ueda2012 ectopic fat-d.mohamed
TRANSCRIPT
Mohamed Kamar
Professor Of Diabetes And Endocrinology
Faculty Of Medicine
Zagazig University
Aswan February 2012
ECTOPIC FAT
FAT AROUND THE BODYIS IT ALL THE SAME?
FAT AROUND THE BODY
• Physiological role of fat----------
The Good
• Too much fat in fat tissue---------
The Bad
• Fat in non-fat tissue-----------------
The Ugly
PHYSIOLOGIC ROLE OF FAT: TRIGLYCERIDE
• Energy dense macromoloecules: 9 kcal/g
• Stored without water
• A 72 kg person has 12 kg fat =110,000 kcal= 60 days (vs 1 day from glycogen)
• 12 kg fat = 126 kg glycogen
• Triglycerides are stored in specialized fat cells (adipocytes)
• The adipose tissue is not just a fat depot
PHYSIOLOGIC ROLES OF FAT: TRIGLYCERIDE

AdiposeAdiposeTissueTissue Unknown Unknown
FactorsFactorsAgouti proteinAgouti protein
RetinolRetinol
PAI-1PAI-1
LeptinLeptinASPASP
AngiotensinAngiotensin
ANG-IIANG-II
AdiponectinAdiponectin
AdipsinAdipsin
ResistinResistin
Bone Morphogenic ProteinBone Morphogenic Protein
IGF-1IGF-1IGFBPIGFBP
TNF-TNF- Interleukins InterleukinsTGF TGF FGFFGFEGFEGF
Fatty AcidsFatty AcidsLysophospholipidLysophospholipidLactateLactateAdenosineAdenosineProstaglandinsProstaglandinsGlutamineGlutamine
EstrogenEstrogen
PHYSIOLOGIC ROLES OF FAT: TRIGLYCERIDE

TOO MUCH FAT IN FAT TISSUE
How much is too much?
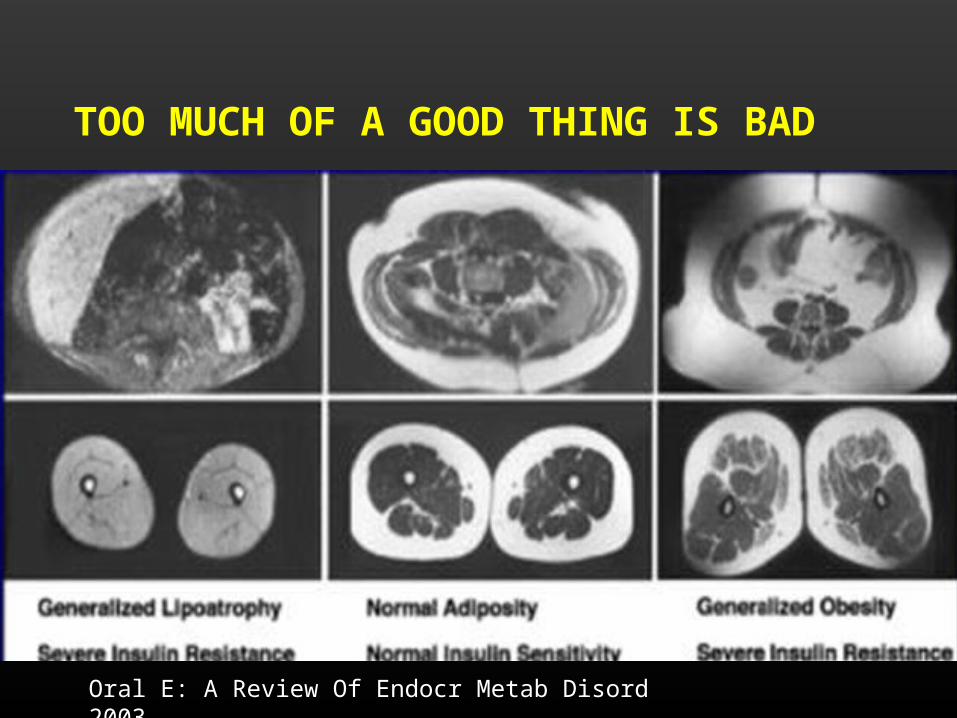
TOO MUCH OF A GOOD THING IS BAD
Oral E: A Review Of Endocr Metab Disord 2003

ANDROID (APPLE) VS. GYNOID (PEAR) OBESITY
AATributeTribute
to a to a PioneerPioneer
Jean Vague (1947)
Adapted from Vague J. Presse Med 1947; 30: 339–40
The amount of Visceral fat determines the risk of developing T2DM and
CVD

TOO MUCH FAT IN FAT TISSUE
• Functional consequences of regional differences
Large viscreal adipocytes:
• Enhanced secretion of FFA
• Lower capavity to stiore fat
• Altered adipokine secretion (leptin, adipnvectin, resistin, viscefatin)
• Inflammation (TNFIL6)
12
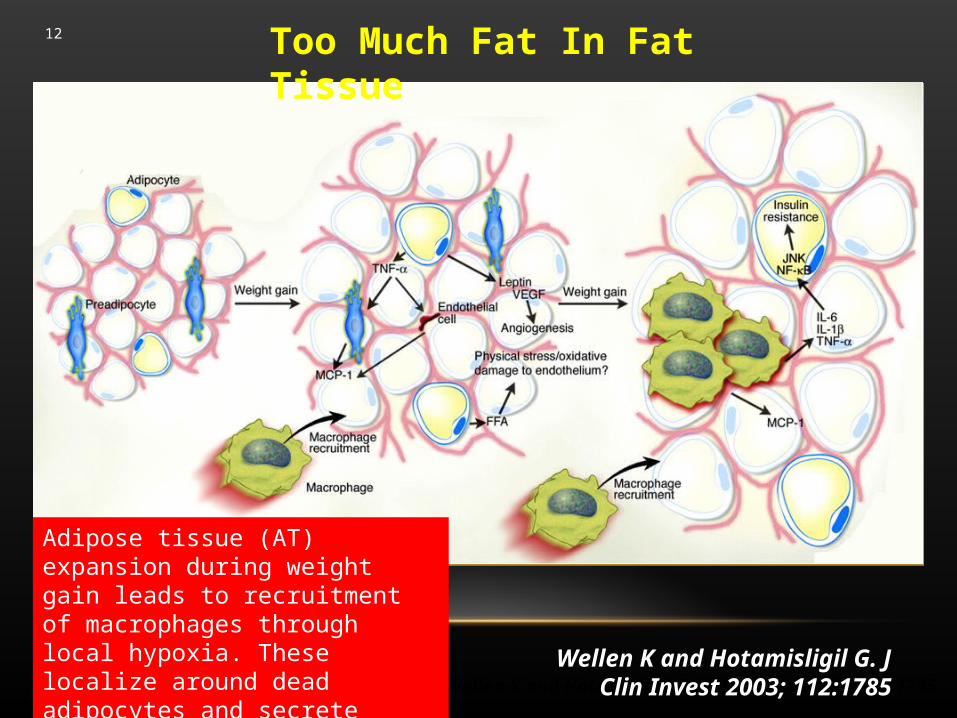
Wellen K and Hotamisligil G. J Clin Invest 2003; 112:1785Wellen K and Hotamisligil G. J Clin Invest 2003; 112:1785
Too Much Fat In Fat Tissue
Adipose tissue (AT) expansion during weight gain leads to recruitment of macrophages through local hypoxia. These localize around dead adipocytes and secrete inflammaiory cytokines

THE UGLY
FAT IN NON-FAT TISSUE

LIPOTOXICITY
• LIVER Non-alcoholic steatohepatitis
• MUSCLE
• Skeletal (insulin resistance, major impact because the muscle is the major site of insulin stimulated glucose disposal)
• Cardiac muscle cardiomyopathy
• Pancreatic beta cells defective insulin secretion
Florence (Italy),September 30 and October 1, 2005
15
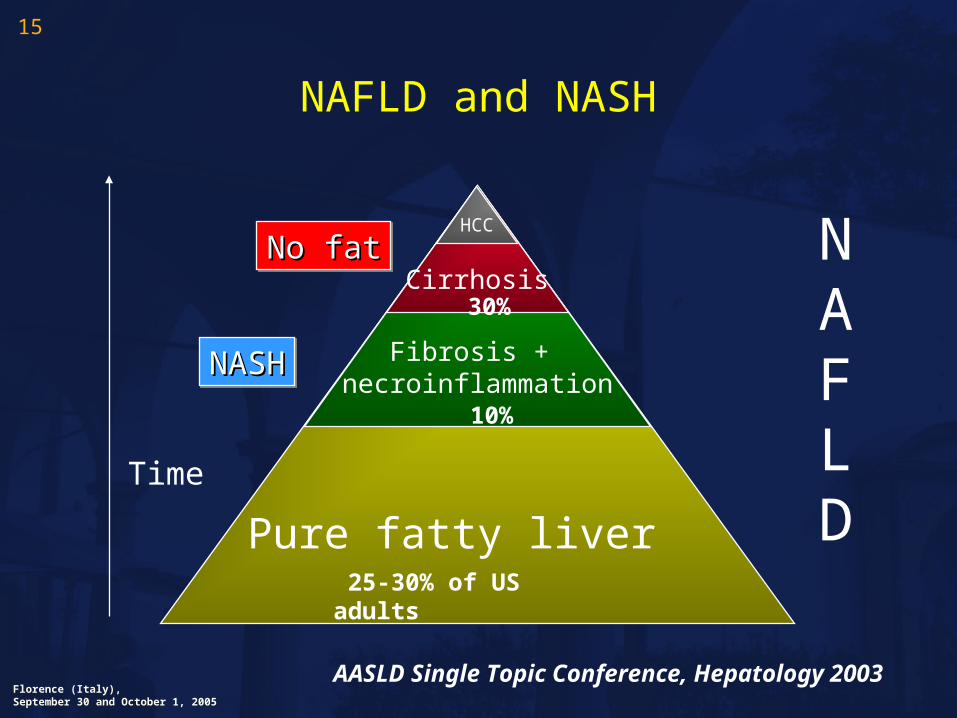
NAFLD and NASH
Pure fatty liver
HCC
Fibrosis + necroinflammation
CirrhosisNAFLD
NASHNASHNASHNASH
No fatNo fatNo fatNo fat
Time
25-30% of US adults
10%
30%
AASLD Single Topic Conference, Hepatology 2003
Florence (Italy),September 30 and October 1, 2005
16
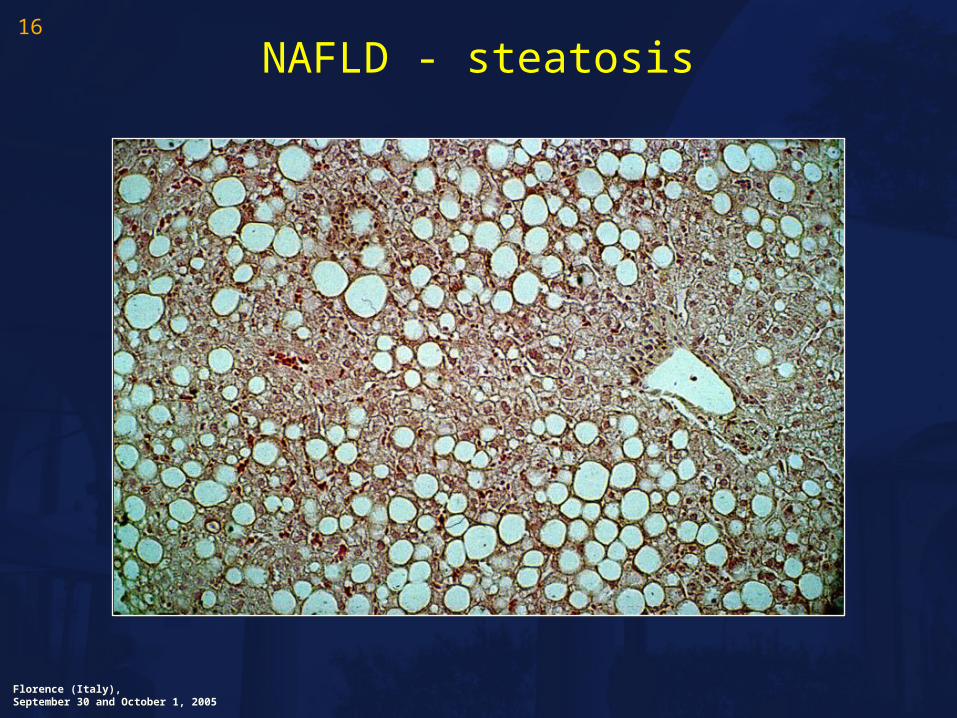
NAFLD - steatosis
Florence (Italy),September 30 and October 1, 2005
17
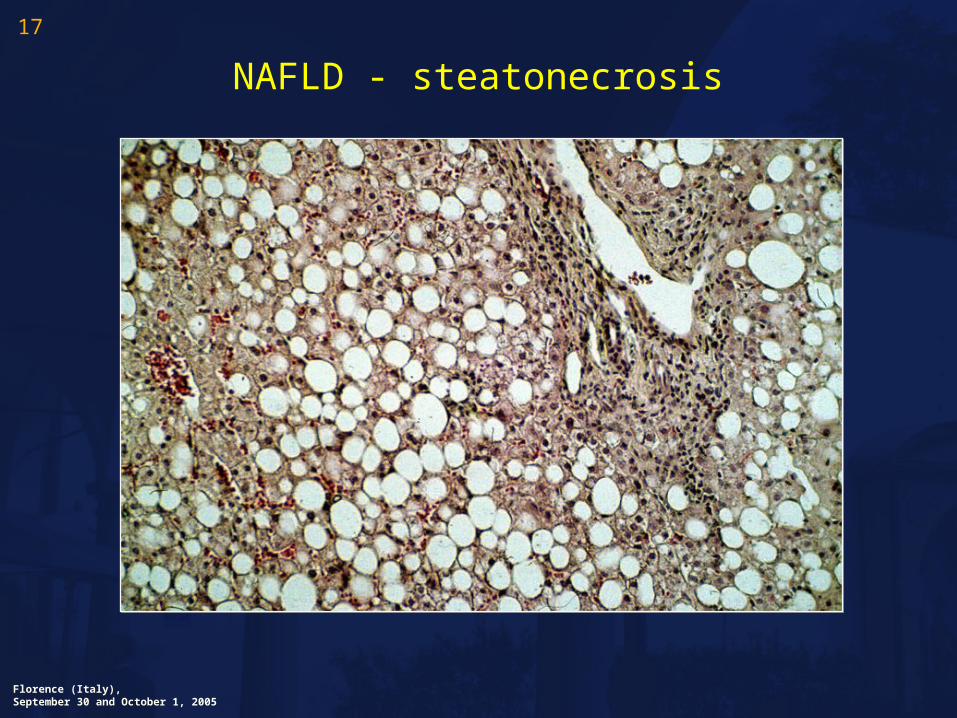
NAFLD - steatonecrosis
DIAGNOSIS OF NAFLD & NASH• Clinical findings
• Few clinical symptoms (upper right quadrant discomfort)
• Requires a high degree of clinical suspicion
• Laboratory
• May be associated with elevation of liver transaminases (ALT>AST)
• May NOT be associated with an elevation of ALT/AST
• Imaging
• U/S: ( echogenicity) 65-80% sensitivity for NAFLD
• Magnetic imaging streptoscopy
• Gold standard
• Very precise and reproducible measure of liver fat
• Restricted to research setting
• Liver biopsy: only way to make a diagnosis of NASH
19
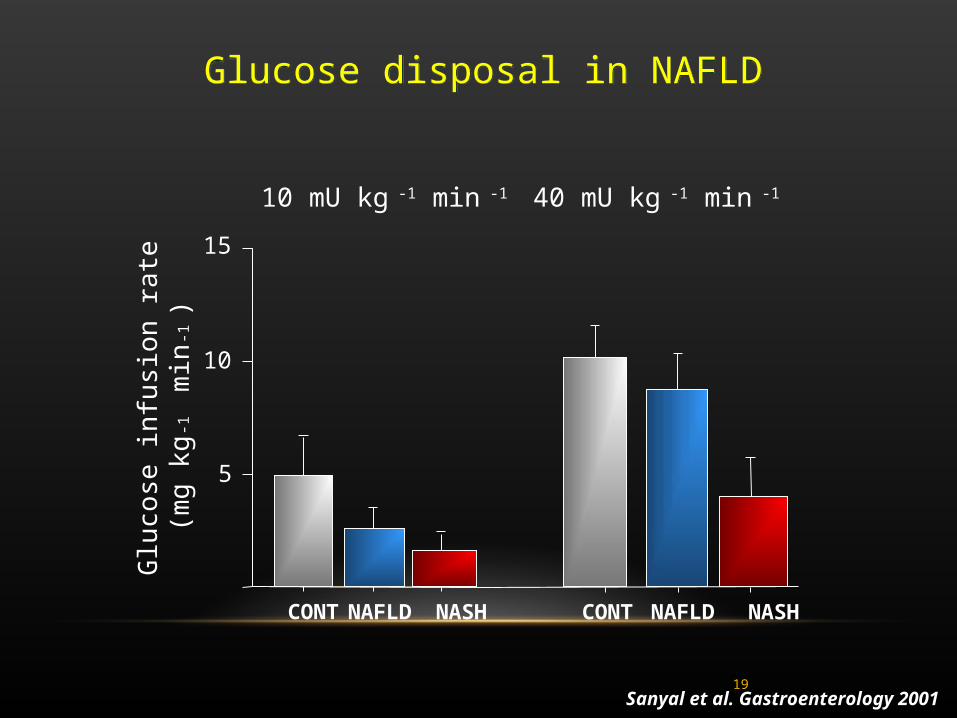
Glucose disposal in NAFLDGlucose disposal in NAFLD
Sanyal et al. Gastroenterology 2001
5
10
15
CONT NAFLD NASH
Glu
cose
infu
sio
n ra
te(m
g kg
-1
min
-1)
CONT NAFLD NASH
10 mU kg -1 min -1 40 mU kg -1 min -1
Fat in the liver is inversely related to
insulin sensitivity
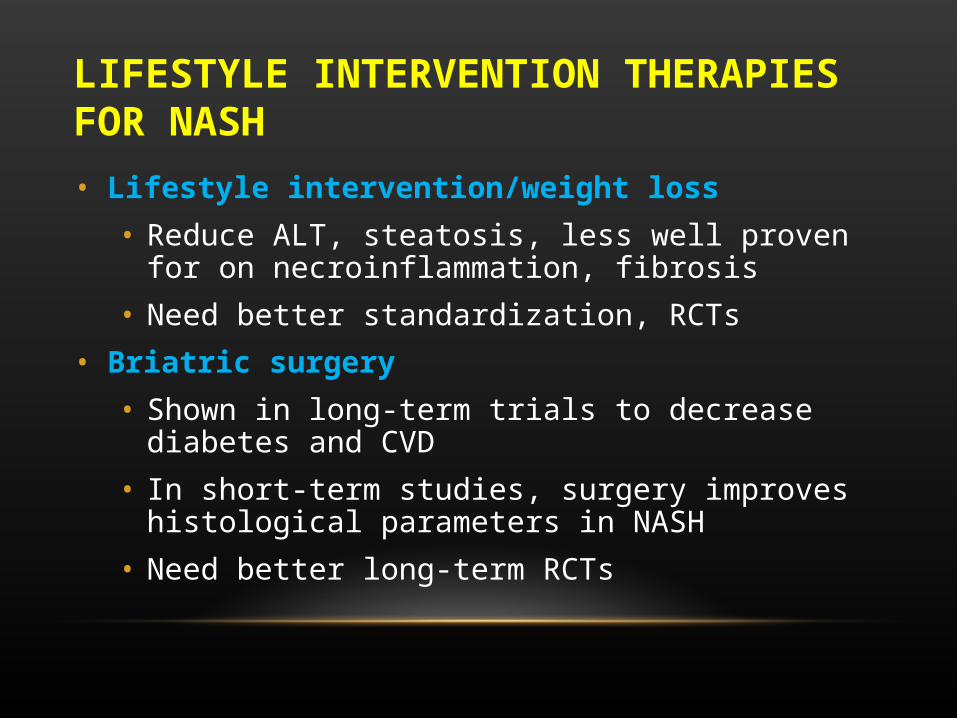
LIFESTYLE INTERVENTION THERAPIES FOR NASH
• Lifestyle intervention/weight loss
• Reduce ALT, steatosis, less well proven for on necroinflammation, fibrosis
• Need better standardization, RCTs
• Briatric surgery
• Shown in long-term trials to decrease diabetes and CVD
• In short-term studies, surgery improves histological parameters in NASH
• Need better long-term RCTs
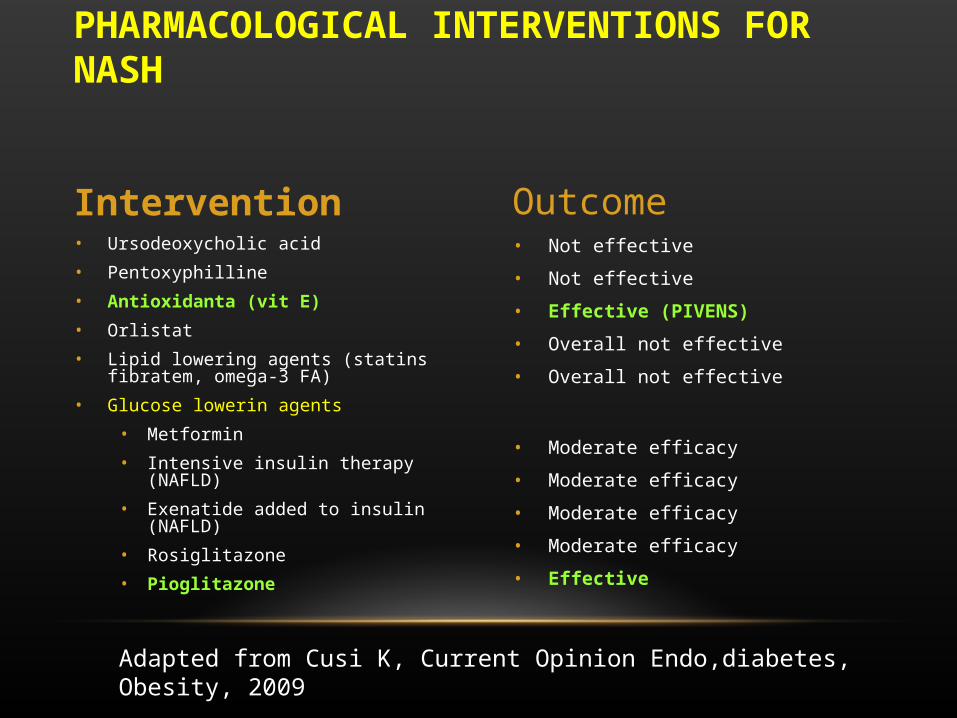
• Not effective
• Not effective
• Effective (PIVENS)
• Overall not effective
• Overall not effective
• Moderate efficacy
• Moderate efficacy
• Moderate efficacy
• Moderate efficacy
• Effective
• Ursodeoxycholic acid
• Pentoxyphilline
• Antioxidanta (vit E)
• Orlistat
• Lipid lowering agents (statins fibratem, omega-3 FA)
• Glucose lowerin agents
• Metformin
• Intensive insulin therapy (NAFLD)
• Exenatide added to insulin (NAFLD)
• Rosiglitazone
• Pioglitazone
PHARMACOLOGICAL INTERVENTIONS FOR NASH
Intervention Outcome
Adapted from Cusi K, Current Opinion Endo,diabetes, Obesity, 2009


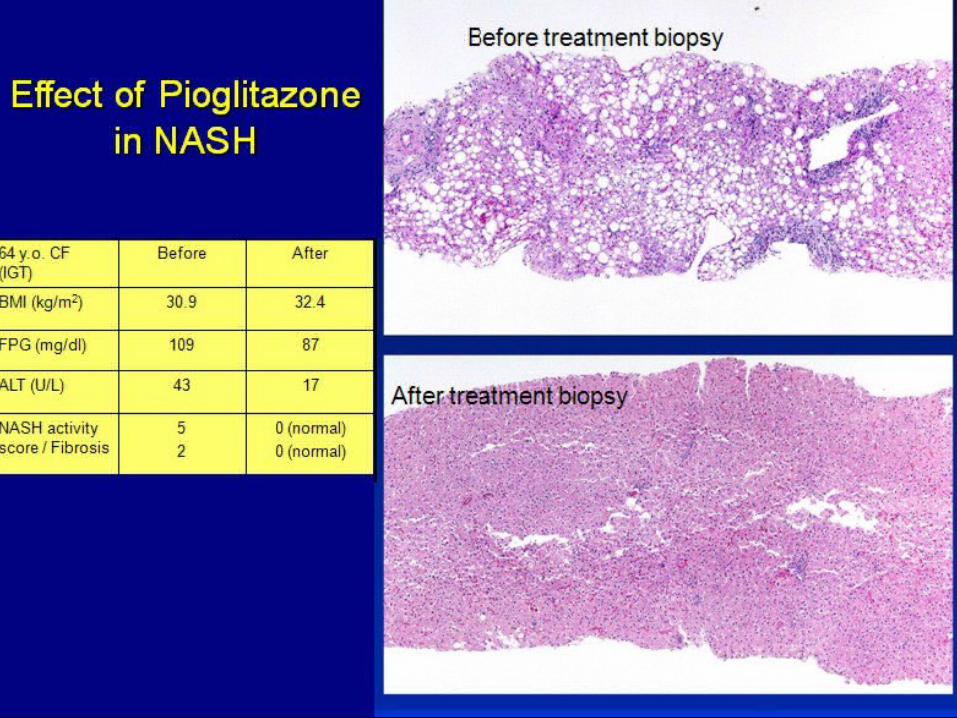

EFFECT OF VTAMIN E, PIOGLITAZONE OR PLACEBO IN PATIENTS WITH NASH
• PIVENS, NEJM, 2010. (247 non DM patients divided in 3 gps)
• Primary endpoint reached in
• 43% on vit E (p<0.01)
• 34% with PIO, 30 mg/d (<0.04)
• 18% with PBO
• Resolution NASH PIO 47%, vit E, 36%
• Similar response for low dose PIO and vitamin E
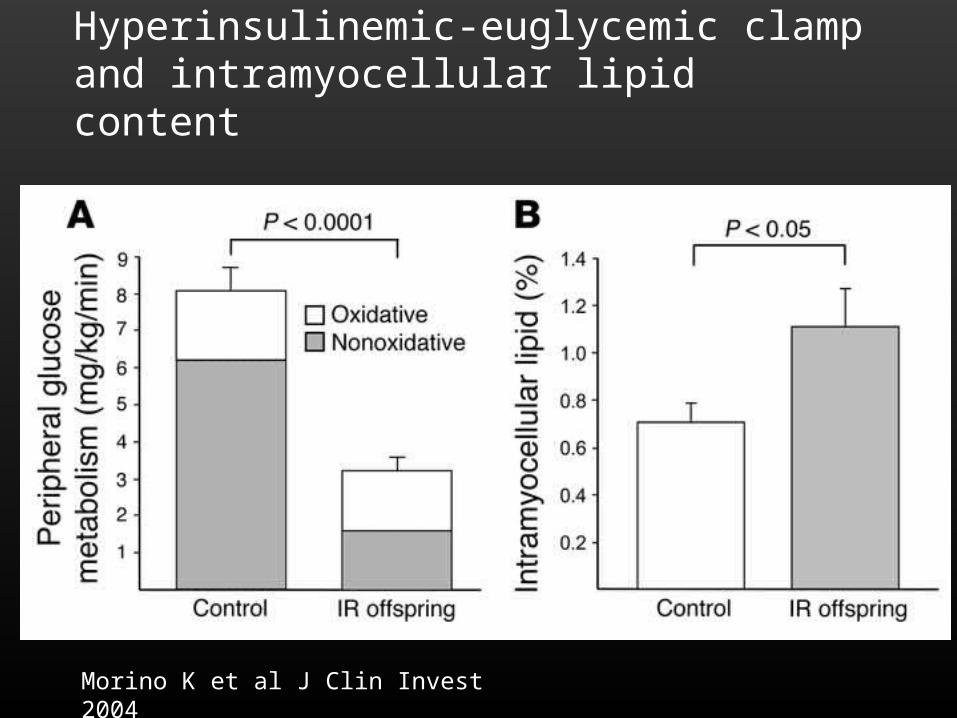
LIPOTOXICITY: SKELETAL MUSCLEHyperinsulinemic-euglycemic clamp and intramyocellular lipid content
Morino K et al J Clin Invest 2004
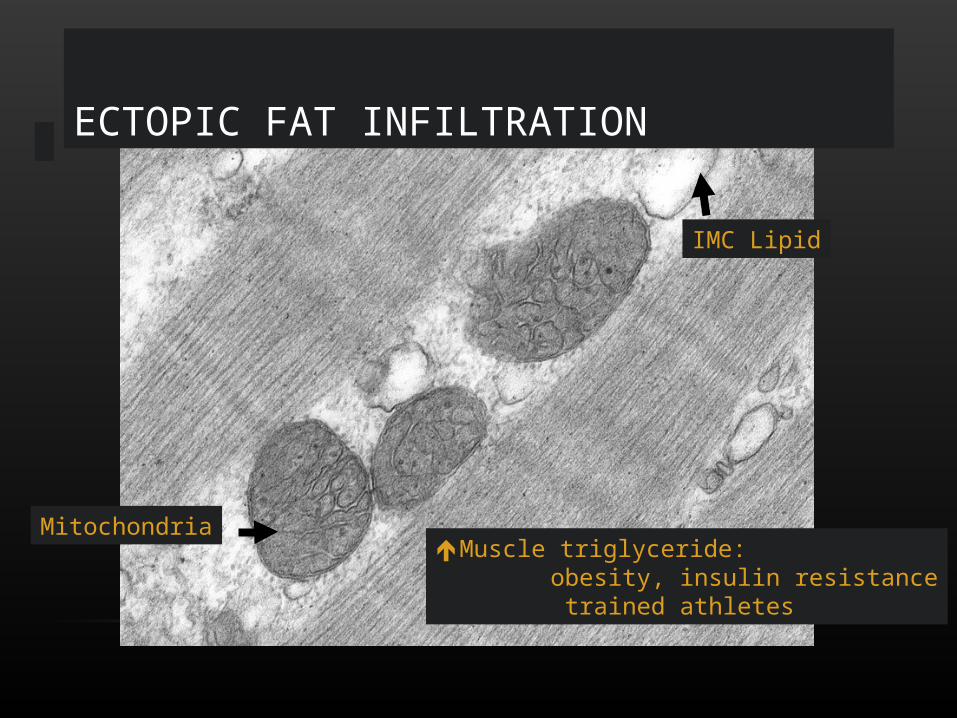
Mitochondria
IMC Lipid
ECTOPIC FAT INFILTRATION
Muscle triglyceride: obesity, insulin resistance trained athletes
31
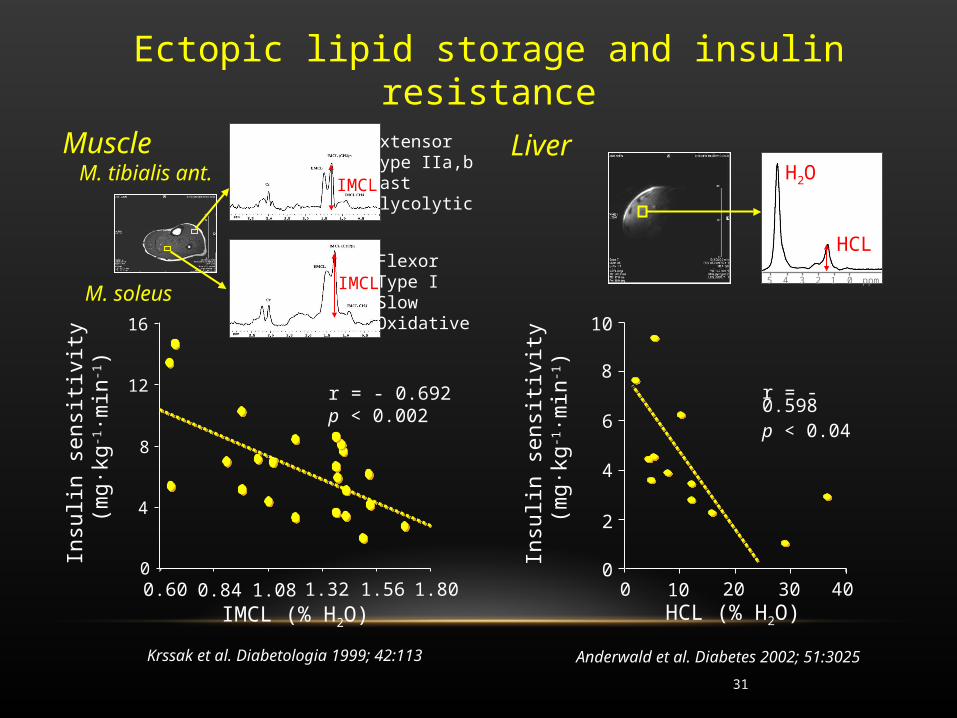
Ectopic lipid storage and insulin resistance
IMCL (% H2O)
0
8
12
16
0.60
4
r = - 0.692p < 0.002
0.84 1.08 1.32 1.56 1.80
Insu
lin s
ensi
tivity
(m
g·kg
-1·m
in-1)
Muscle M. tibialis ant.
M. soleus
IMCL
IMCL
Anderwald et al. Diabetes 2002; 51:3025
0
2
4
6
8
10
0 10 20 30 40
Insu
lin s
ensi
tivity
(m
g·kg
-1·m
in-1)
HCL (% H2O)
r = - 0.598p < 0.04
H2O
HCL
5 4 3 2 1 0 ppm
Liver
Krssak et al. Diabetologia 1999; 42:113
ExtensorType IIa,b FastGlycolytic
FlexorType ISlow Oxidative
32
MUSCLE FAT AND INSULIN RESISTANCESUMMARY
• Muscle lipids correlate variably with insulin resistance (IR) depending on nutritional and excercise status.
• Increased availability of free fatty acids inhibits insulin signalling by activating PKC/NFB and serine phosphorylation of IRS-1. Consequently, FFA decrease glucose transport and induce IR.
• Impaired lipid oxidation is required to raise intracellular availability of FFA and IMCL in obesity.
• Reduced mitochondrial function is tightly associated with IR. Defective muscle ATP synthesis might be responsible for hereditary IR or result from increased availability of FFA in acquired (nutritional/obesity induced) forms of IR.

LIPOTOXICITY: CARDIAC MUSCLE
Zhou Y-T et al Proc National Acad Science 2000
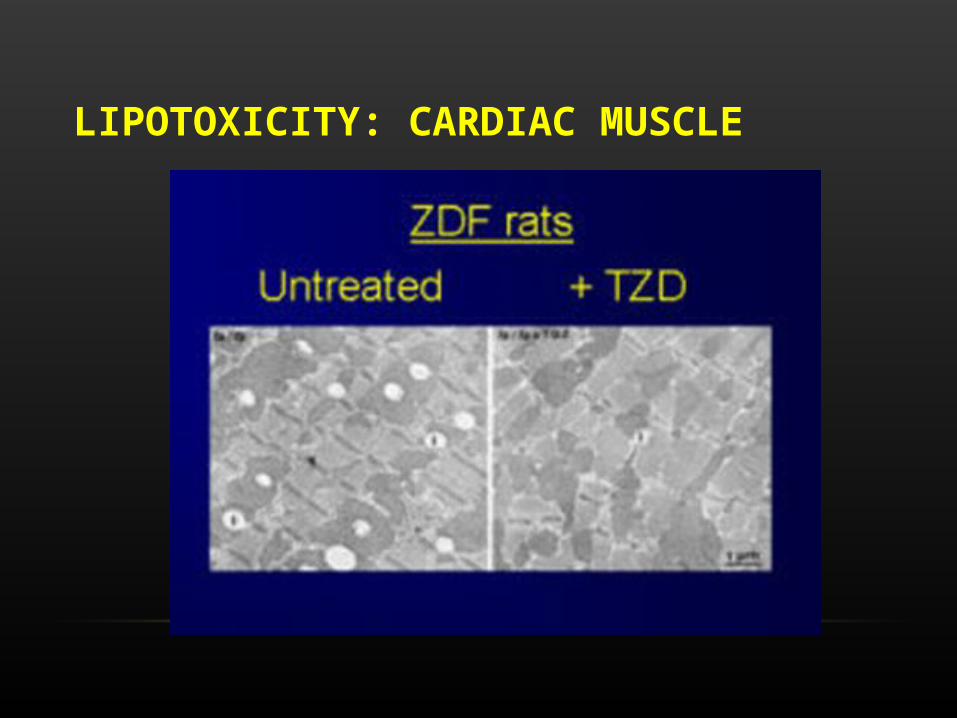
LIPOTOXICITY: CARDIAC MUSCLE

EXCESS FAT IN THE PANCREATIC ISLETS
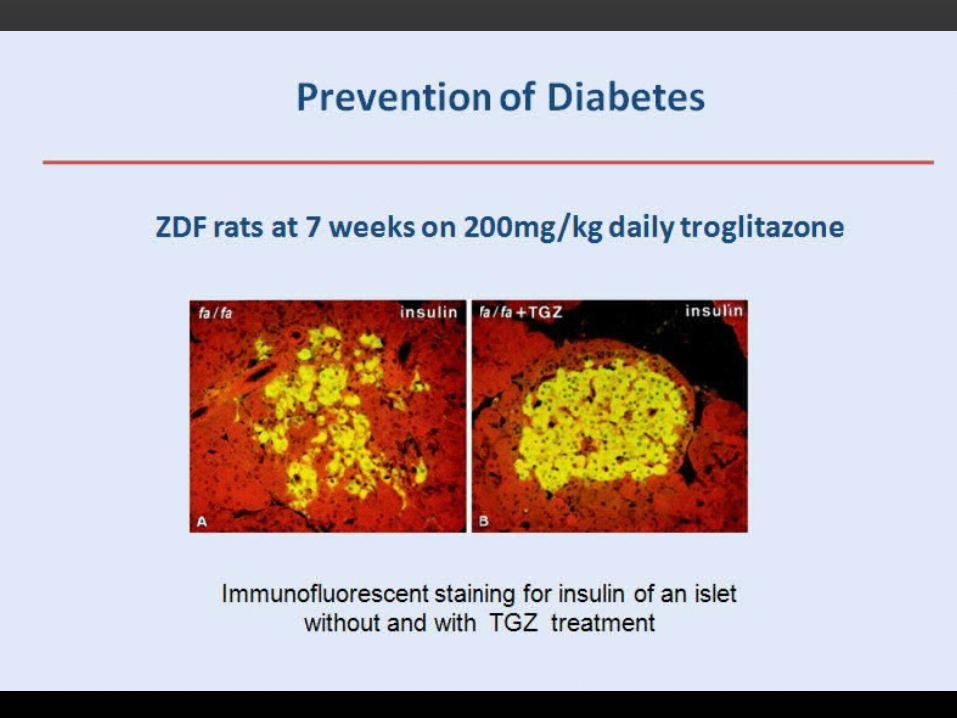
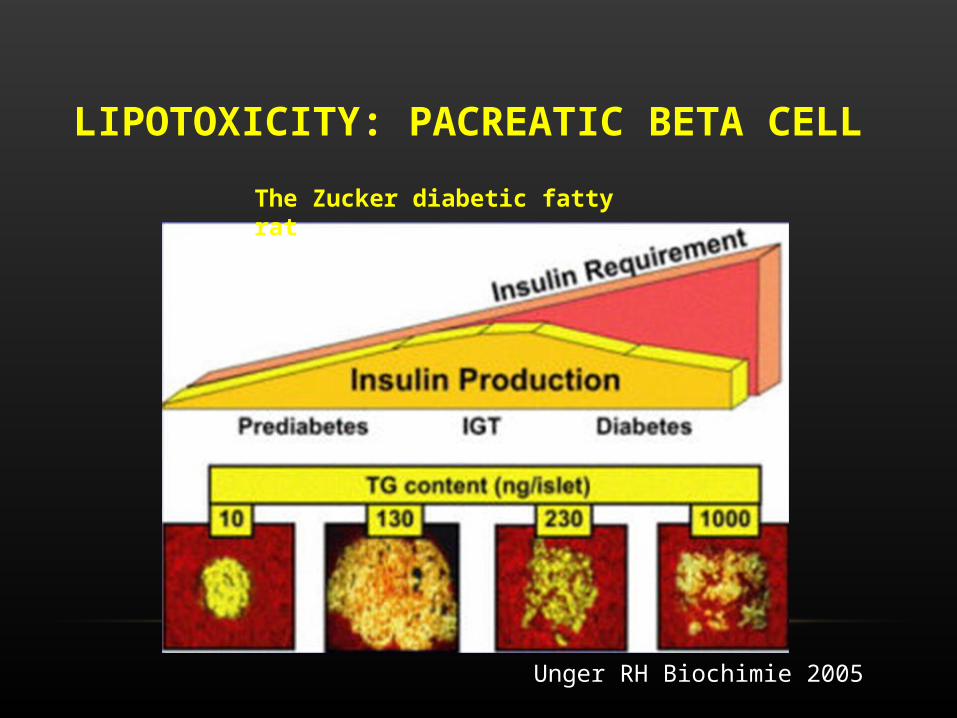
LIPOTOXICITY: PACREATIC BETA CELL
Unger RH Biochimie 2005
The Zucker diabetic fatty rat
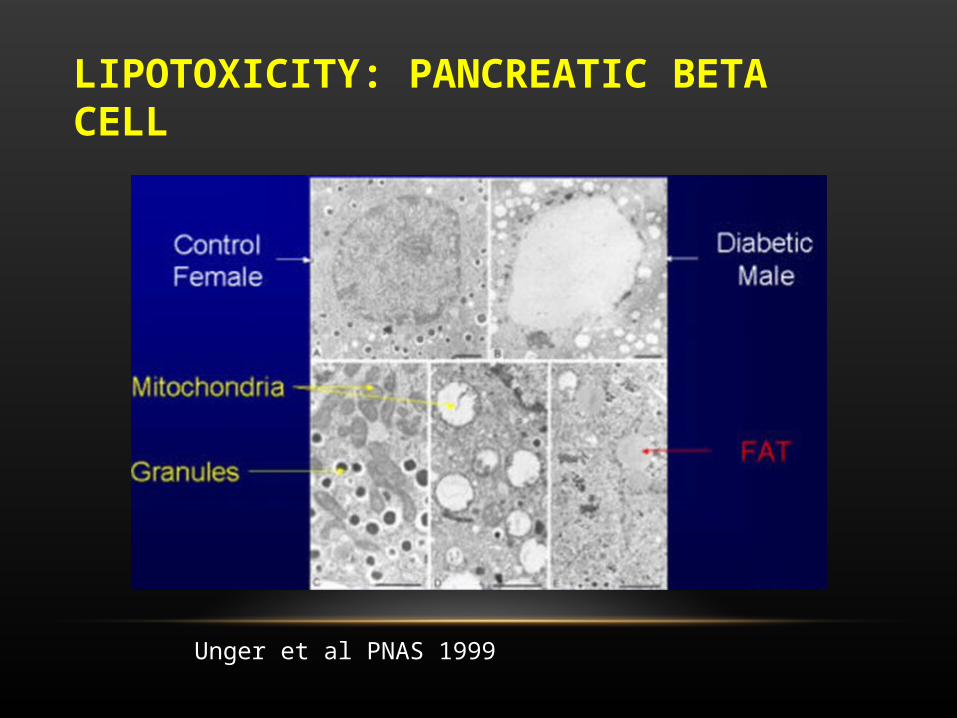
LIPOTOXICITY: PANCREATIC BETA CELL
Unger et al PNAS 1999
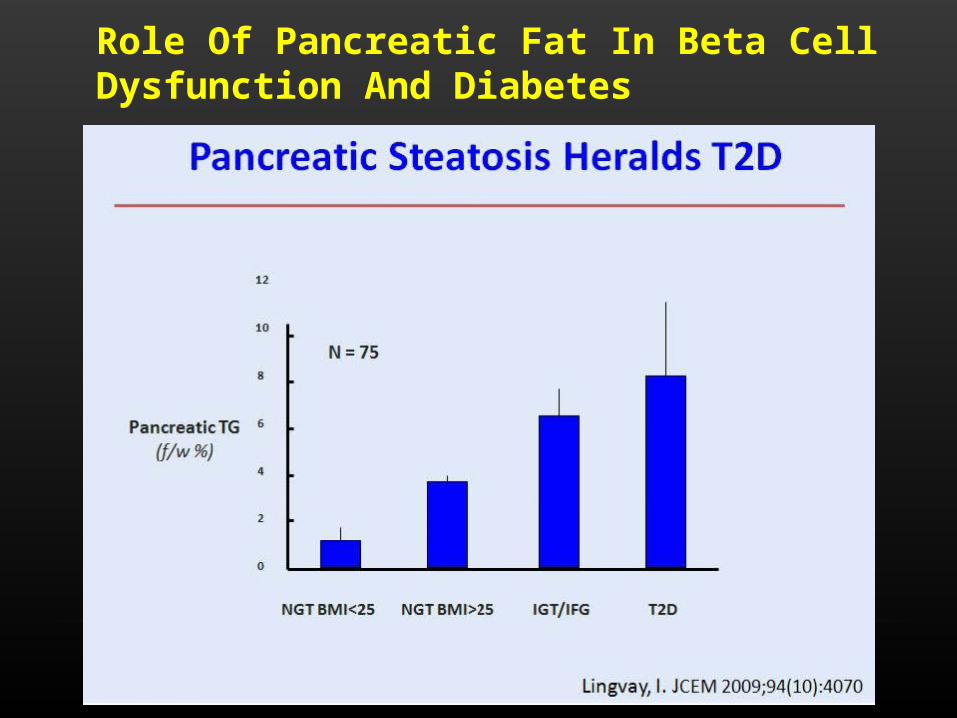
Role Of Pancreatic Fat In Beta Cell Dysfunction And Diabetes
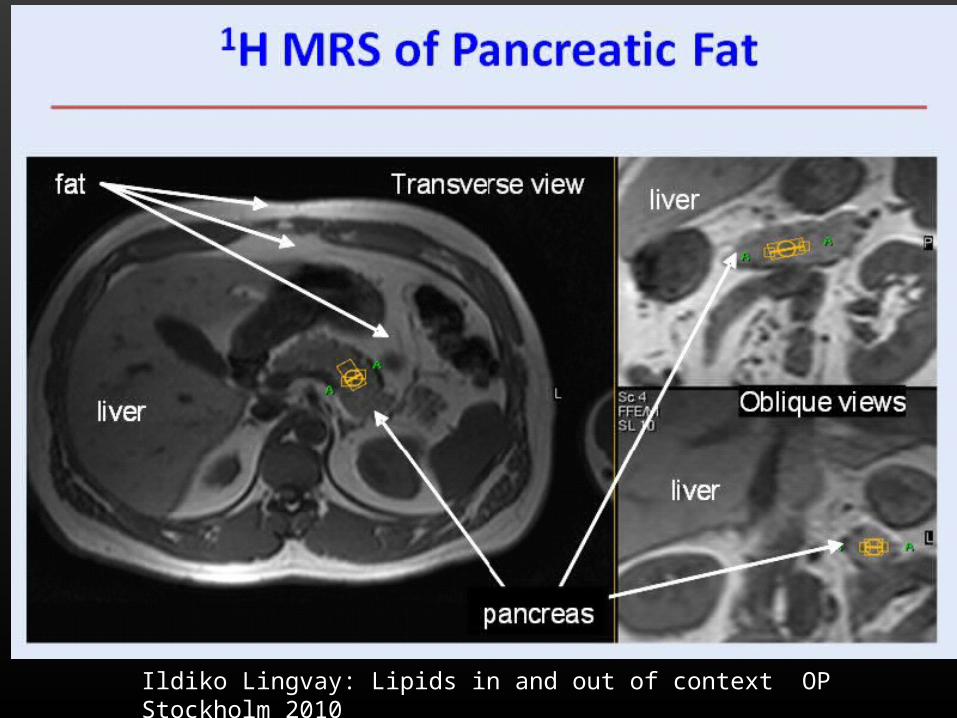
Ildiko Lingvay: Lipids in and out of context OP Stockholm 2010
LIPOTOXICITY: MECHANISMS
•The hallmark of lipotoxicity is the accumulation of fat in non-fat tissue
•But is fat the cause, or merely a marker?
THE PUZZLE OF TRAINED ATHLETES
• Triglycerides accumulate in the muscle tissue of highly physically trained athletes, who demonstrate enhanced insulin sensitivity.
• It has been suggested that muscle triglyceride may not have adverse metabolic consequences in muscle that has the capacity for efficient lipid utilization
GLUCOLIPOTOXICITY• Either hyperglycemia alone or elevated circulating FFAs alone should not
be so detrimental to a cell
• When glucose levels alone are high, glucose is oxidized, and when FFAs alone are high, then they are oxidized instead of glucose.
• FFAs are elevated during fasting, but are not toxic to cells under this low glucose condition.
• When both glucose and FFA levels are high, FFA esters (FACoAs) are high, and cannot be oxidized because glucose-derived malonyl-CoA is also elevated.
• Excess Malonyl-CoA results from excessive glucose metabolism in hyperglycemic hyperinsulinemic diabetic patients
• (Malonyl Co A -->FA synthesis & FA oxidation)
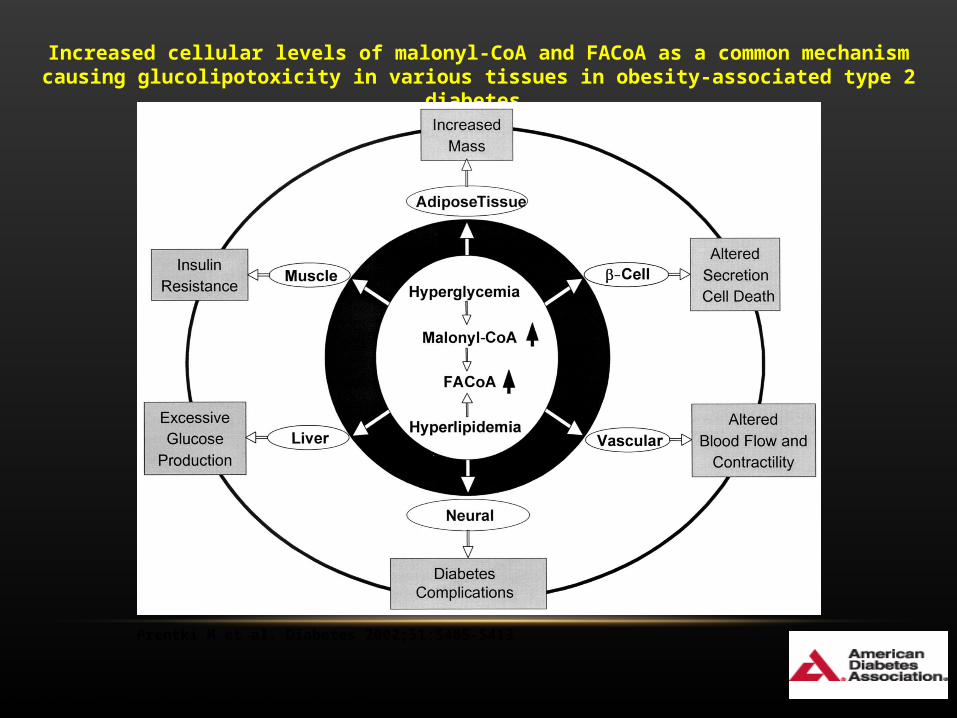
Increased cellular levels of malonyl-CoA and FACoA as a common mechanism causing glucolipotoxicity in various tissues in obesity-associated type 2 diabetes.
Prentki M et al. Diabetes 2002;51:S405-S413
Copyright © 2011 American Diabetes Association, Inc.
LIPOTOXICITY: MECHANISMS
• Triglyceride accumulation is a marker of fat overload
• The “lipotoxic” molecules are not the triglycerides themselves but metabolites derived from fat, e.g., diglycerides, ceramide, etc…
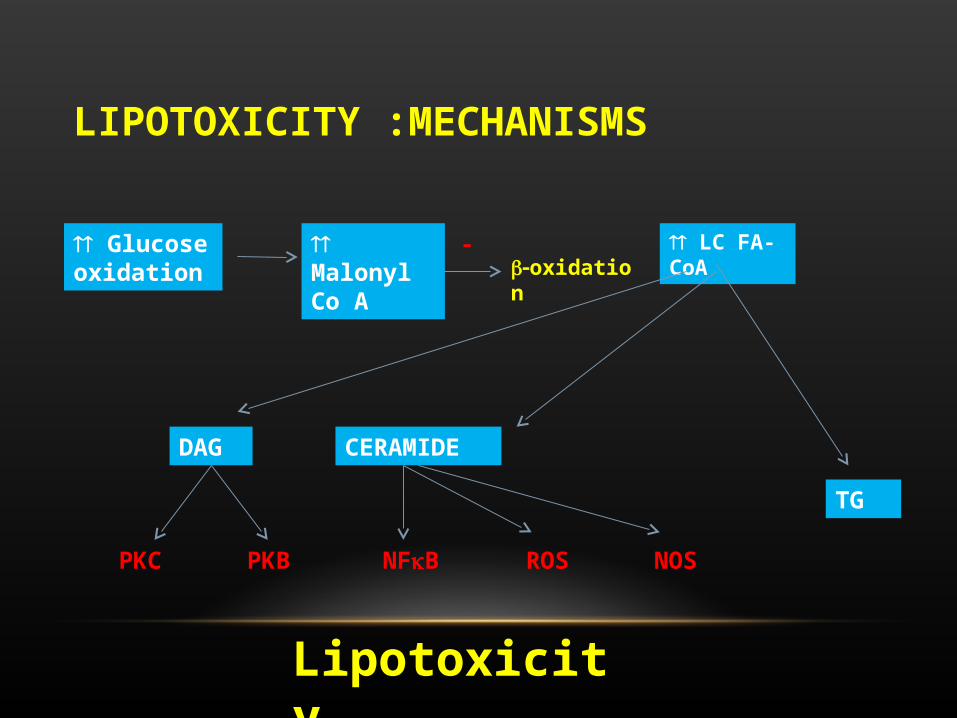
LIPOTOXICITY :MECHANISMS
Glucose oxidation
Malonyl Co A
-oxidation
LC FA-CoA
TG
DAG CERAMIDE
PKC PKB NFB ROS NOS
Lipotoxicity

47
Relationship between decrease in plasma FFA concentration and increase in acute insulin response following acipimox treatment
Paolisso et al. Diabetologia 1998; 41:1127
10 20 30 4020
30
40
50
60r = 0.64p<0.001
De
cre
ase
in p
las
ma
FF
A c
on
c. (
%)
Increase in acute insulin response (%)
LIPOTOXICITY IS IT TREATABLE?

DPP – DIABETES PREVENTION PROGRAM
• 3234 in 25 clinical centers with • BMI >24 (>22 in Asians)• IGT: FPG 95-125 mg/dl or 2HPPG 140-199 mg/dl Randomized to:
• Standard lifestyle + metformin• Standard lifestyle + placebo• Intensive Lifestyle Intervention: 7% weight reduction and 150 min
of exercise/wk• Primary outcome: progression to DM on annual OGTT or
semiannual FPG 126 mg/dl or 2HPPG200 mg/dl
The DPP Research Group. NEJM 2002; 346: 393–403

0 1 2 3 4
0
10
20
30
40
Years from randomizationYears from randomization
Cu
mu
lativ
e in
cid
enc
e (
%)
Cu
mu
lativ
e in
cid
enc
e (
%)
Placebo (n=1082)Placebo (n=1082)Metformin (n=1073, p<0.001 vs. PlaceboMetformin (n=1073, p<0.001 vs. Placebo))Lifestyle (n=1079, p<0.001 vs. Metformin, p<0.001 vs. PlaceboLifestyle (n=1079, p<0.001 vs. Metformin, p<0.001 vs. Placebo))
Incidence of diabetesIncidence of diabetes
Risk reductionRisk reduction31% by metformin31% by metformin58% by lifestyle58% by lifestyle
The DPP Research Group. NEJM 2002; 346: 393–403
LIPOTOXICITY IS IT TREATABLE?
• Tuomelehto NEJM, 2001
• FINNISH DIABETES PRVENTION STUDY GROUP
• 522 subjects with IGT randomized to a control group and an intervention group with 5% weight loss and 30 minutes of exercise daily
• Risk of diabetes reduced by 58%

A CENTRAL ROLE FOR AMP KINASE
• Highly sensitive metabolic sensor
• Ubiquitously expressed
• Modulates the activity of numerous proteins and metabolic pathways

LIPOTOXICITY IS IT TREATABLE?
Exercise Leptin Adiponectin TZD Metformin
AMPK
Malonyl CoA LC CoA FA oxidation FA esterifiication Ceramidesynthesis
Lipolysis
Glucose transport
NFB Oxidative stress
Adapted from Rudermam and Pentki, Nature Reviews, Drug Discovery, 2004
CONCLUSION I
• Fat is good but too much of a good thing is bad
• Too much fat in fat tissue is bad especially in visceral adipose depots
• Lipotoxicity affects many tissues
• Skeletal muscle insulin resistance
• Cardiac muscle cardiomyopathy
• Liver NASH and insulin resistance
• Pancreatic beta cell defective insulin secretion ( in the presence of concomitant hyperglycemia)
CONCLUSION II
• Ectopic accumulation of fat is a marker but probably not a mechanism of lipotoxicity
• Non-oxidative lipid metabolites affect a number of signaling pathways and tissue function that underlie the mechanisms of lipotoxicity
• Shifting lipid metabolism toward oxidation may represent a viable therapeutic option
• AMPK plays a central role in metabolic sensing and is an attractive therapeutic target
No comment

Thank You