tuberculosis & special populations - national-academies.org/media/files/activity...
TRANSCRIPT
Tuberculosis &
Special populations
Sonya Shin, MD, MPH
Division of Infectious Diseases
Division of Global Health Equity
Brigham and Women’s Hospital
Partners In Health, Boston MA

Overview
TB & HIV
TB & Alcohol
TB & PediatricsTB & Pediatrics

Risk factors: special populations
Susceptible
hostsTB MDR-TB,
XDR-TB
Excess morbidity and
mortality

Risk factors: special populations
Susceptible
hostsTB MDR-TB,
XDR-TB
Excess morbidity and
mortality

Godfrey-Faussett et al, 2002 Excess cases of Tuberculosis in Sub-
Sarahan Africa attributable to HIV

Transmission of TB and HIV in
Russia

Experience in Peru: MDR-TB and
HIV co-infection
99 HIV-positive individuals receiving treatment for MDR-TB in Lima, Peru
July 1996 – December 2005July 1996 – December 2005
MOH offers free HAART in 2004; prior to this, donated on individual basis

Experience in Peru: MDR-TB and
HIV co-infection, N=99
ETOH abuse 11%
Previously treated 94%
Extra-pulmonary TB 41% Extra-pulmonary TB 41%
Cavitary disease 46%
Mean CD4 cell count 181

Experience in Peru: MDR-TB and
HIV co-infection
Treatment outcomes
Cure
Failure
Death
Default
in treatment
Transferred

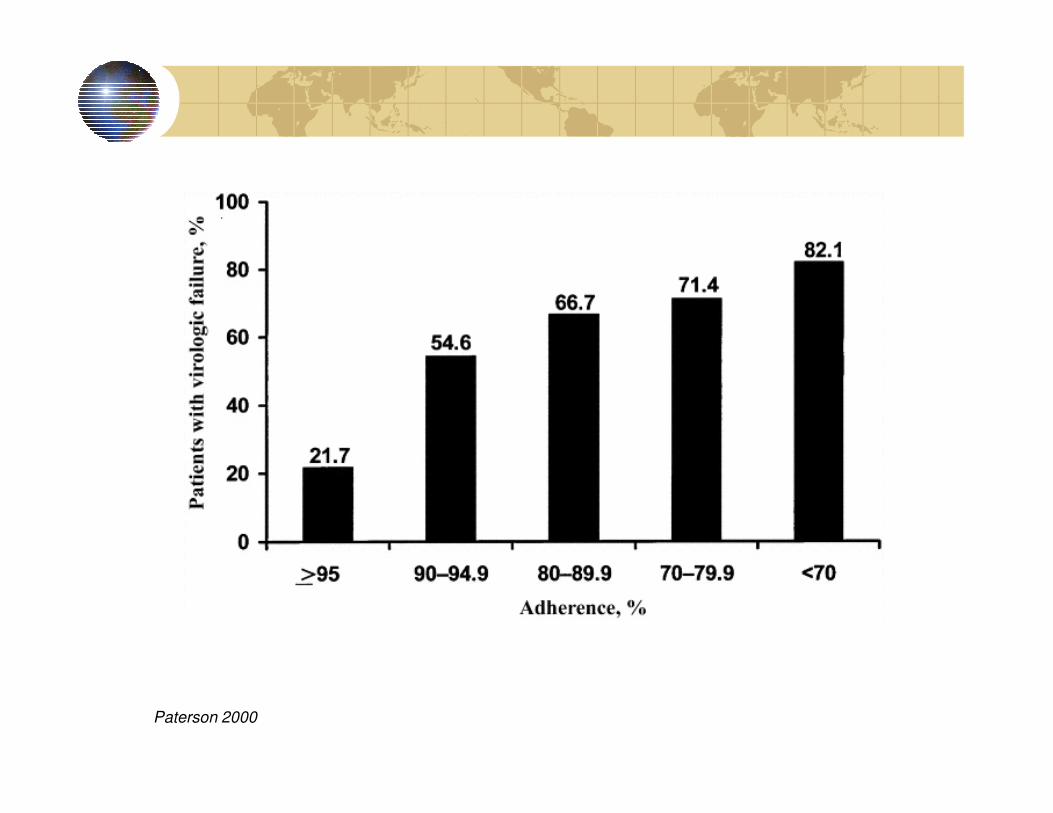
Paterson 2000

DOT for TB and HIV TreatmentHospitalizations and outpatient visits per person-year
Surv
ival D
istr
ibution F
unctio
n 0.75
1.00
Proportion of patients alive and on HAART by time from enrollment
Surv
ival D
istr
ibution F
unctio
n
0.00
0.25
0.50
Time from enrollment (days)
0 100 200 300 400 500 600 700 800
STRATA: CASA Control Censored
Log-Rank test of equality p=0.01

DOT for TB and HIV TreatmentHospitalizations and outpatient visits per person-year
CASA Control
N=33 N=33 IRR (95% CI) IRR (adj) (95% CI)
Unadjusted Adjusted*
Observation days 21160 16628
per enrollee 641.21 503.88
Hospital admissions 25 41
per person-year 0.43 0.90 0.45 (0.19-1.08) 0.42 (0.16-1.10)
Hospital days 315 675
per admission 12.60 16.46 0.77 (0.43-1.35) 0.83 (0.44-1.55)
per person-year 5.43 14.82 0.35 (0.14-0.91) 0.33 (0.11-0.95)
Outpatient visits 1426 1509
per person-year 24.60 33.12 0.73 (0.62-0.87) 0.75 (0.63-0.89)
*Adjusted for drug or alcohol use and marriage status

Risk factors: special populations
Susceptible
hostsTB MDR-TB,
XDR-TB
Excess morbidity and
mortality

TB-Alcohol activities in Tomsk, Russia
Programmatic: Improve management of AUDs within Tomsk TB services within Global Fund (Eur J Public Health 2009)
Research:Prevalence study of AUDs using valid instrument (Substance Use & Misuse 2010)Ethnographic study (Culture, Medicine Ethnographic study (Culture, Medicine and Psychiatry 2010)Role of alcohol on causes of death (IJTLD 2006)Randomized Controlled Trial to assess effectiveness of alcohol interventions on TB and alcohol outcomes (ACER, 2010)

Стандартная Порция Алкоголя (СПА) Standard Drinks Card
4% 1000 мл
= 3 СПА
4% 500 мл
= 1,5 СПА
4% 330 мл
= 1 СПА
Beer / ПИВО Wine / ВИНО
12% 750 мл
= 7,3 СПА
14% 750 мл
= 8,3 СПА
Vodka / ВОДКА
Samogon
Cognac / КОНЬЯК
Whiskey ,Gin / ВИСКИ, ДЖИН
TINCTURE, EAU-DE-COLOGNE
/Настойки , Одеколоны
40% 500 мл
= 16 СПА
40% 100 мл
= 3,2 СПА
5% 330 мл
= 1,3 СПА
Surrogate Spirits, Technical Spirits
Liqueur, Port/Sherry Wine
/Ликёры, Наливки, Портвейн
TOTBS/PIH
40% 700 мл
= 22 СПА
Samogon /Настойки , Одеколоны
40% 30 мл
= 1 СПА
62% 100 мл
= 5 СПА
Surrogate Spirits, Technical Spirits
/ Технические Жидкости
90% 700 мл
= 50 СПА
90% 500 мл
= 35,6 СПА
90% 200 мл (стакан)
= 14 СПА
/Ликёры, Наливки, Портвейн
20% (25%) 100 мл
= 1,6 (2) СПА

Alcohol and TB management:
Integrating ETOH interventions into TB care… in Russiacare… in Russia
Naltrexone
Brief counseling
Potential impact on TB and ETOH outcomes
NIAAA R01 AA016318
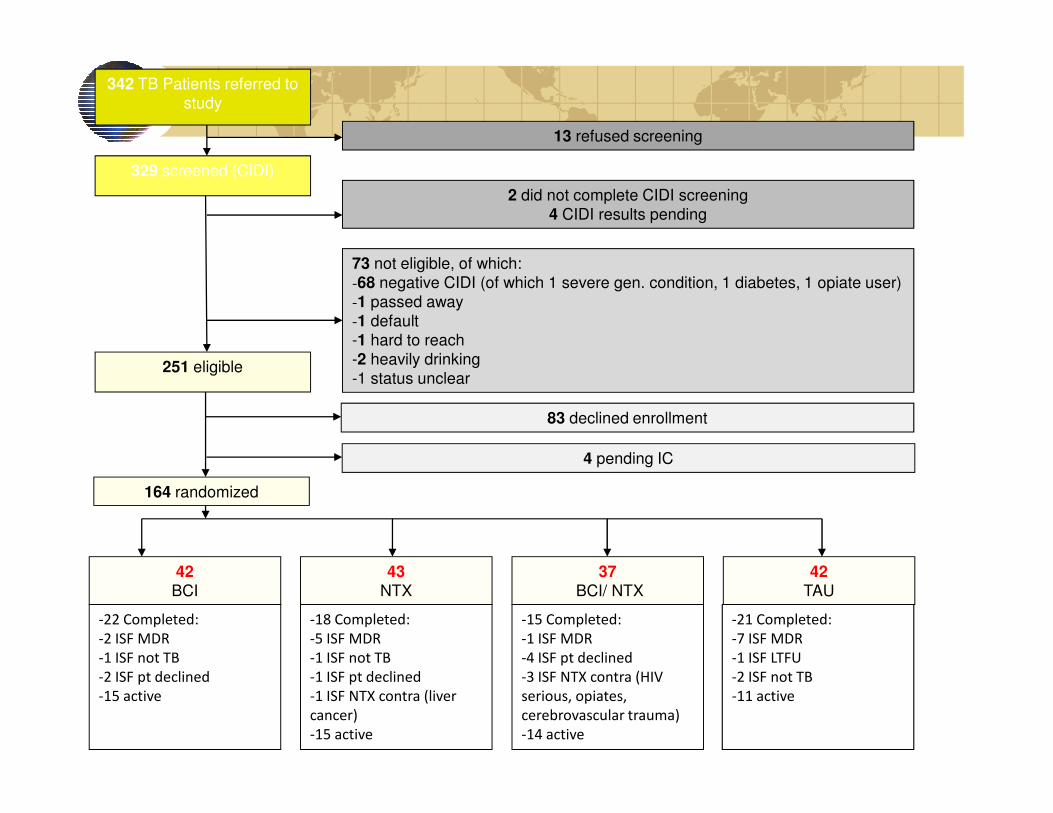
342 TB Patients referred to
study
329 screened (CIDI)
251 eligible
13 refused screening
2 did not complete CIDI screening
4 CIDI results pending
73 not eligible, of which:
-68 negative CIDI (of which 1 severe gen. condition, 1 diabetes, 1 opiate user)
-1 passed away
-1 default
-1 hard to reach
-2 heavily drinking
-1 status unclear
164 randomized
42
TAU
37
BCI/ NTX
43
NTX
42
BCI
83 declined enrollment
4 pending IC
-22 Completed:
-2 ISF MDR
-1 ISF not TB
-2 ISF pt declined
-15 active
-18 Completed:
-5 ISF MDR
-1 ISF not TB
-1 ISF pt declined
-1 ISF NTX contra (liver
cancer)
-15 active
-15 Completed:
-1 ISF MDR
-4 ISF pt declined
-3 ISF NTX contra (HIV
serious, opiates,
cerebrovascular trauma)
-14 active
-21 Completed:
-7 ISF MDR
-1 ISF LTFU
-2 ISF not TB
-11 active

Risk factors: special populations
Susceptible
hostsTB MDR-TB,
XDR-TB
Excess morbidity and
mortality

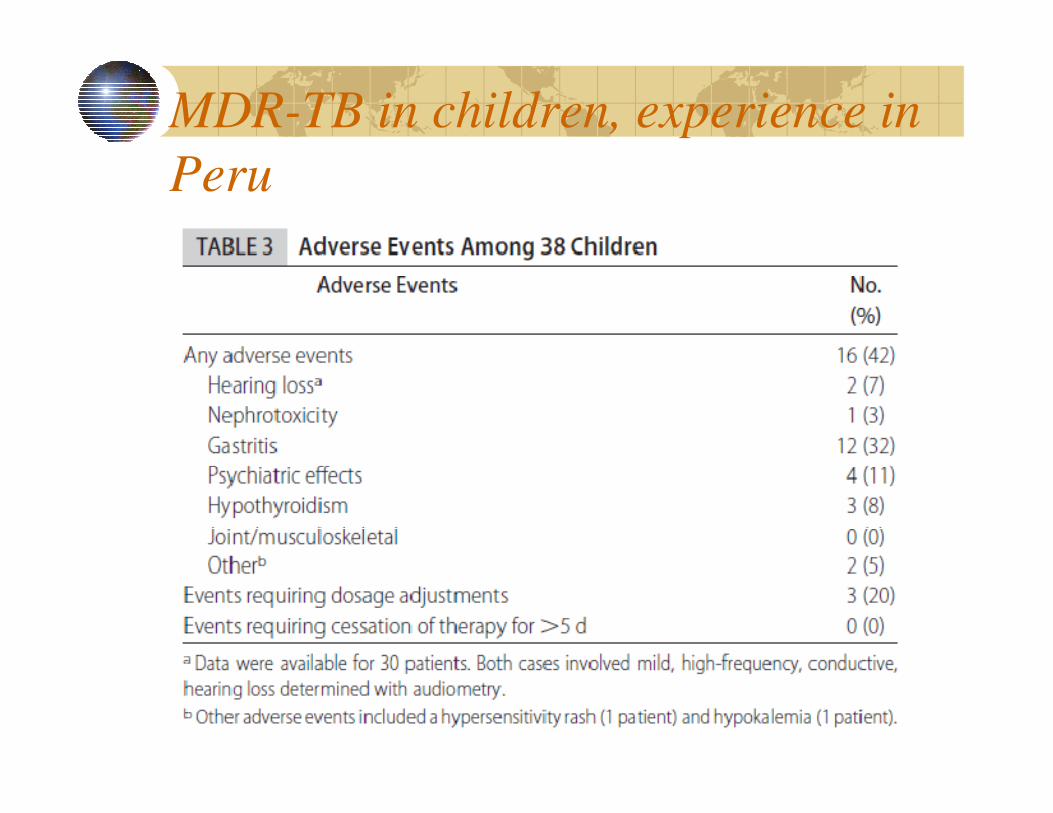
MDR-TB in children, experience in
Peru
38 children
Median age: 11 (2-14)
Primarily household contactsPrimarily household contacts
Time from first TB diagnosis to MDR-TB treatment: 6.5 months (0-46)
Drobac Pediatrics 2006
MDR-TB in children, experience in
Peru


Thank you very much!