trial of a new operative method for recurrent chronic subdural...
TRANSCRIPT

J Neurosurg 61:269-272, 1984
Trial of a new operative method for recurrent chronic subdural hematoma
YuzuRu OKU, M.D., NOBORU TAKIMOTO, M.D., KAZUMI YAMAMOTO, M.D., AND TAKANORI ONISHI, M.D.
Department of Neurosurgery, Kansai Rosai Hospital Hyogo, Japan
~" A new operative method for treating recurrent chronic subdural hematoma is presented. This method consists of complete obliteration of the subdural hematoma cavity and conversion of the hematoma cavity into epidural space. The procedure was carried out in three patients with recurrent chronic subdural hematoma, all of whom made a complete recovery.
KEY WORDS ~ chronic subdural hematoma �9 recurrence �9 operative technique
V ARIOUS methods of treatment for chronic sub-
dural hematoma have been reported) ,4,5,9-13 Evacuation of the hematoma through a single
burr-hole is a form of therapy accepted by many neu- rosurgeons. Although the frequency is low, repeated recurrences of the hematoma may occur after treatment by this method. 1'4,6 During the last 10 years, 83 cases of chronic subdural hematoma were treated by the evac- uation of the hematoma through a single burr-hole in our clinic, and recurrence was observed in three cases. These recurrent cases were treated by reopening the burr-hole and evacuation of the fluid, but unfortunately the fluid collection recurred. A more definitive treat- ment was therefore thought to be required for these patients.
Tyson, et aL,12 treated the recurrent chronic subdural hematoma by a large craniotomy and excision of the external subdural membrane. But even with this method further reaccumulation of subdural fluid was observed. It was then treated by excision of the cranial vault to obliterate the subdural space. This method apparently requires cranioplasty after the patient's con- dition improves. Svien and Gelety l~ also reported the results of craniotomy with removal of external mem- brane performed on patients with chronic subdural hematoma. Following this procedure there was a 37% recurrence rate. Thus, a simple and definitive treatment for recurrent chronic subdural hematoma was sought.
We have tried a simple method of treatment, con- sisting of a craniotomy and conversion of the subdural space into epidural space, for all three cases of recurrent
subdural hematoma in our institution. These patients had good results following this operative method. All three had more or less the same clinical history, so only one case will be presented to illustrate the operative technique.
Case Report
This 67-year-old man had minor head injuries 4 months and 1 month prior to neurosurgical consulta- tion on December 16, 1980. Two days before consul- tation he developed an unsteady gait and on the day of consultation he became obtunded.
First Admission. Neurological examination re- vealed mild left hemiparesis. In spite of slightly dull mental acuity, he was well oriented and responded well to verbal orders. Computerized tomography (CT) at this time revealed marked midline shift toward the left side (Fig. 1 left). A diagnosis of chronic subdural he- matoma was confirmed by right carotid angiography. Under local anesthesia, immediate evacuation and ir- rigation of the hematoma was performed through a single burr-hole. He had a smooth recovery, and the left hemiparesis cleared up the next day. Follow-up CT scans done on December 17 and 24, 1980 (Fig. 1 center) demonstrated gradual reduction of the hematoma cavity.
Second Admission. On January 16, 1981, this pa- tient returned to the neurosurgical clinic with 3 days' history of mild confusion and a tendency to fall back- ward. On neurological examination left hemiparesis was
J. Neurosurg. / Volume 61/August, 1984 269

Y. Oku, et al.
FIG. 1. Left: Computerized tomography scan showing an isodense chronic subdural hematoma on the fight side. Center. Scan taken 8 days after operation. The size of the hematoma cavity and the midline shift were markedly reduced after the evacuation of the hematoma. Right: Scan taken 1 month after surgery showing marked midline shift due to a recurrent isodense subdural hematoma.
observed. A CT scan done on the same day revealed recurrence of the hematoma with a markedly increased midline shift (Fig. 1 right). The patient was immediately taken to the operating room, and evacuation of the
liquid hematoma was done through the reopened pre- vious burr-hole. Again he showed improvement in his neurological condition and also on the follow-up CT scan. However, repeat CT scanning on February 5, 1981, revealed reaccumulation 'o f subdural fluid. He also demonstrated neurological deterioration and the following procedure was carried out.
Operation. Under general anesthesia an osteoplastic craniotomy was performed over the hematoma. The extent of the bone flap was intended to be as large as the size of the hematoma. As much free dura as possible was removed from the hematoma surface, which facil- itates a wide removal of the outer membrane of the hematoma and also reduces the postoperative hemor- rhage from the dural surface. Then the outer membrane of the hematoma was also removed (Fig. 2 center). At
FIG. 2. Schematic representation of the surgical proce- dure. Upper." Preoperative view of the chronic subdural he- matoma. Center: The hematoma is evacuated through a craniotomy. The margin of the external membrane is left attached to the dura mater. Lower." The dura is stripped from the skull. The hematoma cavity is completely obliterated and converted to epidural space.
FIG. 3. Computerized tomography scan 3 months after op- eration showing complete cure of the subdural hematoma.
270 J. Neurosurg. / Volume 61/August, 1984
Operation for recurrent chronic subdural hematoma
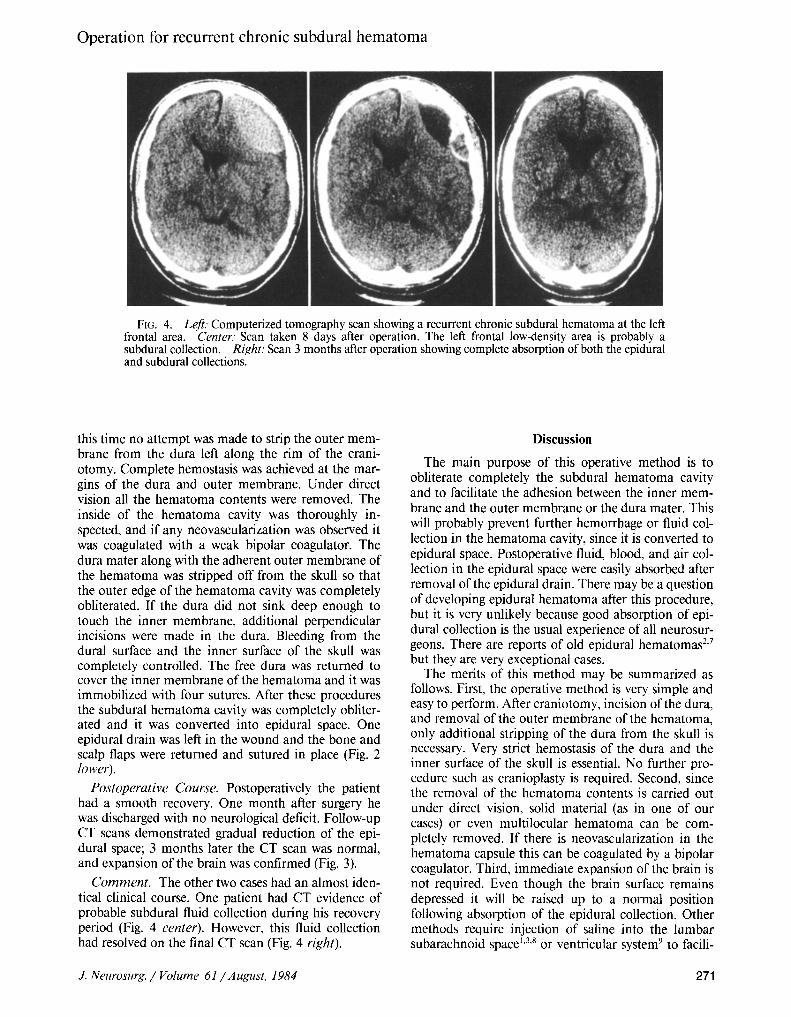
FIG. 4. Left." Computerized tomography scan showing a recurrent chronic subdural hematoma at the left frontal area. Center." Scan taken 8 days after operation. The left frontal low-density area is probably a subdural collection. Right: Scan 3 months after operation showing complete absorption of both the epidural and subdural collections.
this time no attempt was made to strip the outer mem- brane from the dura left along the rim of the crani- otomy. Complete hemostasis was achieved at the mar- gins of the dura and outer membrane. Under direct vision all the hematoma contents were removed. The inside of the hematoma cavity was thoroughly in- spected, and if any neovascularization was observed it was coagulated with a weak bipolar coagulator. The dura mater along with the adherent outer membrane of the hematoma was stripped off from the skull so that the outer edge of the hematoma cavity was completely obliterated. If the dura did not sink deep enough to touch the inner membrane, additional perpendicular incisions were made in the dura. Bleeding from the dural surface and the inner surface of the skull was completely controlled. The free dura was returned to cover the inner membrane of the hematoma and it was immobilized with four sutures. After these procedures the subdural hematoma cavity was completely obliter- ated and it was converted into epidural space. One epidural drain was left in the wound and the bone and scalp flaps were returned and sutured in place (Fig. 2 lower).
Postoperative Course. Postoperatively the patient had a smooth recovery. One month after surgery he was discharged with no neurological deficit. Follow-up CT scans demonstrated gradual reduction of the epi- dural space; 3 months later the CT scan was normal, and expansion of the brain was confirmed (Fig. 3).
Comment. The other two cases had an almost iden- tical clinical course. One patient had CT evidence of probable subdural fluid collection during his recovery period (Fig. 4 center). However, this fluid collection had resolved on the final CT scan (Fig. 4 right).
Discussion
The main purpose of this operative method is to obliterate completely the subdural hematoma cavity and to facilitate the adhesion between the inner mem- brane and the outer membrane or the dura mater. This will probably prevent further hemorrhage or fluid col- lection in the hematoma cavity, since it is converted to epidural space. Postoperative fluid, blood, and air col- lection in the epidural space were easily absorbed after removal of the epidural drain. There may be a question of developing epidural hematoma after this procedure, but it is very unlikely because good absorption of epi- dural collection is the usual experience of all neurosur- geons. There are reports of old epidural hematomas 2'7 but they are very exceptional cases.
The merits of this method may be summarized as follows. First, the operative method is very simple and easy to perform. After craniotomy, incision of the dura, and removal of the outer membrane of the hematoma, only additional stripping of the dura from the skull is necessary. Very strict hemostasis of the dura and the inner surface of the skull is essential. No further pro- cedure such as cranioplasty is required. Second, since the removal of the hematoma contents is carried out under direct vision, solid material (as in one of our cases) or even multilocular hematoma can be com- pletely removed. If there is neovascularization in the hematoma capsule this can be coagulated by a bipolar coagulator. Third, immediate expansion of the brain is not required. Even though the brain surface remains depressed it will be raised up to a normal position following absorption of the epidural collection. Other methods require injection of saline into the lumbar subarachnoid space 1'3'8 or ventricular system 9 to facili-
J. Neurosurg. / Volume 61/August, 1984 271

Y. Oku, et al.
tate the expansion of the brain. These procedures will increase the chance of infection or leave injury over the cortex.
One of our patients demonstrated fluid collection during the follow-up period. We presume this fluid was either in the subdural space (between the inner mem- brane of the hematoma and the arachnoid) or in the subarachnoid space. This collection was probably the result of slow expansion of the brain compared to the absorption rate of the epidural fluid. Although the fluid was absorbed later and the CT scan became normal in this case, the risk of a new subdural hematoma or hygroma developing should always be kept in mind and a follow-up CT scan is considered mandatory.
References
1. Cameron MM: Chronic subdural haematoma: a review of 114 cases. J Neurol Neurosurg Psychiatry 41:834-839, 1978
2. Iwakuma T, Brunngraber CV: Chronic extradural hema- tomas. A study of 21 cases. J Neurosurg 38:488-493, 1973
3. LaLonde AA, Gardner WJ: Chronic subdural hematoma. Expansion of compressed cerebral hemisphere and relief of hypotension by spinal injection of physiologic saline solution. N Engl J Med 239:493-496, 1948
4. Markwalder TM, Steinsiepe KF, Rohner M, et al: The course of chronic subdural hematomas after burr-hole craniostomy and closed-system drainage. J Neurosorg 55:390-396, 1981
5. Matricali B: Subdural suction drainage of haematomas. Surg Neurol 3:245-246, 1975
6. Parkinson D, Chochinov H: Subdural hematomas - - some observations on their postoperative course. J Neu- rosurg 17:901-904, 1960
7. Parkinson D, Reddy V, Taylor J: Ossified epidural he- matoma: case report. Neurosurgery 7:171-173, 1980
8. Robinson RG: The treatment of subacute and chronic subdural haematomas. Br Med J 1:21-22, 1955
9. Smyth HS, Livingston KE: Ventricular infusion in the operative management ofsubdural hematoma, in Morley TP (ed): Current Controversies in Neurosurgery. Phila- delphia: WB Saunders, 1976, pp 566-571
10. Svien HJ, Gelety JE: On the surgical management of encapsulated subdural hematoma. A comparison of the results of membranectomy and simple evacuation. J Neu- rosurg 21:172-177, 1964
11. Tabaddor K, Shulman K: Definitive treatment of chronic subdural hematoma by twist-drill craniostomy and closed-system drainage. J Neurosurg 46:220-226, 1977
12. Tyson G, Strachan WE, Newman P, et al: The role of craniectomy in the treatment of chronic subdural hema- tomas. J Neurosurg 52:776-781, 1980
13. Yashon D, White R J, Bryk JP, et al: Simplified supple- mentary treatment of chronic subdural fluid collections. Neurochirurgia (Stuttg) 14:8-13, 1971
Manuscript received December 31, 1983. Address reprint requests to: Yuzuru Oku, M.D., Depart-
ment of Neurosurgery, Kansai Rosai Hospital, Amagasaki, Hyogo 660, Japan.
272 J. Neurosurg. / Volume 61/August, 1984

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具