typhoid fever
TRANSCRIPT

Pableo, Rachel M.
CASE PRESENTATION

• JS• 6 years old• female• December 1, 2004• Filipino• Roman Catholic• Baggao, Cagayan• 1st time admission• June 16, 2011
General Data

Chief complaint
FEVER
History of Present Illness
9 days PTA- fever(-) other s/sx noted(-) consultation(-) medication taken

History of Present Illness
• 7 days PTA Still with fever(+) cough and colds(-)other s/sx
Consult a PMDDx : PneumoniaTx: Co-amoxiclav (?) mkD Paracetamol (?) mkdno relief
History of Present Illness
• 1 day PTA Still w/ above signs and symptoms
(+) vomiting(+) decrease feeding(+) abdominal pain(+) LBM(-) DOB(-) Consultation and
medications

History of Present Illness
• Few hours PTA persistence of fever
CVMC- Admission

Birth History
• Born to a 24 year old G2P2 (2002) mother • Midwife• NSD• Home• Umbilical cord cut by sterile scissors• Birth weight unrecalled• Vitamin K given
Prenatal History
• (+) PNCU• (+) MVS and FeSo4• No exposure to radiation, teratogenic drugs
and infectious diseases
Neonatal History
• Good suck and good cry• No jaundice• No cyanosis• No respiratory problem• No sepsis• No congenital defect noted

Nutritional history
• Breastfed since birth up to 2 years• Bottlefed with Bona (1:2)• Complementary started at 6 months• Table food introduced at 8 months• Present diet consist of fish, meat and
vegetables
Growth and development
• Smiles at 2 months• Can follow objects at 4
months• Sits with support at 6
months• Sits well at 9 months• Walks well alone at 15
months
• Runs well at 2 years• Knows sex and full
name by 3 years• Recognizes 2 or more
colors at 4 years• Grade I, average
student

Immunization History
• 1 dose BCG• 3 doses DPT• 3 doses OPV• 3 doses Hepa B vaccine• 1 dose measles vaccine• No booster dose given
Personal and Social History
• Eldest in a brood of 2• Father – 31 year old tricycle driver• Mother -29 year old plain housewife• Non-concrete house with 1 room shared by 4
members• Source of drinking water is from a pump well
(not boiled)

Past Medical History
• no known infant illness• No allergy• No history of previous hospitalization

Family History
• Maternal : (-) HPN, (-) DM, (-) bronchial asthma, (-) heart disease
• Paternal : (-) HPN, (-) DM, (-) bronchial asthma, (-) heart disease

Review of system
• No pruritus• No seizure• No headache• No difficulty of
breathing• No chest pain• No abdominal
distention
• No epistaxis• No nose/gum bleeding• No easy bruisability• No myalgia• No arhtralgia

Physical examination
• General survey:Awakeweak-lookingnot in cardiorespiratory distress
Physical examination
• Vital Signs:BP: 90/60CR: 112 bpmRR: 24 cpmTemp: 38.5Weight: 18 kgHeight: 112 cm

Physical examination
• Skin: no pallor no jaundiceno cyanosiswarm to touchgood skin turgor
Physical examination
• HEENT: anicteric sclerapink palpebral conjunctivano alar flaringdry lips and mucosano Tonsillopharygitisno Neck vein engorgement

Physical examination
• Chest and lungs: Symmetrical chest expansionno retraction(+) rales(+) airway entry

Physical examination
• Heart: Adynamic precordiumPMI at 5th ICS LMCLNormal rate regular rhythmno murmur

Physical examination
• Abdomen:flatNormoactive bowel soundsoftnon-tenderno organomegaly
Physical examination
• GUT: Grossly femaleno massno bleeding
Physical examination
• Extremities: No gross deformitiesno edemaCRT 1-2 secsfull and equal pulse

Neurologic Exam
• MSE: Awake, concious and coherentCranial nerves:• CN I: able to smell• CN II: pupils equally reactive to light and
accommodation size 2-3 mm• CNIII, CN IV, CNVI: able to follow objects
without deviation• CNV: (+) corneal reflex

• CN VII: no facial asymmetry• CN VIII: able to hear• CN IX, X: (+) gag reflex• CNXI: good shoulder shrug• CNXII: no tongue deviation

Neurologic Exam
• Motor: able to move extremities in different directions (grade: 5/5)
• Sensory: withdraws to pain 100%• DTRs: (+2) biceps reflex, (+2) Achilles tendon
reflex, (+2) patellar reflex• Reflex: (-) babinsky reflex, (-) kernig’s sign, (-)
Brudzinsky

Salient Features
• 6 y.o• Female• fever• cough and colds• Abdominal pain• Decreased feeding• LBM
T/C TYPHOID FEVER VS MALARIAADMITTING IMPRESSION
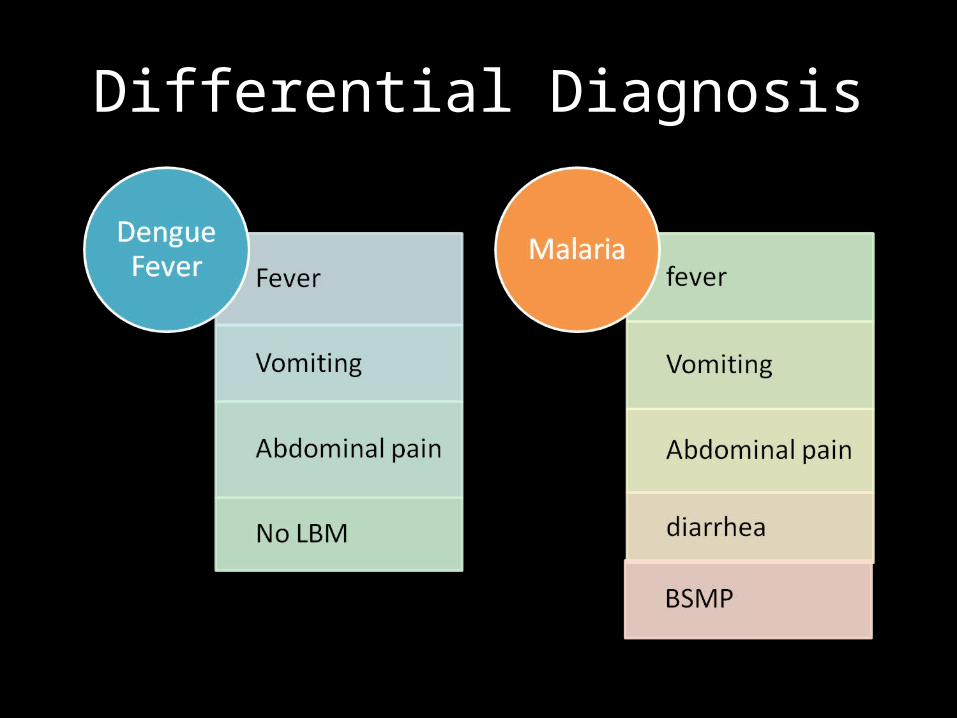
Differential Diagnosis

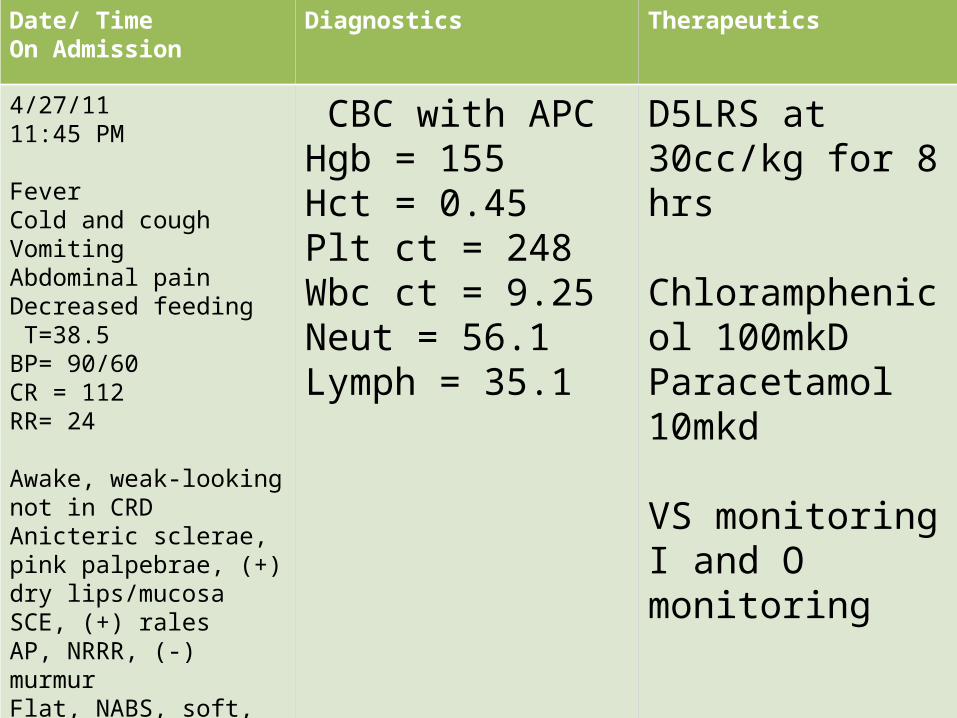
Date/ TimeOn Admission
Diagnostics Therapeutics
4/27/1111:45 PM
FeverCold and coughVomitingAbdominal painDecreased feeding T=38.5BP= 90/60CR = 112RR= 24
Awake, weak-looking not in CRDAnicteric sclerae, pink palpebrae, (+) dry lips/mucosaSCE, (+) ralesAP, NRRR, (-) murmurFlat, NABS, soft, nontenderFull and equal pulse
CBC with APCHgb = 155Hct = 0.45Plt ct = 248Wbc ct = 9.25Neut = 56.1Lymph = 35.1
D5LRS at 30cc/kg for 8 hrs
Chloramphenicol 100mkDParacetamol 10mkd
VS monitoringI and O monitoring
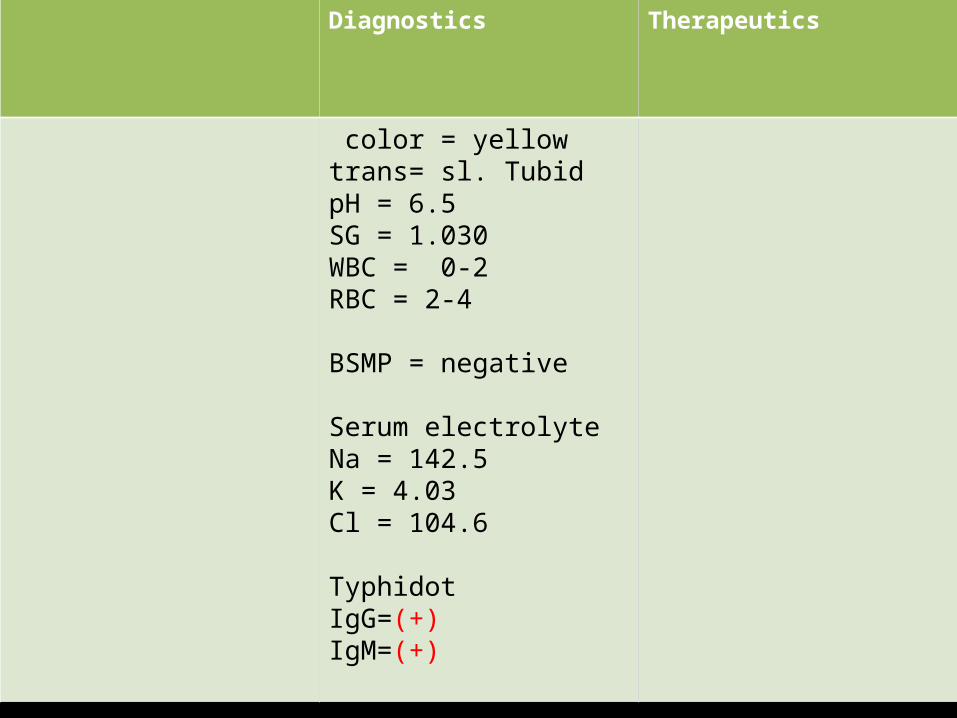
Diagnostics Therapeutics
color = yellow trans= sl. TubidpH = 6.5 SG = 1.030WBC = 0-2RBC = 2-4
BSMP = negative
Serum electrolyteNa = 142.5K = 4.03Cl = 104.6
TyphidotIgG=(+)IgM=(+)
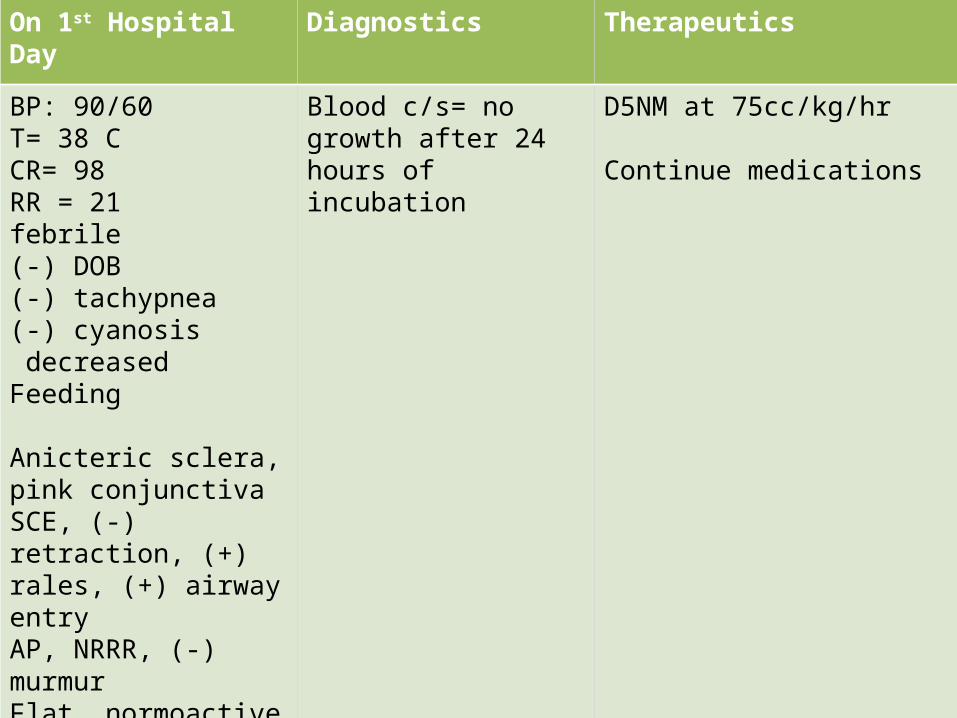
On 1st Hospital Day Diagnostics Therapeutics
BP: 90/60T= 38 CCR= 98RR = 21febrile(-) DOB(-) tachypnea(-) cyanosis decreased Feeding
Anicteric sclera, pink conjunctivaSCE, (-) retraction, (+) rales, (+) airway entryAP, NRRR, (-) murmurFlat, normoactive bowel sound, soft, non tender, (-) organomegalyCRT 1-2sec, full equal pulse
Blood c/s= no growth after 24 hours of incubation
D5NM at 75cc/kg/hr
Continue medications
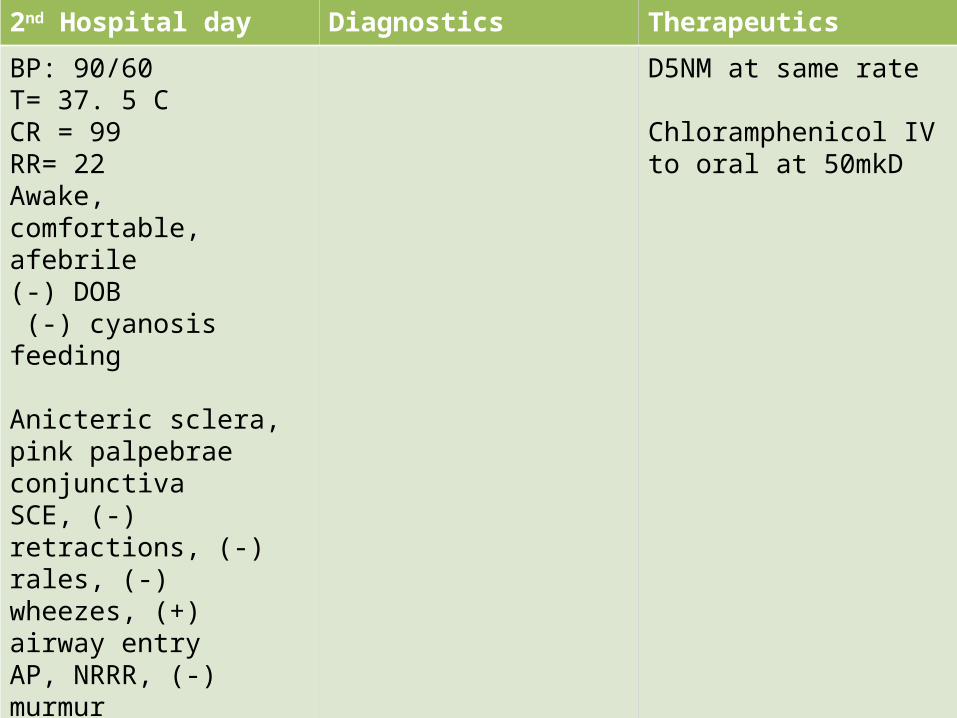
2nd Hospital day Diagnostics Therapeutics
BP: 90/60T= 37. 5 CCR = 99RR= 22Awake, comfortable, afebrile(-) DOB (-) cyanosisfeeding
Anicteric sclera, pink palpebrae conjunctivaSCE, (-) retractions, (-) rales, (-) wheezes, (+) airway entryAP, NRRR, (-) murmurFlat, NABS, soft, non-tender, no organomegalyCRT 1-2 secfull equal pulse
D5NM at same rate
Chloramphenicol IV to oral at 50mkD

3rd Hospital day Diagnostics Therapeutics
AwakeAfebrileBP= 90/60T= 37 CCR = 98RR = 22
(-) DOB(-) tachypnea(-) cyanosis(-) abd pain feedingAwake pink conj, (-) NADSCE, (-) retraction, CBSAP, NRRR, (-) murmurFlat, NABS, soft, non tender, no organomegalyCRT 1-2 sec Full and equal pulses
D5NM at same rate Cont meds
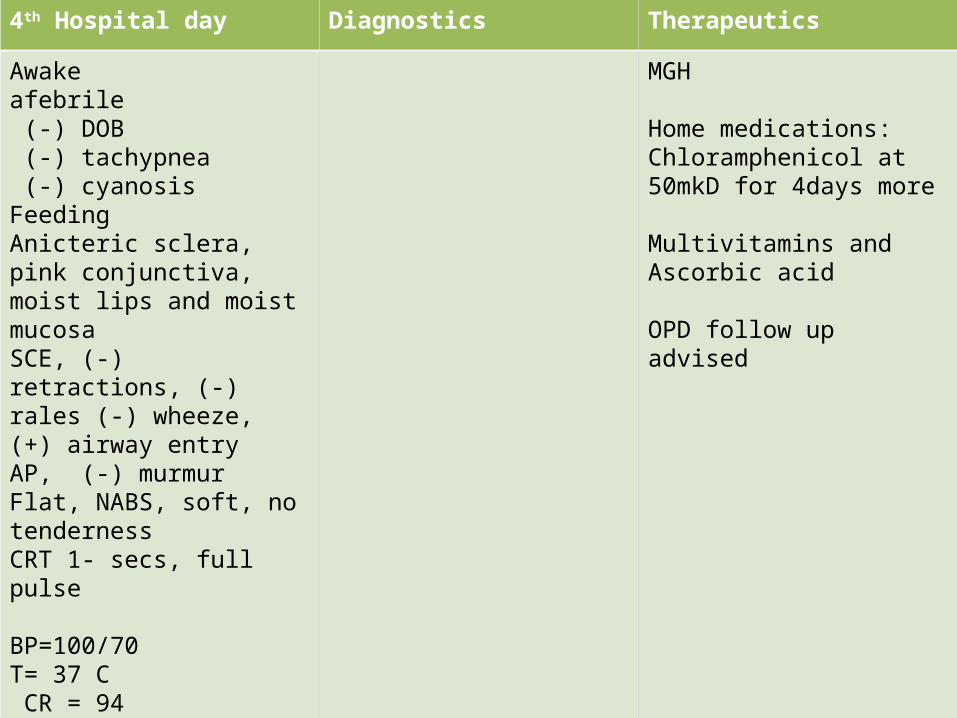
4th Hospital day Diagnostics Therapeutics
Awakeafebrile (-) DOB (-) tachypnea (-) cyanosisFeedingAnicteric sclera, pink conjunctiva, moist lips and moist mucosaSCE, (-) retractions, (-) rales (-) wheeze, (+) airway entryAP, (-) murmurFlat, NABS, soft, no tendernessCRT 1- secs, full pulse
BP=100/70T= 37 C CR = 94RR = 21
MGH
Home medications:Chloramphenicol at 50mkD for 4days more
Multivitamins and Ascorbic acid
OPD follow up advised
TYPHOID FEVERFIINAL DIAGNOSIS


Etiology

the heat-stable lipopolysaccharide components of the
outer membrane
Flagellar heat-labile
proteins
virulence capsular
polysaccharide

Epidemiology
World Health Organization has
estimated that at least 12.5 million cases
occur annually worldwide

Incidence of Typhoid Fever Brown - strongly endemic; orange – endemic;
gray - sporadic cases

Ingestion of foods or water contaminated with human
feces
Water-borne outbreaks due to poor sanitation
and direct fecal-oral spread due to poor personal hygiene Oysters and other shellfish
cultivated in water contaminated by
sewage
In the United States about 65% of the cases result from
international travel
Domestically acquired enteric fever is usually caused by consumption of foods contaminated by individuals
who are chronic carriersCongenital transmission of enteric fever can occur by
transplacental infection



Clinical Manifestations
The IP is usually 7–14 days, but it may range from 3–
30 days, depending mainly on the size of the ingested
inoculum.
The 1st week
The 2nd week

3rd week ( typhoid stage )

4th week (Improvement )
If a person survives until the fourth week, their symptoms will gradually improve
Though weight loss and physical exhaustion can continue for several months.
NEONATES
• cause abortion and premature delivery• enteric fever during late pregnancy may be
transmitted vertically. • The neonatal disease usually begin within 3
days of delivery. • Vomiting, diarrhea, and abdominal distention
are common.

• Temperature is variable but may be as high as 40.5°C. Seizures may occur.
• Hepatomegaly, jaundice, anorexia, and weight loss can be marked.

Complications
Diagnosis
• Results of blood cultures are positive in 40–60% of the patients seen early in the course of the disease,
• stool and urine cultures become positive after the 1st week
Diagnosis
• A culture of bone marrow is the single most sensitive method of diagnosis (positive in 85–90%) and is less influenced by prior antimicrobial therapy
Diagnosis
• Widals test• Typhidot

Treatment
• Chloramphenicol – gold standard• Ampicillin• Amoxicillin• trimethoprim-sulfamethoxazole
Prognosis
• prompt therapy• the age of the patient• previous state of health• the causative Salmonella serotype • appearance of complications

Prevention

Vaccines
• parenteral Typhoid Vaccine• Vi capsular polysaccharide antigen • booster every 2 years• single dose Intramuscularly
• Oral Typhoid Fever Vaccine (Ty 21a )• Similar efficacy• Four enteric-coated capsules are given on alternate
days• Should be repeated every 5 years

Famous victims
