type 1a diabetes immunology and polyglandular syndromes textbook on web with teaching slides
TRANSCRIPT

Type 1A DiabetesImmunology and Polyglandular
Syndromes
Textbook on web with Teaching Slides
www.barbaradaviscenter.org



Develop Insulin 1 and insulin 2 Knockouts with B16 alanine-insulin 2
Insulin 1-KO Insulin 2-KOB:16ala-tg
X X
Insulin 1 - B Chain : FVKQHLCGPHLVEALYLVCGERGFFYTPKS
Insulin 2 - B Chain : FVKQHLCGSHLVEALYLVCGERGFFYTPMS
Insulin 1 (-)
Insulin 2 (-)
B:16ala-insulin 2 (+)
Tyrosine (TAC)
Alanine (GCC)

Nakayama et al. Prime role for an insulin epitope in the development of type 1 diabetes in NOD mice. Nature 435:220, 2005

“Stages” in Development of Type1 Diabetes
Age (years)
Genetic Predisposition
Bet
a ce
ll m
ass
(?Precipitating Event)
Overtimmunologicabnormalities
Normal insulinrelease
Progressiveloss insulinrelease
Glucosenormal
Overtdiabetes
C-peptidepresent
NoC-peptide

Stage I: Genetics• Polygenic-common
HLA DR+DQ+ other MHCInsulin gene PTPN22-lyp?CTLA-4
• “Monogenic”-rare
APS-I: AIRE mutation
IPEX syndrome: FoxP3 mutation

The Major Histocompatibility ComplexHLA: Human Leukocyte Antigens
0 base pairs 1 million
1 million 4 million
DPB1DPA1
LMP2TAP1
LMP7
TAP2DQB1
DQA1DRB1
DRA
CYP 21B C4A HSP70
TNFB C E A
MICA
Class I Region
MHC Class II Region
Class III Region

Human Leukocyte Antigen
human MHC
cell-surface proteins
important in self vs. nonself distinction
present peptide antigens to T cells
CLASS I: A,B,C CLASS II: DR,DQ,DP
HLAJ. Noble

TERMINOLOGY
DRB1*02
DQB1*0302DRB1*0401
DRB1*0401
DRB1*0301
DQB1*0302
DRB1*0401
DQB1*02
Allele:
Haplotype:
Genotype
J. Noble

Autoimmune Polyendocrine Syndromes
• APS-II (Autoimmune Polyendocrine)• APS-I (AIRE mutation) • IPEX (XPID): (Scurfy Mutation) • Anti-insulin Receptor Abs + “Lupus”• Hirata (Anti-insulin Autoantibodies)• POEMS (Plasmacytoma,..)• Thymic Tumors + Autoimmunity• Congenital Rubella + DM +Thyroid

IPEX: Immunodysregulation, Polyendocrinopathy, Enteropathy, X-linked
• Other Names XPID: X-linked polyendocrinopathy, immune dysfunction and diarrhea
XLAAD: X-Linked Autoimmunity Allergic Dysregulation
• Foxp3 Gene Mutation
• Loss of Regulatory T Lymphocytes
• Bone Marrow Transplant with Chimera “Cures”
BDC

APS-I• Autoimmune Polyendocrine Syndrome
Type 1• Autosomal Recessive mutations AIRE
(Autoimmune Regulator) gene• Mucocutaneous Candidiasis/Addison’s
Disease/Hypoparathyroidism• 18% Type 1 Diabetes• “Transcription Factor” in Thymus
BDC

TCR
MHC + Peptide
Autoreactive thymocyte
Self-peptides from "peripheral"
antigens
Tolerization of autoreactive thymocyte
MODEL AIRE Role in Preventing Autoimmunity
Thymic MedullaryEpithelial Cells
AIRE
Mathis/Benoist

Comparison APS-I and APS-II APS-I APS-II
• Onset Infancy• Siblings
AIRE gene mutated• Not HLA Associated• Immunodeficiency
AsplenismMucocutaneous Candidiasis
• 18% Type 1 DM
• Older Onset• Multiple Generations• DR3/4 Associated• No Defined
Immunodeficiency• 20% Type 1 DM
BDC

A family of diseases occurring in families
Type 1A Diabetes
Celiac Disease
Addison’s Disease
Thyroid AutoimmunityBDC
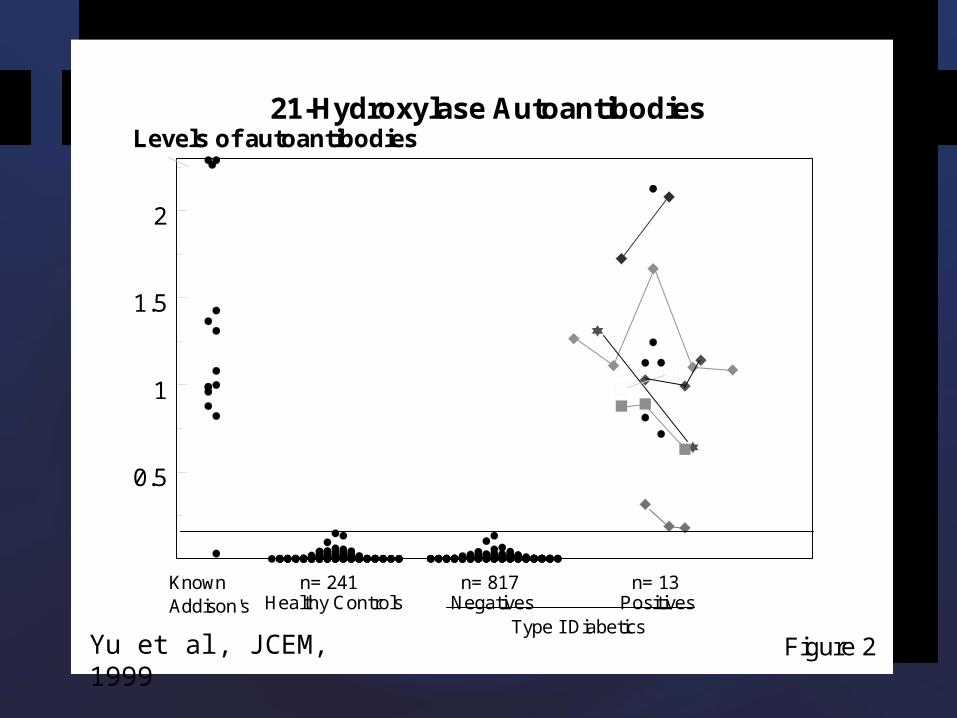
21-Hydroxylase Autoantibodies
0.5
1
1.5
2
Levels of autoantibodies
Healthy Controls Negatives PositivesType I Diabetics
n= 241 n= 817 n= 13
Figure 2
KnownAddison's
Yu et al, JCEM, 1999

Prevalence of TGA by HLA-DR amongst patients with type 1 DM, relatives of DM patients and
general population
0%
5%
10%
15%
20%
25%
DR3+ DR3-
IDDMRelativesPopulation
Prevalence
HLA-DR
BDC

Transglutaminase Autoantibodies and Marsh score (Disease Severity)
0.0
.5
1.0
1.5
2.0
2.5
tTG titer
0 1 2 3Marsh score
Spearman correlation, r = 0.569 p < 0.003
Hoffenberg, J. Peds 137:356 2000

Stage II: Precipitating Event

Diabetes Autoimmunity Study in the YoungSibling/offspring cohortGeneral population cohort
enrolled = 293 high risk 72
429 moderate risk 220
347 average - low risk 401
1,069 All 693
relatives 1,491 1,007
screened = 21,713

Stage III: Autoimmunity

Cytoplasmic ICA kindly provided by the discoverer Franco Bottazzo

Major Autoantibody Targets
• GAD65 (glutamic acid decarboxylase)
• IA-2 (ICA512): Insulinoma Associated Protein
• Insulin

Insulin Autoantibodies
• Usually the first autoantibody to appear• Highest levels in youngest children
developing type 1A diabetes• Mature high-affinity immune responses to
(pro)insulin anticipate the autoimmune cascade that leads to type 1 diabetes. Achenbach et al, J.Clin Invest 2004, 114:589

Stage IV: Progressive Loss Function
Stage V: Overt Diabetes

3
4
5
6
7
0 2 4 6 8 10 12 14
Hb
A1
c (%
)
3
4
5
6
7
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
Hb
A1
c (%
)
3
4
5
6
7
8
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
Hb
A1
c (%
)
3
4
5
6
7
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
Age (years)
Hb
A1
c (%
)
3
4
5
6
7
0 2 4 6 8 10 12 14
3
4
5
6
7
0 2 4 6 8 10 12 14
Age (years)
3
4
5
6
7
0 2 4 6 8 10 12 14
Age (years)
3
4
5
6
7
0 2 4 6 8 10 12 14
Age (years)
Hb
A1
c (%
)
3
4
5
6
7
0 2 4 6 8 10 12 14
A

Blood glucose values inControl vs. Daisy children
DAISY Control-FH Control no FH0
200
400
600
800
1000
1200
1400
Blo
od
glu
cose
, m
d/d
L
Barker et al, Diabetes Care 27: 1399, 2004

We can predict Type 1 diabetes.
We can prevent the disorder in animal models.
We cannot yet safely prevent in man.

NEXT
1. Improved T Cell Assays
2. Trials of antigen-specific therapies prior to autoantibodies.
3. Immunomodulator/Immunosuppressive Trials post-onset and with islet transplantation.
TRIALNET1-800-HALT-DM1
• Dalizumab+ MMF – New Onset Trial
• Oral Insulin Trial – Post Autoantibodies – Relative Screening
• With ITN: Anti-CD3 Trial Multiple course
• JDRF: Oral Insulin Prior to Anti-islet Autoantibodies being planned

Diabetes Autoimmunity Study in the Young (DAISY)
Also: Lars Stene, Patricia Graves, Heather Stanley, Jaime Keen, Peter Chase Carolyn Fronczak, Jennifer Barker, Akane Ide, Andrea Steck