trisomy 21 - sasuogsasuog.org.za/images/nicolaou_11h50.pdf · • it is possible to analyze this...
TRANSCRIPT

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Trisomy 21
Ermos Nicolaou
Wits Maternal and Fetal Medicine Unit
Morningside Medi-Clinic
And C H Baragwanath Hospital
Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
What is the big deal?

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Copenhagen Post

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Citing case law, the High Court noted that such a claim - which would require a court to determine whether a child should have been born - "goes to the heart of what it is to be human, [something that] should not be asked of the law".
Mother sues for son's suffering
Aarti J Narsee | 29 August, 2014
“Had she known the severity of the risk, she would have aborted the fetus”
A damages claim of R6-million for the "wrongful suffering" of a child born with
Down's syndrome was heard in the Constitutional Court yesterday.

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Born to die? Woman sues for “wrongful life”A controversial case is presented before South Africa’s Constitutional Court, which could affect the way people with disabilities are treated
04 Sep, 2014
The case appears to be the first of its kind in South Africa and could go into case law history.
“The applicant appealed directly to the Constitutional Court arguing that South African law should be developed to allow the claim for ‘wrongful suffering’, as it terms the claim, particularly in light of section 28 of the Constitution which enshrines children’s rights, primarily requiring courts to consider the best interests of the child, and the Children’s Act,” the court papers said.

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Constitution (Chapter 2- Section 27/28)
Everyone has right to have access to health care services
No one may be refused emergency medical treatment
(?resuscitation of a 300g infant)
The state must take reasonable legislative and other measures within its available resources to achieve progressive realisation of these rights
Child’s best interests are of paramount importance

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
However ………
Truth does not always equal justice,
nor justice truth

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
So what’s all the fuss?Chromosome abnormalities represent 15% of congenital abnormalities. Of these, about one quarter is trisomy 21.
“Private eugenics” happen every day in hospitals all over the world and by far the most common “victims” are embryos equipped with an extra chromosome 21; Matt Ridley ”Genome”
Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Introduction
• Most foetuses with chromosomal abnormalities have either external or internal defects which can be recognized by detailed ultrasonographicexamination:
-Nearly all fetuses with trisomy 13
-77-100% of fetuses with trisomy 18
-50-75% of fetuses with trisomy 21

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Detection rate
False-positive rate
Unaffected
Affected
5%
FPR
2%
FPR
Screening in pregnancy
Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
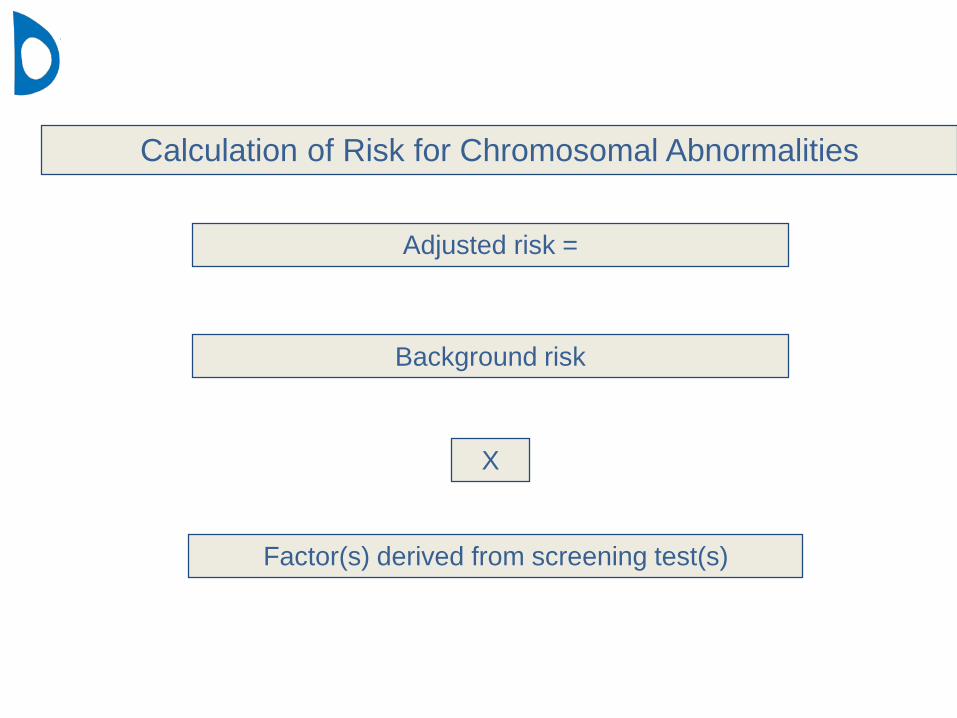
Calculation of Risk for Chromosomal Abnormalities
Factor(s) derived from screening test(s)
Adjusted risk =
X
Background risk
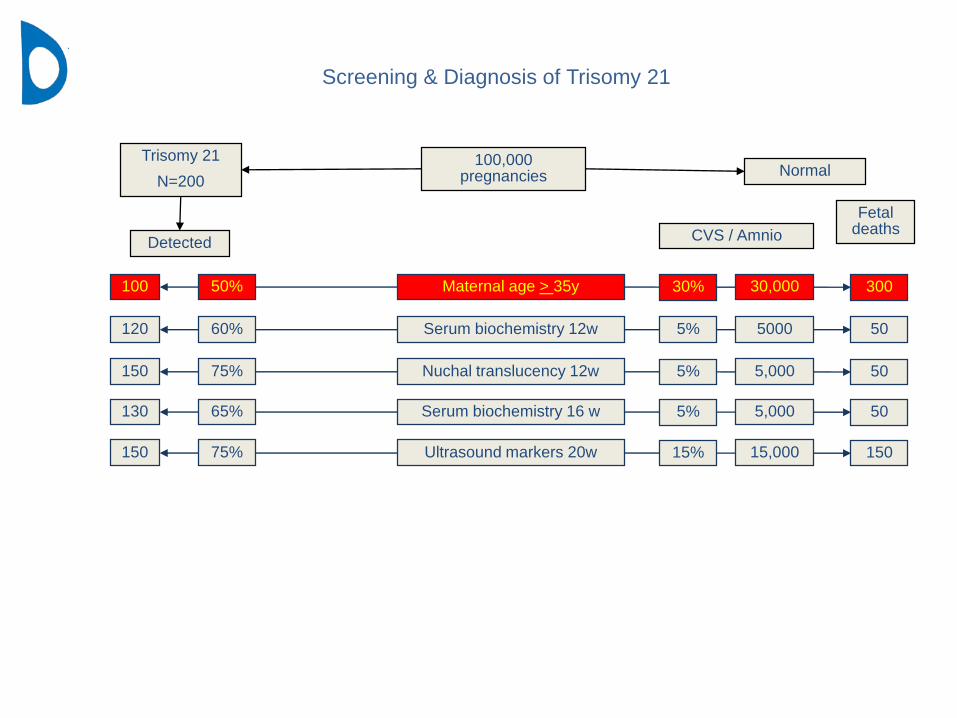
Screening & Diagnosis of Trisomy 21
Maternal age > 35y100 50% 30,000 30030%
Serum biochemistry 12w120 60% 5000 505%
Nuchal translucency 12w150 75% 5,000 505%
Serum biochemistry 16 w130 65% 5,000 505%
Ultrasound markers 20w150 75% 15,000 15015%
100,000 pregnancies
Trisomy 21
N=200Normal
Detected
FetaldeathsCVS / Amnio
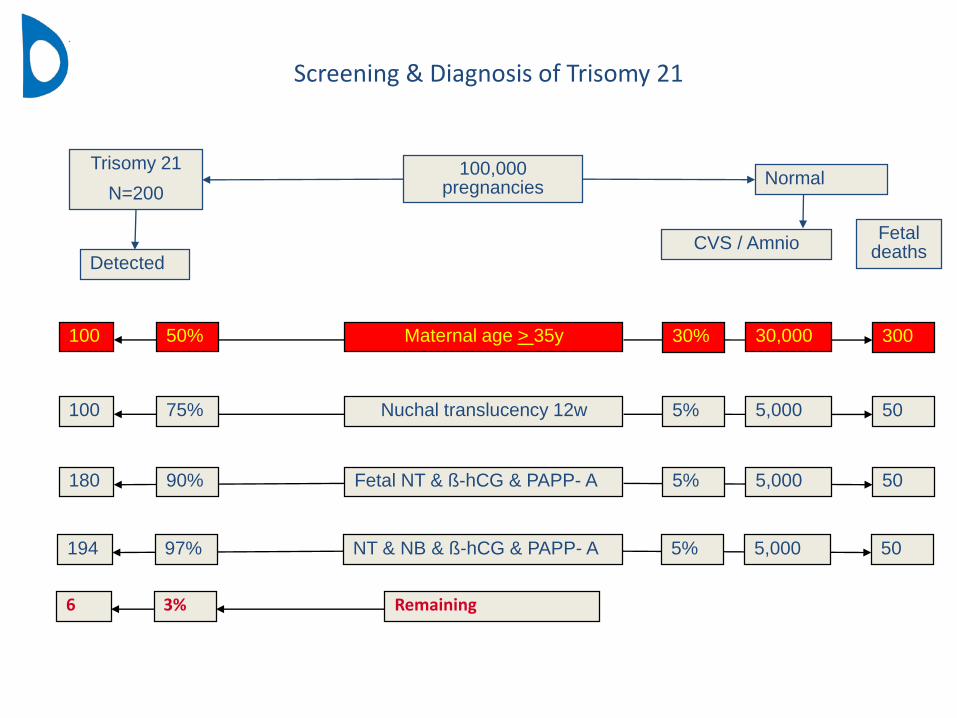
Screening & Diagnosis of Trisomy 21
Maternal age > 35y100 50% 30,000 30030%
100,000 pregnancies
Trisomy 21
N=200Normal
Detected
Fetaldeaths
CVS / Amnio
Nuchal translucency 12w100 75% 5,000 505%
Fetal NT & ß-hCG & PAPP- A180 90% 5,000 505%
NT & NB & ß-hCG & PAPP- A194 97% 5,000 505%
6 3% Remaining

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
Screening for Down’s syndrome: The 1st trimester

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
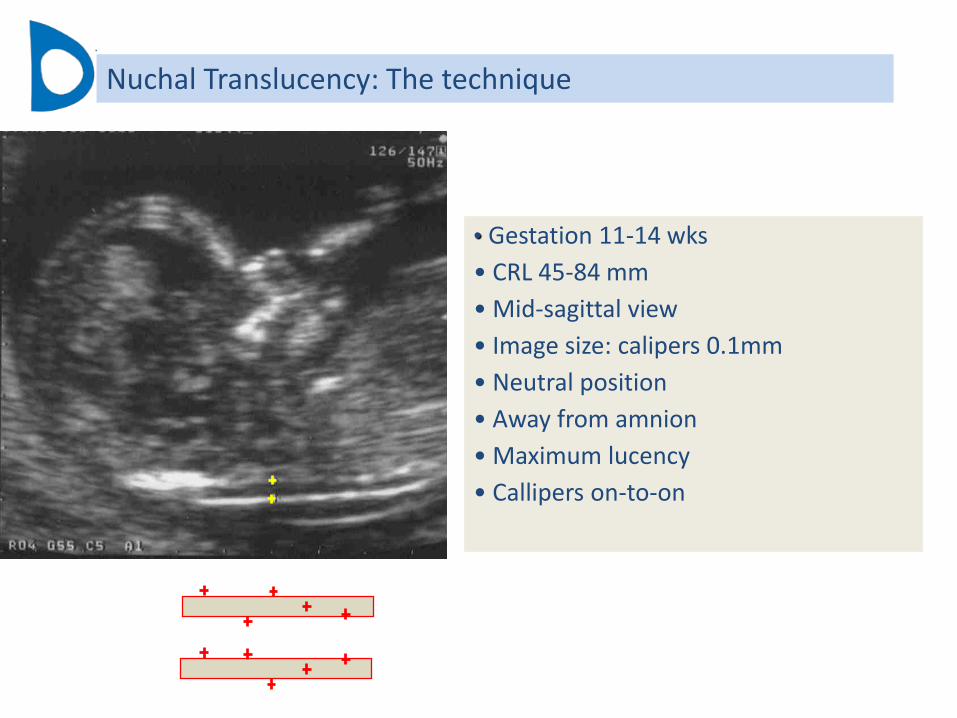
• Gestation 11-14 wks
• CRL 45-84 mm
• Mid-sagittal view
• Image size: calipers 0.1mm
• Neutral position
• Away from amnion
• Maximum lucency
• Callipers on-to-on
Nuchal Translucency: The technique

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
CRL: 54 mm
Calliper placement
Risk (%)
Age (years)
30 35 40 45
100
10
1
0.1
20 25
0.01
1: 600
1: 100
1: 3,700
1.5 2.9
Nuchal Translucency: The technique

0
2
4
6
8
10
12
14
16
18
20
-3.5 -2.5 -1.5 -0.5 0.5 1.5 2.5 3.5
Free ßhCG (SD)
%20
0
2
4
6
8
10
12
14
16
18
-3.5 -2.5 -1.5 -0.5 0.5 1.5 2.5
PAPP-A (SD)
%
Sensitivity 60% ; FPR 5%Spencer et al 1999
1st trimester biochemistry
Free beta HCG: …………. DR 25% PAPP-A: ………………………. DR 42%

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
1st trimester biochemistry

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
Estimated risk for trisomy 21
High-risk (> 1 in 100)2% of the population80% of Trisomy 21
Chorionic villous sampling2.5% of population90% of Trisomy 21
First-trimester screening
Low-risk (<1 in 1000)88% of the population5% of Trisomy 21
Ultrasound scan at 22 w
Intermediate-risk (1/101 – 1/1000)10% of the population15% of Trisomy 21
Ultrasound examination for:Absent nasal bone orAbnormal ductal flow orTricuspid regurgitation orWide facial angle
Positive Negative
cfDNA Test
Modified from Nicolaides, Advances in MFM 2013, London

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
NIPT (or better NIPS)
• During pregnancy, there are fetal cells and cell-free DNA fragments (cfDNA) from the fetus in the maternal circulation: the fetal fraction of cell-free DNA in maternal blood from week 10 is about 10-15% of all cell-free DNA
• It is possible to analyze this cell-free DNA to detect fetal trisomies such trisomy 21
Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
To date, there are two major bioinformatics approaches:
1. the first-generation “quantitative” or counting approach used bymostcfDNA-based tests,
2. The second-generation approach that incorporates genotypic information (SNP) (Natera).
NIPS

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
The way in which the algorithm works is that the sample itself is used as a control to detect gains or losses of chromosomes. For example:47,XXX:2 x Chr 13 ||2 x Chr 18 ||2 x Chr 21 ||3 x Chr X |||
Thus, the median ‘amount’ of each chromosome in the sample itself is two copies (which is quantified to give a particular baseline value, say 10 (where 5 comes from each copy). If the ‘amount’ of any chromosome deviates proportionately from this, it can be determined if a gain (trisomy) or loss (monosomy) is present. Thus for Chr X in this example, its quantitative value would be 3 x 5 = 15. Thus, it can be determined that this sample was 47,XXX.
NIPS

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
in the case of triploidy XXX (69,XXX), there will be three copies of every chromosome:3 x Chr 13 |||3 x Chr 18 |||3 x Chr 21 |||3 x Chr X |||
Thus for every chromosome, the inherent value for each would be a quantitative baseline value of 15. But because there are three copies of each chromosome, the quantitative algorithm estimates that every chromosome is in equal ratio (quantitative proportion) across the genome. Thus, a 69,XXX cannot be differentiated from a 46,XX.
NIPS limitations

Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
Society for Maternal-Fetal Medicine (SMFM) 34th Annual MeetingFebruary 3 - 8, 2014; New Orleans, Louisiana
Currently, the American College of Obstetrics and Gynecology and other specialty organizations recommend NIPT only for high-risk women. NIPT should be used when integrated screening identifies a woman as high risk.
NIPT failed to detect 22% of abnormalities in women younger than 25 years, but this dropped to 8% for women older than 45, "whose risk is driven by the high rate of common age-related aneuploidies for trisomies 18 and 21,"
Abnormality n Percent
Other trisomies 130 4.3
Duplications or deletions 90 3.0
Mosaic sex chromosomal abnormality
63 2.1
Common mosaics (trisomies 13, 18, 21)
32 1.1
Marker 14 0.5
Unbalanced translocations 9 0.3
Pathogenic Abnormalities Not Likely to Be Detected With NIPT
Chris Hani Baragwanath
Academic Hospital
Maternal Fetal
Medicine Centre
Use of biochemistry markers in the detection of Down’s
DR for T21
• Unconjucated estriol:… 4%• AFP: …………………………… 17%• HCG: …………………………… 29%• Combination of free beta HCG, AFP, E3 & MA : DR 60%
Haddow et al
Screening for Down’s syndrome: 2nd trimester 1. Biochemical screening

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Screening for Down’s syndrome: 2nd trimester 1. Biochemical screening
Variable Serum marker
Gestational age increases with GA
Weight inversely proportional to weight
IDDM uE3 and Inhibin A reduced
total/free -hCG unchanged
AFP ?significant effect
Recent bleeding variable increase in AFP
Afro-Carribean race AFP and hCG increased
Multiple pregnancy increased

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
2. “Markers”What is a marker?
• structural anomaly
• visible on ultrasound scan
• rarely of postnatal significance
but
associated with a chromosomal abnormality

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Trisomy 21 ultrasound features
Soft markers
• brachycephaly
• mild ventriculomegaly
• flattening of the face with nasal bone hypoplasia
• nuchal edema
• echogenic bowel
• mild hydronephrosis
• shortening of the limbs
• sandal gap
• clinodactyly
• mid-phalanx hypoplasia of the fifth finger
Structural (Hard) markers
• Atrioventricular septal defects,
• Duodenal atresia
• Congenital Diaphragmatic Hernia

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Abnormalities in Trisomy 21
Major defects
Cardiac (septal) defects
Duodenal atresia, CDH,
Seen in 15% T21 cases
LR for isolated marker 5x
VSD AVSD

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Factor(s) derived from screening test(s)
Adjusted risk
X
Background risk
=
Likelihood Ratio
LRNo defect 0.3 xMild hydronephrosis 1.0 x Short femur 1.5 xShort humerus 4.5 xEchogenic bowel 3.0 x Echogenic foci 1.0 xNuchal fold >6 mm 10.0 xHypoplastic nasal bone 50.0 x
Calculation of Risk for Chromosomal Abnormalities

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Detection rates for Trisomy 21 using ultrasound markers
Author Detection Rate
Sohl 1999 67.3%
Nyberg 2001 68.8%
Smith Bindman 2001 69.0%
Hobbins 2003 71.6%
Bromley 2002 80.5%
Devore 2000 91.2%
Vintzileos 1996 92.8%
Average: 77%

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Incidence of markers / defects in 2nd Trimester scan
Trisomy 21
(%)
Normal
(%)
Positive LR
(95% CI)
Negative LR
(95% CI)
LR for isolated
marker
Nuchal fold 107/319
(33.5)
59/9331
(0.6%)
53.05
(39.37-71.26)
0.67
(0.61-0.72)
9.8
Short
Humerus
102/305
(33.4)
136/9254
(1.5)
22.76
(18.04-28.56)
0.68
(0.62-0.73)
4.1
Short femur 132/319
(41.4)
486/9331
(2.6)
7.94
(6.77-9.25)
0.62
(0.56-0.67)
1.6
Hydronephrosis 56/319
(17.6)
242/9331
(2.6)
6.77
(5.16-8.80)
0.85
(5.16-8.80)
1
Echogenic
Focus
75/266
(28.2)
401/9119
(4.4)
6.41
(5.15-7.90)
0.75
(0.69-0.80)
1.1
Echogenic
Bowel
39/293
(13.3)
58/9227
(0.6)
21.17
(14.34-31.06)
0.87
(0.83-0.0.91)
3
Major
Defect
75/350
(21.4)
61/9384
(0.65)
32.96
(23.29-43.28)
0.79
(0.74-0.83)
5.2
Nyberg et al, 2001 ; Bromley et al, 2002; Nicolaides 2003

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Combination of Markers
Echo-
Foci
Mild Hydr Short
Femur
Short
Humerus
Echo-
Bowel
Nuchal
Fold
Echogenic
Foci
- X8 X15 X30 X25 X80
Mild
Hydronephrosis
X8 - X10 X30 X25 X80
Short
Femur
X15 X10 - X50 X40 X100
Short
humerus
X30 X30 X50 - X100 X300
Echogenic
Bowel
X52 X25 X40 X100 - X200
Nuchal
fold
X80 X80 X100 X300 X200 -
Nicolaides, Ultrasound Obstet Gynecol , 2003

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Nuchal Fold Thickness: LR 10
In TCD view Out-to-out >6mm
Short Humerus LR 4.1
Short Femur LR 1.6 Mild Hydronephrosis LR 1
<20wks AP 5mm
20-24 AP 7mm
25-30 AP 8mm
>30 AP 10mm

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Echogenic Focus in the heart LR 1.1 Hyperechogenic bowel LR 3
Other causesIntra-amniotic bleedFetal hypoxemiaCystic fibrosis

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
• Hypoplastic Nasal Bone
• Defined by :
- non visible nasal bone
- length BPD/NBL >10
J Ultrasound Med. 2002 Dec;21 (12):1387-94Fetal nose bone length: a marker for Down syndrome in the second trimesterBromley B, Lieberman E, Shipp TD, Benacerraf BR

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Trisomy 21 (n=21/34) 61.8%
Normal (n=12/982) 1.2%
Hypoplastic nasal bone
Screening for Trisomy 21
18-23 weeks scan
NB-hypoplastic LR 50 caucasians
NB-hypoplastic LR 20 africans
Cicero, Ultrasound in Obstet Gynecol. 2003 Jan; 21(1):15-8

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Not used in risk calculation but alerts to look for other markers!
Choroid Plexus Cysts

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Author Gestational
age (weeks)
Populati
on
Definition of
choroid plexus
cysts
Choroid
plexus
cysts n
(%)
Karyotype for isolated
choroid plexus cysts
Karyotype for choroid
plexus cysts and other
anomalies
Normal Abnormal Normal Abnormal
Clarke2 1988 16-22 2820 3-14 mm 5 (0.2%) 5 - - -
Camurri3 1989 16-20 3000 ? 10 (0.3%) 9 - - 1 T18
Ostlere4 1990 16-18 11700 ? 100
(0.9%)
97 - - 3 T18
Achiron5 1991 20 5400 8-18 mm 30 (0.6%) 28 1 T18 - 1 T18
Twining6 1991 18-20 4541 3-13 mm 19 (0.4%) 16 - 1 1 T18
1 T21
Chinn7 1991 15-24 1045 2-11 mm 38 (3.6%) 36 - 1 1 Triploidy
Howard8 1992 18-20 4765 ? 51 (1.1%) 50 1 T18 - -
Walkinshaw10
1994
17-19 15565 ? 152
(1.0%)
137 3 T18
1 T21
11 -
Gupta11 1995 16-20 151000 > 5 mm 524
(0.4%)
486 - 29 7 T18
2 T21
Reinsch*12
1997
16-20 7340 > 5 mm 71 (1.0%) 61 1 T18 6 1 T18
2 T21
Kilby13 1997 18-21 16059 ? 301
(1.9%)
263 - 35 2 T18
1 T21
Geary14 1997 20 10481 ? 79 (0.8%) 58 - 17 4 T18
Chitty 15 1998 18-20 13690 ? 84 (0.6%) 78 - 3 3 T18
Total 247406 1464
(0.6%)
1324
(90.5%)
6 T18
1 T21
(0.5%)
103
(7%)
23 T18
6 T21
1 Triploidy
(2%)
Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
No soft markers present - risk reduction
If the 18-23 week scan looks normal (No defects/markers)
•No previous NT scan reduce risk x 3
•With previous NT scan reduce risk x 2

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
• Offer all women 1st Trimester screening
• No need for 2nd Trimester serum screening
• Follow up with a detailed anomaly scan 20-23 weeks
Trisomy 21 screening: Conclusion 1
ACCREDITATION strongly recommended: 34 accredited practitioners in SA, today
Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
No 1st Trimester screening
1. Offer 2nd Trimester screening
2. Major defect offer karyotyping even if isolated(low prevalence, small cost implications)
Trisomy 21 screening: Conclusion 2

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
3. Women > 35 years:
Offer diagnostic tests de novo with soft markers and risk calculation
In women up to the age of 39 years, with a background risk of <1 in 100 the adjusted risk, in the absence of any markers, will reduce to >1 in 300 (reduction by a factor of three) and therefore with a risk cut-off of one in 300 they screen negative.
Trisomy 21 screening: Conclusion 3
Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
4. Women >40 years (low prevalence, small cost implications)
offer diagnostic testing
In women who are older than 40 years old, with no first trimester screening and a
background risk of >1 in 70, the adjusted risk after the second trimester scan
becomes <1 in 210 and therefore still remains screen-positive for Trisomy 21.
An invasive test could be considered here.
Trisomy 21 screening: Conclusion 4
Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
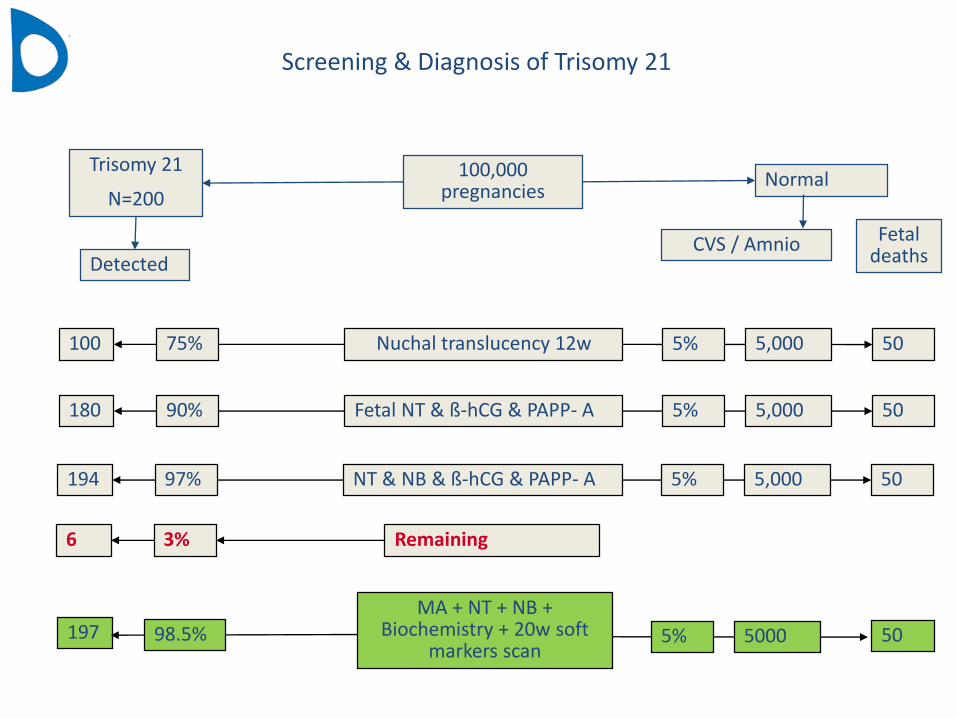
100,000 pregnancies
Trisomy 21
N=200Normal
Detected
Fetaldeaths
CVS / Amnio
Nuchal translucency 12w100 75% 5,000 505%
Fetal NT & ß-hCG & PAPP- A180 90% 5,000 505%
NT & NB & ß-hCG & PAPP- A194 97% 5,000 505%
6 3% Remaining
MA + NT + NB + Biochemistry + 20w soft
markers scan 197 98.5% 5000 505%
Screening & Diagnosis of Trisomy 21

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
Gestation (wks)
Amniocentesis
CVS
Cordocentesis
11w 14w
16w 24w
40w
Amniocentesis CVS Cordocentesis
Diagnosis of chromosomal defects
>23w

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital

Maternal Fetal
Medicine CentreChris Hani Baragwanath
Academic Hospital
WELCOME TO 12TH WORLD DOWN SYNDROME CONGRESS
19th - 21st August 2015 ITC Grand Chola, Chennai THE PANCHAYAT: PROGRAM FOR PERSONS WITH DOWN SYNDROME