tumors of the lung carcinoma 90-95% carcinoid 5 % mesenchymal and others 2-5 %
TRANSCRIPT

Tumors of the lung
Carcinoma 90-95%
Carcinoid 5 %
Mesenchymal and others 2-5 %
Tumors of the lung
Etiology directly related to cigarette smoking
- Statistical evidence for positive relationship between tobacco
smoking and lung carcinoma.
- 87% lung cancers occur in active smokers
- Risk = Average smokers (x10), heavy smokers (>40/day) (x60)
- Passive smokers also have higher risk

Tumors of the lung
Etiology directly related to cigarette smoking
- Clinical evidence.
- Changes in bronchial epithelium in habitual smokers (metaplasia,
dysplasia, carcinoma in situ, squamous carcinoma)

Tumors of the lung
Etiology directly related to cigarette smoking
- Experimental evidence.

Lung carcinoma
- Other Environmental factors:
Radiation, air pollution (radon), asbestos
Lung carcinoma
Series of genetic abnormalities occurring in a step-wise manner,
triggered by a combination of genetic and environmental factors
Oncogenes associated with lung cancer
- cMYC, K-RAS, EGFR, HER-2/Neu
- p53, RB, p16

Initiators:polycyclic aromatic hydrocarbons
Promotors:phenol derivatives

WHO classification (epithelial tumors)
- Squamous
- Small cell
- Adeno (with variants)
- Large cell
- Adeno-squamous
- Ca with pleomorphic sarcomatous elements
- Carcinoid
- Salivary gland type
- Unclassified

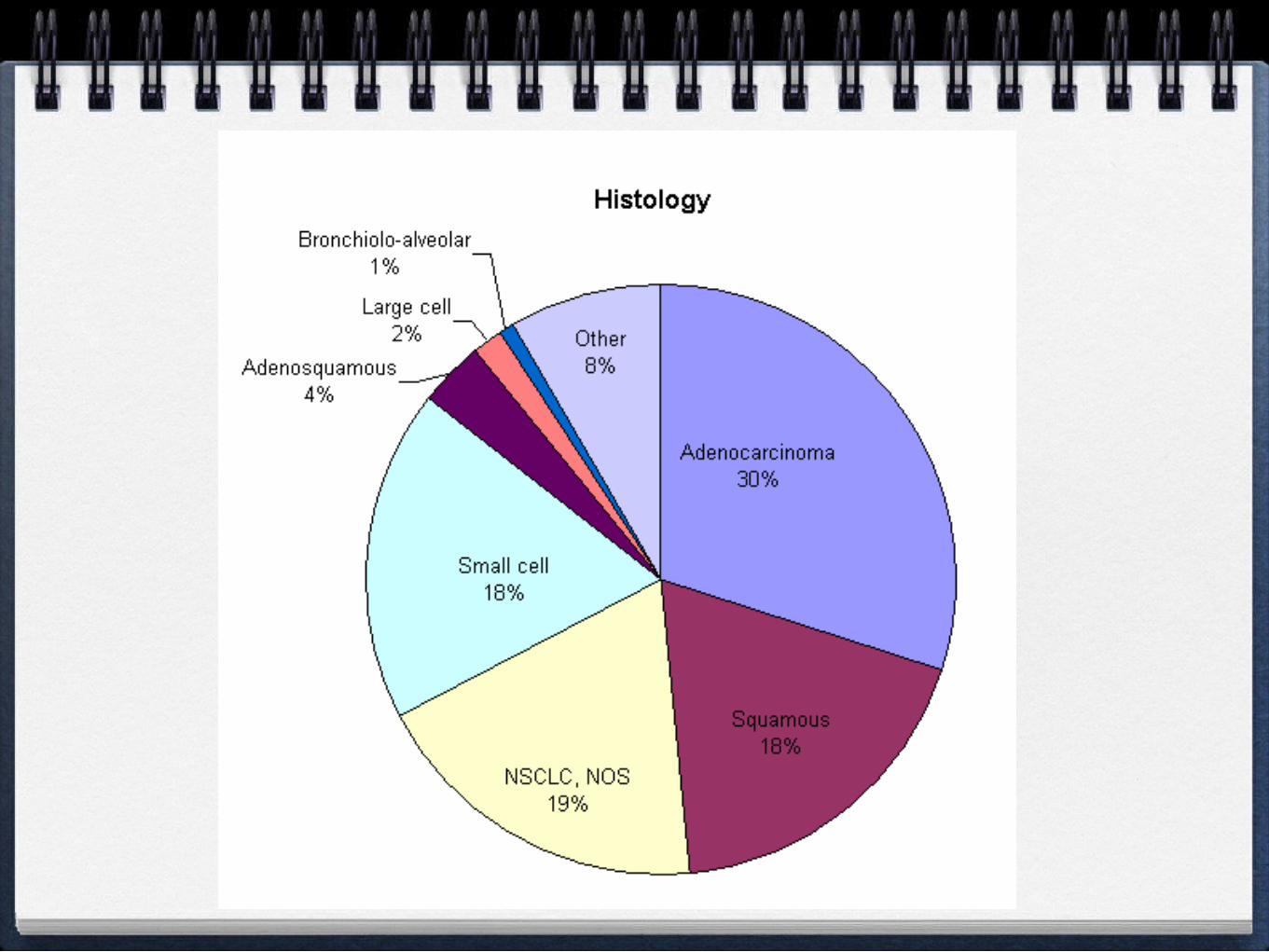
IncidenceSquamous 25-40%
Adeno 25-40%**
Small cell 20-25%
Large cell 10-15%
Practical aspect:
- Small cell Ca: metastasize, show high initial chemoresponsiveness
- Non-small cell ca: less metastases, less chemoresponsiveness
Cancers (except adeno) are centrally located
Increasing incidence of adenoca- Women smokers- Type of cigarettes
Increasing incidence of adenoca- Women smokers- Type of cigarettes
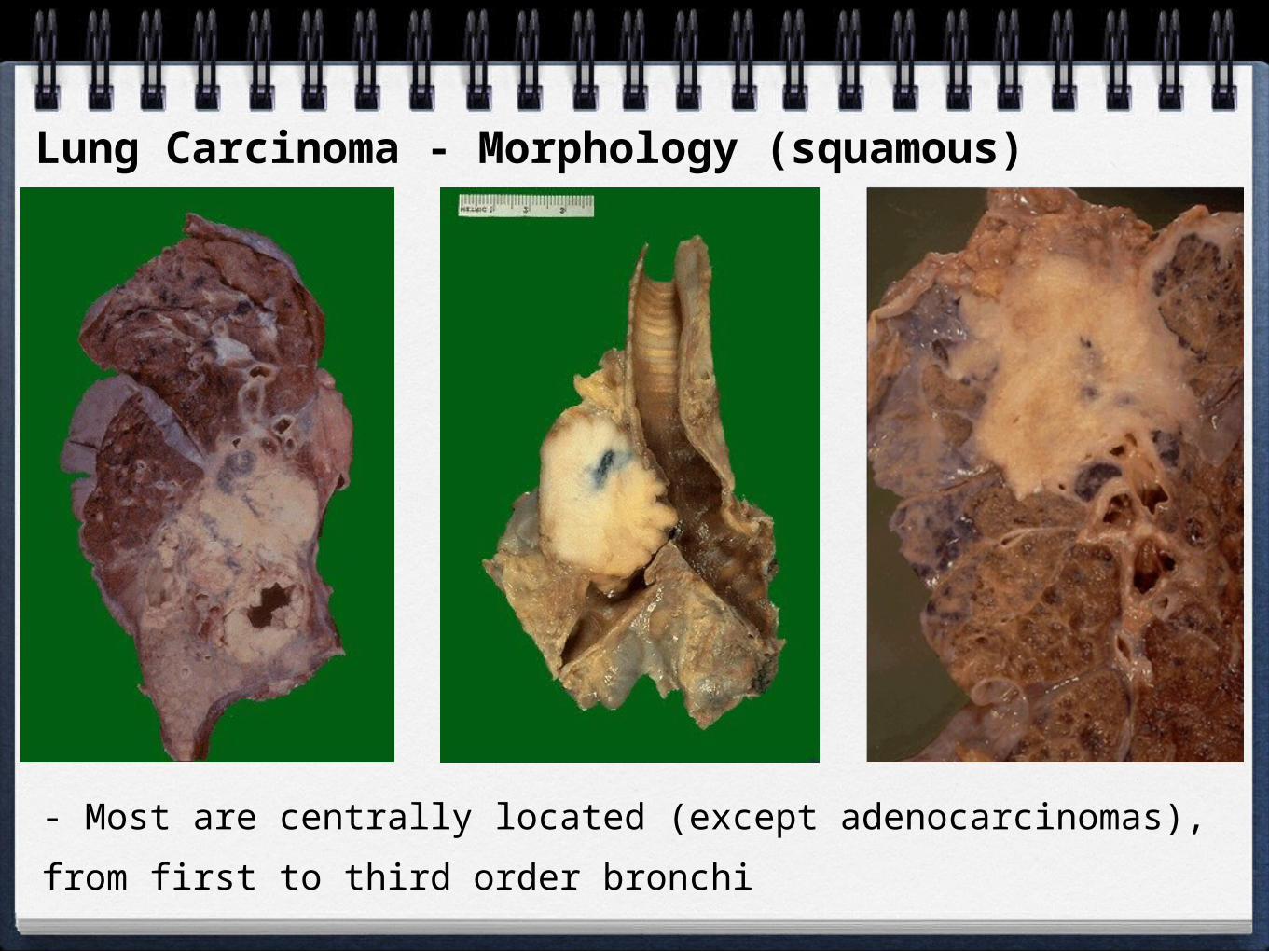
Lung Carcinoma - Morphology (squamous)
- Most are centrally located (except adenocarcinomas), from first to third
order bronchi

Squamous cell carcinoma:
- Close correlation with smoking history
- Begins as dysplasia - carcinoma in situ -
irregular warty growth with elevation and erosion
of bronchial mucosa
- fungates into the lumen
- penetrate bronchus and infiltrate along wall
- cauliflower like intraparenchymal mass
- extension to pleura
- spread to lymphnodes (>50% cases)
- distant spread
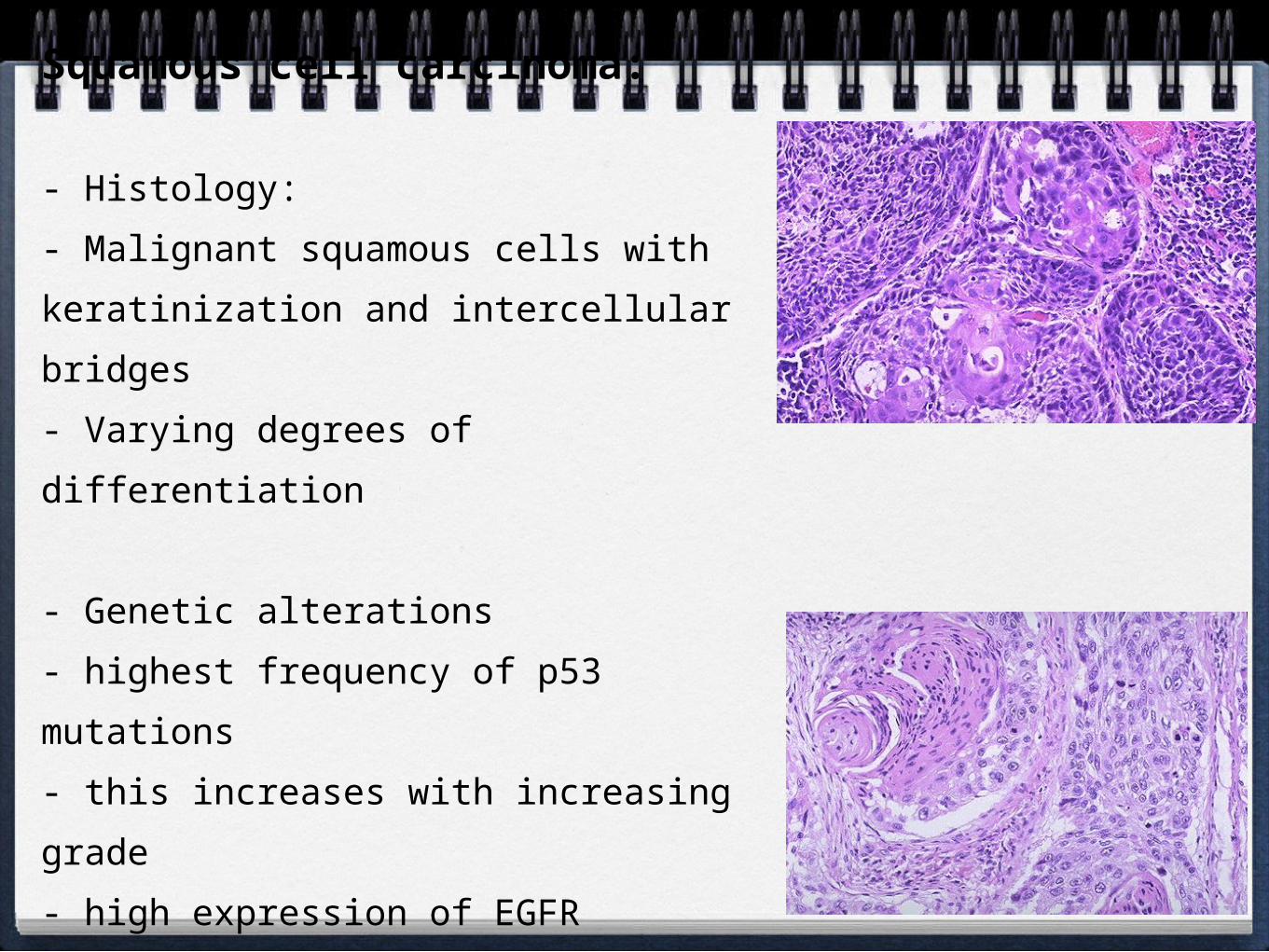
Squamous cell carcinoma:
- Histology:
- Malignant squamous cells with
keratinization and intercellular bridges
- Varying degrees of differentiation
- Genetic alterations
- highest frequency of p53 mutations
- this increases with increasing grade
- high expression of EGFR

Adenocarcinoma- Most common cancer in women and nonsmokers
- More peripherally located and smaller in size
- Often show mixed pattern (acinar, papillary, bronchiolo-alveolar, solid with mucin
- Grow more slowly when compared to squamous, but metastasize widely

Bronchioloalveolar carcinoma
- Almost always peripheral
- Usually appears as multiple nodules
with pneumonia like consolidation
- Nodules have mucoid feel
- Microscopic growth pattern is
characteristic and resembles butterflies
on a fence
- Mucinous and non mucinous subtypes
- Nonmucinous tumors are surgically
resectable

Bronchioloalveolar carcinoma

Small cell carcinoma
Central location
Whitish appearance
Small cells
Granular chromatin
High mitotic activity
Nuclear moulding
Dense core neuro-
secretory granules
Aggressive tumors, strong relationship to smoking

Staging of lung cancer:
TNM staging is used for staging cancer based on anatomic extent of tumor (T),
lymph node metastases (N), and distant hematogenous metastases (M).
Useful for comparing treatment results from different centers
Adenocarcinoma and squamous cell carcinoma tend to be localized for longer
periods.
Small cell carcinoma is particularly responsive to radiation and chemotherapy
Clinical Course
- Most insidious and aggressive neoplasm
- Cough, weight loss, hemoptysis, chest pain, dyspnoea
- Paraneoplastic syndromes due to hormone like substances
Small cell carcinoma - ADH, ACTH,
Squamous cell carcinoma - PTH,
Carcinoid tumors - Serotonin, Bradykinin
Others - Calcitonin, Gonadotropins,
Eaton-Lambert syndrome (Ca channel antibodies)
Peripheral neuropathies, clubbing

Clinical Course
Local tumor effects:
Pneumonia, abscess, collapse Airway obstruction
Lipid pneumonia Secondary to obstruction
Pleural effusion Tumor spread
Hoarseness RLN invasion
Dysphagia Esophageal invasion
Diaphragm paralysis Phrenic nerve invasion
Rib destruction Chest wall invasion
SVC syndrome SVC compression
Horner syndrome Symp ganglia invasion
Pericarditis / tamponade Pericardial invasion
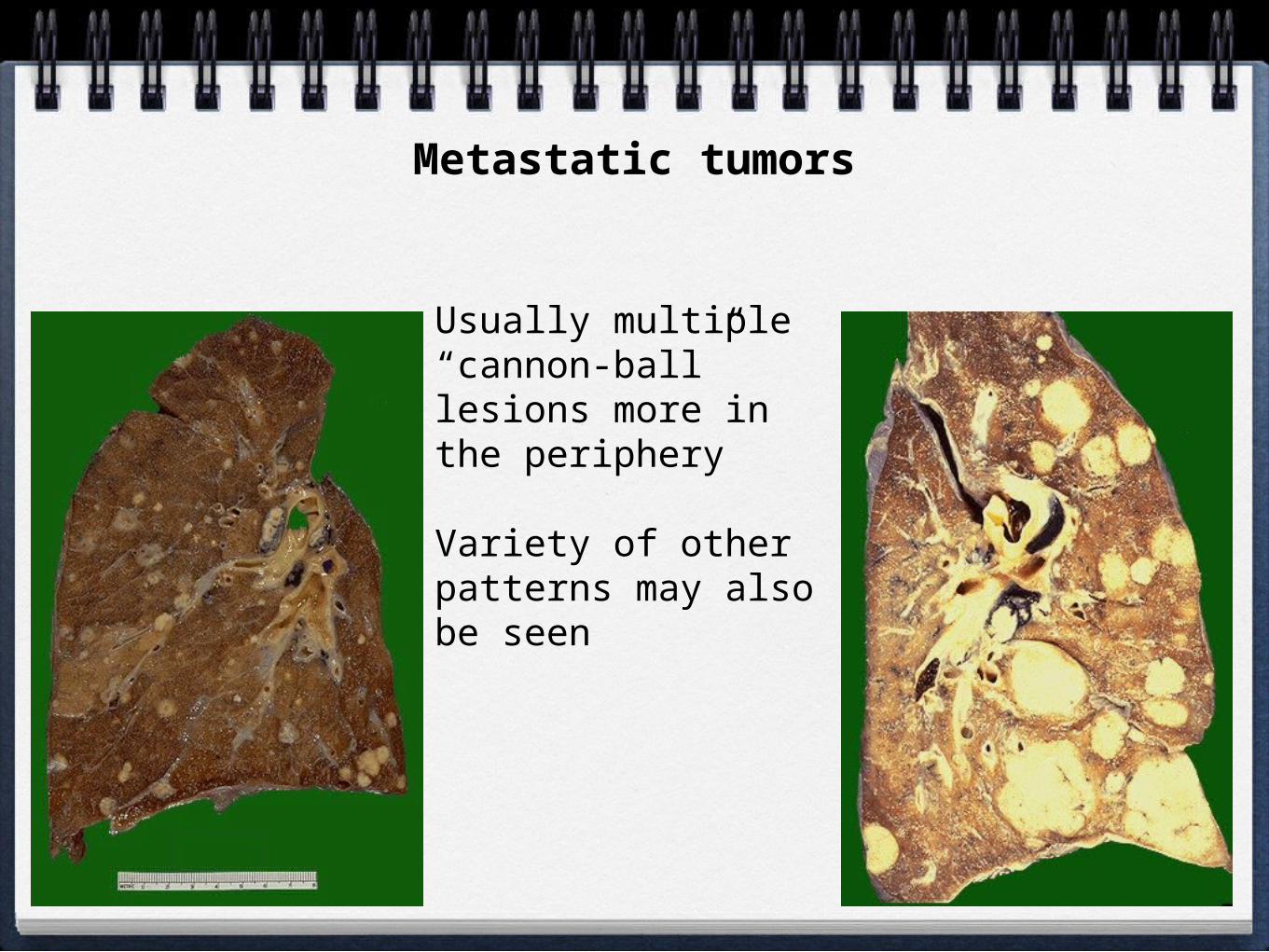
Metastatic tumors
Usually multiple “cannon-ball” lesions more in the periphery
Variety of other patterns may also be seen

Malignant mesothelioma:
- From parietal / visceral pleura
- Related to asbestos exposure
- Diffuse involvement of pleural space with
effusion and invasion of thoracic structures
- Microscopically, epithelioid and sarcomatoid
subtypes