trends in clinic visits and diagnosed c. trachomatis and n. gonorrhoeae infections following the...
TRANSCRIPT
Trends in Clinic Visits and Diagnosed C. trachomatis and N. gonorrhoeae Infections
Following the Introduction of a Co-Pay in an STD Clinic
C. RietmeijerL. Lloyd
G. Alfonsi
Denver Public Health DepartmentDenver, Colorado
Presented at the 2004 National STD Prevention ConferenceMarch 8, 2004
Philadelphia, PA

Background
• Offering of clinical (diagnostic and treatment) services has historically been a key strategy for STD control and prevention
• To maximize the impact of this strategy, STD clinical services have traditionally been offered at no or low cost to the patient
Background - 2
• To offset decreases in public funding, fee for services, usually in the form of co-payments, may be initiated or increased
• However, little is known about the effects of such (co-)payments on access to and utilization of services and the ability of STD control programs to diagnose and treat STDs

Background - 3
• The Denver Metro Health Clinic (DMHC) is the largest STD clinic in the Rocky Mountain region
• Due to budget shortfalls, DMHC was forced to introduce co-payments to its clients in December, 2002
DMHC Co-Payment Structure
• $15– Residents of Denver, Adams, Arapahoe, or Douglas
County presenting with a new problem
• $65– Residents of other counties presenting with a new
problem
• None– Patients with a known positive test for STDs with
documentation of positive results– Contacts of patients with known STDs with
documentation of contacts status– Follow-up visits– HIV testing only ($10.00 optional)

DMHC Co-Pay Statistics2003
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
No Pay
$15
$10
$65
LWBS
Objective
• To evaluate trends in patient visits and diagnosed CT and GC infections prior to and after the introduction of the co-pay at DMHC

Methods - 1
• Retrospective analysis of the computerized DMHC medical record database
• Comparing first three quarters of 2002 (prior to initiation of co-pay) to first three quarters of 2003 (after initiation of co-pay)
Methods - 2
• Analysis of data on GC and CT cases reported for the City and County of Denver to the Colorado Department of Public Health and Environment
• Comparison of DMHC-reported GC and CT cases in Denver with cases reported by other providers for the first 3 quarters of 2002 and 2003

0
200
400
600
800
1000
1200
1400
1600
1800
2000
JAN MAR MAY JUL SEP NOV JAN MAR MAY JUL SEP
# VISITS
2002 2003
Start Co-Pay
Denver Metro Health Clinic Visits2002 -2003

Clinic Visits DMHC 2002– 2003 by Quarter
0
500
1000
1500
2000
2500
3000
3500
4000
1st Qtr 2nd Qtr 3rd Qtr
2002
2003
Total visits 2002 through third quarter: 11,382Total visits 2003 through third quarter: 8,132Difference through third quarter: 3,250 = 28.5%
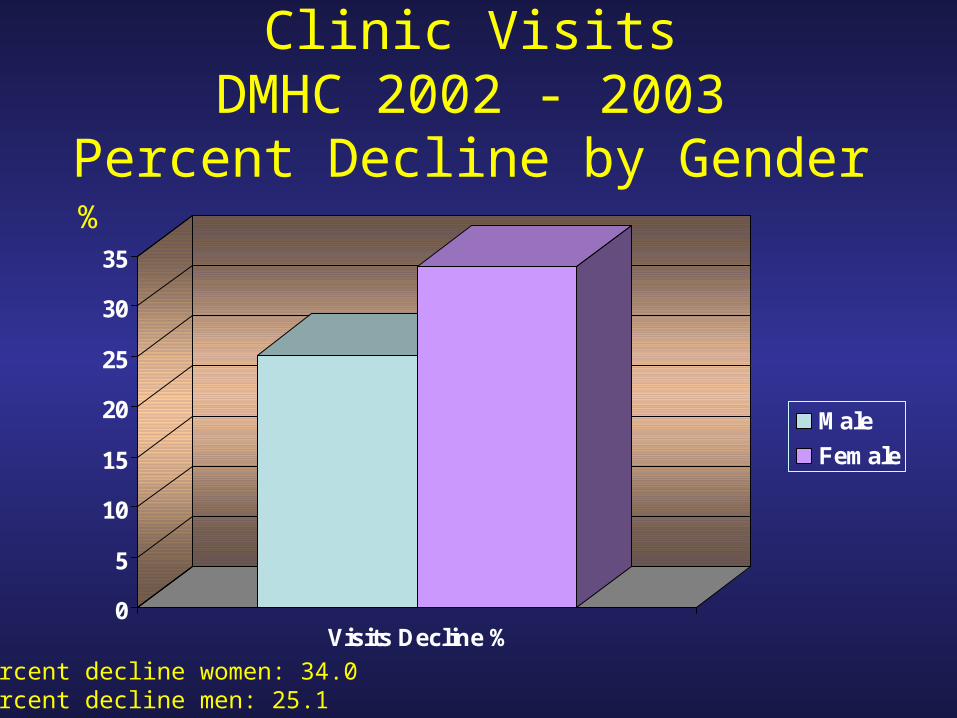
Clinic VisitsDMHC 2002 - 2003
Percent Decline by Gender
0
5
10
15
20
25
30
35
Visits Decline %
Male
Female
%
Percent decline women: 34.0Percent decline men: 25.1

Clinic VisitsDMHC 2002 - 2003
Percent Decline by Age
0
5
10
15
20
25
30
35
40
45
50
Visits Decline %
<20
20 - 29
30 - 39
40 - 49
50+
%
Percent decline age <20: 46.3%

Chlamydia Cases DMHC 2002– 2003 by Quarter
0
100
200
300
400
500
600
1st Qtr 2nd Qtr 3rd Qtr
2002
2003
Total cases 2002 through third quarter: 1519Total cases 2003 through third quarter: 1092Difference through third quarter: 427 cases = 28.1%

Gonorrhea Cases DMHC 2002 – 2003 by Quarter
0
50
100
150
200
250
300
350
1st Qtr 2nd Qtr 3rd Qtr
2002
2003
Total cases 2002 through third quarter: 871Total cases 2003 through third quarter: 539Difference through third quarter: 332 cases = 38.1%
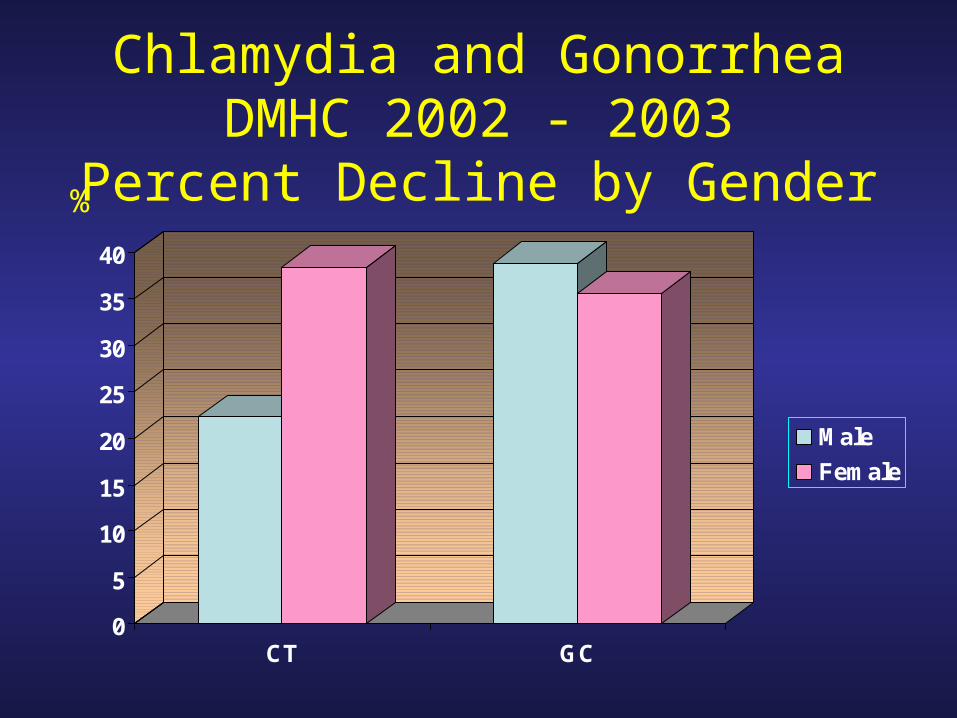
Chlamydia and GonorrheaDMHC 2002 - 2003
Percent Decline by Gender
0
5
10
15
20
25
30
35
40
CT GC
Male
Female
%

Chlamydia and GonorrheaDMHC 2002 – 2003
Percent Decline by Race/Ethnicity
0
5
10
15
20
25
30
35
40
45
50
CT GC
White
Black
Hispanic
Other
%
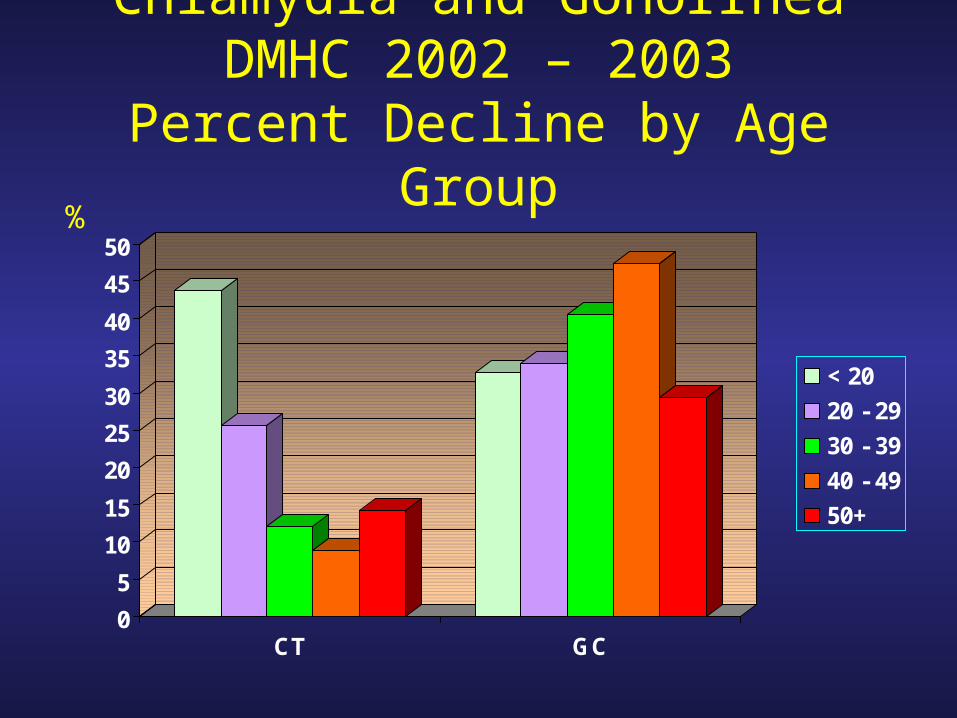
Chlamydia and GonorrheaDMHC 2002 – 2003
Percent Decline by Age Group
0
5
10
15
20
25
30
35
40
45
50
CT GC
< 20
20 - 29
30 - 39
40 - 49
50+
%

• Among those < 25 years:–Total visits were down by 38%
–CT cases were down by 38.2%
–GC cases were down by 33.8%
• This age group accounted for:–85.6% of fewer diagnosed CT infections
–39.6% of fewer diagnosed GC infections

0
200
400
600
800
1000
1200
Visits GC+ Syphilis HIV
2002
2003
Visits and GC Infections Among MSMDMHC 2002 – 2003
Total visits by MSM declined by 229 (21.1%)GC cases among MSM declined by 82 (40.2%)

Chlamydia PrevalenceDMHC 2002 - 2003
By Age
0
5
10
15
20
25
<20 20 - 29 30 - 39 40 - 49 50+
2002
2003
Through third quarter
%
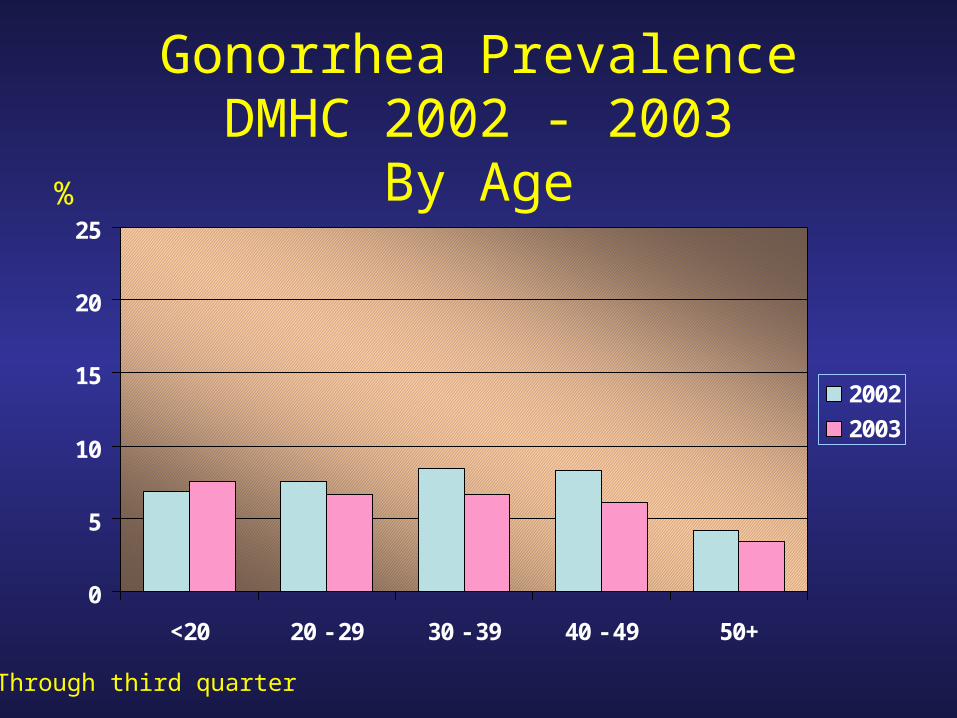
Gonorrhea PrevalenceDMHC 2002 - 2003
By Age
0
5
10
15
20
25
<20 20 - 29 30 - 39 40 - 49 50+
2002
2003
Through third quarter
%
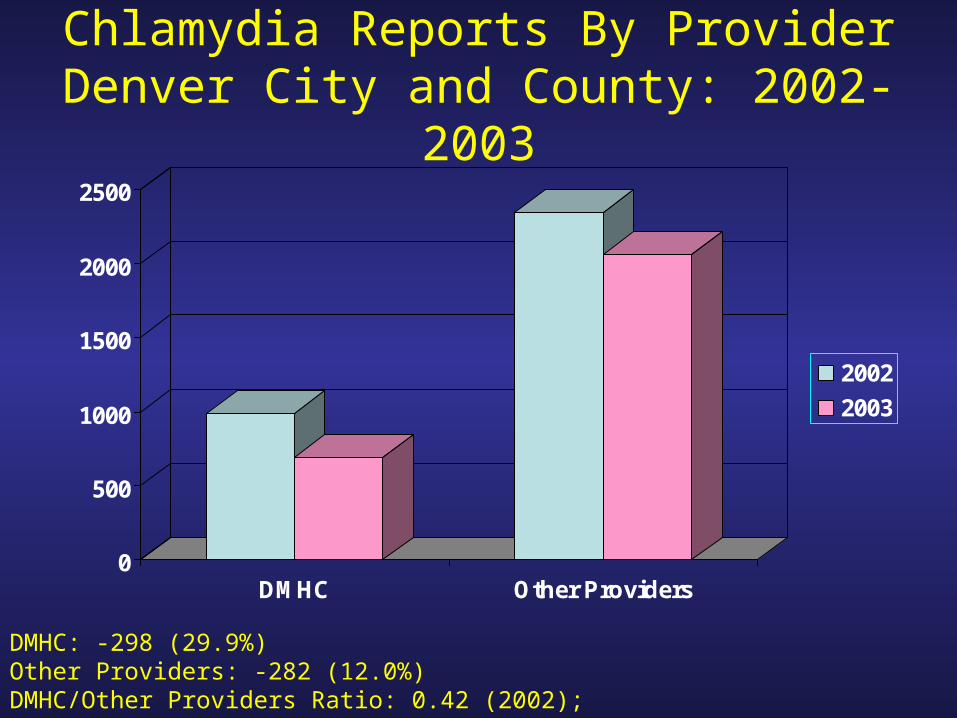
Chlamydia Reports By ProviderDenver City and County: 2002-2003
0
500
1000
1500
2000
2500
DMHC Other Providers
2002
2003
DMHC: -298 (29.9%)Other Providers: -282 (12.0%)DMHC/Other Providers Ratio: 0.42 (2002); 0.33 (2003)

Gonorrhea Reports By ProviderDenver City and County: 2002-2003
0
100
200
300
400
500
600
700
DMHC Other Providers
2002
2003
DMHC: -252 (40.2%)Other Providers: -55 (8.2%)DMHC/Other Providers Ratio: 0.94 (2002); 0.61(2003)

Conclusions
• Findings strongly suggest a causal relationship between institution of the co-pay and declining service utilization
• Persons at risk for gonorrhea, women, and persons younger than 25 years appear to be disproportionally impacted by financial barriers

Limitations
• Simple before-after analysis: cannot prove causal relationship
• Patients may have accessed services outside of DMHC
Implications for Program
• Even the institution of a modest co-pay ($15) may result in significant declines in STD clinic service utilization and diagnosed STDs