u w [ òâ¸p
TRANSCRIPT

がんの手術を腹腔鏡で !?
兵庫県立がんセンター 消化器外科川崎健太郎
腹腔鏡とは?
お腹の中(腹腔内)にカメラ(鏡)を入れテレビにうつす手技です
腹腔鏡

腹腔鏡
腹腔内に炭酸ガスを入れ膨らませます

本日の内容
•腹腔鏡手術とは•本当にいいの?•実際

キズの大きさ
患者さんが術後に目につくのは

胃切除術において
昔の名外科医
•外科医から•よく見える•手が自由に動く•安全•患者さんから•痛い•動けない、息できない•大きなキズが残る
医者からは良くても患者さんにはよくない

キズを小さくしよう!
これ以上小さくすると危険
そこで
腹腔鏡
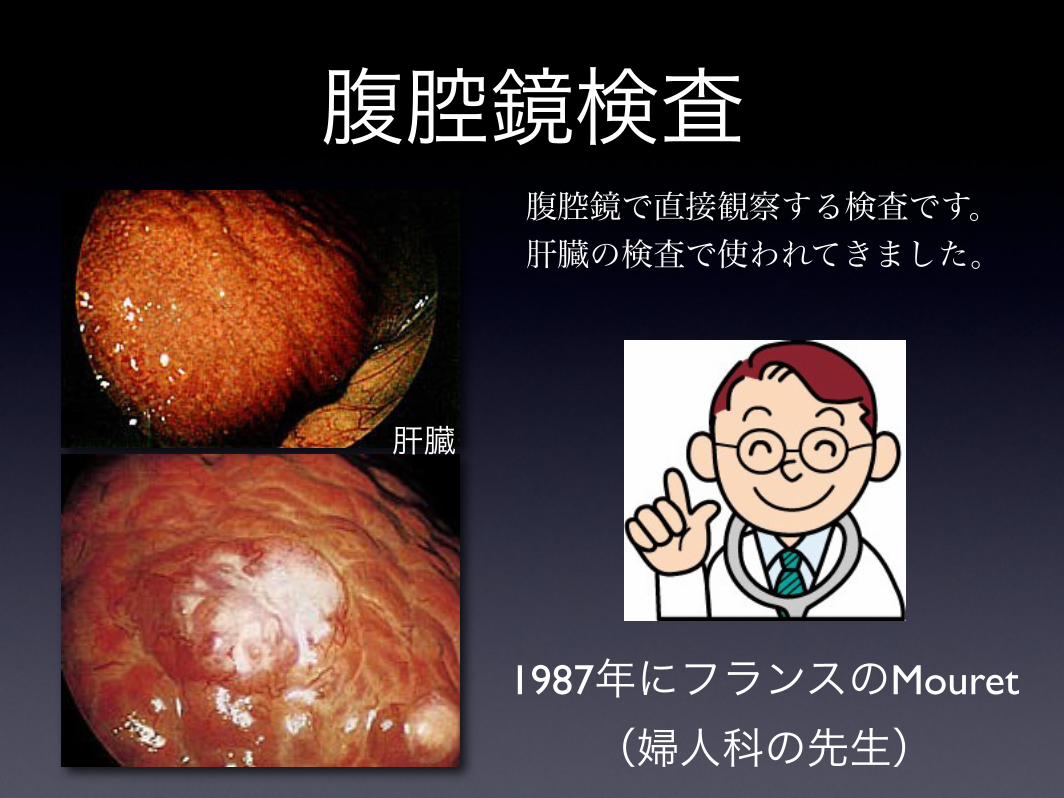
腹腔鏡検査腹腔鏡で直接観察する検査です。肝臓の検査で使われてきました。
1987年にフランスのMouret(婦人科の先生)
肝臓

腹腔鏡手術の歴史• 1987年 腹腔鏡下胆嚢摘出術• 1990年 大腸• 1991年 胃• 1992年 食道• 現在は肝臓、脾臓や膵臓も対象

なぜ?
1. 道具が進歩した。2. 技術が進歩した。3. 患者さんにメリットがあった。

メリット
1.キズが小さくきれいだった2.痛くなく楽で早く退院できた3.合併症が減った

胃切除術において
開腹 腹腔鏡
小さいキズです

胃部分切除術後•1日目から動ける•2日目から水•3日目から食事•7日目点滴終了、退院許可
2006年から開始09.12月までに140名に施行
術後10日前後で退院、合併症は5例
体への負担や合併症も少なく開腹手術よりいいくらいです
キズの小さいやさしい手術
メリット1.キズが小さくきれいだった2.痛くなく楽で早く退院できた3.合併症が減った4.テレビで拡大するのでよく見える
急速に増加しております

日本の現状
90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07
10,000
20,000
30,000
40,000
50,000腹腔鏡手術

日本の現状
90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 070
2,000
4,000
6,000
8,000
10,000
食道癌 胃癌 大腸癌

まとめ:腹腔鏡手術
1.お腹にカメラを入れ行う手術です
2.小さなキズのやさしい手術です
3.患者さん、医師双方にメリットがあります
4.近年急速に増加しております
本日の内容
•腹腔鏡手術とは•本当にいいの?•実際

腹腔鏡は本当にいいの?

腹腔鏡に関連したトラブル
•胆嚢摘出術で失血死•前立腺摘出で失血死•肝切除術での失血死•副腎摘出で膵臓や十二指腸損傷
重大な合併症になりがち!
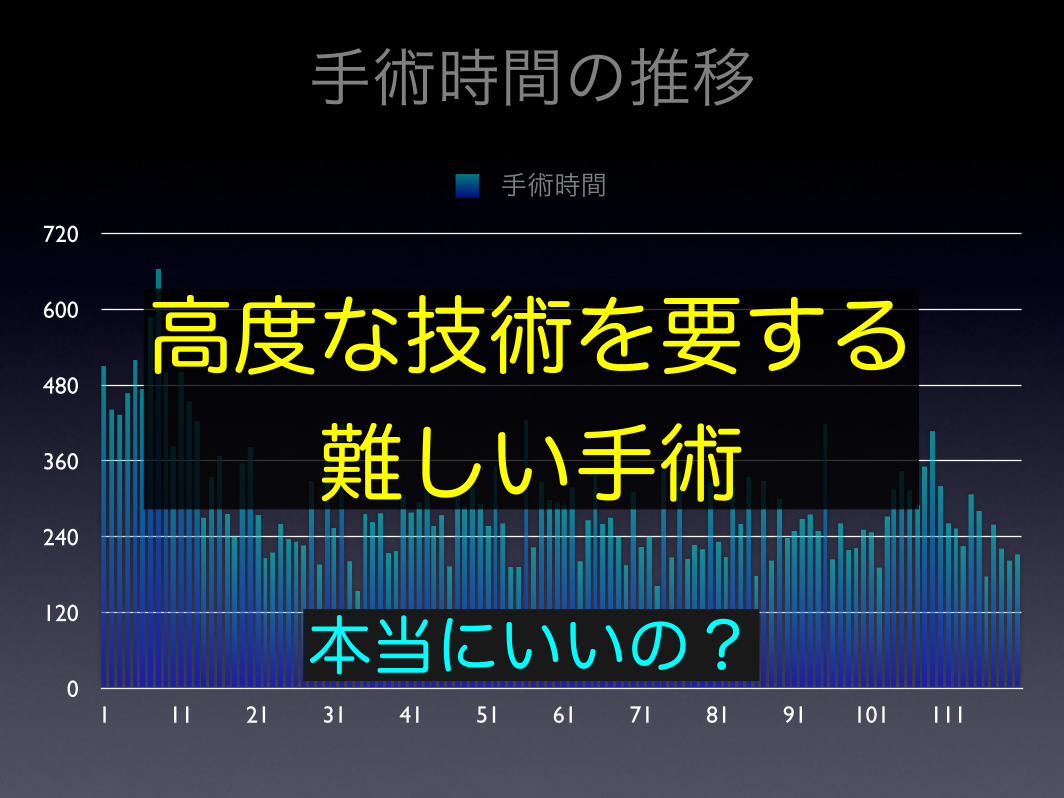
手術時間の推移
0
120
240
360
480
600
720
1 11 21 31 41 51 61 71 81 91 101 111
手術時間
高度な技術を要する難しい手術本当にいいの?

•本当にいいの?1. 安心できる手術のために
•技術認定制度•トレーニング
2. 臨床試験

内視鏡外科学会 技術認定制度
目的:安全な手術を患者様に提供すること
認定医:内視鏡手術を完遂、指導できること
2004年から制度を開始試験の合格率は40%前後
要するに技術テストです

内視鏡外科学会 技術認定制度
目的:安全な手術を患者様に提供すること
認定医:内視鏡手術を完遂、指導できること
2004年から制度を開始試験の合格率は40%前後
要するに技術テストです認定医もいますし、他の外科医も試験合格を目指し頑張っております
学会が中心になり安全な手術のための努力

トレーニング
地道な練習が大事です

•本当にいいの?1. 安心できる手術のために
•技術認定制度•トレーニング
2. 臨床試験

QOLどれだけ人間らしい望み通りの生活を送ることが
出来ているか
安全性
根治性
よい手術
バランスが大事

よい治療かどうかRCT:Randomized Controlled Trial(患者様を振り分けます)=臨床試験
患者様
A BVS

よい治療かどうかRCT:Randomized Controlled Trial(患者様を振り分けます)=臨床試験
患者様
開腹 腹腔鏡VS
臨床試験で良い結果が出て初めて標準治療になります

腹腔鏡の臨床試験•アメリカで大腸がんの患者様を開腹と腹腔鏡に振り分け
•結果•手術時間は開腹の方が短い•創痛、食事開始、入院期間は腹腔鏡が良い•合併症は差がない
根治性は?
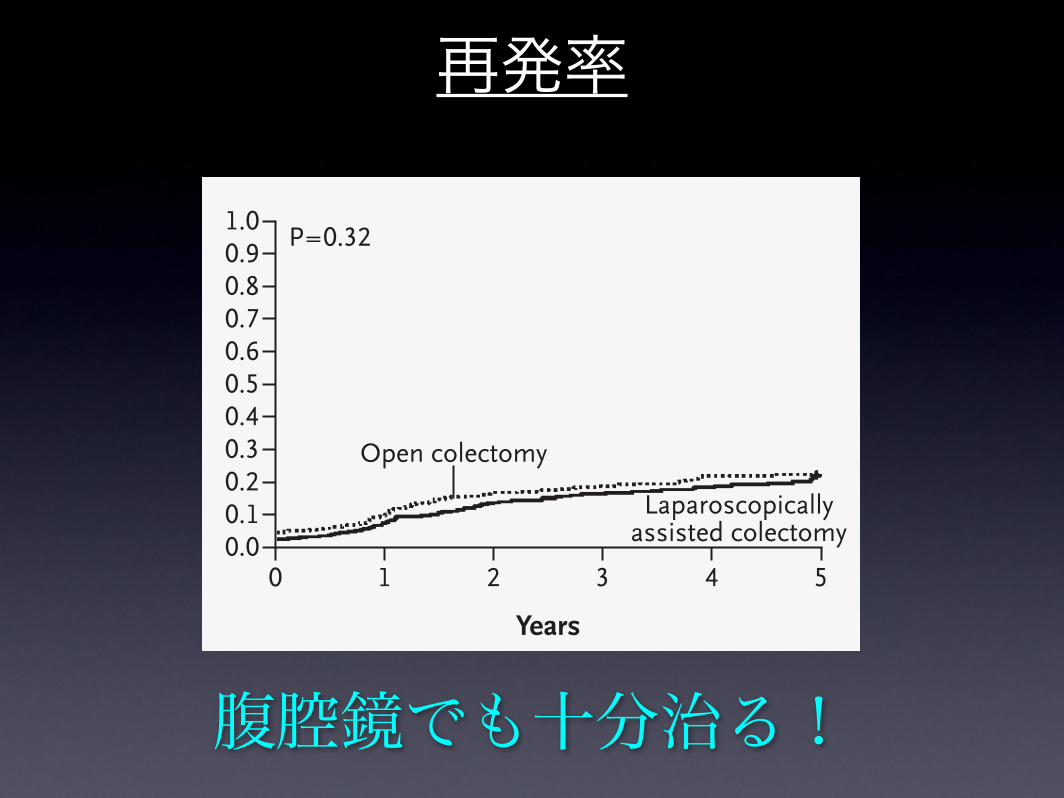
腹腔鏡でも十分治る!
再発率
n engl j med
350;20
www.nejm.org may
13
,
2004
The
new england journal
of
medicine
2056
ed colectomy is not associated with a significantincrease in overall complications.
In addition, other operative factors, includingthe extent of resection — specifically, the number oflymph nodes sampled, the length of bowel andmesentery resected, and the bowel margins — didnot differ significantly between patients who under-went laparoscopically assisted surgery and thosewho underwent open colectomy. It will never be pos-sible to determine whether laparoscopically assistedand open surgery provide the same degree of accu-racy in terms of intraabdominal staging. Theoreti-cally, laparoscopy may be inferior owing to the lossof tactile information provided by traditional sur-gical techniques. In practice, laparoscopy coupled
with solid-organ imaging offers visual capabilitiesthat seem to provide adequate staging information.The finding that the percentage of patients foundto have metastatic disease at surgery did not differsignificantly between groups provides indirect evi-dence of the adequacy of laparoscopic staging. Fur-thermore, there was no trend toward a higher rate ofrecurrence overall or among patients with stage IIIdisease in the group treated laparoscopically, sug-gesting that the presence of undetected abdominalmetastases is not an important limitation of thelaparoscopic approach.
Our finding that laparoscopically assisted colec-tomy, as evaluated in our controlled setting, is safefor patients with colon cancer must be applied cau-
Figure 2. Cumulative Incidence of Recurrence among Patients with Colon Cancer of Any Stage (Panel A), Stage I (Panel B), Stage II (Panel C), or Stage III (Panel D).
The tumor–node–metastasis stage was used. Patients with benign pathological conditions were excluded from this analysis.
1.0
Cum
ulat
ive
Inci
denc
eof
Rec
urre
nce
0.80.9
0.70.6
0.40.3
0.1
0.5
0.2
1.0
0.80.9
0.70.6
0.40.3
0.1
0.5
0.2
0.0
1.0
Cum
ulat
ive
Inci
denc
eof
Rec
urre
nce
0.80.9
0.70.6
0.40.3
0.1
0.5
0.2
0.0
1.0
Cum
ulat
ive
Inci
denc
eof
Rec
urre
nce
0.80.9
0.70.6
0.40.3
0.1
0.5
0.2
0.0
0 1 2 3 4 5
Open colectomy
Laparoscopicallyassisted colectomy
Years
No. at RiskOpen colectomyLaparoscopically
assistedcolectomy
109 118
177 185
240 242
289 311
345 368
395 415
Cum
ulat
ive
Inci
denc
eof
Rec
urre
nce
0.00 1 2 3 4 5
Open colectomy
Laparoscopicallyassisted colectomy
Years
No. at RiskOpen colectomyLaparoscopically
assistedcolectomy
39 56
66 81
85 110
97 133
104 146
112 153
0 1 2 3 4 5
Open colectomy
Laparoscopicallyassisted colectomy
Years
No. at RiskOpen colectomyLaparoscopically
assistedcolectomy
46 37
69 59
93 76
112 103
135 120
146 136
0 1 2 3 4 5
Open colectomy
Laparoscopicallyassisted colectomy
Years
No. at RiskOpen colectomyLaparoscopically
assistedcolectomy
24 25
42 45
62 56
80 73
107 99
121 112
A All Stages B Stage I
C Stage II D Stage III
P=0.32 P=0.65
P=0.50 P=0.49
Copyright © 2004 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at KENRITSU-SEIJINBYO-CENTER on April 26, 2007 .

QOL 安全性
根治性
よい手術
同等
同等どちらかといえば腹腔鏡
大腸がんでは腹腔鏡手術は標準治療

今までの臨床試験の結果大腸 胃 食道
結果 同等 進行中 今後
当院も臨床試験を行っています
臨床試験で良い結果が出て標準治療になります

•大腸がんは臨床試験の結果、開腹手術と同等とされ標準治療
•胃や食道では臨床試験が進行中です•当院も臨床試験参加しております
腹腔鏡の臨床試験
臨床試験にご理解をお願いします。
いいの? まとめ•安心できる手術のために技術認定制度があります
•厳しいトレーニングを行っております•臨床試験で大腸は同等、胃や食道は進行中です

腹腔鏡手術とは
1.キズの小さいやさしい手術2.開腹手術とほぼ同じ3.安全な手術のための努力4.臨床試験があります

腹腔鏡手術とは
1.キズの小さいやさしい手術2.開腹手術とほぼ同じ3.安全な手術のための努力4.臨床試験があります
腹腔鏡でがんの手術は十分に可能です