types of carcinogens clinical aspects of neoplasia paraneoplastic syndromes grading & staging
TRANSCRIPT

Types of Carcinogens
Clinical aspects of neoplasia
Paraneoplastic syndromes
Grading & staging

Carcinogens cause genetic damage and induce neoplastic transformation of cells
1. Chemical carcinogens
2. Radiant energy
3. Microbial – virus, bacteria, parasites
Parasites include • Schistosoma hematobium (Squamous cell carcinoma of the urinary bladder) • Clonorchis sinensis, Opisthorchis viverrini (Cholangiocarcinoma of the bile ducts)

Chemical carcinogenesisINITIATION - permanent DNA damage (mutations)
PROMOTION - can induce tumors in initiated cells, but cannot cause tumors on their own
Direct acting and indirect acting
Tobacco is the agent most responsible for cancer/cancer deaths in the United States.

DIRECT - ACTINGAlkylating Agentsβ-Propiolactone, Dimethyl sulfate, Diepoxybutane, Anticancer drugs (cyclophosphamide, chlorambucil, nitrosoureas, etc.)Acylating Agents1-Acetyl-imidazole, Dimethylcarbamyl chloride
PROCARCINOGENS (REQUIRE ACTIVATION)Polycyclic and Heterocyclic Aromatic HydrocarbonsBenz(a)anthracene, Benzo(a)pyrene (Cigarette Smoke), Dibenz(a,h)anthracene, Methylcholanthrene, 7,12-Dimethylbenz(a)anthracene
Aromatic Amines, Amides, Azo Dyes2-Naphthylamine (β-naphthylamine), Benzedrine, 2-Acetylaminofluorene, Dimethylaminoazobenzene (butter yellow)
Natural Plant and Microbial ProductsAflatoxin B1 , Griseofulvin Cycasin, Safrole, Betel Nuts
OthersNitrosamine and amidesVinyl chloride, nickel, chromiumInsecticides, fungicides, Polychlorinated biphenyls
Carcinogens

Initiation and promotion
Experiments demonstrating the initiation and promotion phases of carcinogenesis in mice.

Events in chemical carcinogenesis

Tumor Progression
RADIATION CARCINOGENESIS
UV light - skin cancers (SCC, BCC, Melanomas)
UV-B, pyrimidine dimers
• X-ray pioneers: skin cancers• Miners of radioactive elements: lung cancers • Atom Bomb survivors: initially leukemias (AML/CML), later
on - solid tumors • Thorotrast (radioactive dye in radiology) - liver sarcoma
Most frequent - acute and chronic myeloid leukemia followed by cancer of the thyroid in the young

MICROBIAL CARCINOGENESIS
RNA virusHuman T-Cell Leukemia Virus Type 1 (HTLV-1): causes T-cell leukemia/lymphoma, endemic in parts of Japan and Caribbean, sporadic elsewhere
‘Tax’ gene product • Stimulates transcription of viral mRNA for its
replication • Activates transcription of genes involved in
proliferation and differentiation of T cells• Inactivates p16/INK4a• Enhances cyclin D activity• Activates NF-κb, a transcription factor • Interferes with DNA-repair functions, inhibits
ATM-mediated cell cycle checkpoints

Oncogenic DNA VirusesHPV, EBV, HBV, KSHV(HHV8)
Human Papillomavirus• Types 1, 2, 4, and 7 (low risk) : benign squamous papillomas (warts)• Types16 and 18 (high risk) : Squamous Cell carcinoma of cervix /
anogenital region
• Two viral genes, E6 and E7• E6 mediates degradation of p53 and BAX• E7 protein binds to the RB protein and displaces the E2F transcription
factors, inactivates CDKIs p21 and p27, activate cyclins E and A
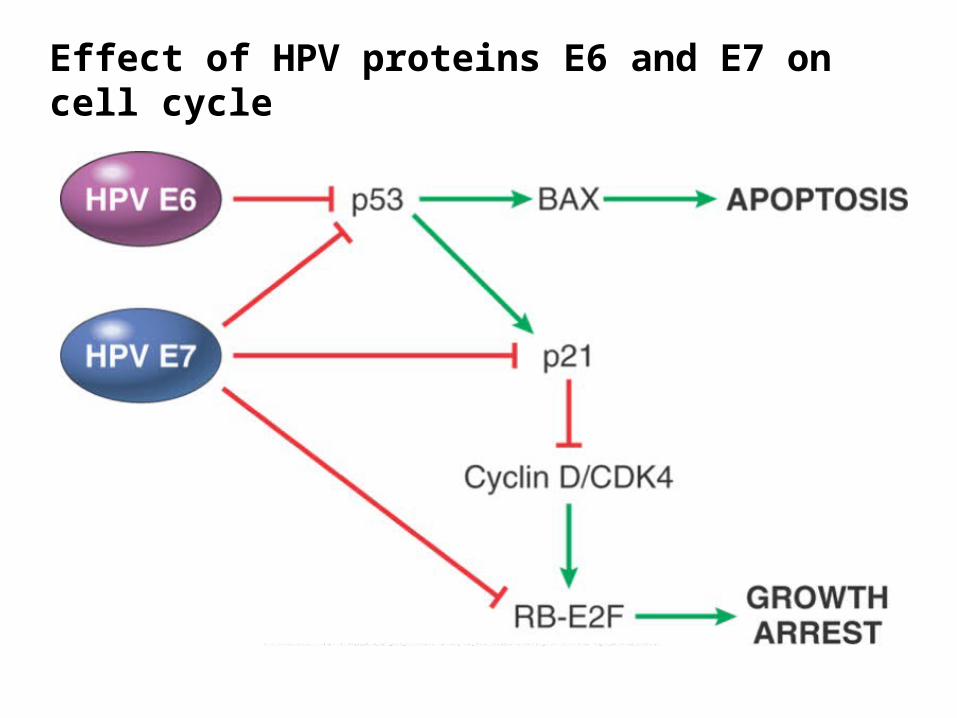
Effect of HPV proteins E6 and E7 on cell cycle
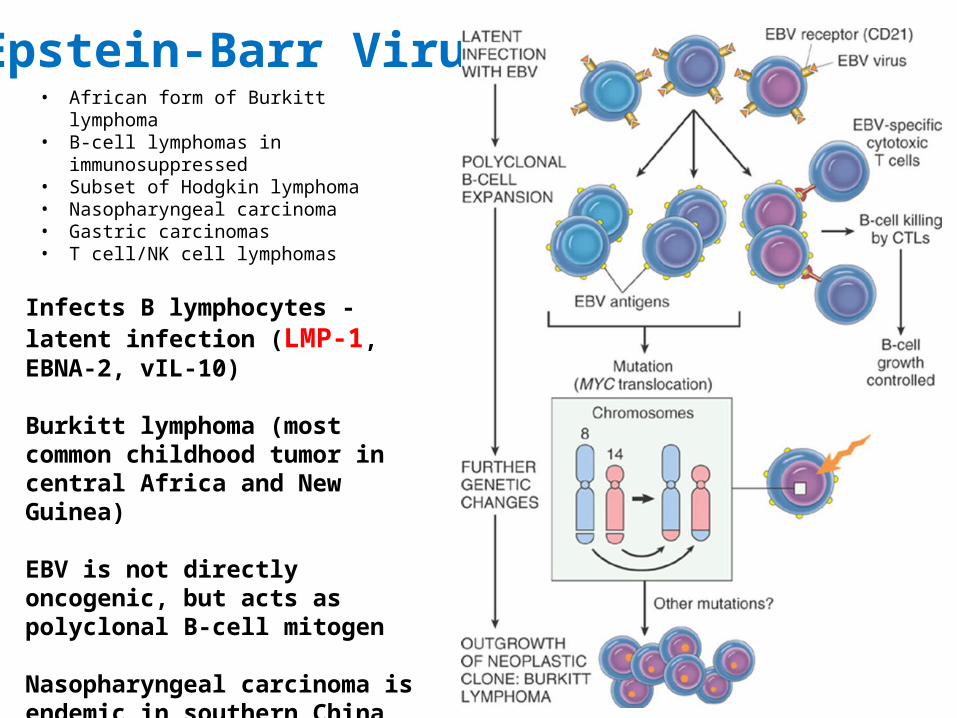
Epstein-Barr Virus• African form of Burkitt lymphoma• B-cell lymphomas in immunosuppressed • Subset of Hodgkin lymphoma• Nasopharyngeal carcinoma• Gastric carcinomas• T cell/NK cell lymphomas
Infects B lymphocytes - latent infection (LMP-1, EBNA-2, vIL-10)
Burkitt lymphoma (most common childhood tumor in central Africa and New Guinea)
EBV is not directly oncogenic, but acts as polyclonal B-cell mitogen
Nasopharyngeal carcinoma is endemic in southern China


Hepatitis B and C Viruses
70 - 85% of hepatocellular carcinomas worldwide are due to infection with HBV or HCV
Maladaptive Immune response promotes tumorigenesis
HBV – Activates NF-κB pathway, HBx gene, viral integration
HCV - Chronic inflammation, HCV core protein

Helicobacter pyloriFirst bacterium classified as a carcinogen
Gastric Adenocarcinoma - increased epithelial cell proliferation in a background of chronic inflammation (cytotoxin-associated gene A - CagA)
Gastric ‘MALT’ lymphoma - infection leads to H. pylori-reactive T cells, which stimulate a polyclonal B-cell proliferation (NF-κB)
Antibiotic therapy can cure lymphoma

HHV-8 causes Kaposi's sarcoma in AIDS(acts via cytokines released from HIV and HSV)
Human Herpes Virus -8

Mechanisms by which tumors evade the immune system

Clinical Aspects of Neoplasia
(1) Location and impingement on adjacent structures
(2) Functional: hormone synthesis / paraneoplastic syndromes
(3) Bleeding and infections when the tumor ulcerates
(4) Fever
(5) Symptoms from rupture or infarction
(6) Cachexia (TNF, Proteolysis-inducing factor, Lipid-mobilizing factor)

Hormone production• Pituitary tumors
– Prolactinoma: prolactin amenorrhea, infertility and galactorrhea
– Somatotropic adenoma Growth hormone gigantism in children and acromegaly in adults
• Adrenal adenoma– Cortisol Cushing’s syndrome– Mineralocorticoids Conn’s syndrome– Sex hormone Adrenogenital syndrome
• Ovarian tumors:– Granulosa theca cell tumor hyperestrinism– Sertoli – leydig cell tumor excess androgen-
Hirsuitism • Trophoblastic tissue
– Hydatidiform mole and choriocarcinoma beta hCGAmmenorrhea & vomiting

Hematological associations with cancer
• Anemia of chronic disease: – Most common type
• Iron deficiency anemia : – right sided colorectal Cancer
• Macrocytic anemia: – due to folate deficiency from rapid
tumor growth– As in Leukemia and lymphomas
• Autoimmune hemolytic anemia: Jaundice, anemia,free Hb in urine– Chronic lymphocytic leukemia

Bone marrow metastasis
• Myelophthisic anemia:– Anemia related to metastasis to bone
marrow• Leukoerythroblastic blood picture:
– Metastasis to bone marrow pushes immature hematopoietic cells ( e.g. nucleated RBC, myeloblasts) into the peripheral blood

Paraneoplastic Syndromes
• 10% of cancers
• earliest manifestation of hidden tumor
• significant clinical issues / lethal
• mimic metastasis, complicate treatment

Clinical Underlying Cancer Mechanism
ENDOCRINOPATHIESCushing syndrome
Small-cell carcinoma of lungPancreatic ca, Neural tumors
ACTH or ACTH-like substance
SIADH Small-cell carcinoma of lung;
intracranial neoplasmsADH or atrial natriuretic
hormonesHypercalcemia
Squamous cell carcinoma of lungBreast carcinoma, Renal carcinoma
Adult T-cell leukemia/lymphoma
PTH related protein (PTHRP),
TGF-α, TNF, IL-1
Hypoglycemia
Ovarian carcinoma, FibrosarcomaOther mesenchymal sarcomas
Insulin or insulin-like substance
Carcinoid syndrome Hepatocellular carcinoma, Bronchial adenoma, Pancreatic Ca
Serotonin, Bradykinin
Polycythemia
Gastric carcinomaRenal carcinoma
Cerebellar hemangioma, Hepatocellular carcinoma
Erythropoietin
Paraneoplastic Syndromes

Clinical Underlying Cancer Mechanism
NERVE AND MUSCLE SYNDROMESMyasthenia Bronchogenic carcinoma Immunological
Disorders of CNS/PNS Breast carcinoma
DERMATOLOGIC DISORDERSAcanthosis nigricans Gastric carcinoma, lung,
uterine carcinomaImmunological;
secretion of EGFDermatomyositis Lung, breast carcinoma Immunological
OSSEO-ARTICULARHypertrophic osteoarthropathy
and clubbing of the fingersBronchogenic carcinoma Unknown
VASCULAR AND HEMATOLOGICVenous thrombosis (Trousseau phenomenon)
Pancreatic carcinomaLung carcinoma. others
Tumor products (mucins activate
clotting)
Nonbacterial thrombotic endocarditis Advanced cancers Hypercoagulability
Red cell aplasia Thymic neoplasms Unknown
OTHERSNephrotic syndrome Various cancers Tumor antigens, immune
complexes
Paraneoplastic Syndromes

HypercalcemiaMost common paraneoplastic syndrome
PTH related peptide
Squamous cell bronchogenic carcinomacarcinomas of the breast, lung, kidney, and ovary
IL-1, TGF-α, TNF, and dihydroxyvitamin D
Investigations may show low PTH, high calcium, high PTHrP with normal/low levels of 1,25-dihydroxyvitamin D
Hypercalcemia due to skeletal metastases as in breast cancer is not a paraneoplastic syndrome

Hypertrophic osteoarthropathy 1% to 10% of patients with bronchogenic carcinomas.
• periosteal new bone formation, primarily at the distal ends of long bones, metatarsals, metacarpals, and proximal phalanges;
• arthritis of the adjacent joints; and • clubbing of the digits.

GRADING AND STAGING OF TUMORS
Grading - based on degree of differentiation of tumor cells
(in some cancers on number of mitoses or architectural features)
Staging - based on size of primary lesion, extent of spread to regional lymph nodes, and presence or absence of blood-borne metastases
- TNM system (American Joint Committee on Cancer Staging)
T:primary tumor, N:lymph node involvement, M:metastases
With increasing size, the primary lesion is characterized as T1 to T4
(T0 - in situ lesion)
N0 - no nodal involvement, N1 to N3 - increasing number of nodes
M0 - no distant metastases, M1 indicates metastases

35 year old woman with breast lump in left upper outer quadrant. It is 7x5cms with irregular margins, and puckering of the overlying skin with retraction of nipple. Nodes are palpable in the right axilla and CT abdomen shows multiple hypoechoic nodules in liver. Microscopy of tumor is provided. • What is your diagnosis? • Grade? stage? • Would you suggest surgical resection of the breast lump? • Will Herceptin be useful?
T0 N0 MO
T2 N1 M0
T4 N1 M1

Which of the following genes may be involved in this lesion?TaxE6E7LMP-1HbxCagA

Lung biopsies from two chronic smokers - immunohistochemical staining of the tumor cells is positive for different substances which would also explain different associated clinical manifestations. One of them had presented with neurologic dysfunction, muscle weakness, nausea , vomiting and polyuria. Which patient and what is the IHC likely to be positive for ? What could the other patient have presented with if there were no respiratory symptoms?A Parathormone related peptideB ErythropoietinC ACTHD ADHE Insulin like substance
A B

Required reading: Robbins Basic Pathology 9E, p198-207
Recommended reading: Robbins and Cotran Pathologic Basis of Disease 8E, p309-322