ucsd neurosurgery sub-intern presentations simon buttrick, msiv mount sinai school of medicine
TRANSCRIPT
UCSD NeurosurgerySub-Intern PresentationsSimon Buttrick, MSIV
Mount Sinai School of Medicine

Case 21 year old male admitted 11/11 after assault with head
trauma Past medical history: multiple fractures Social history: EtOH socially, no smoking, lives with girlfriend Family history: meningioma in mother Exam:
AOx3, appropriate PERRL, EOMI, CNII-XII grossly intact Strength 5/5 throughout Sensation intact in all four extremities




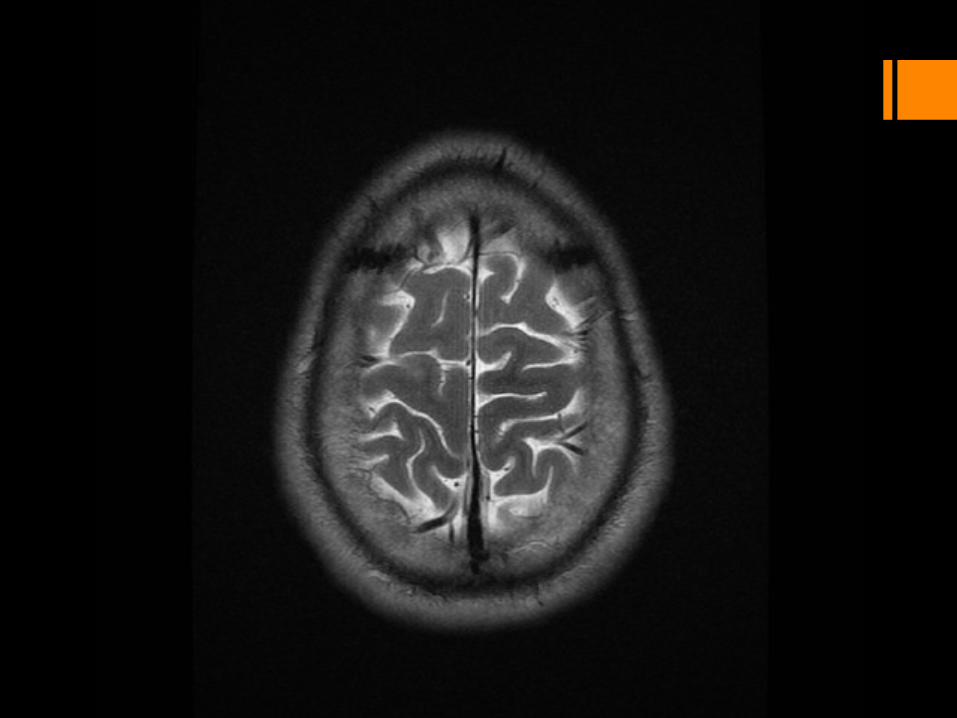




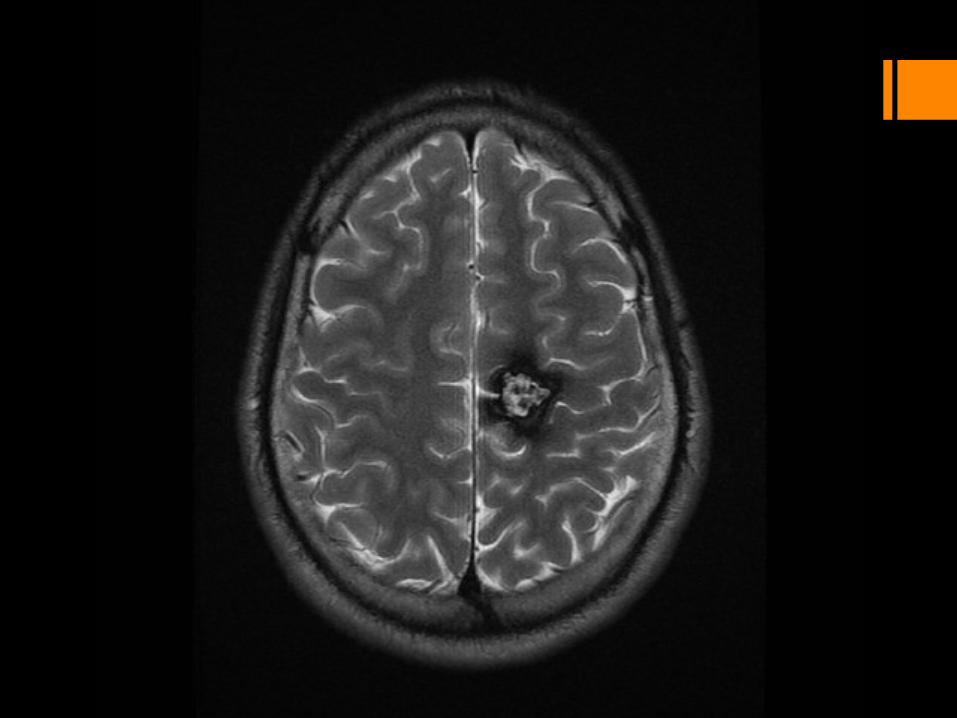















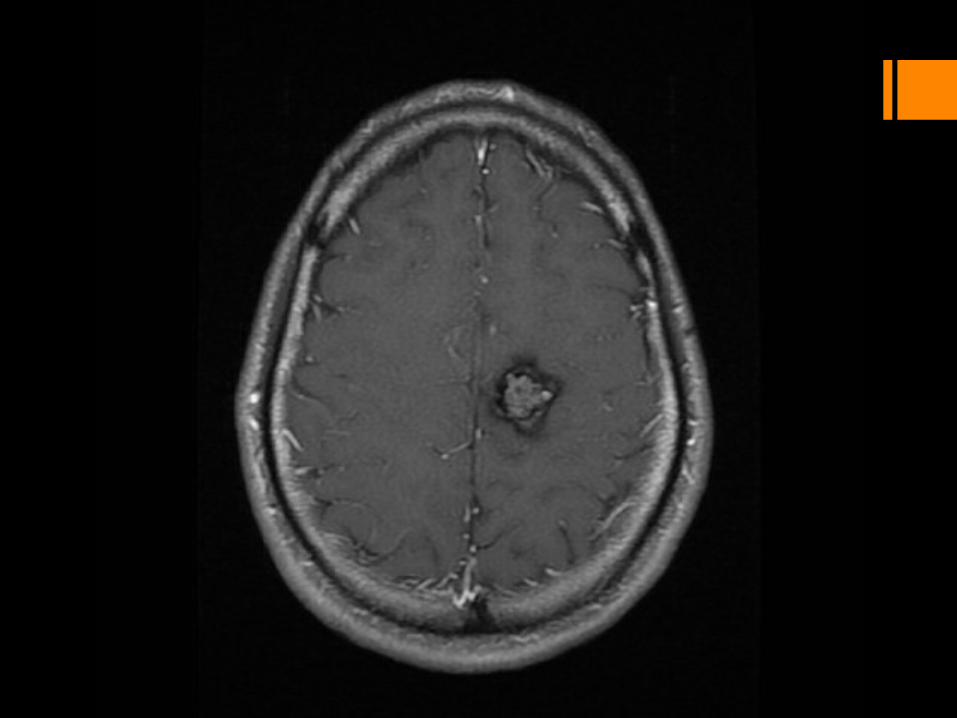















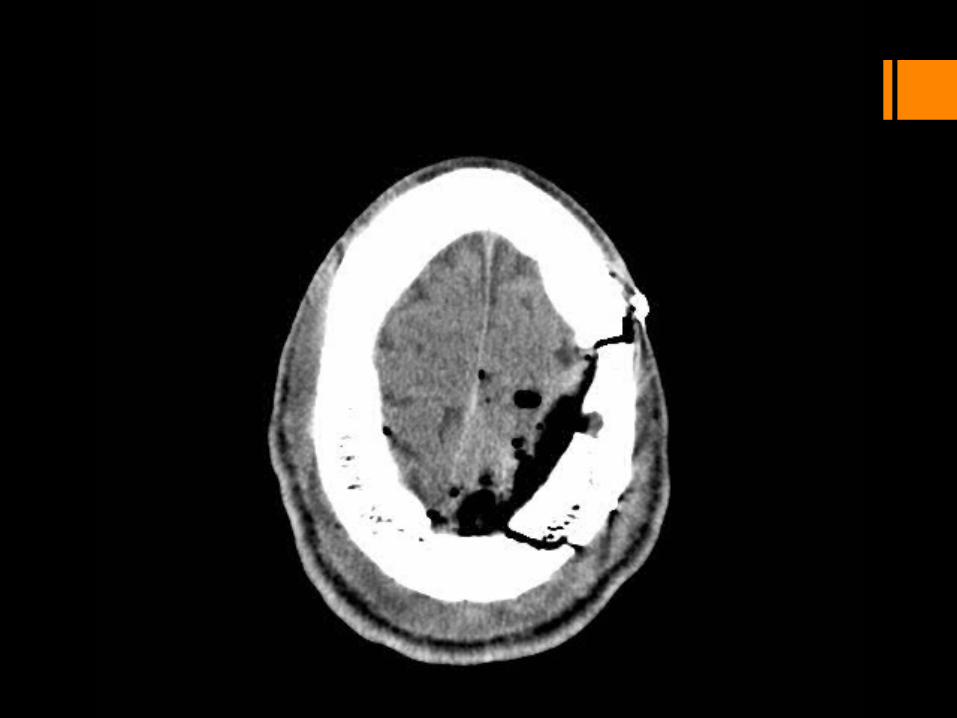
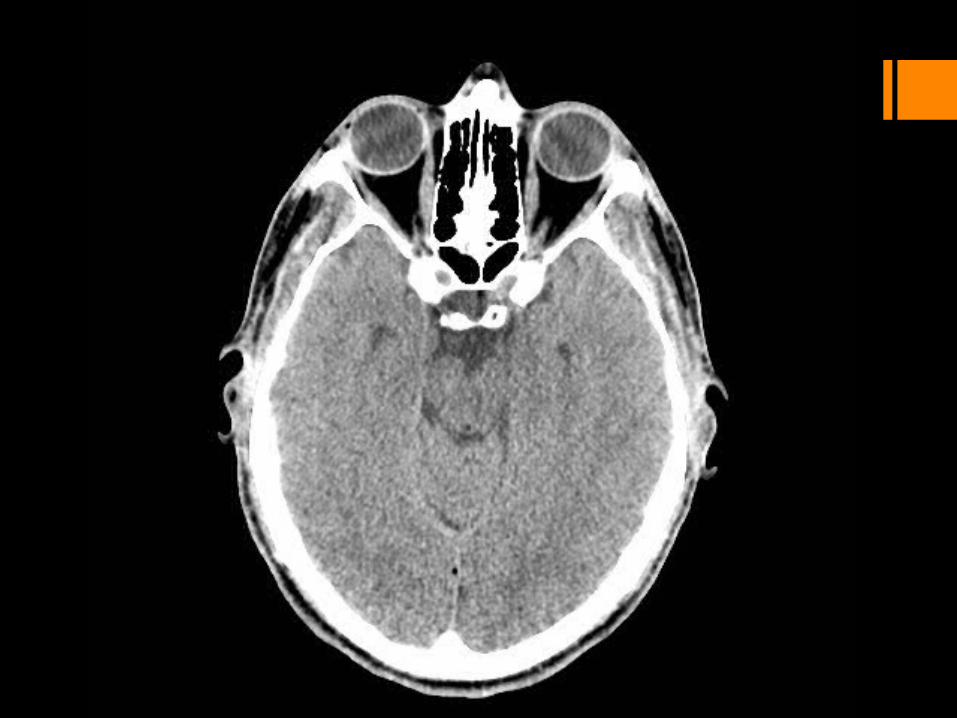
Case - continued Levetiracetam started March 2012: Seizure, head trauma RLE weakness CT head showed slight interval increase in blood products
concerning for cavernoma rupture

preoperative intraoperative
Surgical planning - options
fMRI Magnetoencephalography PET Transcranial magnetic
stimulation
Awake craniotomy Electrocorticography SSEP MEP

preoperative intraoperative
Surgical planning - options
fMRI Magnetoencephalography PET Transcranial magnetic
stimulation
Awake craniotomy Electrocorticography SSEP MEP

Magnetoencephalography Current → Magnetic field → Current Need ~ 50,000 neurons to create a
measureable field (10 fT) Field is measured by numerous
detectors Source estimated (inverse problem)
MEG fMRI
MEG vs fMRI
Direct representation of neuronal activity
Better time resolution
More readily available Cheaper Better studied
Stuffleberg, Clinical Magnetoencephalography for Neurosurgery, Neurosurg Clin N Am 22 (2011) 153–167

MEG EEG
MEG vs EEG
Less distortion of signal by scalp
Better spatial resolution
Sensitive to both tangential and radial components of current
Less signal drop off with distance

Median nerve stimulation

Tibial nerve stimulation

Hand motor response

Foot motor response

transfalcinetranscortical
interhemispheric

Anesthetic considerations Risk of air embolism
Central line Continuous precordial doppler Arterial line
Operating near motor and sensory areas MEP SSEP Brain lab























Post-op course POD1:
Moderate right pronator drift RUE: 4+/5 RLE: proximally 5/5, ankle plantarflexion 3/5, ankle dorsiflexion 2/5,
wiggling toes “95%” sensation in R hemibody Ambulating with physical therapy
POD2: discharged home Mild right pronator drift RUE: 5/5 RLE: proximally 5/5, ankle plantarflexion 4/5, ankle dorsiflexion 3/5,
wiggling toes

Recovery No good data on recovery of motor function after
corticectomy in motor strip In stroke patients, initial degree of paresis is strongest
predictor for recovery

Thank you Special thanks to Dr. Khalessi and Jayant

References Stuffleberg, Clinical Magnetoencephalography for Neurosurgery, Neurosurg Clin N Am
22 (2011) 153–167 Gross et al., The natural history of intracranial cavernous malformations, Neurosurg
Focus 30 (6):E24, 2011 Kekhia et al., Special Surgical Considerations for Functional Brain Mapping, Neurosurg
Clin N Am 22 (2011) 111–132 Hendricks et al., Motor Recovery After Stroke: A Systematic Review of the Literature,
Arch Phys Med Rehabil Vol 83, November 2002