tumor immunology. 14 million new cancer cases/year worldwide /50% mortality 10 16 cell division in a...
TRANSCRIPT

TUMOR IMMUNOLOGY

•14 million new cancer cases/year worldwide /50% mortality•1016 cell division in a lifetime•Each of us carries 60 or more girmline mutations not present in parents

• MORE THAN 100 VARIOUS TUMOR TYPES• MULTISTEP TUMORIGENESIS • DYNAMIC CHANGE OF TUMOR GENOME
– Genetic instability– Oncogenes – ‘gain of function’ change– Tumor suppressor genes – recessive ‘loss of function’ change
• PROGRESSIVE TRANSFORMATION– Benign tumor abnormal, but limited growth– Malignant tumor unlimited growth, break basal membranes,
invasion – Metastatic tumor seeds new tumors at distant sites.
• MULTIPLE LIMITING AND INHIBITORY CHECK POINTS– Growth advantage– Selection
• REGULATORY CIRCUITS– Inherent cell autonomous regulatory mechanisms – Microenvironmental factors
Cancer is a result of multiple mutations
INDEPENDENT OF THE IMMUNE SYSTEM

Benign or malignant tumors

ACTIVATION OF ONCOGENESMitogens
Growth factor receptors Secondary messengers
Tarnscriptional activators Cell cycle genes
INACTIVATION OF TUMOR SUPPRESSOR GENES
Growth inhibitors Cell cycle inhibitors
Programmed cell death genes DNA repair enzymes
Unlimited proliferationSustained angiogenesis
Tissue migration and metastasis
ACQUIRED PROPERTIES
Independent growth factor signalsResistance to growth inhibitory factors
Avoid apoptosis
Hanahan D és Weinberg RA 2000 Cell
Tumor stem cell
Tissue cell
Malignant cell
Malignant transformation

Normal epithelial cells2 APC mutation
Inherited
Adenomatous polip
1 Ras mutation
Adenomatous polip
2 p53 mutation
Colon carcinomaChromosomaltranslocation
Metastatic colon carcinoma
The „multi-hit” model of tumorigenesis
Knudson A.G. 2001
Reaction of the immune system
TOLERANCE
RECOGNITIONTumor antigens
Individual TSA
Common TAACEA
TOLERANCEIMMUNE
RESPONSE
DANGER
INNATE/AQUIRED IMMUNITY

Oncogenesis
Mechanism Action Example
Growth promotion
Overexpression of growth factor receptors (such as epidermal growth factor, or EGF) making cells more sensitive to growth stimuli
c-erb-B2
Increased growth factor signal transduction by an oncogene that lacks the GTPase activity that limits GTP induction of cytoplasmic kinases that drive cell growth
ras
Overexpression of a gene product by stimulation from an oncogene (such as ras) c-sis
Lack of normal gene regulation through translocation of a gene where it is controlled by surrounding genes to a place where it is no longer inhibited
c-abl
Binding of oncogene product to the nucleus with DNA transcriptional activation to promote entry into the cell cycle
c-myc
Loss of tumor suppressor gene function
Lack of regulation of cell adhesion with loss of growth control through cell interaction APC
Loss of down-regulation of growth promoting signal transduction NF-1
Loss of regulation of cell cycle activation through sequestation of transcriptional factors Rb
Loss of regulation of cell cycle activation through lack of inhibition of cell proliferation that allows DNA repair
p53
Limitation of Apoptosis
Overexpression of gene, activated by translocation, prevents apoptosis bcl-2

Oncogene Associated Neoplasms
c-erb-B2 Breast and ovarian carcinomas
ras Many carcinomas and leukemias
c-sis Gliomas
c-abl Chronic myelogenous leukemia, acute lymphocytic leukemia
c-myc Lymphomas
BRCA-1 Breast and ovarian carcinomas
APC Colonic adenocarcinomas
NF-1 Neurofibromas and neurofibrosarcomas
Rb Retinoblastomas, osteosarcomas, small cell lung carcinomas
p53 Many carcinomas
bcl-2 Chronic lymphocytic leukemia, lymphomas
VARIOUS ONCOGENES ARE ASSOCIATED WITH DEFINED NEOPLASMS

CHROMOSOMAL TRANSLOCATION IN BURKITT’S LYMPHOMA
Uncontrolled proliferation due to the activation of c-myc oncogene
EBV induced tumor
8 14 8q- 14q+
c-myc
CHVHc-myc
CHVH

MHC-dependent rejection of tumors

Infective facial tumor in the inbread populations of the Tasmanian devil
About 2/3 of HungaryPopulation half million

THE IMMUNE RESPONSE TO TUMORSHidden, changing, proliferating, evolving target
• Immune surveillence– Few non-self antigens– Poorly immunogenic– Recognized by B and T
lymphocytes
• Tolerance induction– Tumor antigens do exist– Recognized primarily by T
lymphocytes– Induce tolerance
TUMOR ANTIGENSTumor associated antigens – TA
Present also in normal cellsAberrant/disregulated expression in tumor cells
Tumor specific antigens – TSA Unique for individual tumors or tumor types
IMMUNE SYSTEM
Tumor-specific immune responses can be induced
Cytotoxic T lymphocytes can eradicate tumors

Tumor antigens and tumor associated antigens

Tumor-specific antigens

Cancer/testis antigens are expressed almost entirely by cancerous cells, showing little or no expression in healthy tissue, with the exception of normal testis, embryonic ovaries and placenta.
No MHC expressionMany of them X-linked Over 100 in total --- Potential targets for immune therapy

STRUCTURE AND SOURCE OF TUMOR ANTIGENS• MUTATED ONCOGENS AND TUMOR SUPPRESSOR GENES
– Involved in transformation– Cytosolic novel determinants - no major targets– Cellular proto-oncogenes oncogene Ras, p53, Abl
• Point mutation, deletion, chromosomal translocation, viral gene insertion• ABERRANTLY OVEREXPRESSED NORMAL CELLULAR PROTEINS
– Low/rare expression in normal cell – ignorance by the immune system• TUMOR ANTIGENS ENCODED BY GENOMES OF ONCOGENIC VIRUSES
– Immunogenic shared viral proteins • DNA viruses – • Simian virus 40, a polyomavirus that is found in both monkeys and humans. (Large
T-antigen, binds and inactivates p53)• Herpes, EBV- LMP protein strongly trasforming. Homologue of CD40• Papilloma HPV16 HPV18• RNA viruses – • Retroviruses HTLV
• ONCOFETAL ANTIGENS– Silenced during development de-repressed in tumor cells– Tumor markers – carcinoembryonic antigen CEA, specific for carcinomas– Alpha-fetoprotein AFP, hepatocellular carcinoma
• TISSUE-SPECIFIC DIFFERENTIATION ANTIGENS – CD10/CALLA Common Acute Lymphoid Leukemia Antigen, Melanoma

macrophage
DS
NK/γδ
CD4/CD8
PROTECTION
ELIMINATIONImmunsurveillence
EQUILIBRIUM ESCAPE
Genetic instabilityImmune selection
Treg cells
TUMORCD8
CD8
macrophage
DS
NK/γδ
CD4/CD8 METASTASIS
ESCAPING TUMOR VARIANTS

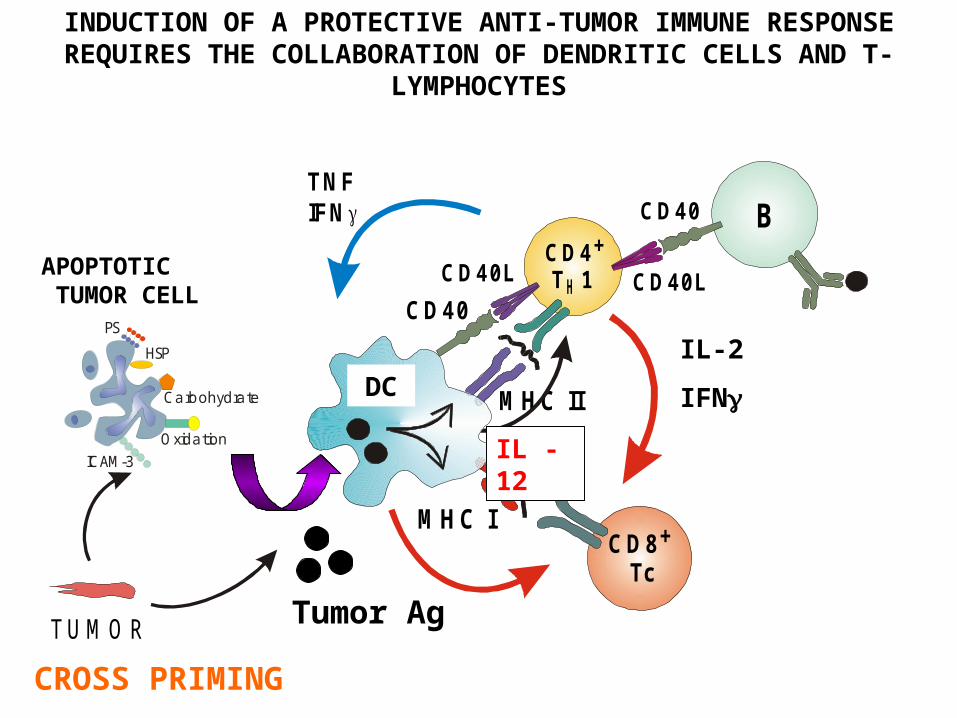
Activation of tumor-specific T-cells by DCCross-presentation
M HC II
CD8+
Tc
IL-12
CD4+
T 1H CD40LCD40L
CD40 B
INDUCTION OF A PROTECTIVE ANTI-TUMOR IMMUNE RESPONSE REQUIRES THE COLLABORATION OF DENDRITIC CELLS AND T-
LYMPHOCYTES
IL-2
IFN
Tumor Ag
CROSS PRIMING
TUMOR
APOPTOTIC TUMOR CELL
PS
OxidationICAM-3
HSP
Carbohydrate
TNFIFN
M HC I
APC
CD40
DC
IL - 12

• TUMOR ANTIGENS– Soluble tumor antigens – inhibit recognition on the cell surface– Antigen modulation – antibody dependent internalization– Masking – antibody binds, no effector function– Low immunogenicity – Peptide antigens – mutations affecting Tc or Th epitopes
• ANTIGEN PRESENTATION– Direct presentation – non professional APC, no MHC class II, no co-stimulatory
molecules– Indirect presentation – by professional APC, soluble CD40 and CD40 ligand inhibit
• CYTOTOXIC T CELL ACTIVITY– MHC – mutation, altered intracellular transport, β2m, locus, allele– Peptide loading – mutation, tumor derived peptides are not presented, TAP
• APOPTOSIS– Soluble Fas – inhibits Fas ligand-mediated apoptosis
• TUMOR DERIVED INHIBITORY FACTORS– TGFβ – G1 block, inhibits tumor growth if sensitive tumors loose their TGFβ
receptor– TGFβ inhibits immune cell activation– PGE2 – immune suppression
• TUMOR DERIVED POTENTIATING FACTORS– Angiogenesis factors – secreted by tumor tissue cells or by immune cells
ESCAPE MECHANISMS OF TUMOR CELLS AND TUMOR TISSUES

Manipulation of the immune response by a tumor.

C 4+
DCD40L
IDCDC2
CD8+
Tc
M
IL-10
CD4+CD25+
CD4+
reg
TOLERANCE INDUCTION BY DENDRITIC CELLS
SIGNAL 1 Tumor antigen YES
SIGNAL 2 Tumor cell NO
Activated APC YES
SIGNAL 3 Natural immunity NO
Inflammation NO
Tumor-associated macrophage (upto 40% of non-malignant cells)
M1 macrophage: MHCII, CD80, 86High iNOS,
M2 macrphage: arginase +

Many tumors loose expression of HLA class I proteinsLoss of HLA class I expression in prostate cancer.
Class I moleculed are stained brown. The stain and HLA class I molecules are not seen on the tumor mass but are restricted to lymphocytes
infiltrating the tumor and tissue stromal cells

Human epithelial tumours can inhibit the response of lymphocytes expressing NKG2D

Vaccination against human papilloma viruses can prevent cervical cancer
•HPV is an oncogenic virus causing genital warts•250000 women die of cervical cancer each year•Almost all cervical and ovarian cancers are HPV positive•Preventing chronic HPV infection should prevent cancer

Vaccination of melanoma patients may cause their tumor to regress
Rec. virus Synthetic peptide vaccine
It is not yet clear when the vaccine would work. Spectrum from remissionto no response

Blocking the inhibitory effects of CTLA4 with a human monoclonal antibody.
(Ipilimumab)
Blocking the PD1/PDL1 interaction with a human monoclonal antibody also works.
2 year survival is over 24% but quite some complications

T-cell responses to tumors can be improved with chimeric Antigen receptors (CARs)
• Low affinity of TCR (compared to virus spec. T cells)• MHC restriction prevents use in the entire population• problem solved by Fv• Variable fragment of the heavy and light chains of a Tumor-specific antibody mad a single chain• Fusion of FV to an intra cell. domain cont. CD28, CD137 and zeta-chain sequences • generates strong signal in the absence of costimulation

B cell tumors can be targeted by CARs specific to CD19

AZ AKTÍV TUMOR-SPECIFIKUS IMMUNTERÁPIA LEHETŐSÉGEIA tumor antigének beviteli módja
Tumor protein
Tumor protein-derived peptide Anti-idiotipe Ab
Vírus-tumor genome
Plasmid DNAModified tumor cell
Irradiated tumor cell
Heat shock protein
Modified DC
Mocellin S et al. Lancet Oncology 2004
Tumor cell lysateLoaded DC
ANTI-TUMOR IMMUNOTHERAPY

Humanized monoclonal antibodies used in the treatment of patients with cancer.

Cytotoxic T-lymphocytesrecognize tumor cells
Activated cytotoxic T-lymphocyteskill tumor cells
CONSEQUENCES OF T-CELL MEDIATED IMMUNITY