tuberculosis in virginia? wendy heirendt, mpa public health advisor division of tb control virginia...
TRANSCRIPT
Tuberculosis in Virginia?
Wendy Heirendt, MPAPublic Health AdvisorDivision of TB ControlVirginia Department of HealthSeptember 12, 2005

Areas to be Covered Tonight
Epidemiology of TB in Virginia Diagnosis, Transmission, Treatment Role of the Health Department
Current TB Challenges in Virginia
329 cases in 2004, <1% decrease from 2002 Majority (39%) of the cases in 25-44 year olds 16.5% were in persons 0-24 years of age
Large number of TB patients are born outside the US 43 nationalities 17 primary language, non-English
Cases reported in 34 of 35 health districts

Number of Reported TB Cases inVirginia, 1986-2004
329

TB Case Rates in Virginia, 1996-2004
Year Cases VA Rate US Rate1996 349 5.3 8.0 1997 349 5.3 7.41998 339 5.2 6.81999 334 4.9 6.4 2000 292 4.1 5.82001 306 4.3 5.6 2002 315 4.5 5.22003 332 4.5 5.12004 329 4.4 4.9

Percent of Reported TB Casesby VA Region: 2003 and 2004
Central20%
Eastern18%
Northern46%
Northwest9%
Southwest
7%
2003
Central15%
Eastern20%
Northern51%
Northwest7%
Southwest
7%
2004
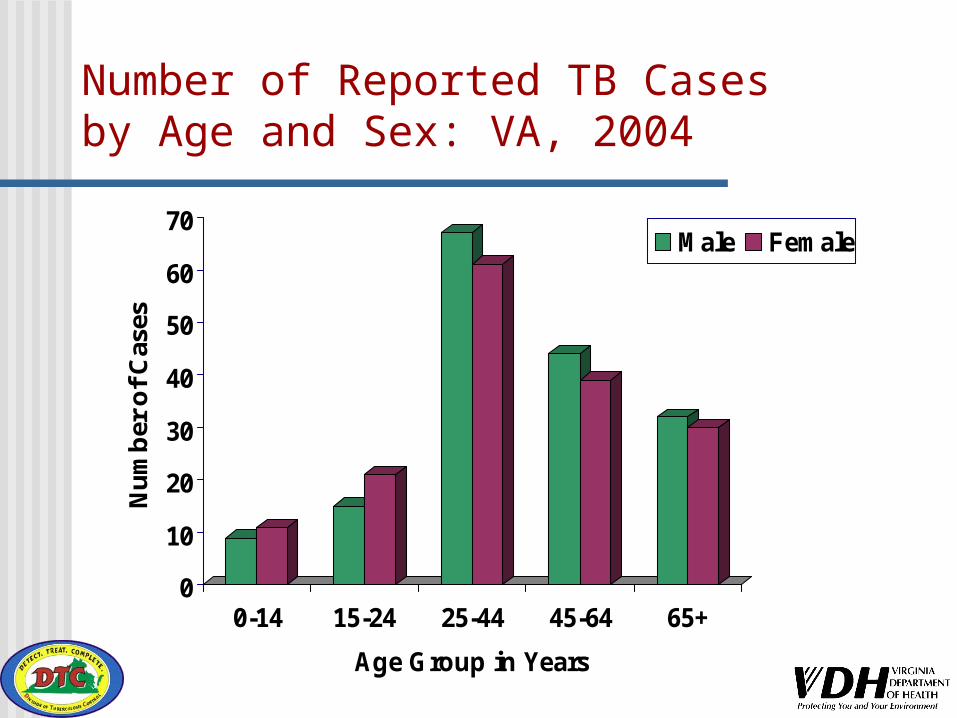
Number of Reported TB Cases by Age and Sex: VA, 2004
0
10
20
30
40
50
60
70
Nu
mb
er o
f C
ases
0-14 15-24 25-44 45-64 65+
Age Group in Years
Male Female

Chart 6
Percent of Reported TB Casesby Age: VA, 1996-2004
0
10
20
30
40
50
1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
Per
cen
t o
f C
ases
0-14 15-24 25-44 45-64 65+

Number of Reported Foreign-Born vs.US-Born TB Cases, VA 1996-2004
0
50
100
150
200
250
1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
Nu
mb
er
of
cases
US Born Foreign Born

*Culture confirmed cases with drug susceptibility tests performed
MDR Cases & Percent of Resistance toAny First Line Drugs: VA, 1998-2004
1
4
7
4
21
10
3.3
11
9.5
14.113.4
12.2
16.3
0
2
4
6
8
10
12
1998 1999 2000 2001 2002 2003 2004
Nu
mb
er
0
2
4
6
8
10
12
14
16
18
Per
cen
t

Number of Reported TB/AIDS Cases: VA, 1993-2004
0
5
10
15
20
25
30
35
Year
Nu
mb
er o
f C
ases
What is TB??
Disease caused by Mycobacterium tuberculosis
Airborne disease passed from person to person
Can be cured with medications Treatment for latent TB infection
Famous TB Patients Doc Holliday of Wild West fame Christy Mathewson of baseball lore Eleanor Roosevelt, First Lady Edgar Allan Poe and associates

How TB is Transmitted
TB transmission occurs when a person with active, infectious TB disease coughs, sneezes, laughs, sings, etc.
TB spreads through the air by inhaled droplet nuclei
TB needs prolonged contact for transmission

Factors Affecting TB Transmission
How infectious is the person with TB disease?
Where does the exposure to TB infection occur?
How much time does a person spend with another person who has infectious TB disease?
source
contact
environment
Infection Can Result in… Limited disease Latent TB, no
symptoms, not sick, positive skin test, cannot transmit to othters
Active Disease progressive, M.tb replicating in any organ, only pulmonary is infectious

Active TB Disease
May be infectious
Has clinical symptoms
Usually pulmonary involvement
Symptoms of Active TB Disease
Prolonged cough(may produce sputum)*
Chest pain* Hemoptysis* Fever Chills
*Symptoms commonly seen in cases of pulmonary (lung) TB
Night sweats Fatigue Loss of appetite Weight loss or
failure to gain weight

Diagnostic Techniques Tuberculin Skin Test
A decision to test is a decision to treat
Sputum collection/testing Chest x-ray Medical evaluation

Medications for TB Disease
Standard medication regimen Minimum of 6 months of therapy,
sometimes longer Initial 4 drug therapy standard:
• Isoniazid (INH)• Rifampin (RIF)• Pyrazinamide (PZA)• Ethambutol (EMB)
Medications may need to be changed if the TB is drug resistant to any medication listed above
Directly Observed Therapy (DOT)
A health care worker watches a TB patient swallow each dose of the prescribed drugs
DOT is recommended for all persons who have TB disease
The health care worker will conduct DOT at a time and place convenient for each patient who has TB disease

Latent TB Infection (LTBI)
Occurs when TB bacteria are in the body, but are inactive or latent
No clinical symptoms of active TB disease Not infectious to others Positive reaction to the TB Skin Test Normal chest X-ray

Treatment of Latent TB Infection (LTBI)
Treating LTBI prevents the development of TB disease, especially for persons at high risk for developing TB disease if infected with TB
Usual medication regimen for treating TB infection Isoniazid (INH) for 9 months Rifampin for 4 months is alternative in
certain circumstances

Persons at Higher Risk forBecoming Infected with TB
Close contacts of persons known or suspected to have active, infectious TB disease
Foreign-born persons from areas in the world where TB is common
Residents and employees of high-risk congregate settings
(Continued on next slide)
Persons at Higher Risk for Becoming Infected with TB
Health care workers who serve high-risk clients
Children exposed to adults in high-risk categories

TB and HIV Coinfection: Reason for Concern For persons infected with TB, HIV positive
status is the strongest risk factor for developing active TB disease
In persons who are HIV positive and have TB infection, the chances of developing TB disease increases from 10% in a lifetime to 7% to 10% each year!

Public Health Implications
Contagious, airborne disease Isolation of the infectious person
must be instituted to prevent transmission
Identification of exposed and infected contacts (by Regulation)
Treatment for all

Case Study 34 y.o. male diagnosed with infectious TB Hx of negative TST, <12 months ago No known TB exposure Family, co-workers tested; no new cases
Is this CI complete?
Another Case Study 30 yo male, infectious pulmonary TB Carpools to work at call center Risk to carpoolers? Workmates? Work from home? Other type of
work for few weeks?
One More 20 y.o. college student Needs baseline TST for practicum at
hospital Hx of BCG vaccination as a child Unsure of TST status TST= 12mm, cxr negative Start student on 9 mos of INH??

TB Issues in a Disaster Known TB cases are displaced[Focus on active; ignore LTBI] Treatment is interrupted Possible transmission – concern in
shelters, buses, cars, homes

Things to Consider Plans- hope TB cases present to HD HD obtains history, treatment info May need cxr, labs Most will be non-infectious Isolate if coughing, not on meds Numbers are likely to be small

TB Prevention and Control: Short Term Shelters Same as acute illness screening on
admission to shelters Look for symptoms Use form; administer by non-HCP Separate symptomatic from the crowd
ASAP….med evaluation ASAP Obtain consent, recent and past medical
hx, placement hx, We are not recommending TST Ignore LTBI…no symptoms, not infectious

TB Prevention and Control: Long Term Shelters Consider additional screening based
on identified risk factors Likely exposure High risk medical conditions
Other Thoughts
For HCPs: Communications (cell/satellite phones,
internet, fax, copiers) Office supplies Confidential files, locked syringe box Past medical histories from home state Refrigeration for vaccines, etc

More Thoughts
For the evacuees Handicap accessible, laundry facilities,
bed linens, showers, food service, phone connections, internet,
Recreational facilities, Playgrounds, other diversions
Mental health resources, social workers Facility ID cards, Medicaid applicaitons

Resources http://
www.bt.cdc.gov/disasters/hurricanes/katrina/shelters.asp
http://www.nationaltbcenter.edu/catalogue/downloads/tbhomelessshelters.pdf
http://www.umdnj.edu/ntbcweb/docs/Contact%20Investigations.pdf
http://www.umdnj.edu/ntbcweb/docs/congregate/CongregateSetting.pdf

For More Information…
Virginia Department of Health Division of TB Control109 Governor Street, First Floor Richmond, VA 23219804-864-7906 http://www.vdh.virginia.gov/epi/tb
Local Health Departmentshttp://www.vdh.virginia.gov/LHD/LocalHealthDistricts.asp
Centers for Disease Control and PreventionDivision of TB Eliminationhttp://www.cdc.gov/nchstp/tb