ulcerative colitis: current management strategy
TRANSCRIPT
7 : 7
ABSTRACT
The primary goals of therapy in the treatment of ulcerative colitis (UC) are to induce remission of patient symptoms as rapidly as possible and maintain remission on a long-term basis. New formulations of mesalazine and corticosteroids show promise in improving compliance and efficacy. There is consistent evidence for the role of cyclosporine in severe UC and expanding evidence for thiopurines in refractory UC. Clinical trials demonstrating the benefit of infliximab in acute severe and chronic active UC have provided insights into the pathogenic inflammatory pathways. The future for the management of UC appears promising as new therapies continue to be added to the treatment armamentarium, and strategies incorporating current and novel therapies continue to evolve.
ULCERATIVE COLITIS: CURRENT MANAGEMENT STRATEGY
Sanjay Bandyopadhyay, Kolkata
Key words : Ulcerative colitis, management, mesalazine, corticosteroids, thiopurines, infliximab.
INTRODUCTION
Ulcerative colitis (UC) is a relapsing non-transmural inflammatory disease that is restricted to the colon (1). Dependent on the anatomic extent of involvement, patients can be classified as having proctitis, left-sided colitis (involving the sigmoid colon with or without involvement of the descending colon), or pancolitis. A few patients also develop ileal inflammation (called backwash ileitis), which occasionally complicates differentiation from Crohn’s ileocolitis (Table 1). Patients typically present with bloody diarrhea (often nocturnal and postprandial), passage of pus, mucus, or both, and abdominal cramping during bowel movements. Severe symptoms are less common in left-sided colitis and proctitis (1).
DIAGNOSIS
UC is a clinical diagnosis, confirmed by objective findings from endoscopic and histological studies. Non-inflammatory bowel
Table 1: Differential diagnosis of ulcerative colitis and Crohn’s disease
Table 2 : Non-inflammatory bowel disease causes of enteritis and colitis
Ulcerative colitis Crohn’s diseaseClinical featuresHaematochezia Common RarePassage of mucus or pus Common RareSmall-bowel disease No (except back-
wash ileitis)Yes
Can affect upper-gastrointestinal tract
No Yes
Abdominal mass Rare Sometimes in right lower quadrant
Extraintestinal manifestations Common CommonSmall-bowel obstruction Rarely CommonColonic obstruction Rerely CommonFistulas and perianal disease No CommonBiochemical featuresAnti-neutrophil cytoplasmic antibodies
Common Rarely
Anti-saccharomyces cerevisiae antibodies
Rarely Common
Pathological featuresTransmural mucosal inflammation No YesDistorted crypt architecture Yes UncommonCryptitis and crypt abscesses Yes YesGranulomas No Yes, but rarely in
mucosal biopsiesFissures and skip lesions Rarely Common
Infectious• Bacterial : Campylobacter spp, Salmonella spp, Shigella spp, Clostridium dif-
ficile, Escherichia coli (enterotoxigenic E coli), Yersinia spp (especially in Crohn’s disease), gonococci, Chlamydia trachomatis, Mycobacterium tuber-culosis, atypical mycobacteria
• Parasitic : Entamoeba histolytica, Cryptospora spp, Isospora spp, Trichuris trichura, strongyloidis
• Viral : cytomegalovirus, herpes simplex (in proctitis), HIV• Mykotic : Candida spp, Aspergillus sppNon-infectious• Inflammatory : diverticulitis, microscopic colitis (collagenous and lympho-
cytic), eosinophilic gastroenteritis, graft vs host disease, radiation related, Behçet’s syndrome, sarcoidosis
• Toxic : postoperative diversion colitis, bile acid loss, non-steroidal anti-inflam-matory and other drugs, laxative use or abuse, antineoplastic chemotherapy
• Malignant : colorectal cancer, small-bowel cancer, neuroendocrine tumors, lymphoma, metastatic neoplasms
• Vascular : ischaemic colitis, vasculitis
Medicine Update 2010 Vol. 20
498
the severity of colitis (Table 5) (4). Endoscopic findings do not always correlate with clinical symptoms. Although therapeutic decisions are based primarily on clinical status, it may be useful to follow sigmoidoscopic mucosal appearance over time in an individual patient if the clijnical response to treatment is uncertain.
Two important subgroups are the patients with fulminant colitis and toxic megacolon. Patients with severe colitis who appear toxic, with fever higher than 1010F, tachycardia, abdominal distension, signs of localized or generalized peritonitis, and leukocytosis, are considered to have fulminant colitis. Toxic megacolon is said to occur when there is radiological evidence of colon dilation to greater than 6 cm in an acutely ill patient (5). Both these conditions are diagnosed clinically and endoscopic examination should be avoided in severe colitis because of the risk of inducing megacolon or perforation.
The Montreal classification of disease extent of ulcerative colitis allows the extent to be defined into three subgroups (Table 6) (6). The subclassification was felt to have clear biological relevance in terms of the response of patients to medical therapy (differential response to topical therapy), and also to be validated by the natural history of the disease, with respect to rates of medication usage, hospitalization, or colectomy. Moreover, the risk of colorectal malignancy was also felt to provide further
disease causes of colitis need to be ruled out (Table 2).
ASSESSMENT OF DISEASE ACTIVITY
Assessment of disease activity is important for prognostication and therapeutic decision making. Several instruments have been developed to allow standardized evaluation of disease activity for UC. Although none is accepted universally as standard, one of the most commonly used for this purpose is that of Truelove and Witts (Table 3) (2). This classification categorizes patients into mild, moderate, or severe disease. This classification is reliable and simple to use in clinical practice, although it is most applicable for patients with extensive colitis and may not adequately reflect disease severity in patients with limited colitis. Additionally, it does not take into account endoscopic findings.
A numerical disease activity instrument that is more useful for patients with limited disease and for conducting clinical trials is the Ulcerative Colitis Disease Activity Index (UCDAI) (Table 4) (3). This disease activity index ranges form 0 to 12, with the higher total scores representing more severe disease. In general, a patient is considered to be in remission if UCDAI is equal or less than 2, and to have severe disease if the score is greater than 10. Clinical response is generally reflected by a decrease by 3 points from the patient’s initial baseline score.
There also are many endoscopic and histologic scales of grading
Table 3 : Truelove & Witts classification of disease severity
Table 4: Ulcerative colitis disease activity index
Table 5 : Endoscopic criteria for assessment of disease activity
WallA. Superficial ramifying blood vessels : normal throughout ; patchy; noneB. Spontaneous bleeding ahead of instrument : non; presentC. Bleeding to light touch (friability) : none; presentD. Granularity : normal smoothness ; granularE. Mucosal surface : normal mat ; dull, lusterless ; wet and shinyF. Ulceration : no ulcers; ulcersG. Valves : normal thin sharp crescent ; swollen; absentGrading of “Activity”(0) Normal : mat mucosa, ramifying vascular pattern clearly visible
through out, no spontaneous bleeding, no bleeding to light touch.(1) Abnormal but not haemorrhagic : appearances between (0) and (2).(2) Moderately haemorrhagic : bleeding to light touch, but no spontane-
ous bleeding seen ahead of instrument on initial inspection.(3) Severely haemorrhagic : spontaneous bleeding seen ahead of instru-
ment at initial inspection, and bleed to light touch.
Table 6: Montreal classification of extent of ulcerative colitis
Extent AnatomyE1 Ulcerative proctitis Involvement limited to the rectum
(that is, proximal extent of inflam-mation is distal to the rectosigmoid junction
E2 Left sided UC (disal UC) Involvement limited to a propor-tion of the colorectum distal to the splenic flexure
E3 Extensive UC (pancolitis) Involvement extend s proximal to the splenic flexure
Symptoms Mild Activity Severe ActivityDaily BMs < 4 >6Rectal Bleeding infrequent frequentTemperature normal normal to elevatedHeart Rate <90 bpm >90 bpmHemoglobin >10gm/100mL <10g/100mLSedimentation Rate <30 mm/h >30 mm/h
1. Stool frequency 0-3: normal1-3: 1-2 stools daily > normal2-3: 3-4 stools3-3: 4 stools
2. Rectal bleeding 0-3: None1-3: Streaks of blood2-3: Obvious blood3-3: Mostly blood
3. Mucosal appearance 0-3: normal1-3: Mild friability2-3: Moderate friability3-3: ExudationSpontaneous bleeding
4. Physician’s rating of disease activity 1-3: Normal2-3: Mild3-3: Moderate4-3: Severe
Maximum score 3

Ulcerative Colitis: Current Management Strategy
499
Table 7: Different 5-aminosalicylic acid formulations and their sites of delivery
Generic name Proprietary name Formulation Sites of delivery Unit strengthMesalazine North American Asascol* Eudragit-S coated tablets (release at pH≥ 7.0) Termibnal ileium, colon 400 mgMesalazine Asacol 800 Eudragit-S coated tablets (release at pH≥ 7.0) Terminal ileum, colon 800 mgMesalazine Mesavant (EU), Lialda (USA)
(SDP 476)Advanced, multimatrix system Terminal ileum, colon 1200 mg
Mesalazine UK, Italy, Netherlands Asacol†
Eudragit-S coated tablets (release at pH≥ 7.0) Terminal ileum, colon 400 mg
Mesalazine Salofalk‡, Mesasal, Cla-versal‡
Eudragit-L coated tablets (release at pH≥ 6.0) Distal ileiu, colon 250 mg, 500 mg
Salofalk Granu-Stix‡ Eudragit-L100, polyacrylate dispression, providone K (Eudragit-NE 40 D, Nonixinol/100), simetikone
80% colon, sigmoid, rectum
500 mg, 1000 mg
Claven Micropelle§ Eudragit L-100-55, Eudragit S-100, dispersible cellulose Ileocaecal valve colon, left-sided colon
1500 mg
Claversal Foam§ Eudragit L-100-55, Eudragit S-100, dispersible cellulose 5 g foam (1000 mg 5-ASA)
Mesalazine Pentaza¶ Ethylecullose-coated microgranules (time dependent release) available as a tablet, capsule or sachet
Duodenum, ileum, colon 250 mg and 500 mg tablets; 500 mg capsules; 1000 mg sachets
Olsalazzine Dipentum 5-aminosalicylic acid dimer linked by azo-bond, available as a gelatin capsule
Colon 250 mg
Sulfasalazine Azulfidine, Salazopyrin 5-aminosalicyclic acid linked to sulapyrndine by azo-bond available as a tablet
Colon 500 mg (200 mg 5-ASA)
Sulfasalazine Azulfidine/Salazopyrin EN-tabs
5-aminosalicyclic acid linked to sulfapyridine by azo-bond, available as a tablet coated with cellulose acetate phthal-ate
Colon 500 mg (200 mg 5-ASA)
Balsalazide Colazide, Colazal 5-aminosalicyclic acid linked to 4-aminobenzoyl-ß-alanine by azo-bond, available as a capsule
Colon 750 mg (262 mg 5-ASA)
5-ASA-5 aminosalicyclic acid. *North Amrican Asacol: originally developed by Tillotts Laboratories. Co,lpermin, UK (later changed name to Tillotts Pharma AG, Ziefen, Switzerland), theen Norwich Eatopn, Norwich, NY, USA, currently Procter and Gamble, Cincinnati, Ohio, USA. Marketed by Procter and Gamble in North America. Manufactured with original Tillotts Laboratories manufacturing process. †UK, Italy, Netherlands Asacol: purchased from Tiltoss Laboratories by Smith Kline French Laboratories (later changed name to Smith Kline Beecheam and then GlaxoSmithKline), Gluliani, and Byk-Gulden. Differences might exist in Eudragit-S coating thickness excipients, and manufacturing processes. No published data establishing the bioequvalence of North American Asacol and UK, Italy, Netherland, Asacol. ‡Manufactured by Dr Falk Pharma in Germany. §Manufactured by Merckle Recordati in Germany. ¶United States Pentasa: 250 mg capsule from Shire Pharmaceuticals (previously developed and marketed by Marion Laboratories, which later merged into Hoechst-Marion-Roussel, then Aventis and now Sanofi). Pentasa is manufactured and distributed by Ferring Pharmaceuticals.
validation for this subclassification. The major drawback of the extent-based classification system was clearly identified to be instability of disease extent over time, once again underlining the dynamic nature of inflammatory bowel disease (6).
NATURAL HISTORY
The distribution of disease activity in a cohort of patients is remarkably constant each year (7). Half of the patients are in clinical remission at any given time, although 90% have an intermittent course. In the first 3-7 years after diagnosis, 25% patients are in remission, 18% have activity every year, and 57% have intermittent relapses. The only significant predictor of remission or relapse is disease activity in the preceding year. After 10 years, the colectomy rate is 24%. (7) More than half the patients with left-sided colitis will progress proximally during 25 years. During the same period, patients with more extensive disease regress in about 75% of cases (8). Overall, patients with UC have a normal life expectancy (9).
CURRENT MANAGEMENT STRATEGY
UC remains a chronic disease without a pharmacological cure that usually requires regular, indefinite therapy to maintain remission. There is now an expanding array of treatment options available to clinicians. Induction and maintenance of remission, mucosal healing, the avoidance of surgical intervention, and decreasing the likelihood of cancer developing are the primary therapeutic goals in UC (10). Treatment is dependent on several important factors, including the anatomical extent of disease (proctitis, proctosigmoiditis and left-sided colitis, and extensive or pancolitis), the severity of disease (mild, moderate, severe, fulminant), disease chronicity (acute as opposed to chronic active), and disease complications (10). Treatment should be individualized based on a patient’s previous symptom response, tolerance to specific medical therapies, and quality of life (11). Therapy is sequential, first to treat acute disease, then to maintain remission. Even with the advent of new therapies surgery should be considered in patients with disease refractory to medical therapy, for certain life

Medicine Update 2010 Vol. 20
500
threatening complications, and in those with multifocal dysplastic lesions or malignancy (10).
MILD-TO-MODERATE ACTIVE COLITIS
5-aminosalicylic acid (5-ASA) or mesalamine remains the treatment of choice for the induction of remission in patients with mild-to-moderate active UC (12). 5-ASAs are available in a wide range of formulations with different release characteristics; differences in drug delivery may account for the variability in efficacy and tolerability among different formulations (Table 7) . 5-ASA is also the mainstay of maintenance therapy (13). Patients who take oral 5-ASA regularly are nearly 6 times more likely to experience regression in disease severity than those who did not, suggesting a disease modifying role of 5-ASA in UC (14).
INDUCING REMISSION:
In patients with mild-to-moderately active proctitis, rectal 5-ASA (enemas, foams, or suppositories), or rectal corticosteroids are established first-line therapies. In this setting, rectal 5-ASA is more effective than both rectal steroids, and oral 5-ASA (15). Suppositories target the site of inflammation and are more appropriate than enemas in proctitis.
Patients with active distal or left-sided colitis can be treated with rectal 5-ASA, oral 5-ASA, or a combination of the both. Rectal therapies have a more rapid effect than oral treatment. Rectal 5-ASA is superior to to conventional rectal corticosteroid for inducing remission of symptoms, endoscopy, and histology of distal UC (15). Combination therapy with oral and rectal 5-ASA may achieve higher remission rates than either therapy
alone (16). Rectal budesonide is of comparable efficacy to conventional corticosteroids but produces less endogenous cortisol suppression (17).
In patients with mild-to-moderate extensive disease, the addition of a 1-g mesalamine enema each night to oral mesalazine produces higher remission rates (18).
The optimal dose of 5-ASA to induce remission for active distal disease is 1 g/day for rectal administration, and 2–4.8 g/day for oral administration (19). Patients who do not respond to an initial course of oral 5-ASA and/or rectal therapy should be treated with oral prednisolone in a dose ranging from 40 mg per day up to 1 mg/kg per day or equivalent (19). Steroids with colonic release properties and reduced systemic bioavailability such as beclomethasone diproprionate or budesonide are now available.
MAINTAINING REMISSION:
Up to 90% of patients can be maintained in remission using oral once-daily 5-ASA therapy (19). For maintaining remission of distal UC and proctitis, rectal 5-ASA is significantly better than placebo and at least as effective as oral 5-ASA (17). If patients relapse enquiry should be made about drug compliance. If further therapy is required the combination of a 5-ASA enema twice weekly with oral 5-ASA 1.6 g daily has been shown to be more effective than oral treatment alone (20). There is also preliminary evidence that time spent in remission is longer when the 5-ASA maintenance dose is increased from 1.2 to 2.4 g daily. Patients with extensive colitis benefit most from an increase in dosage (21).
Fig. 1 : Treatment algorithm for patients with mild-to-moderate active colitis
*Moderately active disease

Ulcerative Colitis: Current Management Strategy
501
5-ASA DOSE AND FORMULATIONS:
The American and European treatment guidelines recommend 5-ASA 2–4.8 g daily and 2–4 g daily, respectively, as an effective dose for the induction of remission for UC (22,23). 5-ASA is available in a number of oral and rectal formulations (Table 7). Most of the available 5-ASA formulations have demonstrated equivalent efficacy in left-sided and extensive disease.
DOSE FREqUENCY:
Once daily 5-ASA therapy is as effective as more frequent dosing in the induction and maintenance of remission of UC (10).
DOSE ESCALATION:
Patients who fail to achieve remission following initial 5-ASA therapy normally have their 5-ASA doses increased (19). Earlier clinical trials comparing the efficacy of different doses of various mesalamine preparations in patients with mild-to-moderate active colitis showed no difference in efficacy (24). However, data from ASCEND study suggest that more intensive therapy (i.e., higher doses) introduced at an earlier stage of moderately active disease may be beneficial (25). Higher doses are associated with increased absorption and greater systemic levels of 5-ASA, although this has not led to any apparent increase in adverse effects.
A treatment algorithm for patients with mild-to-moderately active colitis is shown in Figure 1.
REFRACTORY OR CHRONIC ACTIVE ULCERATIVE COLITIS
Approximately 10%–20% of patients with UC have chronic active disease without achieving clear periods of remission (10). Such patients may achieve remission with systemic steroids, but symptoms often relapse during steroid tapering or soon after their discontinuation (26). Other patients have frequently recurrent episodes of acute colitis, despite adequate 5-ASA therapy. Such patients with chronic active disease and frequently recurrent active disease, in addition to those who have severe disease requiring induction therapy with cyclosporin, can often be successfully treated and maintained on remission with azathioprine (AZA) or 6-mercaptopurine (6-MP) (10).
Azathioprine and 6-Mercaptopurine:
Despite the widespread use of AZA and 6-MP for the treatment of patients with UC, the data supporting such use remain limited. Uncontrolled experience has suggested a benefit (27), but controlled trials have yielded conflicting results (28). Several studies have shown a beneficial steroid- sparing effect of AZA with doses ranging from 1.5– 2.5 mg/kg daily for six months, but the beneficial effects became less clear with longer follow-up (29).
Although AZA and 6-MP are slow in their onset of action, they can contribute to rapid mucosal healing and early induction of remission in pateints treated with steroid (30). AZA maintenance treatment for UC is beneficial for at least 2 years in patients
who achieve remission while taking the drug, but not in those with chronic active disease despite being on AZA. No controlled trial of 6-MP for UC has been conducted, and no study has been performed to compare the efficacy of AZA with 6-MP in patients with UC.
Patients who continue with AZA or 6-MP are less likely to experience a relapse than those who had placebo (31). The most effective doses appear to be AZA 2–3 mg/kg and 6-MP 1–1.5 mg/kg daily, although there has not been a direct comparison of different dose levels (10). In addition, there has been no comparison of initial dose escalation to the weight-based dose or starting at the full maintenance dose. Thiopurines are the most widely used therapy in steroid- dependent disease and are often the recommended therapeutic option before considering surgery, as published in most current guidelines (19,23).
Allopurinol in AZA or 6-MP non-responders:
Failure to respond to thiopurines can relate to non-adherence, inadequate dosing, or the preferential metabolism of the drug to the metabolite 6-methylmercaptopurine (6-MMP), resulting in insufficient amounts of the presumed active metabolite 6-thioguanine (6-TG). Use of allopurinol in AZA or 6-MP non-responders can divert the metabolism of 6-MP toward 6-TG resulting in significant reduction in the prednisolone dose and normalization of aminotransferase levels (32).
Second-line immunomodulator therapy:
Tacrolimus, a calcineurin inhibitor with mechanism of action similar to cyclosporin, has been studied in UC and has the advantage of more predictable absorption and fewer side effects than cyclosporin. Oral tacrolimus can be an alternative effective option in patients with UC refractory to conventional therapy in the short- and medium-term (33). However there are limited data on the long-term outcome of patients on tacrolimus. It can also be used as a bridge to thiopurine therapy, due to its rapid onset of action, usually 2-4 weeks.
Methotrexate:
The only double-blind placebo-controlled trial using oral methotrexate at a dose of 12.5 mg per week showed no therapeutic benefit when compared with placebo (34). More comparative studies with different doses and different routes of administration are required before any definite conclusions can be drawn.
6-thioguanine (6-TG):
6-TG, one of the active metabolite of AZA and 6-MP, has been used as an alternative in selected patients who are intolerant of, or have failed, other immunosupressive therapies. Such use would necessitate use at a low dose with close monitoring of metabolite levels and liver function tests (35). Occurrence of hepatic nodular regenerative hyperplasia during 6-TG therapy may be dose-dependent.

Medicine Update 2010 Vol. 20
502
Infliximab:
Two large randomized placebo-controlled trials, the Active Ulcerative Colitis Trials 1 and 2 (ACT 1 and ACT 2), have evaluated the efficacy of infliximab for the induction and maintenance of remission in more than 700 patients with moderate-to-severely active UC in the outpatient setting. Intravenous infliximab at a dose of 5 mg/kg given at 0, 2, and 6 weeks was effective at inducing clinical remission, improving mucosal healing, and providing a steroid-sparing effect. Clinical and endoscopic improvement was reported in 60%–70% of the treated population, compared with 40% in the placebo-treated group. Infliximab was also associated with significant reductions in UC-related hospitalizations and surgical procedures. There was a 43% reduction in the colectomy rate associated with infliximab, compared with placebo, at 54 weeks (36).
The long-term efficacy of infliximab in UC needs to be confirmed in further studies, and whether the early use of infliximab prevents colectomy in the long term requires further evaluation (37). A systematic review evaluated the efficacy of infliximab in the treatment of patients with moderate-to-severe UC refractory to corticosteroids and/or immunomodulators. Infliximab was effective in inducing clinical response and clinical remission, promoting mucosal healing, and diminishing the need for colectomy in the short term (38).
Fig. 2: Treatment algorithm for the management of chronic active ulcerative colitis
Other novel therapies:
Leukocute apharesis
Leukocyte apheresis, an extracorporeal leukocyte removal therapy, is thought to suppress inflammation by removing circulating activated leukocytes and inflammatory mediators from the blood. Selective apharesis may be effective as a steroid-sparing agent particularly on induction, but not for the maintenance of remission (39). Randomized controlled trials have failed to confirm the results of open-label series and further evaluation may be required (40).
Probiotics
Probiotics appear to be beneficial adjunctive therapies in patients with chronic active disease. VSL#3 and Saccharomyces boulardii have been shown to be effective in inducing remission of mild-to-moderate active UC (41). In terms of disease maintenance, E. coli Nissle 1917 was shown to be equivalent to mesalazine including in-patients who were treated after an acute episode of UC, and VSL#3 was effective in maintaining remission in patients who were intolerant or allergic to 5-ASA (42,43).
Curcumin (Termeric)
Curcumin is a biologically active natural phytochemical substance present in turmeric and has antiinflammatory and antioxidant

Ulcerative Colitis: Current Management Strategy
503
Table 8: Indications and contraindications of infliximab therapy in inflammatory bowel disease
Indications ContraindicationsRefractor luminal (including upper gastrointestinal) CD
Active abscess
Steroid-dependent CD Suspected active tuberculosisRefractory fistulizing CD Intestinal obstructionChronic refractory UC Multiple sclerosis or optical neuritisAcute, severe UC Class III/IV congestive heart failureSystemic manifestations of IBD Previous lymphomaAnkylosing spondylitis and sacroiliitisPyoderma gangrenosumChronic uveitisMetastatic CDFirst-line therapya
Postoperative prophylaxisa
Indeterminate colitisa
Refractory pouchitisa
CD, Crohon’s diseasea Potential indications.
Table 9: Monoclonal antibodies and constructs in the treatment of inflammatory bowel diseaseTarget Compound Manufacturer Stage of development Disease Government approval US/EU
TNF Infliximab Centocor CD, UC CD, UC/CD, UCAdalimumab Abbott CD, UC CD/CDCertolizumab pegol UCB CD CD/-Golimumab Centocor Phase III CD, UCEtanercept Wyeth-Amgen StoppedOnercept Serono Stopped
α4-integrin Natalizumab Elan CD, UC CD/-α4-β7-integrin Vedolizumab (MLN0002) Millennium Phase IIII CD, UCβ7-integrin rhuMab β7 Genentech Phase I UCMadcam-1 PF-00547659 Pfizer Phase II UCIL 12/23 ABT-874 Abbott Phase II CD
Ustekinumab Centocor Phase II CDIFN γ Fontolizumab PDL Halted CDIL-6 receptor Tocilizumab Roche Phase II CDIL-2 receptor Declizumab Roche Stopped UC
Basiliximab Cerimon Phase III UCCD4 cm-t412 Centocor Stopped CDCD3 Visilizumab PDL Stopped UC
N1-0401-01 Novlmmune Phase I/IIa CDCD40 Ch5D12 Tanox Phase I CDCTLA-4 Abatacept BMS Phase III CD, UCCD20 Rituximab Roche Phase III CD, UCIL-17 AIN457 Novartis Phase II CDCXCL10 MDX-1100 (IP-10) Medarex Phase I UC
SEVERE OR FULMINANT ULCERATIVE COLITIS
Only 15 to 20 percent of patients with UC will ever experience an attack of fulminant colitis (45). Patients with pancolitis appear to be predisposed to severe flares. Infectious colitis (including Cytomegalovirus infection) should be excluded with stool culture for bacterial pathogens, C. difficile toxin test in stools and ova/parasites in a fresh stool sample and careful assessment of the mucosal biopsies (46). Supportive therapy for this condition includes relative bowel rest and parenteral nutrition if needed. The value of antibiotics as a prophylactic or adjuvant therapy has not been established. Patients with high fever, signs of peritionitis or high CRP levels should receive broad spectrum antibiotics (e.g. ciprofloxacin + metronidazole). However, initiation of antibiotics should never postpone the decision for procto-colectomy (46).
Corticosteroids:
Corticosteroids are generally used in the intravenous (IV) form either hydrocortisone 100 mg 4 times daily or methylprednisolone 40 mg daily. While mineralocorticoid and anti-inflammatory potencies vary, no data suggests one preparation is superior to another. Adrenocorticotropic hormone (ACTH) promotes endogenous corticosteroid production and may have benefit in steroid-naïve patients, but is no longer recommended due to the potential for adrenal hemorrhage (47). Dividing intravenous bolus dosing is equally effective to a continuous infusion (48). In a recent systematic review of 32 trials with almost 2000 patients who had steroid therapy for acute severe colitis, the overall response to
properties. In a double-blind, controlled trial curcumin appeared to be effective and safe for maintaining remission in patients with quiescent UC (44).
A treatment algorithm for the management of chronic active UC is summarized in Figure 2.
Medicine Update 2010 Vol. 20
504
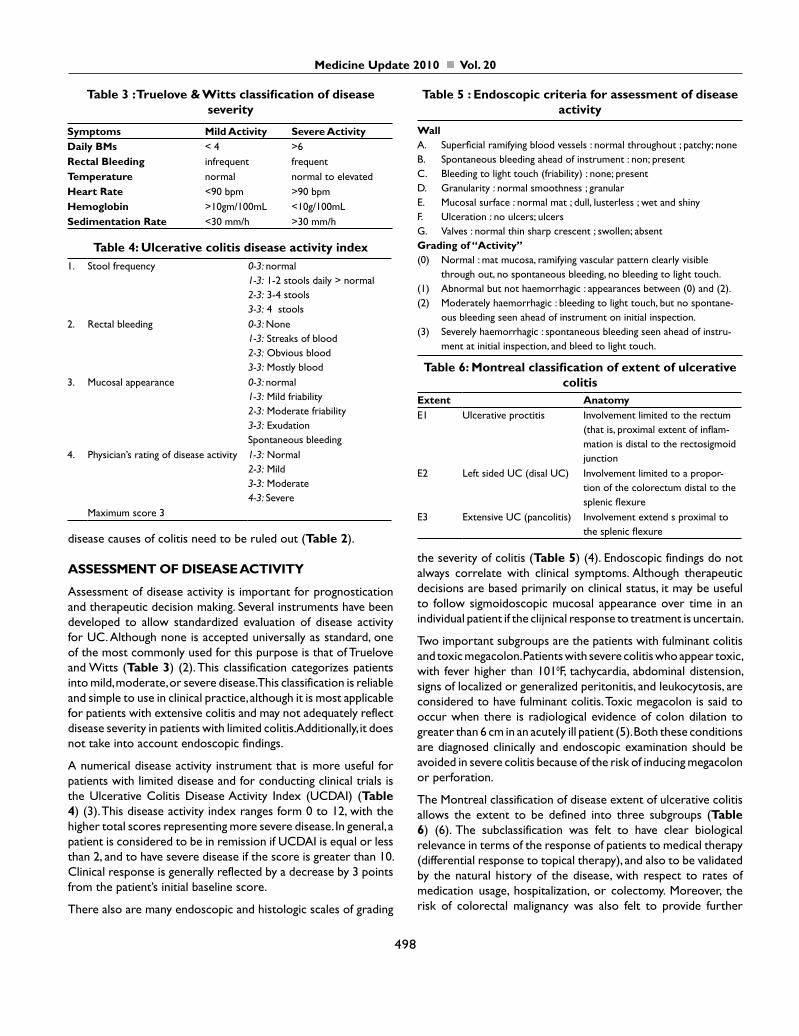
Fig. 3 : Treatment algorithm for the management of severe/ fulminant ulcerative colitis
Table 10 : Indications for surgery in ulcerative colitisCategory ManifestationLife-threatening complications toxic megacolon
colonic perforationmassive haemorrhage
Cancer-related proven cancerpresence of epthelial dysplasia in biopsicscolonic "stricture"cancerophobia
"Unacceptable" disease despite adequate treatment
treatment refractoriness, frequent recurrences/flare-ups, extra-coloni manifestations chronic corticoste-roid dependence side effects/intoler-ance/complications from medica-tions, in particular steroids (cataract, Cushing, osteoporosis, hypertension, hyperglycemia, etc.)unacceptable life style(symptoms incompatible with expectations
steroids was 67% (49). Approximately one-third of patients came to colectomy in the short term. Predictors of decreased response rate to steroids and increased risk for colectomy include greater severity and extent of colitis, and persistence of stool frequency > 8/d or C-reactive protein (CRP) > 45 mg/L beyond three days of treatment (45). Higher levels of glucocorticoid receptor beta (GRβ) have also been associated with glucocorticoid resistance in several studies (50). Of those patients who will respond to IV
steroids, the majority do so within five days [177 of UC 15], but most practitioners continue treatment for 7-10 days (51).
Cyclosporin:
In 1994, the definitive placebo-controlled trial supporting the use of cyclosporin in acute severe steroid-refractory UC showed that 9 of 11 patients failing steroid treatment for fulminant UC improved on cyclosporine (52). In a European controlled trial intravenous cyclosporin was at least as effective as corticosteroids in the treatment of patients with severe UC (53). Randomized controlled trial of cyclosporin to date compared 2 mg/kg with 4 mg/kg intravenous cyclosporin and demonstrated equal efficacy for both treatment groups (54). Low dose therapy is associated with minimum morbidity. Data on long-term outcome of patients treated with cyclosporin showed that, although the initial remission rates are high, most of the responders relapse at 1 year and 58% undergo colectomy at 7 years (55). The long-term outcome can be improved by the introduction of AZA or 6-MP on discharge from the hospital, together with several months of oral cyclosporin as a bridging therapy, and this is effective at avoiding colectomy in about 50% (10). Predictors of poor cyclosporin response in steroid-refractory cases include a temperature > 37.50C, heart rate > 90 beats per minute, a CRP > 45 mg/L and the presence of severe endoscopic lesions (56).
Infliximab:
Infliximab is effective in preventing colectomy in acute severe UC. Approximately one-third of patients receiving infliximab undergo colectomy during the acute admission (compared to two-third receiving placebo) (57). Two or more infusions appear to be

Ulcerative Colitis: Current Management Strategy
505
more effective than single infusion (58). Patients with early clinical response are significantly younger than non-responders and a pANCA-positive and/or ASCA-negative serotype is associated with suboptimal response (59).
In a recent systematic review of 34 studies including 896 patients with moderate-to-severe UC, infliximab was more effective than placebo (including inpatients and outpatients). Remission was achieved in 40% of patients at 9 months follow up (60). Further studies are needed to confirm the long-term efficacy of infliximab in preventing colectomy in fulminant UC.
Cyclosporine versus Infliximab in fulminant colitis:
Most of the current guidelines recommend the use of IV steroid for any attack of fulminant colitis (19,22,23). Cyclosporine or infliximab is considered when the patient fails with steroid even after 5 days and clinically deteriorating (10).
In some patients presenting with their first episode of acute severe UC and naïve to thiopurine therapy, there are sufficient data to suggest that intravenous cyclosporin (without a trial of steroid) followed by the introduction of AZA while still in the hospital, together with 3 months of bridging oral cyclosporin, is an effective strategy (10). In patients who have been maintained on AZA and present with a severe episode of UC, cyclosporin is often not successful; in this setting the use of infliximab is appropriate. Colectomy should also be considered, as it is unlikely that remission can be maintained (10).
In the acute setting, some patients will fail cyclosporine or infliximab. There are limited data available to evaluate the efficacy and safety of switching to the alternative agent. The alternative treatment may allow avoidance of colectomy in the short term in two-thirds of patients. However there is a substantial risk of morbidity, and possibly mortality, associated with such cross-over therapy (61). Controlled trials comparing cyclosporine with infliximab as a first-line therapy for fulminant colitis are in progress.
Adalimumab:
A small open-label study evaluated the efficacy of a humanized anti-TNF alpha antibody, adalimumab, in 10 patients with UC who
had previously responded to infliximab, but had subsequently lost response or became intolerant to the drug. Three patients experienced clinical improvement, and 1 was in remission, at week 4 (62).
Several other biological agents have been used in UC (63). Their indications and contraindications are shown in Table 8. A practically useful classification schema is shown in Table 9 with target agents, stage of development and approval status.
A treatment algorithm for the management for severe or fulminant UC is shown in Figure 3.
SURGICAL MANAGEMENT
Indications for surgical intervention and modalities of surgery are shown in Table 10 and Figure 4. Restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) is the ideal operation (64). Controversial issues in the choice are: the ideal operation for the elderly, the ideal time for intervention in cases of failure of medical treatment, the need to perform mucosectomy and the need for routine proximal diversion (65). All operations for ulcerative colitis can be performed laparoscopically. There has not been any significant difference regarding number of bowel movements, stool consistency, incontinence, need for anti-diarrheal medications, and dietary restrictions between laparoscopic and conventional ileal pouch anal anastomosis (66).
MANAGEMENT OF SPECIAL SITUATIONS
Ulcerative colitis in children (67):
Diagnosis of UC in children and adolescents requires a high index of suspicion. The treatment of pediatric ulcerative colitis differs from that in adults in that maintenance of growth and pubertal development is an important goal in disease management in children. Long term corticosteroid can have an adverse effect on growth. Algorithm for the selection of drug therapy is similar to that practiced in adults. Infliximab may also be beneficial, but further studies are needed to determine its tolerability and efficacy in children. The need for, or timing of, colectomy in children is
Fig. 4 : Overview of surgical modules and their combinations for the management of ulcerative colitis
Medicine Update 2010 Vol. 20
506
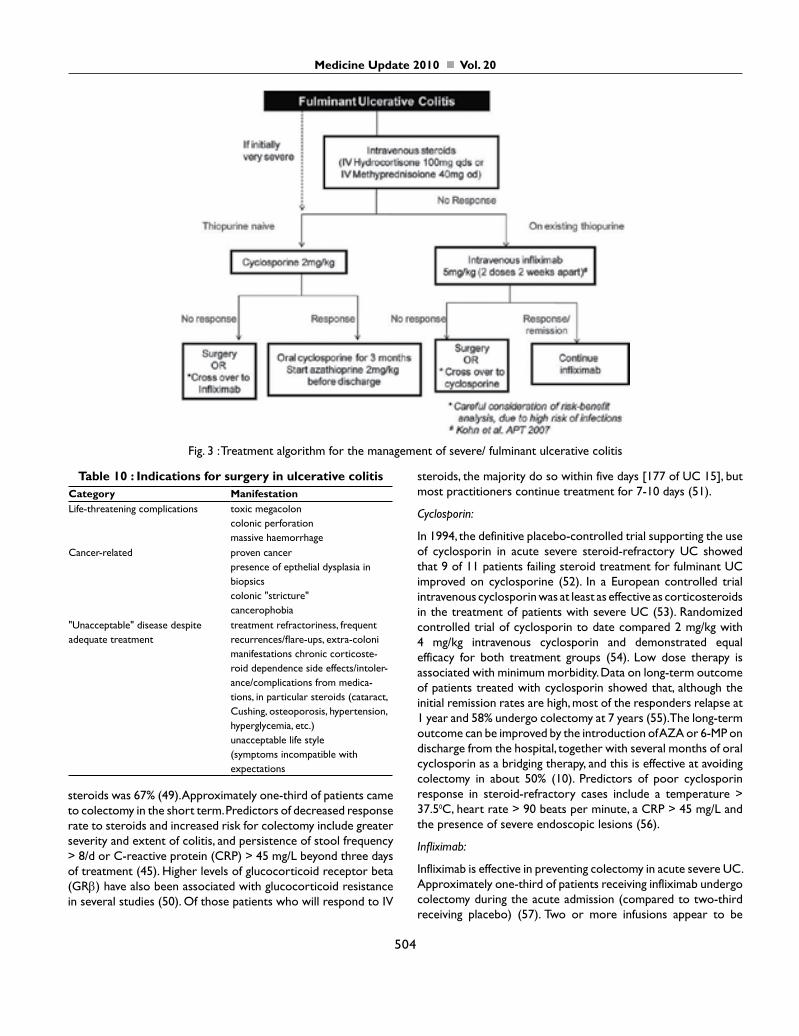
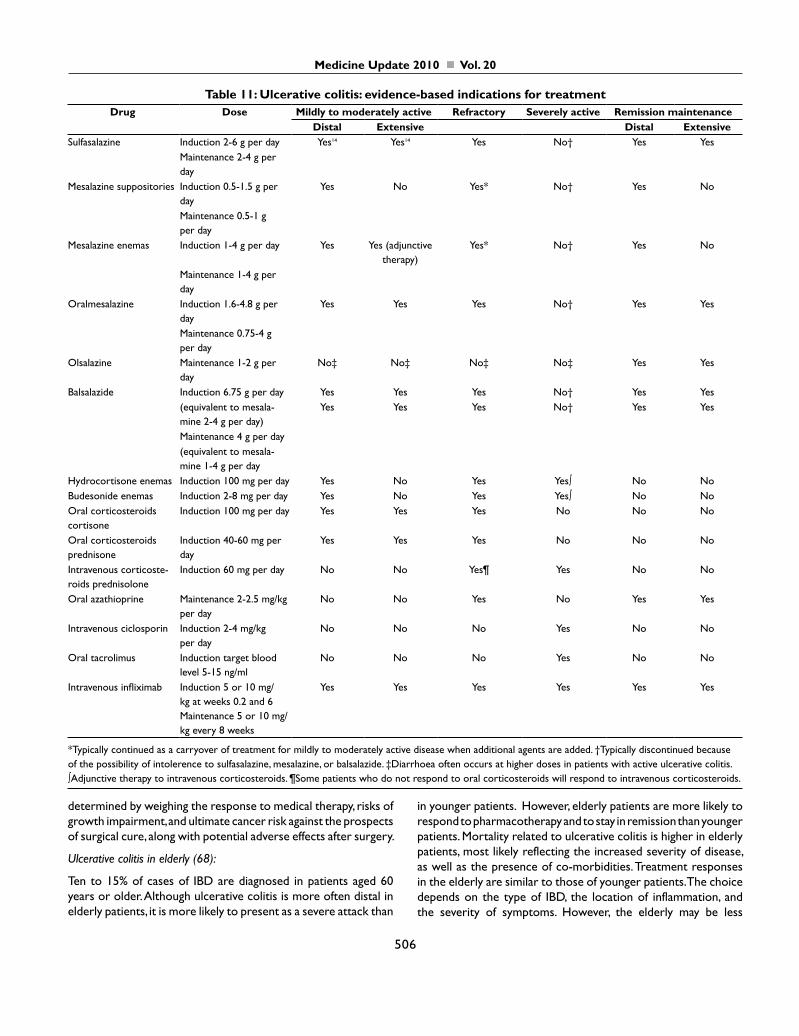
Table 11: Ulcerative colitis: evidence-based indications for treatmentDrug Dose Mildly to moderately active Refractory Severely active Remission maintenance
Distal Extensive Distal ExtensiveSulfasalazine Induction 2-6 g per day Yes14 Yes14 Yes No† Yes Yes
Maintenance 2-4 g per day
Mesalazine suppositories Induction 0.5-1.5 g per day
Yes No Yes* No† Yes No
Maintenance 0.5-1 g per day
Mesalazine enemas Induction 1-4 g per day Yes Yes (adjunctive therapy)
Yes* No† Yes No
Maintenance 1-4 g per day
Oralmesalazine Induction 1.6-4.8 g per day
Yes Yes Yes No† Yes Yes
Maintenance 0.75-4 g per day
Olsalazine Maintenance 1-2 g per day
No‡ No‡ No‡ No‡ Yes Yes
Balsalazide Induction 6.75 g per day Yes Yes Yes No† Yes Yes(equivalent to mesala-mine 2-4 g per day)
Yes Yes Yes No† Yes Yes
Maintenance 4 g per day(equivalent to mesala-mine 1-4 g per day
Hydrocortisone enemas Induction 100 mg per day Yes No Yes Yes∫ No NoBudesonide enemas Induction 2-8 mg per day Yes No Yes Yes∫ No NoOral corticosteroids cortisone
Induction 100 mg per day Yes Yes Yes No No No
Oral corticosteroids prednisone
Induction 40-60 mg per day
Yes Yes Yes No No No
Intravenous corticoste-roids prednisolone
Induction 60 mg per day No No Yes¶ Yes No No
Oral azathioprine Maintenance 2-2.5 mg/kg per day
No No Yes No Yes Yes
Intravenous ciclosporin Induction 2-4 mg/kg per day
No No No Yes No No
Oral tacrolimus Induction target blood level 5-15 ng/ml
No No No Yes No No
Intravenous infliximab Induction 5 or 10 mg/kg at weeks 0.2 and 6 Maintenance 5 or 10 mg/kg every 8 weeks
Yes Yes Yes Yes Yes Yes
*Typically continued as a carryover of treatment for mildly to moderately active disease when additional agents are added. †Typically discontinued because of the possibility of intolerence to sulfasalazine, mesalazine, or balsalazide. ‡Diarrhoea often occurs at higher doses in patients with active ulcerative colitis. ∫Adjunctive therapy to intravenous corticosteroids. ¶Some patients who do not respond to oral corticosteroids will respond to intravenous corticosteroids.
determined by weighing the response to medical therapy, risks of growth impairment, and ultimate cancer risk against the prospects of surgical cure, along with potential adverse effects after surgery.
Ulcerative colitis in elderly (68):
Ten to 15% of cases of IBD are diagnosed in patients aged 60 years or older. Although ulcerative colitis is more often distal in elderly patients, it is more likely to present as a severe attack than
in younger patients. However, elderly patients are more likely to respond to pharmacotherapy and to stay in remission than younger patients. Mortality related to ulcerative colitis is higher in elderly patients, most likely reflecting the increased severity of disease, as well as the presence of co-morbidities. Treatment responses in the elderly are similar to those of younger patients. The choice depends on the type of IBD, the location of inflammation, and the severity of symptoms. However, the elderly may be less

Ulcerative Colitis: Current Management Strategy
507
responsive than younger patients to topical therapy, particularly if they are unable to retain the drug long enough for its effects to occur. Corticosteroids have a higher risk of complications in the elderly (accelerated bone loss, fractures, hypertension, diabetes mellitus, mental status changes) and should be tapered as quickly as possible, ideally within 8 to 12 weeks. Patients should have a baseline assessment of bone density. Postmenopausal women should be counseled on the potential benefits of estrogen replacement. Patients treated with corticosteroids should also receive vitamin D supplementation and close follow up, although prophylactic treatment with a bisphosphonate may also be reasonable. The elderly are more likely to present with severe colitis, which can be associated with high mortality. Aggressive supportive therapy, including antibacterials, fluid replacement, nutritional support, and blood transfusions may be necessary. Narcotics and anticholinergics should be avoided, in order to reduce the risk of precipitating toxic megacolon. Elderly are often not considered ideal candidates for cyclosporin, and may derive more benefit from early surgery. Elderly patients often have anal sphincter dysfunction and have less satisfactory outcomes after a pouch procedure. Therefore, a proctocolectomy and ileostomy (rather than creation of a pouch) is usually preferred in this age group.
Ulcerative colitis in pregnancy (69):
Fertility is usually normal in patients with UC unlike that in active Chron’s disease. Though patients are at an increased risk for small and premature babies, there is no risk of increased fetal loss. Adverse pregnancy outcomes are related to disease activity. Those having inactive disease at conception the likelihood of relapse during pregnancy are 34%. Those with active disease at conception, 27% improve, 24% remain unchanged and 45% deteriorate. All efforts should be channeled into ensuring that the disease is quiescent at conception and during pregnancy. Proper education and planning is required and folic acid is advised before conception. Maintenance treatment should be continued and flare-up of disease activity should be actively treated. Disease activity is more dangerous than most drugs. Breast feeding is encouraged for its beneficial effects.
NUTRITION AND ULCERATIVE COLITIS
Nutrition may play an important role in the pathogenesis and treatment of IBD. The evidence regarding the role of specific dietary components in the pathogenesis of IBD is still inconclusive. Many studies have been subject to methodological limitations. Several studies have reported nutritional and functional deficiencies in IBD patients, especially in Crohn’s disease. It is, however, hard to discriminate between disease-induced and malnutrition-induced changes in nutritional parameters. Maintaining adequate nutritional status has been suggested to be beneficial to the course of the disease in UC (70). Studies have provided further insight into the possible beneficial effects of nutritional supplementation as primary and adjunctive therapy. The effects of specific nutritional therapy may be caused by alterations in intestinal flora and hence
in the production of intraluminal pro-inflammatory substances. Immunonutrients such as fish oils, short chain fatty acids and antioxidants may also play a role in the treatment of UC but conclusive evidence still remains elusive (70).
EPILOGUE
The recent refinement of established therapies and the development of new simple molecules and biological agents have altered the therapeutic possibilities for patients with UC (Table 11). The future for the management of UC appears promising as new therapies continue to be added to the treatment armamentarium, and strategies incorporating current and novel therapies continue to evolve.
REFERENCES1. Baumgart D, Sandborn WJ. Inflammatory bowel disease: clinical aspects
and established and evolving therapies. Lancet 2007;369:1641-57.
2. Truelove SC, Witts LJ. Cortisone in ulcerative colitis: Final report of a therapeutic trial. BMJ 1955;2:1041-8.
3. Sutherland LR, Martin F, Greer S, et al. 5-aminosalicylic acid enema in the treatment of distal ulcerative colitis, proctosigmoiditis, and procti-tis. Gastroenterology 1987;92:1894-8.
4. Baron JH, Connell AM, Lennard-Jones JE. Variation between observers in describing mucosal appearances in proctocolitis. BMJ 1964;2:89-92.
5. Lennard-Jones JE, Ritchie JK, Hilder W, et al. Assessment of severity in colitis. A preliminary study. Gut 1975;16:579-84.
6. Satsangi J, Silverberg MS, Vermeire S, et al. The Montreal classification of inflammatory bowel disease: controversies, consensus and implications. Gut 2006;55:749-53.
7. Langholz E, Munkholm P, Davidsen M, et al. Course of ulcerative coli-tis: analysis of changes in disease activity over years. Gastroenterology 1994;107:3-11.
8. Langholz E, Munkholm P, Davidsen M, et al. Changes in extent of ul-cerative colitis: a study on the course and prognostic factors. Scand J Gastroenterol 1996;31:260-66.
9. Winther KV, Jess T, Longholz E, et al. survival and cause-specific mor-tality in ulcerative colitis: follow-up of a population-based cohort in Copenhagen county. Gastroenterology 2003;125:1576-82.
10. Ng SC, Kamm MA. Therapeutic strategies for the management of ulcer-ative colitis. Inflamm Bowel Dis 2009;15:935-50.
11. Stange EF, Travis SP. The European Consensus on ulcerative colitis: new horizons? Gut 2008;57:1029-31.
12. Sutherland L, Macdonald JK. Oral 5-aminosalicylic acid for induc-tion of remission in ulcerative colitis. Cochrane Database Syst Rev. 2006;CD000543.
13. Sutherland L, Roth D, Beck P, et al. Oral 5-aminosalicylic acid for main-tenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2002;CD000544.
14. Picco MF, Krishna M, Cangemi JR, et al. Oral mesalamine and clinical remission are associated with a decrease in the extent of long-standing ulcerative colitis. Inflamm Bowel Dis. 2006;12:537–42.
15. Regueiro M, Loftus EV Jr, Steinhart AH, et al. Clinical guidelines for the medical management of left-sided ulcerative colitis and ulcerative proc-titis: summary statement. Inflamm Bowel Dis. 2006;12:972–8.
16. Safdi M, DeMicco M, Sninsky C, et al. A double-blind comparison of oral versus rectal mesalamine versus combination therapy in the treatment of distal ulcerative colitis. Am J Gastroenterol. 1997;92:1867–71.
17. Marshall JK, Irvine EJ. Putting rectal 5-aminosalicylic acid in its place: the role in distal ulcerative colitis. Am J Gastroenterol. 2000;95:1628–36.

Medicine Update 2010 Vol. 20
508
18. Marteau P, Probert CS, Lindgren S, et al. Combined oral and enema treatment with Pentasa (mesalazine) is superior to oral therapy alone in patients with extensive mild/moderate active ulcerative colitis: a ran-domised, double blind, placebo controlled study. Gut. 2005;54:960–65.
19. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2004;99:1371–85.
20. D’Albasio G, Pacini F, Camarri E, et al. Combined therapy with 5-ami-nosalicylic acid tablets and enemas for maintaining remission in ul-cerative colitis: a randomized double-blind study. Am J Gastroenterol. 1997;92:1143–7.
21. Orchard T, Probert CS, Keshav S. Review article: maintenance therapy in patients with ulcerative colitis. Aliment Pharmacol Ther. 2006;24(suppl 1):17–22.
22. Travis SPL, Stange EF, Lemann M, et al. European evidence-based con-sensus on the management of ulcerative colitis: current management. J Crohn’s Colitis. 2008;2:24–62.
23. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults. American College of Gastroenterology, Practice Parameters Commit-tee. Am J Gastroenterol. 1997;92:204 –11.
24. Sninsky CA, Cort DH, Shanahan F, et al. Oral mesalamine (Asacol) for mildly to moderately active ulcerative colitis. A multicenter study. Ann Intern Med. 1991;115:350 –5.
25. Hanauer SB, Sandborn WJ, Kornbluth A, et al. Delayed-release oral mesalamine at 4.8 g/day (800 mg tablet) for the treatment of moder-ately active ulcerative colitis: the ASCEND II trial. Am J Gastroenterol. 2005;100:2478 –85.
26. Bianchi PG, Cassinotti A, Ferrara E, et al. Review article: the manage-ment of steroid dependency in ulcerative colitis. Aliment Pharmacol Ther. 2007;26:779 –94.
27. Lobo AJ, Foster PN, Burke DA, et al. The role of azathioprine in the management of ulcerative colitis. Dis Colon Rectum. 1990;33:374–7.
28. Rosenberg JL, Wall AJ, Levin B, et al. A controlled trial of azathioprine in the management of chronic ulcerative colitis. Gastroenterology. 1975;69:96 –9.
29. Kirk AP, Lennard-Jones JE. Controlled trial of azathioprine in chronic ulcerative colitis. Br Med J (Clin Res Ed). 1982;284:1291–2.
30. Ardizzone S, Maconi G, Russo A, et al. Randomised controlled trial of azathioprine and 5-aminosalicylic acid for treatment of steroid depen-dent ulcerative colitis. Gut. 2006;55:47–53.
31. Timmer A, McDonald JW, Macdonald JK. Azathioprine and 6-mercap-topurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2007;CD000478.
32. Sparrow MP, Hande SA, Friedman S, et al. Effect of allopurinol on clinical outcomes in inflammatory bowel disease nonresponders to azathio-prine or 6-mercaptopurine. Clin Gastroenterol Hepatol. 2007;5:209 –14.
33. Ng SC, Arebi N, Kamm MA. Medium-term results of oral tacrolimus treatment in refractory inflammatory bowel disease. Inflamm Bowel Dis. 2007;13:129 –34.
34. Oren R, Arber N, Odes S, et al. Methotrexate in chronic active ulcer-ative colitis: a double-blind, randomized, Israeli multicenter trial. Gas-troenterology. 1996;110:1416 –21.
35. Qasim A, McDonald S, Sebastian S, et al. Efficacy and safety of 6-thio-guanine in the management of inflammatory bowel disease. Scand J Gastroenterol. 2007;42:194 –9.
36. Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induc-tion and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353:2462–76.
37. D’Haens G, Daperno M. Advances in biologic therapy for ulcerative colitis and Crohn’s disease. Curr Gastroenterol Rep. 2006;8:506 –12.
38. Lawson MM, Thomas AG, Akobeng AK. Tumour necrosis factor alpha blocking agents for induction of remission in ulcerative colitis. Co-
chrane Database Syst Rev. 2006;3:CD005112.
39. Sawada K, Kusugami K, Suzuki Y, et al. Leukocytapheresis in ulcerative colitis: results of a multicenter double-blind prospective case- control study with sham apheresis as placebo treatment. Am J Gastroenterol. 2005;100:1362–9.
40. Sands BE, Sandborn WJ, Feagan B, et al. A randomized, double-blind, sham-controlled study of granulocyte/monocyte apheresis for active ulcerative colitis. Gastroenterology. 2008;135:400–9.
41. Mallon P, McKay D, Kirk S, et al. Probiotics for induction of remission in ulcerative colitis. Cochrane Database Syst Rev. 2007;CD005573.
42. Rembacken BJ, Snelling AM, Hawkey PM, et al. Non-pathogenic Esch-erichia coli versus mesalazine for the treatment of ulcerative colitis: a randomised trial. Lancet. 1999;354:635– 9.
43. Venturi A, Gionchetti P, Rizzello F, et al. Impact on the composition of the faecal flora by a new probiotic preparation: preliminary data on maintenance treatment of patients with ulcerative colitis. Aliment Pharmacol Ther. 1999;13:1103–8.
44. Hanai H, Iida T, Takeuchi K, et al. Curcumin maintenance therapy for ulcerative colitis: randomized, multicenter, double-blind, placebo-con-trolled trial. Clin Gastroenterol Hepatol. 2006;4:1502–6.
45. Travis SP, Farrant JM, Ricketts C, et al. Predicting outcome in severe ulcerative colitis. Gut 1996;38:905-10.
46. Van Assche G, Vermeire S, Rutgeerts P. Treatment of severe steroid-refractory ulcerative colitis. World J Gastroenterol. 2008;14:5508-11.
47. Katz JA. Treatment of inflammatory bowel disease with corticosteroids. Gastroenterol Clin North Am 2004;33:171-189, vii
48. Bossa F, Fiorella S, Caruso N, et al. Continuous infusion versus bolus administration of steroids in severe attacks of ulcerative colitis: a ran-domized, double-blind trial. Am J Gastroenterol 2007;102:601-8.
49. Turner D, Walsh CM, Steinhart AH, et al. Response to corticosteroids in severe ulcerative colitis: a systematic review of the literature and a meta-regression. Clin Gastroenterol Hepatol. 2007;5:103–10.
50. Webster JC, Oakley RH, Jewell CM, et al. Proinflammatory cytokines regulate human glucocorticoid receptor gene expression and lead to the accumulation of the dominant negative beta isoform: a mechanism for the generation of glucocorticoid resistance. Proc Natl Acad Sci USA 2001;98:6865-70.
51. Truelove SC, Jewell DP. Intensive intravenous regimen for severe at-tacks of ulcerative colitis. Lancet 1974;1:1067-70.
52. Lichtiger S, Present DH, Kornbluth A, et al. Cyclosporine in se-vere ulcerative colitis refractory to steroid therapy. N Engl J Med. 1994;330:1841–5.
53. D’Haens G, Lemmens L, Geboes K, et al. Intravenous cyclosporine ver-sus intravenous corticosteroids as single therapy for severe attacks of ulcerative colitis. Gastroenterology. 2001;120:1323–9.
54. Van AG, D’Haens G, Noman M, et al. Randomized, double-blind com-parison of 4 mg/kg versus 2 mg/kg intravenous cyclosporine in severe ulcerative colitis. Gastroenterology. 2003;125:1025–31.
55. Campbell S, Travis S, Jewell D. Ciclosporin use in acute ulcerative colitis: a long-term experience. Eur J Gastroenterol Hepatol. 2005;17:79–84.
56. Cacheux W, Seksik P, Lemann M, et al. Predictive factors of response to cyclosporine in steroid-refractory ulcerative colitis. Am J Gastroen-terol. 2008;103:637– 42.
57. Lees CW, Heys D, Ho GT, et al. A retrospective analysis of the efficacy and safety of infliximab as rescue therapy in acute severe ulcerative colitis. Aliment Pharmacol Ther. 2007;26:411– 9.
58. Kohn A, Daperno M, Armuzzi A, et al. Infliximab in severe ulcerative colitis: short-term results of different infusion regimens and long-term follow-up. Aliment Pharmacol Ther. 2007;26:747–56.
59. Ferrante M, Vermeire S, Katsanos KH, et al. Predictors of early re-sponse to infliximab in patients with ulcerative colitis. Inflamm Bowel Dis. 2007;13:123–8.

Ulcerative Colitis: Current Management Strategy
509
60. Gisbert JP, Gonzalez-Lama Y, Mate J. Systematic review: Infliximab thera-py in ulcerative colitis. Aliment Pharmacol Ther. 2007;25:19 –37.
61. Maser EA, Deconda D, Lichtiger S, et al. Cyclosporine and infliximab as acute salvage therapies for each other, in severe steroid-refractory ulcerative colitis. Gastroenterology. 2007;132(suppl 2):S1132.
62. Peyrin-Biroulet L, Laclotte C, Roblin X, et al. Adalimumab induction therapy for ulcerative colitis with intolerance or lost response to inf-liximab: an open-label study. World J Gastroenterol. 2007;13:2328–32.
63. Rutgeerts P, Vermeire S, Van Assche G. Biological therapies in inflamma-tory bowel diseases. Gastroenterology 2009;136:1182-97.
64. Kaiser AM, Beart Jr RW. Surgical management of ulcerative colitis. Swiss Med Wkly 2001; 131: 323-37.
65. Hwang JM, Verma MG. Surgery for imflammatory bowel disease. World J Gastroenterol 2008;14:2678-90.
66. Dunker MS, Bemelman WA, Slors JF, et al. Functional outcome, quality of life, body image, and cosmesis in patients after laparoscopic-assisted and conventional restorative proctocolectomy: a comparative study. Dis Colon Rectum 2001;44:1800-7.
67. Rufo PA, Bousvaros A. Challenges and progress in pediatric inflamma-tory bowel disease. Curr Opin Gastroenterol. 2007;23:406-12.
68. Pardi DS, Loftus Jr EV, Camilleri M. Treatment of inflammatory bowel disease in the elderly: An update. Drugs Aging 2002;19:355-63.
69. Alstead EM. Inflammatory bowel disease in pregnancy, Postgrad Med J 2002;78: 23-6.
70. Geerling BJ, Stockbrugger RW, Brummer R-J M. Nutrition and inflam-matory bowel disease: an update. Scand J Gastroenterol 1999;34:95-105.