uniform labeling of slides and blocks in surgical...
TRANSCRIPT

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Q1. Describe your current role in the laboratory:
Answer Options Response Percent Response Count
Pathologist 16.4% 40
Medical Director 8.6% 21
Histotechnologist/Histotechnician 40.6% 99
QA/QC Coordinator 3.7% 9
Laboratory Manager 29.9% 73
Industry 0.8% 2
Q2. Which of the following bests describes your practice setting?
Answer Options Response Percent Response Count
University hospital/academic medical center 26.9% 74
Voluntary, non-profit hospital 26.9% 74
Proprietary hospital 6.9% 19
City/County/State hospital 9.5% 26
Veterans hospital 1.5% 4
Army/Air Force/Navy hospital 0.4% 1
National/corporate laboratory 4.4% 12
Regional/local independent laboratory (except clinic or group practice and not owned by national corporation(s)) 14.2% 39
Public health, non-hospital 0.0% 0
Clinic, group or doctor-office laboratory 6.2% 17
N/A - industry or vendor 3.3% 9
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
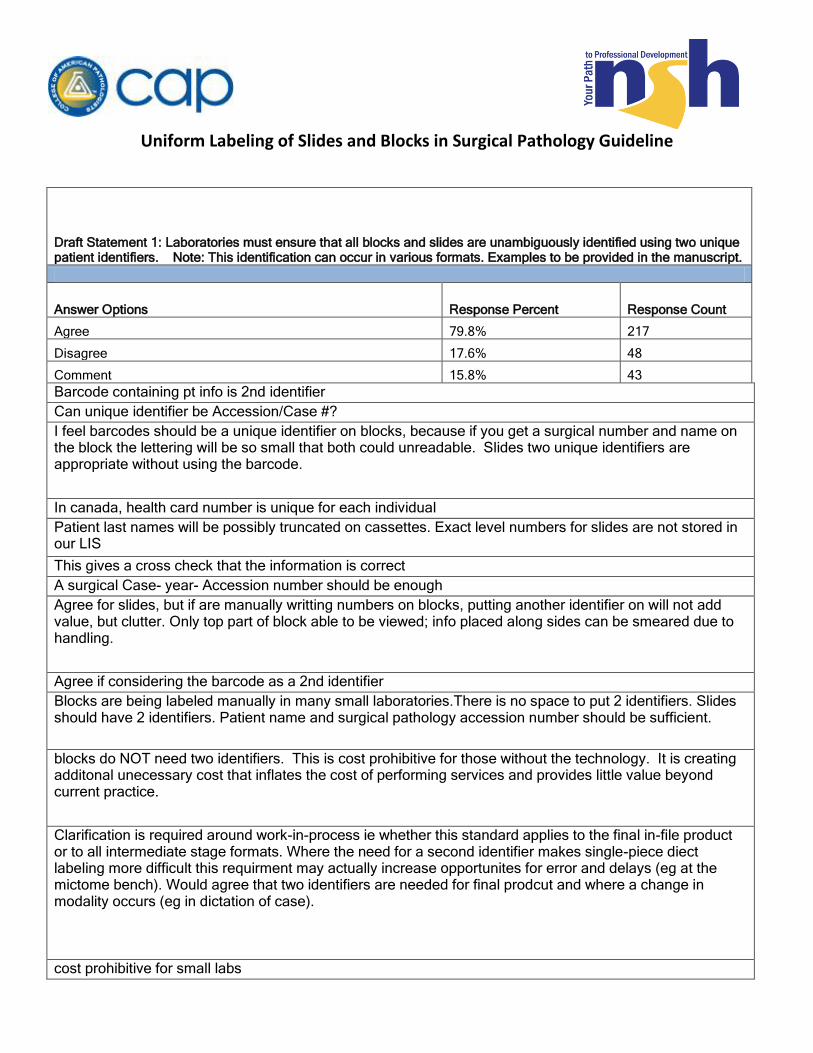
Draft Statement 1: Laboratories must ensure that all blocks and slides are unambiguously identified using two unique patient identifiers. Note: This identification can occur in various formats. Examples to be provided in the manuscript.
Answer Options Response Percent Response Count
Agree 79.8% 217
Disagree 17.6% 48
Comment 15.8% 43
Barcode containing pt info is 2nd identifier
Can unique identifier be Accession/Case #?
I feel barcodes should be a unique identifier on blocks, because if you get a surgical number and name on the block the lettering will be so small that both could unreadable. Slides two unique identifiers are appropriate without using the barcode.
In canada, health card number is unique for each individual
Patient last names will be possibly truncated on cassettes. Exact level numbers for slides are not stored in our LIS
This gives a cross check that the information is correct
A surgical Case- year- Accession number should be enough
Agree for slides, but if are manually writting numbers on blocks, putting another identifier on will not add value, but clutter. Only top part of block able to be viewed; info placed along sides can be smeared due to handling.
Agree if considering the barcode as a 2nd identifier
Blocks are being labeled manually in many small laboratories.There is no space to put 2 identifiers. Slides should have 2 identifiers. Patient name and surgical pathology accession number should be sufficient.
blocks do NOT need two identifiers. This is cost prohibitive for those without the technology. It is creating additonal unecessary cost that inflates the cost of performing services and provides little value beyond current practice.
Clarification is required around work-in-process ie whether this standard applies to the final in-file product or to all intermediate stage formats. Where the need for a second identifier makes single-piece diect labeling more difficult this requirment may actually increase opportunites for error and delays (eg at the mictome bench). Would agree that two identifiers are needed for final prodcut and where a change in modality occurs (eg in dictation of case).
cost prohibitive for small labs
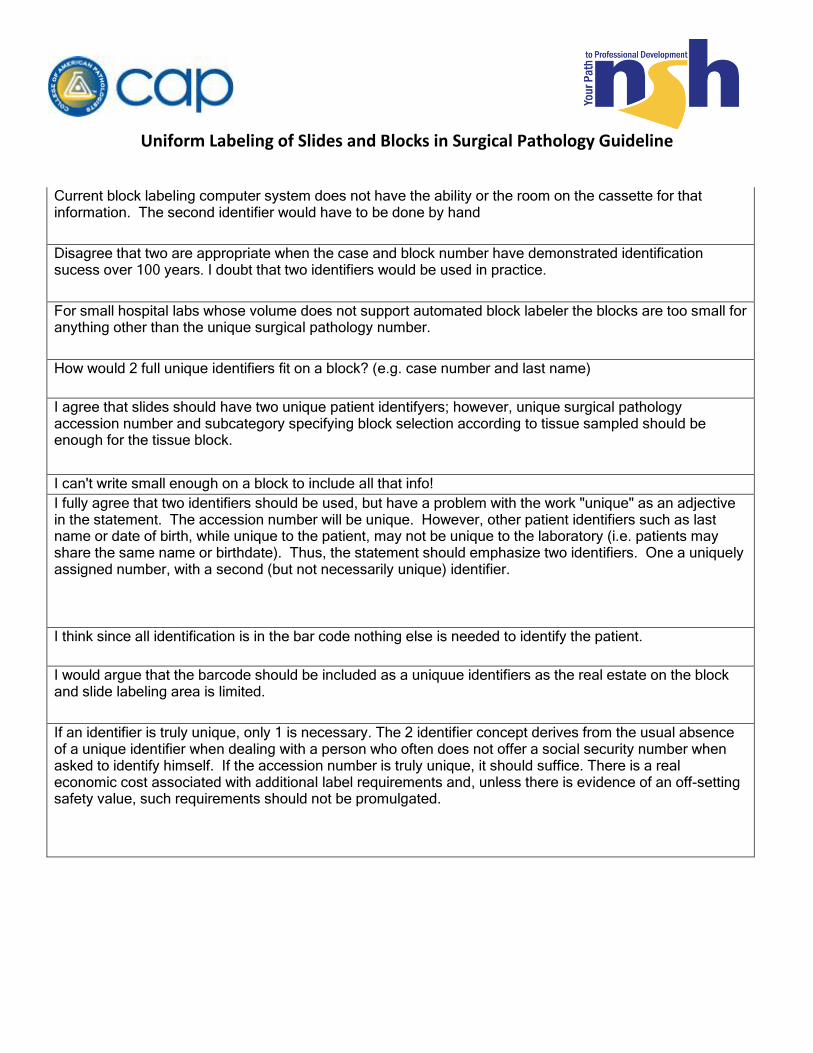
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline Current block labeling computer system does not have the ability or the room on the cassette for that information. The second identifier would have to be done by hand
Disagree that two are appropriate when the case and block number have demonstrated identification sucess over 100 years. I doubt that two identifiers would be used in practice.
For small hospital labs whose volume does not support automated block labeler the blocks are too small for anything other than the unique surgical pathology number.
How would 2 full unique identifiers fit on a block? (e.g. case number and last name)
I agree that slides should have two unique patient identifyers; however, unique surgical pathology accession number and subcategory specifying block selection according to tissue sampled should be enough for the tissue block.
I can't write small enough on a block to include all that info!
I fully agree that two identifiers should be used, but have a problem with the work "unique" as an adjective in the statement. The accession number will be unique. However, other patient identifiers such as last name or date of birth, while unique to the patient, may not be unique to the laboratory (i.e. patients may share the same name or birthdate). Thus, the statement should emphasize two identifiers. One a uniquely assigned number, with a second (but not necessarily unique) identifier.
I think since all identification is in the bar code nothing else is needed to identify the patient.
I would argue that the barcode should be included as a uniquue identifiers as the real estate on the block and slide labeling area is limited.
If an identifier is truly unique, only 1 is necessary. The 2 identifier concept derives from the usual absence of a unique identifier when dealing with a person who often does not offer a social security number when asked to identify himself. If the accession number is truly unique, it should suffice. There is a real economic cost associated with additional label requirements and, unless there is evidence of an off-setting safety value, such requirements should not be promulgated.
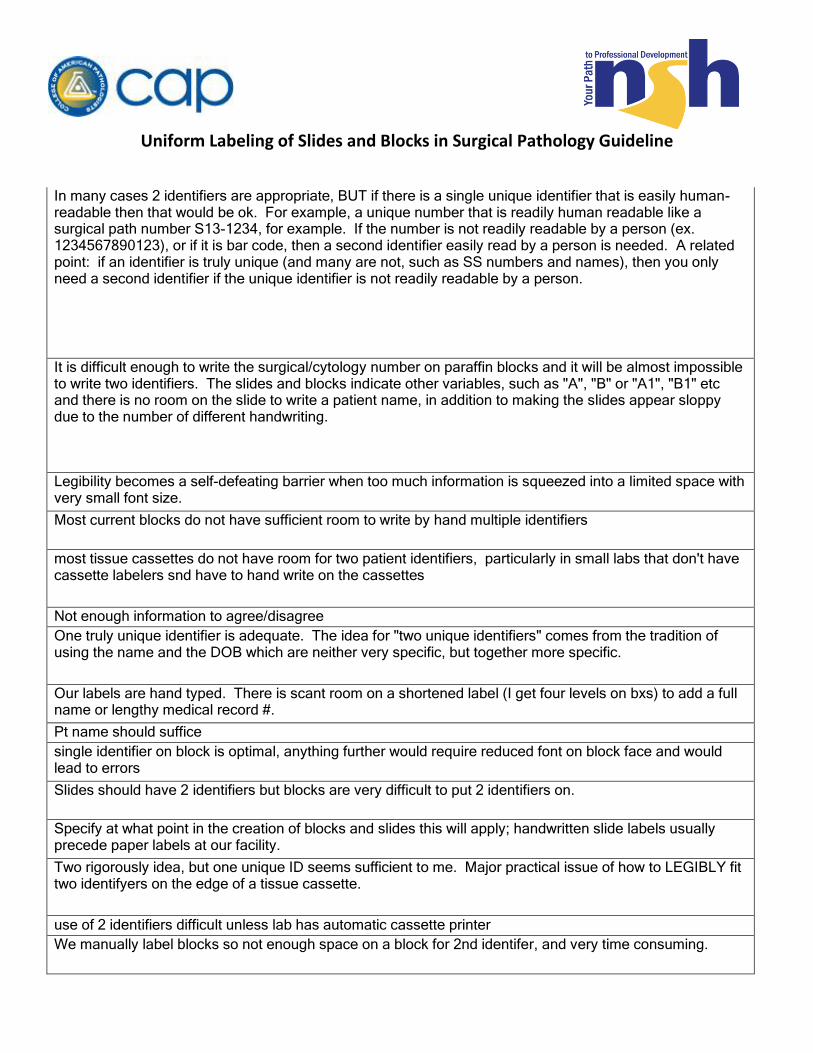
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline In many cases 2 identifiers are appropriate, BUT if there is a single unique identifier that is easily human-readable then that would be ok. For example, a unique number that is readily human readable like a surgical path number S13-1234, for example. If the number is not readily readable by a person (ex. 1234567890123), or if it is bar code, then a second identifier easily read by a person is needed. A related point: if an identifier is truly unique (and many are not, such as SS numbers and names), then you only need a second identifier if the unique identifier is not readily readable by a person.
It is difficult enough to write the surgical/cytology number on paraffin blocks and it will be almost impossible to write two identifiers. The slides and blocks indicate other variables, such as "A", "B" or "A1", "B1" etc and there is no room on the slide to write a patient name, in addition to making the slides appear sloppy due to the number of different handwriting.
Legibility becomes a self-defeating barrier when too much information is squeezed into a limited space with very small font size.
Most current blocks do not have sufficient room to write by hand multiple identifiers
most tissue cassettes do not have room for two patient identifiers, particularly in small labs that don't have cassette labelers snd have to hand write on the cassettes
Not enough information to agree/disagree
One truly unique identifier is adequate. The idea for "two unique identifiers" comes from the tradition of using the name and the DOB which are neither very specific, but together more specific.
Our labels are hand typed. There is scant room on a shortened label (I get four levels on bxs) to add a full name or lengthy medical record #.
Pt name should suffice
single identifier on block is optimal, anything further would require reduced font on block face and would lead to errors
Slides should have 2 identifiers but blocks are very difficult to put 2 identifiers on.
Specify at what point in the creation of blocks and slides this will apply; handwritten slide labels usually precede paper labels at our facility.
Two rigorously idea, but one unique ID seems sufficient to me. Major practical issue of how to LEGIBLY fit two identifyers on the edge of a tissue cassette.
use of 2 identifiers difficult unless lab has automatic cassette printer
We manually label blocks so not enough space on a block for 2nd identifer, and very time consuming.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline We use a cassette and slide printer and the room is limited for two identifiers. At present CAP requires two identifiers on the frozen section slides only.
Where there is limited space, I think common sense needs to prevail. We use 2-D barcodes on our blocks & slides currently. The blocks have very limited space, we manage the bar-code, a case number and consider that acceptable.
Will this prevent mislabeling of blocks? Are we checking the name when we are cutting the block?
You should be able to trace the assigned accession number back to 2 patient identifiers, but not require 2 identifiers on the slides and blocks.
You should distinguish slides from blocks in this recommendation. For those institutions that do not currently employ bar or QR code systems (and there are still many small labs that don’t), there is insufficient room on the cassette to have two separate unique identifiers along with other necessary markings (levels, special stains, etc). Having two indicators on the slide is easy and does not add significant expense, but that is not true for cassettes.
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
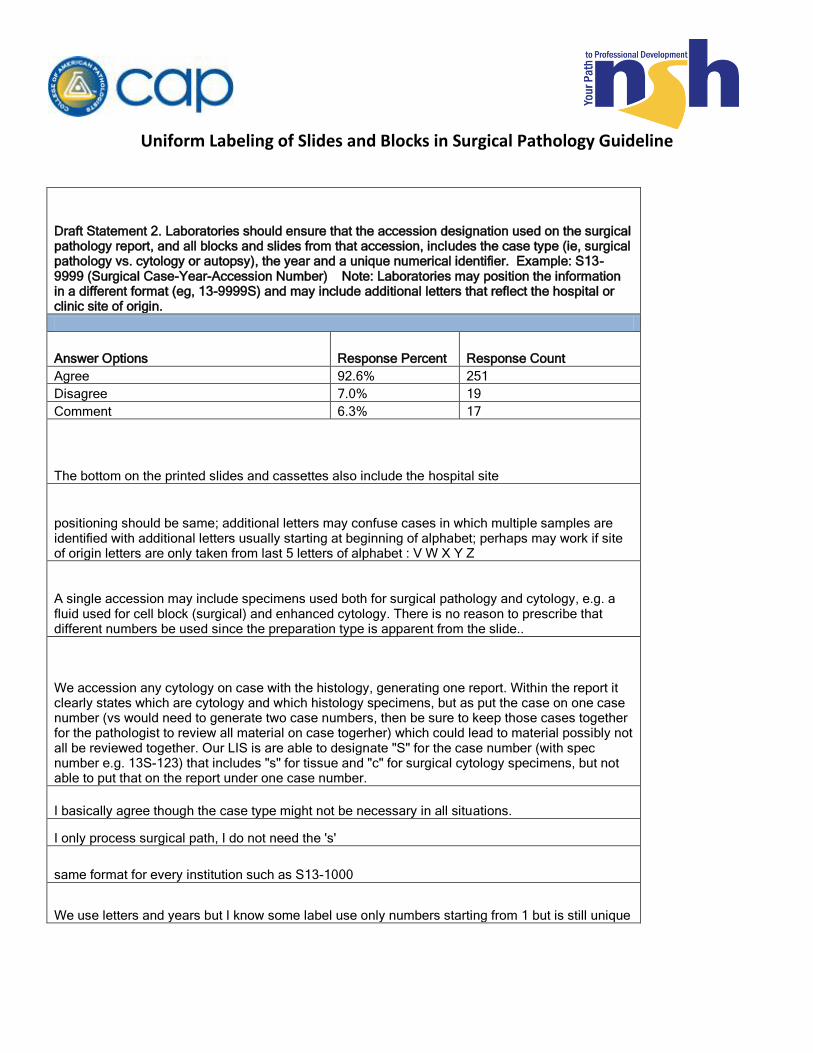
Draft Statement 2. Laboratories should ensure that the accession designation used on the surgical pathology report, and all blocks and slides from that accession, includes the case type (ie, surgical pathology vs. cytology or autopsy), the year and a unique numerical identifier. Example: S13-9999 (Surgical Case-Year-Accession Number) Note: Laboratories may position the information in a different format (eg, 13-9999S) and may include additional letters that reflect the hospital or clinic site of origin.
Answer Options Response Percent Response Count
Agree 92.6% 251
Disagree 7.0% 19
Comment 6.3% 17
The bottom on the printed slides and cassettes also include the hospital site
positioning should be same; additional letters may confuse cases in which multiple samples are identified with additional letters usually starting at beginning of alphabet; perhaps may work if site of origin letters are only taken from last 5 letters of alphabet : V W X Y Z
A single accession may include specimens used both for surgical pathology and cytology, e.g. a fluid used for cell block (surgical) and enhanced cytology. There is no reason to prescribe that different numbers be used since the preparation type is apparent from the slide..
We accession any cytology on case with the histology, generating one report. Within the report it clearly states which are cytology and which histology specimens, but as put the case on one case number (vs would need to generate two case numbers, then be sure to keep those cases together for the pathologist to review all material on case togerher) which could lead to material possibly not all be reviewed together. Our LIS is are able to designate "S" for the case number (with spec number e.g. 13S-123) that includes "s" for tissue and "c" for surgical cytology specimens, but not able to put that on the report under one case number.
I basically agree though the case type might not be necessary in all situations.
I only process surgical path, I do not need the 's'
same format for every institution such as S13-1000
We use letters and years but I know some label use only numbers starting from 1 but is still unique
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
I'm open to being convinced, but I don't see why case types must be distinguished specifically on the block in particular. Again, only limited information can fit on a block before codes get too cryptic or writing too small/illegible. Year and unique ID is fine-- and standard practice everywhere I've seen.
Our accrediting body allows us to define what the format is as long as it is unique
Requires major changes to our existing LIS, would have to create entirely new accessions. On the report I agree, not on blocks and slides.
If everything will fit. Sometimes causes problems with barcoding.
Not practical for research or veterinary setting
I agree with the statement provided that the lab divides cases by type. If they do not have different case types then I don't see a need to specify. For instance, if a lab chooses to have a single accession wheel for both surgical and autopsy cases and the "number" portion is not reused for different case types, then I don't see the need to require that the case type be included. For most labs the case type is going to be necessary.
Although every specimen accession should be represented by a unique alpha-numeric designation, including letters for the case type (i.e., S for surgicals; C for cytologies) should be left to the discretion of the laboratory. I see no patient safety reason why a lab couldn't include FNAs (for example) with their surgical accessions. I would change "numerical" identifier to "alphanumeric."
must be uniform, S13-9999 a, b, c or 1, 2, 3
I disagree with the "different format (eg, 13-9999S)" if you want a uniform labeling system.
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
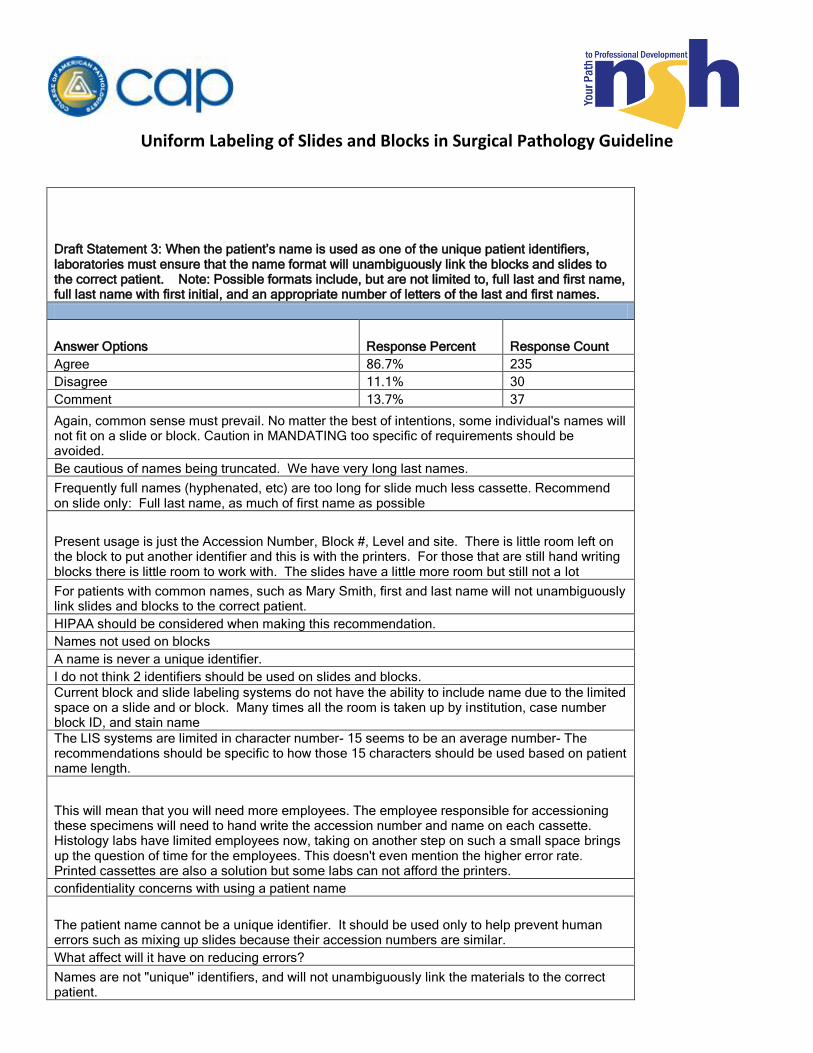
Draft Statement 3: When the patient’s name is used as one of the unique patient identifiers, laboratories must ensure that the name format will unambiguously link the blocks and slides to the correct patient. Note: Possible formats include, but are not limited to, full last and first name, full last name with first initial, and an appropriate number of letters of the last and first names.
Answer Options Response Percent Response Count
Agree 86.7% 235
Disagree 11.1% 30
Comment 13.7% 37
Again, common sense must prevail. No matter the best of intentions, some individual's names will not fit on a slide or block. Caution in MANDATING too specific of requirements should be avoided.
Be cautious of names being truncated. We have very long last names.
Frequently full names (hyphenated, etc) are too long for slide much less cassette. Recommend on slide only: Full last name, as much of first name as possible
Present usage is just the Accession Number, Block #, Level and site. There is little room left on the block to put another identifier and this is with the printers. For those that are still hand writing blocks there is little room to work with. The slides have a little more room but still not a lot
For patients with common names, such as Mary Smith, first and last name will not unambiguously link slides and blocks to the correct patient.
HIPAA should be considered when making this recommendation.
Names not used on blocks
A name is never a unique identifier.
I do not think 2 identifiers should be used on slides and blocks.
Current block and slide labeling systems do not have the ability to include name due to the limited space on a slide and or block. Many times all the room is taken up by institution, case number block ID, and stain name
The LIS systems are limited in character number- 15 seems to be an average number- The recommendations should be specific to how those 15 characters should be used based on patient name length.
This will mean that you will need more employees. The employee responsible for accessioning these specimens will need to hand write the accession number and name on each cassette. Histology labs have limited employees now, taking on another step on such a small space brings up the question of time for the employees. This doesn't even mention the higher error rate. Printed cassettes are also a solution but some labs can not afford the printers.
confidentiality concerns with using a patient name
The patient name cannot be a unique identifier. It should be used only to help prevent human errors such as mixing up slides because their accession numbers are similar.
What affect will it have on reducing errors?
Names are not "unique" identifiers, and will not unambiguously link the materials to the correct patient.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
This one is really hard to do when we get hypened names, or common names like Maria Rodriguez.
Item fro m 2 is standard and should be required. Name is totally optional.
names get close to unique only so as written doesn't work -- try looking up Jose Garcia or John SMith
I would recommend not using a name as an identifier
This presents all sorts of HIPPA issues if a bar code is not used.
I would prefer last name and first initial.
Sometimes it is very difficult to fit a full last name and first name on such a small label.
case number and patient's last name with first inital
If name is identical, LIS or EMR used should of course note multiple matches, and prompt somehow for additional identifiers (e.g. DOB, MRN).
Full name will not fit in some cases in a font that is readable.
Would have to be an appropriate number of letters. Many full last names alone will not fit on blocks and slides
Our accrediting body allows us to define what the format is as long as it is unique
HIPAA problems could arise with Name on slide when sending slides out of laboratory
No Names
I assume this to mean that the format used must be consistent across all blocks and slides.
It seems as if the decision has been made to use the patients name as the second identifier. This survey is not asking for the best choices as a second identifier.
common names present lack of specificity
the limitations of existing printing technologies, the need for legibility and the scant surface area for labeling of blocks that may require more info than simply case and name but alos specimen source, cutting protocol and additional conatiner and sample designations will make "unambiguous" difficult as character limits will need to be set.
Not enough information to agree/disagree
I think that the statement is phrased in a confusing manner. A name, even a complete name, is never considered a unique patient identifier by itself. The name format will not ensure that blocks/slides are linked to the correct patient since multiple patients may have the exact same names.
Current LIS version anfd the size of the label limits the lenght of the name. If the patient last name is very long it may be cut off and no first name will appear. I think this is acceptable
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
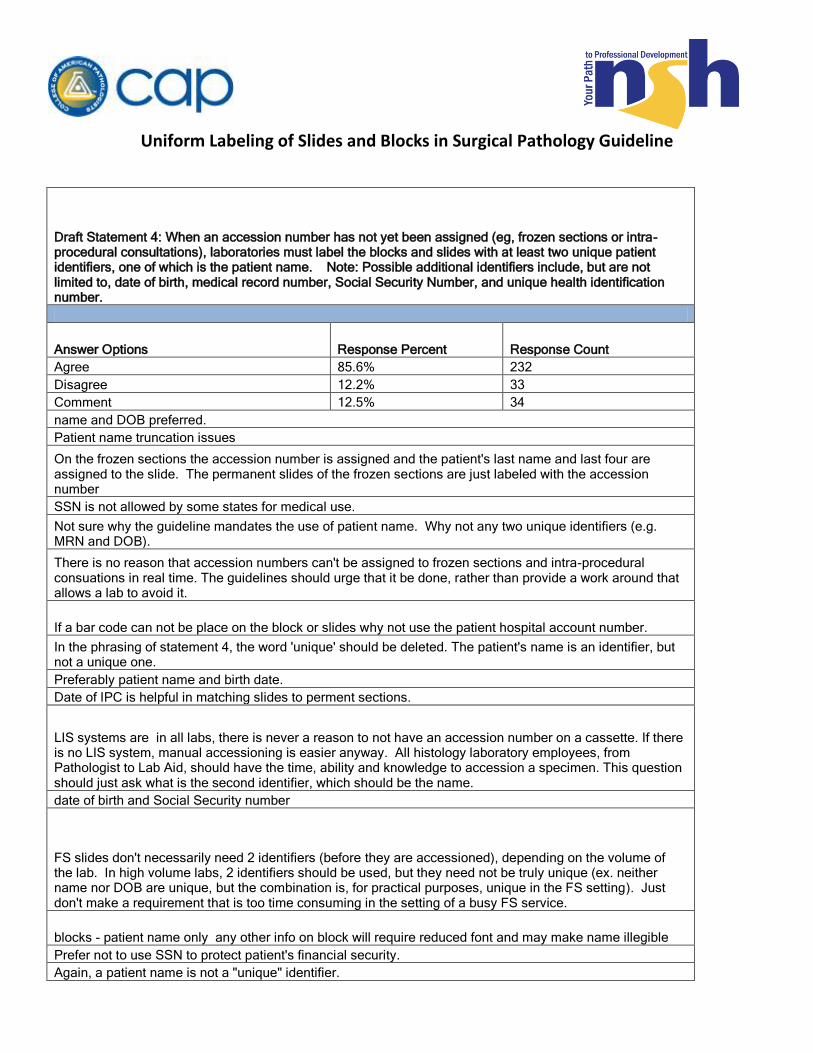
Draft Statement 4: When an accession number has not yet been assigned (eg, frozen sections or intra-procedural consultations), laboratories must label the blocks and slides with at least two unique patient identifiers, one of which is the patient name. Note: Possible additional identifiers include, but are not limited to, date of birth, medical record number, Social Security Number, and unique health identification number.
Answer Options Response Percent Response Count
Agree 85.6% 232
Disagree 12.2% 33
Comment 12.5% 34
name and DOB preferred.
Patient name truncation issues
On the frozen sections the accession number is assigned and the patient's last name and last four are assigned to the slide. The permanent slides of the frozen sections are just labeled with the accession number
SSN is not allowed by some states for medical use.
Not sure why the guideline mandates the use of patient name. Why not any two unique identifiers (e.g. MRN and DOB).
There is no reason that accession numbers can't be assigned to frozen sections and intra-procedural consuations in real time. The guidelines should urge that it be done, rather than provide a work around that allows a lab to avoid it.
If a bar code can not be place on the block or slides why not use the patient hospital account number.
In the phrasing of statement 4, the word 'unique' should be deleted. The patient's name is an identifier, but not a unique one.
Preferably patient name and birth date.
Date of IPC is helpful in matching slides to perment sections.
LIS systems are in all labs, there is never a reason to not have an accession number on a cassette. If there is no LIS system, manual accessioning is easier anyway. All histology laboratory employees, from Pathologist to Lab Aid, should have the time, ability and knowledge to accession a specimen. This question should just ask what is the second identifier, which should be the name.
date of birth and Social Security number
FS slides don't necessarily need 2 identifiers (before they are accessioned), depending on the volume of the lab. In high volume labs, 2 identifiers should be used, but they need not be truly unique (ex. neither name nor DOB are unique, but the combination is, for practical purposes, unique in the FS setting). Just don't make a requirement that is too time consuming in the setting of a busy FS service.
blocks - patient name only any other info on block will require reduced font and may make name illegible
Prefer not to use SSN to protect patient's financial security.
Again, a patient name is not a "unique" identifier.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
These procedures are done one at a time. I believe there is sufficient time to assign a accession number while the pathologist is reading the frozen sections or immediately following the procedure. A name will suffice in the meantime.
Name (F,L) alone is sufficient in low volume laboratories that do not do multiple cases at the same time. OR assign a temp. surgical pathology number.
For situations where questions 3 and 4 could apply at the same facility, identifiers should be consistent.
why insist on a name when dob, rmn are more unique? Agree with 2 identifiers on FS slides etc
It is sufficient to label the blocks and slides with patient name only.
There is very limited space to label slide. Manually labeled slides take up even more space.
May not have time/ space to include patients' name and another identifier along with the part and FS/pass # on the slide
Again, blocks may not be able to fit two IDs legibly. Requirement for two IDs on a slide may be needed in larger labs where there may be multiple consults going on simultaneously. In a small lab where this almost never happens, it seems excessive to me. We assign accession numbers also immediately when the consult (i.e. frozen etc.) is received.
Two identifiers are sufficient. No SSN please.
Our accrediting body allows us to define what the format is as long as it is unique
Slides, not blocks, again due to the lack of space and time when we are still manually labeling blocks.
I think with today's bar coding a barcode that tracks back to requisiton submitted with request for frozen and dob or name and bar code etc would be sufficient for 2 unique identifiers,
I would be stronly opposed to the use of the social security number (whole or last 4). MRN would be my preference.
I don’t disagree with this recommendation, but the wording seems to suggest that when an accession number has been assigned, only one identifier is sufficient. If you're going to require two identifiers for all slides, this should be changed to “Laboratories must label slides with at least two unique patient identifiers, including the accession number if one has been assigned. When an accession number has not yet been assigned (eg, frozen sections or intra-procedural consultations), one of the identifiers must be the patient’s name.” As I stated previously, I do not think you should require two unique identifiers for cassettes, so I would restrict this to slides.
Yes, two identifiers should be used, but social security number should not be one of them. SSN's are sensitive patient information that many groups have suggested should never be used as a patient identifier.
all blocks and slides are first accessioned. use the case number and last name
We currently label frozen section slides with patient's name and add the accession number when it's available, usually within minutes after receiving specimen.
Pt name only should suffice. How many different Bob Smiths are going to have frozen sections the same day in the same lab??

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 5: Laboratories should label each specimen container with a unique alpha-numeric designation and each block and slide from that specimen container should have the same corresponding designation.
Answer Options Response Percent Response Count
Agree 97.8% 261
Disagree 2.2% 6
Comment 3.4% 9
Specimen A, B, C. Blocks A1, A2, B1, B2, C1, C2, CFS1
I would agree to this as long as there was a key to look up what the designation represented.
Absent robust outcome evidence of the safety in this particualr context of alternating letters and numbers, there is no need for such discussion.
Clarify what you mean. Accession number? If not, number is adequate; or simply A, B, C... regardless of Site - refer to requisition - e.g., A might be same part as B, only one is superior one is inferior
speimen containers should have the identifier on both side and top of container
however there still needs to be made a designation which one is the block and slide
Small bottles whose tissue will be all embedded do not need year or type designation; last two numbers may suffice.
This recommendation should reflect the fact that you’ve already recommended a unique number for each accession. Also, the statement that each block and slide should have the same corresponding designation could be misunderstood to mean that they should all be labeled identically. Perhaps you could say “Laboratories should label each specimen container with a unique alpha-numeric designation that incorporates the accession number. Each block and slide prepared from that specimen container should be labeled with that unique alpha-numeric designation.”
Alternating letters and numbers are crucial. For example, particular sites sampled from a single accession should be identified in such a way there is no possibility of misreading or misfiling the slide & blocks, e.g., Several blocks from a case, S13-100, should be S13-100 A, S13-100 B, or S13-100 A1, etc, not S13-100 1, S13-100 2 etc.
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
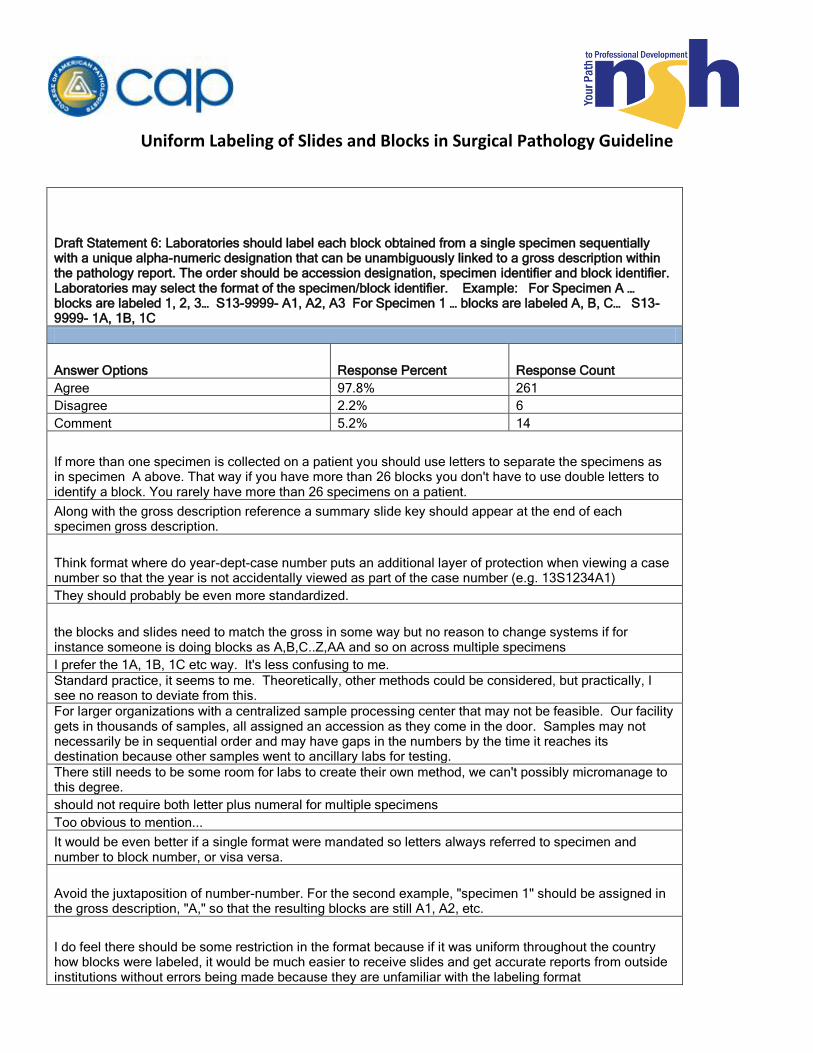
Draft Statement 6: Laboratories should label each block obtained from a single specimen sequentially with a unique alpha-numeric designation that can be unambiguously linked to a gross description within the pathology report. The order should be accession designation, specimen identifier and block identifier. Laboratories may select the format of the specimen/block identifier. Example: For Specimen A … blocks are labeled 1, 2, 3… S13-9999- A1, A2, A3 For Specimen 1 … blocks are labeled A, B, C… S13-9999- 1A, 1B, 1C
Answer Options Response Percent Response Count
Agree 97.8% 261
Disagree 2.2% 6
Comment 5.2% 14
If more than one specimen is collected on a patient you should use letters to separate the specimens as in specimen A above. That way if you have more than 26 blocks you don't have to use double letters to identify a block. You rarely have more than 26 specimens on a patient.
Along with the gross description reference a summary slide key should appear at the end of each specimen gross description.
Think format where do year-dept-case number puts an additional layer of protection when viewing a case number so that the year is not accidentally viewed as part of the case number (e.g. 13S1234A1)
They should probably be even more standardized.
the blocks and slides need to match the gross in some way but no reason to change systems if for instance someone is doing blocks as A,B,C..Z,AA and so on across multiple specimens
I prefer the 1A, 1B, 1C etc way. It's less confusing to me.
Standard practice, it seems to me. Theoretically, other methods could be considered, but practically, I see no reason to deviate from this.
For larger organizations with a centralized sample processing center that may not be feasible. Our facility gets in thousands of samples, all assigned an accession as they come in the door. Samples may not necessarily be in sequential order and may have gaps in the numbers by the time it reaches its destination because other samples went to ancillary labs for testing.
There still needs to be some room for labs to create their own method, we can't possibly micromanage to this degree.
should not require both letter plus numeral for multiple specimens
Too obvious to mention...
It would be even better if a single format were mandated so letters always referred to specimen and number to block number, or visa versa.
Avoid the juxtaposition of number-number. For the second example, "specimen 1" should be assigned in the gross description, "A," so that the resulting blocks are still A1, A2, etc.
I do feel there should be some restriction in the format because if it was uniform throughout the country how blocks were labeled, it would be much easier to receive slides and get accurate reports from outside institutions without errors being made because they are unfamiliar with the labeling format

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 7: When multiple slides are cut from a single block, laboratories should label each slide continuously in order of cutting. This slide identifier should come after the specimen identifier and block identifier. Example: S13-9999-A1-1, S13-9999-A1-2, S13-9999-A1-3 Note: The laboratory may determine the exact labeling format for multiple slides.
Answer Options Response Percent Response Count
Agree 89.9% 240
Disagree 9.0% 24
Comment 11.2% 30
any deeper levels have " additional slide"
Our LIS does not store the slide level number, would be hard to place on a label electronically
when cutting multiple slides from the same ribbon, not always important to have slide order
I personally feel it is easier to have L1, L2, L3, etc in the center of the slides as this seems easier to see
that seems confusing to me, it can be mis-interpreted
S13-9999-A1-L1 (for level 1)
With the obligatory, where necessary. Initially, the sectioning is important for the pathologists, but further cutting for stains doesn't require cut numbers so long as the focus of DX is still present UNLESS otherwise noted/requested by a pathologist.
This may be problematic if LIS access is not available at each cutting station or if HTs are responsible for adding notes to paraffin blocks.
The example could be confusing. A better labeling method would be Recut 1, Recut 2, or Step 1, Step 2
some pathologists prefer slides to say 'Level-1, Level-2, Recut-1 or Deeper-1, Deeper-2".
So long as they can be separate lines e.g., line 1: S13-9999 Line 2 (or alternate location) A1-1
The lab should label each slide continuously in order of cutting, but the example shown is a confusing format. The order number should not be written on the same line as the accession number for better clarification.
We do this by use of parenthesis [eg: 13S1234A1(1)]
easier to see deeper1 or recut 1 recut 2 recut 3
While I would like to agree, this may be difficult for the LIS to accomplish. I'll use an example of slides which levels are taken for H&E along with blank levels for possible later use for ihc. The LIS is going to label the H&E levels A-1-1, A-1-2, A-1-3 because the other slides have not been given to the pathologist, and may never even be stained. If ihc is requested, these slides will be given numbers A-1-4, A-1-5, A-1-6. With our LIS we also have controls built in. We do not batch controls, but each antibody for each case has its own set of control slides. These slides are also given unique slide identifiers.
In our department, we hand write on our printed labels a designation for levels/deepers to denote additional deeper sections taken from a single block.
If levels are they L1, L2, & L3?
The slide number can be confusing to many. It's determined at accessioning and added later when requested. Slide number should be indicated only if levels or deepers.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
With our practice, the orginal slide is not labeled with levels, recuts are labeled with levels" recuts 4-8 "
This works for the initial set of slides. When additional levels/stain/recuts etc. are ordered there is no way to tell where to start with the third designation. With multiple additional orders this number would get more confusing than helpful.
I agree that they need to be designated but would designate them different from above
The example is good; standardize the laboratory practice to this format rather than allowing labs to determine format.
I disagree because I feel that to making too many changes are too many numeric values on lettering can make for some type of confusion for the future
Levels should be indicated as levels
another numeral is too easily confused with other parts of slide identification, should add letter or word e.g. "level" or Lev"
Many if not most AP lab IT systemns are ill-equipped even today to assist with sequential labeling of slide sections perfectly.
Prefer alphanumeric L1, L2, etc (level1, etc) or S1, etc (serial 1) depending on whether these are deeper step levels or serial levels from same ribbon
It may be useful to discuss the situation where recuts are obtained at a later date. Histology personnel may not know if (or how many) levels were prepared earlier.
Again, it would be preferable to mandate what the format should be for designating additional levels so everyone understands labels from any institution.
Should be standardized across country how labeling is performed

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 8: The laboratory should label the slides with the histochemical (HC), immunohistochemical (IHC) and/or special procedure (eg, FS, touch prep) after the accession, specimen, block and slide identifiers. When the HC technique or IHC antibody clone used may affect the interpretation, that information should also be included on the slide. Example: S13-9999- A1-1 FS S13-9999-A1-1 Pan-Keratin (AE1/AE3) S13-9999- A1-1 AFB (versus S13-9999-A1-1-Ziehl-Neelsen or S13-9999-A1-1-Wade-Fite) Note: The panel concludes that surgical pathology slides without an explicit stain name are inherently implied to be an H&E stain; no additional labeling is required. The EP also believes that the labeling of control slides or control tissue on test slides is beyond the scope of this project; however, they conclude that laboratories should establish a clear and standardized method for distinguishing control tissues from patient tissues.
Answer Options Response Percent Response Count
Agree 92.1% 245
Disagree 6.8% 18
Comment 11.7% 31
all our QC slides have it clearly identified - Trichrome QC
slide order is important no mattter the test/stain applied
Again I like it in larger letters and in the center, above the actualy specimen # (identifier) S13-1999
controls and negative should be labeled as such
Again - common sense indicates that all of the information may not fit on a slide. I consider the order DESCRIPTION in the LIS (eg. Pan-Keratin) can include the clone details, the slide label needs to be uncluttered and easily read by humans to prevent errors.
This is too cumbersome. This is the type of information that should be relegated to the Path Report. Yes, the stain designation should be apparent from tle ID on the slide so the stains can be distinguished but we're basically asking for a prelim Path Report on the slide label now.
I see no need to have an antibody clone on the slide label even when it may affect interpretation. The report should specify said clone.
Antibody clone should only be included if multiple clones of the same antibody exist in the practice
If control sections can not be on the same slide as the test patient, the control slide must have the case number(s) listed in it for traceability purposes. Ideally the control should be in the same slide as the patient sample but this not always possible. Example. S13-99999. Gram CONTROL
Clone information will be difficult to document on each slide, it should however, be known to the pathologists through other means, and signed off by an approving pathologist if changed.
limitations of space on a label # of characters
clone name not necessary
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
In our lab we have two seperate platforms that generate our labels in different formats for our IHC versus our H&E stains, however the two identifier concept is applied in this manner.
S13-9999-AFS1-1, S13-9999-BFS1-1,etc.
I think we are moving toward including clone information in reports but certainly doesn't need to be on a slide; this info is discoverable if it really matters in the report or in lab SOPs
Ctl designation by label format or write on patient slide
I would prefer the first or second choice.
because of the number of different stains- I feel the H&E should be identified as such
I hear there are some labs that actually something other than an H&E as their "standard" stain (e.g. Movat pentachrome or whatever). Non-H&E "standard" stains should probably be labelled with the stain name, in case the slides are reviewed by outside institution(s).
Clone is getting a little silly, that information would be available in a manual.
If the full name of the procedure cannot fit, an easily understood abbreviation can and should be substituted
Why not include control labeling in this process, or do you believe that it would be too complex if one control is used for multiple cases, how would you label for that?
Again agree need stain and case number bu the A1-1 I disagree with
Control slides are necessary and should be identified as well
I think every institution should be able to format labels their own way. No need to mandate label formats.
would not include clone on slide, can be found in IHC report
stain names/clones/etc may need to be abbreviated due to space limitations and this should be explicited supported/accepted
prefer FS to precede block number
FS and TP should be accepted as slide identifiers as well. Our software designates the frozen block as FS anf the numbering of the rest of the blocks starts wilth A. (1 FS and 3 regular blocks equals 4 total blocks. Blocks are labeled as FS (if multiple, then FSA, FSB) and the other blocks as A, B, C. This should be acceptable.
I believe H&E should be placed on the slide
IHC or other special stains need only to include the name of the stain or Ab. Including clone information and other detailed record-keeping should be available in the workbench records, not necessarily on the slide label. Too much information may dilute the essential data (i.e., ID and stain). In other workds, there is a risk of lowering the "signal:noise ratio" on the slide label. I agree with the other points.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 9: No recommendation can be made for or against standardization of abbreviations and conventions.
Answer Options Response Percent Response Count
Agree 80.9% 212
Disagree 14.1% 37
Comment 13.4% 35
always try to avoid abbreviations if possible
As long as a clone or test methods are maintained in the lab.
Standardizing will be very costly to smaller hospitals
the labeling of recuts should be standardized as all labs label differently, not always clear as to what they mean
Use of multi-dimensional barcodes would allow all of this info to be captured for each specimen and subsequent slides/stains.
Prefer to see a uniform, standardized abbreviation and labelling
As a large lab it would be great if there was a standardized way of labeling specimens as we get a lot of outside cases that are labeled haphardley.
It may not be possible to standardize abbreviations nationwide or internationally. But each lab should be required to establish and conform with their own list of standard abbreviations, which should be made available to all relevant personelle.
Each lab must have a 'key' or 'legend' in their procedure manual which clarifies abbreviations and conventions of stains.
Standarization of abbreviations should be compliant with hospital based approved abbreviations if these are to be used in a document that will be included in the final medical record.
Due to finite amount of space on a label, we have a listing of acceptable abbreviations for stain names, ect. that are used in the department. Since some labs have technology to support labeling and some still perform by hand, think the best possible choice at this time would be for each lab to determine what abbreviations are acceptable for their use (keeping in mind how terms generally shortened in the Pathology community).
every lab should adopt their individual 2 identifiers
That's true. In our hospital system, we have lab assistants writing Alcian Blue in these formats: Al Bl, A. Blue, AB.
I believe that a standard abbreviation for HC stains in particular would be useful to specify the particular staining convention used on a specimen, for example Brown-hopps vs Brown-Brenn gram stains. IHC stains would be more of hurdle and I see no need to apply this concept to those stains especially considering the seemingly constant growth of these markers.
agree generally, but format could be standardized as in syntax or could be required to be defined as checklist item for SOP for accreditation
For the future, t would be really useful and safe to have standard abbreviations
I don't think standardization can be recommended so there is no recommendation for standardization; not for or against
Use ISO standards whenever possible.
If there is no standard it must be defined in the report

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
An attempt should be made to standardize abbreviations across the globe. One of the problems in particular is the fact that a particular antibody can be called by several different names. This should be changed so that a specific antibody has one name used globally.
recommend that each laboratory must have its standarized list that is readily available for outside institution, if requested
A recommendation could be made to perhaps improve standardization, but admittedly yes, it'd be onerous to enforce and continually update. Probably wouldn't satisfy anybody.
I agree that it would onerous and unnecessary
I don't agree that IHC is reasonably standardized - current practice varies from labeling with short abbreviated name of the analyte to catalogue-derived names "BRST-2" and even clone designations. I think there should at least be consensus that the slide label should identify the analyte being tested.
Again do you feel that this would be too much work?
Recommended abbreviations would be a good start but items requiring changes would be onerous
I agree but from past experience I believe that both pathologist and technologist need to more aggressive when writing down patients identified on these slides it is imperative otherwise errors will continue
If standardization is to be implemented, it must be incorporated into current practices over time.
current systems can be grandfathered but all new systems developed should use standardized labelling
It would be painful, but standardized abbreviations should be adopted. Misinterpretation of abbreviations is a classic cause of medical error. Although I agree it is infrequently a problem in this setting, I have seen cases where abbreviations were misinterpreted, resulting in diagnostic error.
absolutely imperative to institute standard labeling
Where universally accepted abbreviations exist, e.g., CD3, CK7, CK20 exist, there should be an effort to use them. Where there are alternative conventions, e.g., Melan-A & MART-1, no standardization is likely to be achieved.
Standardization of abbreviations should be a goal in pathology as it should throughout medicine.
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
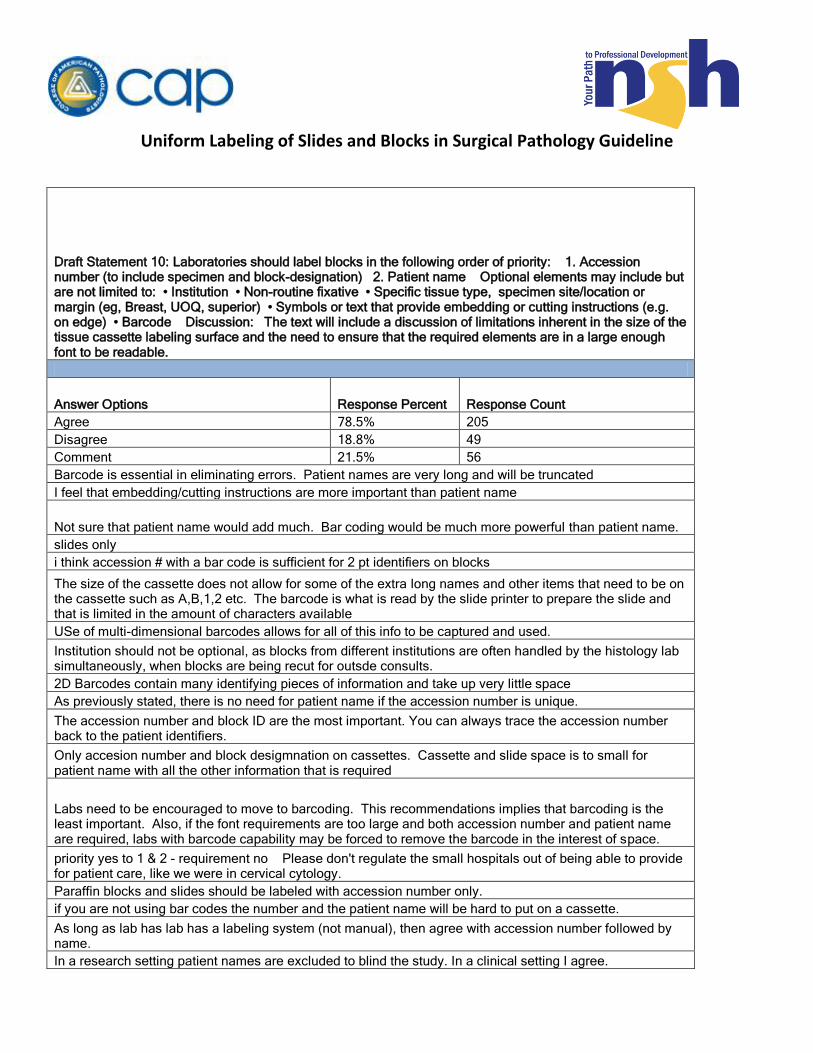
Draft Statement 10: Laboratories should label blocks in the following order of priority: 1. Accession number (to include specimen and block-designation) 2. Patient name Optional elements may include but are not limited to: • Institution • Non-routine fixative • Specific tissue type, specimen site/location or margin (eg, Breast, UOQ, superior) • Symbols or text that provide embedding or cutting instructions (e.g. on edge) • Barcode Discussion: The text will include a discussion of limitations inherent in the size of the tissue cassette labeling surface and the need to ensure that the required elements are in a large enough font to be readable.
Answer Options Response Percent Response Count
Agree 78.5% 205
Disagree 18.8% 49
Comment 21.5% 56
Barcode is essential in eliminating errors. Patient names are very long and will be truncated
I feel that embedding/cutting instructions are more important than patient name
Not sure that patient name would add much. Bar coding would be much more powerful than patient name.
slides only
i think accession # with a bar code is sufficient for 2 pt identifiers on blocks
The size of the cassette does not allow for some of the extra long names and other items that need to be on the cassette such as A,B,1,2 etc. The barcode is what is read by the slide printer to prepare the slide and that is limited in the amount of characters available
USe of multi-dimensional barcodes allows for all of this info to be captured and used.
Institution should not be optional, as blocks from different institutions are often handled by the histology lab simultaneously, when blocks are being recut for outsde consults.
2D Barcodes contain many identifying pieces of information and take up very little space
As previously stated, there is no need for patient name if the accession number is unique.
The accession number and block ID are the most important. You can always trace the accession number back to the patient identifiers.
Only accesion number and block desigmnation on cassettes. Cassette and slide space is to small for patient name with all the other information that is required
Labs need to be encouraged to move to barcoding. This recommendations implies that barcoding is the least important. Also, if the font requirements are too large and both accession number and patient name are required, labs with barcode capability may be forced to remove the barcode in the interest of space.
priority yes to 1 & 2 - requirement no Please don't regulate the small hospitals out of being able to provide for patient care, like we were in cervical cytology.
Paraffin blocks and slides should be labeled with accession number only.
if you are not using bar codes the number and the patient name will be hard to put on a cassette.
As long as lab has lab has a labeling system (not manual), then agree with accession number followed by name.
In a research setting patient names are excluded to blind the study. In a clinical setting I agree.
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Space on blocks is very limited, We have a barcode tracking system and a barcode is not optional. Since the barcode is a necessity we only have room left over for the accession number - There is no room for a second identifier i.e. patient name
do not agree with patient name barcode instead
I agree except for the patient name. The patient name should be the last item in the list, because its purpose is for preventing human error, not primarily to identify the slide. Also, having the patient name, while reasonable, is not essential for this purpose--you could use initials, a truncated patient name, or something else. A question--does having the full patient name on the slide/block raise a HIPAA issue if you have slides sitting on the counter in the pathology office where visitors may be present? Having the font large enough to read is critical, especially for us older pathologists!!
Problematic for labs without cassette printer and is it proven to reduce errors
Difficult to include 2 ID unless lab has automatic cassette labeler
In our hospital, we only write the accession number on the labeling surface of the cassette. We fear the labeling will be unreadable with more information for older techs. Optional elements are written on the side of the cassette.
For a lab using a cassette labeler, this will certainly be much easier than the lab still hand labeling. We still write cassette identifiers, and include the accession number on the face of the cassette. On the side are other elements such as year, laterality, or cutting instructions. There is no room to include the patient name when writing.When we send blocks out, a slide label is placed onthe top of the block. Although not an ideal solution, it does provide the recipient with the correct, detailed information to return the specimen block to the correct lab.
Blocks ..accession number only wth block designation. Do not even include ANY discussion about other informaton. It will turn into a requirment.
Accession number should be traceable to patient Name.
3D bar codes, as an optional element, can contain an enormous amount of information
Cassettes are not large enough for patient names and accession numbers.
Hardest rule to implement will be fitting case number and name on cassettes.
Limited space prohibits case number and name. There would be no space for the specimen type, prudent to the histologist.
Currently, there isn't enough room on a block to have a patient's name and an accession number if you also need to have other elements like bx, FS etc which usually come on the second line
I believe the name should come first. When looking at many slides it is easy for the numbers to be confused. Names are more unique and seem to be easier on the eyes.
not much room on the blocks for name AND accession number
Again, caveat regarding ability to fit patient's name on a cassette legibly.
The Barcode can be considered another ID to substitue patients name,, I think that should be a consideration
The barcode is a unique identifier and essential to have present for workflow. It is a proven way to limit labeling errors. Using the barcode to scan the case essentially links that block with all patient identifiers and the accession number. The barcode within our system would be the number one priority for identification and patient safety.
I don't feel there is sufficient space on the block to add more than the accession number. If a case is to be sent out of the lab a label containing the additional information could be added to the back of the block
Again, patient name fitting on a block will be difficult when hand-written; would liklely be illegible. Hard enough of a slide but at least doable and would still be legible.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline If there isn't space these two criterion are most important
currently we use 1. accession # and a barcode
given the demonstrable reduction of labeling errors reduction, and the augmentation of proper handling, processing, transit and storage of materials when using barcodes, I would think that the barcode should be an essential element, probably more important than patient name if there is limited space on the label. I would, in fact, suggest that the committee make a strong recommendation in favor of the routine use of integrated barccodes in histology practice.
I agree with 2 identifiers (accession and patient initials, but full patient name and other information does not wirh our current labeling systems due to size limitations and barcodes
disagree with patient namesthis will add cost to test to add names to each block and slide when reimbursemenst are consistently decreasing
patient name could be problematic because of spacing. However, specimen case #/date would be a minimum.
Patient name should not be included; this prevents preferential treatment of one case to another and also protects patient/client privacy. Accession number is suffiecient but inclusion of other institutional identifiers should be allowed.
No Names.
Again, it seems as if the decision has been made to use the patients name as the second identifier. This survey is not asking for the best choices as a second identifier.
I would again suggest that in a quality lab with single-piece workflow the value of specimen cource and special instructions may outweigh the value of adding the name identifier where surface area is limited
I believe that institution should be required. I am not sure that patient name is reasonable to include on blocks due to space limitations. Local medical record number may be an acceptable alternative, especially if institution is included.
As stated before, for labs without automated labeling systems, there is insufficient room on tissue cassettes to have two separate unique identifiers along with other necessary markings.
2nd patient identifier should not have to be patient name. Other unique identifier would be OK, or even preferable as names are not unique. How about the medical record number?
Accession number first. Institution designation might be more important, than patient's name, if the block is sent to an other laboratory for processing. Embedding and cutting instructions would be the second most important if the block is processed in-house. It would go to third place, if the block is sent to an other lab.
We hand write the acc #. Adding a name will be overly time consuming, particularly for large cases.
Barcode is essential to prevent errors
I have not seen many blocks with more than accession number, block designation and maybe a bar code.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 11: Laboratories should label slides in the following order of priority: 1. Accession Number (to include specimen, block, and section number) 2. Patient Name 3. Stain /Procedure Name Optional elements may include but are not limited to: • Institution • Non-routine fixative type • Specific tissue type, specimen site/location or margin (eg, Breast, UOQ, superior) • Barcode Discussion: The order was previously addressed in KQ 1-4. The text will include a discussion of the benefits of including institutional name for reducing errors related to consultations.
Answer Options Response Percent Response Count
Agree 81.2% 211
Disagree 17.3% 45
Comment 17.7% 46
maybe here is where abbreviations could be used for the individual hospitals
Switch 2 and 3
Agree but we use Accession # and patient medical record number (MRN), stain, and procedure name.
I feel that stain/procedure name is more important than patient name.
Section number is not stored in our LIS
Again with a unique accession number, not sure that patient name adds that much value
Our facility consists of two hospitals so we have to put our institution name on the block and slide. Therefore when a block or slide is sent it is identifiable for proper return.
Technology must be used to take this field beyond the manual state of today - use of 3-D barcoding or other advances should be a priority.
Needs additional input
Institution should not be optional, as slides from different institutions are often viewed simultaneously, when reviewing a current case and a consult case on the same patient.
If Institutional Name is not on slides I suggest a 'generic' label with Institutional Name AND Address (at least City/State) be placed on the opposite side of the slide when slides leave the Institution. Just think how many "General Hospitals", "Mercy Hospitals", "St. John's Hospitals" etc. there are in the world.
Accession numbers can be traced back to 2 patient identifiers. Patient name on blocks and slides is unnecessary and could result in possible HIPPA violations if not disposed of properly.
Accession, Stain / Procedure Name / Institution. No Patient name- no room on the slide for it
Labs need to be encouraged to move to barcoding. This recommendations implies that barcoding is the least important. Also, if the font requirements are too large and both accession number and patient name are required, labs with barcode capability may be forced to remove the barcode in the interest of space.
Label slides and blocks with accession number only
As long as lab has lab has a labeling system (not manual), then agree with accession number followed by name.
In a research setting patient names are excluded to blind the study. In a clinical setting I agree.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Again with a specimen tracking system the barcode is not an optional element on anything. Space is limited - barcoding/specimen tracking is the way of the future - barcode needs to be included on the primary list of patient identifiers
no patient name
Order as follows: 1. Accession Number 2. Stain / Procedure Name 3. Institutional name 4. Patient Name
Agree except for the name. See question no. 1 above for further commentary.
Institution should be on all slides.
accession number, stain/deeper or recut, pt name, hospital or institution
facility should be required. Syntx for tissue that affects handling should be standardized syntax defined in SOP
Including patient names creates space issues on slides and blocks. The accession numbers need to be as large as possible for the benefit of the pathologist. If you shrink these numbers to fit another identifier, you are only going to create an environment for conducive for errors. If the pathologist cannot easily identify the accession number, the chance for an error is increased. Also, not all laboratories are large enough to warrant having a bar code system. Fitting just the accession number, block number, level, and any additional stains takes up all of the room on the slide, leaving no room to include a patient name.
I prefer only the first three identifiers and also a date.
The human readability aspect is essential for priority #1 and 2. When a barcode can provide all of this information and more it should be a higher priority depending on the computer system and workflow and use of the barcode.
The order to which laboratories label slides is arbitrary as long as it is traceable.
I feel that this is the best way so that we know what slides to expect when we need to come back to current cases and pull them in the future.
we currently do all of the above except for the patient name
given the demonstrable reduction of labeling errors reduction, and the augmentation of proper handling, processing, transit and storage of materials when using barcodes, I would think that the barcode should be an essential element, probably more important than patient name if there is limited space on the label. I would, in fact, suggest that the committee make a strong recommendation in favor of the routine use of integrated barccodes in histology practice.
Again SAccession number yes, patient intials only or barcode number etc i don't believe patient name should be only option, then stain
against adding patient name
Pt name and stain unnecessary in routine slide
Patient name should not be included; this prevents preferential treatment of one case to another and also protects patient/client privacy. Including of accession number and procedure is sufficient.
No Names
patient name should be optional
I think that Institution should be required, and that it is more important for slides than blocks since slides are much more frequently shared/moved between institutions. I am not sure if there is enough space to include complete names. local medical record numbers have the advantage of being of finite length, so I would prefer Acc Num, Insititution, MRN, leading XX characters of last name and first initial
This conflicts with the recommendations under Question 1. Those state that patient name can be one of the two unique identifiers, but name is not required. Perhaps this could be changed to 1. Accession number; 2. Other unique identifier; 3. Stain
Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
I think the institution name should be required. I see every now and then a consult where we can't figure out where the slides originated. Also what about medical record number as an alternate patient identifier to name?
1. Accession number 2. Institution 3. Patient name 4. Stain These identifiers fit on the label, if the patient full name is not a requirement (which is an issue with very long names)
No room on a shortened bx label for name.
Barcode is essential to prevent errors
Patient name, accession number and stain name should be the same point size and easily readable. NO MICROPRINT!!!!!
Because slides are often sent from one institution to another I believe the institution should be on the label unless there is

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 12: Laboratories should label blocks and slides received in consultation with their own institution’s unique accession number. Laboratories should not obscure the original label when relabeling. Discussion: Suggestions include double labeling on the back or bottom of the slide if necessary, and application of a label to the back side of the paraffin block, with addition of paraffin if needed.
Answer Options Response Percent Response Count
Agree 91.2% 237
Disagree 8.1% 21
Comment 10.8% 28
toom many of our refered out slides have had our label obscured
Technology via 3-D or other barcoding will allow all info to be captured and tracked.
While I agree with this in theory, it is difficult to not obscure the original label. If we follow the guidelines after someone else has already followed these guidelines, there is no reasonable way to not obscure the original. Best case scenario, one institution etches slides while another labels so the information is available but obscured. With two labels and the need for this information, one must be covered to have the second available. Technology often prevents double labeling because, for example, our coverslipper would malfunction with the extra thickness of a double labeled slide.
This is not feasible in high volume automated scenarios. You must place the label on the front and top of the slide. Perhaps a digital image could be captured of every received slide (or collection of received slides) to preserve original labelling data.
Per my comment on previous question, the receiving lab label should not completely cover the sending lab's label.
Such relabeling is necessary only if the reference institution intends to retain the slides or blocks. If they are returned to the referring institution, that institution's unique identifier is sufficient if referenced in the consultant's report.
Any correspondence (reports issued, letters) should contain both the original and consultation case numbers.
Leave it to the lab. I don't like getting slides back when I can't read the original label, I don't want to get new S13-9999 mixed up with my institution numbers. The consultants are responsible for using my patinet name and number in thier own way... How does Mayo do it?
label over top of original label, new label must have reference site unique accession number on it.
Yes, unless labeling somehow interferes with the use of the slide or block in the evaluation.
some original labels are paper and will not stand up to solvents, etoh, ss etc.
The challenge of double labeling a slide without obscuring the original label is a difficult one. Being able to view the original label has merit upon return of the consulted slides to the original institution. As long as the double labeling on the back of the slide doesn't cause issues with the automated processes such as staining and coverslipping, I believe this would be the best option.
Referral lab should NOT add anything to the slide. Imaging of the slide is possible and documentation of the slide, block, etc. can be put in the referral report.
also should track original label designation in electronic records, source and date of receipt. Could be an identifer in assigned unique number such as OU for outside case in accession number, but always retain or track original label

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline Consult should be a separate and unique system, this is a topic for future discussion.
Concern about confusion or the opportunity to miss the corrected label on the back side of the block. Using a corrected label over the top of the patient information section of the cassette should also be allowable. The previous information is still available by peeling back the corrected label.
The block can also be labeled on the side rather then the back side
Wholeheartedly agree with consult institution NOT obscuring the initial labelling. I'd also recommend against using the underside of the slide-- the label in this position inhibits the ability to properly maintain the focus plane, and is particulary noticeable when on higher-power objectives.
Our accrediting body recommends this approach.
THis is ideal but not always feasible, I think being able to identify specimen as consult, and having your labs accession number and being able to track through that accession number the original site and their accession should be sufficient.
We put a slide label on each consult block, and label each consult slide with a label on the back
Original identifiers should remain for traceabiltiy.
I am not in favor of applying a label to the back of the slide. It raises the slide and interferes with viewing the specimen under the microscope.
Not sure double labeling of block is necessary.
new label can overlay the original due to space
I do not receive cases for consult.
Sometimes cases go to more than one outside institution. I really dislike labels placed on the back of slides.
We receive very few slides for consultation and they are all "confirming consults" for patients coming to our hospital for treatment. I feel this should be optional.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Draft Statement 13: If additional H&E, special, and/or IHC stains are prepared from the consultation block, laboratories should label slides in the following order of essential elements: 1. Accession Number: a) Surgical Pathology/Year/unique number (Exact format TBD by laboratory) b) Specimen followed by block followed by slide designation followed by stains and/or procedures (Exact Format TBD by laboratory) 2. Patient Name Discussion: The text will note that the CAP LAP requires an accession number. The text will provide a general discussion on the relabeling of slides and how not to deface original slide labels. The text will also include a general discussion on some of the challenges of tracking consultation slides if the original institution’s name is not on the label.
Answer Options Response Percent Response Count
Agree 85.3% 221
Disagree 11.2% 29
Comment 14.7% 38
Slides prepared and generated from consult material should have the accession number of perorming location applied. We use a consultation case prefix OC-13-999 with each consult case listed as specimens A, B, etc.
Accession number and patient medical record number which is a more unique identifier in our system.
Most slides received for consultation do not have room to label with multiple identifiers
Barcode is essential
Again, not sure that patient name is value added in light of a unique accession number.
Technology via 3-D or other barcoding will allow all info to be captured and tracked.
There is not enough space to fit all of this AND it be large enough to be easily read
Currently we accession consult cases and include both the original case information AND our new accession case information on the slide labels. We do NOT overlabel the referred block at all, as it is searchable in the LIS.
Patient name unnecessary.
You should have the original institutution's name in the report that you issue. There is no reason to have the submitting institution's name on any slides you produce.
No patient name. With all the information required on the small slide label, will not fit
If have a manual system, then putting patient name can be an issue. Agree with doing it as stated if lab has automated labeling system.
Again with barcode tracking systems the barcode is not an optional item - space is very limited
Di=o not agree with 2. label font size limitiations
b. If by specimen you mean the referring institution accession number, I agree. If you mean the anatomic site, I disagree.
This is not clear WHOS accession number? original lab or referral. This is poorly written and should be discarded as written.
This is unclear -- whose accession number and what is specimen about. Presumably consultation blocks should get a specific identifier just like a primary specimen. Thus your priorities should be the same of accession, some hint at block number and then stains.

Uniform Labeling of Slides and Blocks in Surgical Pathology Guideline
Name should not be on the label. Imagine if your lab does not have an automated labeling system how this label would look. There is only so much information that can fit into the space on a slide label or block label.
A new label could be on back or bottom if possible.
This needs more work. Not clear
Again the order is arbitrary as long as it is traceable
Label with our institution's accession, then consult accession number, then stain, etc.
we do all but the patient name
I would argue that a barcode is a better and more reliable tracking tool in consult materials
Again this may be ideal but current printing options will not allow full patient name in addition to other items.
Only repeat/recut slides from the original block should designated as repeat/recut in some manner determined by the laboratory.
Too much!
Patient name should be second, after accession number
Why not DOB instead of the patient’s name?
patient name should be optional
Not enough information to agree/disagree
If a consulting lab is going to make additional slides, I think that they should label the same way that they would label their own cases. By this I mean that they should use their own accession number and formats. Institution should definitely be mandatory here since there are now going to be slides made on a single case at two different labs. I don't think that "Surgical Pathology" is required or correct. 1. The lab making the slides may have a separate number wheel for consults. 2. The consult may be a cytology or autopsy case in which case "surgical pathology" is incorrect and misleading. Same caveats to patient name apply. I would prefer that local mrn be present as well as some portion of patient name (xx char last name and first initial).
I find this one very confusing. When additional slides are prepared from a consultation block, there is no “relabeling” of slides; they are simply labeled with the accession number assigned to that case and the unique designation for each slide. The discussion about not defacing original labels does not apply here. Also, what is meant by “Surgical Pathology” in 1a, and “Specimen” in 1b? Why wouldn’t you simply apply the same rules that were covered earlier?
Slides should also have the name of the consulting institution!
The institution name must be on the label.
I do not receive cases for consultation.
The accession number on the slides should be the number of the institution performing the consult. These slides would then be the property of that institution and retained by that institution.
A single accession number on the slide label eliminates ambiguity which could result in misfiling. If referring institution (A) sends block S13-100 B1 to the recipient institution (B), only the accession number of institution B (along with patient name and stain) should appear on the slide. The correlation of the slide prepared from the block to the referring institution's accession should be made only in the report text.