ubp 10-1-2018 health affairs - betheresandiego.orgbetheresandiego.org/storage/files/ubp 10-1-2018...
TRANSCRIPT

University of Best Practices October 1, 2018
Health Affairs: September 2018
Welcome!
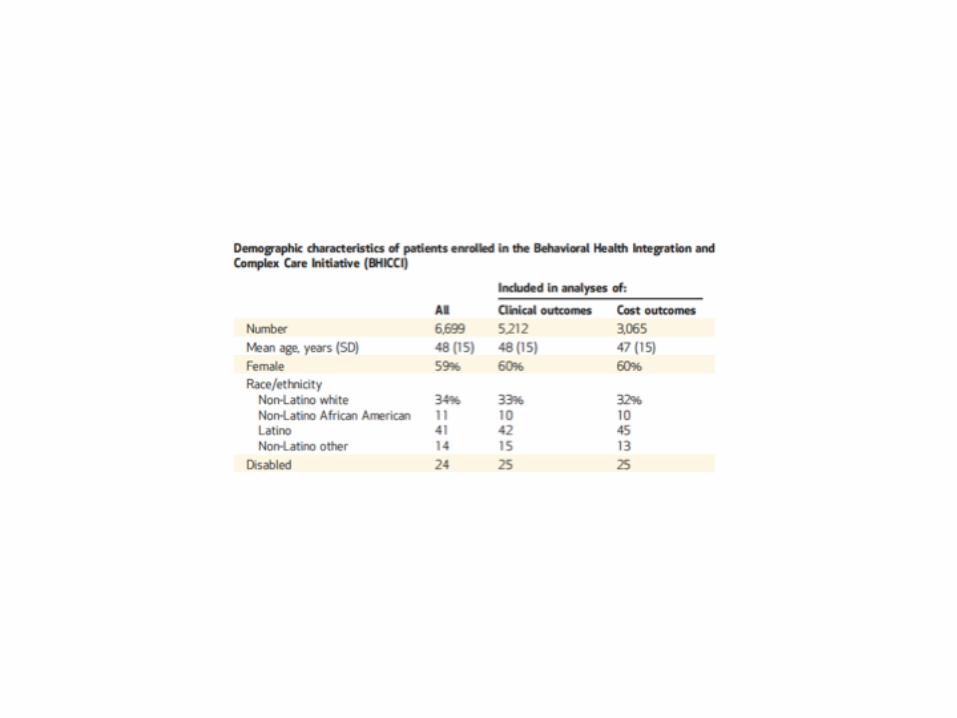
Evaluation of the Behavioral Health Integration and Complex Care Management Initiative
Todd Gilmer, PhD
Chief , Division of Health PolicyDepartment of Family Medicine and Public Health
University of California, San Diego
Collaborators
• Marc Avery, PhD• University of Washington
• Benjamin Henwood, PhD LCSW• University of Southern California
• Elizabeth Siantz, PhD MSW• University of California, San Diego
• Kimberly Center, MA• University of California, San Diego
• Elise Pomerance, MD MPH• Inland Empire Health Plan
• Jennifer Sayles, MD MPH• Inland Empire Health Plan
Overview
• Context for BHICCI• Goals of BHICCI• BHICCI approach to implementation• Learning evaluation using mixed methods• Evaluation results
• Process: staffing, transformation of the care team• Outcomes / Triple aim: quality / clinical, cost, patient satisfaction• Implementation: system-level findings
• Discussion and Implications
Takeaways
• Intensive, complex efforts were required to implement a complex care intervention in a complex environment• BHICCI had a major impact on the patient experience
• “I mean for me I really think they saved my life …”
• Sustainability was a serious focus of BHICCI• Health plan transformation• Targeting health home funding

Inland Empire Health Plan
• Leased 207,000 ft2 space in 2012• 565,000 members in 2012• 1.2 M members in 2017
• Non-profit, Medi-Cal Managed Care Plan• San Bernardino and Riverside
Counties• Two-Plan Counties
Access Challenges for IEHP Members
• Despite gains in insurance coverage, IEHP members continue to face challenges in accessing health care • Shortage of primary care physicians and specialty providers• Siloed funding streams that effectively separate and disconnect physical
health, behavioral health, and substance use treatment providers
• BHICCI aims to improve physical and behavioral health outcomes through a team-based, ‘whole person’ approach to address physical, behavioral, social and environmental needs for complex patients• Sustainability is addressed by preparing participating organizations
for value-based case rate funding as Health Homes, due January 2019
IHI Breakthrough Series
• Emphasizes collaborative learning to achieve major changes in health care delivery• Based on an understanding that sound science exists on improving
quality and reducing costs of care, but is not applied in practice• Close the gap by creating a structure in which organizations can learn
from recognized experts and each other• Short term (6-15 month) learning system that brings together large
numbers of teams to seek improvement in a focused topic area
Core Domains of the BHICCI
• Organizational Leadership• Integrated Care• Integrated Complex Care Management• Population Health Management• Multidisciplinary Team-Based Care• Team Experience• Patient Experience
Practice Coaching
• Practice coaches provided individualized, hands-on guidance to support successful implementation of integrated, chronic care management and person-centered health care• Practice coaches fostered collaborative relationships, empowered
teams, and facilitated whole person care using a relational coaching approach that was guided by several core values: • Learner-centered, collaborative problem solving, partnering and mutuality,
intentionality, social justice and team vitality
• Coaching activities were tailored for each organization• Practice coaches had years of experience in practice change
Quality Improvement
• Each participating organization engaged in quality improvement activities using the Model for Improvement• Practice coaches challenged BHICCI teams to identify and test change
ideas utilizing the Plan-Do-Study-Act (PDSA) framework• Teams received ongoing training in identifying appropriate change
ideas, making hypotheses, testing the ideas, and in building upon previous PDSA test cycles in a process known as “PDSA ramps”
Learning Sessions
• Semiannual learning sessions were designed as an opportunity for participating organizations to develop collaborative relationships through small group discussions and activities• The learning sessions were also used to introduce change ideas,
share data, and develop strategies for quality improvement
Mixed Methods Approach – Triple Aim
• Quantitative data• Clinical outcomes captured in a registry• Cost of services was derived from accounting and administrative data
• Qualitative data• Focus groups (n=8) to measure patient experience• Two focus groups were conducted and analyzed in Spanish
Patient Experience
• Patient voice• Perceived benefits of a care team member who would hear and incorporate
the patient’s expressed care goals, needs and preferences
• Care coordination• Helpful to facilitate appointments with primary care providers and specialists,
especially when embarking on a new relationship with a new type of specialist
• Communication among providers• Patients were impressed with the level of communication among their team
• A desire for direct personal involvement in care• Some participants articulated a desire to have more direct personal
involvement with communication that pertained to their health care needs
Patient Voice
• “I mean for me I really think they saved my life because at the time I was just so frustrated with trying to tell someone something and then they’re trying to tell me like they know my body better than I do … So this team, they came into the doctor’s office, and that’s when they introduced themselves while I was waiting to see the doctor. They came in before the doctor. And it’s awesome.”
Provider Communication
• “I've been in pain management for over 30 years… The fact [is] that there are multiple doctors here that actually talk to each other and kind of bounce ideas off of each other, that they work together to get a treatment program.” • Another patient from a Spanish language focus group described: “All
of the information, appointments, doctors, and reports are in harmony.”
Desire for Direct Personal Involvement in Care
• “I would actually like to meet with all of them at same time… maybe once a quarter … to make sure they all knew what I wanted and all knew the goals set, because maybe they’re having meetings, maybe they’re not. So at least once every three months, or four months, please have all of you for 15 minutes sitting down in the same room with me.”
Conclusions – Triple Aim
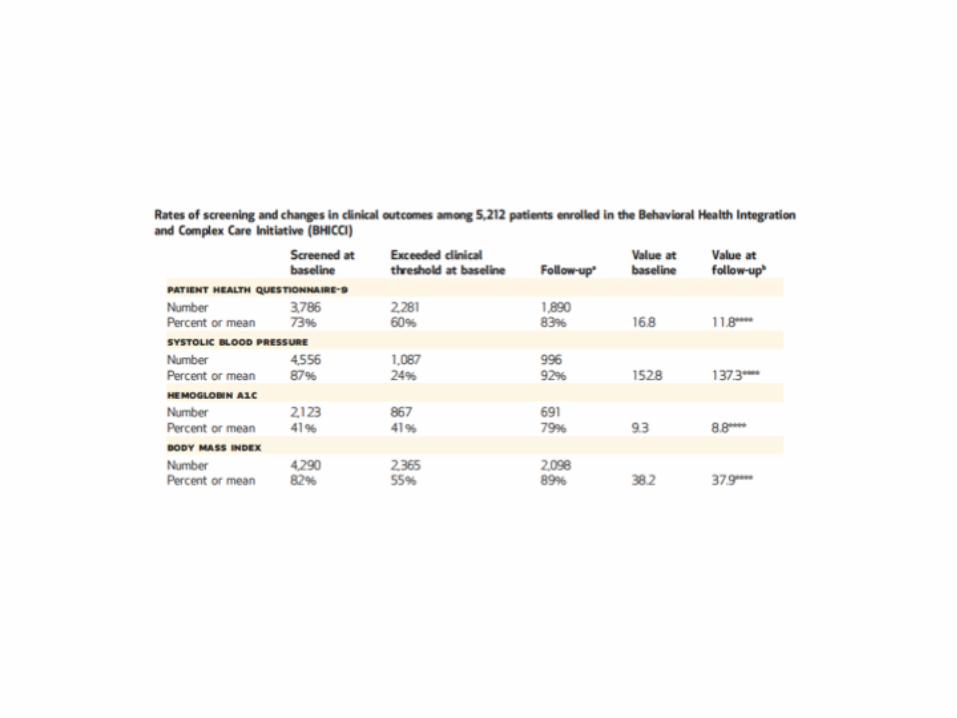
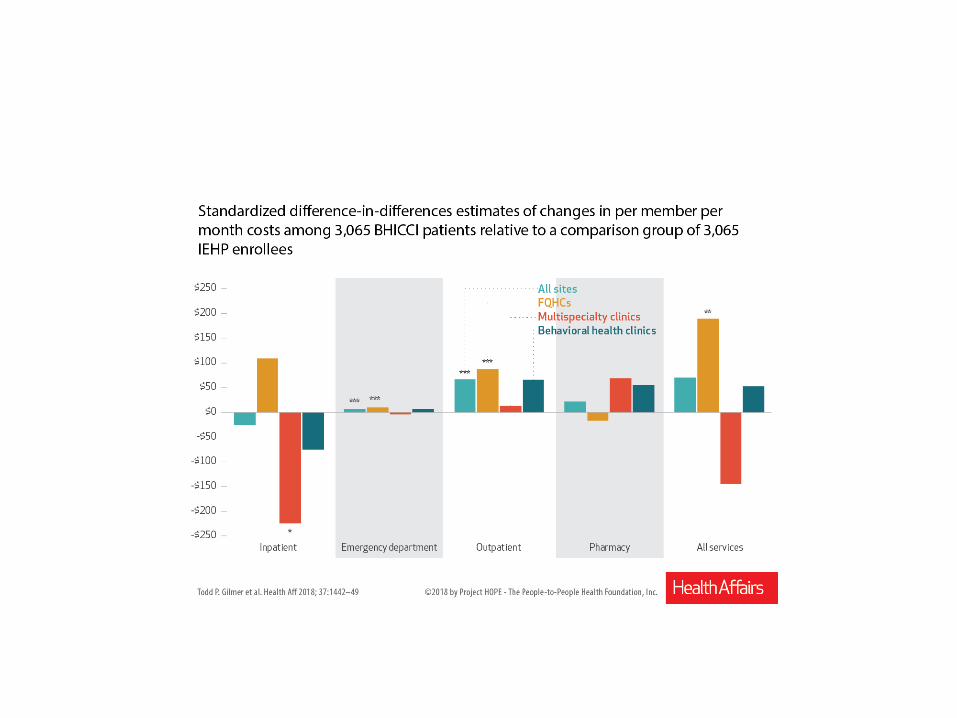
• Several indicators suggest successful implementation of the initiative:• Improvements in clinical indicators for common chronic conditions• Reductions in inpatient costs in some programs• Patients valued the changes they experienced in their health care
• Caveats• Improvements in clinical indicators are somewhat less than what is typically
seen in more narrowly defined disease management programs• Decline in inpatient costs was not consistent across programs
Limitations in the Evaluation
• Timeline for analysis was limited to one year• Clinical effectiveness and cost offsets may increase over time
• Focus on clinical outcomes for common chronic conditions• May have missed changes in clinical outcomes related to complex chronic
conditions
• Non-randomized• Comparison group for cost analysis may have differed in unmeasured
characteristics
Sustainability
• Over the implementation period, the BHICCI transitioned from a pilot program limited in scope to a central effort of IEHP• Activities that were initiated by outside consultants have been
institutionalized by IEHP staff• Internalizing the tracking of clinical outcomes data• Hiring some of the lead consultants who designed and implemented the
BHICCI into key leadership positions• Hiring practice coaches to continue to support practice change
• IEHP targeting funding for health homes to support BHCCI
Transformational Leadership
• Bradley Gilbert, MD, MPP
• First Medi-Cal HMO to earn National Committee for
Quality Assurance (NCQA) Accreditation
• NCQA Accreditation for Disease Management
• Multi-faceted and multi-disciplinary Wellness
Program, to encourage members to live healthy lives and prevent illness
• Over six years, IEHP’s membership increased 160%.
• Formidable provider network, including more than
1,150 primary care physicians and 2,300 specialists.
Thank you!

Christine Thorne, MD, MPHMedical Director, Be There San Diego
One in Five Fewer Heart Attacks: Impact, Savings, and Sustainability in San Diego County-Wide Collaborative
One in Five Fewer Heart Attacks: Impact, Savings and Sustainability in San Diego County CollaborativeAuthors: Allen Fremont, Alice Y. Kim, Katherine Bailey, Hattie Rees
Hanley, Christine Thorne, R. James Dudl, Robert M. Kaplan, Stephen M. Shortell, and Anthony N. DeMaria

Be There San Diego Framework
29
Community ActivationActivate San Diegans at risk for heart attacks and strokes through partnerships with community based organizations.
Healthcare Team ActivationActivate Healthcare Teams to ensure every patient in our region is receiving the best treatment for the prevention of heart attacks and strokes.
Healthcare System ActivationActivate our regional healthcare system to work collaboratively to eliminate heart attacks and strokes.
Grounded in a commitment to Health Equity and Collaborative Approaches to Driving Down Heart Attacks and Strokes through Control of LDL, BP and HbA1c
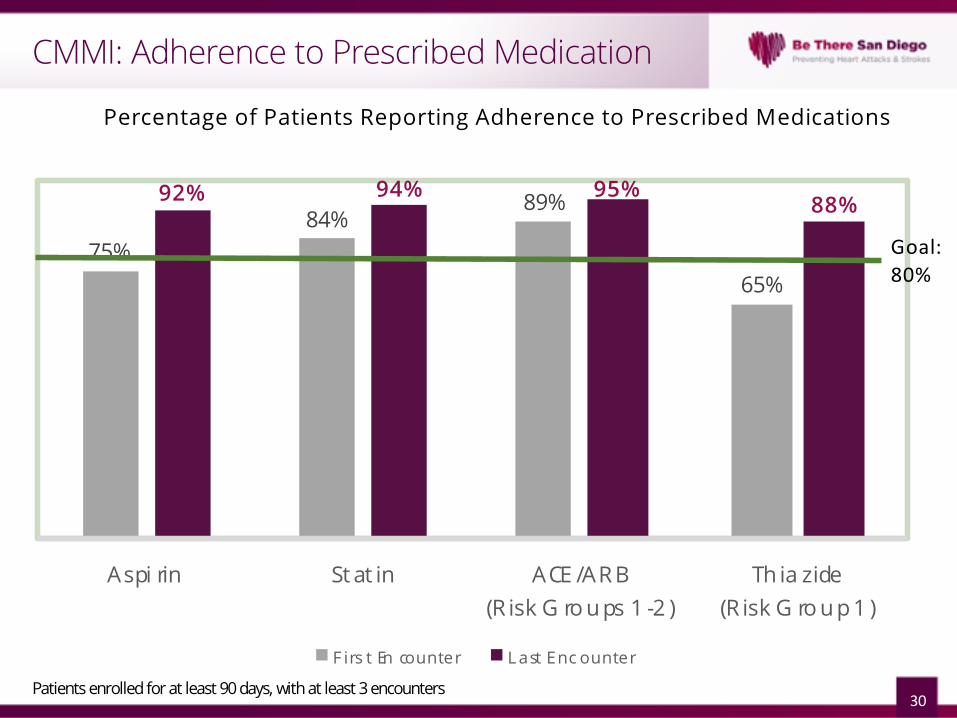
CMMI: Adherence to Prescribed Medication
30
75%84%
89%
65%
92% 94% 95%88%
Aspi rin St at in ACE /AR B(R isk G ro u ps 1 -2 )
Th ia zide(R isk G ro u p 1 )
F irs t En counter L ast Enc ounter
Patients enrolled for at least 90 days, with at least 3 encounters
Percentage of Patients Reporting Adherence to Prescribed Medications
Goal: 80%
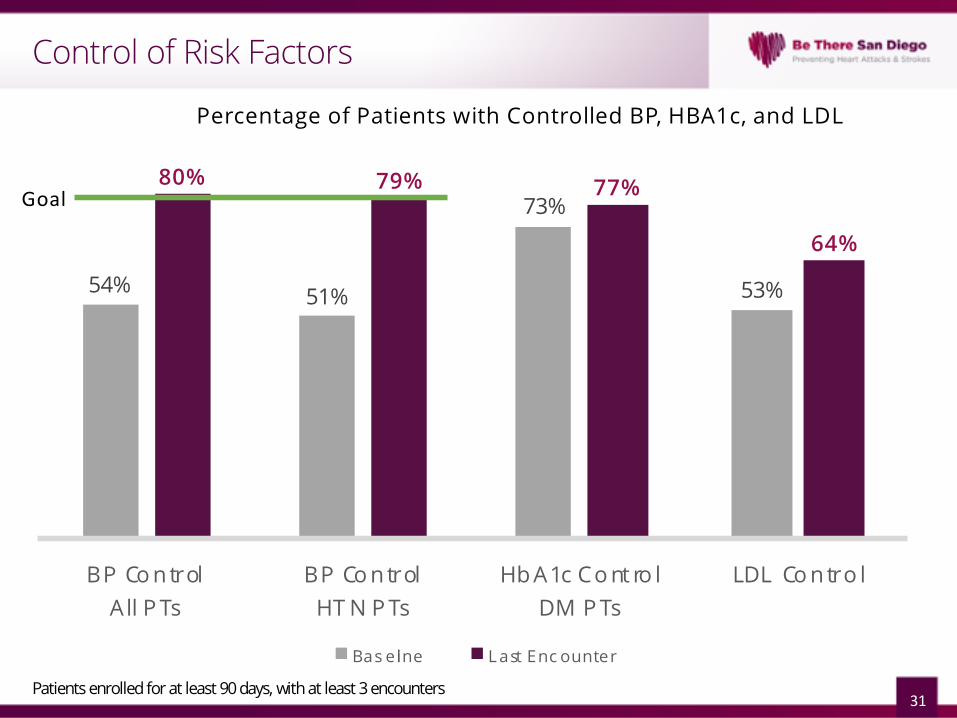
Control of Risk Factors
31
54% 51%
73%
53%
80% 79% 77%
64%
BP Co n trolA ll P Ts
BP Co n trolHT N P Ts
Hb A1c Co nt ro lDM P Ts
LDL Co n tro l
Bas eline L ast Enc ounter
Patients enrolled for at least 90 days, with at least 3 encounters
Percentage of Patients with Controlled BP, HBA1c, and LDL
Goal

UBP and Annual Summit
32
Publicly Available Recommendations
• Recommendations focus on organizational approaches to implementing best practices for managing chronic disease.
• Developed with funding from the CDC and County of San Diego HHSA.
• Topics include:• Team-Based Care• Self-Measured Blood Pressure
Monitoring• Undiagnosed Hypertension• Diagnosis and Management of
Prediabetes• Integrating Community Health
Workers• Pharmacy Integration in Hypertension
Control• Linking with Community Pharmacists• Addressing Food Insecurity
REACH: SESD Faith Community Response
“We believe that each person is born with dignity and divinity with purpose. Chronic heart disease has robbed so many in our community of the greatest joy of fulfilling their purpose. We will no longer sit idly by. We will ‘Be There’ for every member of our community to lift them to their greatness in health.”
34

Impact
35
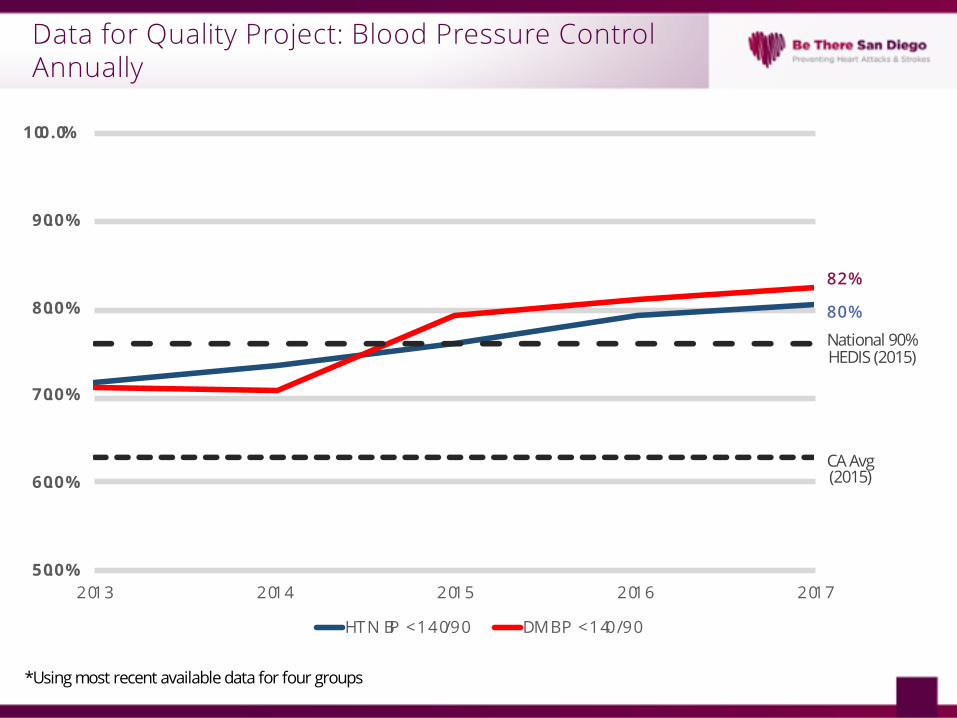
Data for Quality Project: Blood Pressure Control Annually
*Using most recent available data for four groups
80%
82%
CA Avg(2015)
National 90% HEDIS (2015)
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
2013 2014 2015 2016 2017
HTN BP < 140/90 DM BP < 140/90
Hypothesis
Improving control of hypertension, hyperlipidemia and diabetes will prevent major adverse cardiac events, such as myocardial infarction.
- RCI Original Hypothesis
37
Testing the Hypothesis
§Compare rates of myocardial infarction in San Diego to the rest of the state of California• Differences in Differences
oAllows for control of baseline differences that can reflect baseline variation in population and diagnosis of MI
oCompares time after the formation of RCI in San Diego in the early post and late post period to the time before the formation of Be There San Diego
38
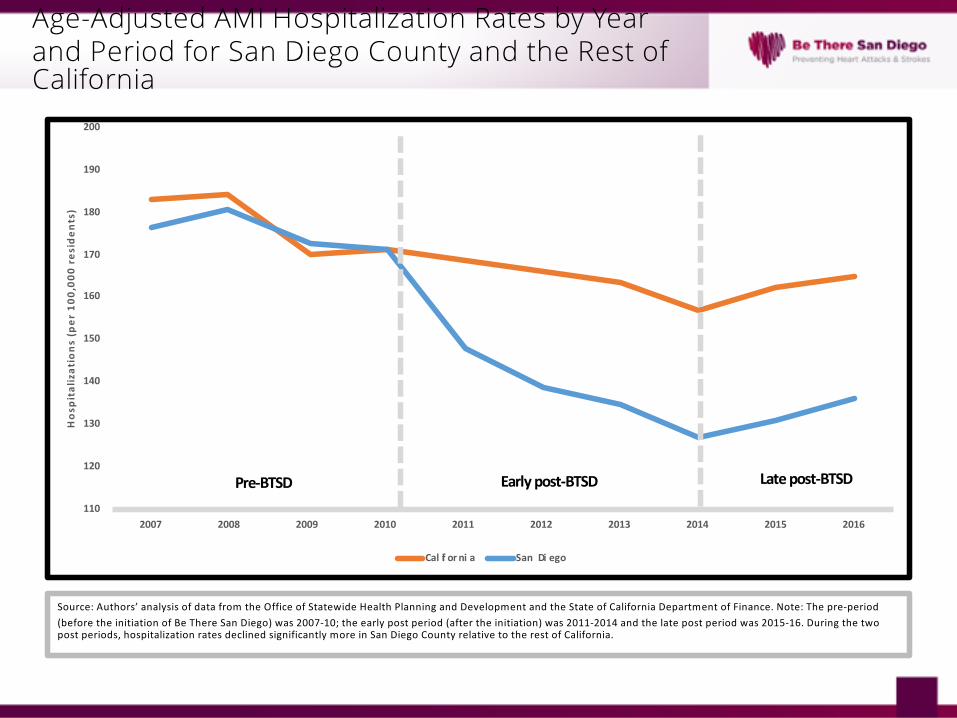
Age-Adjusted AMI Hospitalization Rates by Year and Period for San Diego County and the Rest of California
110
120
130
140
150
160
170
180
190
200
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Hos
pita
lizat
ions
(per
100
,000
res
iden
ts)
Cal if or ni a San Di ego
Early post-BTSD Late post-BTSDPre-BTSD
Source: Authors’ analysis of data from the Office of Statewide Health Planning and Development and the State of California Department of Finance. Note: The pre-period (before the initiation of Be There San Diego) was 2007-10; the early post period (after the initiation) was 2011-2014 and the late post period was 2015-16. During the two post periods, hospitalization rates declined significantly more in San Diego County relative to the rest of California.
Calculating the Prevention
§Calculated the expected rate each year if had maintained the relationship San Diego had to California rate for the pre-BTSD period• Calculated the difference between those
rates• Multiplied by 2014 inflation adjusted AMI
hospitalization cost §Did the reverse for the State of California
40
Calculated AMI Hospitalizations Avoided and Cost Savings during Post-BTSD Periods
§ San Diego• Acute MI Hospitalizations Avoided: 3,826
• Cost Savings: $85.8 Million (2011-2016)
§ California• Potentially avoidable AMI’s if California had
matched San Diego’s AMI rates: 41,706• Potentially avoidable costs associated with
those AMI’s: $935 Million over 6 years
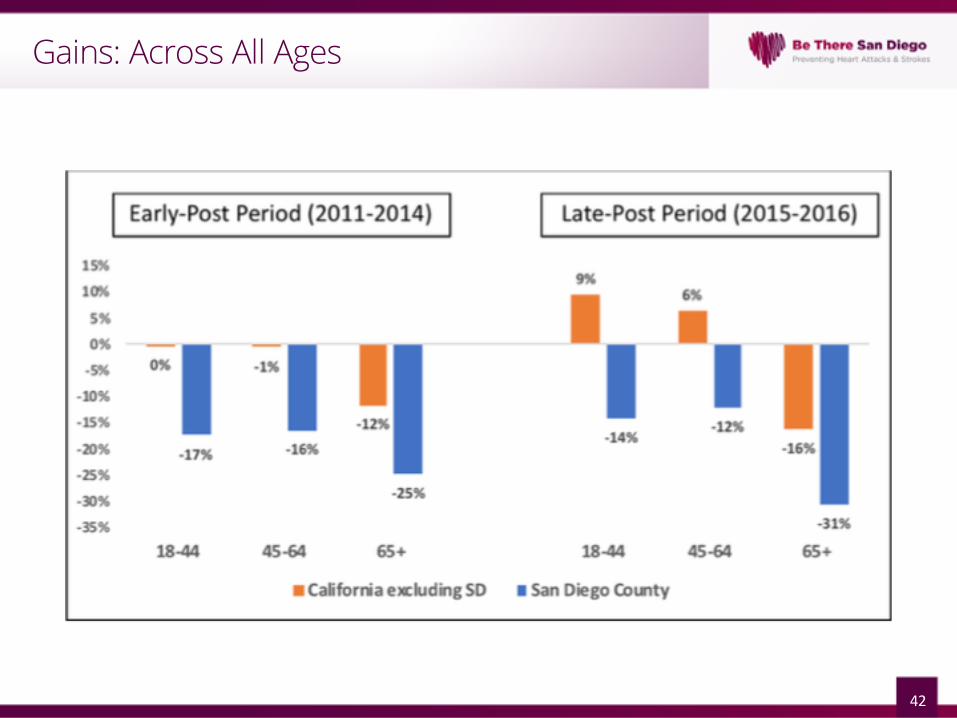
Gains: Across All Ages
42
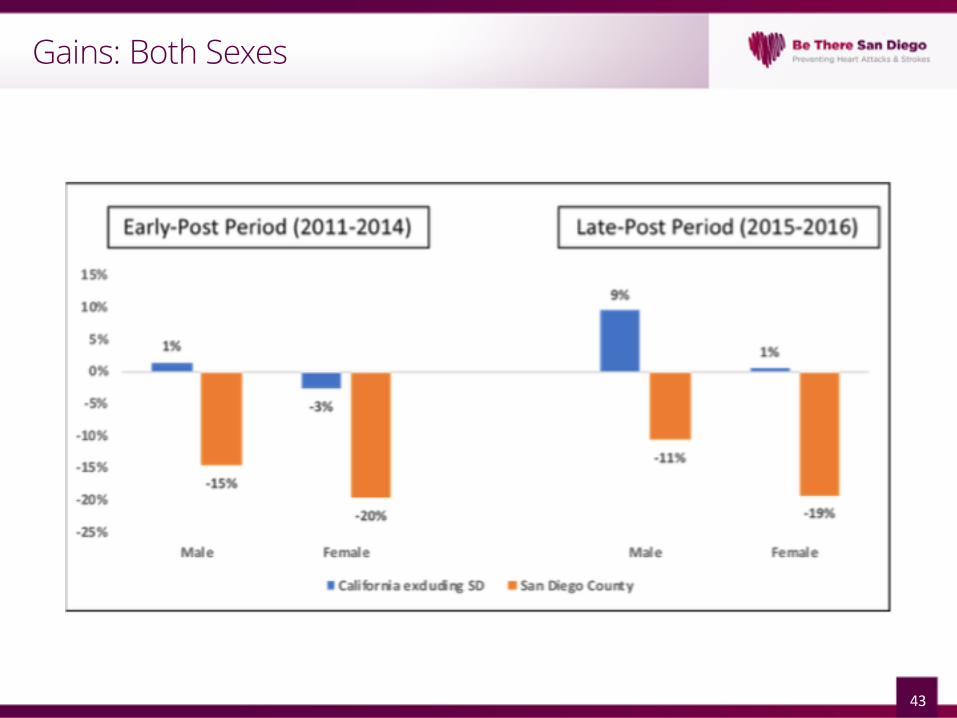
Gains: Both Sexes
43
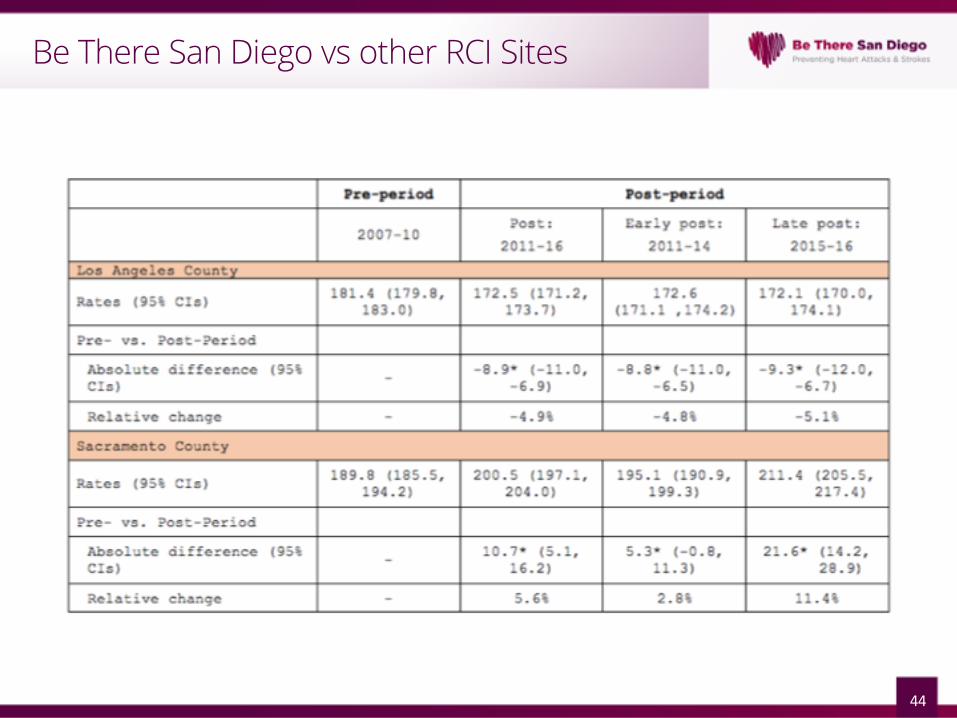
Be There San Diego vs other RCI Sites
44
Data Group: The Secret Sauce?
§Medical directors from FQHCs, Kaiser, Scripps, Sharp, UCSD come together monthly at Data for Quality Project• Primary care
§ Full collaboration§Data Sharing and Transparency§Trust§Shared goals§Honest Discussions
45

Credit to Go Around
46
Bump in the Road?
§Why are AMI’s Increasing since 2014?• Normal random variation (2 years of data)• New trend
oIncreased diagnosis of MI with new high sensitivity troponins
oIncreased coding of AMI with ICD 10oIncreased AMI
§Changing recommendations for lipid control
§Other unknown cause
47
§Statewide and Nationally• Spread the collaborative to other
communities oReplicate results
§ Locally: Maintain and grow• Staffing• Grant support• Adjust to changing incentives in
healthcare• Voluntary participation
48
Next steps
Acknowledgements
§ Right Care Initiative of the University of California
§ RAND Corporation
§ Stanford University’s Clinical Excellence Research Center
§ UC Berkeley School of Public Health
§ California Department of Managed Health Care
§ Sharp Rees-Stealy Medical Group
§ Kaiser Permanente
§ Scripps Coastal Medical Group
§ University of California, San Diego
§ Kaiser Permanente Care Management Institute
§ Blue Shield of California
§ San Diego County Medical Society
§ North Coast Family Medical Group
§ Multicultural Health Foundation
§ Neighborhood Healthcare
§ County of San Diego
§ Scripps Clinic
§ La Maestra Community Health Centers
§ San Diego Family Care
§ Vista Community Clinic
§ San Ysidro Health Center
§ American Heart Association
§ San Diego Black Nurses Association
§ United African American Ministerial Action Council
§ Champions for Health
§ San Diego Health Connect
§ 211 San Diego
The Right Care Initiative’s launch of the San Diego University of Best Practices collaborative and associated research was funded by the National Heart, Lung, and Blood Institute, National Institutes of Health (1RC2HL101811). The work of Be There San Diego has been partially funded by the Department of Health and Human Services (HHS) through the Centers for Medicare and Medicaid Services (1C1CMS331345) and Centers for Disease Control and Prevention (U58DP005622). The contents are solely the responsibility of the authors and do not necessarily represent the official views of HHS or any of its agencies.

Thank you