uc combined conference childhood development
TRANSCRIPT

UC Combined Conference
Childhood Development September 9, 2009
Brad Sobolewski, MD Cincinnati Children’s Hospital Medical Center
Goals
To succinctly review normal pediatric development from birth to age 5
To delve into some sample cases that you may encounter at CCHMC
To show lots of cute pictures

What I’m not going to talk about
School age and adolescent development
Specific learning disabilities
How to do a formal developmental screen
The detailed process of referral for developmental delay

Caveats
This is a pretty broad topic
Learning about development takes lots of practice
It is reasonable to become comfortable with normal milestones by the end of your EM residency
Broadest
topic ever

Polling the Attendings
Why is an understanding of the normal
progression of pediatric developmental
milestones important for the Emergency
Medicine Resident?
Know normal from abnormal
It can help reassure parents
It’s an important part of assessing mental
status

Polling the Attendings
In what circumstances in the Pediatric ED is an understanding of normal development MOST important? Trauma and abuse
Neurological disorders – especially with developmental regression
The severely ill child

How can I get smarter?
Read a book
Observe ’well’ kids
in the ED
Spend time in a
Pediatric clinic
Have kids
Borrow other
peoples’ kids

General developmental framework
Gross Motor – sitting, walking, jumping, and overall large muscle movement
Fine Motor - eye-hand coordination, manipulation of small objects, and problem solving
Language - hearing, understanding, and using language
Social - getting along with people and caring for personal needs

At their own pace…
Developmental milestones are not attained on a
rigid schedule
Children develop in bursts
Things may occur out of sequence
If there are no stairs in the home a child won’t
necessarily know how to climb them
Bilingual babies learn words slower, but catch up by 2
to 3 years
It is important to get a general gestalt in the ED,
not to do a Denver II screen

A guide to the following sections
I’m going to go over normal development
in 3 age ranges
0 to 12 months
Infants 12 to 36 months
Toddlers 3 to 5 years
Preschool

A guide to the following sections
Gross Motor
>90% of children can
do the things listed in
these tables
Fine Motor
Language
Social
Red Flags – reasons to be concerned if a child is unable to do stuff
After each section you’ll see a ‘wrap up’ slide wrap up

0 to 12 months
Infants
Normal development

Stuff that happens from 0 to 12 months
Lots of stuff happens…
Development can go awry in any of the main areas
But the main issues that parents face include; Feeding
Sleep
Fussiness/Colic
Stress
Safety

In room D3
Mayonaze’s mother is worried because she
thinks that her tangy two month old son had a
‘seizure’ because of the H1N1 flu
She went to put him down and he opened his
eyes ‘really wide’ and flailed his arms out
He was a full term baby, and is otherwise
healthy
She wants to know how soon till her baby gets a
head CT

Two months
Gross Motor Lifts head up
Fine Motor Follows to the midline
Language Vocalizes
Social Smiles responsively
Fails to vocalize or react to noises

Four months
Gross Motor Sits while supported with steady head
Fine Motor Follows 180o
Language Laughs
Social Regards own hand
Cannot lift head up, doesn’t vocalize

Six months
Gross Motor Rolls over, May sit unsupported
Fine Motor Reaches, looks for dropped object
Language Turns to sounds
Social Works for an out of reach toy
Doesn’t grasp items, poor trunk muscle control

Nine months
Gross Motor Stands while holding onto support,
cruises
Fine Motor Transfers object to other hand, pincer
grasp
Language Single syllables (da, ma)
Social Feeds self
Cannot roll over or sit with minimal support

Primitive reflexes
Exhibited only by neurologically intact infants
Some have adaptive and survival reasons for existing (rooting)
Others served a more evolutionary value when we were at risk for sabertooth tiger attack
Persistence should trigger a neurologic eval
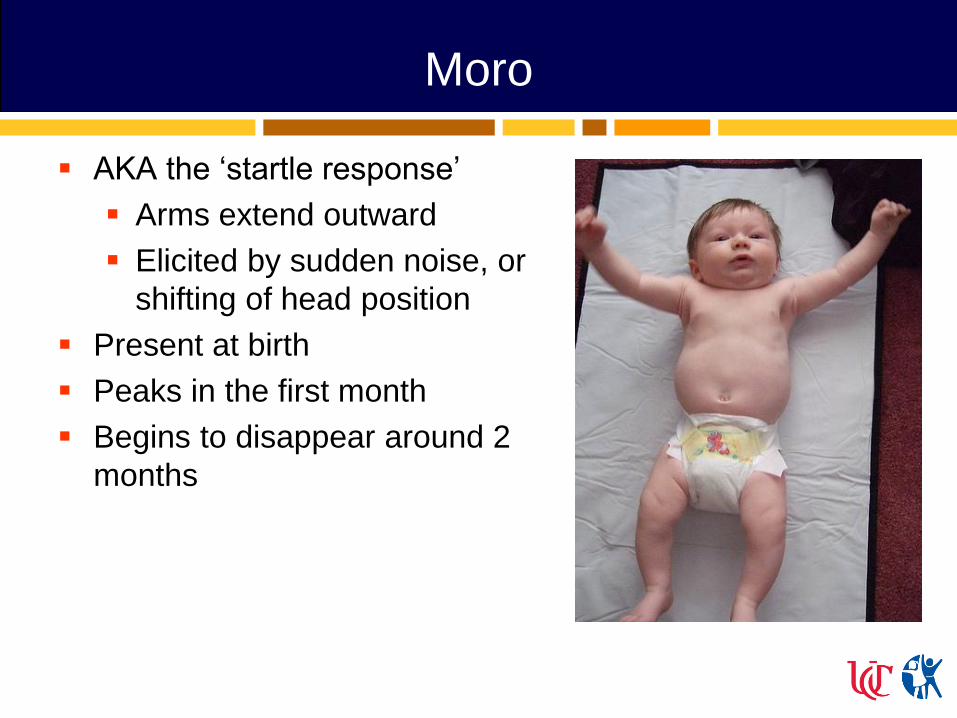
Moro
AKA the ‘startle response’
Arms extend outward
Elicited by sudden noise, or
shifting of head position
Present at birth
Peaks in the first month
Begins to disappear around 2
months
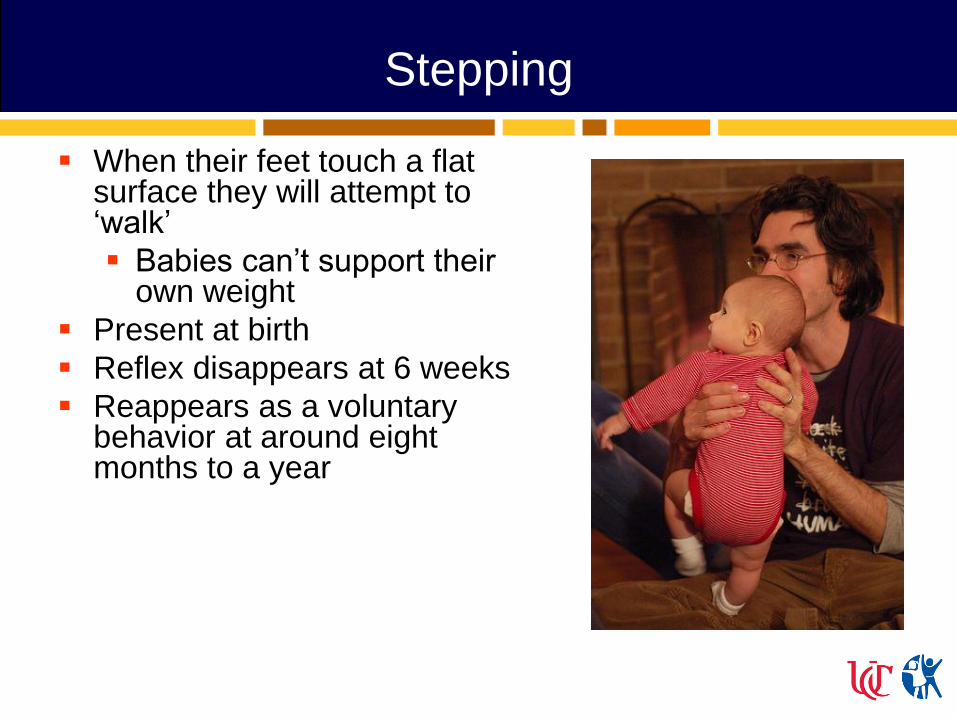
Stepping
When their feet touch a flat surface they will attempt to ‘walk’
Babies can’t support their own weight
Present at birth
Reflex disappears at 6 weeks
Reappears as a voluntary behavior at around eight months to a year

Rooting/Sucking
Newborns turn head toward anything that strokes their cheek or mouth,
Move head in steadily decreasing arcs until the object is found
They will move directly to the object after 3 weeks of breastfeeding
Present at birth
Disappears around four months
Thereafter under voluntary control

Tonic neck reflex
AKA ‘fencing’ posture
When the head is turned to
the side, the arm on that side
will straighten and the
opposite arm will bend
Prepares the infant for
voluntary reaching
Present at one month
Disappears at around four
months
If unable to move out of this position or still present past six months of age - think upper motor neuron disorder

Palmar grasp
Fingers grasp an
object stroking the
palm
Present at birth
Persists until five or
six months
Very cute

Plantar grasp
Plantar flexion of the foot when the sole is stroked Toes plantarflex around object
Present at birth
Persists until five or six months
Abnormal is the ‘Babinski Sign’ Upper motor neuron control is
interrupted
Dorsiflexion of the foot
The Babinski reflex is often confused with the plantar grasp. It is
also present at birth and fades around the first year. When the
side of the foot is stroked, the toes to fan out

Galant
Stroking the skin along the
side of an infant's back will
cause them to swing towards
the side
Present at birth
Fades between four to six
months
Abnormal beyond six months
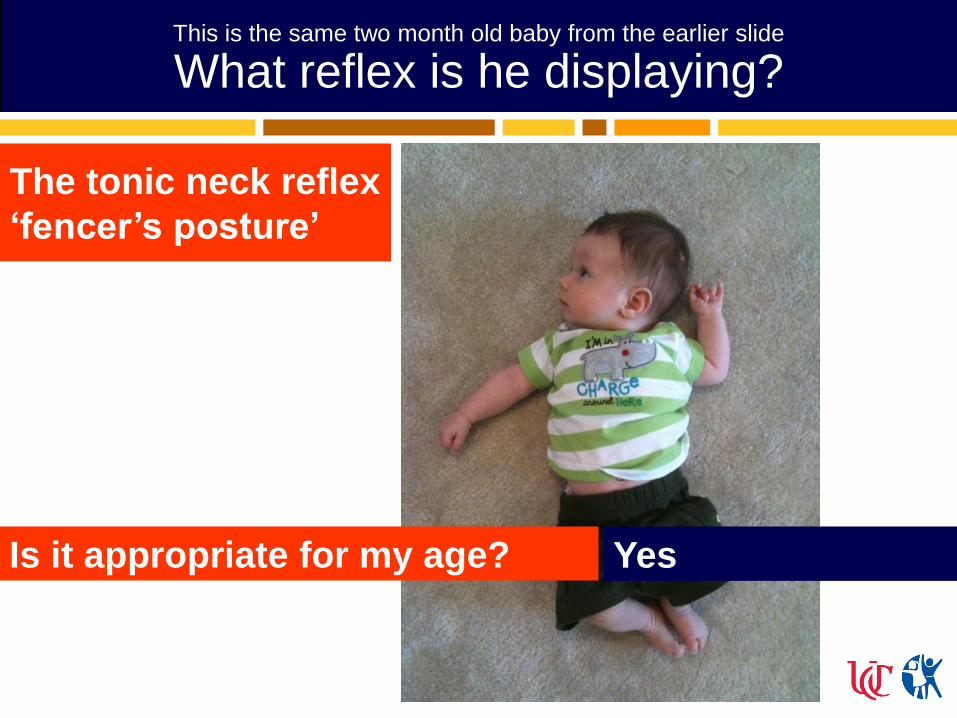
This is the same two month old baby from the earlier slide
What reflex is he displaying?
Yes Is it appropriate for my age?
The tonic neck reflex
‘fencer’s posture’

Back to room D3
Mayonaze’s mom is getting impatient
You correctly ascertain that this baby was not having seizures, and instead explain to Mrs. Hellman what the ‘startle response’ is
She thanks you for the miracle and whips out of the ED

During infancy most kids will learn to…
Gross Motor – roll over, crawl, and
maybe walk
Fine Motor – pick up small objects, play
Language – learn their first word(s) (dada,
mama)
Social – feed themselves (sort of), engage
us in what stimulates them
wrap up

12 to 36 months
Toddlers
Normal development
Stuff that happens from 12 to 36 months
Delays can be noted in all four categories
The main issues that parents face include;
Nutrition
Sleep
Potty training
Discipline
Safety

In room B4
Two year old Donatello is here because his mother witnessed a frightening event.
After she refused to buy him a Diego Monster Truck at Meijer he cried, screamed, made a scene and then ‘passed out’, briefly turning blue around the lips
She thought she saw someone infected with H1N1 in the dairy aisle
Donatello’s mother is demanding a CAT scan or something?

12 months
Gross Motor Pulls to stand, may start walking
Fine Motor Bangs 2 objects together
Language 1 word, babbles
Social protodeclarative pointing, pat-a-cake
Cannot pull to stand and/or support own weight

15 months
Gross Motor Walks well, stoop and recover
Fine Motor Puts block in cup
Language One word
Social Waves bye-bye, drinks from cup
Does not speak one word

18 months
Gross Motor Walks backwards, runs
Fine Motor Scribbles
Language 3 words, points to one body part
Social Helps in house
Can’t walk


2 years
Gross Motor Kicks ball forward, walks up steps
Fine Motor Stacks four blocks
Language Points to 2 pictures
Social Removes garments
Unable to complete fine motor tasks, vocabulary not increasing

2½ years
Gross Motor Jumps up
Fine Motor Stacks six blocks, imitates vertical line
Language Points to 6 body parts, half of speech
is understandable
Social Puts on clothing
No understandable speech
Back to room B4
Donatello’s mom is getting impatient
You are fairly certain that Donatello did not have a seizure, a heart attack, or an infection with H1N1
You do however think that he had a breath holding spell
After your reassurance mom is relieved, and feels like she went through the shredder

Breath holding spells
Peak 1-5 years of age with incidence of 4.6%
Always provoked by pain, anger, or frustration
Two types
Cyanotic type (80%)
Prodrome of crying, forced expiration, apnea then syncope (vagal response)
Generalized cyanosis and LOC
generalized clonic jerks, opisthotonos, and bradycardia may also be seen
Pallid type (20%)
Triggered by response to fear, pain, or injury
Especially after an unexpected minor blow to the head
Initially quiet, end expiratory breath-holding, then pallor, brief loss of consciousness and muscle tone and a fall to the ground
Unless the child is ill appearing or has an injury, no workup is needed

You are seeing an ill appearing 12 month old male
with hydrocephalus. His dad is concerned that he
has lost some milestones. Which of the following
should ALL developmentally normal 12 month old
children be able to do well?
I think we have a problem here…
A. Walk independently
B. Sit without support
C. Roll over
D. Make consonant sounds (da, ma)
As toddlers most kids will learn to…
Gross Motor – run and jump, throw a ball
Fine Motor – Scribble, stack blocks
Language – identify objects and body
parts, put 2 or more words together (50-
75% of language is understood)
Social – get dressed, help with chores at
home, play with peers
wrap up

3 to 5 years
Preschool
Normal development

Stuff that happens from 3 to 5 years
Problems in this age range are more related to social and language development
Parents deal with;
Nutrition
Sleep
Discipline
Safety
School

In room A7
Bayonette is a sharp 3½ year old female who is being seen in the ED for awakening after screaming
Mom is convinced that her daughter is having severe abdominal pain because she has H1N1
Bayonette is jumping up an down singing the theme from ‘The Wiggles’
Mom wants a CT scan of her belly

3 years
Gross Motor Throws ball overhand
Fine Motor Stacks six blocks, wiggles thumb
Language Names 4 pictures, most speech is
understandable
Social Brushes teeth with help
No social interaction or reciprocity

4 years
Gross Motor Hops, balances on each foot for 2
seconds
Fine Motor Stacks 8 blocks, draws person with 3
parts
Language All speech is understandable
Social Copies a circle
Speech is hard to understand

5 years
Gross Motor Walks backwards
Fine Motor Prints first name
Language Speak in sentences
Social Uses the toilet independently, plays
games with rules and follows them
Cannot speak in sentences

Back to room A7
Bayonette’s mom is getting impatient
Your physical exam is entirely normal, except for the fact that she is ticklish
You slice through the tension in the room and explain to mom that you think her daughter had a night terror
She wonders if it can be caused by H1N1?

Night/sleep terrors
Start around 1 months, peak between 5-7 years
Rarely recur in the same night and their
Occur 1-3 times a month
Duration – up to 30 minutes
Common features include;
Sudden, dramatic arousal with vocalization, agitation, and fear
Tachycardia, diaphoresis, mydriasis (autonomic symptoms)
Difficult to arouse
Fall back to sleep spontaneously after several minutes
Amnesia after the event
Triggered by stress, sleep deprivation, and medications
stimulants, neuroleptics, sedatives, and antihistamines.
Recording episodes on video-EEG and polysomnography is necessary when the diagnosis is unclear

As preschoolers most kids will learn to…
Gross Motor – Throw a ball well, balance
on one leg
Fine Motor – Draw pictures of people,
display handedness
Language – Speak clearly and
understandably, learn colors
Social – Brush their teeth, play organized
games
wrap up

How old am I?
A. 12 months
B. 15 months
C. 21 months
D. 24 months
I know 3 words – mama, dada, and baba (bottle)
Hand me a crayon, and I’ll scribble
I can walk across the living room all by myself
I wave bye-bye when grandma goes home
B. 15 months

Special circumstances
Global delays Prematurity
Social and language delays Autism spectrum disorders
Motor delays Cerebral palsy

Special circumstances - Preemies
These babies often have many medical problems
The more premature you are the longer it will take to catch up
Adjust milestone assessment for gestational age
A 2 to 3 month lag is common
Most healthy preemies should catch up to their peers by age 2-3

Special circumstances - Autism
A group of neurodevelopmental disorders characterized by deficits in Socialization
Communication
Behavior
Motor development is not typically impaired
Symptoms are always present before age 3

Special circumstances - Autism
2/3 did not acquire communication skills before age two
1/3 have relatively normal development during the first 12 to 24 months of life, then regress
1/4 to 1/3 achieve early language milestones, but have regression of language, communication, and/or social skills between 15 to 24 months of age Can be gradual or sudden
Ally with parents in the ED to find ways to successfully examine and interact with their autistic child

Special circumstances - CP
Heterogeneous group of static clinical syndromes characterized by motor and postural dysfunction Spasticity, chorea, dystonia, ataxia
Voluntary movements are uncoordinated, stereotypic, and limited. Require effort and concentration to perform simple movements
Sometimes an attempted voluntary movement may evoke a primitive reflex, or mass muscle movements
Associated disorders are common (Murphy, 1993) Mental retardation 65%,
Epilepsy 46%
Sensory impairment 15%
Murphy, et al. Prevalence of cerebral palsy among ten-year-old children in metropolitan
Atlanta, 1985 through 1987. J Pediatr 1993 Nov;123(5):S13-20

Special circumstances - CP
2-3/1000 - 8 year olds have CP
Multifactorial etiology Known causes account for a small proportion of cases
Most are thought to be due to prenatal factors
Perinatal asphyxia plays a role in some
Risk factors from a study of 213 Australian children with CP (Strijbis, 2006) Prematurity 78%
Intrauterine growth restriction 34%
Intrauterine infection 28%
Antepartum hemorrhage 27%
Severe placental pathology 21%
Multiple pregnancy 20%
Strijbi, et al. Cerebral palsy and the application of the international criteria for acute
intrapartum hypoxia. Obstet Gynecol. 2006 Jun;107(6):1357-65

Special circumstances - CP
Tips for the H&P in CP
Ask parents about their
child’s motor tone to get
an accurate exam
Accommodate for
sensory disorders
Don’t just assume that
all of these kids also
have mental retardation

Resources
‘The Pocket’ pages 80 and 81
Bright Futures (AAP)
Touchpoints: your child's emotional and behavioral development by T. Berry Brazelton

Things you can do/observe in the ED
6 months
Watch the infant sit
Stand infant and see if she bears weight on both legs
Give her a block or toy and watch her transfer it to the other hand
9 months
Offer little pieces of paper to pincer
Wave or give ‘five’ at greeting
Call his name when his back is turned to you and see if he turns to look at you

Things you can do/observe in the ED
12 months
Watch her walk or stand
Ask her to give block back or put in container
Wave bye
15-18 months
Point at something and watch him look in the direction that you point
Ask ‘where is mommy?’ and see if he points
Give him a doll or stuffed animal and ask him to hug it
Watch them scribble

Things you can do/observe in the ED
18-24 months
Ask her to point to a specific picture in a book
Have her name an object in a book
Ask her to jump (2 feet off ground)
3 years
Ask him what his name is and if he is a girl or
a boy? (should get it right)

Things you can do/observe in the ED
4 years Give her 5 tongue depressors and ask her to count
them
Draw a person (you should see 3 features)
Do your physical first then watch her dress while you talk to mom
Ask her to balance on one foot ( should balance 5 seconds)
5 years Have him hop and skip
Ask him to spell or name four letters in his name

The big 5
Take home points about childhood development The four major areas of development are gross
motor, fine motor, language, and social
Beware if the kid doesn’t… Vocalize at 1 year (worry about autism)
Walk at 18 months (worry about motor neuron disease)
Have understandable speech at age 4
‘Loss of milestones’ is a major red flag in progressive neurologic disorders
You will only become more experienced by examining healthy children and talking to their parents
You can easily assess development in a very short time in the ED