ui-fhs desk reviewmpffs6apl64314hd71fbb11y-wpengine.netdna-ssl.com/wp-content/... · web viewthe...
TRANSCRIPT
UI-FHS DESK REVIEW ANDFIRST PHASE STAKEHOLDER MAPPING
Universal Immunization through Improving Family Health Services (UI-FHS) is managed by JSI Research & Training Institute, Inc. and is funded by the Bill & Melinda Gates Foundation. JSI works in collaboration with its implementing
2012JSI Research &Training Institute, Inc.
Rahel T. Gizaw

partner the Center for Vaccine Development of the University of Maryland School of Medicine (CVD) and the Ethiopian Health and Nutrition Research Institute (EHNRI).
ContentsAcronyms 3I. INTRODUCTION, PURPOSE AND OVERVIEW OF THE EXERCISE
5II. MAJOR HEALTH AND EPI STRATEGIES
6III. RI PERFORMANCE, TRENDS, AND DISCUSSION
14IV. EPI RELATED RECOMMENDATIONS WITH SUMMARY OF CONTEXT BEHIND RECOMMENDATION 20V. INTRODUCTION, PURPOSE, OVERVIEW OF STAKEHOLDER MAPPING EXERCISE
22VI. RI, MNCH AND QI WORK IN ETHIOPIA
23VII. HEALTH AND MNCH WORK 36VIII. QUALITY IMPROVEMENT WORK IN ETHIOPIA 45
2 | P a g e

AcronymsAEFI Adverse Events Following ImmunizationAIDS Acquired Immune Deficiency SyndromeANC Antenatal CareART Antiretroviral TherapyARISE African Routine Immunization System EssentialsBPR Business Process Reengineering BSC Balanced ScorecardCAHW Community Animal Health WorkerCBRHA Community based reproductive health agentsCHD Child Health DaycMYP Comprehensive Multi – Year PlanCSO Civil Society OrganizationsCVD Center for Vaccine Development at the University of MarylandDPT Diphtheria-Pertussis-Tetanus VaccineEDHS Ethiopian Demographic Health SurveyEDSSO Economic Development Social Service OfficeEEOS Extended Enhanced Outreach StrategyEHNRI Ethiopian Health and Nutrition Research InstituteENA Essential Nutrition ActionsEOS Enhanced Outreach Strategy EPI Expanded Program on ImmunizationERIA Enhanced Routine Immunization ActivitiesESHE Essential Services for Health in Ethiopia FLHW Front Line Health WorkerFMoH Federal Ministry of Health GAVI Global Alliance for Vaccine and ImmunizationGoE Government of EthiopiaHDA Health Development Army HEP Health Extension ProgramHEWs Health Extension WorkersHIV Human Immunodeficiency VirusHMIS Health Management Information SystemHSDP Health Sector Development PlanICC Inter Agency Coordinating CommitteeIEC Information Education CommunicationIIP Immunization in PracticeIMCI Integrated Management of Childhood IllnessIMNCI Integrated Management of Neonatal and Childhood Illnesses IPC Inter Personal CommunicationITN Insecticide Treated NetsJRF Joint Reporting FormJSI John Snow Inc.LAFP Long Acting Family PlanningLLINs Long Lasting Insecticide treated netsMDG Millennium Development GoalMNCH Maternal, Newborn and Child HealthNID National Immunization DaysPAB Protection at BirthPCQI Participatory Community Quality Improvement
3 | P a g e
PHCU Primary Health Care UnitQI Quality ImprovementRCS Record Check Study RED Reaching Every DistrictRHB Regional Health BureauRI Routine immunization SIA Supplemental Immunization ActivitiesSNNP Southern Nations and Nationalities PeoplesSNIDs Sub – National Immunization Days TBA Traditional Birth AttendantTOT Training of TrainersTT Tetanus ToxoidUNICEF United Nations Children’s FundUSAID United States Agency for International DevelopmentVAS Vitamin A SupplementationVCHW Volunteer Community Health WorkerVPDs Vaccine preventable diseasesWFP World food programWHO World Health OrganizationWoRHO Woreda Health Office
4 | P a g e
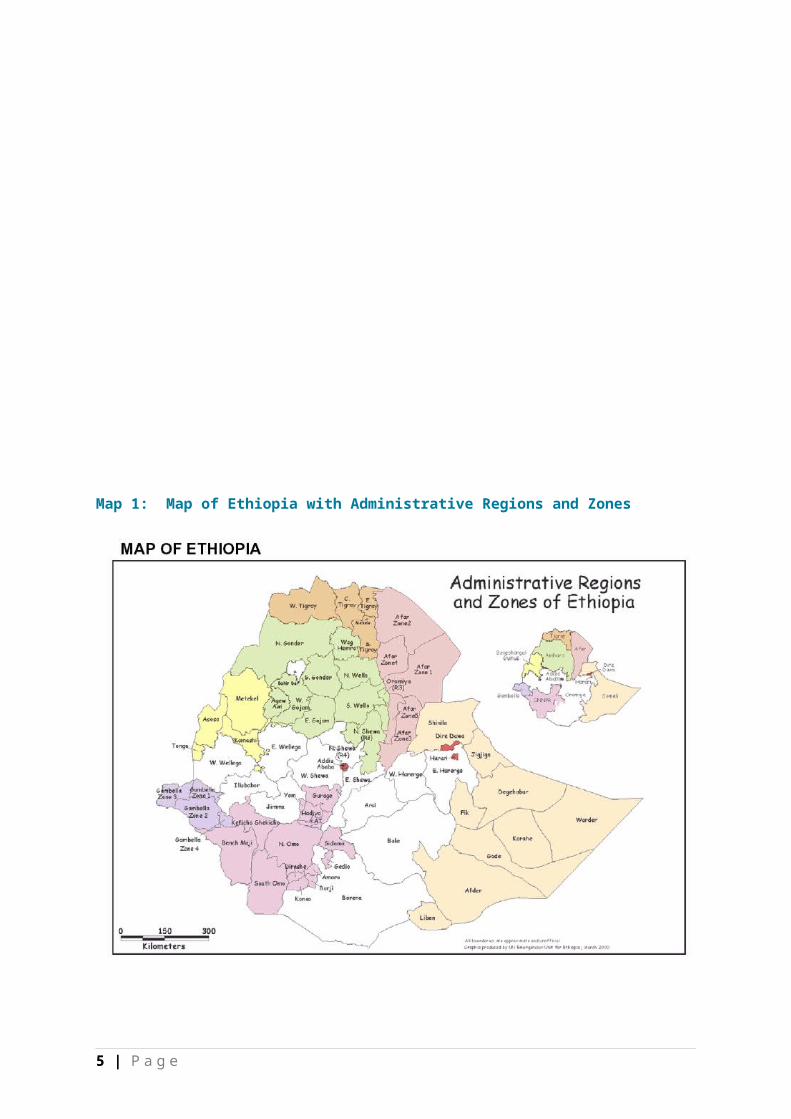
Map 1: Map of Ethiopia with Administrative Regions and Zones
I. INTRODUCTION, PURPOSE AND OVERVIEW OF THE EXERCISE
For more than a decade, Ethiopia has undergone a period of deliberate, rapid and intense change in the health sector, with much of the change at the community level. These investments have led to sizable improvements to the health status of its population. Under-five mortality, in particular, has seen a dramatic drop – falling by 28% in the past five years alone, from 123 per 1,000 live births to 88 per 1,000 live births (EDHS 2011). Nonetheless, mortality numbers remain high. The current level of under-five mortality translates to 500,000 deaths annually and ranks 6th in the world in number of deaths. It is believed that 72% of these deaths are due vaccine preventable diseases (22).
In recognition of this, JSI Research & Training Institute, Inc. has designed and been awarded a 2.5 years learning grant from Bill & Melinda Gates Foundation to undertake a learning project on universal immunization. The grant will study whether improving family health services will enhance universal immunization.
5 | P a g e

The project seeks to develop evidence to inform the Federal Ministry of Health (FMoH) on – whether and how to pursue nationwide universal child immunization in Ethiopia; whether universal immunization should be with family health approaches; and what it will take to do so effectively, affordably and sustainably.
The project will build upon local understanding to introduce improved routine immunization (RI) practices in three agrarian and pastoral learning woredas, build capacity, and translate lessons for sustained immunization systems to inform policies and practices. The learning woredas are: Assaieta in Afar, Hintalo Wajerate woreda in Tigray, and Arbegona in SNNP Regional States. These woredas were selected to represent rural and pastoralist operating environments in Ethiopia. It also includes one woreda (Hintalo Wajerate) with good immunization performance and one woreda (Arbegona)that has experienced repeated measles outbreaks. The project will be undertaken in close collaboration with the FMoH, the Center for Vaccine Development at the University of Maryland (CVD), the Ethiopian Health and Nutrition Research Institute (EHNRI) and other key stakeholders working in immunization in Ethiopia.
Understanding the existing health strategies, programs, best practices, and stakeholders is critical to inform the design of nationwide universal child immunization in Ethiopia if it is to be integrated with family health approaches. To do so, a desk review and stakeholder mapping exercise was commissioned. The consultant reviewed both published and unpublished documents as well as conducted interviews over a two week period. The desk review, in particular, builds on the National RI Situation Analysis done by ARISE project and consists of a report that provides an overview of major health, expanded program on immunization (EPI) and Maternal, Neonatal, and Child Health (MNCH) strategies implemented over the past decade. The desk review summarizes these efforts and provides an overview of the results. The desk review also examines performance and progress over time in EPI and presents a trend interpretation based on documents reviewed. The stakeholder mapping exercise presents work currently being done in the area of RI, MNCH, and general quality improvement in health with an emphasis on the “who, what, and where” of the health sector actors. It also highlights best practices achieved by these actors and whether these best practices have been sustained.
II. MAJOR HEALTH AND EPI STRATEGIES
Ethiopia is the 2nd most populous country in Africa with a population of 83 million people. It has one of the largest and most topographically challenging land masses in Africa and is home to a great diversity of cultures, all of which presents a challenge to the provision of immunization and other health services. The main causes of child death in Ethiopia are pneumonia 28%; neonatal conditions 25%, diarrhea 20%, malaria 20%, measles (4%) and HIV 1%. Of the
6 | P a g e
vaccine preventable diseases (VPDs), measles, in particular, remains an important cause of childhood illnesses and death in Ethiopia. Every year 18,800 children die from measles and 100% of these deaths are preventable with 99% of intervention coverage (36).
The Government of Ethiopia (GoE) launched its EPI in 1980 with the objective of increasing immunization coverage by 10% annually and reaching 100% by 1990 (8). Since then, the GoE has launched further initiatives to improve immunization coverage, including immunization campaigns as well as delivering vaccinations through static health facilities, outreach services, and mobile teams.
The first polio supplemental immunization activity was conducted in 1996 in nine selected cities followed by full National Immunization Days (NIDs) and Sub-National Immunization Days (SNIDs) annually from 1997 to 2005. As a result, the number of children immunized with OPV increased from about 7.5 million in 1997 to 15.5 million during the 2005 NIDs. Ethiopia achieved Acute Flaccid Paralysis (AFP) surveillance certification level in 2004 and had been polio-free from November 2006 to April 2008. In April 2008, however, two cases and the wild type one polio virus were detected in Gambella Regional State. From May to June, emergency supplementary immunization activities (SIAs) were conducted in Gambella Regional State and surrounding zones, targeting more than half a million children under the age of five years in 52 woredas. Additional campaigns were conducted over a wider geographical area covering the Ethio- Sudan and Ethio-Kenya borders, targeting 2.2 million children under five. A total of seven polio SIAs were conducted with coverage above 90% .The administrative coverage was 102% and Record Check Study (RCS) 96%. The percent of zero doses were 20.5% and 1.2 % by administrative coverage and RCS respectively (8). Since then, however, the risk of a new polio outbreak has increased because of drought and conflicts in the horn of Africa. The drought, in particular, has resulted in a shortage of funding in the 1st quarter of 2011, and led to the scale back and delay of SIAs in Ethiopia, Kenya, Uganda, and Eretria. The effect of the drought on their immunity will also make children more susceptible to polio infection (30).
The 2002-2003-2004 phased measles campaign reached over 28 million children aged between 6 months and 15 years. Although the follow up measles campaign has been initiated at the end of 2005 and its implementation resulted in significant reduction of measles cases, outbreaks were identified in almost all regions of the country prior and after the implementation of the campaign which raised a question on the quality and potency of vaccine (30). In April 2004, the Enhanced Outreach Strategy (EOS) was introduced with support from UNICEF and the World Food Program (WFP). This served as a transition from intensive campaigns to routine immunizations until the Health Extension Program (HEP) becomes ready to deliver vaccines. The EOS targeted seven million children living in 325 drought-prone/food-insecure woredas, it aimed at offering a set of high impact child survival interventions twice a year (Vitamin-A Supplementation (VAS), de-worming, and EPI mobilization. In some districts
7 | P a g e

EOS included measles immunization for children under 2 years of age who haven’t yet been immunized for measles – so called “missed opportunity” children),Tetanus Toxoid (TT) SIAs, and Insecticide Treated Nets ( ITN). In addition, the nutritional status of children and pregnant women were assessed. Whenever possible, other interventions such as hygiene education, Long Lasting Insecticide treated Nets (LLINs) distribution, and Information Education Communication (IEC) were also included. Overall, EOS was found to be an effective strategy for delivering supplemental immunization (26). Extended Enhanced Outreach Strategy (EEOS) and other EOS-based programs have been launched since 2005 targeting districts less affected by food insecurity.
Map 2: Enhanced Outreach Strategy (EOS) woredas Source: Yodit Sahlemariam, Integration of child survival interventions in Ethiopia to reach MDG, 3rd Global immunization Meeting19-21 February 2008
There was an increase in national DPT3 coverage since the introduction of Reaching Every District (RED) phased approach in 2003/04 (1). Thirteen low performing zones (out of the country total of 85) were selected for the first phase -- the RED approach was later scaled up to all districts. This approach aimed to reach every child in every district with immunization services by prioritizing hard to reach children and devising specific strategies to address the specific barriers (operational, staff motivation, capacity building) to delivering immunization services in the district. The approach includes the following components – 1) re-establishing fixed and outreach vaccination services; 2) supportive supervision, 3) strengthening linkages between community and service; and 4) monitoring for improving immunization service performance. Although the RED implementation has led to improving DTP3 and measles coverage, the evaluation of RED approach conducted in July 2007 indicated that major gaps remained in all the components of RED approach.
8 | P a g e

This included inadequate integrated and refresher training, managerial capacity gaps, lack of cold chain technicians to ensure maintenance of the system, inadequate inventory of vaccine/materials and poor stock management, infrequent supervisory visits, inadequate tracking of defaulters, and lack of reporting that disaggregates by services provided by fixed, outreach and mobile outlets(12).
In 2003, FMoH launched a new health care plan the “Accelerated Expansion of Primary Health Care Coverage” through a comprehensive HEP designed to provide universal primary health care coverage by 2009. The HEP is designed to focus on four areas—disease prevention; family health; environmental hygiene and sanitation; and health education and communication. Its main approach is transferring skills and knowledge in health to households as a mechanism of improving health outcomes. Health Extension workers (HEWs) are supposed to spend 75% of their time visiting families in their homes, performing outreach activities, and spend the remaining 25% at the health post providing routine immunization services, injectable contraceptives, and other preventive health and educational services. HEWs are also meant to work in close collaboration with voluntary health workers such as the community-based reproductive health agents (CBRHA) who provide reproductive health and family planning outreach at the household level. The HEP is the most significant (and in many areas, the only) effort to bring health services to the remote and rural areas of Ethiopia.
In 2004, the FMoH of Ethiopia endorsed the National Strategy for Child Survival. This strategy focuses on a number of priority, high-impact interventions, that will be scaled-up to increase access and use of child health services.
In October 2006, the government adopted a national commodity supply system to ensure that vaccines, essential drugs, and other health commodities are available to the public health facilities.
The World Health Organization (WHO) introduced Integrated Management of Childhood Illnesses (IMCI) globally in the mid-1990s as a holistic protocol to improve the quality of care for sick children that can be administered by frontline health workers (FLHWs). In particular, it focuses on improving immunization, nutrition counseling, and referrals during sick child visits. To meet Ethiopia’s specific needs, Essential Service for Health in Ethiopia (ESHE I) led the adaptation and simplification of the standard international IMCI protocol. Given Ethiopia’s reliance on HEWs as FLHWs, IMCI was considered overly technical for the majority of Ethiopia’s FLHWs. In addition, neonatal conditions that account for nearly 40% of under-five deaths in Ethiopia and had not been included in the international IMCI protocols. ESHE worked closely with the FMoH, WHO, UNICEF, and other stakeholders to adapt the training materials and the new Integrated Management of Neonatal and Childhood Illness (IMNCI) protocol was launched in 2007. The IMNCI approach set new
9 | P a g e
directions and standards for child care in Ethiopia by designing a strategy to improve the management of childhood illness. It links preventive and curative services so that programs such as immunization, nutrition, and control of malaria, prevention and control of acute respiratory infection, diarrhea, HIV/AIDS are implemented in an integrated manner (33). In this fashion, IMNCI was an early approach that linked family health/neonatal services with RI at community and health facility level.
Despite the increase in DPT3 immunization coverage through the implementation above mentioned strategies, the emerging regions (Afar, Benishangul-Gumez, Gambella, Somali) lagged behind their immunization targets and the risk of outbreaks remains high. To address this problem, the GoE introduced Enhanced Routine Immunization Activities (ERIA) in 2009. This strategy is designed to strengthen the existing routine immunization programs by addressing barriers to high immunization coverage in the four emerging regions and zones with large number of unvaccinated children. ERIA components include advocacy visits, micro planning and registration with community participation, immunization in practice/cold chain/vaccine management training, and supportive supervision. ERIA has since been scaled up in other regions.
The key intervention of ERIA is the use of immunization days – 2-3 days/month in each kebele to provide immunization to the community by HEWs. Immunization days also provide an opportunity for HEWs to trace unvaccinated children who did not appear during immunization against a pre-implementation registration list. The strategy also utilizes kebele administrators and community workers for social mobilization to increase demand for vaccination in the community (10). To serve mobile populations in pastoralist areas, mobile health teams were established in 2007 in Somali and Afar regional states. The mobile health teams include nurses, HEWs, health officers, and kebele administrators to provide health and other services, including EPI. In 2009, mobile health team strategy has been scaled up to all four emerging regions with the aim to reach unvaccinated children in mobile and hard to reach communities with four visits a year(8).
In 2009 the Comprehensive Multi-Year Plan (cMYP 2010-2014), a strategic EPI plan, was developed within the framework of Global Immunization Vision and Strategies’. The cMYP was developed with the GIVS’ four strategic themes and in line with the health sector development program (HSDP IV).
Building on the recent successes of the HEP program, the FMoH launched a new Health Development Army (HDA). The HDA is organized as a network with one model family per five households; the model family approach encourages families who are lagging behind to adopt safe health practices. HDA hoped to
10 | P a g e
improve the scale up of best practices and improve community ownership and mobilizing families.
In addition to the above mentioned strategies, the GoE has also been developing crosscutting tools to improve the overall performance and quality of the health system. In 2007, FMoH introduce Business Process Reengineering (BPR), a nationwide reform implemented as a part of the government’s civil service reform. BPR was intended to create a fundamental rethinking and redesign of business processes to achieve improvement in performance measures such as cost, quality, service and speed. In the process, innovative ideas and benchmarked best practices were introduced, leading to new processes and revised organizational structures, eventually forming eight core processes and five support processes (1).
Following BPR, FMoH introduced the Balanced Scorecard (BSC) tool, a strategic planning and performance tool that links the day-to-day work of employees with the overall goals of organization and health sector in general. This tool also helps to improve performance of the sector by keeping track of its performance from four performance lenses (capacity building, internal process, financial and community perspectives) (21).
Other reforms also in motion include health facilities revenue retention and utilization; facility governance reforms systematization of fee waivers for those who cannot afford to pay; exemption of MNCH services; outsourcing of non-clinical services; and the establishment of private wings with the objective of strengthening the supply side and delivery quality health services.
In addition, to address the financial barriers to access health services, the GoE has recently initiated pilots of Community Based Health Insurance for informal sector and Social Health Insurance for the formal sector. Lastly, The FMoH has developed comprehensive human resource for health strategy and incentive packages are underway to address the critical human resource shortage in the country.
Table 1: Major Strategies of the past decade relating to the health system and EPI (2001-2011)
A. Health Strategies summaryWhat: strategy/approach & description
When: years
Where: to woreda level if possible
Who: lead agencies
Health Extension Program (HEP): In 2003 FMoH launched the “Accelerated Expansion of Primary Health care coverage” through Health
2004 -present
Nationwide FMoH supported by GAVI, UNICEF, WHO,USAID and many other partners
11 | P a g e

Extension Program designed to provide universal coverage by 2009. HEP packages include health promotion, preventive and some curative services both at the health posts and house to house visits.
Expected Outcome: Achieving universal health coverage
Integrated Management of Neonatal and Childhood illness (IMNCI): community and facility based IMNCI was launched in 2007 as a strategy to improve the management of childhood illness, linking preventive and curative services so that programs such as immunization, nutrition, and control of malaria, prevention and treatment of Acute Respiratory Infection (ARI), diarrhea, HIV/AIDS are implemented in an integrated manner.
Outcome: Reduced death, illness and disability, improved growth and development among children <5
2007 -present
Nationwide FMoH, ESHE led. Close collaboration with FMoH, WHO, UNICEF and other stakeholders to adapt and simplify standard international IMCI approach
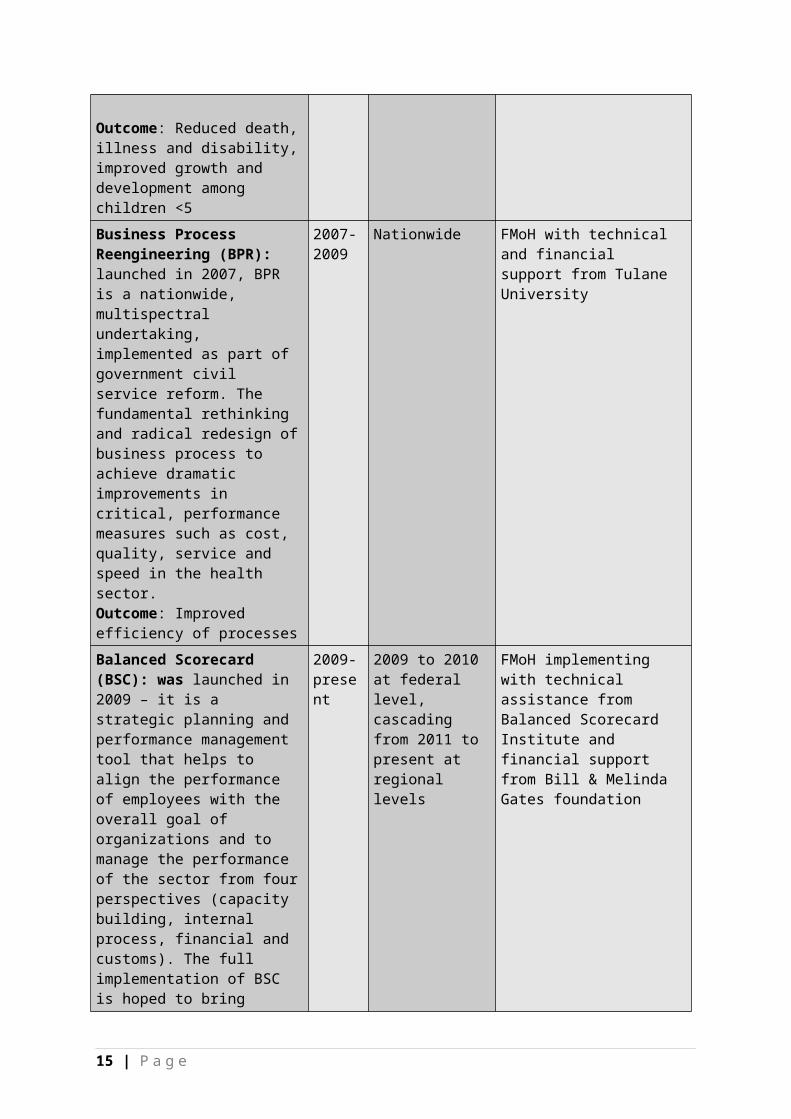
Business Process Reengineering (BPR): launched in 2007, BPR is a nationwide, multispectral undertaking, implemented as part of government civil service reform. The fundamental rethinking and radical redesign of business process to achieve dramatic improvements in critical, performance measures such as cost, quality, service and speed
2007-2009
Nationwide FMoH with technical and financial support from Tulane University
12 | P a g e

in the health sector.Outcome: Improved efficiency of processesBalanced Scorecard (BSC): was launched in 2009 – it is a strategic planning and performance management tool that helps to align the performance of employees with the overall goal of organizations and to manage the performance of the sector from four perspectives (capacity building, internal process, financial and customs). The full implementation of BSC is hoped to bring performance improvement and alignment in the health sector in Ethiopia.
Expected Outcome: Improved performance and alignment of day to day work of employees with the overall goal of the sector.
2009- present
2009 to 2010 at federal level, cascading from 2011 to present at regional levels
FMoH implementing with technical assistance from Balanced Scorecard Institute and financial support from Bill & Melinda Gates foundation
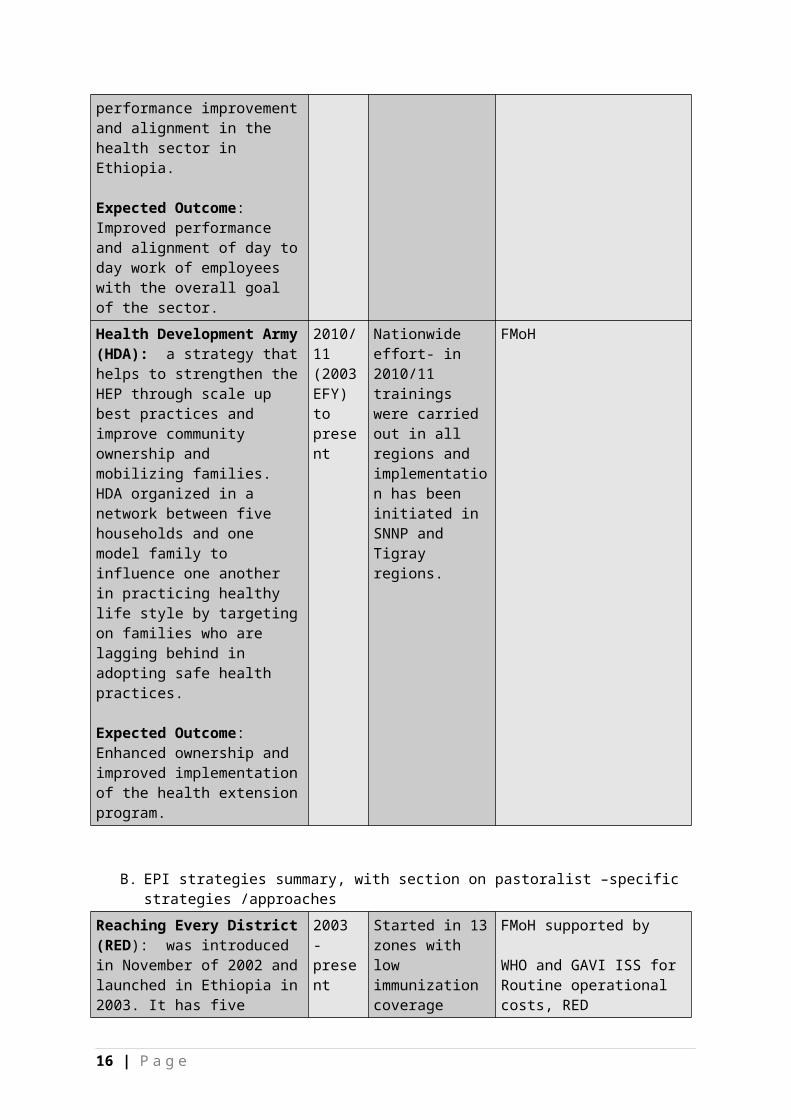
Health Development Army (HDA): a strategy that helps to strengthen the HEP through scale up best practices and improve community ownership and mobilizing families. HDA organized in a network between five households and one model family to influence one another in practicing healthy life style by targeting on families who are lagging behind in adopting safe health practices.
Expected Outcome: Enhanced ownership and improved implementation of the health extension program.
2010/11 (2003 EFY) to present
Nationwide effort- in 2010/11 trainings were carried out in all regions and implementation has been initiated in SNNP and Tigray regions.
FMoH
13 | P a g e

B. EPI strategies summary, with section on pastoralist –specific strategies /approaches
Reaching Every District (RED): was introduced in November of 2002 and launched in Ethiopia in 2003. It has five components. These are re-establishment of regular outreach services; supportive supervision: on-site training; community links with service delivery; monitoring and use of data for action; better planning and management of human and financial resources.
Outcome: Improved capacity of districts to plan, budget and implement immunization services and enhanced community involvement and participation to achieve 80/80 goal.
2003 -present
Started in 13 zones with low immunization coverage later scaled up to all districts
FMoH supported by
WHO and GAVI ISS for Routine operational costs, RED orientation workshops,Trainings and RED Micro planning.
UNICEF, WHO and GAVI ISS -Social mobilization, Per diem, Fuel for Outreach, Kerosene for refrigerators, Maintenance of vehicles (cars and motorcycles)Electric consumption, Review meetings (per diem, stationary, venue, etc.), Advocacy and awareness raising.
IRISH AID for the purchase of motorcycles.
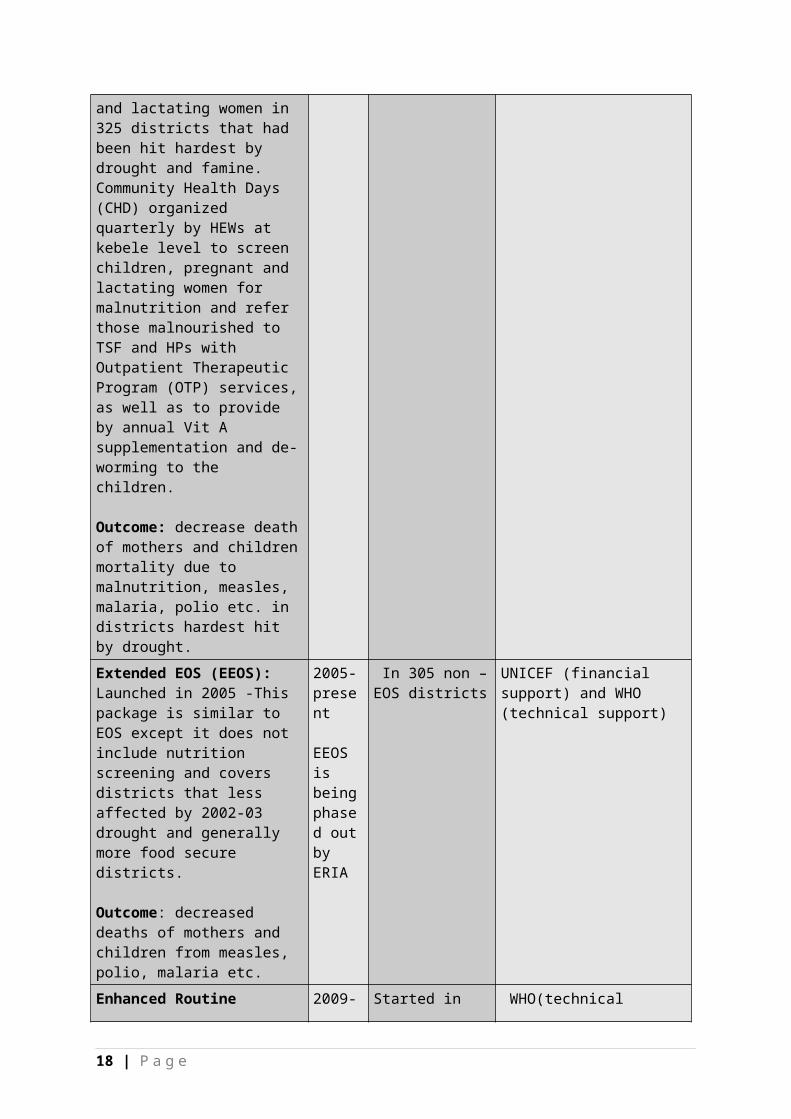
Enhanced Outreach Strategy (EOS): was launched in April 2004 as a bridge strategy to increase access and coverage of health services until the HEP become fully operational. The services include biannual (every six month) mass mobilizations to provide vitamin A supplementation, de-worming, nutrition screening and, in some woredas, vaccinations to children form 6-59 months old and pregnant and lactating women in 325 districts that had been hit hardest by drought and famine. Community Health Days (CHD) organized quarterly by HEWs at kebele level to screen
2004- presentEOS is being phased out by ERIA
325 drought-prone/food-insecure districts
FMoH, UNICEF, WHO and WFP
14 | P a g e
children, pregnant and lactating women for malnutrition and refer those malnourished to TSF and HPs with Outpatient Therapeutic Program (OTP) services, as well as to provide by annual Vit A supplementation and de-worming to the children.
Outcome: decrease death of mothers and children mortality due to malnutrition, measles, malaria, polio etc. in districts hardest hit by drought.Extended EOS (EEOS): Launched in 2005 -This package is similar to EOS except it does not include nutrition screening and covers districts that less affected by 2002-03 drought and generally more food secure districts.
Outcome: decreased deaths of mothers and children from measles, polio, malaria etc.
2005-present
EEOS is being phased out by ERIA
In 305 non – EOS districts
UNICEF (financial support) and WHO (technical support)
15 | P a g e
Enhanced Routine Immunization Activities (ERIA): was launched in June 2009 designed to strengthen the existing RI and reduce the number of unvaccinated children in the four emerging regions and zones with large number of unvaccinated children (>10,000) using the existing routine immunizations. ERIA components include advocacy visits, micro planning and registration of under one children by HEWs and community volunteers, IIP/ cold chain/vaccine management training, supportive supervision. Unimmunized children are immunized at specific immunization sites and dates conducted (2-3 days/month). HEWs later revisit the ones that did not get vaccinated during immunization days. The strategy also utilizes kebele administrators and community workers for social mobilization to increase demand for vaccination.
Expected outcome: The number of un vaccinated children will be reduced; immunization coverage especially in emerging regions will be improved; the capacity of Regions/Zones and their respective Woredas to implement quality EPI activities will be strengthened and the demand for immunization among communities will be increased.
2009- present
Started in Somali and Afar and later scaled up to four emerging and ERIA regions.
WHO(technical support) and UNICEF and GAVI(financial support)
16 | P a g e

Pastoralist specific strategies: What
When: years
Where: to woreda level if possible
Who: lead agencies
Mobile Health Team –In 2007 established in Somali and Afar regional states. The mobile health team includes (nurse, HEW, health officer, kebele administrators and other professionals) provide mobile health services including EPI and other services using transportation. Mobile Health Team has been scaled up to all four emerging regions since 2009 Mobile health team reach each village four times a year to reach unreached children in mobile and hard to reach community.
Outcome: The number of un vaccinated children will be reduced; improved immunization coverage and the demand for immunization among communities in pastoralist area will be increased.
2007 to present
. FMoH and RHBs with technical support from WHO and financial support from UNICEF
III. RI PERFORMANCE, TRENDS, AND DISCUSSIONThis graph (right) shows DTP1 and DTP3 vaccination coverage trend (diphtheria-tetanus-pertussis first and third doses, respectively) in Ethiopia from 1981 through 2010 (based on WHO/UNICEF estimates; updated July 2011). Massive external financial and technical support, mostly from UNICEF, throughout the 1980’s in pursuit of a 1990 global goal of universal childhood immunization resulted in rapid DTP3 coverage increases from less than 5% to 50% DTP3 by 1990. After
17 | P a g e
National DPT 1 & DPT 3 Coverage, 1981-2010
1990, donor funding declined and coverage dropped precipitously, a pattern similar to other countries with weak and underfunded health systems. Ethiopia, in particular, experienced a change in government in 1991. The associated instability also contributed to the decrease in immunization coverage.
Within several years, however, coverage returned to 1990 levels and beyond but stagnated through the late 1990s. A steady, but slow, increase could be seen in the past 9-10 years until the present time, reaching 86% for DTP3 in 2010 (based on WHO/UNICEF estimates; national reported data). The gap between DTP1 and DTP3 coverage (drop-out rate; see difference between magenta and blue lines in graph above) began to narrow starting in about 2002 with the availability of Immunization Services Support (ISS) funding from the Global Alliance for Vaccines and Immunization (GAVI) and the introduction of the Reaching Every District (RED) strategy (1). Lack of awareness, both for of the need for follow-up doses and of the follow-up locations/times, contributed to the high drop-out rate. Community mobilization and behavioral change efforts can therefore improve demand for follow-up vaccinations.(13) While DTP are not the only antigens of interest, it is indicative of the strength of the routine system to deliver successive vaccine doses of perceived good quality to a population which is prepared to receive them.
While Ethiopia’s boom and bust vaccination cycle in the late 1980’s and early 1990s provides a cautionary tale, it was not unique. The challenges in sustaining external vertical programs remain a cautionary tale that policy makers should take heed. (1)
Source1981
1990
1995
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
Official Country 3%49% 57%
42% 51%
51% 52% 66%
69% 72%
73% 81%
79% 86%
WHO/ UNICEF 3%49% 57%
56% 63%
59% 58% 68%
69% 72%
73% 81%
79% 86%
18 | P a g e
0102030405060708090
100DTP1DTP3
Source: WHO/UNICEF coverage estimates for 1980-2010, as of July 2011.

Table 2: National infant DTP3 coverage, 1980-2010(Official country, WHO/UNICEF and various survey estimates
Table 3: Demographic Health Survey data 2011
19 | P a g e
2000 DHS: 21%(x) 2005 DHS: 32% 2010 DHS : 37%
2011 DHS: 37%

Source TT PAB Penta 1 Penta 3 OPV3 MCV Basic Immunization
2011 DHS 48% 64% 37% 44% 56% 24%
Basic vaccination – BCG, measles and three doses each of DPT and polio vaccine excluding polio vaccine given at birth
Routine Immunization Coverage Trends: Ethiopia’s history of vaccination coverage (following Table) shows the general agreement on the one hand between the official reported coverage and the WHO/UNICEF estimate of coverage, and on the other hand the significant difference between that estimate and the Demographic and Health Survey (DHS) results from 2000, 2005 and 2010 (note: survey reflects estimated coverage 12-23 months prior to survey date). To add confidence to reported and surveyed coverage in light of these measurement variations, serological evidence of protection will be collected.
20 | P a g e

Map 3: Coverage Map of Zones 2007-2010 Source (2007 -2009) (1), and 2010(35)
National coverage estimates often mask sub-national differences in performance, this is an especially pressing concern given the geographic and ethnic diversity of Ethiopia. The maps above provide an illustration of the sub-national vaccine coverage change over time (2007-2010). Similar maps showing the numbers of unimmunized children, drop-out rates, vaccine stock outs and other program indicators by zone are also helpful in identifying specific performance problems requiring attention. Even when reports overestimate coverage, as is likely the case in Ethiopia, given consistent measurement, they can still be used to compare variations across regions and over time. From the Map 3, we see that although an increasing number of zones are reporting high coverage (DTP3>90%) between 2007- 2010, zones in pastoralist have consistently underperform. This calls for continued effort to address low immunization performance in these regions.
21 | P a g e
2009 20082007DTP3 <50%
DTP3 50-79%
DTP3 80-89%
DTP3 ≥90%
2010

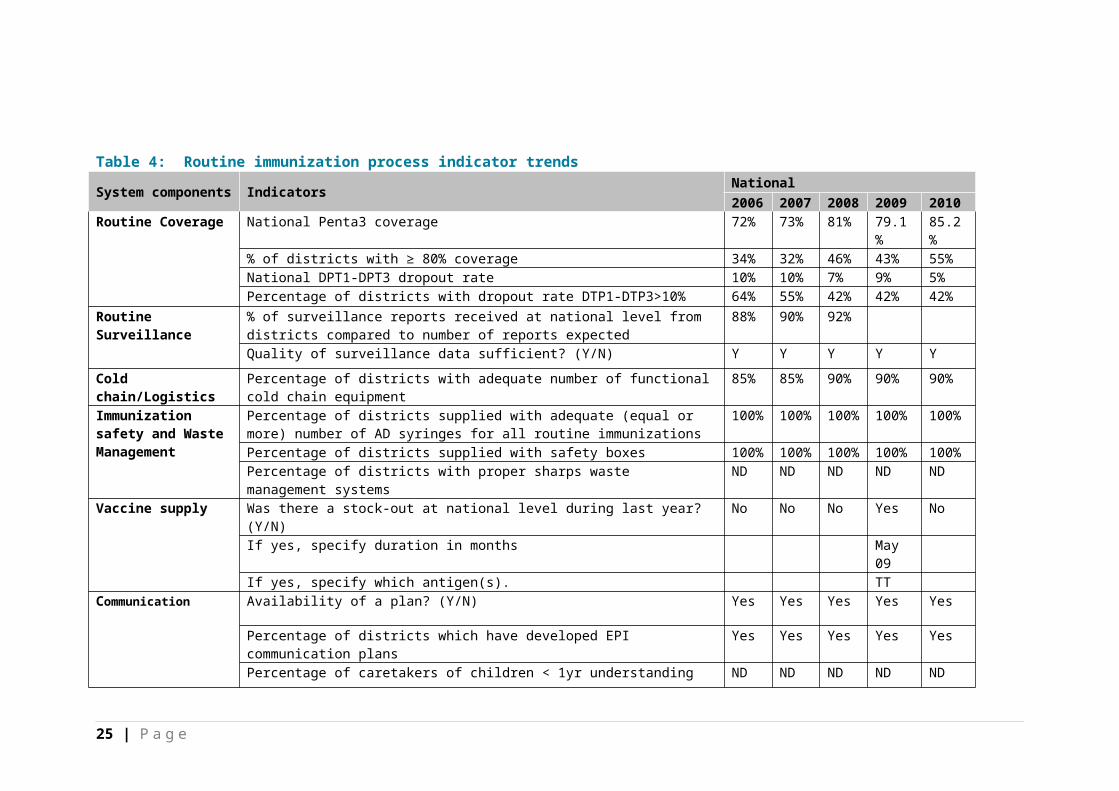
Table 4: Routine immunization process indicator trendsSystem components Indicators
National2006
2007
2008
2009 2010
Routine Coverage National Penta3 coverage 72% 73% 81% 79.1%
85.2%
% of districts with ≥ 80% coverage 34% 32% 46% 43% 55%National DPT1-DPT3 dropout rate 10% 10% 7% 9% 5%Percentage of districts with dropout rate DTP1-DTP3>10% 64% 55% 42% 42% 42%
Routine Surveillance
% of surveillance reports received at national level from districts compared to number of reports expected
88% 90% 92%
Quality of surveillance data sufficient? (Y/N) Y Y Y Y Y
Cold chain/Logistics
Percentage of districts with adequate number of functional cold chain equipment
85% 85% 90% 90% 90%
Immunization safety and Waste Management
Percentage of districts supplied with adequate (equal or more) number of AD syringes for all routine immunizations
100%
100%
100%
100% 100%
Percentage of districts supplied with safety boxes 100%
100%
100%
100% 100%
Percentage of districts with proper sharps waste management systems
ND ND ND ND ND
Vaccine supply Was there a stock-out at national level during last year? (Y/N) No No No Yes NoIf yes, specify duration in months May
09If yes, specify which antigen(s). TT
Communication Availability of a plan? (Y/N) Yes Yes Yes Yes Yes
Percentage of districts which have developed EPI communication plans
Yes Yes Yes Yes Yes
Percentage of caretakers of children < 1yr understanding the importance of routine immunization.
ND ND ND ND ND
Financial sustainability
What percentage of total routine vaccine spending was financed using Government funds?(including loans and excluding external public financing)
6% 6% 6% 7% 5%
22 | P a g e

Management planning
Are a series of district indicators collected regularly at national level?(Y/N)
Y Y Y Y Y
Percentage of all districts with micro plans. 100%
100%
100%
100% 100%
Research/ studies Number of vaccine related studies conducted/being conducted ND ND ND ND 1NRA Number of functions conducted 0 0 0 1National ICC Number of meetings held last year 20 5 5 10 6Human Resources availability
Percentage of sanctioned posts of vaccinators filled 100%
100%
100%
100% 100%
Percentage of health facilities with at least 1 vaccinator 100%
100%
100%
100% 100%
Percentage of vaccinators time available for routine EPI 50% 40% 30% 30% 30%Number of vaccinators / 10.000 population 4 4 4 4 4
Transport / Mobility
Percentage of districts with a sufficient number of supervisory/EPI field activity vehicles/motorbikes/bicycles in working condition
70% 70% 80%
Waste Management
Availability of a waste management plan Yes Yes Yes Yes YesVaccine wastage monitoring at national level for all vaccines? (Y/N) Yes Yes Yes Yes Yes
Linking to other Health Interventions
Were immunization services systematically linked with delivery of other interventions (Malaria, Nutrition, Child health etc.)?
Yes Yes Yes Yes Yes
Program Efficiency
Timeliness of disbursement of funds to district and service delivery level
Yes Yes Yes Yes Yes
Source: JRF and http://apps.who.int/immunization_monitoring/en/globalsummary/countryprofileresult.cfm
23 | P a g e

As shown on Table 4, the overall trend for RI process indicators such as Pentvalent 3 coverage and the percentage of districts with adequate number of functional cold chain equipment have improved in the past few years. These successes relate to the implementation of RED and ERIA during the time frame. The start of ERIA also contributed to a 7% increase in DPT3 coverage and 4% decrease in DPT1- DPT3 dropout observed in 2009-10. Encouragingly, most of the RI process indicators remained the same or increased over the past few years. However, it should be noted that the availability of various plans (communication, waste management, microplans) and supply data does not necessary translate to appropriate use of plans and supplies. Collection of data and a closer look at plan implementation could identify additional causes of low performance in immunization. In the same table, it should be noted that although the number of vaccinators to population remained the same over the last five years there has been a significant reduction (10%) in the percentage of time vaccinators spend on EPI from 2006-2008. This remained the same in 2008-2010. The reason behind the reduction in time spent on vaccination needs to be further investigated since this could negatively affect EPI coverage in the future. Key RI process indicators, such as the percentage of districts with a waste management system and the percentage of caretakers of children < 1 year are unavailable, which limits our understanding of the underlying causes of inadequate performance in RI. Operational research on vaccine related issues is also lacking. We lack the ability to answer why outbreaks of VPDs persist when high immunization coverage is reported. Finally, it is recognized that less than 10% of funding for routine vaccines comes from government funding. This calls into question the sustainability of the provision of routine vaccinations.
24 | P a g e
IV. EPI RELATED RECOMMENDATIONS WITH SUMMARY OF CONTEXT BEHIND RECOMMENDATION
Table 6: Summary of key recommendations relating to routine immunization (general and pastoralist-specific)Key recommendations (summarize similar recommendations into one “theme” instead of listing all recommendations)
Contextual issues behind recommendation
Human resource development – train and assign a skilled technician on refrigerator maintenance. This person can serve as the person in charge of managing refrigerator maintenance at lower levels. Train HEWs on Interpersonal communication (IPC).(5,8,15)
Lack of cold chain maintenance skills at lower level is a persistent problem. Community lack of awareness is the leading cause of children being unimmunized and high drop out rate indicating the inadequate ICP skills of HEWs
Improve vaccine management by improving vaccine collection and supply through computerizing vaccine stock management in all districts and direct delivery of vaccines to health facilities.(8)
There is very poor stock control, much vaccine wastage, inadequate cold chain equipment and vaccine availability at lower levels.
Improve routine EPI data quality and management through availing EPI data recording and reporting tools, improved supportive supervision, providing relevant or refreshing training to supervisors and HEWs on how to collect, report and analyze for decision making.(8)
Lack of timely data, over and under reporting, limited appreciation and utilization of data at <40% EPI report timeliness for some regions.
Finance - increase the budget for EPI programs including purchasing of kerosene and solar system for the refrigerators by Regional Health Bureaus (RHBs).(21)
Lack of kerosene posing a problem for functioning of refrigerators at regional and lower levels.
Pastoralist specific recommendations Contextual issues behind recommendationStrengthen the full implementation of the HEP in pastoral communities and make a continued effort to deploy female HEWs; equip HEWs with food and water but not per-diem. HEWs need to understand the realities on the ground and to then modify planning, registration, reporting and monitoring of EPI activities as well as understand the socio economic, cultural, mobility patters and work closely with community and kebele
Majority of HEWs in pastoralist areas are males resulting in limited contact with mothers and females, limited knowledge of trainers about realities of working in pastoralist communities. Providing per diem is blocking the purpose of vaccination and getting coverage, HEW refusing to vaccinate without additional money.
25 | P a g e

administrators to better plan and implement ERIA.(21,23)Establish synergy between public health and veterinary services to deliver human and animal health interventions.(9)
There is poor collaboration between public health and veterinary services
Use a combination of static and mobile services to address the issue of high mobility in pastoralist area.(9)
Pastoralist communities are known for a high level of mobility which makes it difficult to provide immunization services through static services only
26 | P a g e

A. SUMMARIZED overview of recommendations for EPI in general relating to RI
The provision of quality routine immunization requires:1. The availability of efficient and effective cold chain system.2. Skilled human resource in vaccine management.3. Refrigerator maintenance.4. Availability of potent vaccines and equipment at health facilities
and outreach services 5. Timely collection, reporting and utilization of data for making
evidence-based decision making.
Ethiopia has faced various problems such as poor cold chain system, inadequate skilled human resources, poor vaccine management and inadequate vaccine storage capacity at different times. To address these problems, the country has devised several strategies such as developing and implementing a cold chain rehabilitation plan which resulted in significant improvements in storage capacity at the federal level and increased availability of fully functional refrigerators at all levels. A cost-effective and micro-managing system, “Clustering” was also designed to ensure that health posts are better linked to other facilities where refrigerators are stationed. Various cascaded trainings on refrigerator maintenance have also been given by the FMoH in collaboration with UNICEF, and guidelines were developed and implemented on injection safety and waste disposal.
Despite these efforts, major problems remain, such as the shortage of assigned skilled technicians to maintain refrigerators at sub-national levels, weak vaccine stock and inventory management at regional and health facilities, and poor distribution for vaccines and injection materials. This has resulted in the overstocking of vaccines at the central level while there is a shortage at sub national levels. In addition, there is inadequate supervision and monitoring of EPI programs from peripheral regions which has resulted in delayed reporting.
To address the above problems, it has been recommended to : 1) improve routine EPI data quality and management through availing EPI data recording and reporting tools; 2) improve supportive supervision, providing relevant or refreshing training to supervisors and HEWs on how to collect, report and analyze EPI data for decision making (8); 3) allocate increased funding for EPI activities including purchasing of kerosene for refrigerators or the installment of solar-powered refrigerator systems; 4) leverage the clustering approach until refrigerators becomes available in all health posts; 5) continue providing cascaded training for technicians on refrigerator maintenance and making sure that they are assigned as the focal person to handle refrigerator maintenance issues at lower levels; and 6) improve vaccine and injection material distribution and inventory management at regional and health facility level (8).
27 | P a g e

B.EPI recommendation for pastoralist specific areas
It is estimated that 9.8 million Ethiopians live the pastoralist life style, which means Ethiopia has one of largest pastoralist populations in Africa. Ethnic groups including the Somali, the Afar, some Oromo groups (particularly the Borena and Kereyu), many groups in South Omo Zone of SNNPR, and the Nuer in Gambella, constitute the majority of the Ethiopian pastoralists. The pastoral areas are characterized by unpredictable and unstable climatic conditions as well as ecologically fragile environments. Seasonal movement is the unique lifestyle of pastoralists, which affects the ability to deliver health care (and immunization services) from static facilities. In pastoralist areas, the health infrastructure is generally poor – the small number of hospitals and health facilities that do exist are unevenly distributed and fail to provide the minimum package of primary health care services. Most facilities operate at a level far below their intended capacity and are poorly organized, staffed and managed, resulting in low utilization rates. The FMoH recognizes that the current lack of an appropriate health service delivery package for the pastoralist communities and the need to develop a viable strategy for health service delivery. Hence, “Health Service Delivery to Pastoralists" was a strategy developed by the FMoH and an attempt was made to tailor the Health Extension Program (HEP) package to the needs and life styles of pastoralists, which included the translation of the program documents to local languages.
In addition, as part of the federal government’s efforts to provide technical assistance to the emerging regions (of which the pastoralist regions are part), a board composed of members from six ministries was established under the Ministry of Federal Affairs including a technical committee for the integration of support to these regions. Moreover, the Pastoralist Health Promotion and Disease Prevention Directorate was established within the FMoH to focus on providing healthcare to pastoralist communities. As a result of these efforts and many others, there has been an improvement in child health indicators for the pastoralist areas but much remains to be done. Immunization coverage for pastoralist areas is lagging behind the national average – in 2010, the national full immunization coverage was 65.5 %, while the percentage of children fully immunized in Somali was 30.3%, 41.3% in Afar, and 35.9 % in Gambella (9).
Although all the EPI recommendations provided for non-pastoralist regions also holds true for pastoralist regions, some of the specific recommendation to pastoralist areas include the need to use mobile health teams to deliver services to mobile populations. The HEP needs to give more consideration to socio-cultural and livelihood situation of pastoralists, including settlement patterns, belief systems, seasonal movement patterns, and social organizations (which includes utilizing the traditional governance system – the role of elders/religious or opinion leaders and information dissemination systems, such as the Daagu of Afar is believed to be critical to making continued enhanced RI services available in pastoralist areas). There is also a need for HEWs to adopt the planning, registration, reporting and monitoring of EPI programs which reflects
28 | P a g e

the reality of the pastoralist society – this can be done by working closely with the community and kebele administrators. One way to work with the community is to translate reports into the local language, this could enhance ownership. Additionally, the region could ask the community for help register children; this is especially helpful when there is no fixed address. The more involved the HEWs are in the planning process the more flexibility they will have to negotiate with the community on an immunization schedule. It is also recommended that a continued effort be made to employ female HEWs in place of male HEWs whenever possible. The idea is to increase the contact between HEWs and mothers and girls, which is easier when the HEWs are female. Furthermore, it would be best if the HEWs were able to speak the language and understood the culture of the pastoralist area – this could help to get more buy in from the community. Equipping the HEWs with adequate food, water and required equipment is more important than financial incentives to sustain the program (23). Given the strong attachment that the pastoralist communities have with their livestock, it is recommended that public health services collaborate with veterinary services to improve access and health care coverage in pastoral communities. Lastly, it is imperative to have a strategy that combined the provision of static and mobile services. (9)
V. INTRODUCTION, PURPOSE, OVERVIEW OF STAKEHOLDER MAPPING EXERCISE
The 2nd part of this review is an initial stakeholder mapping exercise, which is performed in order to better understand the partners working in RI, MNCH, Quality Improvement (QI) and where their operation is located. This exercise also identifies the type of support different partners provide and the “best practices”/innovations or exemplary sustainable success in RI, MNCH and QI that they have achieved in order to scale-up and improve immunization programs in the country.
As the project evolves, the stakeholder mapping exercise will include woreda specific components on stakeholder engagement and an analysis or review of the power/influence structures in the woreda providing additional information on how stakeholders affect immunization and health programs in Ethiopia. In order to perform this initial phase of the stakeholder mapping, the consultant has reviewed published and unpublished documents by focusing mainly on partners operating within the last five years. This report highlights some of the major partners working in the areas of RI, MNCH and QI based on the information available. This report tries to highlight the major partners’ area of support by location and timeframe, where innovations or exemplary sustainable successes have been achieved using a narrative summary and a series of maps and tables. “Innovative” is defined as an idea/approach/strategy/or task that has showed some creative way of solving problems at the local level. Innovations
29 | P a g e

may sometimes be described as “best practices”. The consultant remained impartial in the selection of innovative practices.
VI. RI, MNCH AND QI WORK IN ETHIOPIA
A. Overview of RI, MNCH and QI work in Ethiopia
Ethiopia has a strong Inter-agency Coordination Committee (ICC), which is made up of high-level decision makers from the FMoH and partners including WHO, UNICEF, Japanese International Cooperation Agency (JICA), Rotary and the CORE group. There are two sub-committees under the ICC, the technical sub-committee and social mobilization sub-committee. The main ICC meets quarterly and sub-committees meet monthly. The ICC is the advisory body to the FMoH and also supports programs in resource mobilization and advocacy visits to regions and other partners. Some regions with low immunization coverage (Afar, Benshangul Gumuz, Gambella, Somali) also have ICC at the regional level (1).
Strengthening the health system of the country is critical in improving not only RI and MNCH but also other programs in the country. The GoE has increasingly emphasized the need to invest in health system strengthening to sustain achievements and to bring about significant improvement in the health status of the population. Despite this, few partners are currently working in health system strengthening, which was unexpected. Some of the major partners who are working in health system strengthening through the Health Management Information System, Human Resource Development and Health Extension Programs include WHO, UNICEF, CDC, USAID and Gates Funded partners such as JSI, Pathfinder and Tulane University. UN organizations usually work at national level whereas USAID partners work mostly in some or in all major regions (Amhara, Oromia, SNNP and Tigray)(11).
The routine immunization program is funded primarily by partners and the GoE. Partners largely channel their funds through UNICEF and WHO (Some of which include GAVI, JICA, European Union, CIDA etc.). UNICEF and WHO operate at national level and provide different kinds of technical and financial support in routine immunization, some of which include health system strengthening, M & E, supporting the health extension program (HEP), control of vaccine-preventable diseases and other major communicable diseases, capacity building of human resources, introduction of new vaccines, and provide support to national and regional review meetings.
GAVI operates at national level and provides an enormous amount of resources to improve the general health system and immunization services in Ethiopia. It operates in four areas namely: Immunization Service support (ISS), Injection safety Support (INS), New Vaccine Introduction support (NVS) and Health system Strengthening (HSS). GAVI funding for ISS started in 2002 mainly to
30 | P a g e

strengthen routine immunizations based on ICC. GAVI support of ISS was used to purchase injection equipment and safety boxes for EPI programs to transition from reusable syringes and needles to Auto disabled syringes from 2002-2004. Since 2004, the Development Agency of Ireland and UNICEF have been providing funding for injection supplies.
GAVI’s introduction of new vaccines support helped to introduce hepatitis B and Haemophilus influenza type B in the form Pentavalent in March 2007. The FMOH also introduced PCV 10 Pneumococcal vaccine in 2011 and this vaccine is believed to substantially contribute to the achievement of MDG4 by decreasing the leading cause of U5M Pneumonia in Ethiopia. The FMOH is in the process of preparing to introduce the Rota vaccine by 2012, to prevent diarrhea.
GAVI HSS support is used to strengthen the Ethiopian health system by supporting human resources for the delivery of basic health services through HEP, to improve the supply, distribution and maintenance systems and enhance the organization and management of health service delivery. There are many USAID and Gates partners supporting RI, MNCH and Quality improvement programs in Ethiopia, mainly through strengthening HEP, some of which include several projects by JSI and Pathfinder. Please find below the summary on each project:
The Gates-funded “Last Ten Kilometres” (L10K) Project, implemented by JSI Research & Training Institute Inc. (JSI R&T), operates in 115 woredas in four regions—Amhara, Oromia, SNNP, and Tigray regions—to support the health extension program of the GOE. The project aims to strengthen the bridge between households, communities and HEP primarily by mobilizing families and communities to engage households and improve community health practices, ultimately leading to improved key reproductive, maternal, neonatal and child health (RMNCH) outcomes and contribute towards achieving MDGs 4 and 5 (i.e., decrease maternal and child mortality rates). The L10K provides technical support and grants programs to strengthen the capacity of the regional and local organizations to implement innovative community based strategies to improve RMNCH (15).
Essential Services for Health in Ethiopia Project (ESHE) is a USAID funded JSI project that was launched in 1995 and continued the project as ESHE II from 2003-2008. ESHE operated in three regions namely Amhara, Oromia and SNNP, that represents 55 million of the more than 74 million population of Ethiopia. The ESHE project provided support to reduce famine vulnerability, hunger, and poverty, aimed to increase human capacity and social resiliency. ESHE also provided support on immunization, integrated management of newborn and childhood illnesses (IMNCI), and essential nutrition actions (ENA). Community mobilization activities to increase parents' role in caring for their families was also undertaken. National and regional health management
31 | P a g e

information systems and health care financing (HCF) were also improved.(27)
Pathfinder – A USAID funded organization that worked in partnership with JSI to implement the Integrated Family Health Program (IFHP) project. IFHP is a 5 years project (2008 - 2013) and operates in 6 regions, including the four major regions, 283 woredas covering 42 million people. The project builds upon on ESHE and Family Planning (FP) projects to create an integrated Reproductive health (RH/MNCH) program to support key interventions and health systems. IFHP aims to sustain past achievements in family planning, immunization and promotion of essential nutrition actions (ENA), empower the Health Extension Workers (HEWs) through designing maternal health strategy and implementing the successful transition of NGO management model to support the HEP. IFHP also works closely with other JSI projects such as L10K, Ethiopian Saving New Born Lives (SNL), Urban Health Extension Program (UHEP) on community mobilization, BCC training material development and BCC rollout of volunteer Community Health Workers (VCHW) and partners with DELIVER, Supply Chains for Community Case Management (SC4CCM) and SNL on health system strengthening (11).
Ethiopia Saving New Born Lives (SNL) -SNL received funding from the Gates Foundation for a period, from August 2007 to August 2011. It operates in two regions (Oromia and SNNP) covering 22 health facilities, with an estimated population of 660,000. The project focus on Strengthening and evaluating the implementation of the HEP according to existing policies and assessing the effectiveness and cost of integrating community-based identification and management of infections (neonatal & pneumonia) in <5 children by HEWs into the current HEP/IMNCI guidelines(11).
Urban Health Extension Program (UHEP): This JSI funded project started in September, 2009 and operates in 17 towns in Amhara Region (in Bahir Dar, Gondar, Debre Markos, Dessie), in Oromia Region, SNNP Region, Tigray (in Mekele, Adigrat, Maichew, Axum and Shire), Harari Region (Harar Town), Addis Ababa City Administration (Yeka Sub-city)and Dire Dawa (Dire Dawa Town). The project focuses on providing support and scaling-up, implementing and monitoring of the GoE’s UHEP to improve access /increase demand for health services (with the entry point/platform for addressing HIV). In addition, UHEP’s work involves capacity building of urban helath extension workers (UHEWs) to identify MARPs and provide services to improve overall health outcomes. This includes HIV prevention, care and support services (to facilitate ‘bridge’ between MARPs and UHEP through UHEW and engage Civil Society Organizations (CSOs/Community Based Organizations (CBOs) working with vulnerable populations).
32 | P a g e
Supply Chains for Community Case Management (SC4CCM) – This JSI project started in March 2011 and operates in Amhara, Tigray, Oromia and SNNP regions. SC4CCM identify, demonstrate and institutionalize Supply Chain Management practices that improve the availability and use of selected essential health products in community-based programs to treat children <5.
DELIVER – A USAID funded JSI project focusing on providing support in the implementation of new integrated health commodity supply system (LMIS) and leadership in RH/FP with commodities and coordination.
HMIS Scaling up (SU) Project – USAID funded 3 years project for scaling up HMIS project in SNNP region.
University Research Co. – A USAID Health Care Improvement Project (HCI) operating since 2007 - present. URC is working with other implementing partners to apply standards for programs serving orphans and vulnerable children (OVC). HCI is developing, testing and documenting a model to facilitate community support for children and families affected by HIV/AIDS in Dire Dawa and Debre Zeit, in Oromia Region.
Maternal & Neonatal Health in Ethiopia Partnership (MaNHEP) – This 2 years Gates funded project established to Improve the capability and performance of frontline workers ‘team’ such as Health Extension Workers (HEWs), Community Health Workers (CHWs) Traditional Birth Attendants (TBAs) to provide evidence-based packages for MNH services (e.g. hygienic delivery, hand washing & cord care) covering the period from birth-to-48 hours to increase the demand from women and families for targeted MNH services and promote self-care behaviors around the time of birth .
Making Medical Injections Safer- A USAID funded project operating in Amhara, Oromia, Tigray and SNNP, Addis Ababa and other urban areas. The project’s goal is to ensure that every health facility has trained health care workers who administer only appropriate injections safely, using safe injection devices and management of health care waste, using methods that are safe for the community and the environment.
CORE GROUP/CCRDA – signed a strategic partnership agreement with CCRDA in November 2001 to implement polio eradication project in different parts of Ethiopia. It operates in 67 woredas in seven regions namely Somali, Afar, Gambela, Amhara, Benshangul, SNNP and Oromia targeting U5. CORE Group implements its project activities through eight international NGOs namely (CARE Ethiopia, Christian Children Fund Ethiopia, Plan Vision Ethiopia, Save the Children USA, World Committee and African Medical Research Foundation) and four local NGOs (Pastoralist Concern, Hararghe Catholic Secretariat, Alemtena Catholic Church and the Ethiopian Evangelical Church Mekenae Yesus).
33 | P a g e

Some of achievements of CORE group working in collaboration with FHB, FMOH, WHO UNICEF, Rotary international and other partner organizations, conducting regional advocacy workshops on immunization and surveillance activity in Gambella, Benishangul and Afar regions. To fill the gap of the national facility-based surveillance and EPI interventions, CGE initiated and implemented CBS using more than 3,200 community volunteers, surveillance focal persons in 54 woredas in seven regions. The officer and director of CGE secretariat and partner organizations provided technical and logistics support for polio SIAs conducted in various project implementation areas. To improve the routine immunization, CGE through its implementing organizations provided maintenance, fuel and spare parts supports to motorbike and cold chain equipment, as well as training, recording and reporting materials to health facilities. CGE developed effective partnerships among its implementing partners for polio eradication efforts (31).
Clinton Health Access Initiative (CHAI) - As one of the partners of the GoE, CHAI supports the introduction and nationwide implementation of the pneumococcal vaccines in Ethiopia. CHAI supports the GoE to assess which vaccines were being exposed to potentially damaging and extreme temperatures during storage and transportation. The findings have resulted in a plan by the FMOH to train health workers on vaccine management and strengthen the cold chain. CHAI also intends to assist the GoE in the introduction of rotavirus vaccine by 2013. CHAI will work with the several new emerging market suppliers in the next five to ten years, to help increase access to the new vaccines that the country is introducing (32)
34 | P a g e

Table 7: Overview of Contribution/Participation by Main Development Partners of EPI, MNCH, QI 2011
Area Partners (not including FMOH)
Location by partner
(specific to regions/zones/woredas, list by partner working where)
Health System Strengthening, Monitoring, HMIS & Quality Assurance
Tulane University, JSI, CDC, WHO, UNICEF, GAVI, Global Fund
WHO & UNICEF - National, CDC through Tulane University – National, GAVI and Global Fund – National, JSI – SNNP
Support to Health Extension Program and training of HEWs
WHO, UNICEF, UNFPA, GAVI, USAID, DFID, JSI, USAID (Pathfinder),
WHO, UNICEF ,UNFPA and GAVI – National, JSI(UHEP)–Amhara, Oromia, Tigray, Addis Ababa, Harari, SNNP, USAID (Pathfinder) Amhara, Oromia, Tigray and SNNP, JSI – IFHP (Amhara, Oromia and SNNP)
Capacity building for Human Resources Development in the health sector
WHO, UNFPA, USAID, Tulane University
All at National level
Strengthening control of vaccine-preventable diseases and other major communicable diseases
WHO, UNICEF , EU, GAVI, JICA, CDC, Irish Aid and Rotary
All at National level
New vaccine introduction WHO, UNICEF, Clinton Health Access Initiative (CHAI), Core Group, GAVI
All at National level
Quality improvement in health URC, MaNHEP, L10K, and SNL
University Research Co – Dire Dawa, Oromia -Addis Ababa MaNHEP – Amhara and Oromia; L10K – Amhara, Tigray, Oromia and SNNP;, SLN – Oromia & SNNP
Data quality improvement in immunization
WHO, IFHP IFHP – Amhara, Benishangul-Gumuz, Oromia, SNNPR, Tigray
Review meeting support (technical/financial)
IFHP, UNICEF, WHO UNICEF & WHO, IFHP – National
Peer learning focus in health UNICEF, WHO UNICEF, WHO – National
35 | P a g e

(positive deviance, focus on idea sharing through cross visits, etc.)
36 | P a g e

B. Routine Immunization work in Ethiopia
i. Geographic support for RI – NA ii. Financial support for RI
Table 8: financial advocacy efforts for RI by “system” PHC-related and ERIA-related RI supportArea – system/PHC related
Partners Location
( specific regions/zones/woredas, list by partner working where)
Advocacy with parliamentarians for immunization
Sabin SIF, UNICEF & WHO, CORE
All at National level except CORE
Capacity building of WorHOs to allocate adequate funds to woreda
UNICEF & WHO, ICC National
Area – PIRI/ERIA related Partners Location
ERIA in ZLUC (zones with large number of unimmunized children)
WHO, UNICEF National
iii) Innovative and sustained successes in RI by agency
Table 9: Innovations and sustained successes in RI
Innovations in RI Partner Location (if specific regions/zones/woredas available, list by partner working where)
Timeframe of innovation
Reaching Every District (RED): approach was introduced in November 2002 and was launched in Ethiopia in 2003. It has five components. These are re-establishment of regular outreach services; supportive supervision: on-site training; community links with service delivery; monitoring and use of data for action; better planning and management of human and financial resources.
GAVI, WHO, UNICEF
Started in 13 zones (phase 1), 45 zones (phase 2) and scale- up to 58 zones in all regions
2003-2007
Enhanced Routine Immunization Activities (ERIA): launched in June 2009 and designed to strengthen the existing RI and reduce the number of unvaccinated children in the four emerging regions and zones with large numbers of unvaccinated children using
UNICEF, WHO, GAVI
Started 2 woredas in Jijga zone (Somali) and now scaled up to all other emerging regions.
2009- present
37 | P a g e
existing routine immunizations. ERIA components include advocacy visits, micro-planning and registration, IIP/ cold chain/vaccine management training, and supportive supervision.
38 | P a g e

C. Reaching Every District (RED):
Introduction: To achieve a sustainable and equitable access to good quality immunization services and accelerate progress towards the 80/80 goal, GAVI partners proposed in 2002, a new approach “Reaching Every District” as a strategy towards achieving its goal of reaching >80% DTP3 coverage in every district of >80% of developing countries by 2005. This is being referred to as the "80/80 goal". The RED strategy means reaching every child, in every district with quality immunization services. In Ethiopia, immunization services are delivered as part of the integrated maternal and child health services at health facilities and outreach sites. Hence, the operational strategy to implement the RED concept was also designed in an integrated manner, using EPI services, as the platform.
The RED approach was introduced in Ethiopia in November 2002 and was launched in 2003 to address the issue of inadequate capacity building and lack of motivation of staff at district level. RED has five components that help to put procedures at each level of the national health system. This includes building the capacity at district level, develop an annual work plan, implement and monitor the plan.
Implementation: For the first phase of the RED project implementation 13 zones with the lowest performance rates were selected by the FMoH. The selected zones were funded and supported technically by WHO between 2003 and early 2004. Additional zones were added in 2004 which reached a total of 44 zones (in phase II). By 2007, the number of zones officially designated as “RED zones” reached 79 out of the selected 85 zones. However, the remaining 6 zones although not officially designated as RED zones, were carrying out immunization activities using the five main components of RED.
During the first phase of the RED implementation, orientation and micro-planning workshops and health worker training courses were conducted. Since then, RED continues to supervise its activities. In 2007, a RED micro –planning training workshop was carried out at zonal level. In addition, valuable
39 | P a g e
The five operational components of RED:
1. Re-establishing fixed and outreach vaccination services for under-served communities,
2. Provide supportive supervision in the form of on-site training for supervisors and possibly integrating the supervision of other health services;
3. Creating linkages between community and services through regular meetings to increase demand for immunization and enhanced community participation ,
4. Monitoring of data systems and data quality assurance, to direct planning and managerial actions at district level and data usage at health facility level; and

resources were provided for RED, including refrigerator spare parts, motorcycles, EPI coverage wall charts, supervision checklists and supervision record books, which were presented to the health facilities in RED zones. During the implementation of the RED approach, refresher training courses and micro-planning workshops was also provided to health workers and zonal health offices, in RED zones, using immunization in practice and mid-level management training modules. In addition, the Ethiopia RED approach guide was also developed.
A summary of some of the RED approaches - strengths, weaknesses and achievements as noted in the RED evaluation report of 2007 - are as follows:
The strength of the RED approach at national level was the strong commitment to implement the RED Approach, which by 2007 was rolled out to all regions. It was closely identified with strengthening routine immunizations; possessing an active Interagency Coordinating Committee (ICC); exhibiting progress with the training and a deployment plan for (HEWs); and securing GAVI Alliance ISS rewards for a total of $10 million, which was received for coverage improvements which were achieved in 2004 and 2005.The weakness of the approach was the EPI management personnel shortages, at national level.
Some of the major strengths identified at WorHOs and health facilities include:
A RED “Field Guide & Tools” document was developed. Most health centers conduct immunization sessions on a daily basis. HEWs (6,000 currently) are working to help the community ,Vaccines/supplies conditions and distribution methods were found adequate; More outreach sites have been opened since the RED approach started and almost all planned outreach sessions are being held (estimated to deliver about 75% of all vaccinations),
The approach was integrated with some other primary health care (PHC) activities and community involvement in the planning of outreach sites and session days in some areas. Community Health Promoters (CHP) were also involved and participated in review meetings, with their training supported by local NGOs, and there were examples of other health staff such as (TBA) and community-based reproductive health and family planning agents (CBRHA) working to mobilize communities.
Supervisors visited health posts quite frequently, with an integrated supervision checklist and funding for supervision costs. Woreda Councils were responsible for health matters and allocation of funding.
Immunization coverage monitoring charts were generally available at district and health facility levels. The EPI Registration Book was available in most places, and review meetings are conducted regularly. A steady rise in diphtheria, pertussis, tetanus (DPT) and measles vaccine coverage and in district DPT performance has been perceived since the introduction of the RED approach.
40 | P a g e

•21%
5660 63
76 78 80
51 51 52
66 69 72
40 42 44
5559
63
0
10
20
30
40
50
60
70
80
90
100
2001 2002 2003 2004 2005 2006Year
%
DPT1 DPT3 Measles
Fig 2: EPI Coverage by Antigen 2001- 2006
Achieved Results: As shown in Figure 2 at right, the trend of DPT1 coverage—a major indicator of access to health services—showed a significant (17%) increase between 2003 and 2006. However, there were differences among districts and zones. The major increases illustrated in the chart correspond to the period following the introduction of RED and shows a dramatic increase in the percent of children immunized in the zones targeted in 2003.
Utilization of services following initial contact—indicated by DPT3 coverage—is a major indicator of the capacity and strength of a health system. In the same figure, we see a marked increase in DPT3 coverage after the introduction of RED in 2003. Figure 3 also supports the impact of RED on DTP3 coverage, illustrating an increasing trend in the number of DTP3 vaccinated children in RED districts as compared to non-RED districts. Figure 4 illustrates how the number of districts with DPT3 coverage greater than 50% decreased by 65%, from 46 districts in 2002 to 18 in 2006. In the same time period, the number of districts with DPT3 coverage of greater than or equal 80% increased from 9 to 29 districts in the same time period. It is believed that these changes were primarily due to improved coverage in the poorly- performing districts that were targeted by the RED approach.
Fig 3. RED Approach Outcome: DTP3 coverage pre/post RED Infants Immunized in RED and non-RED districts 2002 -2006
It is important to note that coverage data for the group of RED zones as a whole shows that while there has been significant progress with DPT and measles
41 | P a g e
2002 2003 2004 2005 20060
200,000400,000600,000800,000
1,000,0001,200,0001,400,0001,600,0001,800,0002,000,000
non-RED
RED

46 45
27 26 18
23 29
34 4038
9 725 20
29
0%
20%
40%
60%
80%
100%
2002 2003 2004 2005 2006
DTP3≥80%DTP3 >50%<80%DTP3<50%
•13
•Source: Country Datasheet Ethiopia 7_10_07, uncorrected
2003 RED Introduced in first __ districts2004 RED expanded to additional __ districts
coverage, there were still unacceptably high drop-out rates from DPT to measles immunization and therefore continued exposure to and risk of outbreaks of measles.
Challenges: There was little evidence to show the use of data to address health facility poor performance areas. In many places, attention is not focused on monitoring measles coverage and fully immunized children, even where dropout rates from DTP1 to measles vaccines remains high. Even in the “RED Zones” as a group, this dropout rate has not improved much since 2003 and measles remains a significant public health problem in Ethiopia.
Figure 4: RED Approach Outcome – DTP3 pre/post REDThere was also poor documentation of defaulters and select immunization data did not indicate which strategy (static, outreach or mobile) was used to provide the immunization services. Many outreach sites are poorly attended, and there was poor documentation of outreach and fixed sessions. RED micro-planning was not conducted in most health facilities, and the catchment
area maps in most woredas and health facilities (where available) lacked adequate detail. The Ethiopia RED Field Guide was usually not found at the facility level.
In all seven zones, many of the health managers and staff were posted within the last year. As a result, the new staff was not working in the facilities when the RED approach was introduced in 2003/2004, and had not received orientation or handover training. Additionally, EPI refresher training was not provided for most of the health staff interviewed. In addition, there was inadequate inventory of vaccine and materials and stock management in many places, and vaccine wastage was not monitored. Guidelines and standards for supervision and written supervision schedules were routinely unavailable, and supervisory visits were often irregular, conducted without checklists, and not prioritized by areas of low performance.
The evaluation team found written community mobilization plans in only half of the woreda immunization programs, only one-third of the budget for social mobilization was utilized, and insufficient Information, Education and Communication (IEC) materials were available at all levels. Most health workers had not received training on inter-personal communication (IPC) and social mobilization, and over half of health facilities visited did not hold regular meetings with the community. There was also limited advocacy by health officers to woreda administrations for their involvement in immunization. One of
42 | P a g e
•0
•<1/100,000
•>=1/100,000
the important finding is that measles is still a great burden in many areas of Ethiopia. Contrary to the documented numbers, and a steady rise in DPT coverage, measles is still lagging behind.
Table 10: RED Zones - 2003 and 2006 reported DPT and Measles Coverage (by one year of age)/Drop-Out, and Left-Out, (%)
Year DPT1 Coverage (%)
DPT3 Coverage (%)
Measles Coverage (%)
DPT1 – DPT3 Dropout Rate (%)
DPT1 – Measles Dropout Rate (%)
Left Out (%)
RED Zones
2003 55 43 36 22 34 45
2006 78 67 55 12 28 24
Note: it was presumed that there was negligible immunization given above one year of age, but the data was not available at present to verify this.
As shown in Map 4, the lack of progress in addressing dropout rates of measles immunization in the RED Zones appears to have affected the overall reported coverage for Ethiopia. This was not a new issue: the 2005 Ethiopia RED evaluation report commented that: “Despite a very positive increase in average coverage, the data show some relatively extreme variations among the 13 RED Zones in terms of DPT and measles immunization coverage and related immunization dropout rates”.
Map 4: Measles Incidence Rate per 100,000 Populations, Ethiopia: 2007 Also in the RED and non-RED Zones, DPT1 to measles immunization dropout rates continues to be unacceptably high. However, because of SIAs that the data analyzed did not capture, it was not possible to determine whether these rates tell the full story of what happened over the past two years with measles immunization coverage and DPT1 measles dropout rates. In RED and non-RED zones, 26% and
27% of infants respectively who received DPT1 vaccines but did not receive the measles vaccine.
43 | P a g e
1

The other challenge identified that could affect the sustainability of RED approach were:
Staffing issues, such as vacant key positions, high turnover rates Lack of handover arrangements when staff members leave, Possible over-dependency on outreach service delivery compared with
fixed sites, dependence on left over funds from campaigns for routine programs
expenditures/activities, uncertainty about what will happen after campaigns finish and the huge
cost of newly introduced vaccines compared with traditional ones, all donor funded.
Conclusions: RED approach has shown a positive trend in increasing DPT3 coverage in RED Zones. However to achieve high coverage, lower levels (health facility and health post) need to be involved in RED micro-planning activities and receive more comprehensive training, there is a need for high quality and frequent supportive supervision and a need to counteract the effects of high staff turnover. In addition, National norms are needed to assist district health authorities in choosing the sites, locations and frequencies of outreach sessions and health facilities should use their data and maps to improve the planning of the numbers, frequency and location of outreach sessions to make outreach as efficient, as possible. Last, but not least, increasing routine measles immunization coverage and reducing DPT1-measles dropout rates should be given high priority by the routine programs in all zones (RED and non-RED) in the future.
Enhanced Routine Immunization Activities (ERIA)
Target Area for ERIA 12 ZLUC and 4 Emerging Regions
Zones in NPA Somali Afar B. GumuzGambela
44 | P a g e

Map 5: Target Areas for ERIA 12 ZLUC and Four Emerging RegionsSource: Reaching Unvaccinated Children in Ethiopia EPI Managers Meeting, PPT Maputo 10-12 March 2010
D. Enhanced Routine Immunization Activity
Introduction: Routine immunization coverage in emerging regions namely Afar, Gambella, Somali, and Benshangul has not reached the targeted figures and planned objectives, posing a risk of outbreaks and importations of diseases, such as wild polio virus. Map 5 shows that the geographical distribution of the unvaccinated children by the end of 2009, as well as the regional contributions. 86% of the unvaccinated children were located in four regions: Oromia, Amhara, SNNP and Somali.
Reaching children in zones with the largest number of unimmunized children and in the emerging regions will require overcoming a number of critical barriers such as poor health systems, poor demand, access and utilization of health services, as well as inadequate human and financial resources that have slowed progress. The ERIA approach was therefore designed, initially for the emerging regions, but were later scaled-up to other regions, to address critical barriers to high vaccination coverage.
Implementation: ERIA has three areas of focus: pre-implimentation, implementation and post- implmentation. In the pre-implimentation stage, - some emergin regions conducted high level advocacy meetings highlighting the need for immunizing every child. Regional ICC committee also established and selected woredas with high numbers of unvaccinated children, based on HEWs registration of targeted children (surviving infant) using the registration book. Each kebele should have one team composed of one health worker (nurse, health officer, FHW) and each kebele should follow one standard immunization registration book. During the implementation stage, vaccine providers are not allowed to use or refer to the registration book used for house to house registration. However, Woreda EPI coordinators or supervisors should use the house to house registration book to counter check whether children registered ast household level are vaccinated and properly recorded on the existing routine immunization book or not.
Micro-planning was performed by identifying all the limitations associated with the ERIA and to develop appropriate strategies to resolve them using problem solving apporaches. The first step is to analyze the status of the routine immunization situation in each kebele, which includes identification of hard to reach areas and high risk populations, assessment of the available human,
45 | P a g e

material and financial resources and barriers and constraints in improving routine immunization coverage.
Registrationn of infants for immunization visits takes place during house to house visits by the HEWs in collaboration with kebele adminstrators, religious leaders and community mobilizers who conduct social mobilization activities, using public criers, megaphones, church and mosque announcements, leaflets announcing the need for immunization, which specify the date and place of immunization. Vaccines are then procured, collected and distributed.Orientation and deployment of one supervisor from RHB for each woreda with a vehicle to provide supportive supervision to the vaccination providers . Training of HEWs on how to conduct ERIA was also provided..
Implmentation: 1st, 2nd and 3rd rounds of ERIA was conducted on immunization days (usually 3-4 days) between March and June of 2009. Vaccination providers checked the vaccination status of children, provided vaccinations (BCG, Penta, OPV & Measles ), vaccination cards were given to each child. Advice was also given to caretakers on adverse events following immunization (AEFI), the date of the next appointment & handling of vaccination cards.
Post implmentation: Supportive supervison in 3-4 kebeles (per day) was conducted using a supervisory checklist, daily communication with central coordinators and supervisors submitted supervisory reports. Reporting – the RI reporting format was modified and used by kebeles and antigens. Review meetings were held frequently and a in few woreda were conducted on a daily basis. After each rounds of ERIA at regional level with the heads of WoHos and woreda EPI coordinators, minutes from the review meeting were documented properly.
Fig 5: Children vaccinated (Penta3) in 1st 9 months (July – March)
VS. last 3 months (April – June)(29
Achieved Results: In 2010, 14 zones were selected for ERIA in SNNP, Oromia and Amhara – this is in addition to the already implementing pastoralists regions. Three rounds of ERIA were implemented in April, May, June/ July in
46 | P a g e
Object 4

the selected 14 ERIA zones. The results showed positive results at the end of the three rounds as Compared to pre-ERIA period of 9 months (July to March) to reduce the large number of unvaccinated children. There was a 100% increase in 6 of the 14 ERIA implementation zones (Arsi, E/Hararghe, Guji, W/Arsi, B/Mali, Gomgofa,) and 50 to 100% increase in 5 of the zones (Jimma, Bale, N/Gonder, N/Shewa, S/Gonder), Borena and sidama had <50 % increase and a decline in coverage in south wello (29).
Challenges: Despite the successes, there were several challenges in the implementation of ERIA, some of which included variations in performance in targeted zones for instance, inadequate outcome in Amhara region, variations in implementation modalities, communication gaps between regional level and ZHD with delays in funds transfer, Competing priorities: polio SIAs, poor monitoring of ERIA impact and lack of timely data for action.
Conclusion: Efforts to reduce the large number of unvaccinated children in early 2010, using ERIA approach have shown positive results in the majority of targeted zones, which indicate that the ERIA approach is effective in increasing coverage in prioritized zones, with low coverage and large numbers of unvaccinated children. However, sustained efforts to address the observed challenges are needed to ensure that all targeted children are reached, on a regular basis with routine services.
VII. HEALTH AND MNCH WORK
I) Geographical support for MNCH
47 | P a g e

Map 6. L10K project coverage in the focus regions and woredas.Source: L10 k, Baseline Household survey summary report, August 29, 2009
II) Innovative and sustained successes in MNCH
Table 11: Innovations and sustainable successes in health and MNCH
48 | P a g e

Innovations in health/MNCH
Partner Location (if specific regions/zones/woredas available, list by partner working where)
Time frame of innovation
Health Extension Program (HEP): started in 2005 and is being implemented as an innovative approach to bring primary health service closer to the community through HEWs (34,000). HEWs are charged with providing promotional, preventive care including immunization and some treatment services. HEP is also supported by model households to further strengthen the program and share the burden of Health Extension workers.
GAVI, UNICEF, WHO, USAID, JSI, Pathfinder & MaNHEP
GAVI, UNICEF WHO national JSI (UHEP,)–Amhara, Oromia, Tigray, A.A, Harari, SNNPUSAID (Pathfinder) Amhara, Oromia, Tigray and SNNP, JSI (ESH) Amhara, Oromia and SNNP; MaNHEP – Amhara and Oromia; L10K – Amhara, Tigray, Oromia and SNNP;
Launched in 2005 to present
Taking Long Acting Family Planning (LAFP): Implanon Insertion Service to the Community
JSI (IFHP ) & Pathfinder
Oromia, Amhara, SNNP and Tigray
2008 – 2013
A. Health Extension Program (HEP)
Introduction: In 2003, the FMoH launched a new health care plan—the Accelerated Expansion of Primary Health Care Coverage—through a comprehensive Health Extension Program (HEP). Recognizing the huge gap between need for health services and health care available, the FMoH has focused on “providing quality promotive, preventive, and selected curative health care services in an accessible and equitable manner to reach all segments of the population, with special attention to mothers and children.”(5) More than 84 percent of Ethiopians live in rural areas, many remote and difficult to access. The policy places particular emphasis on establishing an effective and responsive health delivery system for those who live in rural areas. The government recognized the need to develop health care delivery capacity “designed to improve the health status of families, with their full participation, using local technologies and the community’s skill and wisdom.” (5)
The HEP draws on the same principles as the expansion of primary health care strategy, but focuses on the improvement of preventive behaviors within the
49 | P a g e

household and involves fewer facility-based services. The HEP philosophy is that if the right knowledge and skills are transferred to the community level, households can take responsibility for producing and maintaining their own health status.
At the core of HEP implementation is a sizeable cadre of HEWs, who are trained to implement a Health Extension Package of 16 healthcare activities (see box above) at the kebele (village) level. The GoE trained over 34,000 HEWs by 2011(5). All HEWs are women, except in Afar and Somali, where HEWs include both females and males. Other qualifications include being at least 18 years of age, having a minimum of a 10th grade education, and being recruited directly from the communities in which they will work. Local recruitment increases the motivation of HEWs and also enhances buy-in and acceptance of the program by the community they serve. HEWs must complete a one-year course of instruction and field training, provided by Technical and Vocational Education Training Schools (TVETs), and operated by the Ministry of Education. Upon completion of training, HEWs are assigned, in pairs, to kebeles where they staff health posts and work directly with individual families.
Implementation: HEWs provide health promotion, preventive and basic curative services by spending 75% of their time visiting families in their homes and performing outreach activities and the remaining 25% working at the health posts. HEWs also play a critical role as a referral system from the grassroots level to broadening access to the continuum of care at Primary Health Care Unit (primary hospital, health center and five health posts) and referral hospitals. Some of the services HEWs provide include routine immunization services, family planning education, maternal and child health services, HIV/AIDS, and malaria preventions. In addition, to address strong community demand
50 | P a g e
The HEP spans four technical areas & 16 packages of services:
A. Hygiene and Environmental Sanitation
Proper and safe excreta disposal system
Proper and safe solid and liquid waste management
Water supply safety measures Food hygiene and safety
measures Healthy home environment Arthropods and rodent control Personal hygiene
B. Disease Prevention and Control
HIV/AIDS prevention and control TB prevention and control Malaria prevention and control First AID
C. Family Health Services
Maternal and child health Family planning Immunization Adolescent reproductive health Nutrition
D. Health Education and Communication
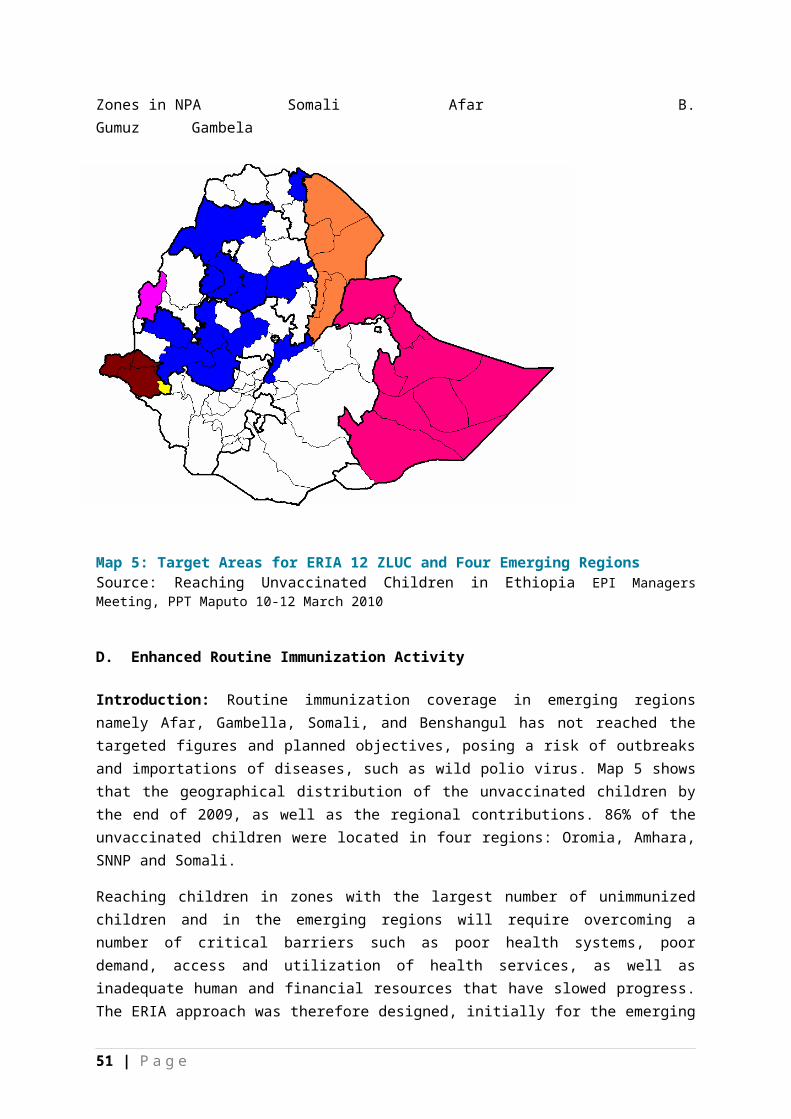
for basic curative care, HEWs are trained to provide first aid; treat malaria, dysentery, intestinal parasites, and other ailments; and to refer cases to the nearest health center when more complicated care is needed.
In order to enhance their health education efforts, HEWs enlist capable families previously involved in community work and train them as model households, adopting healthy behaviors that set a positive example for their neighbors. HEWs initially train 40-60 families in the Health Extension Package activities, followed by two more groups in order to collectively reach 360 families each year. At the conclusion of this training, families that implement 75% of the 16 packages will graduate and receive a certificate recognizing them as model families. Model families actively assist and encourage their family members and neighbors to implement the HEP packages by setting a positive example (4).
The baseline survey conducted by L10K on the impact of community-based services conducted between 2005 -2009 in four regions (Amhara, Oromia, SNNP and Tigray) demonstrates that household visits and establishing model households are effective HEP strategies that result in a significant increase in availability of latrines in household, number of LLINs in households, contraceptive prevalence rate, women receiving at least two ANC visits, neonatal tetanus protected childbirth, and fully immunized children. FMoH also acknowledges that most of the achievements made during HSDP III and IV are attributable to the implementation of the HEP with the support from partners.
Results Achieved: Different development partners including GAVI, UNICEF, WHO, USAID, and USAID partners (JSI, Pathfinder) supported the program and several remarkable achievements have been documented by partners. Some of which include, the unprecedented increase in contraceptive use from 15% in 2005 DHS is largely attributable to the health extension program (15), final evaluation of HSDP III (2005-2008) shows satisfactory performance of immunization attributed to HEP’s. In addition, HEWs have been shown to be successful by significantly improving coverage of bed nets, family planning, exclusive breastfeeding practices, and improved hygiene behavior. The involvement of HEWs has improved case detection and treatment success rates for TB in places with poor health service coverage, in southern Ethiopia. ANC coverage (for at least one visit) and neonatal tetanus protected births have also improved significantly. Iron supplements during pregnancy are improving, though it is not keeping pace with ANC (2).
Challenges: On the other hand, HEP found that it needs improvement in the following areas: HEWs rarely address health messages concerning pregnancy care, newborn care, and treatment practices for sick children. Coverage of some critical services, especially women’s access to safe and clean delivery, essential newborn care, postnatal care services for mothers and newborns, and management of childhood illness remains low. In particular, although institutional delivery has improved slightly; it was found to still be relatively low at 12%. In addition, deliveries assisted by HEWs are low even though the HEWs
51 | P a g e

are receiving in-service training. The low uptake in these services is due both to lack of HEW capabilities and lack of demand (2).
Conclusion: HEP is an innovative approach for achieving universal primary health care services especially by bringing health services closer to the community, increasing demand and utilization of health services at health facilities. However, this requires addressing the observed gaps in a collaborative manner.
B. Taking Long Acting Family Planning (LAFP) Implanon Insertion Service to the Community
Introduction: Ethiopia -the second most populous nation in Africa with a total population of over 80 million is due to the result of frequent childbearing or high fertility rates—often corresponding with a large unmet need for family planning (FP). In Ethiopia, women still have, on average, about 5.4 children each, and the unmet need for FP stands at 34%. To meet the unmet need for family planning in Ethiopia, all modern methods (from short acting to long acting) as well as permanent methods are available in the country. However, the shorter-term methods such as pills and injectable are mostly used. The access and utilization of Long Acting Family Planning (LAFP) methods is very limited especially among the rural communities since the provision of the service was limited to health centers and hospitals. In response to the growing demand for LAFP services among rural women in Ethiopia, FMoH launched HEWs training on Implanon insertion, a LAFP method. This was to be provided at Health Posts (HPs) level where the service was available to rural communities. Following this direction, the Integrated Family Health Program (IFHP) became the prime partner in training of HEWs and also providing consumables and other commodities to HPs during the post training intervention period. The objective of the training was to increase the contraceptive method mix and choices at the lower health care system, improve the national Contraceptive Prevalence Rate (CPR), and ultimately improve maternal well-being and family health.
Implementation: IFHP conducted the initial pilot training of HEWs in eight selected woredas of Oromia, Amhara, SNNP and Tigray regions of Ethiopia; and immediately backed it up with a post-training follow up assessment. The result of the training and follow up assessment was finally presented to the FMOH at a national review meeting on Implanon scale up. After the meeting, direction was given by the FMOH to nationalize Implanon insertion by HEWs. Based on the Ministry’s directive, IFHP scaled up the training in 140 woredas in the four mentioned regions.
Achieved Results: The decentralization of provision of LAFP-Implanon insertion service at health post level saves time and money and consequently the lives of especially rural women by bringing the service closer to them. It
52 | P a g e

added another much needed skill to the HEWs, improving their acceptance by their communities.
The project reports show that 571 health extension workers’ supervisors and 570 health professionals received training of trainers (TOT) on Implanon insertion to date. In the subsequent rollout trainings 3,772 HEWs were trained. During the practicum sessions of the TOTs 10,617 mothers received the service; similarly 28,910 and 110,970 mothers received it during and after the rollout trainings respectively.
It is IFHP’s belief that the trainings and material support it provided within its operation regions has contributed to the increment of the CPR from 15% in 2005 to 29% in 2011 and to the proportion of current implant users that increased from 0.1% in 2005 to 3.4% in 2011.
Preliminary analysis of data collected from 7,251 participants during practicum sessions of the trainings show that older women (34-44) and those with six or more children preferred long acting FP methods. Likewise, the high number of new accepters of implants shows the demand for LAFP methods in the face of limited contraceptive choices at the community level and demonstrates the appropriateness of the intervention (17).
Conclusion: Expanding Implanon insertion services to the health post level and shifting implanon insertion from health centers and hospitals to health posts increases access and utilization of long acting family planning methods and broadens the method mix at the community level, which will help to reduce untimed or unwanted pregnancies and their subsequent potential complications. It also reduces the time and money that would have been spent to travel long distances to get the service at health centers and hospitals. In general, increased contraceptive availability and use at health post level is a simple and cost-effective means of meeting the unmet need for family planning that will help Ethiopia to limit the rapid population growth and thereby positively impact socio-politico- economic and cultural aspects of rural community.(17)
III) Innovations and sustained successes in community involvement (in health and on volunteers for animal health)
Table 11: Innovations and sustained success in community involvment( in health and on volunteers for animal health or from agriculture)
53 | P a g e

Innovations in community involvement
Partner Location (if specific regions/zones/woredas available, list by partner working where)
Timeframe of innovation
Community Health promoters initiative - community volunteer are recruited to support government’s bold Health Service Extension Program: two paid female health extension workers in every community
JSI (ESHE), JSI (L10K),USAID(Pathfinder), MaNHEP ,SNL
ESHE – Amhara, Oromia, SNNPPathfinder & JSI Amhara, Oromia, SNNP, TigrayMaNHEP – Amhara & OromiaSNL – Oromia & SNNP
ESHE 2003-2008Pathfinder -2002L10K -2007 -2011ManHEP 2008-2011IFHP & pathfinder (2008-2013)SNL – 2007-2011
AFRM Africa project in Afar region have made significant positive impact in preventing and treating livestock disease using community based animal health workers(CAWHs).
FARM Africa Afar (Gewane, Amibara, Telalak woreda)
May 1998 to present
C. Innovative approach in community involvement - Voluntary Community Health Workers (vCHWs):
Introduction: vCHWs were initiated by GoE with technical support from Essential Services for Health in Ethiopia (ESHE II) a USAID funded project implemented through JSI between (2003-2008) in Amhara, Oromia and SNNP regions. The initiative is to support the government’s bold health service extension program by recruiting volunteers from the community to support HEWs. Later, JSI (IFHP) and Pathfinder created partnerships to build on the ESHE project and FP projects to create an integrated RH/MNCH program to support key interventions and health systems. vCHWs include Community-Based Reproductive Health Agents (CBRHAs), Trained Traditional Birth Attendants (TTBAs), Community Health Promoters (CHPs), and community volunteers for prevention of malaria and other health problems. ESHE project has established a network of 30,000 community health promoters (CHPs) in 101 woredas and Pathfinder works in 357 woredas and 60% of woredas overall, between these two programs.
54 | P a g e

Implementation: vCHWs are arranged in such a way that ten vCHWs support one HEW, to reach 500 households on six thematic areas (EPI, exclusive and complementary feeding, Vitamin A, Environmental sanitation and hygiene, Malaria and Family Planning) .vCHWs are selected using specific criterias such as being active, engaged community members, 50% women promoters, fair representation and diversity, geographic spread over the community) which helps to get buy-in and acceptance of vCHW by the community. vCHWs are motivated to work because they help their families in practicing healthy health practices first and teach their neighbours and as a result they become recognized in the community. vCHWs get 2 days training on action oriented phased training on communication skills, practice oriented, familiarizing with BCC materials and field practice promoting messages. The capacity of health extension workers also helps them to work with
community volunteers to reach more households. They also use family cards to teach parents how to provide care for children until they reaches age of two. This card also helps to harmonize health messages from HEWs and health community promoters. Successes are celebrated using nonfinancial incentives to encourage volunteerism and ensure the sustainability of the program. Some of the non-financial incentives were certification, provision of badges and IDs for high performing Volunteers, posting their photographs at public places etc….which serve as a NFI for sustaining the HEW program. HEWs are responsible to organize, train and supervise these volunteers as one coordinated group that supports their goals and further integrates understanding of healthy behaviors into the community. As the result of these efforts, the following major achievements have been obtained (3).
Achieved Results: The ESHE project trained more than 54,500 volunteer community health workers to assist HEWs – more than 12 million people were reached.
Findings show that in the three regions combined, DPT1 coverage increased significantly (p<0.0001) from 65% in 2003/04 to 75% in 2008 (27). The trend was not uniform across the three regions, however. In Amhara, there was a remarkable increase from 65% to 83%; in SNNP, from 62% to 76%. No such trend was noted in Oromia.DPT3/Penta3 coverage, being an indicator of EPI completion, has also shown an increasing trend in the three regions combined, from 46% to 57% during the period. Coverage and trend for measles are often confounded by campaign effects. In the three regions combined, measles coverage revealed that only a little more than half of children aged 12 to 23
55 | P a g e
Healthy actions VCHWsundertook and promotedincluded:• Antenatal care services• Essential newborn care• Breastfeeding• Fully immunizing children• Introducing complementaryfoods at six months• Modern family planning• Recognizing and seekingcare during illness• Insecticide-treated bed nets• Hand washing, safe waterstorage, and constructionand use of latrines

months had received measles vaccines. The trend remains nearly unchanged at 53% and 55% in 2003/04 and 2008, respectively. In Amhara and SNNP, positive significant temporal trends in measles coverage were also noted. A reversal trend seemed to occur in Oromia. On the whole, findings suggest that immunization coverage in the 101 ESHE-supported woredas combined showed significant improvement since 2003/04, although far short of the universal target of 80%. In addition, early initiation of very beneficial colostrum first breast milk increased from 46% to 72%. Pregnant women protected from anemia with iron foliate supplementation increased from 29% to 46% during the implementation period, in ESHE project implementation areas. The table below also demonstrates the added value of vCHW in improving immunization (PCG and DPT3) and Vitamin A Supplementation (27).
Table 12
Immunization & Vit A supplementation status of children 12-23 of age in village with and without vCHW in Ankasha district of Amhara region (2008)
s.n
Immunization & vitamin A
Village with CHWs (n)
Village with CHWS(%)
Village without CHWS
Village without CHWs (%) P- value
1 BCG152/225
67.6%118/ 225 52.40%
0.001*
2 DPT3197/225
87.5%178/ 228 78%
0.007*
3 Measles174/225
77.3%136/ 228 59.60%
0.005*
4 Vitamin A 281/317 88%266/ 315 84.40% 0.122
Source: Reaching Unvaccinated Children in Ethiopia EPI Managers Meeting, PPT Maputo 10-12 March 2010
Challenges: The short time between the introduction of pentavalent vaccines and the withdrawal of trivalent vaccines affected routine EPI coverage. Orientation of frontline health workers on pentavalent vaccines was delayed, resulting in late introduction of DPT-Hib-HepB vaccines. Inefficiency in operation and maintenance of refrigerators and lack of coordination among partners continues to affect EPI achievements.
Conclusion: vCHW and communities have a great potential to support the HEWs in primary health in rural Ethiopia mainly by improving demand for vaccinations among communities through model households, involvement in surveillance of VPSs (AFP, Measles, NNT etc.) to assist with tracking drop outs.
56 | P a g e

Hence, the health extension program should actively involve vCHWs community mobilization and behavioral change activities at household and community level.
D. Voluntary community involvement for animal health
Introduction: Community animal health workers (CAHWs) have been operating in Ethiopia for over two decades. In 2002 a participatory impact assessment team selected two projects, FARM Africa’s and Save the Children UK’s projects, to assess the impact of CAHWS on veterinary service, livestock morbidity, mortality and productivity and community perception about CAHWs and to draw key lessons for policy makers. Although both projects used innovative animal health apporaches, this summary shares the experience of FARM africa project. FARM africa is an NGO operating and implemeting a pilot pastoral development project in three woredas(Gewane, Amibara and Telalak) of Afar region.
Implementation: CAHWs project was designed in 1998 from a participatrory planning workshop that involved all stakeholders. The project used an unique extension appraoch, the mobile outreach camp(MOC), which operates every three months,
helped to create strong linkage between the community/stockowner and the project to enhance sense of ownership. Before starting the implementation of the program, the project had a community meeting and dialogue at the mobile camps (MOC) which significantly helped for securing and recruiting beneficial CAHWs. The project also facilitates a community action plan (CAP) that identify specific tasks and acitivities before the MOC moves to a different location and.
FARM Africa staff, in collaboration with veterinarian and Economic Development Social Service Office (EDSSO) veterinary staff, selected CAHWs using diffent selceiton criteria including: livestock owner, individuals recongnized and respected by the community, individauls not engaged in other populations in other occupation, being married and settled but still willing to move with the community and free from addiction. A two week training was provided to CAHWs by two veterinanrians from the project in collaboration with regional, zonal and woreda level (EDSSO) at MOC on vaccinations, deworming, treating infections, wound treatments, external parasites, eye treatment, castration and hoof trimming. CAHWs receive a certificate and a veternary kit worth of 2000 ETB. The assessment indicates that CAHWs work every day, in
57 | P a g e
Healthy actions VCHWsundertook and promotedincluded:• Antenatal care services• Essential newborn care• Breastfeeding• Fully immunizing children• Introducing complementaryfoods at six months• Modern family planning• Recognizing and seekingcare during illness• Insecticide-treated bed nets• Hand washing, safe waterstorage, and constructionand use of latrines
some cases nine hrs per day, and walk between 30 minutes to six hours to serve scattered villages.
They serve 6-10 villages in and out of their kebele. They also travel along with livestock during migration in search of food and water to areas very far area away from their residence. Despite the challenges CAHWs face, such as inadequate and inconsistent drug supplies at reasonable prices (which force them to purchase drugs at private stores at higher prices) and the lack of spare parts for their equipment, they are motivated to work and serve their community even with minium benefits (earned income and being able to treat their animal) and fullfil their commitment. They also feel that they have a social obligation to serve their community. CAHWs’ regular monitoring activity took place with FARM in collaboration with EDDSSO once every month. During their visit, they collect reporting sheet which summerize in the performance of CAHWs. There is also a monitoring committee at kebele level (clan leader, kebele chairman and elders) who monitor the performance of CAHWs and poor performing CAHWs can be suspended and the kit returend. The community pays for the service they receive from CAHWs. Should a consumer refuse to pay, he/she will be enforced to pay by the clan leaders.
Results: The findings of the assessment show that livestock diseases for which CAHWs are trained and equipped to treat have shown significant reduction during the intervention period (1998 -2002)resulting in reduction of cattle mortality. In addition, the results shows that CAHWs have reached pastoralists located far and remote coners where conventional veterinary service is totally absent. In such area CAHWs service delivery system is most appropriate and practical one, socially accepted and owned by the community. CAHWS also helped to increase reporting and quick response to emergencies, on time reporting of out breaks and increased utlization of moder veternary services( Government and CAHWs) as opposed to traditional healers.
Challenge: Although CAHWs were technically competent they became less motivated due to failutre to get quality drugs, incentives from participating in to vaccination campaigns and lack of morale supports. However the CAHW’s commitment and strong involvment from the community in the monitoring process made them effective. The quality of services have deteroriated in some woredas due to lack of technical support and proper supervison.
Conclusion: CAHWs has been an effective strategy of delivering quality animal health services in far and remonte of pastoralist areas by addressing the observed inadequacy drug supply and replenishment system and placement of improved incentives for CAHWs such as revising drug sell price(27).
58 | P a g e

VIII. QUALITY IMPROVEMENT WORK IN ETHIOPIAi. Geographic support for quality improvement for health – N/Aii. Innovations (best practices) and sustained successes in quality
improvement in health by agency
Table 13: Innovations and sustained successes in QI for healthInnovations in QI for health
Partner Location (if specific regions/zones/woredas available, list by partner working where)
Timeframe of innovation
Primary Health Care Unit (PHCU) Review Meetings improve MNCH/PMTCT Uptake
IntraHealth
Tigray Oct 2009
The Participatory Community Quality Improvement (PCQI)
L10K Tigray, SNNP, Oromia and Amhara??
2010
A. Primary Health Care Unit (PHCU) Review Meeting to Improve MNCH/PMTCT uptake
Introduction: According to the FMoH’s Annual Performance Report EFY 2003, of an estimated 90,311 HIV+ pregnant women in the country, only 8,365 (9.3%) received ARVs (complete), and only 4945 of an estimated 14,276 HIV+ newborns received PMTCT prophylaxis. This reflects both the low utilization of ANC services at health facilities and the high number of positive women lost to follow-up. In part, this was also due to low rates of institutional delivery remain low at an estimated 11%
The Community PMTCT project began in October 2009 and aims to improve the uptake of maternal health services as well as improve follow-up of HIV+ pregnant women and HIV-exposed infants until age two. A key intervention to strengthen the community follow-up and referral of HIV+ pregnant mothers and HEI has been strengthening the Primary Health Care Unit (PHCU) through technical and financial supports to conduct regular performance review/planning meetings. A PHCU comprises one health center with five satellite health posts, is led by the HC manager and is responsible for the performance on health indicators through the PHCU. The intention is the PHCU staff hold regular meeting to review the performance of the PHCU, exchange information, share experiences and transfer skills among the Health Extension Workers (HEWs) and health center staff.
While regulations exist that explain the composition, roles and responsibilities of various actors, little implementation guidance was provided to HC managers.
59 | P a g e

The CPMTCT project has provided both technical support and per diems for HEW in more distant sites.
Implementation: Discussions with RHB, WorHOs and HC managers to agree the type of support required and its duration with a view to regular meetings that can be sustained over time. IntraHealth has assisted the WorHOs in explaining the regulations that establish the PHCU mechanism, as well as providing technical assistance to HC managers and woredas regarding structuring the meetings using performance improvement methodologies. While the government’s recommendation is to hold monthly PHCU meetings, in some cases, due to distances and the need for transport allowances or per diems, meetings happen less frequently.
Monthly uptake of core MNCH services, supplies/drug availability, referral uptake, and the HIV+ mother and HEI tracking wall chart are reviewed at the PHCU meetings, causes for performance gaps identified and action plans developed. On the job training and informational updates also performed as needed, usually at the end of a session. For example, review for HEW of the normal/abnormal blood pressures for pregnant women, a review of FANC and the need for all pregnant women to visit the HC level at least once in their pregnancy, partograph (re)training for health center labor and delivery staff.
Using Tigray as an example, Intrahealth through the CPMTCT project supported 179 PHCU meetings at 44 health centers in the past year. Costs have included staff time and per diems for some of the meetings. The agreement with RHB is based on their assertion that they have or will have a budget for quarterly meetings, but request transport and/or per diem assistance for monthly meetings are needed initially to cement the PHCU and improve MNCH performance. IntraHealth shared costs but did not supported every meeting, 39 of the 44 health centers mentioned actually hold monthly meetings. Intrahealth proposes a budget of $320/year per health center for review meetings and to support HC supervision to HP level.
Results: While trend analysis in CPMTCT supported health centers shows a steady increase in service utilization (ANC, SBA, C&T of pregnant women, male partner testing), this is not only a result of the PHCU meetings. More directly related to the meetings is the increased uptake -- whether at CPMTCT supported health center which generally do not offer HAART, or other facilities, of ARV prophylaxis for mothers and HEI. In Tigray, 91% of eligible HIV+ pregnant women received ARV prophylaxis/HAART. Of 194 HIV+ pregnant women identified in the year, only 19 are lost to follow-up, 22 were under 28 weeks at last data point, 153 received ARV prophylaxis/HAART. Not including those who have changed addressed or refused follow-up, there have been 110 deliveries in the past year among HIV+ women, 107 at a facility and three in the home, 98 of the infants are reported to have received ARV prophylaxis.
Conclusion: The HC staff and HEWs find the PHCU meetings an opportunity to improve their knowledge/skills on MNCH/PMTCT and related topics. The PHCU is found to be an important forum to have common and shared catchment plans
60 | P a g e

PCQI’s Primary Objective
To improve the quality of community maternal and neonatal health care services by:
- Creating a shared sense of responsibility among the community members and health providers for better health services;
- Stimulating demand for and utilization of quality services; and
- Empowering communities to take initiative and responsibility to improve
and increase performance in terms of service uptake and the continuum of care such as linkages of HIV+ women and HEIs for getting subsequent services, and efficient management of supplies/commodities at Health Centers and Health Posts levels. For example, lost-to follow-up among HIV+ mothers and HEI has been reduced as have stock outs and wastage of drugs and other supplies. With minimum technical and financial support from CPMTCT project, it found to be such a sustainable practice that many of the PHCUs started regular monthly performance review by themselves.
In order to be more comprehensive and sustainable, it will be wise to prepare coordinated plan it all developmental partners operating the catchments of the respected PHCU, monetary or non-monetary recognition for good performers at least once a quarter to create sense of healthy competition and increase eagerness among staff based on concrete criteria during the meeting; and sharing experiences among other strong PHCUs, especially on facilitation and planning skills to managers and HEP supervisors.
Different sorts of tracking tools have existed at health center level for some time, but until the PHCU there hasn’t been a mechanism to share information about referral uptake, defaulters and follow-up. The review meetings provide this forum. Provided that it is affordable and with a minimal level of technical support, these review/planning meetings can be institutionalized for HC managers/ PHCU
B. Innovation The Participatory Community Quality Improvement (PCQI)
Introduction: Participatory community quality improvement (PCQI) is an approach implemented by the Last Ten Kilometers (L10K) Project (JSI in Ethiopia) to improve quality and accessibility of health care through greater
involvement of the community and Health Extension Workers (HEWs). Using this approach, community members and HEWs are involved in defining, implementing and monitoring the quality improvement process.
Implementation: PCQI is being piloted in 90 kebeles (sub-districts) in 14 L10K-supported woredas (districts). Within each of these woredas, PCQI is being implemented in one or two health centers, each linked with five to ten health posts. Each health post serves a population of approximately 5000 people. Similar to other community-based quality improvement approaches, PCQI relies on
61 | P a g e

the involvement of community members. First, the community members are critical to identifying the main bottlenecks and barriers to the access and quality of services. Second, community members have the responsibility of monitoring and targeting improvements for the quality of services at the community level and at health posts. Every quarter, meetings are held in each participating kebele. In these gatherings, community members identify areas for improvement of access to services and quality of service provision, and also suggest possible adjustments and advances in these problem areas. HEWs also meet quarterly to discuss the quality issues identified by the community. Then, representatives from each of the above mentioned meetings share their findings through a “Bridging the Gap” workshop, and then establish a Quality Improvement team and a clear plan of action to improve access to and quality of services provided.
Achieved Results: Less than a year into the implementation of PCQI, outcomes are not yet quantifiable. However, a number of positive changes have been observed using the ‘Most Significant Change’ technique 1. Some of the barriers to better access to and quality of care identified through the PCQI process include: harmful traditional beliefs, lack of access to services by pregnant and laboring women, lack of services available at night, and HEWs’ insufficient practical experience assisting with deliveries. While each community has developed its own strategies to mitigate these challenges, some common themes have emerged.
The PCQI process has been instrumental in increasing the involvement of, and sense of responsibility for, the health services provided for the community. This has resulted in a number of community-driven initiatives. Examples include: a firm commitment to the maintenance and improvement of roads leading to clinics, building stretchers to carry laboring or sick women to health facilities, building HEW lodging near health facilities to enable them to provide emergency services during the night, and a pooling of funds to buy supplies such as a bed and linens for the health posts. In at least one woreda, youth associations have been recruited to assist in transporting laboring women to the clinic.
To address the lack of understanding in regards to the services provided by the clinic, orientation sessions were conducted at clinics to provide community leaders and members of the general public a better understanding of the services offered at the clinics, as well as the standards of care that these individuals can expect to receive. In addition, religious leaders and teachers were trained to provide messages condoning harmful practices and to promote the use of health clinics.
Finally, to address the potential skill gap of HEWs to perform safe deliveries, Quality Improvement teams organized learning exchange visits for HEWs. Visits were conducted to larger health centers that specialize in maternal
1
62 | P a g e
care so as to provide practical experience for the HEWs in delivery and immediate newborn care. On-the-job mentoring is also encouraged and provided.
Conclusion: Less than a year into its implementation, the PCQI approach has noticeably increased community involvement in and responsibility for health service delivery. This involvement has resulted in tangible improvements such as the commitment of community resources for the procurement of beds and stretchers for transporting laboring women, as well as noticeable bettering of infrastructure at the community level (including roads to health facilities). It is anticipated that the PCQI approach could yield similar results in other resource poor settings. Further, this process has helped ensure that HEWs improve their skills in safe delivery through practical experience working with experienced staff at specialized maternal health centers.
In the coming months, JSI will continue to implement the PCQI approach, and will focus on evaluating and documenting the process to further identify and apply lessons learned. Baseline data on service utilization, quality of services, and health outcomes have been collected, and these measurements will be repeated to assess for changes in these outcomes) (16).
REFERENCES:
1. ARISE. (2009). Routine Immunization Situation Analysis. Arlington, VA: JSI Research & Training Institute, Inc.
2. Bill & Melinda Gates foundation. (2009). The Ethiopian Health Extension Program: A Synthesis of Findings, Gaps and Recommendations.
3. Carnell, M. (2005). Jump-starting the rapid scale-up of community health promotion in Ethiopia. ESHE project.
4. Ethiopia’s Health Extension Program: Pathfinder International’s support 2003-2007, February 2008
5. Ethiopian Health Sector Development III( 2005/06 -2010/11), Mid Term Review. (2008). Volume I component report, Addis Ababa: Retrieved Dec 28, 2011 from http://www.med.or.jp/english/journal/pdf/2009_04/279_286.pdf.
6. Experience of Afar Region in Enhanced Routine Immunization Activities (PPT presentation)
7. Ethiopian Federal Ministry of Health. National Child Health Strategy for Ethiopia. Family Health Department.
8. Ethiopian Federal Ministry of Health. (2009). Comprehensive Multi-Year Plan 2010 -2014, Addis Ababa.
9. Ethiopian Federal Ministry of Health, WHO, UNICEF, Report on assessment of Health provision among Pastoralist Communities in Ethiopia, August 2011
10. Ethiopian Federal Ministry of Health. (2010). Enhanced Routine Immunization (ERIA) Guideline.
63 | P a g e
11. Integrated Family Health Program. Ethiopia & BIG/DC Monthly Meeting, February 24, 2010.
12. Ethiopia Country Report. (2007). In Depth Evaluation of the Reaching Every District Approach to improving Routine Immunization.
13. L10K. Impact of Community Based Primary Health Care Program in Ethiopia. Addis Ababa, Ethiopia: JSI Research & Training Institute, Inc.
14. L10K. (2009). Baseline House hold survey report, Amhara, Tigray, Oromia, SNNP. Addis Ababa, Ethiopia: JSI Research & Training Institute, Inc.
15. L10K. Baseline House hold survey summary Report. Addis Ababa, Ethiopia: JSI Research & Training Institute, Inc.
16. L10K. (2011). Brief outlines the Participatory Community Quality Improvement Approach (PCQI) that L10K is implementing in select woredas in Ethiopia.
17. Scaling up of community Based Delivery of Implanon. (2010). John Snow Inc. & Pathfinder International.
18. L10K. (2009). Community Health Workers: Exploring Volunteerism as a sustainability model: Policy Brief Vol. 1 January 2009.
19. L10K. (2009). Trend in Reproductive, Maternal, Neonatal and Child Health indicators areas, Tigray Region 2005-2009. Addis Ababa, Ethiopia: JSI Research & Training Institute, Inc.
20. Ethiopian Ministry of Health. (2004). National Strategy for Child survival in Ethiopia. (final draft)
21. Ethiopian Federal Ministry of Health. (2011). Annual Performance Report HSDP IV (2010/11). Policy, Planning and Finance General Directorate.
22. Ethiopian Federal Ministry of Health. (2011). Health Sector Development Program (HSDP IV). Policy, Planning and Finance General Directorate.
23. Afar Pastoralist Development Association. (2009). Reaching Pastoralist communities with vaccination, Paper detailing Afar Pastoralist Development Association experience from 2005- 2009.
24. Reaching Unvaccinated Children in Ethiopia EPI Managers Meeting: Maputo, 10-12 March, 2010.
25. The Government of Federal Democratic Republic of Ethiopia. (2001). Proposal for support submitted to the Global Alliance for Vaccines and Immunization (GAVI) and vaccine Fund.
26. Sahlemariam, Y. Integration of child survival interventions in Ethiopia to reach MDG, 3rd Global immunization Meeting: 19-21 February, 2008.
27. http:// www.eshe.org.et28. Ethiopian Impact Assessment Team. (2002). Impact assessment of
community based animal health workers in Ethiopia.29. ERIA Review Meeting: Nov 18, 2010.30. http://www.coregroup.org/our-technical-work/initiatives/polio/188-
ethiopia31. http://www.ccrdaethiopia.org/index.php?
option=com_content&view=article&id=56&Itemid=141
64 | P a g e

32. http://www.clintonhealthaccess.org/program-areas/maternal-and-child- health/vaccines
33. USAID. Final Report of Essential Health Services in Ethiopia November 2003 - September 2008.
34. Reaching unimmunized children: Ethiopian Experience, EPI Managers’ Meeting for Eastern and Southern Africa. Mombasa, Kenya: 18-20, March 2009.
35. World Health Organization. (2011). Overview of Routine Immunization Performance.
36. National Child Survival Strategy Document July 2005.
65 | P a g e