trouble shooting of vr
TRANSCRIPT

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 1/40
Mechanical Ventilators
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 2/40
Mechanical
Ventilation

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 3/40
I. Objectives:
y Define mechanical ventilation.
y To learn the different major modes of mechanical
ventilation.
y To familiarize one·s self with the major parts and settings of
the mechanical ventilator.
y Describe appropriate nursing actions when each of the
major ventilator alarms sound.

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 4/40
II. Definition of terms:
M echanical Ventilation:
Forces air into the lungs either invasively(endotracheal tube or tracheostomytube)or non-invasively (mask) using mechanical ventilators

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 5/40
To achieve the goals without
damaging the lungs
To optimize gasexchange
To reproduce the body'snormal breathing
mechanism

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 6/40
Abbreviations:ETT: Endotracheal Tube PEEP: Positive End Expirator y Pressure
CPAP: Continuous Positive Airway Pressure, PEEP with no rate
PIP: Peak inspirator y pressure
MAP: Mean Airway Pressure
RR: Respirator y Rate Ti,Te: Inspirator y and expirator y times
I:E: Ratio of inspirator y to expirator y time
Vt: Tidal Volume, volume of each breath
SaO2: arterial oxygen saturation determined by arterial blood gas analysis
SpO2: arterial oxygen saturation determined by pulse oximetr y
FiO2: Fractional inspired oxygen HFV: High Frequency Ventilation
HFOV: High Frequency Oscillator y Ventilator/Ventilation
Amplitude: (aka Delta P) Setting on HFV. Difference between
maximum and minimum airway pressure
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 7/40
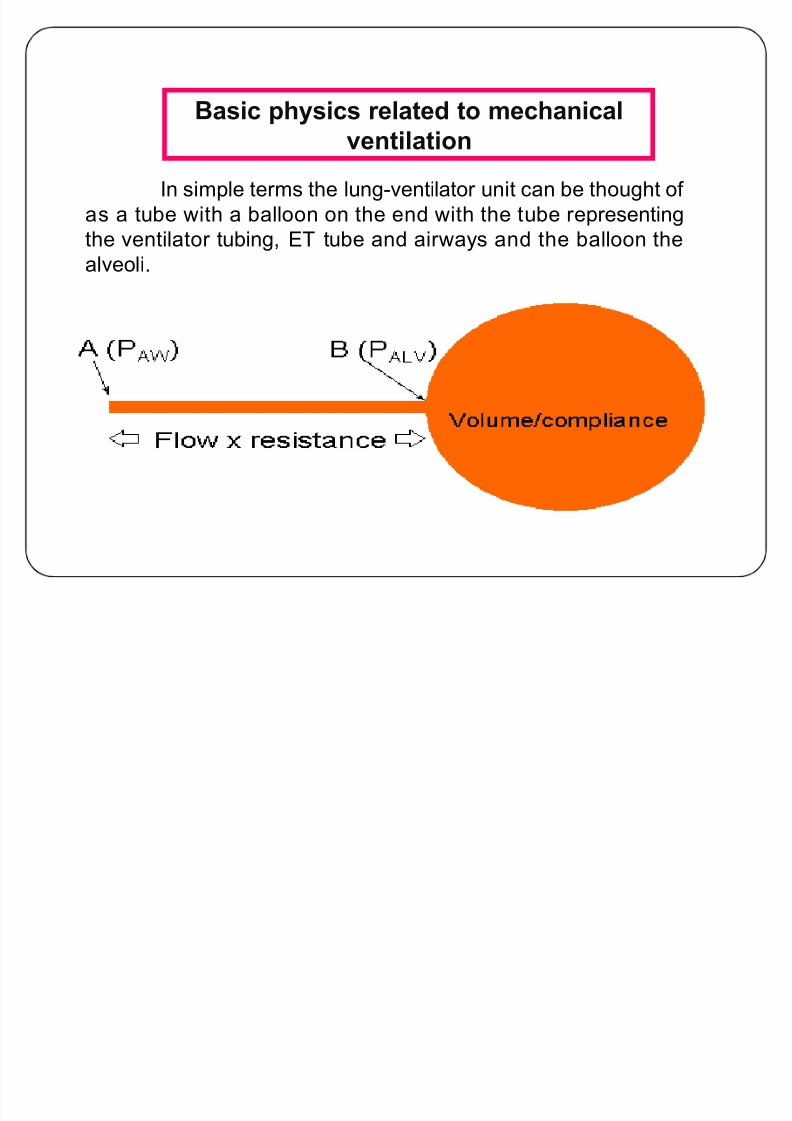
Basic physics related to mechanical
ventilation
In simple terms the lung-ventilator unit can be thought of
as a tube with a balloon on the end with the tube representing
the ventilator tubing, ET tube and airways and the balloon the
alveoli.
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 8/40
M
anually bag thepatient
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 9/40
Bilevel Positive Airway
Pressure Ventilation (BiPAP)

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 10/40
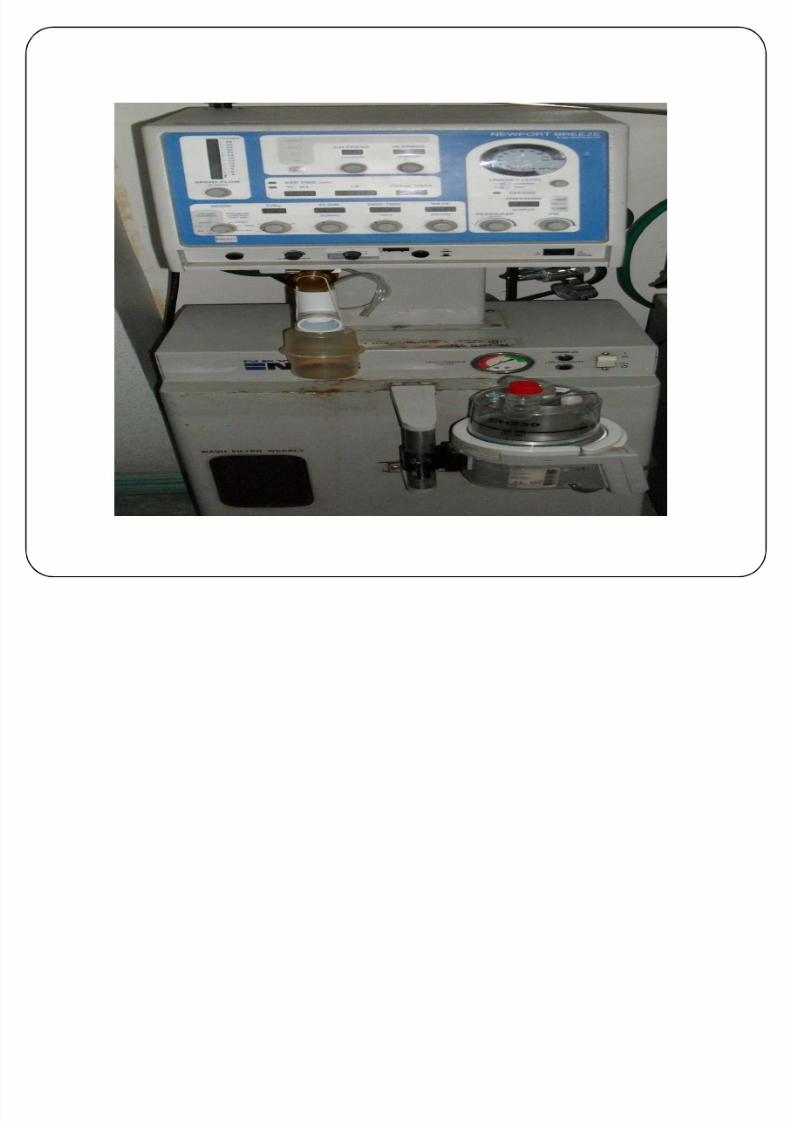
M echanicalVentilator
-is a machine that generates acontrolled flow of gas into a patient·s
airways with either negative pressure
(iro
n lung)o
r po
sitive pressure.

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 11/40
Negative pressure mechanical ventilators, like
the iron lung, encased the thoracic cavity externally in
an air-tight chamber . The chamber was used to create anegative pressure around the thoracic cavity, thereby
causing air to r ush into the lungs to equalize the
pressure. The iron lung is shown below.

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 12/40
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 13/40

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 14/40
Three Types of Ventilators
1. Volume-cycled
- Ventilator delivers gas until a set tidal volume has been
achieved regardless what the pressure would be.
E.g. Normal lung: TV = 500cc with PIP = 15
Stiff lung: TV = 500cc with PIP = 35 or 45
2. Pressure-cycled
- Ventilator will cycle & will deliver that preset TV
until the ventilator senses that it has obtained the
set pressure.E.g. PIP = 25 Ventilator is triggered Gas is delivered via ET
PIP of 25 is
reachedVentilator cycles off Enter exhalation phase
Classified accdg to cycling
mechanism

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 15/40
Three Types of Ventilators
3. Time-cycled
-is used much less frequently
- in the past used in anesthesia machines
- Preset inspirator y time
E.g. Set @ 3 sec. Ventilator is triggered Gas f lows for 3 sec.
As 3 sec is
reached
Flow of gas is
terminated

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 16/40
III. Modes of Ventilation
H ow the patient interacts w/ the mechanical ventilator
1. Controlled Mechanical Ventilation (CMV)
Ventilator is set to deliver a certain volume of gas in a
set period of time.
Rarely used.
E.g. R R = 10 bpm & TV = 500cc
This means, the patients receives 500cc ever y 6 seconds
What happens if the patient breathes @ 8x or 20x per
minute? Or initiates a breathe @ 3 seconds?
What happens if the patient takes a TV= 200cc or 700cc?

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 17/40
III. Modes of Ventilation
2. Assist Control Mode - AC
The ventilator guarantees that the patient will
receive the set minimum number of breaths, although
he/she is able to demand (trigger) more.
Most commonly used mode.
E.g. TV = 500cc; BUR = 10 bpm
This means that the patient receives 500cc ever y 6 seconds.
What happens if the patient initiates a breathe @ 3 second?
What happens if the patient wants 200cc of breathe?
TV= 500cc given.
TV= 500cc

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 18/40
III. Modes of Ventilation
3. Synchronized Intermittent Mandator y Ventilation
(SIMV)
Weaning mode
Advantages:
Patient is able to maintain their respirator y strike
It is more comfortable
Mean airway pressure is less
Less hyperventilation
In contrast with AC mode, SIMV mode allows the
patient to have their own rate & tidal volume.

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 19/40
III. Modes of Ventilation
4. Positive End Expirator y Pressure (PEEP)
Is the level of baseline pressure during the use of a
separate mode of ventilation.
Use in conjunction
with other modes
It prevents closing of alveoli.
E.g.
PEEP @ 5 cm H20

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 20/40
III. Modes of Ventilation
5. Pressure Support Ventilation
Overcomes the resistance of ventilator tubings
Decreases the work of breathing
E.g. TV = 500cc & PIP = 30Patients in the ICU unit:
They may need to breathe adequate spontaneous breathe of
500cc 10/12x a minute but, they can¶t.
Pressure support ventilation mode augment pressure
support
Therefore, the work they do to get 400cc gets them 500cc.
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 21/40
Complications
1. Nosocomial Pneumonia
2. Barotrauma
Not only due to high pressures
Due to high volumes and shear injur y
Damages the alveolar tissue & leads to alveolar r upture
3. Gas trapping
Occurs if there is insufficient time for alveoli to empty
before the next breath. E.g., asthma & COPD
4. Cardiovascular compromise
Due to high intrathoracic pressure. In an extreme case can
lead to cardiac arrest with pulseless electrical activity.
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 22/40
Part I ± In summar y
1. Three types of ventilators:
Volume-cycled
Pressure-cycled
Time-cycled
2. Modes of Ventilation
CMV
AC SIMV
PEEP
Pressure support
3. Complications
Nosocomial pneumonia
Barotrauma
Gas tapping
Cardiovascular
compromise

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 23/40
IV. Ventilator Controls and Settings
(Puritan Bennett)
A. Panel Controls:
1. Normal Volume/ML or Tidal Volume:
- each volume of air that the clientreceives with each breath
- spirometer indicates whether the patient is receivingcorrectTV or amount delivered with each machine breath

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 24/40
2. Rate:
- number of ventilator breaths delivered per minute (set as
desired)
3. Peak flow:
- set f or peak unrestricted flow
- start at approximately 40LPM, adjust to
accordance with volume and rate settings

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 25/40
4. Power
5. Normal Pressure Limit and sigh pressure limit
6. Sensitivity:
- set f or patient eff ort to trigger inspiration
7. Manual Normal, Manual Sigh, Sigh volume

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 26/40
8. Oxygen percentage or FiO2
9. Expiratory resistance
10. Nebulizer
B. Panel Indicator Lights:
1. Assist:
- lights if patient triggers inspiration
- also lights if sensitivity is overset

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 27/40
2. Pressure:
- lights if system pressure reaches set limit
- check f or airway o bstruction
3. Ratio:
- lights if inspiration is longer than expirationwhen unit is controlling
4. Sigh:
- lights during a sigh breathing cycle
- may be used to prevent atelectasis

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 28/40
5.
Ox
ygen:
- lights green if with oxygen enrichment
- lights red if oxygen supply is inadequate
- at turn on, may light red momentarily; this
denotes proper initial filling of the accumulator

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 29/40
C. Other Controls and Indicators:
1. Spirometer ² indicates TV
2. Spirometer alarm
3. Humidifier
4. Thermometer
5. Pressure alarm ² sounds if system pressure
reaches set limit
6.
Ox
ygen alarm7. Temperature alarm
8. PIP/Peak Inspiratory pressure

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 30/40
IV. Sharpening your skills - trouble shooting
VR:
A. Assessment:
1. How severe is the pro blem?
2. Does the patient require immediate
resuscitation?2. Check:
2.1 Is the chest moving and is it moving
symmetrically?
2.2 Is the patient cyanosed?

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 31/40
2.3 What is the arterial saturation?
2.
4 Is the patient hemo
dynamically stable?
3. Diagnosis:
- ventilator/ circuit pro blems can be distinguished
from ET or patient pro blems by taking the patient
off the ventilator and continually bagging the patient
with a self
² inflating resuscitator.

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 32/40
IV. B. Identifying Causes of Alarms:
1. High airway pressure:
Why does it matter?
a. High airway pressure may cause barotrauma b. It signifies a deterioration in the patients
clinical state.
c. It may result in hypoventilation of the patient .
Many ventilates cycle from inspiration to expiration immediately if the pressure alarm
limit is reached.

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 33/40
as a result, inspiration is terminated early and the tidal volume is
reached.
Causes:
a.Ventilator pro blems:
- excessive tidal volume
- excessive flow or expensively short inspiratory
time
- high airway pressure alarm limit too low

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 34/40
2.Ventilator malfunction ² rare
b. Circuit pro blems:
1. Fluid pooling in circuit ² empty
2. Fluid pooling in filter3. Kinking of circuit - fix

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 35/40
C. ET Obstruction:
1. due to sputum ² needs suctioning
2. Patient is coughing or holding her breath or is
biting the ET
D. IncreasedAirway Resistance
1. bronchospasm

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 36/40
E. Decreased Respiratory System Compliance:
1. Parenchymal disease
2. Pleural disease (pneumothorax/hemothorax)
3. Decreased chest wall compliance
e.g. Patient is anxious or fights the ventilate4. Decreased Ventilated lung volume
a. Sputum plugging ² good suctioning
b. Labor/ lung collapse
c. Endo bronchial intubation

8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 37/40
1.Assess patient
2. Disconnect patient from ventilator and manually
ventilate using self ² inflating resuscitator.
Assess the ´feelµ of the lungs. If the patient is
difficult to ventilate it is a pro blem with the
endotracheal tube or the respiratory system.
3.
Fo
r ventilato
r and circuit pro blems, check ventilat
or
settings and function, and check circuit f or o bstruction
or kinking.
Management:
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 38/40
Fo
r patiento
r ET
pro blems, e
xamine the patient l
ookingparticularly f or wheeze, asymmetrical chest expansion and
evidence of collapse. Pass a suction catheter through the ETT to
check its patency.
4. Chest X ²ray ² needs doctor·s order.
5. Contact RCS personnel
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 39/40
Low pressure alarms goes off:
1. Patient is ́ overbreathingµ ² drawing more air than theventilator delivers.
2. There·s a leak in the system, from a hole in the tubing, adisconnected tube, a leak around the cuff, or a leak inthe humidifier.
8/7/2019 trouble shooting of VR
http://slidepdf.com/reader/full/trouble-shooting-of-vr 40/40
Thank you !!!