob-lems with a fresh outlook and in a more balancedmanner. No rules, however, can be laid down,each patient and each problem must be assessedand treated individually.
Iodine Preparation. There is one short riderthat should be added to the subject of treatment;some of the younger patients especially do nottolerate thiouracil well and if the thyrotoxicosis isof moderate severity only can be brought to a safeoperative level with iodine alone. In selectedcases this method of preparation still has a definiteplace.Radioactive Iodine
It is not possible yet to assess the part radio-active iodine is ultimately likely to play in thediagnosis or treatment of thyrotoxicosis. En-
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

298 POSTGRADUATE MEDICAL JOURNAL June i953------------ -- --- - -···:-· ------------------ - ------------i~i.ixn~"ll 1~~~"
.PYRAM.iDAL
IOB.... ...
i,
FIG. 22.-Operation specimen showing the pyramidallobe.
couraging reports have been received from anumber of centres. The amount of radioactiveiodine present in the thyroid gland itself can bemeasured by means of a Geiger counter. If theamount of radioactive iodine present in the plasmais determined at the same time, the thyroid iodineclearance rate can be measured and this is ofdiagnostic value. From here it is removed both bythe thyroid and the kidneys. The rate of uptakeby the thyroid is related to the activity of the gland,being rapid in toxic goitre and slow in myxoedema.In consequence, during the same period there isproportionately less or more iodine available forexcretion by the kidneys and this amount can bemeasured.These variations form the basis of tests which
can be used for diagnostic purposes to determinethe presence or absence of thyrotoxicosis-and isespecially valuable in those doubtful cases in whichthe clinical picture may be complicated by ananxiety state. It is equally useful in determiningthe degree of hypothyroidism in a case ofmyxoedema and can be helpful in circumstanceswhen the B.M.R. is likely to be inaccurate.
For therapeutic purposes the dosage is basedon the severity of the toxicity and the size of thegland. A single dose is usually sufficient but sub-sequent smaller doses may have to be given. Thevery simplicity of the treatment naturally makes itpopular with patients. The clinical responsenormally follows a similar pattern; in the first fewdays the gland becomes tender, to be followed inthe course of the first week by an exacerbation oftoxicity. Clinical improvement follows at the endof the first fortnight and in four weeks 97 per cent.of the radioactivity is dissipated.
* :.:P'""o,::c
*..:::
FIG. 23.-Pyramidal lobe recurrence.
Until we know whether the threats of carcino-genesis, the kidney or ovarian or bone marrowdamage are real or groundless, it will be wise toreserve I183 for the treatment of patients over theage of 50, for cases of recurrent thyrotoxicosis andpatients who are unsuitable for operation or whoare resistant or sensitive to the anti-thyroid agents.In the meantime its potentialities continuecautiously to be explored.The Vocal CordsA routine pre-operative and post-operative
laryngoscopy should be done before and afterevery thyroidectomy.
Pre-operative laryngoscopy occasionally revealsa paralyzed cord; in some instances this may in-fluence the surgeon's decision to operate and inothers will exonerate him if symptoms developsubsequent to operation. The examination is ofparticular importance in patients who have had aprevious thyroid operation or if carcinoma of thethyroid is suspected. (Figs. 19, 20 and 2I). Thevocal cord changes and associated dangers inmyxoedema have been referred to on p 287.
Post-operative laryngoscopy is essential if atrue estimate of the frequency of vocal cord
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from
June 1953 RIDDELL: The Treatment of Thyrotoxicosis 299
..:. .....
...i:
...*..
*.......sl*li
i...'
::'. ;i::::-
...'...: - .. - -'
-'¢ --..
..... ::i ;-
FIG. 24.-Adherent scar due to central drainage.
damage following thyroidectomy is to be obtained.Vocal cord paralysis following thyroidectomy iscommoner than supposed and its incidence iscertainly higher after the ' blind' operation thanwhen the recurrent laryngeal nerve is identified.My own practice is always to identify eithervisually or by palpation the recurrent laryngealnerve on one side in a bilateral operation. Existingstatistics tend to be based on the selective post-operative examination of vocal cords in thosepatients only who have hoarseness of voice or otherobvious symptoms of recurrent laryngeal nervedamage. This system fails to reveal those cases ofunilateral recurrent nerve damage in which symp-toms are minimal as a result of rapid compensatoryreadjustment by the normal cord. There are aconsiderable number of such cases and there is thedanger that it may be assumed that there has beenno nerve damage unless we practice a routine post-operative laryngoscopic examination in all patientswho have had a thyroidectomy.
The Operation of Thyroidectomy (for toxicgoitre)The operation for thyrotoxicosis-sub-total
thyroidectomy-is now practised with a consider-able measure of standardization. It is usual toremove approximately seven-eighths of each lobe,having tied both superior and inferior thyroidarteries and identified at least two parathyroidglands and one recurrent laryngeal nerve. It isnot the purpose of this article to discuss technicaldetails which are far better learnt by watching ageneral surgeon with special experience in thyroidsurgery at work, but attention is drawn to thefollowing points:
I. In my experience it is not necessary to per-form a bilateral operation for a unilateral ' toxicadenoma' provided the contralateral lobe is ex-plored and appears normal to inspection andpalpation.
2. The pyramidal lobe should always be re-
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

300 POSTGRADUATE MEDICAL JOURNAL June 1953
IIIII,' /'%..--..*4%%-
FIG. 25.-A tension haematoma deep to the pretrachealfascia. Removal of skin stitches and Michel clipswill not adequately release the pressure on thetrachea.
*;LTC.r'l
.?
FIG. 26.-An opening is left in the pretracheal fascia-inferiorly.
10 ) %I 1% #I I
% 00% %
FIG. 27.-Escape of blood is possible through openingin pretracheal fascia into the subcutaneous tissues.
moved as recurrence of toxicity can occur in thisremnant (Figs. 22 and 23).
3. Drainage should be of the simplest kind-and subcutaneous-with the drainage dam emerginglaterally-at the extremities of the wound-andnever from its centre as puckering may follow whenthe patient swallows. (Fig. 24).
4. The pretracheal fascia should never be com-pletely sewn up in the midline or a tension haema-toma may develop deep to it and cause sudden andsevere dyspnoea (Fig. 25). If an opening is de-liberately left (Fig. 26) and bleeding from thegland occurs the blood is able to escape sub-cutaneously (Fig. 27).
BIBLIOGRAPHYANSELL, G., and MILLER H. (1952), Lancet, ii, 5.CATTELL, R. B. (I949), 'Transactions of the American Goitre
Association,' p. 201.DONALD, C. (1945), The Postgrad. Med. J., 21, 41.FRASER, R., and HARRISON, R. J. (1952), Lancet, i, 382.NEWSHOLME, G. A. (1952), Lancet, ii, 805.POCHIN, EF E. (1950), Ibid., ii, 84.
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from

ThyrotoxicosisThe Treatment of
Victor Riddell
doi: 10.1136/pgmj.29.332.2821953 29: 282-300 Postgrad Med J
nhttp://pmj.bmj.com/content/29/332/282.citatioat: Updated information and services can be found
These include:
serviceEmail alerting
corner of the online article. this article. Sign up in the box at the top right Receive free email alerts when new articles cite
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 17, 2018 - Published by http://pmj.bmj.com/Downloaded from