triggers, bundles, protocols, and checklists-what every...
TRANSCRIPT

Expert Reviews ajog.org
PATIENT SAFETY
Triggers, bundles, protocols, andchecklistsewhat every maternal careprovider needs to knowKavita Shah Arora, MD, MBE; Larry E. Shields, MD; William A. Grobman, MD, MBA;Mary E. D’Alton, MD; Justin R. Lappen, MD; Brian M. Mercer, MD
The rise in maternal morbidity and mortality has resulted in national and internationalattention at optimally organizing systems and teams for pregnancy care. Given thatmaternal morbidity and mortality can occur unpredictably in any obstetric setting,specialists in general obstetrics and gynecology along with other primary maternal careproviders should be integrally involved in efforts to improve the safety of obstetric caredelivery. Quality improvement initiatives remain vital to meeting this goal. The evidence-based utilization of triggers, bundles, protocols, and checklists can aid in timely diagnosisand treatment to prevent or limit the severity of morbidity as well as facilitate interdis-ciplinary, patient-centered care. The purpose of this document is to summarize thepertinent elements from this forum to assist primary maternal care providers in theirutilization and implementation of these safety tools.
Key words: obstetric quality, patient safety, quality improvement
he United States is one of the few
T developed countries in the worldwith an increasing maternal mortalityrate.1 Equally disconcerting is that itsrate of 17 maternal deaths per 100,000live births is ranked 60th in the world.2While the maternal mortality rate
From the Department of Obstetrics andGynecology, MetroHealth Medical Center, CaseWestern Reserve University, Cleveland, OH(Drs Arora, Lappen, and Mercer); Patient Safety,Dignity Health, San Francisco, CA (Dr Shields);Maternal Fetal Medicine, Marian RegionalMedical Center, Santa Maria, CA (Dr Shields);Division of Maternal-Fetal Medicine, Departmentof Obstetrics and Gynecology, NorthwesternUniversity, Feinberg School of Medicine,Chicago, IL (Dr Grobman); and Department ofObstetrics and Gynecology, ColumbiaUniversity Medical Center, New York, NY(Dr D’Alton).
Received June 20, 2015; revised Sept. 13,2015; accepted Oct. 8, 2015.
The authors report no conflict of interest.
Corresponding author: Kavita Shah Arora, MD,MBE. [email protected]
0002-9378/$36.00ª 2016 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.ajog.2015.10.011
444 American Journal of Obstetrics & Gynecology
is alarming, the number of deaths isdwarfed by the number of women whoexperience severe maternal morbidities,and these complications have increased>75% from 1998 through 1999 and2008 through 2009, affecting approxi-mately 2-4 women per 1000 livebirths.3-5 Furthermore, marked dispar-ities remain in maternal healthoutcomes for those of racial/ethnicminority and/or low socioeconomicstatus.2,5 The causes of the rise inmaternal morbidity and mortality aremultifactorial and likely include theincreasing maternal age, body massindex, and prevalence of comorbidmedical conditions, along with theincreasing cesarean delivery rate.6
Multifaceted and collaborativeapproaches to optimizing maternalhealth in the United States have beenadvancing, exemplified by initiativessuch as state-level perinatal quality col-laboratives.7-9 These collaboratives haveprioritized core obstetric safety pro-grams that are focused on postpartumhemorrhage, severe hypertension, andvenous thromboembolism.10,11 Re-cently, national attention has been
APRIL 2016
directed to the development and imple-mentation of regionalized systems ofmaternal care to facilitate provision ofservices in risk-appropriate settings.12
This regionalization of obstetric caremay result in improved outcomes forwomen known prior to delivery to be atrisk for severe morbidities (eg, maternalheart disease or placenta accreta).13-15
Yet, even if such regionalization were tobe widely enacted, most women in theUnited States would continue to bedelivered in lower-acuity birthing cen-ters and hospitals by primary maternalcare providers (obstetricians, familymedicine physicians, and midwives)and not in specialized, tertiary-carecenters by maternal-fetal medicine sub-specialists. Hemorrhage, acute severehypertension, venous thromboembo-lism, sepsis, and cardiovascular collapse(eg, secondary to amniotic fluid embo-lism) are examples of the complicationsthat can occur unexpectedly in patientsconsidered to be low risk.
Therefore, because maternal mor-bidity and mortality can occur unpre-dictably in any obstetric setting, primarymaternal care providers should be inte-grally involved in efforts to improve thesafety of obstetric care delivery. Qualityimprovement initiatives remain vital tomeeting this goal. While the sciencebehind quality improvement is rapidlyevolving, there are several core tools thathave been demonstrated to improve thequality and safety of care. Triggers,bundles, protocols, and checklists areexamples of tools that: (1) are evidence-based and can facilitate measurable im-provements in quality of care, (2) aidtimely diagnosis and treatment to pre-vent or limit the severity of morbidity,and (3) are customizable for localimplementation. These tools also have

FIGURE 1Maternal early warning criteria
Early warning system proposed by National Partnership for Maternal Safety.
BP, blood pressure.
Arora. Triggers, bundles, protocols, and checklists for obstetric safety. Am J Obstet Gynecol 2016.
ajog.org Patient Safety Expert Reviews
the potential to facilitate interdisci-plinary, patient-centered care and tocontribute to a culture of safety. It isimportant to note, however, that theimplementation ofmany of these tools inobstetrics is still in its early stages. Thus,recommendations for implementationare often based on data from otherspecialties, expert opinion, or clinicalconsensus, although the body of directevidence in obstetrics supporting utili-zation continues to grow.
While the primary benefit of theadoption of this set of tools would be toimprove patient outcomes, there areseveral appealing secondary benefits aswell. The implementation of qualityimprovement initiatives has been asso-ciated with decreased costs related toprofessional liability litigation andadverse outcomes. For example, datafrom a national health care systemwith >200 hospitals documented adecrease inmalpractice claims from 14-6per 10,000 births after the institution of aquality improvement program.16 Payers,specialty societies, and national policy-makers also have placed an emphasison quality and patient safety throughtheir endorsement of publically report-able metrics, reimbursement throughpay-for-performance mechanisms, andmandating of continuing physician ed-ucation through maintenance of certifi-cation.10,17-19 The purpose of thisdocument is to summarize the defini-tion, purpose, and supporting evidence,as well as provide examples of triggers,bundles, protocols, and checklists toassist primary maternal care providers intheir utilization and implementation ofthese safety tools.
TriggersDefinition and purposeTriggers can be used prospectively orretrospectively. Prospectively, a “trigger”is used to identify an event or conditionthat mandates further action by thehealth care team.16,20 This action isdesigned to facilitate timely interventionand reduce practice variation to improveefficiency and safety. While “notify MDif” orders are commonplace, triggers notonly notify the maternal care provider,but also require further action by the
entire health care team. Retrospectively,a “trigger tool” is a list of predefinedoccurrences likely to indicate an actionor potential adverse event and aregenerally used for retrospective internalquality monitoring and improvement.21
ExamplesExamples of prospective triggers includepatient agitation, new onset of difficultyof movement, or specific thresholdsfor abnormal vital signs.22 While utilizedfor >20 years in the nonobstetricpopulation, early warning systems forabnormal vital signs have been lesscommonly utilized in obstetrics.23
Effective early warning systemsinclude an expectation for surveillance,defined criteria for abnormalities, and aprotocol for direct provider assessmentafter an abnormality is detected. An earlywarning system can serve as both adiagnostic and communication tool,highlighting an increased risk forcompromise prior to clinical decom-pensation, so that care can be escalatedto limit the severity ofmorbidity.24 Thus,triggers can help to identify patients atrisk of decompensation and preventmorbidity by facilitating the escalation ofcare. Recently, several early warningsystems have been either created specif-ically for pregnancy or adapted for use inthe obstetric context and are termed“maternal” or “modified” obstetric earlywarning systems.23-26 While a compre-hensive review of modified obstetricearly warning systems is beyond thescope of this discussion, it is notable that
APRIL 2016 Am
this type of early warning system hasbeen broadly implemented by theUnited Kingdom’s National HealthService.25
In the United States, the NationalPartnership for Maternal Safety wasformed in response to the risingmaternalmortality rate and evidence demon-strating the contribution to this rate ofdelays in recognition and treatment ofhemorrhage and hypertension as well asprevention of thromboembolism. Thiscollaborative initiative included theAmerican Congress of Obstetriciansand Gynecologists (ACOG); Society forMaternal-Fetal Medicine; AmericanAcademy of Family Physicians; AmericanCollege of Nurse-Midwives; and Associ-ation of Women’s Health, Obstetricand Neonatal Nurses, among others.It has proposed an early warningsystemematernal early warning criteria(MEWC)ethat incorporates aspects ofthe United Kingdom’s early warningsystem. In the MEWC system, any oneabnormal value should trigger a responseby the health care team, includingbedside assessment by a clinician(Figure 1).24 This system, ideally incor-porated into the electronic medicalrecord, provides a practical tool to facil-itate timely recognition of and responseto acutematernal illness andmay serve asa framework for quality improvement onobstetric units. Figure 2 graphically de-picts one health system’s individual earlywarning system along with a guide toassist physicians in the initial evaluationandmanagement of abnormal vital signs.
erican Journal of Obstetrics & Gynecology 445

FIGURE 2Escalation due to early warning system
Example of individual health system’s early warning system with protocol for initial evaluation (L.E. Shields, MD, written communication, May 14, 2015).
02, oxygen; bili, bilirubin; bnp, b-type natriuretic peptide; BP, blood pressure; CT, computed tomography; DBP, diastolic blood pressure; DIC, disseminated intravascular coagulation; echo, echocardiogram;ekg, electrocardiogram; HR, heart rate; ICU, intensive care unit; LFTs, liver function tests; MAP, mean arterial pressure; MTP, massive transfusion protocol; PIH, pregnancy-induced hypertestion; pulse ox,pulse oximetry; RR, respiratory rate; RRT, rapid response team; SBP, systolic blood pressure; Temp, temperature.
Arora. Triggers, bundles, protocols, and checklists for obstetric safety. Am J Obstet Gynecol 2016.
Expert Reviews Patient Safety ajog.org
Since only 10-20% of errors arereported through the traditional ad-hocchart and outcome review, a moreeffective method to accurately identifyadverse events is needed.16,20 Retro-spective obstetric trigger tools, such asthe Adverse Outcome Index (AOI)illustrated in the Table or an algorithmfor severe maternal morbidity duringdelivery hospitalizations, can assistclinicians and administrators inanalyzing rates of complications, guidingfurther in-depth review, and monitoringthe impact of quality improvementprograms.6,27,28
Supporting evidenceOutside of obstetrics, early warningsystems have demonstrated an ability toidentify pediatric patients who are morelikely to need intensive care unit (ICU)
446 American Journal of Obstetrics & Gynecology
admission from the emergency depart-ment and to lessen the chance of read-mission after colorectal surgery.29,30 In asystematic review of 13 unique earlywarning system models, the predictivecapability, as quantified by the area un-der the receiver-operating characteristiccurve, for cardiac arrest models rangedfrom 0.74-0.86 and for death rangedfrom 0.88-0.93, suggesting high predic-tive values for both.31 In the obstetricalliterature, while validation studies areunderway for the MEWC, the use ofother modified obstetric early warningsystems has been associated withimprovement in mortality rates inmaternal ICUs, and also improvement inthe recording of vital signs in the clinicalsetting of maternal bacteremia.26,32 Theutilization of trigger tools such as theAOI to improve system policies also has
APRIL 2016
been associated with a reduction in theoccurrence of adverse events.16,27,28
BundlesDefinition and purposeThe Institute for Healthcare Improve-ment (IHI) defines bundles as small setsof evidence-based, independent in-terventions that when implementedtogether in an all-or-none fashion resultin significantly improved outcomescompared to when they are imple-mented individually.16 The power of thebundle is the synergistic effect of eachevidence-based component, so that thesummative increase in quality of care isgreater than would be realized with in-dividual interventions. The Safe Moth-erhood Initiative from ACOG District IIuses the term, “bundle” to signify acollection of materials (eg, checklists,

TABLEAdverse Outcome Indexindicators28
Indicator
Blood transfusion
Maternal death
Maternal ICU admission
Maternal return to operating room orlabor and delivery
Uterine rupture
Third- or fourth-degree laceration
Apgar score <7 at 5 min
Fetal traumatic birth injury
Intrapartum or neonatal death >2500 g
Unexpected admission to neonatalICU >2500 g and for >24 h
Example of retrospective trigger tool for qualityassessment.
ICU, Intensive care unit.
Arora. Triggers, bundles, protocols, and checklists forobstetric safety. Am J Obstet Gynecol 2016.
ajog.org Patient Safety Expert Reviews
protocols, educational materials) that istargeted toward a particular morbiditysuch as hemorrhage or severe hyper-tension in a multifaceted and compre-hensive approach.33
ExamplesThe IHI has advanced several perinatalbundles including those for the useof oxytocin in labor induction andaugmentation and for operative vaginaldeliveries with vacuum. In its labor in-duction bundle, the IHI recommendsthat there is clear delineation of thefollowing 4 elements: (1) the approachto assessment of gestational age, (2) thestandard recognition and managementof fetal heart rate tracings, (3) theperformance of pelvic assessment, and(4) the recognition and appropriatemanagement of tachysystole.16
The Council on Patient Safety inWomen’s Health Care, a larger umbrellainitiative over the National Partnershipfor Maternal Safety, has developed a4-phase bundle concerned with obstetrichemorrhage: (1) readiness, (2) recogni-tion and prevention, (3) response, and(4) reporting/systems learning.34 TheSafe Motherhood Initiative proposeda hypertension bundle that details thedifferential diagnosis of hypertensionin pregnancy; defines triggers toprompt further evaluation and treat-ment; and provides algorithms forcommon antihypertensive medicationadministration, checklists for eclampsiamanagement, and educational materialfor providers regarding qualityimprovement.33
Supporting evidenceIn an evidence report for the Agency forHealthcare Research and Quality, anexpert panel recommended that the IHI5-item bundle regarding the approachto central lineeassociated bloodstreaminfections should have a high level ofsupport for universal adoption given thesustained and cost-effective reductionof central lineeassociated bloodstreaminfections from 7.7-1.6 per 1000 percatheter day after implementation.35
Similarly, for those undergoing emer-gency laparotomy, a surgical bundle thatincludes early antibiotics, goal-directed
fluid therapy, and reduction of the timeto surgery has been associated with areduction in mortality from 15.6-9.6%.36 In obstetrics, neither the IHIperinatal bundle nor the one proposedby the Greater New York Hospital As-sociation’s Perinatal Safety Committeeon fetal monitoring have specificallydemonstrated improved maternalsafety.16,37 However, given that eachcomponent of these bundles has beenshown to correlate with improved out-comes independently, it stands to reasonthat this series of individual clinicalsteps grouped together could also beassociated with improved care, thoughevaluation after implementation isnecessary.37 Certain aspects of thesebundles, such as checklists on manage-ment of hypertension or hemorrhage,were based, in part, on the approachesthat in some studies have demonstratedto improve maternal morbidity andmortality.38 Furthermore, early data af-ter implementation of the Council onPatient Safety in Women’s Health Care’smaternal hypertension bundle areassociated with a reduction in severematernal morbidity.39
Protocols and ChecklistsDefinition and purposeProtocols and checklists serve toaugment memory and limit the chanceof human error.40,41 Such tools areparticularly useful in highly stressfulenvironments such as labor and deliveryunits. By improving communication andstandardizing responses, these toolsallow for necessary clinical variation inpractices, while reducing unnecessaryclinical variation that can lead tomedicalerrors. Protocols and checklists help toremind clinicians of details that formbaseline expectations of actions evenwhen the care pathway is complex.Protocols are precise and rigid plans ofaction for a specific problem or clinicalscenario, while checklists are informa-tional aids that ensure consistency andcompleteness.
ExamplesACOG, the IHI, and others have focusedon common clinical presentations inwhich protocols and checklists can lead
APRIL 2016 Am
to improved quality of care.16,40 Oneexample is a protocol for the diagnosisand management of severe hypertensionin pregnancy, with the specific goal thatan intravenous antihypertensive agent beadministered in a timely fashion afteridentification of a severe blood pressureelevation (systolic blood pressure >160mmHg or diastolic blood pressure>110mm Hg).42 Another example is a post-partum hemorrhage protocol that in-cludes early blood product transfusionand escalation of care (an example of apublished protocol is illustrated inFigure 3).43-46 A formalized delineationof steps for the management of ashoulder dystocia represents anotherexample.47 A fourth example is the use ofa checklist prior to the performance of anoperative vaginal delivery to ensure that ateam time-out is performed, the bladderis drained, and fetal position and stationare confirmed.48 Finally, the successsurgical time-outs prior to surgery toverify laterality and preoperative antibi-otic prophylaxis at cesarean deliveryrepresent examples of improvements inclinical care due to standardization ofactions through the implementation ofprotocols and checklists.49-50
erican Journal of Obstetrics & Gynecology 447

FIGURE 3Postpartum hemorrhage protocol
Example of individual institution’s postpartum hemorrhage protocol.
Arora. Triggers, bundles, protocols, and checklists for obstetric safety. Am J Obstet Gynecol 2016.
Expert Reviews Patient Safety ajog.org
Supporting evidenceMultidisciplinary surgical checklistshave been demonstrated to be associatedwith an absolute decrease in both sur-gical complications and mortality.Similar checklists exist to reduce theincidence of adverse drug events, venousthromboembolism, and surgical-siteinfections, among other morbidities.51
In obstetrics, the use of a postpartumhemorrhage protocol has been associ-ated with more rapid use of pharma-ceutical and procedural interventionsand an increase in the days between ICUadmissions at the institution.44 Finally,investigators have demonstrated reducedmaternal morbidity with checklistsregarding oxytocin administration,postpartum hemorrhage management,and hypertension treatment.38,52,53
448 American Journal of Obstetrics & Gynecology
ImplementationWhile the need for a consistent approachto evaluation and treatment in acutesituations is well established, thereremain significant barriers to imple-mentation of these patient safety tools.41
Five such potential barriers are thepotential to decrease individualization ofcare, to be less suited to the local envi-ronment, to have limited uptake, toencourage overdiagnosis, and to requirethe performance of periodic reassess-ments of impact. The first potentialbarrier to implementation is that someproviders mistakenly believe that pro-tocols and safety tools diminish clinicalcare by compromising individualizationand physician autonomy. The afore-mentioned core quality tools assist inreducing variability and improving
APRIL 2016
reliability of action, particularly instressful situations during which humanand system-level errors aremore likely tooccur. Importantly, these tools are notintended to preclude physician judg-ment or the ability to individualize care.Rather, they are meant to allow healthcare providers to avoid distractions andenhance patient care by providing anevidence-based foundation upon whichtheir attention, judgment, and individ-ualization can be directed. Thus, thesetools can serve to augment, rather thandetract, from high-quality, patient-centered care.
A second barrier to widespreadimplementation is that triggers, bundles,protocols, and checklists may need to beindividualized for each institution’smodel of care, local patient population,
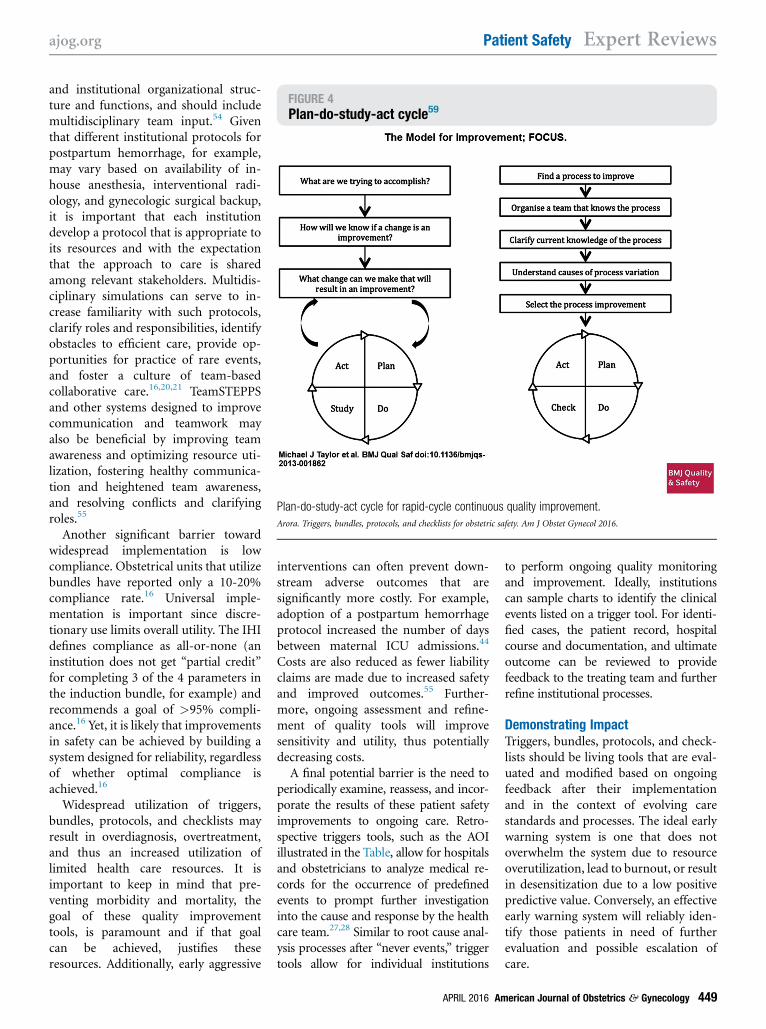
FIGURE 4Plan-do-study-act cycle59
Plan-do-study-act cycle for rapid-cycle continuous quality improvement.
Arora. Triggers, bundles, protocols, and checklists for obstetric safety. Am J Obstet Gynecol 2016.
ajog.org Patient Safety Expert Reviews
and institutional organizational struc-ture and functions, and should includemultidisciplinary team input.54 Giventhat different institutional protocols forpostpartum hemorrhage, for example,may vary based on availability of in-house anesthesia, interventional radi-ology, and gynecologic surgical backup,it is important that each institutiondevelop a protocol that is appropriate toits resources and with the expectationthat the approach to care is sharedamong relevant stakeholders. Multidis-ciplinary simulations can serve to in-crease familiarity with such protocols,clarify roles and responsibilities, identifyobstacles to efficient care, provide op-portunities for practice of rare events,and foster a culture of team-basedcollaborative care.16,20,21 TeamSTEPPSand other systems designed to improvecommunication and teamwork mayalso be beneficial by improving teamawareness and optimizing resource uti-lization, fostering healthy communica-tion and heightened team awareness,and resolving conflicts and clarifyingroles.55
Another significant barrier towardwidespread implementation is lowcompliance. Obstetrical units that utilizebundles have reported only a 10-20%compliance rate.16 Universal imple-mentation is important since discre-tionary use limits overall utility. The IHIdefines compliance as all-or-none (aninstitution does not get “partial credit”for completing 3 of the 4 parameters inthe induction bundle, for example) andrecommends a goal of >95% compli-ance.16 Yet, it is likely that improvementsin safety can be achieved by building asystem designed for reliability, regardlessof whether optimal compliance isachieved.16
Widespread utilization of triggers,bundles, protocols, and checklists mayresult in overdiagnosis, overtreatment,and thus an increased utilization oflimited health care resources. It isimportant to keep in mind that pre-venting morbidity and mortality, thegoal of these quality improvementtools, is paramount and if that goalcan be achieved, justifies theseresources. Additionally, early aggressive
interventions can often prevent down-stream adverse outcomes that aresignificantly more costly. For example,adoption of a postpartum hemorrhageprotocol increased the number of daysbetween maternal ICU admissions.44
Costs are also reduced as fewer liabilityclaims are made due to increased safetyand improved outcomes.55 Further-more, ongoing assessment and refine-ment of quality tools will improvesensitivity and utility, thus potentiallydecreasing costs.A final potential barrier is the need to
periodically examine, reassess, and incor-porate the results of these patient safetyimprovements to ongoing care. Retro-spective triggers tools, such as the AOIillustrated in the Table, allow for hospitalsand obstetricians to analyze medical re-cords for the occurrence of predefinedevents to prompt further investigationinto the cause and response by the healthcare team.27,28 Similar to root cause anal-ysis processes after “never events,” triggertools allow for individual institutions
APRIL 2016 Am
to perform ongoing quality monitoringand improvement. Ideally, institutionscan sample charts to identify the clinicalevents listed on a trigger tool. For identi-fied cases, the patient record, hospitalcourse and documentation, and ultimateoutcome can be reviewed to providefeedback to the treating team and furtherrefine institutional processes.
Demonstrating ImpactTriggers, bundles, protocols, and check-lists should be living tools that are eval-uated and modified based on ongoingfeedback after their implementationand in the context of evolving carestandards and processes. The ideal earlywarning system is one that does notoverwhelm the system due to resourceoverutilization, lead to burnout, or resultin desensitization due to a low positivepredictive value. Conversely, an effectiveearly warning system will reliably iden-tify those patients in need of furtherevaluation and possible escalation ofcare.
erican Journal of Obstetrics & Gynecology 449

Expert Reviews Patient Safety ajog.org
Rapid-cycle continuous qualityimprovement “identifies, implements,and measures changes” over a series ofweeks and months rather than years.56
Using this method, bundles, protocols,and checklists can be studied and refinedusing the iterative 4-stage plan-do-study-act cycle (Figure 4).57 Analysescan be conducted using statisticalprocess control charts to demonstratesignificant change over time and toaccelerate the rate of improvement. TheIHI also offers an improvement trackeron its World Wide Web site to allow easyvisualization of changes in quality met-rics over time. The use of these visualgraphs can serve as powerful evidence ofimprovement to patients, physicians,and administrators.58
ConclusionThe rise in maternal morbidity andmortality has resulted in national andinternational attention at optimallyorganizing systems and teams for preg-nancy care. Primary maternal care pro-viders, as core members of these systemsand teams, should play a crucial leader-ship role in these efforts. Thus, at a timeof increasing national focus on bothquality and safety of medical care, it isimportant that primary maternal careproviders participate in the imple-mentation of quality improvement toolssuch as triggers, bundles, protocols, andchecklists. Given the growing evidencein obstetrics and in other fields of med-icine that such quality improvementtools improve health outcomes, it islikely that adoption of these tools byhospitals and health care policy organi-zations will continue to rise. Byembracing their adoption, primarymaternal care providers can improve thequality of care provided to individualsand improve the safety of the health caresystem overall. -
REFERENCES
1. WHO, UNICEF, UNFPA TWB and the UNPD.Trends in maternal mortality: 1990 to2013; 2014.2. Creanga AA, Berg CJ, Syverson C, Seed K,Bruce FC, Callaghan WM. Pregnancy-relatedmortality in the United States, 2006-2010.Obstet Gynecol 2015;125:5-12.
450 American Journal of Obstetrics & Gynecology
3. Callaghan WM, Grobman WA, Kilpatrick SJ,Main EK, D’Alton M. Facility-based identificationof women with severe maternal morbidity: It istime to start. Obstet Gynecol 2014;123:978-81.4. Grobman WA, Bailit JL, Rice MM, et al. Fre-quency of and factors associated with severematernal morbidity. Obstet Gynecol 2014;123:804-10.5. GrobmanWA, Bailit JL, Rice MM, et al. Racialand ethnic disparities in maternal morbidity andobstetric care. Obstet Gynecol 2015;125:1460-7.6. Callaghan WM, Creanga AA, Kuklina EV.Severe maternal morbidity among delivery andpostpartumhospitalizations in theUnited States.Obstet Gynecol 2012;120:1029-36.7. New York State Perinatal Quality Collabora-tive. Available at: http://www.albany.edu/sph/cphce/mch_nyspqc.shtml. Accessed May 8,2015.8. Ohio Perinatal Quality Collaborative. Availableat: https://www.opqc.net/. Accessed May 8,2015.9. California Perinatal Quality Care Collabora-tive. Available at: https://www.cpqcc.org/.Accessed May 8, 2015.10. American College of Obstetricians and Gy-necologists. Quality and safety in women’shealth care, 2nd ed. Washington (DC): ACOG;2000.11. Council on Patient Safety inWomen’s HealthCare. Available at: http://www.safehealthcareforeverywoman.org/. Accessed May 2, 2015.12. American College of Obstetricians andGynecologists. Levels of maternal care. Ob-stetric care consensus no. 2. Obstet Gynecol2015;125:502-15.13. Wright JD, Herzog TJ, Shah M, et al.Regionalization of care for obstetric hemorrhageand its effect on maternal mortality. ObstetGynecol 2010;115:1194-200.14. Olive EC, Roberts CL, Algert CS, Morris JM.Placenta previa: maternal morbidity and place ofbirth. Aust N Z J Obstet Gynaecol 2005;45:499-504.15. Mhyre JM, Shilkrut A, Kuklina EV, et al.Massive blood transfusion during hospitalizationfor delivery in New York State, 1998-2007.Obstet Gynecol 2013;122:1288-94.16. Institute for Healthcare Improvement. How-to guide: prevent obstetrical adverse events.Cambridge (MA): Institute for HealthcareImprovement; 2012.17. Centers for Medicare and MedicaidServices. Quality measures and performancestandards. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Quality_Measures_Standards.html. Accessed April 20, 2015.18. ACOG. Maintenance of certification: part3ecognitive expertise test. Available at: http://www.acog.org/About-ACOG/ACOG-Departments/District-Newsletters/District-VIII/December-2012/Maintenance-of-Certification. AccessedApril 20, 2015.19. Bisognano M, Cherouny PH, Gullo S.Applying a science-based method to improve
APRIL 2016
perinatal care. Obstet Gynecol 2014;124:810-4.20. Griffin FA, Resar RK. IHI global trigger toolfor measuring adverse events. 2nd ed. IHIinnovation series white paper. Cambridge(MA): Institute for Healthcare Improvement;2009.21. Institute for Healthcare Improvement.Perinatal chart review tool. Available at: http://app.ihi.org/extranetng/content/fdb3913c-db0f-481f-9553-1ee7ed523088/affa65b0-e571-4033-89b9-f7e2deb05068/PerinatalTriggerTool_New Feb 2010.pdf. Accessed April 20, 2015.22. American Congress of Obstetricians andGynecologists. Preparing for clinical emergen-cies in obstetrics and gynecology. ObstetGynecol 2014;123:722-5.23. Edwards SE, Grobman WA, Lappen JR,et al. Modified early obstetric warning systems(MEOWS): diagnostic performance for severesepsis in women with chorioamnionitis. Am JObstet Gynaecol 2015;212:536.e1-8.24. Mhyre JM, D’Oria R, Hameed AB, et al. Thematernal early warning criteria: a proposal fromthe National Partnership for Maternal Safety.Obstet Gynecol 2014;124:782-6.25. Singh S, McGlennan A, England A,Simons R. A validation study of the CEMACHrecommended modified early obstetric warn-ing system (MEOWS). Anaesthesia 2012;67:12-8.26. Carle C, Alexander P, Columb M, Johal J.Design and internal validation of an obstetricearly warning score: secondary analysis of theIntensive Care National Audit and ResearchCenter Case Mix Program database. Anaes-thesia 2013;68:354-67.27. Mann S, Pratt S, Gluck P, et al. Assessingquality in obstetrical care: development of stan-dardized measures. Jt Commm J Qual PatientSaf 2006;32:497-505.28. Pettker CM, Thung SF, Norwitz ER, et al.Impact of a comprehensive patient safety serieson obstetric adverse events. Am J ObstetGynecol 2009;200:492.e1-8.29. Seiger N, Maconochie I, Oostenbrink R,Moll HA. Validity of different pediatric earlywarning scores in the emergency department.Pediatrics 2013;132:e841-50.30. Li LT, Mills WL, Gutierrez AM, Herman LI,Berger DH, Naik AD. A patient-centered earlywarning system to prevent readmission aftercolorectal surgery: a national consensus usingthe Delphi method. J Am Coll Surg 2013;216:210-6.e6.31. Smith MEB, Chiovaro JC, O’Neil M, et al.Early warning system scores for clinical dete-rioration in hospitalized patients: a systematicreview. Ann Am Thorac Soc 2014;11:1454-65.32. Maguire PJ, O’Higgins AC, Power KA,Daly N, McKeating A, Turner MJ. Maternalbacteremia and the Irish maternity early warn-ing system. Int J Gynaecol Obstet 2015;129:142-5.33. ACOG. Safe motherhood initiative bundles.Available at: http://www.acog.org/About-ACOG/

ajog.org Patient Safety Expert Reviews
ACOG-Districts/District-II/Safe-Motherhood-Initiative-Bundles. Accessed April 20, 2015.34. Council on Patient Safety. Patient safetybundle: obstetric hemorrhage. Available at.Accessed, http://www.safehealthcareforeverywoman.org/get-hemorrhage-bundle.php April20, 2015.35. Making health care safer II: an updatedcritical analysis of the evidence for patient safetypractices. Available at: http://www.ahrq.gov/research/findings/evidence-based-reports/services/quality/ptsafetyII-full.pdf. Accessed April20, 2015.36. Huddart S, Peden CJ, Swart M, et al. Use ofa pathway quality improvement care bundle toreducemortality after emergency laparotomy. BrJ Surg 2014;102:57-66.37. Minkoff H, Berkowitz R. Fetal monitoringbundle. Obstet Gynecol 2009;114:1332-5.38. ClarkSL,Christmas JT, FryeDR,Meyers JA,Perlin JB. Maternal mortality in the UnitedStates: predictability and the impact of protocolsof fatal postcesarean pulmonary embolism andhypertension-related intracranial hemorrhage.Am J Obstet Gynecol 2014;211:32.e1-9.39. Shields LE, Kilpatrick S, Melsop K,Peterson N. Timely assessment and treatmentof preeclampsia reduces maternal morbidity.Am J Obstet Gynecol 2015;212:S69.40. American College of Obstetricians and Gy-necologists. Standardization of practice toimprove outcomes. Obstet Gynecol 2012;119:1081-2.41. Gawande A. The checklist manifesto: howto get things right. New York (NY): MetropolitanBooks; 2009.42. Clark SL. Strategies for reducing maternalmortality. Semin Perinatol 2012;36:42-7.
43. Lappen JR, Seidman D, Burke C, Goetz K,Grobman WA. Changes in care associated withthe introduction of a postpartum hemorrhagepatient safety program. Am J Perinatol 2013;30:833-8.44. Einerson BD, Miller ES, GrobmanWA. Doesa postpartum hemorrhage (PPH) patient safetyprogram result in sustained changes in man-agement and outcomes? Am J Obstet Gynecol2015;212:140-4.e1.45. Shields LE, Smalarz K, Reffigee L, Mugg S,Burdumy TJ, Propst M. Comprehensive mater-nal hemorrhage protocols improve patient safetyand reduce utilization of blood products. Am JObstet Gynecol 2011;205:368.e1-8.46. Shields LE, Wiesner S, Fulton J,Pelletreau B. Comprehensive maternal hemor-rhage protocols reduce the use of blood prod-ucts and improve patient safety. Am J ObstetGynecol 2015;212:272-80.47. Grobman WA, Miller D, Burke C,Hornbogen A, Tam K, Costello R. Outcomesassociated with introduction of a shoulderdystocia protocol. Am J Obstet Gynecol2011;205:513-7.48. American College of Obstetricians and Gy-necologists. Operative vaginal delivery. No 17.2000.49. De Vries EN, Prins HA, Crolla RMPH, et al.Effect of a comprehensive surgical safety systemon patient outcomes. N Engl J Med 2010;363:1928-37.50. American Congress of Obstetricians andGynecologists. Patient safety in the surgicalenvironment. Obstet Gynecol 2010;116:786-90.51. Health Research and Educational Trust.Checklists to improved patient safety. Chicago
APRIL 2016 Am
(IL): Health Research and Educational Trust.2015. Available at, http://www.hpoe.org/checklists-improve-patient-safety. Accessed May 31,2015.52. Clark S, Belfort M, Saade G, et al. Imple-mentation of a conservative checklist-basedprotocol for oxytocin administration: maternaland newborn outcomes. Am J Obstet Gynecol2007;197:480.e1-5.53. Clark SL, Meyers JA, Frye DK, Perlin JA.Patient safety in obstetricsethe HospitalCorporation of America experience. Am JObstet Gynecol 2011;2014:283-7.54. American Congress of Obstetricians andGynecologists. Clinical guidelines and stan-dardization of practice to improve outcomes.Obstet Gynecol 2015;125:1027-9.55. TeamSTEPPS. Available at: http://teamstepps.ahrq.gov/. Accessed April 20, 2015.56. Robert Wood Johnson Foundation. Qual-ity/equality glossary. Available at: http://www.rwjf.org/en/library/research/2013/04/quality-equality-glossary.html. Accessed April 20,2015.57. Institute for Healthcare Improvement.Plan-do-study-act (PDSA) worksheet. Availableat: http://www.ihi.org/resources/Pages/Tools/PlanDoStudyActWorksheet.aspx. AccessedApril 20, 2015.58. Institute for Healthcare Improvement.Improvement tracker. Available at: http://app.ihi.org/workspace/tracker/. Accessed April 20,2015.59. Taylor MJ, McNicholas C, Nicolay C,Darzi A, Bell D, Reed JE. Systematic review ofthe application of the plan-do-study-act methodto improve quality in healthcare. BMJ Qual Saf2014;23:290-8.
erican Journal of Obstetrics & Gynecology 451