trends in lifestyle cardiovascular risk factors in women: analysis from the canadian national...
TRANSCRIPT
International Journal of Nursing Studies 39 (2002) 229–242
Trends in lifestyle cardiovascular risk factors in women:analysis from the Canadian National Population Health
Survey
Julia Wong*, Shirley Wong
School of Nursing, Dalhousie University, 5869 University Avenue, Halifax, NS, Canada B3H 3J5
Received 27 July 2000; received in revised form 11 December 2000; accepted 18 February 2001
Abstract
Cardiovascular disease (CVD) is the leading cause of death and disability among women. The present investigation
analyzed data from the National Population Health Survey to examine the prevalence trends of self-reported lifestyleCVD risk factors in adult women. Results indicated an upward prevalence trend in physical activity and high bloodpressure, and significant increased prevalence rates in obesity in the lower middle and middle income groups. Logisticregression analysis showed that increased physical activity and advancing age were significant predictors of CVD; age
confers more than a one-fold risk for developing heart disease and hypertension. Implications of the study results fornursing practice are discussed. # 2002 Elsevier Science Ltd. All rights reserved.
Keywords: Cardiovascular risk factors; Women; Prevalence trends
1. Introduction
Cardiovascular disease (CVD) is the leading cause ofdeath world wide, but rates vary considerably among
countries. Published studies clearly show that CVD is nolonger a ‘‘man disease’’; the Framingham Studyreported that two-thirds of sudden death occur amongwomen with no history of heart disease (Kannel, 1986).
In the mid-1990s, age-standardized cardiovascularmortality rates in women ranged from a high of 633deaths per 100,000 population in the Russian Federation
to a low of 139.9 per 100,000 population in France(WHO, 1998). Among the 22 selected countries,England and Wales ranked 4th and 8th in ischemic
heart disease (IHD) and CVD for women, respectively.The mortality rates were 117.9 and 238.4 per 100,000population for IHD and CVD. Comparatively, Canada
fared better, ranking 11th and 18th in mortality fromIHD and CVD for women (WHO, 1998), and ischemic
heart disease accounted for 49.7% among women
(Heart and Stroke Foundation of Canada, 2000a).Classic CVD risk factors such as hyperlipidemia,
hypertension, cigarette smoking, physical inactivity,
diabetes mellitus, certain lipoproteins and obesity applyto both sexes, but they affect women differently(Johansen et al., 1990). The strongest risk factors forwomen appear to be advancing age, low high-density
lipoprotein cholesterol (HDL-c) concentrations, tobaccouse and diabetes mellitus (Judelson, 1994).Frequently, women fail to recognize the personal
relevance of heart disease. They tend to focus onreproductive organ concerns rather than general healthissues and are generally more fearful of breast, ovarian
and uterine cancer than of heart disease (Walters, 1992;Pilote and Hlatky, 1995). Preventive health services tofemales during physician office visits are more likely
to focus on cancer screening than on coronaryheart disease (Horton, 1992). A recent Heart andStroke Foundation Survey of Canadian women age45–74 (Heart and Stroke Foundation of Canada, 2000b)
reported some unsettling results with respect to*Corresponding author. Tel.: +1-902-494-2535; fax: +1-
902-494-3487.
0020-7489/02/$ - see front matter # 2002 Elsevier Science Ltd. All rights reserved.
PII: S 0 0 2 0 - 7 4 8 9 ( 0 1 ) 0 0 0 1 3 - X

protecting their future heart health. Women with animmediate family history of CVD were no more likely to
take charge of their heart heath, in spite of the evidencethat a positive family history of heart disease can doublea woman’s own risk. Furthermore, awareness of the
cardiovascular benefits of hormone replacement therapy(HRT) for postmenopausal women was low (29% risingto 65% when they were prompted). This scenario istroubling for two reasons, (1) it suggests that women
appear to understand little or to deny their cardiac risks,and (2) despite an increasing attempt to educate the laypublic, women do not seem to recognize their ability to
control these risk factors. Based on Statistics Canadapopulation projections and current trends in age-specificmortality rates, projections to 2016 suggest that the
numbers of CVD for women will increase by 28%between 1995 and 2016 while the number of deathsattributed to CVD for men will not increase (LCDC,
Health Canada, 1999). The number of cardiovascular-related deaths in women will most likely surpass deathsin men in the near future. Thus far, there are nopublished reports that track the sex-specific trends in
CVD risk factors. Coronary heart disease (CHD) inwomen has not been studied as comprehensively as inmen. Results from studies of men have frequently been
generalized to women, which may not always beappropriate or even dangerous (Khan, 1993; Gurwitzet al., 1992). While there is considerable knowledge
about major risk factors of CHD, less is known aboutthe effects of altering these factors on reduction of CHDmortality and morbidity among women. A paucity ofdata on the sex-specific trends in CVD risk factors
warrants population-based investigations. The presentinvestigation set out to examine the prevalence trends ofself-reported lifestyle CVD risk factors (hypertension,
overweight, diabetes, inactivity, and current smoking) inadult women for the period 1994–1997 using data fromthe National Population Health Survey. Knowledge
about and recognition of these risk factors will enablenurses and other health professionals to design moreresponsive and targeted clinical interventions for this
vulnerable population.
2. Existing knowledge
2.1. Physical inactivity and cardiovascular disease
Physical inactivity, an independent risk factor forcoronary artery disease (CAD) in women, is the mostprevalent coronary risk factor (Anda et al., 1990).
Exercise appears to have beneficial effects on cardiovas-cular risk factors for women. A study of an Australiancohort reported that previously sedentary women who
increased their fitness level over 4 years showedsignificant improvement in their blood lipid levels and
systolic blood pressure (Sedgwick et al., 1993). Blair et al.(1989) reported that women with the lowest fitness had a
relative risk of death nearly five times higher than thephysically fit women. Even in older age, a reduction inmyocardial infarction risk by 50% was evident with
modest leisure-time activities, equivalent to 30–45min ofwalking three times weekly (Lemaitre et al., 1995). Thisobservation is confirmed by Kushi et al. (1997) whodemonstrated a graded inverse association between
physical activity and all-cause mortality in postmeno-pausal women. Ashton et al. (2000) examined therelationship between reported physical activity and a
range of CHD risk factors in 1407 females aged 30–64years. Their results indicated that increasing activity wasassociated with lower systolic and diastolic blood
pressures, total triglycerides, cholesterol and body massindex.Emerging evidence suggests that cardiovascular health
benefits can also be realized in non-conventionalphysical activity programs. In a randomized clinicaltrial, Dunn et al. (1997) demonstrated that lifestylephysical activity counseling is as effective as a traditional
structured exercise program in reducing CVD riskfactors among healthy, sedentary, middle-aged menand women. After 6 months of intervention, 78% of
lifestyle participants and 85% of Structured participantswere engaging in 30min or more of moderate-intensityphysical activity on most days of the week. Both groups
had significant reductions in total cholesterol, totalcholesterol/high-density lipoprotein ratio, diastolicblood pressure, and percentage of body fat. Theseinvestigators concluded that these effective lifestyle
physical activity and counseling strategies could be usedin a wide variety of settings.
2.2. High blood pressure and cardiovascular disease
High blood pressure is an independent risk factor for
heart disease in women (Johansen et al., 1990; Judelson,1994). The incidence of hypertension increases with agein both sexes; but hypertension occurs significantly more
frequently in women (Heart and Stroke Foundation ofCanada, 1995). Isolated systolic hypertension with lossof arterial elasticity is more prevalent among older
women than their male counterparts. Published datashowed that these women have an elevated risk of deathfrom stroke or CHD (Fiebach et al., 1989). TheFramingham data showed that for coronary disease,
hypertensive women and men have almost identical riskratios: 2.2 for women versus 2.0 for men at 36 years’follow-up (Kannel, 1996).
Left ventricular hypertrophy (LVH) is a major sequelof chronic hypertension. Investigation of Levy et al.(1990) showed that for all cardiovascular deaths and
deaths from all causes, women with LVH had a greaterincrease in relative risk than men. In addition, these
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242230

investigators also found that women with isolatedsystolic hypertension had more than twice the odds of
having LVH as did their male counterparts.Hypertension studies conducted in Europe and the
United States involving over 13,000 women aged 30–69
reported a decrease in all causes of mortality amongtreated versus control women (Medical Research Coun-cil, 1985; Hypertension and Detection Follow-upProgram, 1979). In general, trials that have included a
large number of women have shown favorable effects ofhypertensive therapy in terms of CAD events for olderwomen (SHEP, 1991; Dahlof et al., 1991).
2.3. Cigarette smoking and cardiovascular risk
Cigarette smoking is a powerful risk factor for CADwith the risk of cardiac events increases in relation to thenumber of cigarettes smoked daily. In the Systolic
Hypertension in the Elderly Program Study, both menand women over 60 years of age who smoked had 73%more CAD-related events than did non-smokers (Frostet al., 1996). The Nurses Health Study reported a
significant correlation among the number of cigarettessmoked and the risk of angina pectoris, non-fatalmyocardial infarction, and fatal CAD (Willett et al.,
1987). However, the risk declines rapidly after smokingcessation and approaches non-smokers’ level by 3–5years. In a longitudinal study, Prescott et al. (1998)
observed that cigarette use increases the risk of coronaryevents more for women than for men. One notableaspect of cigarette smoking is that it appears to alter
estrogen metabolism in premenopasual (Michnociczet al., 1986) and postmenopausal women (Baron et al.,1988).Cigarette smoking is also a risk factor for stroke
(Oparil, 1998). The risk of stroke for smokers was higherfor women than for men, and the risk for formersmokers has been found consistently to be lower than
that for current smokers (Wolf et al., 1992). Thus,smoking imparts the greatest risk for women already athigh risk due to older age, overweight, hypertension and
diabetes.
2.4. Diabetes and cardiovascular disease
Women with diabetes assume a risk for heart diseasethat closely approaches that of men (Barrett-Connoret al., 1991). Data from the Nurses Health Study showed
that maturity-onset diabetes mellitus confers a three- toseven-fold excess of cardiovascular events (Mansonet al., 1990). Diabetes is associated with less favorable
prognosis for women than for men compared with theirnon-diabetic counterparts (Fuller et al., 1980; Donahueet al., 1987).
Non-insulin dependent diabetes mellitus is associatedwith marked increase in the risk of CAD. Premenopausal
diabetic women experience a rate of CAD similar to thatof diabetic men, and a risk of CAD five times greater
than their age-matched non-diabetic peers (Barrette-Connor and Bush, 1991). The reasons for the relativelygreater impact of diabetes on CAD risk in women
remained undefined, but are likely related to athrogeniclipids and lipoprotein changes associated with insulinresistance (Walden et al., 1984).
2.5. Obesity and cardiovascular risk
Obesity in women is clearly linked to a worsening of
cardiovascular risk (Johansen et al., 1990; Reeder et al.,1992; Manson et al., 1990). The relationship of obesityto CAD risk in women may be due to body fat, estrogen
synthesis, and lipoprotein metabolism (Keys et al.,1984). Furthermore, the type of obesity is an indepen-dent risk for CAD in women. Upper body obesity
pattern is common among older women. A preponder-ance of abdominal fat has been shown to be a risk factorfor cardiovascular disease and diabetes, whereas pro-portionally more femoral fat is not statistically asso-
ciated with these diseases (Bjorntop, 1988).The Nurses Health Study (Manson et al., 1990) has
provided convincing evidence on the relationship of
obesity and changes in weight with the risk of coronaryevents. The risk of each type of coronary events(coronary death, myocardial infarction, angina with
stress test, angioplasty, or bypass surgery) increases withgreater body mass index (BMI). In the subsequentevaluation of women in ‘‘normal’’ weight ranges, Willett
and colleagues (1995) demonstrated a graded increase inthe risk of myocardial infarction or coronary death withhigher weight and BMI over 14 years of follow-up.
2.6. Socioeconomic status and cardiovascular disease
Socioeconomic status (SES) has been demonstrated to
be a strong and consistent determinant of health. Thereis substantial evidence for an inverse relationshipbetween socioeconomic status, CVD mortality and risk
factors. Lynch et al. (1996) observed that, comparedwith the highest income quintile, individuals in thelowest income quintile had age-adjusted relative hazards
of 2.66 and 4.33 for cardiovascular mortality and acutemyocardial infarction, respectively. Similarly, Escobedoet al. (1997) reported that indicators of low SES (familyincome, occupational status, and educational attain-
ment) account for most of the excess prematurecoronary heart disease among black Americans in theirstudy. The relationship between SES and cardiovascular
mortality extends to CVD risk factors where highlysignificant relationships have been documented betweenvarious indicators of SES and blood pressure, total
cholesterol, physical inactivity, smoking, and BMI(Winkleby et al., 1990; Shea et al., 1991; Luepker et al.,
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242 231

1993). Winkleby and colleagues (1999) examined theassociation between education and income, two indica-
tors of SES and ethnicity with six risk factors }
smoking, hypertension, obesity, leisure-time inactivity,hypercholesterolemia, and diabetes. Both indicators of
SES and ethnicity were independently associated withCVD risk factors. This finding is consistent with Poduriand Grisso’s investigation (1998) in which they observeda substantial increase in the prevalence of CVD risk
factors among the low-income women.
3. Objectives of the study
The present investigation was designed to:
1. assess the impact of SES on lifestyle CVD risk factorsin adult Canadian women,
2. examine the prevalence trends of lifestyle cardiovas-
cular risk factors in this population, and3. explore the association between these risk factors andthe prevalence of cardiovascular disease (heartdisease and hypertension).
4. Methods
4.1. Study design
The present study analyzed the cross-sectional datafrom cycles 1 and 2 of the National Population Health
Survey (NPHS). The NPHS is the first national healthsurvey of its kind conducted in Canada. The purpose ofthis survey was to measure the health status ofCanadians in order to expand knowledge of the
determinants of health. The following is a briefdescription of the study design and data collectionprocedure of the Survey (Statistics Canada, 1998).
The initial wave of data collection (cycle 1) took placefrom June 1994 to June 1995. Data for cycle 2 werecollected from June 1996 to August 1997. The NPHS
covered household and institutional residents in allprovinces and territories, except persons living on IndianReserves, on Canadian Forces bases and some remote
areas. The Survey focused on behaviors or conditionsamenable to prevention, treatment, or intervention.Thus, data collected were factors related to good health,not just those related to illness.
The 1994–95 Survey sample was created by firstselecting households and then within each householdchoosing one member to be the longitudinal respondent.
For the second cycle, the distinction was made betweenthe sample selected for longitudinal purposes and thesample chosen for cross-sectional purposes. The core
sample selected was 20,095 and 17,276 for cycles 1 and 2,respectively. Cross-sectionally, the core target popula-
tion for cycle 2 Survey included all household membersliving with longitudinal respondents. The sample size in
the second cycle was slightly diminished from the firstcycle due to attrition of the sample, deaths, out-of-scopecase, untraceable cases and non-respondents. The
present study analyzed only data from the first andsecond cycles of the NPHS obtained from the femalerespondents aged 20 or older.
4.2. Data collection
The Survey used questions that were designed for
computer-assisted interviewing (CAI) to allow program-ming of the associated logical flow into and out ofthe questions. With CAI, the interview can be controlled
based on answers provided by the respondent. On-screen prompts are displayed to the respondent andinterviewer for correction of inconsistencies. Clarity
and quality of the questions were pre-tested beforethe main Survey was implemented in the field. Thiswas accomplished by using focus groups duringdevelopmental stages of the questionnaires to study
various aspects of their content. In addition, two fieldtests were carried out with the aim to observerespondent reaction to the Survey, to obtain estimates
of time for the various sections, and to study theresponse rates.The 1994–95 NPHS was collected primarily by
personal interview whereas the second cycle of theSurvey was collected primarily by telephone; respon-dents in the core sample were first contacted by
telephone. Personal visits were made only if therespondent did not have a telephone, if the interviewermade a personal visit in the course of tracing arespondent, or upon request by the respondent. Inter-
views were conducted by interviewers who were part-time employees hired and trained specifically to carryout the CAI interviewing method.
4.3. Measurements
For the purpose of the present study, the followinglifestyle CV risk factors were extracted from the NPHS(cycles 1 and 2) data set for analyses. Lifestyle risk
factors included in the study were obesity, physicalinactivity, cigarette smoking, high blood pressure, anddiabetes mellitus. Although serum cholesterol concen-trations is a well-documented CV risk factor in women,
however, no measurements were made in any of theSurvey cycles.(a) Obesity was defined as a BMI527. BMI was
calculated by dividing the weight in kilograms by theheight in meters squared (BMI=weight (kg)/height(m2)).
(b) Physical inactivity was reflected by the physicalactivity index, a derived variable based on the
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242232

respondent’s derived energy expenditure. Energy expen-diture is calculated by using the frequency and time
per session of the physical activity as well as its METvalue. MET is a value of metabolic energy costexpressed as a multiple of the resting metabolic rate.
NPHS did not ask the respondent to specify the intensitylevel of their activities, therefore, the MET valuesadopted correspond to the low-intensity value of eachactivity. Respondents who averaged 3.0+ kcal/kg/day
of energy expenditure were categorized as active. Anactive physical activity index is approximately theamount of exercise that is required for cardiovascular
health benefits. Individuals who averaged 1.5–2.9 kcal/kg/day were classified as moderately active; they mightexperience some health benefits but little cardiovascular
benefit. Those respondents with an energy expenditurebelow 1.5 kcal/kg/day were considered inactive (Statis-tics Canada, 1998).
(c) High blood pressure}respondents’ response to thequestion ‘‘Do you have high blood pressure diagnosedby a health professional?’’ was used to categorize themas being hypertensives or normotensives.
(d) Cigarette smoking}type of smoker was usedas a surrogate measurement of the frequency ofcigarette smoking. Similar to the physical activity
index, type of smoker is also a derived variablebased on the respondent’s response to the followingthree questions: ‘‘At the present time do you smoke
cigarettes daily, occasionally or not at all?’’, ‘‘Have youever smoked cigarettes at all?’’, and ‘‘Have you eversmoked cigarettes daily?’’ The respondent was categor-ized into daily smoker, occasional smoker but was
former smoker, always an occasional smoker, formerdaily smoker, former occasional smoker, and neversmoked.
(e) Diabetes}NPHS did not specify the type ofdiabetes. Respondents were asked to indicate if they hadbeen diagnosed with diabetes.
5. Data analysis
Data were grouped and analyzed using a StatisticalAnalysis Software (SAS) program package. Since the
Survey data are either nominal or ordinal measure-ments, descriptive statistics (frequency distributionand percentages) were used to assess the prevalencerates in lifestyle CV risk factors. Chi-squared test was
used to test significance of changes in prevalence.Logistic regression was employed to estimate therisk of developing heart disease and hypertension in
women with these risk factors. A p-value 50.05 wasconsidered statistically significant in single variablecomparisons. Bonferroni correction for multiple vari-
able analyses was used to determine the level ofsignificance (Polit, 1996).
6. Results
6.1. Demographic statistics
Responses from 8653 adult women (age 20–80 and
over) in the first cycle and 35701 women in the secondcycle of the Survey were analyzed. The majority of therespondents were married (56.7% in the 1994–95 cohort,and 56.3% in the 1996–97 cohort). Overall, the
prevalence rates of women in the low-income groups(no income to550,000) were significantly reduced in thesecond cycle of the Survey. Similarly, there was a
reduced number of women with a reported annualhousehold income 5$50,000; this reduction did notreach statistical significance (Fig. 1).
6.2. Association of SES and CV risk factors
We assessed the impact of SES (measured by theannual household income) on CV risk factors byexamining the distribution of CV risk factor prevalence
rates by income groups. In the present investigation,SES was arbitrarily divided into quintiles of annualhousehold income: the first quintile was 5$10,000; thesecond, $10,000–$29,999; the third, $30,000–$49,999; thefourth, $50,000–$79,999, and the fifth quintile5$80,000. Table 1 presents changes in the prevalenceof CV risk factors between two cycles of Survey
according to income quintiles.As shown in the Table 1, there was a downward
trend in the prevalence of physical inactivity across
Fig. 1. Frequency distribution of income of women aged 20
and older, 1994/95 and 1996/97.
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242 233
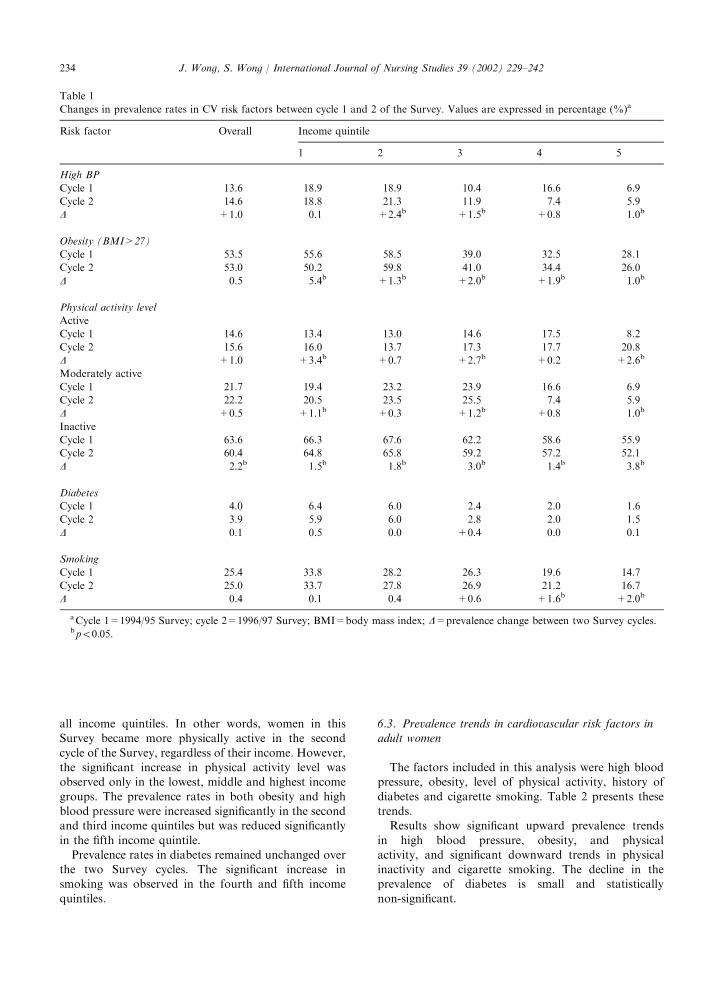
all income quintiles. In other words, women in thisSurvey became more physically active in the second
cycle of the Survey, regardless of their income. However,the significant increase in physical activity level wasobserved only in the lowest, middle and highest income
groups. The prevalence rates in both obesity and highblood pressure were increased significantly in the secondand third income quintiles but was reduced significantly
in the fifth income quintile.Prevalence rates in diabetes remained unchanged over
the two Survey cycles. The significant increase insmoking was observed in the fourth and fifth income
quintiles.
6.3. Prevalence trends in cardiovascular risk factors inadult women
The factors included in this analysis were high bloodpressure, obesity, level of physical activity, history of
diabetes and cigarette smoking. Table 2 presents thesetrends.Results show significant upward prevalence trends
in high blood pressure, obesity, and physicalactivity, and significant downward trends in physicalinactivity and cigarette smoking. The decline in theprevalence of diabetes is small and statistically
non-significant.
Table 1
Changes in prevalence rates in CV risk factors between cycle 1 and 2 of the Survey. Values are expressed in percentage (%)a
Risk factor Overall Income quintile
1 2 3 4 5
High BP
Cycle 1 13.6 18.9 18.9 10.4 16.6 6.9
Cycle 2 14.6 18.8 21.3 11.9 7.4 5.9
D +1.0 �0.1 +2.4b +1.5b +0.8 �1.0b
Obesity (BMI>27)
Cycle 1 53.5 55.6 58.5 39.0 32.5 28.1
Cycle 2 53.0 50.2 59.8 41.0 34.4 26.0
D �0.5 �5.4b +1.3b +2.0b +1.9b �1.0b
Physical activity level
Active
Cycle 1 14.6 13.4 13.0 14.6 17.5 8.2
Cycle 2 15.6 16.0 13.7 17.3 17.7 20.8
D +1.0 +3.4b +0.7 +2.7b +0.2 +2.6b
Moderately active
Cycle 1 21.7 19.4 23.2 23.9 16.6 6.9
Cycle 2 22.2 20.5 23.5 25.5 7.4 5.9
D +0.5 +1.1b +0.3 +1.2b +0.8 �1.0b
Inactive
Cycle 1 63.6 66.3 67.6 62.2 58.6 55.9
Cycle 2 60.4 64.8 65.8 59.2 57.2 52.1
D �2.2b �1.5b �1.8b �3.0b �1.4b �3.8b
Diabetes
Cycle 1 4.0 6.4 6.0 2.4 2.0 1.6
Cycle 2 3.9 5.9 6.0 2.8 2.0 1.5
D �0.1 �0.5 0.0 +0.4 0.0 �0.1
Smoking
Cycle 1 25.4 33.8 28.2 26.3 19.6 14.7
Cycle 2 25.0 33.7 27.8 26.9 21.2 16.7
D �0.4 �0.1 �0.4 +0.6 +1.6b +2.0b
aCycle 1=1994/95 Survey; cycle 2=1996/97 Survey; BMI=body mass index; D=prevalence change between two Survey cycles.bp50:05.
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242234

6.4. Relationship of risk factors to cardiovascular disease
Logistic regression analysis was used to estimate theodds of developing heart disease and hypertension in
women with these CVD risk factors. In the regressionmodel, self-reported diagnosis of heart disease was thedependent variable, and high blood pressure, BMI,physical activity index, diagnosis of diabetes, smoking,
age group, and annual household income were the
dependent variables. A similar regression model was
used to estimate the odds ratio for developing hyperten-sion; in this model, hypertension was the dependentvariable, and BMI, physical activity level, diagnosis of
diabetes, smoking, age, and annual household incomewere the explanatory variables. Tables 3 and 4 presentthe analysis results.As shown in Table 3, age, physical activity, high
blood pressure, and household income were significant
Table 2
Prevalence trends in lifestyle CV risk factors in women aged 20 and older, 1994/95 and 1996/97a
Risk factor 1994/95 1996/97 p-value
n (%) n (%)
High blood pressure 1172 (13.6) 5198 (14.1) 50.001Obesity (BMI527) 4021 (48.1) 18029 (48.8) 50.001Physical activity level
active 347 (11.9) 5986 (16.2) 50.001moderately active 591 (20.4) 8260 (22.4) 50.001inactive 1966 (67.7) 22689 (61.5) 50.001
Diabetes 347 (4.0) 1403 (3.8) NS
Cigarette smoking 2526 (29.6) 9390 (25.4) 50.001
aNS=statistically nonsignificant.
Table 3
Logistic regression: prediction of the likelihood of developing heart disease in women, age 20 and older; (a) cycle 1 and (b) cycle 2 of
the Surveya
Predictor variable b Wald chi-square p-value Odds ratio
(a) 1994/95 Survey
Physical activity level 0.3103 12.2116 0.0005 1.364
Age 0.2931 90.7096 0.0001 1.341
Household income �0.1595 34.4134 0.0001 0.853
High blood pressure �0.8199 53.0062 0.0001 0.440
BMI �0.0010 0.1265 0.7221 0.999
Cigarette smoking �0.0526 3.2147 0.0730 0.949
Diabetes �0.4220 6.1007 0.0135 0.656
Intercept �3.1588�2Log likelihood 795.920 with 7 DF
p–value 0.0001
(b) 1996/97 Survey
Age 0.2973 483.5570 0.0001 1.346
Physical activity level 0.0827 21.4014 0.0001 1.086
High blood pressure �0.7508 202.4365 0.0001 0.472
Diabetes �0.6860 76.7987 0.0001 0.504
Household income �0.0018 7.9813 0.0047 0.998
BMI 0.0018 2.4656 0.1164 1.002
Cigarette smoking �0.0024 0.5959 0.4401 0.998
Intercept �6.9434�2Log likelihood 3212.485 with 7 DF
p-value 0.0001
aBMI=body mass index.
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242 235

predictors of heart disease in both Survey cycles(p50:007). However, age and level of physical activityemerged as the strongest risk factors and were directly
related to an increased probability for developing heartdisease. These findings imply that older women whowere physically active had a one-fold risk of developing
heart disease than the less active, younger women.With respect to hypertension, age, household income,
and history of diabetes were significant risk factors.
However, age emerged as the most important predictorof hypertension in both Survey cycles (OR=1.4 in cycle1 and 1.39 in cycle 2); it confers more than a one-fold
risk for developing hypertension. Although diabetes andhousehold income were also significant predictors ofhypertension, they impart minimal risks (see Table 4).
7. Discussion
7.1. Socioeconomic status and lifestyle cardiovascularrisk factors
Socioeconomic factor may account for the increasedprevalence rates in high blood pressure and obesityobserved in our analysis. As shown in Fig. 1, a notice-
able proportion of women in the Survey (40% in the firstcycle and 28% in the second cycle) were in the lower
middle income group. Logistic regression analysisindicated that household income was a significantpredictor of cardiovascular disease, albeit not a major
one (Tables 3 and 4). Low SES has been reported to be arisk factor for CHD incidence and mortality in women.Poduri and Grisso’s investigation (1998) showed that
knowledge and understanding of CV risk factors issuboptimal among low-income women. In a prospectiveSwedish study, low socioeconomic status of the husband
was significantly associated with risk of MI in middle-aged women (Lapidus and Bengtsson, 1986). In theFramingham cohort, women with eight years of educa-
tion or less had almost four times the risk of developingcardiovascular disease than women with >12 years ofeducation (Eaker, 1989). Furthermore, obesity is mostprevalent among population with low income. Luepker
et al. (1993) documented a significant relationshipbetween several different indicators of socioeconomicstatus and body mass index. Obesity is an environmental
issue, and the primary determinants of obesity are highcalorie intake and low level of activity. The significantchange in the prevalence of obesity and diabetes in our
analysis may be best understood in light of emergingevidence that fasting hyperinsulinemia is typical ofpatients with non-insulin dependent diabetes mellitus,and is often associated with obesity (Nordt et al., 1995).
Weight loss (especially with reduction of visceral
Table 4
Logistic regression: prediction of the likelihood of developing hypertension in women, age 20 and older; (a) cycle 1 and (b) cycle 2 of
the Surveya
Predictor variable b Wald chi-square p-value Odds ratio
(a) 1994/95 Survey
Age 0.3382 326.1100 0.0001 1.402
Diabetes �1.1320 77.2067 0.0001 0.322
BMI �0.0052 9.3775 0.0022 0.995
Household income �0.0453 7.4551 0.0063 0.956
Physical activity level 0.0937 3.2402 0.0719 1.098
Cigarette smoking 0.0171 0.7745 0.3788 1.017
Intercept �2.6201�2Log likelihood 1258.687 with 7 DF
p-value 0.0001
(b) 1996/97 Survey
Age 0.3295 1667.4237 0.0001 1.390
Household income �0.0021 23.6634 0.0001 0.998
Diabetes �1.0719 302.1440 0.0001 0.342
Physical activity level 0.0323 5.7131 0.0168 1.033
BMI 0.0004 0.4213 0.5163 1.000
Cigarette smoking 0.0001 0.0039 0.9499 1.000
Intercept �6.9434�2Log likelihood 6089.641 with 7 DF
p-value 0.0001
aBMI=body mass index.
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242236

obesity) will improve insulin sensitivity and reduce therisk of the development of type 2 diabetes (Ashley and
Kannel, 1974).
7.2. Trends in cardiovascular risk factors in adult women
There is evidence to suggest that physical activity
reduced heart disease mortality and morbidity forwomen (Blair et al., 1989; Powell et al., 1987). Indeed,published data have clearly demonstrated that physicalactivity is associated with favorable levels of CVD risk
factors (Bijnen et al., 1996; Stender et al., 1993). Asteady decline in cardiovascular disease death rates inwomen since mid-1960s in Canada (Heart and Stroke
Foundation of Canada, 2000a) corroborates our findingof a significant increase in the prevalence of physicalactivity and a reduction in cigarette smoking. Our
finding of an upward prevalence trend in physicalactivity and high blood pressure is puzzling andunexpected. This observation is at odds with the
published data, which showed favorable effects ofincreased physical activity on CV risk factor reduction.However, a search of literature indicates that suchparadoxical trend indeed exists, and has been previously
reported. The finding of an increasing trend in physicalactivity and blood pressure in our study is compatiblewith that of the study by Pols et al. (1997) of 4575
women age 49–70 years in which they noted that bloodpressure (systolic and diastolic) was highest in womenwho performed heavy manual work, and was inversely
related to the time spent in leisure-time activities.Housework, walking and cycling were the three physicalactivities most frequently reported by the study subjects.Vaz de et al. (1999) also found that nearly three-quarters
of the population participants engaged in some type ofphysical activity, but more than one-third were over-weight (31%) or obese (10%). The significant associa-
tion between obesity and high blood pressure has beenreported in the literature (Ford and Cooper, 1991; Weir,1991), but the exact mechanism responsible for the
observation of a rise in physical activity with acorresponding increase in blood pressure remains to beelucidated.
Our finding of reduced prevalence in smoking andincreased prevalence in obesity is consistent with theobservation of Hu et al. (2000) of a substantial decline(40%) in the numbers of female participants who
smoked, but an increase (38%) in the prevalence ofoverweight, defined as a BMI525. The explanationoffered by Hu and co-workers is that the dietary
glycemic load in their subjects was increased due to ahigh intake of refined carbohydrates. In contrast,Rosengren et al. (2000) reported an upward trend in
obesity over a period of 30 years among smokers andformer smokers in their study. However, their study
involved men only, and it is possible that smoking mighthave differential effects on body weight in women.
In our study, prevalence of obesity and high bloodpressure increased significantly in the lower middleincome (group 2) and middle income (group 3) groups;
their level of physical activity increased minimally andnon-significantly in income group 2 (0.7%) but sub-stantially and significant in group 3 (2.7%). It is likelythat these two income groups engaged in activity such as
housework or some type of manual work, which maynot require much energy expenditure. In the presentinvestigation, we used self-reported data of physical
activity. Roberts (1995) challenged the accuracy of self-reported data as scientific measurement of the preva-lence of CV risk factors. Overestimation or under-
estimation of physical activity may account for theobserved upward prevalence trends in hypertension andobesity among women in the lower income groups,
despite an increase in physical activity levels.Our finding of a significant upward prevalence trend
in hypertension (0.5%) is in agreement with previouslypublished data (Fortmann et al., 1990; Puska et al.,
1983). Several explanations may account for thisobservation. First, an increased awareness of hyperten-sion as a major risk factor for CVD may motivate the
Survey participants to have their blood pressure checkedregularly. In fact, 58% and 59% of women in the NPHSreported having their blood pressure test less than 6
months in the first and second cycles of the Survey,respectively (data not shown). This increase in theproportion of women having regular blood pressuremonitoring, can translate into an increased percentage
of women diagnosed with high blood pressure. Sec-ondly, our analysis indicated that the rise in theprevalence of high blood pressure is associated with an
increase in obesity (Table 2). The close associationbetween hypertension and obesity has been firmlyestablished. Investigation by Ford and Cooper (1991)
demonstrated that BMI was positively related to theprobability of developing hypertension, independent ofage. The exact mechanism responsible for this relation-
ship remains unclear, but it is postulated that augmentedBMI requires both an increase in intravascular volumeand cardiac output to meet metabolic requirements.Such volume overload can result in elevated blood
pressure (Weir, 1991).
7.3. Relationship of risk factors to cardiovascular disease
The logistic regression analysis of heart disease andhigh blood pressure showed that physical activity and
age were significant predictors of CVD. The finding of adirect relationship between increased physical activityand cardiovascular disease is unexpected but is consis-
tent with that of the investigation by Pols et al. (1997) inwhich they observed an association between a higher
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242 237

activity level of work or housework and a higher level ofcardiovascular disease risk indicators (blood pressure,
heart rate, BMI, waist/hip ratio, and waist circumfer-ence). The mechanism underlying this positive associa-tion is unknown, but one may surmise that older
participants in the NPHS might have subclinical heartdisease, hypertension or both, which might not havebeen diagnosed by the health professionals. If this werethe case, high level of physical activity could precipitate
a cardiovascular event in those whose cardiac functionmight have been compromised secondary to augmentedblood pressure. The inverse relation between heart
disease and high blood pressure noted in our analysis(Table 3) argues against the speculation that hyperten-sion contributes to an increased odds for developing
heart disease. The self-reported diagnosis of high bloodpressure may inflate or deflate its prevalence; this mightaccount for the inverse relationship between hyperten-
sion and heart disease. Nonetheless, the fact that agewas positively related to heart disease and high bloodpressure clearly suggests that older women are at highrisk for CVD.
8. Implications for nursing
Cardiovascular disease is primarily a lifestyle disease,and is amenable to changes. Research shows that CVD
can be slowed significantly or progression halted whenpreventive programs have been instituted at the begin-ning stages of the disease (Chesebro et al., 1982). Health
professionals have advocated primary prevention ofCVD for many years, but it seems that women in generalare not heeding the message. Despite increased physicalactivity, women participants in the NPHS demonstrated
an increase in the prevalence of obesity and high bloodpressure. In the last two decades, a number ofcommunity-based heart health programs have been
developed in the US and UK (Carleton et al., 1995;Brownson et al., 1996; Baxter et al., 1997; Tudor-Smithet al., 1998), but reports of these projects indicated
inconclusive and inconsistent results with respect toprogram efficacy. Hu et al. (2000) speculated that therecent lack of decline in the incidence of coronary heart
disease may be a reflection of stagnation of changesattributable to prevention. The issues of programrelevance and appropriateness perceived by participantswith varied needs and lifestyle may also contribute to a
lack of demonstrable program effectiveness.Primary prevention is directed towards reducing an
individual’s encounter with CV risk factors. Giardina
(1998) argued for early dialogue between the physicianand patient to foster preventive steps, and to identifythose women who are at high risk for CVD. However,
there is evidence indicating that a high proportion ofpatients’ visits to physician office does not include
counseling for prevention of CVD (Giardina, 1998;Centers for Disease Control and Prevention, 1998).
Furthermore, published data showed that women’sconfidence in their physicians is not optimal, citingcommunication problems as the leading reason of their
dissatisfaction (Taylor et al., 1993; Tobin et al., 1987).Health promotion and patient education historicallyfalls in the domain of nursing (Novak, 1988), a windowof opportunity now exists for nurses to lead the health
promotion movement. Lile (1990) maintained thatidentifying women who are at risk for CVD andinitiating programs to achieve an optimal risk profile
and to delay the progression of the disease is a challengeto the professional nurse. She proposed a plan to meetthis challenge; it consists of (a) providing health
information to maintain or strengthen the existingwomen’s health, (b) focusing on and supporting ofpositive behaviors and coping strategies, and (c)
desensitizing the existing or possible deleterious riskfactors. Although primary prevention efforts such as ahealthier diet, increased physical activity, and smokingcessation carry great promise in reducing CVD risk
factors, to our knowledge, few interventions aredesigned specifically for women, in particular olderwomen. Thus, prior to designing and implementing any
primary intervention strategies, it is imperative fornurses to obtain information about women’s healthbehavior profile, their readiness to change, as well as
their interest in dietary, physical activity, and smokingcessation interventions, either at the community orindividual level.It is well documented that socioeconomic status is
strongly associated with cardiovascular risk factors(Martinez et al., 1999; Margetts et al., 1999; Choiniereet al., 2000). This SES (income) gradient for CVD risk
factors is also borne out by our analysis. One reasonmight be that lower socioeconomic groups tend to beassociated with an unhealthy lifestyle including
consuming a more atherogenic diet, engaging in lessexercise, having higher blood pressure, and smokingmore. Hazuda et al. (1986) observed that employed
women ate a less atherogenic diet than full-time house-wives. In view of this evidence, nurses need to considerthe individuals’ SES to ascertain that strategies forreducing CVD risk factors are perceived as relevant and
realistic. The goal of nutrition teaching and counseling isto develop an enjoyable eating style that will result inbetter health and quality of life. Nurses and dietitians
focus their teaching on fat, cholesterol, sodium andcalorie information of food, including culturally specificfoods.
Recently, there is a better understanding of thecomplex relationship between physical activity and lifecircumstances in women. Scharff et al. (1999) noted that
women who have children performed less structured andless intense physical activities of daily living. Those in
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242238

the oldest age category cited health as the most commonmotivator for physical activity, but were also the least to
perform physical activity. Wilcox et al. (2000) alsoreported that older age, less education, and lack of socialsupport are the major barriers to leisure-time physical
activities among rural and urban women in their study.These findings imply unequivocally that community-based cardiovascular prevention programs need to bedeveloped specifically for the older, less educated
women. Furthermore, our finding of a significant andpositive association between level of physical activityand cardiovascular disease suggests that the intensity of
physical activity for this high-risk group needs to beprescribed and these women’s responses to increasedphysical activity must be monitored regularly by health
professionals.The objective of physical activity intervention is to
enhance the individuals’ quality of life when performed
on a regular basis. Hence, creative, flexible strategiesthat incorporate physical activity into the daily routineshould be used in CV risk reduction program to meet theunique needs of women at different stages of their life.
Nurses experienced in conducting behavior change teachwomen problem-solving approaches to learn cognitiveand behavioral skills appropriate for their level of
motivational readiness for physical activity adoptionand life circumstances (Dunn et al., 1997).Pearson (1999) maintained that efforts to control
CVD should invest strategically in research to under-stand the prevalence of, and risks associated with, CVDrisk factors, as well as in measures to prevent or modifyrisk. The discrepancy between increased physical activty,
high blood pressure, obesity and lower SES could not beexplained physiologically. Further nursing research iswarranted to examine the relationship between SES
status, employment status, and the prevalence of CVrisk factors. Different types of physical activity such asleisure-time, occupational, transportation and house-
hold activities should be evaluated with respect to theirimpact on CV risk in women across the life span. Inaddition, the impact of SES status and employment
status on various types of physical activity needs to beexplored. These qualitative and quantitative data wouldinvariably illuminate the diversity and socioculturalspecificity of women’s perspectives that may be im-
portant if healthy lifestyle and quality of life are to beachieved.
9. Conclusion
Cardiovascular disease is not only the leading cause ofdeath among women in developed countries, it is morelethal and less aggressively treated in women than in
men. Despite an intense education campaign aiming atimproving cardiovascular risk profile, discouraging
statistics on the status of women’s heart health emerge.To date, there are few heart health programs that target
exclusively on women. In addition, the misconceptionsabout women’s risk of cardiovascular disease shared byboth patients and physicians, may be partly responsible
for women being unaware of their risk for heart disease.The focus of contemporary nursing has shifted from
provision of care to patients in the acute care setting tohealth promotion and illness prevention. Nursing has a
responsibility to develop strategies to decrease the risk ofCVD and its often tragic consequences. The emphasis ofprimary prevention should be placed on increased
physical activity and weight reduction in overweightwomen, to reduce the chance in developing hypertensionand heart disease. This intervention must be relevant to
the women’ socioeconomic status and culture. Thepublic, particularly women, must be encouraged toparticipate in community-based or individual-based
programs directed at reducing the risk for heart disease,and improving the quality of life. Barrett-Connor (1994)maintained that prevention programs directed towardswomen would have a broader public health impact than
those directed towards men. Behavior modification by awoman often will result in better diet and behavior forher partner and children.
References
Anda, R.F., Walker, N.M., Wooten, K.G., Mast, E.E.,
Escobedo, L.G., Sanderson, L.M., 1990. Behavioral risk
factor surveillance, 1988. MMWR: Morbidity and Mortality
Weekly Report 39 (SS-2), 1–3.
Ashley, F.W., Kannel, W.B., 1974. Relation of weight change
to change in atherogenic traits: the Framingham study.
Journal of Chronic Diseases 27, 103–114.
Ashton, W., Nanchahal, K., Wood, D., 2000. Leisure-time
physical activity and coronary risk factors in women. Journal
of Cardiovascular Risk 7 (4), 259–266.
Baron, J.A., Adams, P., Ward, M., 1988. Cigarette smoking
and other correlates of cytologic oestrogen effect in
postmenopausal women. Fertility and Sterility 50, 766–771.
Barrette-Connor, E., Bush, T.L., 1991. Estrogen and coronary
heart disease in women. JAMA 265, 1861–1867.
Barrett-Connor, E.L., 1994. Heart disease in women. Fertility
and Sterility 62 (Suppl. 2), 127S–132S.
Barrett-Connor, E.L., Cohen, B.A., Wingard, D.L., Edelstein,
D.L., 1991. Why is diabetes mellitus a stronger risk factor for
fatal ischemic heart disease in women than in men? The
Rancho Bernado Study. JAMA 265, 627–631.
Baxter, T., Milner, P., Wilson, K., Leaf, M., Nicholl, J.,
Freeman, J., Cooper, N., 1997. A cost effective, community
based heart health promotion project in England: prospective
comparative study. British Medical Journal 315 (7108), 582–
585.
Bijnen, F.C., Feskens, E.J., Caspersen, C.J., Giampaoli, S.,
Nissinen, A.M., Menotti, A., Mosterd, W.L., Kromhout, D.,
1996. Physical activity and cardiovascular risk factors among
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242 239

elderly men in Finland, Italy, and the Netherlands. American
Journal of Epidemiology 143 (6), 553–561.
Bjorntop, P., 1988. The association between obesity, adipose
tissue distribution, and disease. Acta Medica Scandinavica
723, 121–134.
Blair, S.N., Kohl, H.W.III, Paffenbarger Jr., R.S., Barlow,
C.E., 1989. Physical fitness and all cause mortality: a
prospective study of health of men and women. JAMA
262, 2395–2401.
Brownson, R.C., Smith, C.A., Pratt, M., Mack, M.E., Jackson-
Thompson, J., Dean, C.G., Dabney, S., Wilkerson, J.C.,
1996. Preventing cardiovascular disease through commou-
nity-based risk reduction: the bootheel heart health project.
American Journal of Public Health 86, 206–213.
Carleton, R.A., Lasater, T.M., Assaf, A.R., Felfman, H.A.,
McKinlay, S., 1995. The Pawtucket Heart Health Program:
community changes in cardiovascular risk factors and
projected disease risk. American Journal of Public Health
85, 777–785.
Centers for Disease Control and Prevention, 1998. Missed
opportunities in preventive counseling for cardiovascular
disease } United States, 1995. MMWR: Morbidity and
Mortality Weekly Report 47(3), 91–95.
Chesebro, J.H., Fuster, V., Elveback, L.R., Frye, R.L., 1982.
Strong family history and cigarette smoking as risk factors of
coronary artery disease in young adults. Britsh Heart Journal
47, 78–83.
Choiniere, R., Lafontaine, P., Edwards, A.C., 2000. Distribu-
tion of cardiovascular disease risk factors by socio-economic
status among Canadian adults. Canadian Medical Associa-
tion Journal 162 (9 Suppl.), S13–S24.
Dahlof, B., Lindholm, L., Hansson, L., Schersten, B., Ekbom,
T., Wester, P.O., 1991. Morbidity and mortality in the
Swedish Trial in old patients with hypertension. (STOP-
Hypertension.). Lancet 338, 1281–1285.
Donahue, R.P., Abbott, R.D., Reed, D.M., Yano, K., 1987.
Postchallenge glucose concentrations and coronary heart
disease in men of Japanese ancestry: the Honolulu Heart
Program. Diabetes 36, 689–692.
Dunn, A.L., Marcus, B.H., Kampert, J.B., Garcia, M.E., Kohl
III, H.W., Blair, S.N., 1997. Reduction in cardiovascular
disease risk factors: 6-month results from Project Active.
Preventive Medicine 26 (6), 883–892.
Eaker, E.D., 1989. Psychological factors in the epidemiology of
coronary heart disease in women. Psychiatric Clinics of
North America 12, 167–174.
Escobedo, L.G., Giles, W.H., Anda, R.F., 1997. Socioeconomic
status, race and death from coronary heart disease. American
Journal of Preventive Medicine 13, 123–128.
Fiebach, N.H., Herbert, P.R., Stampfer, M.J., Colditz, G.A.,
Willett, W.C., Rosner, B., Speizer, F.E., Hennekens, C.H.,
1989. A prospective study of high blood pressure and
cardiovascular disease in women. American Journal Epide-
miology 130, 646–654.
Ford, E.S., Cooper, R.S., 1991. Risk factors for hypertension in
a national cohort study. Hypertension 18, 598–606.
Fortmann, S.P., Winkkleby, M.A., Flora, J.A., Haskell, W.L.,
Taylor, C.B., 1990. Effect of long-term community health
education on blood pressure and hypertension control: the
Stanford Five-City Project. American Journal of Epidemiol-
ogy 132, 629–646.
Frost, P.H., Davis, B.R., Burlando, A.J., Curb, J.D., Guthrie,
G.P., Isaacsohn, J.L., Wassertheil-Smoller, S., Wilson, A.C.,
Stamler, J., for the Systolic Hypertension in the Elderly
Research Group. 1996. Coronary heart disease risk factors in
men and women aged 60 years and older: findings from the
Systolic Hypertension in the Elderly Program (SHEP).
Circulation 94, 26–34.
Fuller, J.H., Shipley, M.J., Rose, G., Jarrett, R.J., Keen, H.,
1980. Coronary-heart-disease risk and impaired glucose
tolerance. Lancet 1 (8183), 1373–137.
Giardina, K.G., 1998. Call to action: cardiovascular disease in
women. Journal of Women’s Health 7 (1), 37–43.
Gurwitz, J.H., Nananda, F., Avorn, J., 1992. The exclusion of
the elderly and women from clinical trial in acute myocardial
infarction. JAMA 268, 1417–1422.
Hazuda, H., Haffner, S., Stern, M., Knapp, J., Eifler, C.,
Rosenthal, M., 1986. Employment status and women’s
protection against coronary heart disease. Findings from
the San Antonio heart study. American Journal of Epide-
miology 123, 623–640.
Heart and Stroke Foundation of Canada, 1995. Heart Disease
and Stroke in Canada, 1995. Ottawa.
Heart and Stroke Foundation of Canada, 2000a. The changing
face of heart disease and stroke in Canada, Ottawa. Avail-
able from: URL: Http://www.hc-sc.gc.ca/hpb/lcdc/bcrdd/
hdsc2000/index.html.
Heart and Stroke Foundation of Canada, 2000b. Heart and
Stroke Foundation survey of Canadian women 45–75, 1999,
Ottawa. Available from: URL: Http://www.hc- sc.gc.ca/En/
p-newsletter/Release02.html.
Horton, J.A. (Ed.), 1992. The Women’s Health Data Book. A
Profile of Women’s Health in the United States. The Jacobs
Institute of Women’s Health, New York, Elsevier, Amster-
dam.
Hu, F., Stampfer, M., Manson, J.A., Grodstein, F., Colditz, G.,
Speizer, F., Willett, A., 2000. Trends in the incidence of
coronary heart disease and changes in diet and lifestyle in
women. New England Journal of Medicine 343, 530–537.
Hypertension and detection Follow-Up Program (HDFP) Co-
operative Group, 1979. Five-year findings of the hyperten-
sion detection and follow-up program. mortality by race, sex
and age. JAMA 242, 2572–2577.
Johansen, H., Nargundkar, M., Nair, C., Neutel, I., Wielgosz,
A., 1990. Women and cardiovascular disease. Chronic
Disease in Canada 11 (3), 41–47.
Judelson, D.R., 1994. Coronary heart disease in women. Risk
factors and prevention. JAMWA 49 (6), 186–197.
Kannel, W.B., 1986. Silent myocardial ischemia and infarction:
insights from the Framingham study. Cardiology Clinics 4
(4), 583–591.
Kannel, W.B., 1996. Blood pressure as a cardiovascular risk
factor: prevention and treatment. JAMA 275, 1571–1576.
Keys, A., Menotti, A., Aravanis, C., Blackburn, H., Djordevic,
B.S., Buzina, R., Dontas, A.S., Fidanza, F., Karvonen, M.J.,
Kimura, N., et al., 1984. The seven countries study: 2289
deaths in 15 years. Preventive Medicine 13, 141–154.
Khan, K.T., 1993. Where are the women in studies of coronary
heart disease? British Medical Journal 306, 1145–1146.
Kushi, L.H., Fee, R.M., Folsom, A.R., Mink, P.J., Anderson,
K.E., Sellers, T.A., 1997. Physical activity and mortality in
post-menpausal women. JAMA 277, 1287–1292.
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242240

Lapidus, L., Bengtsson, C., 1986. Socioeconomic factors and
physical activity in relation to cardiovascular disease and
death. A 12 year follow up of participants in a population
study of women in Gothenburg, Sweden. British Heart
Journal 55, 295–310.
LCDC, Health Canada, 1999. Number of cardiovascular
disease deaths by sex, actual and projected Canada, 1950–
2016. Cited in Heart and Stroke Foundation of Canada,
2000a. The changing face of heart disease and stroke in
Canada, Ottawa. Available from: URL: Http://www.hc-
sc.gc.ca/hpb/lcdc/bcrdd/hdsc2000/index.html.
Lemaitre, R.N., Heckbert, S.R., Psaty, B.M., Siscivick, D.S.,
1995. Leisure-time physical activity and the risk of nonfatal
myocardial infarction in postmenopausal women. Archives
of Internal Medicine 15, 2302–2308.
Levy, D., Garrison, R.J., Savage, D.D., Kannel, W.B., Castelli,
W.P., 1990. Prognostic implications of echocardiographically
determined left ventricular mass in the Framingham Heart
Study. New England Journal of Medicine 322, 1561–1566.
Lile, J.L., 1990. A nursing challenge for the 90s: reducing risk
factors for coronary heart disease in women. Health Values
14 (4), 17–21.
Luepker, R.V., Rosamond, W.D., Murphy, R., Sprafka, J.M.,
Folsom, A.R., McGovern, P.G., Blackburn, H., 1993.
Socioeconomic status and coronary heart disease risk factor
trends: the Minnesota heart survey. Circulation 88, 2171–
2179.
Lynch, J.W., Kaplan, G.A., Cohen, R.D., 1996. Do cardiovas-
cular risk factors explain the relation between socioeconomic
status, risk of all-cause mortality, cardiovascular mortality,
and acute myocardial infarction? American Journal of
Epidemiology 144, 934–942.
Manson, J.E., Colditz, G.A., Stampler, M.J., Willett, W.C.,
Rosner, B., Monson, R.R., Speizer, F.E., Hennekens, C.H.,
1990. A prospective study of obesity and risk of coronary
heart disease in women. New England Journal of Medicine
322, 882–889.
Margetts, B.M., Rogers, E., Widhal, K., Remaut de Winter,
A.M., Zunfit, H.J., 1999. Relationship between attitudes to
health, body weight and physical activity and level of
physical activity in a nationally representative sample in the
European Union. Public Health and Nutrition 2 (1A), 97–
103.
Martinez, J., Kearney, J., Kafatos, A., Paquet, S., Martinez-
Gonzalez, M., 1999. Variables independently associated with
self-reported obesity in the European Union. Public Health
and Nutrition 2 (1A), 125–133.
Medical Research Council Working Party, 1985. MRC trial of
treatment of mild hypertension. Principal results. British
Medical Journal 291, 97–104.
Michnocicz, J.J., Herschcopf, R.J., Naganuma, H., Bradlow,
H.L., Fishman, J., 1986. Increased 2-hydroxylation of
oestradiol as a possible mechanism for antioestrogenic effect
of cigarette smoking. New England Journal of Medicine 315,
1305–1309.
Nordt, T.K., Sawa, H., Jujii, S., Sobel, B.E., 1995. Induction of
plasminogen activator inhibitor type-1 (PAI-1) by proinsulin
and insulin in vivo. Circulation 91, 764–770.
Novak, J.C., 1988. The social mandate and historical basis for
nursing’s role in health promotion. Journal of Professional
Nursing 4 (2), 80–87.
Oparil, S., 1998. Pathophysiology of sudden coronary death in
women: implications for prevention. Circulation 97, 2103–
2105.
Pearson, T.A., 1999. Cardiovascular disease in developing
countries: myths, realities, and opportunities. Cardiovascular
Drugs and Therapy 13 (2), 95–104.
Pilote, L., Hlatky, M.A., 1995. Attitudes of women toward
hormone therapy and prevention of heart disease. American
Heart Journal 129, 1237–1243.
Poduri, A., Grisso, J.A., 1998. Cardiovascular risk factors in
economically disadvantaged women: a study of prevalence
and awareness. Journal of National Medical Association 90
(9), 531–536.
Polit, D.F., 1996. Data Analysis and Statistics for Nursing
Research. Appleton and Lange, Stamford, CT.
Pols, M.A., Peeters, P., Twisk, J., Kemper, H., Grobbee, D.,
1997. Physical activity and cardiovascular disease risk profile
in women. American Journal of Epidemiology 146, 322–328.
Powell, K.E., Thompson, P.D., Caspersen, C.J., Kendrick, J.S.,
1987. Physical activity and the incidence of coronary heart
disease. Annual Review of Public Health 8, 253–287.
Prescott, E., Hippe, M., Schnohr, P., Hein, H.O., Vestibo, J.,
1998. Smoking and the risk of myocardial infarction in
women and men: longitudinal population study. British
Medical Journal 316, 1043–1047.
Puska, P., Salonen, J.K., Nissinen, A., Tuomilehto, J.,
Vartiainen, E., Korhonen, H., Yanskanen, A., Ronnqvist,
P., Koskela, K., Huttunen, J., 1983. Change in risk factors
for coronary heart disease during 10 years of a community
intervention programme (North Karelia Project). British
Medical Journal 287, 1840–1848.
Reeder, B.A., Angel, A., Ledoux, M., Rabin, S.W., Young,
T.K., Sweet, L.E., Canadian Heart Health Surveys Research
Group, 1992. Obesity and its relation to cardiovascular risk
factors in Canadian adults. Canadian Medical Association
Journal 146 (11), 2009–2019.
Roberts, R.J., 1995. Can self-reported data accurately
describe the prevalence of overweight? Public Health 109
(4), 275–284.
Rosengren, A., Eriksson, H., Larsson, B., Svardsudd, K.,
Tibblin, G., Welin, L., Wilhelmsen, L., 2000. Secular changes
in cardiovascular risk factors over 30 years in Swedish men
aged 50: the study of men born in 1913, 1923, 1933, and 1943.
Journal of Internal Medicine 247 (1), 111–118.
Scharff, D., Homan, S., Freuter, M., Brennan, L., 1999. Factors
associated with physical activity in women across the life
span: implications for program development. Women and
Health 29 (2), 115–134.
Sedgwick, A.W., Thomas, D.W., Davies, M., 1993. Relation-
ships between changes in aerobic fitness and changes in blood
pressure and plasma lipids in men and women: the ‘Adelaide
1000’ 4-year follow up. Journal of Clinical Epidemiology 46
(2), 141–151.
Shea, S., Stein, A.D., Basch, C.E., Lantigua, R., Maylahn, C.,
Strogatz, D.S., Novick, L., 1991. Independent association of
educational attainment and ethnicity with behavioral risk
factors for cardiovascular disease. American Journal of
Epidemiology 134, 567–582.
SHEP Cooperative Research Group Prevention of stroke by
antihypertensive drug treatment in older persons with
isolated systolic hypertension, 1991. Final results of the
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242 241

Systolic Hypertension in the Elderly Program (SHEP).
JAMA 265, 3235–3264.
Statistics Canada, 1998. National Population Health Survey,
1996/97, Ottawa. Catalogue No. 82-567.
Stender, M., Hense, H.W., Doring, A., Keil, U., 1993. Physical
activity at work and cardiovascular disease risk: results from
MONICA Augsberg Study. Internal Journal of Epidemiol-
ogy 22 (4), 644–650.
Taylor, H., Bass, H., Hoeffler, L., 1993. The health of American
women. Report on a poll conducted for the Commonwealth
Fund, Louis Harris & Associates, NY.
Tobin, J.N., Wassertheil-Smoller, S., Wexter, J.P., Steingart,
R.M., Budner, N., Lense, L., Wachspress, J., 1987. Sex bias
in considering coronary bypass surgery. Annals of Internal
Medicine 107, 19–22.
Tudor-Smith, C., Nutbeam, D., Moore, L., Catford, J., 1998.
Effects of the Heartbeat Wales programme over five years on
behavioural risks for cardiovascular disease: quasi-experi-
mental comparison of results from Wales and a matched
reference area. British Medical Journal 316 (7134), 818–822.
Vaz de, A., Graca, P., Afonso, C., D’Amicis, A., Lappalainen,
R., Damkjaer, S., 1999. Physical activity levels and body
weight in a nationally representative sample in the European
Union. Public Health and Nutrition 2 (1A), 105–113.
Walden, C.E., Knopp, R.H., Wahl, P., Beach, K.W., Strand-
ness Jr., E., 1984. Sex difference in the effect of diabetes
mellitus on lipoprotein triglycerides and cholesterol concen-
trations. New England Journal of Medicine 311, 953–959.
Walters, V., 1992. Women’s views of their main health
problems. Canadian Journal of Public Health 83, 371–374.
Weir, M.R., 1991. Impact of age, race, and obesity on
hypertensive mechanisms and therapy. American Journal of
Medicine 90 (Suppl. 5A), 5A-3S–5A-14S.
WHO, 1998. 1996 World Health Statistics Annual. World
Health Organization, Geneva.
Wilcox, S., Castro, C., King, A.C., Houseman, R., Brownson,
R.C., 2000. Determination of leisure-time physical activity in
rural compared with urban older and ethnically diverse
women in the United States. Journal of Epidemiology and
Community Health 54 (9), 667–672.
Willett, W.C., Green, A., Stampler, M.J., 1987. Relative and
absolute excess risks of coronary heart disease among women
who smoke cigarettes. New England Journal of Medicine
317, 1303–1308.
Willett, W.C., Manson, J.E., Stampler, M.J., Colditz, G.A.,
Rosner, B., Speizer, F.E., Hennekens, C.H., 1995. Weight,
weight change, and coronary heart disease in women: risk
within the normal weight range. JAMA 273, 461–465.
Winkleby, M.A., Cubbib, C., Ahn, D.K., Kraemar, H.C., 1999.
Pathways by which SES and ethnicity influence cardiovas-
cular disease risk factors. Annals of the New York Academy
of Sciences 896, 1919–2009.
Winkleby, M.A., Fortmann, S.P., Barrett, D.C., 1990. Social
class disparities in risk factors for disease: eight-year
prevalence patterns by level of education. Preventive
Medicine 19, 1–12.
Wolf, P.A., Cobb, J.L., D’Agostino, R.B., 1992. Epidemiology
of stroke. In: Barnett, H.J.M., Mohr, J.P., Stern, B.M. (Eds.),
Stroke: Pathophysiology, Diagnosis, and Management, 2nd
Edition. Churchill Livingstone, New York, pp. 3–27.
J. Wong, S. Wong / International Journal of Nursing Studies 39 (2002) 229–242242