united states anny inspector general agency warrior care
TRANSCRIPT

United States Anny Inspector General Agency
Inspection of the Warrior Care and Transition Program
Table of Contents
COVER l-ETTER 1 EXECUTIVE SUMMARY 2 Summary of Observations and Recommendations
TAB AD POLICIES AND PROCEDURES
TAB B - SUPPORT SYSTEMS FOR SOLDIERS AND FAMILY MEMBERS
TAB C -MANAGEMENT OF MEDICAlLY NOT READY SOLDIERS
TAB D - OTHER MATTERS
TAB E co POSITIVE NOTES
TAB F - METHODOLOGY
APPENDIX 1 bull Directive
APPENDIX 2 - Stakeholder Briefing
APPENDIX 3 bull Acronym List
_)z-r- ___
bull FOR OFFIelAL USE 8NLY lNe lIoeument MaIne Iftfonnetloft which 18 Eltempt ampem Manltateiy DlIlOIGIMIIliI HllderDIe FFaedem ef farm 1st IIssemlllatl8 8p1i)hiltlled pI elfytelteed tIy JIlt
UlJited States Army Inspector General Agency
Inspection of the Warrior Care and Transition Program
Table of Contents
COVER LETTER 1 EXECUTIVE SUMMARY 2 Summary of Observations and Recommendations
TAB Amiddot POLICIES AND PRPCEDURES
Observation 11 No single synchronized source document outlining governing policies Amiddot1 guidance and regulatory requirements
Observation 12 Warrior Transition Unit (WTU) fosters a focused environment of Amiddot17 healing and transitioning however WT personal motivations may drive transition decisions
Observation 13 A mixture of combat wounded injured and ill Soldiers In the WTU Amiddot20 has created perceptions leading to leadership medical management public relations and small unit cohesin challenges
Observation 14 Challenges exist to Implement rapidly issuedchangIng policy without A-23 the-requisite resources
Observation 15 Subordinate commanders and some healthcare providers consider A-25 Fragmentary Order (FRAGO) 3 WTU entrance criteria to be vague and inconsistently
applied
Observation 16 Medical Commands (MEDCOM) accountability processes for A-27 Soldiers evacuated out of theater result in Immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
Observation 17 Most WTU cadre are concerned with inconsistencies in determining A-29 the Medical Retention Decision Point (MRDP)
Observation 18 Selection ofWTU cadre shifted from best qualified- to good and Amiddot31 first available
Observation 19 The current WTU classroom-centrlc and theory-based instruction A-33 does n equately prepare thscadre to perform their duties
~ _ ~ ~ _ ~ ~ ~ ~l ~
RJR OFFiew lfSE ONLY This documellt contains Infomnllton which hi Exempt from Mandatory Disclosure under the FliIItdom CIf IlIfcnmlillon Act Bi8IIamlnamp1ion Ie proIdbltiad Me wUlDFlzed bJAR 20 1
Observation 110 Most MUs visited are not meeting the intent and implementation A-35 of the Comprehensive Transition Plan (CTP)
Observation 111 Most Warrior Transition Units have not implemented the Transition 14-37 Review Board (TRB)
Observation 112 Army-wide specialty care shortages existin Behavioral Health 14-39 Occupational Therapy and Physical Therapy and contribute to delays in Soldiers treatment and healing
Observation 113 Army is failing to properly document Line of Duty (LOD) for A-41 Reserve Component (RC) Soldiers - critical to the follow-on care and transition for the RC Soldier
Observation 114 Perception that Warriors in Transition are not held to same A043 standards of dlscip6ne as required in other Army units
TAB B - SUPPORT SYSTEMS FOR SOLDIERS AND FAMILY MEMBERS
Observation 21 Soldier and Family Assistance Centers (SFAC) are underutilized B-45 however they provide WTs with a level of personal ~ce ahd an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
Observation 22 Providing services for Component (COMPO) 213 WTs and Families 8-47 is challenging due to the dispersion of state resources
Observation 23 Communities outside the gate are beginning to selectively support 8-48 onlV combat-wounded WTs with incentives resulting in non-standardized practices across installations
TAB C MANAGEMENT OF MEDICALLY NOT READY SOLDIERS
Observation 31 The Army does not use common terms of reference to accurately C-49 determine statUs of medically not readY -medically non-deployable and -not available Soldiers
Observation 32 Army medical fitness determination processes have not kept pace C-52 with Army Force Generation (ARFORGEN) requirements
bull FOR OfFIeIAL USE ONLY
11M doeumerd eontaiM infonnatJon which Is Eumpt lronl MCIIIdaIoIy Disclosure under the Freedom Df Informllltlon Act BI8 lnatl Is pnmIbIted except authorized by AR it-1
rrs T
Observation 33 Army medical capabilities do not support the needs of the C-S5 Medlcany Not Ready (MNR)Me9ically Non-Deployable(MND) in units
Observation 34 Current medical priorities do not assist commanders In maintaining e-57 a fit fighting force that Is medically ready to deploy
Observation 35 Leaders are concerned abOut Soldiers that Permanent Change e-g of Station (PCS) with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury (TBJand Post-Traumatic Stress Disorder(PTSDraquo
Observation 36 Soldiers in the Medical Evaluation Board (MEB)lPhysical Evaluation C-59 Board(PEB) process that are not assigned to a WTU are disadvantaged from a lack of information lower priority In access to care and length of Mea I PEB process
Observation 37 Individual Ready Reserve (IRR) Soldiers are often not identified CmiddotSU as non-deployable until they reach a mobilization pla~onn approximately 42 days or more after recalled to active duty
TAB 0 middotOTHER MATTERS
Other Matter 1 Leaders health care professionals and Soldiers stated that MEBIPEB 0middot1 inefficiencies affect the Armys ability to mee~ the needs of Soldiers and the Army in a timely manner
other Matter 2 Umited andor no interoperability between DoD Armed Forces Health 0middot3 Longitudinal TeChnology Application (AHL TA) Department of Veterans Affairs (VA) Veterans Health Information Systems and Technology Architecture (VISTA) TRICARE network and civilian provider information systems
Other Matter 3 COMPO 213 are not longer a strategic reserve current Army resources D-4 appear to be insufficient to medically sustain RC in an operational environment
Other Matter 4 The majority of medical management staff have some level of concern 0middot6 for personal safety in managing increasing numbers of Soldiers with behavioral health issues
Other MaHer 5 Most healthcare providers interviewed(Primary care Managers (PCM) Dmiddot7 Nurse case Managers (NCM) estimate 25-3S of WTs are dependent on or addicted to dlllgs
rr r 7FII bull bull mrs r T
reR erFlCIAL WE ONLyen Tld8 cIoeliliNid eontahas lilfOiliiatlonwtllcfi Is _lip 11 Mandatot) DlscIusu IIlide III Feedom of blfonatfOiI Act Dissemination i9 prohibited -=tld Q8 autbolf2ed by AR 28-1
TAB E POSITIVE NOTES
Positive Note 1 Some units Implemented pain and prescription management Emiddot1 programs to assist in the reduction of medication dependency
Positive Note 2 Fort Braggs Focused Transition Review (FTR) is a multidiscip6nary Emiddot1 platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Eisenhower Army Medical Centers In-patient substance addictionE-1 program provides for more effective Command and Control (e2) and Medical Management (M2) of Soldiers with addiction diagnoses
Positive Note 4 4th Infantry Division (IO) Building The Soldier Athlete fitness Emiddot1 program motivates Medically NonmiddotDeployable (MND) Soldiers focuses on abilities instead of disabilities
Positive Note 5 Evans Army Community Hospital Fort Carson established robust E 1 Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
TAB F METHODOLOGY
APPENDIX 1- Directive
APPENDIXmiddot2 bull Stakeholder Briefing
APPENDIX 3 bull Acronym List
71- ~ - - 7 Q bullbull mE FOR ornetAL USE ONLY
This do_em eeftt8IM fnIonnallon Which Exempt from Malldatol DfscIosule IJlld8i ttl Fteedum of Infoi Illation Id mluatloii Ie prohlbrted except aalhOitzed by Aft 2001
SA I G-ZA
DEPARTMENT OF THE ARMY OFFICE OF THE INSPECTOR GENERAL
1700 A1fIIV PENTAGON WASHINGTON DC 2031G-t700
MEMORANDUM FOR SECRETARY OF THE ARMY
SEP 22 2010
SUBJECT Results of the Warrior Care and Transition Program Inspection
1 The US Army Inspector General Agency conducted an Inspection of the Warrior Care and Transition Program from 27 January 2010 to 30 June 2010 Three objectives were assessed (further discussed in paragraph 3)
2 Background In February 2007 the Army established the Army Medical Action Plan (AMAP) now known as the Warrior Care and Transition Program to effectively manage Soldiers receiving outpatient care A~ its heart the Warrior Transition Unit (WTU) Is an organizational and cultural shift In how the Army cares for its wounded ill and injured Soldiers
a There are currently 29 WTUs on Army installations and ninecpmmunity-based warrior transition units (CBWTU) These units are designed to provide support to Soldiers who are expected to require at least six months of rehabilitative care and the need for middotcomplex medical case management for active component (COMPO) or -definitive heaHhcare for reserve component Soldiers The units have dedicated phYSicians nurses behavioral health professionals and military leaders These leaders and healthcare professionals are charged with ensuring Soldiers needs are met their care is coordinated and their Families concerns are addressed
b Since June 2007 the WTU returned 12956 Soldiers to duty with an average stay of seven months During that same period 13504 $Oldiers transitloned from the Army with an average WTU stay of over 14 months as cited in a report by Plans Analysis and Evaluations (PAampE) Office of The Surgeon General (OTSG) on Warrior Transition Status dated 14 June 2010 The current combined WTU and CBwru population Is approximately 9500
c There is a misperception that all or most Warriors in Transition(WT) were wounded In combat OTSG Status Report statistics show only 10 were wounded In combat 37 were evacuated from a combat zone due to disease and non-battle injuries and 53 had illnesses or injuries not associated with combat (COMPO 1 Soldiers command-referred and COMPO 2 and 3 Soldiers in mobilization and de-mobilization)
FOR OFFICIAl USE ONLY Oisseminmn is prohibited expect 8S authorized by AA 20 1
This Document contains information EXEMPT FROM MMlDATORV DISCLOSURE under FOIA Eemptioo 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
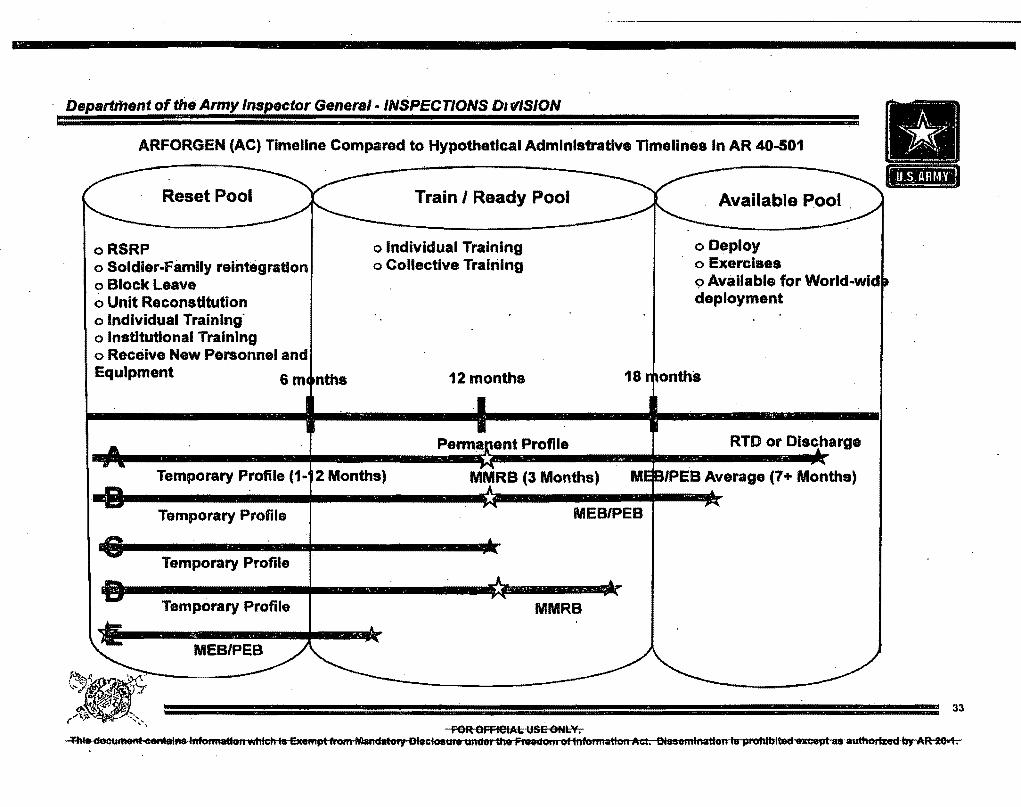
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
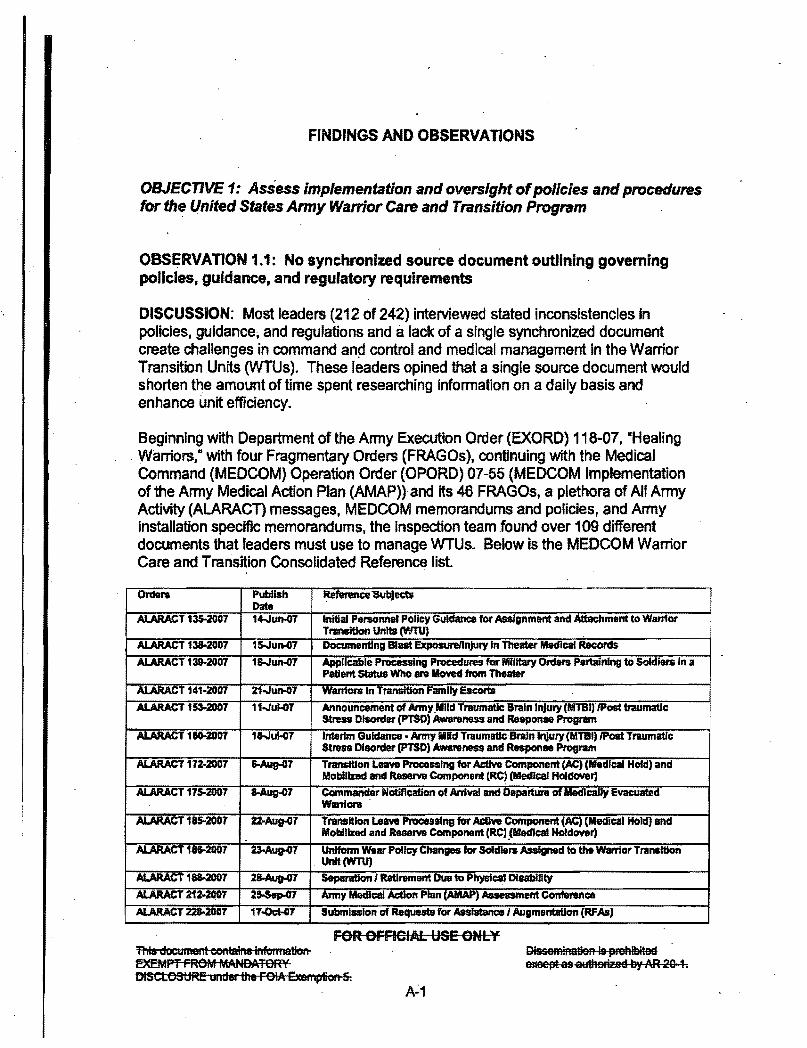
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
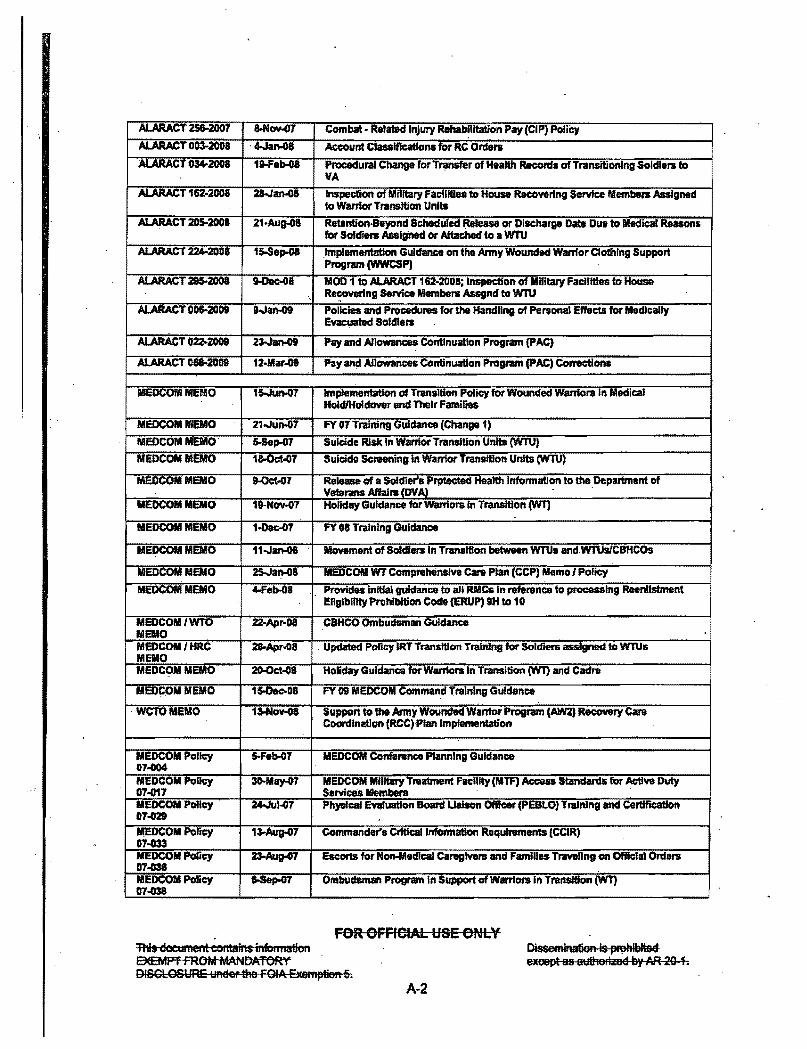
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
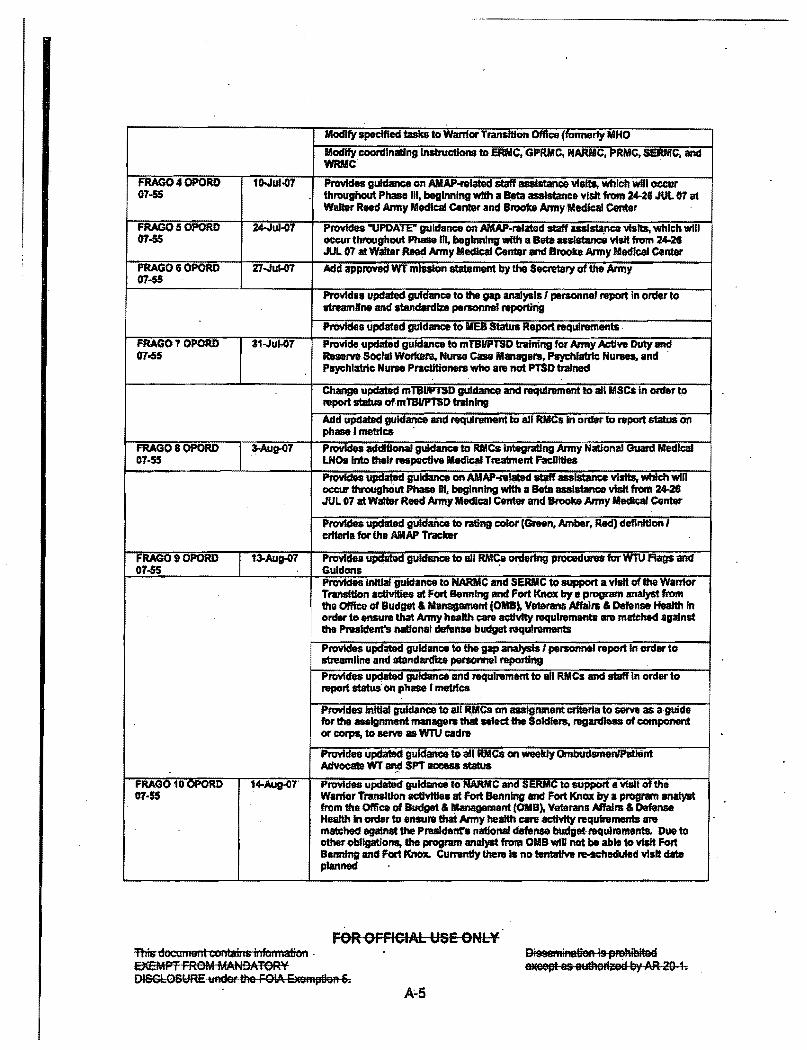
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
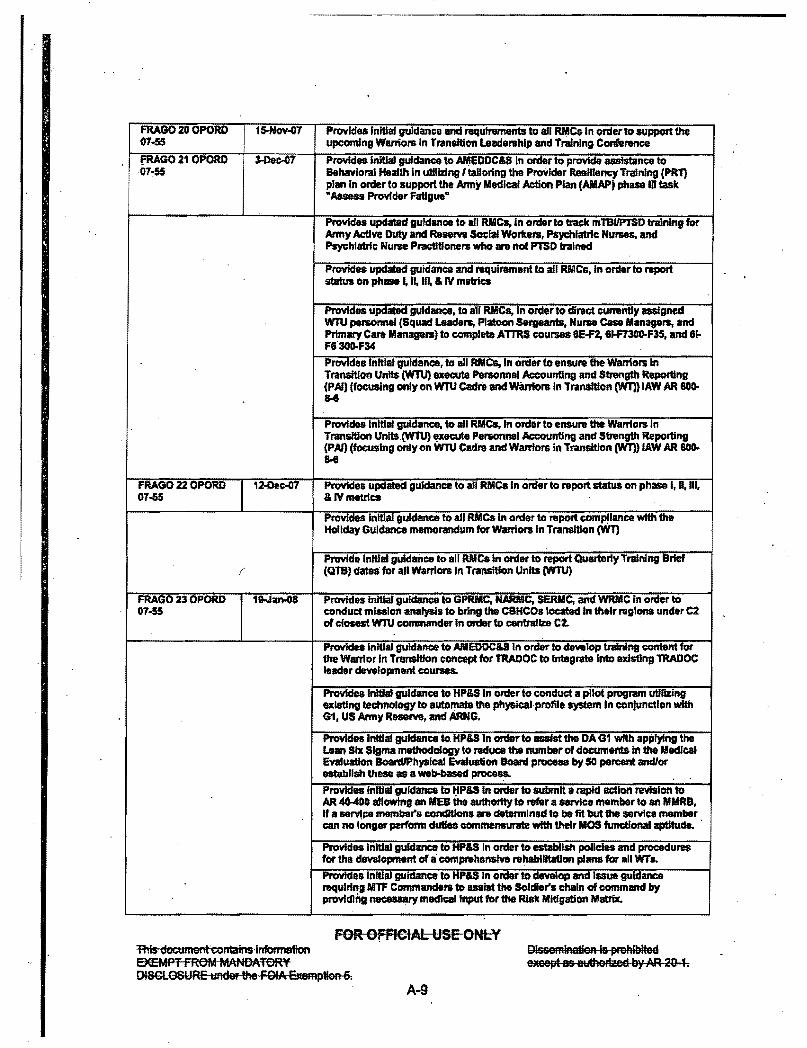
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
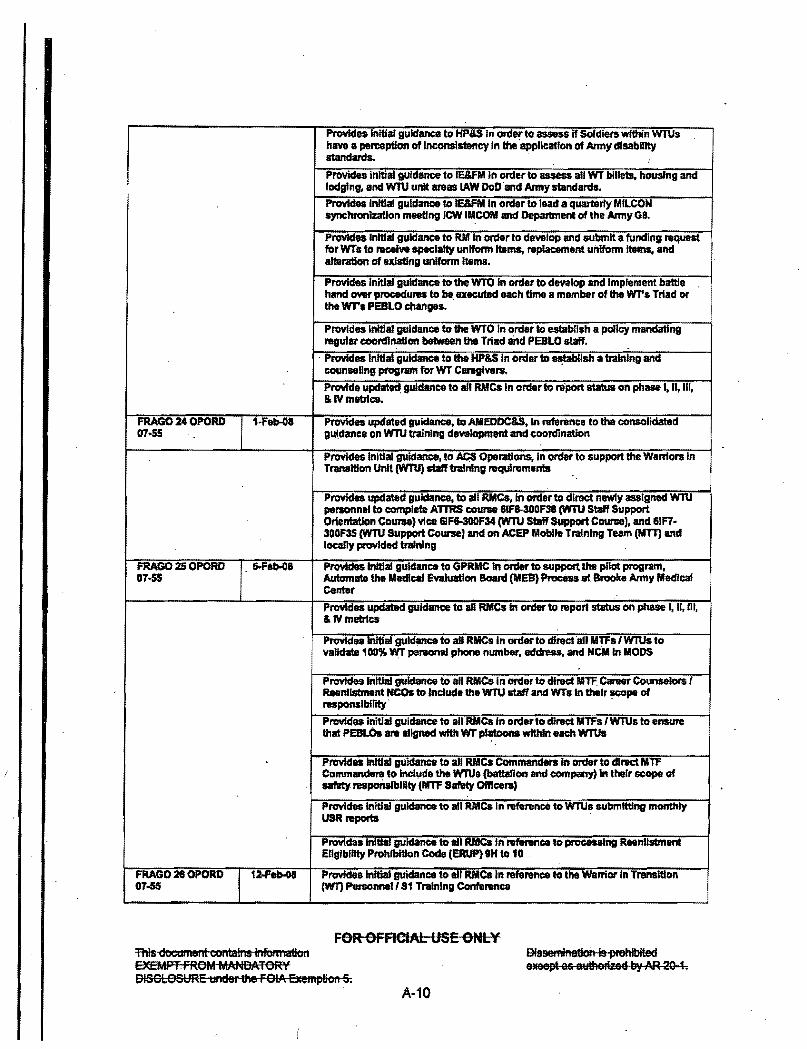
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
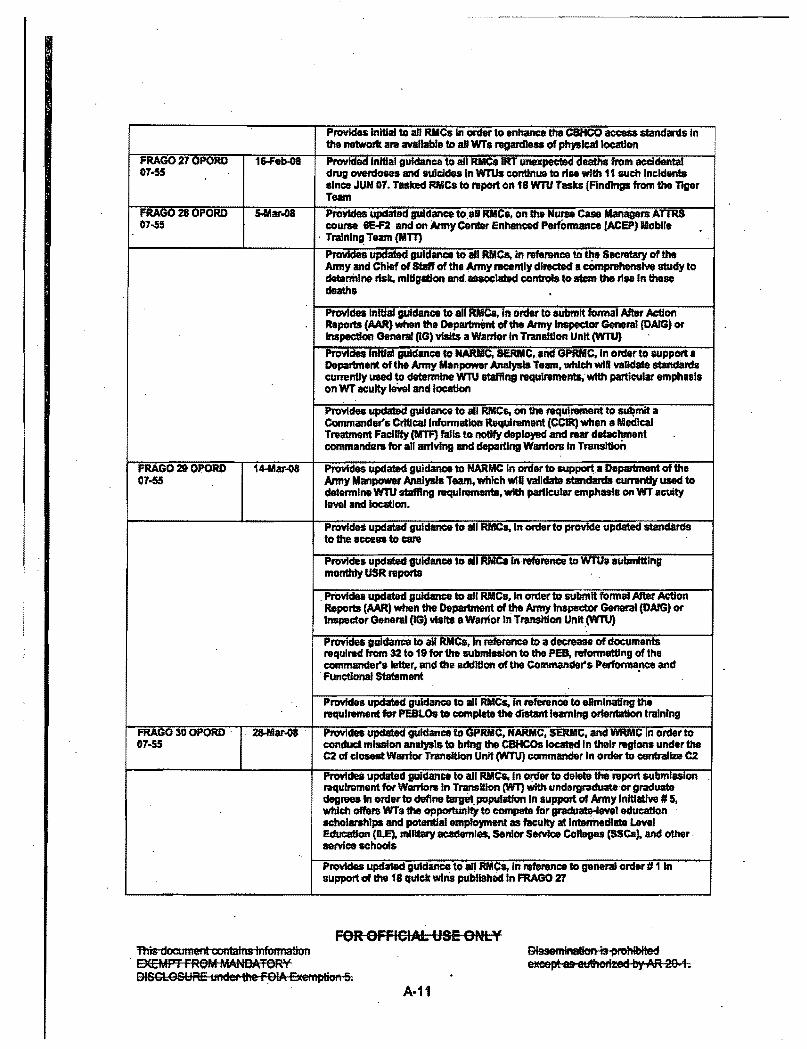
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
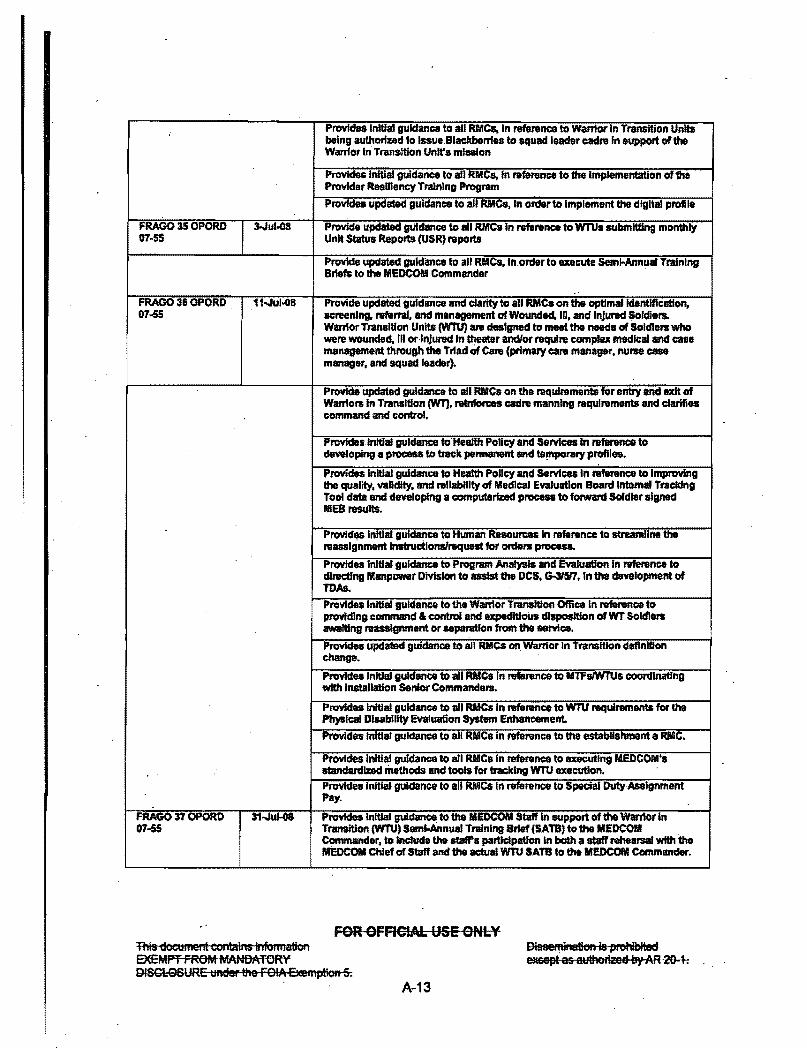
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6

UlJited States Army Inspector General Agency
Inspection of the Warrior Care and Transition Program
Table of Contents
COVER LETTER 1 EXECUTIVE SUMMARY 2 Summary of Observations and Recommendations
TAB Amiddot POLICIES AND PRPCEDURES
Observation 11 No single synchronized source document outlining governing policies Amiddot1 guidance and regulatory requirements
Observation 12 Warrior Transition Unit (WTU) fosters a focused environment of Amiddot17 healing and transitioning however WT personal motivations may drive transition decisions
Observation 13 A mixture of combat wounded injured and ill Soldiers In the WTU Amiddot20 has created perceptions leading to leadership medical management public relations and small unit cohesin challenges
Observation 14 Challenges exist to Implement rapidly issuedchangIng policy without A-23 the-requisite resources
Observation 15 Subordinate commanders and some healthcare providers consider A-25 Fragmentary Order (FRAGO) 3 WTU entrance criteria to be vague and inconsistently
applied
Observation 16 Medical Commands (MEDCOM) accountability processes for A-27 Soldiers evacuated out of theater result in Immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
Observation 17 Most WTU cadre are concerned with inconsistencies in determining A-29 the Medical Retention Decision Point (MRDP)
Observation 18 Selection ofWTU cadre shifted from best qualified- to good and Amiddot31 first available
Observation 19 The current WTU classroom-centrlc and theory-based instruction A-33 does n equately prepare thscadre to perform their duties
~ _ ~ ~ _ ~ ~ ~ ~l ~
RJR OFFiew lfSE ONLY This documellt contains Infomnllton which hi Exempt from Mandatory Disclosure under the FliIItdom CIf IlIfcnmlillon Act Bi8IIamlnamp1ion Ie proIdbltiad Me wUlDFlzed bJAR 20 1
Observation 110 Most MUs visited are not meeting the intent and implementation A-35 of the Comprehensive Transition Plan (CTP)
Observation 111 Most Warrior Transition Units have not implemented the Transition 14-37 Review Board (TRB)
Observation 112 Army-wide specialty care shortages existin Behavioral Health 14-39 Occupational Therapy and Physical Therapy and contribute to delays in Soldiers treatment and healing
Observation 113 Army is failing to properly document Line of Duty (LOD) for A-41 Reserve Component (RC) Soldiers - critical to the follow-on care and transition for the RC Soldier
Observation 114 Perception that Warriors in Transition are not held to same A043 standards of dlscip6ne as required in other Army units
TAB B - SUPPORT SYSTEMS FOR SOLDIERS AND FAMILY MEMBERS
Observation 21 Soldier and Family Assistance Centers (SFAC) are underutilized B-45 however they provide WTs with a level of personal ~ce ahd an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
Observation 22 Providing services for Component (COMPO) 213 WTs and Families 8-47 is challenging due to the dispersion of state resources
Observation 23 Communities outside the gate are beginning to selectively support 8-48 onlV combat-wounded WTs with incentives resulting in non-standardized practices across installations
TAB C MANAGEMENT OF MEDICALLY NOT READY SOLDIERS
Observation 31 The Army does not use common terms of reference to accurately C-49 determine statUs of medically not readY -medically non-deployable and -not available Soldiers
Observation 32 Army medical fitness determination processes have not kept pace C-52 with Army Force Generation (ARFORGEN) requirements
bull FOR OfFIeIAL USE ONLY
11M doeumerd eontaiM infonnatJon which Is Eumpt lronl MCIIIdaIoIy Disclosure under the Freedom Df Informllltlon Act BI8 lnatl Is pnmIbIted except authorized by AR it-1
rrs T
Observation 33 Army medical capabilities do not support the needs of the C-S5 Medlcany Not Ready (MNR)Me9ically Non-Deployable(MND) in units
Observation 34 Current medical priorities do not assist commanders In maintaining e-57 a fit fighting force that Is medically ready to deploy
Observation 35 Leaders are concerned abOut Soldiers that Permanent Change e-g of Station (PCS) with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury (TBJand Post-Traumatic Stress Disorder(PTSDraquo
Observation 36 Soldiers in the Medical Evaluation Board (MEB)lPhysical Evaluation C-59 Board(PEB) process that are not assigned to a WTU are disadvantaged from a lack of information lower priority In access to care and length of Mea I PEB process
Observation 37 Individual Ready Reserve (IRR) Soldiers are often not identified CmiddotSU as non-deployable until they reach a mobilization pla~onn approximately 42 days or more after recalled to active duty
TAB 0 middotOTHER MATTERS
Other Matter 1 Leaders health care professionals and Soldiers stated that MEBIPEB 0middot1 inefficiencies affect the Armys ability to mee~ the needs of Soldiers and the Army in a timely manner
other Matter 2 Umited andor no interoperability between DoD Armed Forces Health 0middot3 Longitudinal TeChnology Application (AHL TA) Department of Veterans Affairs (VA) Veterans Health Information Systems and Technology Architecture (VISTA) TRICARE network and civilian provider information systems
Other Matter 3 COMPO 213 are not longer a strategic reserve current Army resources D-4 appear to be insufficient to medically sustain RC in an operational environment
Other Matter 4 The majority of medical management staff have some level of concern 0middot6 for personal safety in managing increasing numbers of Soldiers with behavioral health issues
Other MaHer 5 Most healthcare providers interviewed(Primary care Managers (PCM) Dmiddot7 Nurse case Managers (NCM) estimate 25-3S of WTs are dependent on or addicted to dlllgs
rr r 7FII bull bull mrs r T
reR erFlCIAL WE ONLyen Tld8 cIoeliliNid eontahas lilfOiliiatlonwtllcfi Is _lip 11 Mandatot) DlscIusu IIlide III Feedom of blfonatfOiI Act Dissemination i9 prohibited -=tld Q8 autbolf2ed by AR 28-1
TAB E POSITIVE NOTES
Positive Note 1 Some units Implemented pain and prescription management Emiddot1 programs to assist in the reduction of medication dependency
Positive Note 2 Fort Braggs Focused Transition Review (FTR) is a multidiscip6nary Emiddot1 platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Eisenhower Army Medical Centers In-patient substance addictionE-1 program provides for more effective Command and Control (e2) and Medical Management (M2) of Soldiers with addiction diagnoses
Positive Note 4 4th Infantry Division (IO) Building The Soldier Athlete fitness Emiddot1 program motivates Medically NonmiddotDeployable (MND) Soldiers focuses on abilities instead of disabilities
Positive Note 5 Evans Army Community Hospital Fort Carson established robust E 1 Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
TAB F METHODOLOGY
APPENDIX 1- Directive
APPENDIXmiddot2 bull Stakeholder Briefing
APPENDIX 3 bull Acronym List
71- ~ - - 7 Q bullbull mE FOR ornetAL USE ONLY
This do_em eeftt8IM fnIonnallon Which Exempt from Malldatol DfscIosule IJlld8i ttl Fteedum of Infoi Illation Id mluatloii Ie prohlbrted except aalhOitzed by Aft 2001
SA I G-ZA
DEPARTMENT OF THE ARMY OFFICE OF THE INSPECTOR GENERAL
1700 A1fIIV PENTAGON WASHINGTON DC 2031G-t700
MEMORANDUM FOR SECRETARY OF THE ARMY
SEP 22 2010
SUBJECT Results of the Warrior Care and Transition Program Inspection
1 The US Army Inspector General Agency conducted an Inspection of the Warrior Care and Transition Program from 27 January 2010 to 30 June 2010 Three objectives were assessed (further discussed in paragraph 3)
2 Background In February 2007 the Army established the Army Medical Action Plan (AMAP) now known as the Warrior Care and Transition Program to effectively manage Soldiers receiving outpatient care A~ its heart the Warrior Transition Unit (WTU) Is an organizational and cultural shift In how the Army cares for its wounded ill and injured Soldiers
a There are currently 29 WTUs on Army installations and ninecpmmunity-based warrior transition units (CBWTU) These units are designed to provide support to Soldiers who are expected to require at least six months of rehabilitative care and the need for middotcomplex medical case management for active component (COMPO) or -definitive heaHhcare for reserve component Soldiers The units have dedicated phYSicians nurses behavioral health professionals and military leaders These leaders and healthcare professionals are charged with ensuring Soldiers needs are met their care is coordinated and their Families concerns are addressed
b Since June 2007 the WTU returned 12956 Soldiers to duty with an average stay of seven months During that same period 13504 $Oldiers transitloned from the Army with an average WTU stay of over 14 months as cited in a report by Plans Analysis and Evaluations (PAampE) Office of The Surgeon General (OTSG) on Warrior Transition Status dated 14 June 2010 The current combined WTU and CBwru population Is approximately 9500
c There is a misperception that all or most Warriors in Transition(WT) were wounded In combat OTSG Status Report statistics show only 10 were wounded In combat 37 were evacuated from a combat zone due to disease and non-battle injuries and 53 had illnesses or injuries not associated with combat (COMPO 1 Soldiers command-referred and COMPO 2 and 3 Soldiers in mobilization and de-mobilization)
FOR OFFICIAl USE ONLY Oisseminmn is prohibited expect 8S authorized by AA 20 1
This Document contains information EXEMPT FROM MMlDATORV DISCLOSURE under FOIA Eemptioo 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6

Observation 110 Most MUs visited are not meeting the intent and implementation A-35 of the Comprehensive Transition Plan (CTP)
Observation 111 Most Warrior Transition Units have not implemented the Transition 14-37 Review Board (TRB)
Observation 112 Army-wide specialty care shortages existin Behavioral Health 14-39 Occupational Therapy and Physical Therapy and contribute to delays in Soldiers treatment and healing
Observation 113 Army is failing to properly document Line of Duty (LOD) for A-41 Reserve Component (RC) Soldiers - critical to the follow-on care and transition for the RC Soldier
Observation 114 Perception that Warriors in Transition are not held to same A043 standards of dlscip6ne as required in other Army units
TAB B - SUPPORT SYSTEMS FOR SOLDIERS AND FAMILY MEMBERS
Observation 21 Soldier and Family Assistance Centers (SFAC) are underutilized B-45 however they provide WTs with a level of personal ~ce ahd an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
Observation 22 Providing services for Component (COMPO) 213 WTs and Families 8-47 is challenging due to the dispersion of state resources
Observation 23 Communities outside the gate are beginning to selectively support 8-48 onlV combat-wounded WTs with incentives resulting in non-standardized practices across installations
TAB C MANAGEMENT OF MEDICALLY NOT READY SOLDIERS
Observation 31 The Army does not use common terms of reference to accurately C-49 determine statUs of medically not readY -medically non-deployable and -not available Soldiers
Observation 32 Army medical fitness determination processes have not kept pace C-52 with Army Force Generation (ARFORGEN) requirements
bull FOR OfFIeIAL USE ONLY
11M doeumerd eontaiM infonnatJon which Is Eumpt lronl MCIIIdaIoIy Disclosure under the Freedom Df Informllltlon Act BI8 lnatl Is pnmIbIted except authorized by AR it-1
rrs T
Observation 33 Army medical capabilities do not support the needs of the C-S5 Medlcany Not Ready (MNR)Me9ically Non-Deployable(MND) in units
Observation 34 Current medical priorities do not assist commanders In maintaining e-57 a fit fighting force that Is medically ready to deploy
Observation 35 Leaders are concerned abOut Soldiers that Permanent Change e-g of Station (PCS) with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury (TBJand Post-Traumatic Stress Disorder(PTSDraquo
Observation 36 Soldiers in the Medical Evaluation Board (MEB)lPhysical Evaluation C-59 Board(PEB) process that are not assigned to a WTU are disadvantaged from a lack of information lower priority In access to care and length of Mea I PEB process
Observation 37 Individual Ready Reserve (IRR) Soldiers are often not identified CmiddotSU as non-deployable until they reach a mobilization pla~onn approximately 42 days or more after recalled to active duty
TAB 0 middotOTHER MATTERS
Other Matter 1 Leaders health care professionals and Soldiers stated that MEBIPEB 0middot1 inefficiencies affect the Armys ability to mee~ the needs of Soldiers and the Army in a timely manner
other Matter 2 Umited andor no interoperability between DoD Armed Forces Health 0middot3 Longitudinal TeChnology Application (AHL TA) Department of Veterans Affairs (VA) Veterans Health Information Systems and Technology Architecture (VISTA) TRICARE network and civilian provider information systems
Other Matter 3 COMPO 213 are not longer a strategic reserve current Army resources D-4 appear to be insufficient to medically sustain RC in an operational environment
Other Matter 4 The majority of medical management staff have some level of concern 0middot6 for personal safety in managing increasing numbers of Soldiers with behavioral health issues
Other MaHer 5 Most healthcare providers interviewed(Primary care Managers (PCM) Dmiddot7 Nurse case Managers (NCM) estimate 25-3S of WTs are dependent on or addicted to dlllgs
rr r 7FII bull bull mrs r T
reR erFlCIAL WE ONLyen Tld8 cIoeliliNid eontahas lilfOiliiatlonwtllcfi Is _lip 11 Mandatot) DlscIusu IIlide III Feedom of blfonatfOiI Act Dissemination i9 prohibited -=tld Q8 autbolf2ed by AR 28-1
TAB E POSITIVE NOTES
Positive Note 1 Some units Implemented pain and prescription management Emiddot1 programs to assist in the reduction of medication dependency
Positive Note 2 Fort Braggs Focused Transition Review (FTR) is a multidiscip6nary Emiddot1 platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Eisenhower Army Medical Centers In-patient substance addictionE-1 program provides for more effective Command and Control (e2) and Medical Management (M2) of Soldiers with addiction diagnoses
Positive Note 4 4th Infantry Division (IO) Building The Soldier Athlete fitness Emiddot1 program motivates Medically NonmiddotDeployable (MND) Soldiers focuses on abilities instead of disabilities
Positive Note 5 Evans Army Community Hospital Fort Carson established robust E 1 Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
TAB F METHODOLOGY
APPENDIX 1- Directive
APPENDIXmiddot2 bull Stakeholder Briefing
APPENDIX 3 bull Acronym List
71- ~ - - 7 Q bullbull mE FOR ornetAL USE ONLY
This do_em eeftt8IM fnIonnallon Which Exempt from Malldatol DfscIosule IJlld8i ttl Fteedum of Infoi Illation Id mluatloii Ie prohlbrted except aalhOitzed by Aft 2001
SA I G-ZA
DEPARTMENT OF THE ARMY OFFICE OF THE INSPECTOR GENERAL
1700 A1fIIV PENTAGON WASHINGTON DC 2031G-t700
MEMORANDUM FOR SECRETARY OF THE ARMY
SEP 22 2010
SUBJECT Results of the Warrior Care and Transition Program Inspection
1 The US Army Inspector General Agency conducted an Inspection of the Warrior Care and Transition Program from 27 January 2010 to 30 June 2010 Three objectives were assessed (further discussed in paragraph 3)
2 Background In February 2007 the Army established the Army Medical Action Plan (AMAP) now known as the Warrior Care and Transition Program to effectively manage Soldiers receiving outpatient care A~ its heart the Warrior Transition Unit (WTU) Is an organizational and cultural shift In how the Army cares for its wounded ill and injured Soldiers
a There are currently 29 WTUs on Army installations and ninecpmmunity-based warrior transition units (CBWTU) These units are designed to provide support to Soldiers who are expected to require at least six months of rehabilitative care and the need for middotcomplex medical case management for active component (COMPO) or -definitive heaHhcare for reserve component Soldiers The units have dedicated phYSicians nurses behavioral health professionals and military leaders These leaders and healthcare professionals are charged with ensuring Soldiers needs are met their care is coordinated and their Families concerns are addressed
b Since June 2007 the WTU returned 12956 Soldiers to duty with an average stay of seven months During that same period 13504 $Oldiers transitloned from the Army with an average WTU stay of over 14 months as cited in a report by Plans Analysis and Evaluations (PAampE) Office of The Surgeon General (OTSG) on Warrior Transition Status dated 14 June 2010 The current combined WTU and CBwru population Is approximately 9500
c There is a misperception that all or most Warriors in Transition(WT) were wounded In combat OTSG Status Report statistics show only 10 were wounded In combat 37 were evacuated from a combat zone due to disease and non-battle injuries and 53 had illnesses or injuries not associated with combat (COMPO 1 Soldiers command-referred and COMPO 2 and 3 Soldiers in mobilization and de-mobilization)
FOR OFFICIAl USE ONLY Oisseminmn is prohibited expect 8S authorized by AA 20 1
This Document contains information EXEMPT FROM MMlDATORV DISCLOSURE under FOIA Eemptioo 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6

rrs T
Observation 33 Army medical capabilities do not support the needs of the C-S5 Medlcany Not Ready (MNR)Me9ically Non-Deployable(MND) in units
Observation 34 Current medical priorities do not assist commanders In maintaining e-57 a fit fighting force that Is medically ready to deploy
Observation 35 Leaders are concerned abOut Soldiers that Permanent Change e-g of Station (PCS) with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury (TBJand Post-Traumatic Stress Disorder(PTSDraquo
Observation 36 Soldiers in the Medical Evaluation Board (MEB)lPhysical Evaluation C-59 Board(PEB) process that are not assigned to a WTU are disadvantaged from a lack of information lower priority In access to care and length of Mea I PEB process
Observation 37 Individual Ready Reserve (IRR) Soldiers are often not identified CmiddotSU as non-deployable until they reach a mobilization pla~onn approximately 42 days or more after recalled to active duty
TAB 0 middotOTHER MATTERS
Other Matter 1 Leaders health care professionals and Soldiers stated that MEBIPEB 0middot1 inefficiencies affect the Armys ability to mee~ the needs of Soldiers and the Army in a timely manner
other Matter 2 Umited andor no interoperability between DoD Armed Forces Health 0middot3 Longitudinal TeChnology Application (AHL TA) Department of Veterans Affairs (VA) Veterans Health Information Systems and Technology Architecture (VISTA) TRICARE network and civilian provider information systems
Other Matter 3 COMPO 213 are not longer a strategic reserve current Army resources D-4 appear to be insufficient to medically sustain RC in an operational environment
Other Matter 4 The majority of medical management staff have some level of concern 0middot6 for personal safety in managing increasing numbers of Soldiers with behavioral health issues
Other MaHer 5 Most healthcare providers interviewed(Primary care Managers (PCM) Dmiddot7 Nurse case Managers (NCM) estimate 25-3S of WTs are dependent on or addicted to dlllgs
rr r 7FII bull bull mrs r T
reR erFlCIAL WE ONLyen Tld8 cIoeliliNid eontahas lilfOiliiatlonwtllcfi Is _lip 11 Mandatot) DlscIusu IIlide III Feedom of blfonatfOiI Act Dissemination i9 prohibited -=tld Q8 autbolf2ed by AR 28-1
TAB E POSITIVE NOTES
Positive Note 1 Some units Implemented pain and prescription management Emiddot1 programs to assist in the reduction of medication dependency
Positive Note 2 Fort Braggs Focused Transition Review (FTR) is a multidiscip6nary Emiddot1 platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Eisenhower Army Medical Centers In-patient substance addictionE-1 program provides for more effective Command and Control (e2) and Medical Management (M2) of Soldiers with addiction diagnoses
Positive Note 4 4th Infantry Division (IO) Building The Soldier Athlete fitness Emiddot1 program motivates Medically NonmiddotDeployable (MND) Soldiers focuses on abilities instead of disabilities
Positive Note 5 Evans Army Community Hospital Fort Carson established robust E 1 Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
TAB F METHODOLOGY
APPENDIX 1- Directive
APPENDIXmiddot2 bull Stakeholder Briefing
APPENDIX 3 bull Acronym List
71- ~ - - 7 Q bullbull mE FOR ornetAL USE ONLY
This do_em eeftt8IM fnIonnallon Which Exempt from Malldatol DfscIosule IJlld8i ttl Fteedum of Infoi Illation Id mluatloii Ie prohlbrted except aalhOitzed by Aft 2001
SA I G-ZA
DEPARTMENT OF THE ARMY OFFICE OF THE INSPECTOR GENERAL
1700 A1fIIV PENTAGON WASHINGTON DC 2031G-t700
MEMORANDUM FOR SECRETARY OF THE ARMY
SEP 22 2010
SUBJECT Results of the Warrior Care and Transition Program Inspection
1 The US Army Inspector General Agency conducted an Inspection of the Warrior Care and Transition Program from 27 January 2010 to 30 June 2010 Three objectives were assessed (further discussed in paragraph 3)
2 Background In February 2007 the Army established the Army Medical Action Plan (AMAP) now known as the Warrior Care and Transition Program to effectively manage Soldiers receiving outpatient care A~ its heart the Warrior Transition Unit (WTU) Is an organizational and cultural shift In how the Army cares for its wounded ill and injured Soldiers
a There are currently 29 WTUs on Army installations and ninecpmmunity-based warrior transition units (CBWTU) These units are designed to provide support to Soldiers who are expected to require at least six months of rehabilitative care and the need for middotcomplex medical case management for active component (COMPO) or -definitive heaHhcare for reserve component Soldiers The units have dedicated phYSicians nurses behavioral health professionals and military leaders These leaders and healthcare professionals are charged with ensuring Soldiers needs are met their care is coordinated and their Families concerns are addressed
b Since June 2007 the WTU returned 12956 Soldiers to duty with an average stay of seven months During that same period 13504 $Oldiers transitloned from the Army with an average WTU stay of over 14 months as cited in a report by Plans Analysis and Evaluations (PAampE) Office of The Surgeon General (OTSG) on Warrior Transition Status dated 14 June 2010 The current combined WTU and CBwru population Is approximately 9500
c There is a misperception that all or most Warriors in Transition(WT) were wounded In combat OTSG Status Report statistics show only 10 were wounded In combat 37 were evacuated from a combat zone due to disease and non-battle injuries and 53 had illnesses or injuries not associated with combat (COMPO 1 Soldiers command-referred and COMPO 2 and 3 Soldiers in mobilization and de-mobilization)
FOR OFFICIAl USE ONLY Oisseminmn is prohibited expect 8S authorized by AA 20 1
This Document contains information EXEMPT FROM MMlDATORV DISCLOSURE under FOIA Eemptioo 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6
TAB E POSITIVE NOTES
Positive Note 1 Some units Implemented pain and prescription management Emiddot1 programs to assist in the reduction of medication dependency
Positive Note 2 Fort Braggs Focused Transition Review (FTR) is a multidiscip6nary Emiddot1 platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Eisenhower Army Medical Centers In-patient substance addictionE-1 program provides for more effective Command and Control (e2) and Medical Management (M2) of Soldiers with addiction diagnoses
Positive Note 4 4th Infantry Division (IO) Building The Soldier Athlete fitness Emiddot1 program motivates Medically NonmiddotDeployable (MND) Soldiers focuses on abilities instead of disabilities
Positive Note 5 Evans Army Community Hospital Fort Carson established robust E 1 Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
TAB F METHODOLOGY
APPENDIX 1- Directive
APPENDIXmiddot2 bull Stakeholder Briefing
APPENDIX 3 bull Acronym List
71- ~ - - 7 Q bullbull mE FOR ornetAL USE ONLY
This do_em eeftt8IM fnIonnallon Which Exempt from Malldatol DfscIosule IJlld8i ttl Fteedum of Infoi Illation Id mluatloii Ie prohlbrted except aalhOitzed by Aft 2001
SA I G-ZA
DEPARTMENT OF THE ARMY OFFICE OF THE INSPECTOR GENERAL
1700 A1fIIV PENTAGON WASHINGTON DC 2031G-t700
MEMORANDUM FOR SECRETARY OF THE ARMY
SEP 22 2010
SUBJECT Results of the Warrior Care and Transition Program Inspection
1 The US Army Inspector General Agency conducted an Inspection of the Warrior Care and Transition Program from 27 January 2010 to 30 June 2010 Three objectives were assessed (further discussed in paragraph 3)
2 Background In February 2007 the Army established the Army Medical Action Plan (AMAP) now known as the Warrior Care and Transition Program to effectively manage Soldiers receiving outpatient care A~ its heart the Warrior Transition Unit (WTU) Is an organizational and cultural shift In how the Army cares for its wounded ill and injured Soldiers
a There are currently 29 WTUs on Army installations and ninecpmmunity-based warrior transition units (CBWTU) These units are designed to provide support to Soldiers who are expected to require at least six months of rehabilitative care and the need for middotcomplex medical case management for active component (COMPO) or -definitive heaHhcare for reserve component Soldiers The units have dedicated phYSicians nurses behavioral health professionals and military leaders These leaders and healthcare professionals are charged with ensuring Soldiers needs are met their care is coordinated and their Families concerns are addressed
b Since June 2007 the WTU returned 12956 Soldiers to duty with an average stay of seven months During that same period 13504 $Oldiers transitloned from the Army with an average WTU stay of over 14 months as cited in a report by Plans Analysis and Evaluations (PAampE) Office of The Surgeon General (OTSG) on Warrior Transition Status dated 14 June 2010 The current combined WTU and CBwru population Is approximately 9500
c There is a misperception that all or most Warriors in Transition(WT) were wounded In combat OTSG Status Report statistics show only 10 were wounded In combat 37 were evacuated from a combat zone due to disease and non-battle injuries and 53 had illnesses or injuries not associated with combat (COMPO 1 Soldiers command-referred and COMPO 2 and 3 Soldiers in mobilization and de-mobilization)
FOR OFFICIAl USE ONLY Oisseminmn is prohibited expect 8S authorized by AA 20 1
This Document contains information EXEMPT FROM MMlDATORV DISCLOSURE under FOIA Eemptioo 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6

SA I G-ZA
DEPARTMENT OF THE ARMY OFFICE OF THE INSPECTOR GENERAL
1700 A1fIIV PENTAGON WASHINGTON DC 2031G-t700
MEMORANDUM FOR SECRETARY OF THE ARMY
SEP 22 2010
SUBJECT Results of the Warrior Care and Transition Program Inspection
1 The US Army Inspector General Agency conducted an Inspection of the Warrior Care and Transition Program from 27 January 2010 to 30 June 2010 Three objectives were assessed (further discussed in paragraph 3)
2 Background In February 2007 the Army established the Army Medical Action Plan (AMAP) now known as the Warrior Care and Transition Program to effectively manage Soldiers receiving outpatient care A~ its heart the Warrior Transition Unit (WTU) Is an organizational and cultural shift In how the Army cares for its wounded ill and injured Soldiers
a There are currently 29 WTUs on Army installations and ninecpmmunity-based warrior transition units (CBWTU) These units are designed to provide support to Soldiers who are expected to require at least six months of rehabilitative care and the need for middotcomplex medical case management for active component (COMPO) or -definitive heaHhcare for reserve component Soldiers The units have dedicated phYSicians nurses behavioral health professionals and military leaders These leaders and healthcare professionals are charged with ensuring Soldiers needs are met their care is coordinated and their Families concerns are addressed
b Since June 2007 the WTU returned 12956 Soldiers to duty with an average stay of seven months During that same period 13504 $Oldiers transitloned from the Army with an average WTU stay of over 14 months as cited in a report by Plans Analysis and Evaluations (PAampE) Office of The Surgeon General (OTSG) on Warrior Transition Status dated 14 June 2010 The current combined WTU and CBwru population Is approximately 9500
c There is a misperception that all or most Warriors in Transition(WT) were wounded In combat OTSG Status Report statistics show only 10 were wounded In combat 37 were evacuated from a combat zone due to disease and non-battle injuries and 53 had illnesses or injuries not associated with combat (COMPO 1 Soldiers command-referred and COMPO 2 and 3 Soldiers in mobilization and de-mobilization)
FOR OFFICIAl USE ONLY Oisseminmn is prohibited expect 8S authorized by AA 20 1
This Document contains information EXEMPT FROM MMlDATORV DISCLOSURE under FOIA Eemptioo 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6

SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
3 Inspection Summary The inspection team visited 17 installations with WTUs or caWTUs to assess their policies procedures and support systems Additionally the Inspection team assessed brigade and below unit procedures in managing Soldiers considered medically not ready (MNR) or medically not deployable (MND) Inspectors contacted over 2100 individuals during the inspection which included seniorunit commanders healtheare profesSionals cadre members WT and Family members rhe inspections determined that while the WTU leaders and staff are dedicated to supporting ourWTs there remained issues that must be improved This report outrrnes 24 observations 5 other matters and 56 recommendations
a Inspection Objective 1 (Assess Implementation and oversight of policies and procedures for the US Army Warrior care and Transition Program)
(1) The inspection team concluded that wru leaders and Cadre were dedicated and committed to assuring care and transition of Warriors back to duty or into Civilian life as productive veterans Inspectors interviewed 786 wr and determined that most felt that being aSSigned to a transition unit was the best place for them to recuperate however it remains soiety on the Soldiers personal motivations as the driving factor to either return to duty or decide to transition out of the Army Briefings and orientations provided by transition units helpeducate WTs on medical disability entitlements and often influence Sordiers personal motivations There is a noticeable sense of awareness about these entitlements among the wrs intervieWed However the lnspectof$ noted that the Warrior Care and Transition Program lacked a single synchronizing document outlining governing policies guidance and regulatory requirements There are numerous orders messages and policy memos that guide the program creating varying interpretations and in some cases confusion at the unit level rhe inspection team specifically assessed the eligibility criteria that was published in FRAGO 34 (July 2008May 2009) and found it vague The criteria of middotcomplex medical case management and -definitive healthcare are ambiguous and applied inconSistently to Soldiers seeking admission to a transition unit
(2) The Comprehensive Transition Plan (CTP) is the cornerstone of the WTs roadmap to healing and transitioning back to the force or to veteran status This guidance was inconsistently applied amiddotnd misunderstood within the WTUs The CTP sets Initial expectations for entering WTs and also guides medical providers and unit leaders to plan and assist WTs in the healing process
(3) Lastly the demand fQr behavior health services has increased as more Soldiers are diagnosed with PostTrajmatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI) Most WTU cadre and WTs s~ted specialty care provider shortages contribute to delays in diagnosis and treatment and thereby increasing length of stays
FOR OFFICiAl USE ONLY Dissemination Is prohibited expect as authorized by AR 20middot1
2 This Document contains information EXEMPT FROM MANDATORV DISCLOSURE IInder FOIAo Exemptien 5 applies
SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6

SA I G-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
b Inspection Objective 2(Assess Warrior Care and Transftion support systems for Soldiers and Family members) The Army Installation Management Command (IMCOM) assumed the mission of establishing and operating Soldier and Family Assistance Centers (SFAC) as part of the Warrior Care and Transition Program SFACs provide specialized Soldier and Family support services including but not fimited to child care legal assistance pastoral care travel claims lodging assistance for non-Invitational Travel Orders (ITO) Family members vehicle registration and translation services Although the services provided by the SFAC can be found In Army Community Service (ACS) and Soldier Processing Centers it is focused to support a smaller population with unique requirements such as providing a higher level of service catering to each individuars time and attention and maintaining access to more tranquil environments The team determined that the services may be underutilized on some installationsdue to the small population that they support
c Inspection Objective 3 (Assess tools and processes Implemented by Commanders to manage Soldiers who are tlMedically Not Ready (MNR)tl) Tactical unit commanders are challenged by the increasing numbers of assigned Soldiers who are MNR but are not part of a WTU Leaders face many challenges in managing Soldiers undergoing medical determination throughout the ARFORGEN cycle There is a Significant amount of medical resources dedicated to treating the WTU population which represents only about 26 of the MNR population The rest of the MNR Soldiers compete for the limited amount of medical resource remaining MNR SoldIers in tactical units undergoing medical determination processes profiles and board actions such as MOSMedical Retention Board (MMRB) Medical Evaluation Board (MEB) and Physical Evaluation Board (PES) can take up to 24 months nearly a full ARFORGEN cycle as cfted in GEN(R) Franks Task Force Report rrhe Franks Report) in April 2009 These processes are not synchronized with the ARFORGEN cycle The Armys medical resources are stretched and encumbered by anincreasing population of Soldiers that cannot deploy
4 Other Matters There were matters that did not fatl within the scope of our assessment butwere deemed appropriate for further discussion in this report The most Significant was the MEBPEBboard Inefficiencies which affected the Armys abilfty to meet Soldiers needs A majority of those Int~rvlewed stated that the processes are complex disjointed confusing and lengthy In The Franks Report WTs stated that the board process is stow reportedly taking a year or more to initiate and an additional 18-24 months to complete Less than1 0 of Soldiers In the MEBPEB process retuflcent to duty Which Impacts unit readiness In practicalfty Soldiers pending an MEB should be considered a loss to the unit which allows for a trained and ready replacement to be requisitioned Delays in the board processes cause existing efforts to expire and thereby repeating them which further draws on already limited resources Measurement of the board timeline is difficult when health care providers can stop start and terminate board actions tn some cases Soldiers identify -new conditions requiring initial evaluations or assessments Most of the subjects Interviewed were concerned that medical staffing is
FOR OFFICIAL USE ONLY Dissemination is prohibited expect as authorized 8) AR 20-1
3 This Document contains InformatioA EXEMPT FROM MANDATORY DISCLOSURE urlder FOJA Exemption 5 applies
SAIG-ZA SUBJECT Results of Warrior Care and Transition Program Inspection
insufficient to support timely MEBIPEB middotprocessing A detailed discussion of this is In the written report
5 Recommendations The report contains 56 recommendations for implementation as well as 24 observations and five other matters which should be considered by appropriate proponents as outlined in the body of the report Upon your approval the Director Army Staffwilldirect execution on your behalf
6 Follow-up The deficiencies enclosed in this report will be entered into the USAIGA Corrective Action Oversight System Designated responsible entities will provide bishymonthly status updates I recommend the Inspector General Agency conduct a follow-up inspection in 12 months upon approval of this report to determine the effectiveness of implementing the recommendations provided
Encl
~e WILLIAM H MCC~ Major General usY Acting The Inspector General
Reportof Inspection of the Anny Warrior Care and Transition Program
CF UNDER SECRETARY OF THE ARMY CHIEF OF STAFF ARMY VICE CHIEF OF STAFF ARMY
APPROVED0~ 11 DISAPPRO~- _____ _ SEEME~ __ ~~ ____ _
FOR OFRCIAl USE ONLY esseminatfon is prehibited eKpeGt as authorized by AR 20-1
4 This Doetlment oontsins information EXEMPT FROM MANDATORY DISCLOSURE under POIA Exemption 5 applies
Summary of Observations and Recommendations
OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States ArmyWarrior care and Transition Program
OBSERVA nON 11 No synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS
a OTSGMEDCOM Publish a single synchronized document to govem the Warrior Care and Transition Program Warrior Transition Command Is developing a single source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
OBSERVATION 12 Warrior Transition Units (WTU) foster a focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
OBSERVA nON 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has created perceptions leading to leadership medical management pubUc relations and small unit cohesion challenges
RECOMMENDATION
OTSGIMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior care and Transition Program
OBSERVATION 14 Challenges exist to implement rapidly Issuedchanging policy withoUt the requisite resources
RECOMMENDATION
OTSGMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 34 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS
a OTSGIMEDCOM Define acomplex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs OTSG Is currentfystaffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBwrU wrs with a length of stay greater than 12-months withoutMEB start date
b ASA(MampRA)lG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical Retention Processing 2 (lViRP2) and Active Duty Medical Extension (ADM E) into one order similar to COMPO 1
OBSERVATION 16 MEDCOMs accountability processes for Soldiers evacuated out of theater result In immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
RECOMMENDATION
OTSGlMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to detennine if they meet WTU entrance criteria
OBSERVATlON 17 Most WTU cadres are concerned with Inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS
aOTSGIMEDCOM Redefine the MRDPto be m~re clear concise and proscriptive develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP middotOTSG is currently staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTulcewru WTs with a length of stay greater than 12-months without MEB start date
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and pub fish policy regarding treatment of additional medical conditions subs$quent to admittance Into the Warrior Care and Transition Program (WCTP)
OBSERVATION 18 Selection of WTU Cadre shifted from best qualified to good and first available
RECOMMENDATIONS
a ASAMampRA)lG1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer Assignment POlicies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
OBSERVATION 19 The current Warrior Transition Unit (WTU) classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health Issues side effects of prescription medications and includes sensitivity training
b OTSGIMEDCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGIMEDCOM Require WTU Primary Care Managers to attend cadre training within 3Q days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
OBSERVATION 110 MostWTUs visited are not meeting the Intent and implementation of the Comprehensive Transition Plan (CTP)
RECOMMENDATION
OTSGIMEDCOM Provi~e policy and guidance to support automated CTP and enforcere-enforce the Implementation and execution WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
OBSERVATION 111 Most Warrior Transition Units (WTU) have not implemented the Transition Review Board (TRB)
RECOMMENDATIONS
a OTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASA(MampRA)lG1 establish reporting requirements of TRB resufts
c OTSGiMEDCOM Assessmiddot the feasibility of combining the TRB and the CT
OBSERVATION 112 Army-wide specialty care shortages exist in Behavioral Hearth Occupational Therapy and Physical Therapy and contribute to delays In Soldiers treatment and healing
RECOMMENDATIONS
a Army G3SI7 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
b ASA(MampRA)lG1 lew G3I5f1 and OTSGIMEDCOM review rOA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA MampRA)lG~ ICW G3S17 and OTSGMEDCOM confirm salary competitiveness amongbehavforar specialists
OBSERVATION 113 Army is failing to properly document Line of Duty (LOD) investigations for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS
a ASAMampRA)lG1 Publish message to commanders emphasizing required completlonof LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and TJAG ensure education and training tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)G1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGIMEDCOM Adopt LOD module in MODS as the Annys dedicated line of duty tracking system
OBSERVAnON 114 Perception that Warnors In Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS
a OTSGIMEDCOM ICW TJAG Emphasize the importance of maintaining good order and discipline and ensure WTs are herd to the Army standards of discipline
bOTSGIMEDCOM Implement cadre training that Is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
OBJECnVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warnors in Transition (WTs) with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounternear-tenn resource challenges (facilities funding and staffing)
RECOMMENDATIONS
a IMCOM Conduct cost-benefltanaysls to detennlne if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGlMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
OBSERVATION 22 Providing services for COMPO 213 Warriors in Transition (WT) and Families is challenging due to the dispersion of state resources
RECOMMENDATION
OTSGMEDCOM and ASA MampRA)G1 ICW IMCOM ARNG OCAR and Army PAD Establish a steering committee to detennlne most effective methods to deliver Information and servloo$ to COMPO 213 WTs and Families
OBSERVATION 23 Communities outside the gate are beginningmiddotto selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS
a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community Incentives
OBJECTIVE 3 Assess tools and processes implement~d by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Army does not use commonterms of reference to aCcurately determine status of medically not ready II medically non-deployable and not available Soldiers
RECOMMENDATION
OTSGMEDCO~ ASA(MampRA)G1 G3517 ICW FORSCOM Standardize terminltlogy for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
OBSERVATION 32 Anny medical fitness determination processes have not kept pace-with ARFORGEN requirements
RECOMMENDATIONS
a OTSGlMEDCOM ASAMampRAG1 00517 and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitnessmiddot for duty and retention or separation from the Anny
b ASAMampRA)G1 Code Soldiers in MES process as a oss allowing for replacement requisition
OBSERVATION 3~3 Army medical capabilities do not support the needs of the Medical Not ~eady (MNR)lMedical Non-Deployable (MND) in units
RECOMMENDATIONS
a OTSGlMEDCOM ASA(MampRA)lG 1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigate current limitations
b OTSGIMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deplOying RC brigade to assist in managing MNRlMND Soldiers The Integrated Disability Evaluation System currently in pilot program phase may enhance visibility of the system formiddotthe Soldierthe Army and the Veterans Administration
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION
OTSGlMEDCOM ASA(MampRA)lG1 and G3I517 Conduct a comprehensive MNRlMND support needs study to determine If medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instituted by the Army may assist commanders in managing their MNRlMND Soldiers
OBSERVATION 35 Leaders are concerned about Soldiers that PCS with known or unknown medical issues particularty behavioral heatth issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION
ASA(MampRA)G1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR40-501 11-48 (3) updating of MEDPROS commanders must emphasize medical In-processing to capture profile limitations and acknowledge Soldiers recent past deployment hiStory
OBSERVAnON 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are dIsadvantaged from a lack of information lOwer priority in access to care and length of MEBPEB process
RECOMMENDATIONS
aIMCOM Conduct cost-benefit analysis to detennine if SFAC services should be availablemiddotto all Soldiers in the MEB process
b OTSGlMEDCOM Make all MEa Soldiers same priority in access to care as WTs
c OTSGIMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBIPEB process to begin sooner Installation MedicaManagement Centers rerently instituted by the Army will assist in providing information to MNRlMND Soldiers undergoing the MEBIPEB process
OBSERVATION 3~7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization pJatfonn approximately 42 days or more ~fterrecalled to active duty
RECOMMENDATION
ASA(MampRA)G1 HRC ICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specific SRP within 25 days of mobilization prior to attending WIT MOS training and assignment to a deploying unit
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
RECOMMENDATIONS
a~ OTSGMEDCOM Continue implementation of reoommendations provided by GEN(R) Franks Task Force
b OTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGIMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Determine the laws that need to be changed in order to expedite the MEBPES processes and improve effICiencies between the Army and VA
OBSERVATION 2 limited andor no InteroperabiJitybetween DoD (AHL TA) VA (VISTA) TRICARE network and civilian provider infonnation systems
RECOMMENDATION
OTSGMEDCOM Improve the interoperability between DoD (AHL TA) VA (VISTA) and TRICARE network infonnation systems
OBSERVATION 3 COMPO 213 are no longer a strat~ic reserve current Army resources appear to be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRAG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to addflss RC medical care requirements as an operational force
b OTSGlMEDCOM ICW ASA(MampRAG1 G3517 ARNG and aCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
OBSERVATION 4 middotThe majority of medical management staff have some level of concern for personal safety in managing increasing numbers-of Soldiers with behavioral health issues
RECOMMENDATION
IMCOIVI ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
OBSERVATION 5 Most healthcare providers Interviewed (Primary care Man~gers Nurse case Managers) estimate 25-35 of WTs are dependent on ot addicted to drugs
RECOMMENDA TJONS
a OTSGMEDCOM Evaluate procedures for prescribing meetication and consider expansion of aHemative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MrFs
TASAmiddot
FfNDINGS AND OBSERVATIONS
OBJECTIVE 1 AsSess implementation and oversight of policies and procedures for the United States Army Warrior care and Transition Program
OBSERVAT10N 11 No synchronized source document outlining governing policies guidance and regulatory requirements
DISCUSSION Most leaders (212 of 242) interviewed stated inconsIstencies In policies guidance and regulations and a lack of a single synchronized document create challenges in command an~ control and medical management in the Warrior Transition Units (WTUs) These leaders opined that a single source document would shorten the amount of time spent researching information on a daily basis and enhance unit efficiency
Beginning with Department of the Anny Execution Order (EXORD) 118-07 Healing Warriors- with four Fragmentary Orders (FRAGOs) continlling with the Medical Command (MEDCOM) Operation Order (OPORD) 07-55 (MEDCOM Implementation of the Anny Medical Action Plan (AMAPraquo) and its 46 FRAGOs a plethora of All Army Activity (ALARACn messages MEDCOM memorandums and poliCies and Army installation specific memorandums the inspection team found over 109 different documents that leaders must use to manage WTUs Below is the MEDCOM Warrior Care and Transition Consolidated Reference list
Orders Publish ~nmceSubJects Dale
AJARACT 135-2007 14-Jun-G7 Initial Personnel Policy Guidance for Assignment and Attachment to Warrior Transition Unl1s (WTU)
AlARACT 138-2007 15oJun-D7 Documentlng Blast ExposurellnJury In Theater Medical Records
ALARACT 139-2007 1sJun-D7 Applicable Processing ProcedUAS for Military Orders Pertaining to Soldiers In a Palent Status WhO are Moved from Theater
ALARACT 141-2007 21Jun-D7 lnT - Family Escorts
ALARACT 153-2007 11Ju~ Announcement of ArmyMlld Traumatic Brain Injury (MTBI) Post traumatic StASs DhIorder (PTSD) Awareness and Response Program
ALARACT 160-2007 1sJul-07 Interim Guidancemiddot Army Mnd Traumatic BraIn Injury (MTBI) Post Traumauc Stress Disorder (PTSD) Awareness and Response Program
ALARACT 172middot2007 6-Aug-07 Transition Leayene ProcelSlna for AcIIYe Component (AC) (Medical Hold) and MoblllDd and Reserw Component (Re) (Medical HoldoVer)
ALARACT 175-2007 8-Aug47 Commander NotifIcalon of ArrIval and Departura of Medically Evacuated WantOl8
A1NtACT 185-2007 Z2middotAug01 Transition Leave Processing for AdJw Component (AC) (Medical Hold) and Mobilized and Rase Component (RC) Medical Holdover)
AI 4RlarT 18i-2007 23-Aug-07 Unlfonn Wear Policy Changes for Soldiers Assigned to the warrtor Transition UnIt(WTU)
NNWflm ~ DIcabIty AlARACT 21J2007 Y Medical ActIon Plan (AJIMP) Aueasment ConfweIIca
ALARACT 228-2007 17oct-C17 ubml8lllion of ReqUQts for Asslatancel Augmentation (RFAs)
fOR OFfiCIAL USE ONLY This dOCtlment contains llifolillation ~MPf FROM ~1ANDATORY DISaoOSUm ulld the FOIA ExemptiClll5
DissemlAatien is pmhlbitee eMept as aaFized by AR 20 1
ALARACT _ Combat - Retalad Injury Re~lItalion Pay (CIP) Policy
ALARACT 0 4-Janoa Account ctasslflC2tlona for RC Ordens
ALARACT PRlC8durai Change for TflII)Sfer of Health Recorda of Transitionlng Soldiers to VA
ALARACT 182-2008 2aJan-Ga Inspeclion of Military FaclllUes to House Recovering ServIce Members Assigned to Warrior Transition Units
AIARACT 205-2001 21-Aug08 RetentionmiddotBeyond Scheduled Release or Discharge D_ Due to Medical Reasons for Sotcfl8lS Assigned or AttacIIed to a WTU
ALARACT 224-2001 15-SelM8 Implementation Guidance on the Anny Wounded Warrior Clothlng Support Program (wwcsPI
AtARACT 295-2008 9-Dec-Oa MOD 1 to ALARACT 182-2008 Inspection of_Military Facilities to House Re~rlnl Serrice Members Assgnd to wru
ALARACT 006-2009 Wan-09 Policies and ProceduteS for the Handling of Personal Effects for Medically Evacuated Soldlens
-ALARACT 022-Z009 23-Jan-09 Pay and Allowances Continuation Program (PAC)
ALARACT 068-2009 12-Mar~ Pay an Allowances Continuation Program (PAC) Corrections
MEDCOIVI MEMO 15Jun07 Im~~entation of Transition Policy for Wounded Warriors In Medical HoIdfHo1dOY8T and Their Families
MEDCOMMEMO 21Ju~7 FY 07 Training Guidance (Change 1)
MMEMO 5-SeJHJ7 Suicide Risk In Warrior Transition Unfts (WTU)
COM MEMO 1aoet~7 Suicide Screening In Warrior Transition Unfts (WTU)
MEDCOMMEMO 9-OctoOl Release of a Soldiers P~ HeaHh Infonnatlon to the Department of Veterans Affdrs mvamp
MEDCOMMEMO 19-NOY-07 Holiday Guidance for wantors In Transition (W1)
MEDCOMMEMO 1-Dec-OT FY 08 Training Guidance
IIIEDCOM MEMO 11Jan-08 Movement of SoIdIenoln Transition between WTUs andWTlnlCBHCOs
IIIEDCOMwMO 25-Jan-G8 MEDCOM WT Comprehensive care Plan (CCP) Memo I Policy
MEDCOMMEMO 4-Feb-08 Provides initial guidance to all RMCs In reference to processing Reenlistment Eligibility ProhlbllionCode (ERUP) 9H to 10
MEDCOMWTO 22-Apr-D8 CBHCO Ombudsman GuIdance MEMO MEDCOMHRC 28-Apr-08 Updated poruy IRT Transition Training for Soldiers assigned to WlUs MEMO MEDC9MMEMO 2OOctoOa Holiday Guidance for Warriors In Transition (W1) and Cadra
MEDCPII MEMO 1SoOacgtOB FY 09 MEOCOM Command Training Guidance
WCTOMEMO 13-Nov-08 Support to Ute Amly Wounded Wantor Program (AM) Recovery Care CoordInation (RCC) Plan Implementation
MEOCOM Policy 5-Feb-07 IIEDCOM Conference Planning Guidance 0704104 MEDCOM Policy 3O-May-07 MEDCOM Military Treatment Facility (IfF) Access Standards for ActIve Duty 01~7 Services Members MEDCOM Policy 24JuJ07 Ph)Slcal Evaluation Board Ualson Officer (PEBlO) Training and CertiflCation 07-021 BIEDCOM Policy 1~Aug07 Ccmmander8 CritIcaIlnfonnation RequlnJmenl$ (CCIR) 07033 MEDCOM Policy 23-Aug-07 Escorts for Non-MedlcaJ careg1Yer8 and Families Traveling on Official Ordeno 07-1136 MEDCOM Policy 6-Sep-07 Ombudsman Program In Support of Warriors In Transition (WT) 01-1136
FOR OFFICIAL USE ONLY This doaiment contains information Dissemination Is ~hlblt9d
exeept as aulhsftzed by AR 20-1 BEEMPT FROM MANDATORY DISCLOSURE Iileer the FOIA Exemptieft 6
MEDCOII Policy 26-Sep-01 Metrics and Procedures for Improving Medical EvaJuation Board (MES) and 01-040 Physfcal Evalu8llOn Soard (PEB) PnIcesslng
MEDeOM Pollqo 2Wep07 Patient Movement from OUtsIde Continental United States (OCONUS) and 07-041 Reception ofWantors In Transition to ContInental United States (CONUS)
Military Treatment Facllrtles (MTfs)
MEDCOM Policy 250Mar Exemption for WTU tadre to PROAS and YEO AUG Assignmenl$ 01-003 MEDCOM Policy 0U14
Ntay-OB Wi Hlgb Risk Medication Review amp the Scle Provider Prognun
MEDCOM Policy 14-May-OS Accountability I Management of WT ReceIVIng tare at Remote Facilities 01J418 MEDCOM PoIIy WuI-08 MEDCOM Mmtary Treatment Facility (MTF) Acces8 Standards for ActIve Duty 08-028 Services Mambare
MEDCOM Policy 9-Jun-OB Transfer CIf~~~ In Transition (WTs) Assigned to ~de ~~nentat United 08-030 S1atea (OCONUS) Wamor Transition Units (WTUs) to CONUS MUs
IIIEDCOM Policy 23-Aug(18 I Warrior Transition Unit (WTU) Rlak Anesamant and Mitigation Policy 08-038 MEDCOM PoDey 1oMar-D9 Comprehensive Transition Plan (CTP) Polley 0g11
HQDA EXORD 051middot 19-1111ar-07 ISO CSA Wounded Soldier Family Hotline 07 HQDAEXORD11IJ 2Jun-01 Healing Warriors 07 FRAG01 to HQDA 11-Aug-07 Healing Warriors EXORD 118-07 FRAOO 2 to HQDA 14-Dec-07 Healing Wamonl EXORD 118-07
FRAGa 3 to HQDA 1JuJ08 Healing Warriors EXORD 118-01
FRAGa 4 to HQDA 19-May09 W1V Transition Review Board EXORD 118-07
OPORD09-22 27JM-09 Sulcfda and Accidental Death tnlerventlon-USAMEDCOM
OPORD09-12 15-Dec(18 Virtual Family RaadII1QS Grvup (vFRG)
OPORD08-21 7feb-Ol MEDCOM Soldler Transfer amp Regulating Tracking Centll
OPORDUTmiddot55 5Jun-01 MEDCOM lmpIamentation of the Army MedIcal ActIon Plan (MAP)
Annu A OPORD 5Jun-01 Medical Hold amp Medical Holdover Consolidation 07-55 Annex B OPORD s-Jun07 W1V Staffing 07-55 Annex C OPORD 5Jun07 Operatlonal capability BenctunarkB 07-55 Annex D OPORD I fiJun07 GIOSS8IyJ 07-55 Annex E OPORD bull 5Jun-OJ nrnellnal Calendar 07-55
Annex F OPORe 5Jun-07 WTI CDRI CSM1SG OrIentation Schedule 07-55
Annex G OPORD 5Jun-07 QuiCk Wins 07-55 Annex H OPORD stun47 Reports 07-55 Annex I OPORD 07middot 5Jun07 RlHaslgnment or Attachment of SoIdlens to the Wantor Transition Unit (W1V 55 MnuJOPORD 5oJun07 PatIent Admlnfstratlron OT-55
FOR OFFICiAl USE ONLY Thi document eonfains irTfoIl1lation SEEMFT FROM MANDATORY DISClOSURE tinder the FOIA ampemptien 5
Dissemination is prohibited exeept as alol1herized by AR 20-1
A-3
Annex K OPORO 5-Jurt007 Wanlor In Transition Program Standards 07-55 Annex L OPORD 5-Jun-Q7 Strategic Communications Plan 01middot55 Annex III OPORD 15-Jun-07 Facilltiel 07middot55 Annex N OPORD 15-Jun-07 Establishing Community Based Health Care Organization - Puerto Rico ICBHCO OT-55 ~
Annex 0 OPORD 15-Jun-07 Access tothe MODS Warrior Transition and Soldier Patient Tracking 07-55 AppDcatlons
i Annex P OPORD 15-Jun-07 Memorandum of Agreement (MOA) Between HQDA InstaJlation Management 07-55 Command (COM) and USAMEDCOM Concemlnll Comand amp Contnll of
Warrior Transition Units (WTU) and Medical Retention Processing Units (MRPU)
Annex Q OPORD 2Ju1-07 Ombudsmen 07middot55 Annex R OPORO 1QJuJ07 Staff Assistance Visits 07-15 Annex S OPORD 5-Nov-07 Resource Management 07middot55 Annex T OPORD 1-Feb-08 WTU Training Requlntmen1S 07-55
FRAGa 1 OPORD ampoJun-07 USAMEDCOIVI conducts an assessment as to RMCs wlll meet the required 07-55 suspense dates
FRAGa 2 OPORD 15-Jun-07 ProvIdu updated Information ntganfing MyIVIEB and SFACs 07-55
Add an additional specffted task to NARMC
Add two edditlonaispecHledta8ks to SERMC
Add three additional tasks to aU RMCs
Provides updated WIIb links for several WTU-related handbook templates and the latest edition of MEDCOM NOW
Provides factlities-nllated guidance to the RIIICs
Provides guidance and reporting requirement for MODSmiddotWT and Soldier Patient Tracking ProvkIea the MEDCOIVlIIMCOM Memorandum or Agreement regarding MHlMHO consolidation
FRAGa 3 OPORD 2-Julor Provides an upuate on WTU lOA 07-55
Provide guidance In the design and processing or flags for wrus
Add a speclfled task to AMEDDCampS ntgardlng a leadership study
Modify spedfied task to ERMC ntg1Irdlng SFAC Handbook
Modify specified tasks to GPRMC
lIIod1fy specified tasks to NARIIC
Modify specified tasks to PRMC
Modify epselfied tasks to SERMC
Modify speclfied _lea to WRIIIC
Modify specified task to AC5 Operations
Add opacified tasks to ACS HPU regarding standardized Triad training
Modify ipClCIfteCI tallm to ACS HR
Add 8 specified task to AC$ IEFM regarding facility maintenance proC8SSQ8
Add a specified task to DlR PASoE f8IJlIIrdlng WT surges
FOR OFFICIAl USE ONLY This document contaiIlS InfOrmation EXEMPT FROM MANDAToRY DISClOSURE under the FOIA EKempIiOft-amp
Oissemiftatiools prohibited except as authorized by Nt 2Q 1
Modify specified tasks to Wanior TIillISHIon Oftice formerly MHO
Modify coordinating Instructions to ERIIIC GPRMC HARMC PRMC SERMC and WRMC
FRAGa 4 OPORD 1oJuIQ7 Provides guidance on AMAPlatect staff _Istance visits which will occur 07-55 throughout Phasalll beginning with a Beta assistance vISIt from 24-28 JUL 07 at
Walter Reed Army Medica Center and lroob Army Medical Center
FRAGa Ii OPORD 24-JuIQ7 Provides UPDATE guidance on MAPmiddotrefated staff uslstance visits whhh will 07-55 occur throughout Phase m beginnIng wfth a Bata uslstanca visit from 24-21
JUL 07 at Walter Reed Arm Medical Center and Brooke Army Medical Center
FRAGO 15 OPORD 2TJul-07 Add applCMld WT mission statament by the Secretary of the Army 07middot55
Provides updated guidance to tha gap anaIysls I personna report In order to streamline and standardize personnel reporting
PlOYides updated guidance to MEl Status Report requlramants
FRAGa OPORD 31-Ju1Q7 Provide updated guidance to mTBIIPTSD training for Nrny Aetlve Duty and 07-55 ReaerveSoc11l Workers Nurse Case Managara PsyIhlatl1c Nurses and
Payhlatrlc Nurse Practitioners who are not PT$D trained
Cbanga updated mTB~D guidance and requirement to all MSCS In order to report statu8 ofmTBIIPTSD training
Add updated guldmce and requirement to all RMCs In order to report status on phase I metrlce
FRAGO 8 OPORD 3-Aug07 Provides additional guidance to RMCs integrating Anny National Guard Medical 07middot55 LNOa Into thalr respective MecflCal Treatment FacDItIe8
ProvideS updated guidance on AMAPlated _ assistance visits which win occur throughOut Phase DI beginning with a Beta asaIlIance visit from 24-21 JUL 07 at WaItGr Reed Arm Medical Center and Brooke Arm Medical Center
Provides updated guidance to rating color (Green Amber Red) definition I crtterla for the MAP Tracker
FRAGO 9 OPORD 13-Aug07 ProvIdea upclated guidance to all RM~ ordering procechns for WTU Rags and 07-55 Guidons
Provides initial guidance to NARMC and SEAMC to support a Visit offha Warrior Transition activities at Fort Benning and Fort KnCIX by e program analyst from
I the OIftco of Budget ampl8anagament COMB) VateranaAffaIIS amp Deftnse Health In order to ensure that Army health eare acttvIty requIrementS 1119 matched against the PresIdents naIIonai dllfunse budget requirements
Provides updated guidance to the gap analysis I personnel report In order to streamline and standilUCllu personnel reporting
ProvidM updated guidance and requirement to a RMCs and staff In order to report status on pbase I metrfca
PlOYid89 initial guidance to an RMCs on asslgnlnent criteria to S8IV8 as a gUide for the Ignment manage that select the Soldler8 regardless of component or corps to serve as wru cadre
Provides updated guidance to all RMCs on weekly OmbudsmenlPatI8nt Advocate WT ~ SPT access status
FRAG010 OPORD 14-Aug07 Provides updated guidance to NARMC and SIRMC to support a visit of the 07middot55 WarrIor Transition activities at Fort Benning and Fort KnCIX by a program analyst
from tha OfIice of Budget amp lIIanalJemant (OMB) Veterans AffaI amp Defense Health In ordar to ensure that Army health care activity requirements are matched against the Prasldenta national defense bllclgat requirements Due to other obligations the program analylt from OMI wfll not be able to visit Fort Banning and Fort Knox Currently there Is no tantalfva re-scheduled visit date planned
FOR OFFICIAL USE ONLY This dOCUlliellt co-utah is ilifollilation EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptioo 6
OieeemiAatien Is pmhiblteEi 8)(f38It as authedzed by AR 20 1
FRAGa 11 OPORD Z30Au9ltl1 Provides updated guidance on the requlremenUo submit Commanders 07-55 Crftlcallnformatlon Requirement (CCIR) When a Medical Treatment Facfllty (MTF)
fails to notify depl0J8d and rear detadunent commandera for aD arrivfng and departing Warriors In Transition
Provides notJflcatlon guidance when a Serious incident or Commanders Critical information Requirement ewnt OCCUIS with a Soldier gned to I Warrior Transition Unit
DeIlgnata the sactlonlactMty responsible for the notification activity In writing
Provides additional reporting guidance to Human Resources Command based on inquiries from the field
FRAG0120PORD 24-Au907 Provides initial guidance to Almy Medical Department Center and SdIooI 07a (AMEDDCampS) Warnor TranslUon OffIce (WTO) and ACS Operations on the
development of the warrior In TransltJon training modules
ProvIdetI updated guidance and requlrerpent to all RMCs In order to report status on phase I metrlca
ProvIdes updated guidance to all RMCs on Wanlor In Transition definition change
FRAGO 13 OPORD 3QAug-07 Provides updal8d guldance to all RMCs ordering procedures for wru Flags and 07-55 Guidons
Provides updatecf guidance to mTBIIPTSD training for Arm ActIve Duty and ReselVl Social Worbrs Nurse Case Managers Psychiatric NtmI8I and Psychiatric Nurse PractitIoners who are not PT$O trafned
Provides updated guidance d I8CfUlrement to all RMCs andmiddotstaff In erder to report status on phase I metrfcs
Provides initial guidance to an RMCs In raference to MILPER Message Number 07225 Transition Services for Soldlera AssIgned to Warrior Transition Units CWTU and Adjustment of VA Benefits Briefing Delivery
Provides updated guidance to an RMCson MTFs providing updated wru Cadre rostenI to the Warrior TransHIonOffice
Provides updated guidance to all RMCs on Warrior In Transition definition change
Provides updated notification guidance when a Serloua incident or Commanders Critical Information Requfrement evant occurs with a Soldier assigned to a Wanior Transition UnH
~~GO 14 OPORD 7sep-07 Provtdea Initial guidance to allUlCs In reference to AlARACT 18512007 07middot55 Transition Leave Processing for Active Component (AC) (Modical Hold) and
Mobilized and Raserw Component (RC) (Medical Hoidowr)
Provides initial guidance to all RMCs in reference to ALARACT 1I8l2007 SepanltionRetlnlment Due to Physlcel DIsability DTG 28 1622Z AUG 07
Providu Initial guidance to all RMClln nftrence to thamp establishment of a HQDA DCa Go1 website for all Go1 MItPER Messages ALARACTs and Warrior Transition Unit (WTU) consolidated G1 guidance
Provides Initial guidance to PRMC and MEDCOM JAG in th8 completion of the mIssion analysis for new HQDA EXORD tasks
FRAG01S0PORD 1t-Sep-07 Provides updated guidance to NARMC on MAPmiddotrelated staff assistance viSits 07middot55
Provides updated guidance and NqUirement to PRMC In order to report adcHld task to the AMII TraCker Report
Provides updated guidance and requirement to all RIIIC In order to report status on phase I matrics
FOR OFFICIAl USE ONLY ThIs document comaln Information SEEMPT FROM MANDATORY DI~CbQSURE Uflder 1M FOIA E-xeFftplieA 5
DlssemiMIIaA 19 PftINbited 63tee1R 8S eulherized by AR 29 1
AfJ
ProvIdes InHJai gultlance and requirement to aD RMCs In reference to havlng MTf WTU Case Manage aasIat USMC Wounded Wantons tracking In MeanT to acquire Defense Knowledge Online accounts 80 that the Martne can view hlsfher MyMEBpage
Provides updated guidanca to all RMCs on Warrior in Transition definition change and wrs assigned as duty drtvara I cadre (Annex I (Re-assignment or Attachment of Soldiers to the Warrior Transitionmiddot Unit (WIU) Provides initial guidance to all RMCa In reference to the Warrior Transition Office hostingmiddot Case Manager OrIentation and Training Conference at Walter Reed
FRAGO 18 OPORD 28-Sep-07 Provides updated guidance to all RMCs in refw8nce to the Wantor Transition ONi5 Offlce hosting a case Manager Orientation and Training Conference at Walter
Reed
Provides Initial guidance to all RMCa on COMPO accuracy to ensure that all COMPOs ant staffed with the equlVBIent COMPO as stned In the DA G-3 applOVlld TDA
Provides InWai guidance to aU RMCa In reference to the WarrIor Transition OffIce launching a new website on AKO for MCa to tile best practices local peDcy and procedures and standardized local forms
Provides initial guidance to HPampS and Reserve AffaIrs in reference to conducting analysis Of all celRa regarding lata notlfIcatJon (beyond 24 hours) to Main Body and Rear Detachment Commanders upon arrival and departure of WTs to MTFs lAW ALARACT 17512007
Provides InWai guidance to HPU In refurence to updating OTSGJMEOCOM Policy Memorandum osG15 Release of Protected Health hlfonilatlon (PHI) to WTU Commands
Provides lnltJal gufdance to HPampS In mwence to updating Annex I to MEDCOM OPORD07-55 ProvIdes Initial pldance tomiddota11 RMCs In order to direct W1Us ~ Issue WT mlsampianlchaln of command contact Information cards to WTs
ProvIdes initial pldanceto all DCs In reference to submitting wru HOWling Inspection Report and Medical FKIIIUes ~nt Report to MEDCOM ACSIEFM
FRAGO 17 OPORD 15-Ocl-tJ7 Prvvfdes updated guidance to all RMCs In ntferenee to requirement to submit a 07s5 Commanders Crftlcallnformation Requirement (CClR) when a Medical
TreatmentFacllIly (MTF) faII8 to notIfydeployvd and rear detachment commanders for all arriving and departing Wantors In Transition
Provides updated guidance to all RIIICs on MTFs providing current WTU cadre rosters to U1e Warrior Transition OftIce
Provides ~pdated guidance to Ifl RMCs in order to direct WTUs to Issue wr mission I chain of command contact Information cards to WTe
PnwJdeslnltlal guidance to all RMCs In order to direct WTJs to standardize cadre I unit voice mall greeting me8118g9S on all official mRltary phone answertng machines and govemrnent ceD phones I blackberries voice man
Provides updated guidance and requirement to all Mes In order to report added taskS to the AMAP Tracker Report
ProvIdeS updated guidance to all RMCs on asslgntng WTs as duty drivers I cadre
Provides InWaI guidance to all RMCs In Ilferenee to revlewtng the attached document tltJecILesaons Laarned
FRAGO 18 OPORD 1T()ct-oT ProvIdes updated guidance to all RYCs In refurence to requirement to 07lt55 organizationally align TRIAD Support within the WTUs
FOR OFFOW USEONLV
This doctlment contains inlormation E3(EMPT FROM MANDATORY DISCLOSURE tinder lie FOIA Elcemption 5
Di998miAalieA is p9hibited eeept as ampIlAelf2ed by AR 21) 1
Provides updated dinKtlon to all RMCs and MTFa to conduct 100 baseline medication review and reconciliation
Provides updated guidance to an RMCs In order to direct the conduct of Suicide Risk Asnssments Provides Initial guIdance to all RMCs In order to direct WTUs to conduct wr accovntabillty
Provides Initial guidance to all RMCs In order to direct WTUs to ensure that WTa complywittl the Anny Urinalysis Program
Provides InitiaI guidance to all RMCsin order to direct WTUs to provide emergency contact information to the wr FamiDes
ProvIdes Initial guidance to all RMCs in order to GnSUn1I that WTU cadre mambena have proper leadership and communicative aldlls to lead the WTs
ProvIde Initial guidance to all RIIC In order to ensure the Intltgration of all specialty care to Include medication and prafile reconciliation
ProvIdes Inlttalguldanclt to all RMCs In order to dIrect WTU commande to property align teSOUn8S and report shortfalls
FRAGO19 OPORD
J 5-Nov-01 ProvIdes updated guldance and requirement to all RMCs and staff In order to
07-55 report status on phase 1 II 10 amp IV matrlcs
Provl~ updated mlBlIPlSD guidance and requirement to an MlCs in order to report status of mTBIIPlSD training ProvIdes updated guidance to all DCs In order to decrease rvport requirement tasb to the AMN Tracker Report
ProvIdes updated guidance to NARMC and ERMC on AMN-reIa1ed statf assistance visits
Provides initial guldance~ to all RMC In order to ensure the Integratton of Resource ManagementAnnu
ProvIdes updatad guidance and requirement to all RMcs In nrlerence to having MTF PAD asampist USIIIC Wounded Wanion tracking in MEBnT to acquire Defense KnDWIedge Online Kcounts 80 that the Marine can view llelr My Mea page
Provtdes upcialadguldance and requirement to all RIICln order to report Intemal SAY comPliance and findings Provtdes Inltta guidance to aD RMCs in order to ensure Ihafsubordlnate MTFelWTUs are provtdlng escorts for wr during In-processIng and out-processing
Provtdes Initial guidance to all RMCs for the issue of a government IMPAC Credit card to the WTUs
Provides Initial guidance to all RIIIICs In order to direct currently assigned WTU personnel (Squad Leaders Platoon Sergeants Nurse Case Managers and Primary Care Managers) to complete ATTRS courses BEf2 61middotf7300FS5 and6J Ft3tJ0F34 I ~IltiaI guidance to all RMCln order to direct WTU Commanders to
an office call with their respective Senior Mission Commander
Provtdes InlUaI guidance to an RMCs in order to direct W1U Commanders to schedult 1111 offIclat office call with their atatau Veterane AffaIrs OffIcer
Provides InitIalguldattce to all RMCs In order to direct WTU Commande and CBHCOa to coordinate for sensftfYity training for WTU amp CBHCO Cadre
ProvtdeS initial guidance to all RMCsIn ordar to ensure MTFs validate that Ombudsmen posters are posted In WTU area and MTFs and Ombudsmen bualnlSS cards are giftn to IMIry Incoming WT and family member
Provtdes lniUal guidance to an RMCsIn Order to submit foIIOWoup actions taken In (Isponae to the AMAP SAY
FOR OFFICIAL USE ONLY This documellt contains infomation EXEMPT FROM MANDATORY DISCLOSURE tinder ttle FOil exemption 5
9issemiAatien is prehibiteEi exeept as alltheFlzed by AR 20 1
A-8
FRAGO 20 OPORD 15-Nov-01 Provides Initial guldanca and requirements to an RMCs in order to SUpport the 01-55 upcoming Warriors In Transition leadership and Training Conference
fRAGO 21 OPORD ~Dec-07 Provides initial gufdance to AMEDDCampS In order to provide asslstance to 07~55 Behavioral Health in utiflzlng I tailoring the ProVider ReslUency Training (PRl)
plan In order to support the Army Medical Action Plan (AMAP~ phaS81D task Aaaes ProvfderFatlgue
Provides updated guidance to all RMCa in order to traek mTBIIPTSD training for Army ActIve Duty and Raserve Social Workers Psychlatrfc Nurses and Psychlatrfc Nurse Practitioners who are not PTSD traIned
Provides updated guidance and requirement to all RIIIICa in order to raport status on phase I If III amp IV matrics
ProvIdes updated guidance to all RMes In order to direct curreRUy assigned WIU personnel (Squad leaders PlatoGn Sergeants Nurse case Managers and PrImary Care Managers) to complete ATTRS coursas BE-F2 6Jf7300F35 and 61-F8301I-F34
ProvIdaalnltlaJ guIdance to all MCs In order to ensure ihe Warriors In Transition Units (WTU) execute Personnel Accounting and Strength Reporting (PAl) (foeusing only on WTU Cadre and warriors In TranaHion (WT)) lAW AR SOD-U
Prvvtdes Initial guidance to all RMCa in order to ensure the Wantors In Transition Unlts(WTU) 4p[ecute Personnel Accounting and Strength Reporting (PAl) (focusing only on WTU Cadre and Warriors in Transition (WT) lAW AR SOD-U
FRAGO 22 OPORD 12-Dee-07 Provides updated guidance to all RMCs In order to report status on phase I II III 01-55 amplVmetrlcs
Provides Initial guidance to all AMCs In order to report complance with the Holiday Guidance memorandum for warriors In Transi1lon(W1)
PrvvIde Inltalguidance to all RYe-In order to report Quartel1) Training Brief ( (QlB) dates for all Warriors In Transition Units (W1U)
FRAGO 23 OPORD 1Nan-08 ProvIdes initial guidance to GPRMCr NARMCr SERMC and WRMC in order to 07middot55 conduct mission anatysIs to bring the CaHCOs located In their ruglons under C2
of cfosest wru commander In onIerto centrallzit C2
Providea Initial guidance to AIVIEDDCamp8ln order to dewlop tndnIng content fOr the Wantor In TnmsItIon concept for TRADOC to Integrate Into existing TRADOC leader clevefopment courses
ProvIde8 Initial guidance to HPampS In order to conduct a pilot program utilizing existing technology to automata the ph)Sicalprofile system In conjunction with G1 US Army ReselV9 and ARNG
ProvIcIes Inltlal ~ce to HPampS In onIarto lItISIat the DA 61 wftb applyfng the Lean Six Sigma methodology to reduce the number of documents in the Medical Evaluation BoardIIhyslcal Evaluation Board process by 50 percent andor establish these as a web-based process
Provides Initial guidance to tlPampS In order to submit a rapid adIon rellslon to AR 40-400 allowtng an MEB the authotfty to refer a service member to an ORB If a sarvie membars conditions ani detannlnad to be fit but the service member can no lOnger perform duties commenampUT8lD with their IIOS functional aptitude
ProvIdes Initial gulcfance to HPas In order to establish policies and procedures for the dllV8Jopment of a COII1pn1henslve rehabilitation plans for all WTL
ProvIdes Initial guidance to HPampS In order to dewlap and Issue guidance requiring MTF Commandere to llB8iat the Solcllers chain of command by provIcllna necessary m8CllcallnpUt for the R18k Mitigation Matrix
FOR OFFICIAL USE ONLY This ckxumenteontains information EXEMPT FROM MANDATORY IgtISGlOSURE lAd the FO EMmptioo 6
DlseeminaliEm 1amp pmhlbited EmGept as ellorized by AR 20 1
A-9
Provides Initial guidance to HPIS In ord~ to assess if Soldiers within WfUs have a peneption of In~nslsteney In the application of Anny disability standards Provides initial guidance to IEampfM In order to assess all WT billets housing and lodging and wru unit 111888 lAW DoD and Amry standards
Provides Initlal guidance to IEampFM in order to lead II quarterly MILCON synchtonizatlon meeting JCW IMCOM and Department of the Army GR
Provides Initial guidance to RM In order to dewlop and submit a funding request for WTs to receive specialtY uniform Items replacement uniform Items and allaratlon of existing uniform items
Provides Initial guidance to the WTO In order to develop and Implement battle hand OWl procedUJ8S to be ueculBd each time a member of the WTs Triad or the wr PESLO changes
Provides Initial guidance to the WTO In order to qtabR$h a policy mandating reautlt coordination between the Triad and PESLO staff bull
Provides Initial guldartce to the HPampS In order to ~blish a training and counseling program for WT Caraglvel8
Provide updat guidance to all RMCs In order to report status on phase II Uf amp IV metrtcs
FRAGO 24 OPORD 1middotFeb-08 Provides updated guidance to AMEDOCampS In referilnca to the consolidated 07-55 guIdance on WTU trainlngdewloprnent and coordination
Provides Initial guidance to AcS Operations In order to support the Wamors In Transition Unit (W1U) staff training ntqutrements
Provides updated guidance to all RMCs in order to direct newly assigned wru personnlJl to complete ArrRS course 61f8300F36 cwru Staff Support Orientation CoIP1l8) vice 61F6-300F34 cwru SIaff Support Courae) and 61F7-300F35 (WTU SUpport Course) and on ACEP Mobile Training Team (MTT) and loeaJly pnwlded training
FRAGO 25 OPORD 5-FIb-OI Provides initial guidance to GPRMC In order to suppoft the pnot program 01middot55 Automate the lIIedical Evaluation Board (liES) Process at Brooke Army Medical
Center
Provides updated guidance to aD AMCs In order to report status on phase I II m amplVmeb1cs
Prvvtdes initial guidance to all RMes In ordarto direct all MTFalWTUs to validate 100 WT penlOllai phone number address and Nqlln MODS
Provides initial guidance to an AMCs In onter to direct MTF Career Counselors f Reenlistment NCOs to Include the WTU staff and yenITs In their ~pa of ruponslbillty
PrcMdes initial guidance to aURMCs In order to drrect MTFs (WTUs to ensure that PEBLOs are aligned with wr ptatoons within each WTUs
Provides initial guidance to all AMCs Commanders in order to direct MTF Conunande~ to Include the WTUs (battalIon and company) In their scope of safety reaponalblllty (MTF Safety OffIcers)
Provides Initial guidance to all Des In reference to WlUs submitting monthly USR reports
PnlYldaa InItIaJ guidance to all RMCs In reference to processing Reenlistment Englbillty Prohibition Code (ERUP) IH to 10
FRAGO 26 OPORD 12-feb-08 Provfdeslnitial guidance to all AMCs In reference to the Warrior In Transition 01-55 (WTl P8n0nneI8f training Confantnce
FOR OFRCfAl USE ONLY ThIs docttment contains infom mOil aEMPTFROM MANDATORY DISCLOSURE under the FOIA Exempticn 5
Dissemination is prehiblted eJleept as atrtttGlimd by M 2Q 1
A-10
i
Provides Initial to an RIle In order to enhance the C8HCO access standards In the natworIt are 21181Jable to all WTs nIgIIIdIess of ph)BJeai location
FRAGO 27 OPORD 16-Felgt08 Provided Initial guidance to all RMCs IRT unexpected deaths from accidental 07-55 drug overdoses and sUicides In WTUs continue to rise with 11 such Incidents
since JUN 07 Tasked RIICs to report on 18 WTU Tasks (Findings from the Tiger Team
FRAGa 28 OPORD sMar-08 ProvIdes updated guidance to811 RIICs on h Nurse CUe Managers ATlRS OHi course 6E-F2 and on Army Center Enhanced PerfOnnance (ACEP) Mobile
Tralnln~ Team (MlT)
ProvIcses updated guidance to all RMca in reference to ~ SICretaJy of the Army and Chief of StaR of the Army nteently dlreded bull comprehensive study to determine rtstc mitigation antfll8aOClated controls to stem the n88 In these deaths
ProvIdes InlUaI guidance to all RYCs in order to submit Ionnal After ActIon Reports (AAR) when the Department of the Anny Inspector General (DAIG) or inspection General (16) YIsHs a warrior In Transition Unit (WTU)
lnlUaI gulcSance to NARIIIC SERMCand GPRMC In order to support a Department of the Army Manpower AnalysIs Team which wlR validate standiuds currently used to determine W1lJ staffing rsqulrementswIth particular emphlsls on WT acuity IIMII and location
ProvIdes updated guldance to all RIles on the rsqulrwnent to sulmlt a Commanders CritIcal Inklnnallon Requil1llnent (CCIR) when a Medical Treatment Facility (MTF) falls to notify deployed and 1881 detact)ment commanders for all arriving and departing Warrlora IrI Transition
FRAGO 29 OPORD 14-Mar08 ProvIdes updated guidance to NARMC In order to support Depatment of the 07-55 Anny Manpower Analysis Team which wiD vandate standards currently used to
c1etennlnllwnJ stalling raqulrements with particular emphasis on WT acUity lewl and location
ProvideS updated guidance to all RMC In ontarto provide updated standards to the 8cceamp8 to care
ProvIdes updated guidance to all RMCIIlnrvference to WJUIJ ubmlttlng monthly USR reports
Provides updated guidance to all RMCs In order to submit formallUt2r ActIon Reports (AM) when the Department of Itte Army Inspector General (DArG) or Inspector General (IG) visits a Warrior In Transition Unlt(WTU)
Provides guidance to all RMCaIn reference to a decrease of documents required fIom 32 to 19 for the submIasIon to the PEB reformatting of the commanders letter and the addition of the Commanders Performance and functional Statament bull
PrcMdes updated guidance to all RMe In reference to ellmlnalfng the requirement for PEBLOs to complete the distant learning orientation trainIng
FRAGO 30 OPORD 28-Mar-08 Provides updated guidance to GPRMC NARMC SERMC and WRMC In order to 07-55 conduct mlaalon analysis to bring the C8HCOs locattd In their reglonll under the
C2 of closest Wamor Transition Unit (WTU]commander In order to cenballie C2
ProvIdea updated guicSance to all RMCs In o~ to delete Itte report submlaslon requirement fotWamors In TransWon (WT) with undrgraduateor graduate degraes In order to define tarptpopuillfon In support of Army Inltiatfve 5 which offens WTs the opportUnity to compata for gradumHeYe1 education scholarships and potential employment as faculty at Intermediate Level Education (ILE) military academies Senior Service Collages (SsCa) and othermiddot service schools
Provides updated guidance to an RIIICs In reference to general order 1 In support of the 18 quick wfns published In FRAGa 1
FOR OFFICIAL USE ONLY This docullient willalliS illfoml8tion
SEEMPT FROM MANDATORY OISGlOSURE tinder the FOIA Exemplion 5
OissemiAaticm is prohibited elCeept as 8tJthoriEed by AR 2()1
A-11
ProvIdes initial guidance to an RIlle In reference to directing WTUs to review distribute and complywlth the uPdated Behavior Health care of Service lIIembers standing operating procedure (SOP) Social Work IlIIlsslon Statement and White Paper
Provides Initial guidance to a11 RMCs In reference to dfrecting WTUamp to submit Knen shots of all horne vruwn programs (determined by local WTU staff to be essential In managing WT) to the Warrior Trensltlon OffIce (WTO)
ProvitIellnitial guidance to all RMCs In order to determine dothlng modification requirements In support of WTs and estabnsll a supporting HQDA program for unifonn modlflcm60ns
Pr0vide8 Initial guidance to all RIlle In refallnce to the upcamlng Warrior Transition Comprehensive Care Plan Workshop
Provides updated guidance to all RMCs In reference to Guidelines for Eligibility SeleCtion and Acceptance Criteria for Referral to a WTU
FRAGO 31 OPORD 1oAproa Provides initial guidance to GPRMC NARMC SERMC and WRMCIn support of 07-55 Human RQources (HR) staff asalstanca yisrts In order to __ the
effectiveness of 8JdstIn9 Hmnm Resource systems and provide training guidance and recommendations for process ImpllMlllents
ProvIdn updated guidance to all RMes In order to delete the report submls$lon requirement for the AMAP Tra~r report
ProvIdes updated guidance to aD RIlICs In reference to MUs submltUng monthly USR reporta
ProvIdes initial guidance to all RMCs In reference to Special Duty Assignment Pay (SDAP) forWfU squad leaclere and platoon ~
FRAGO 320PORD 1~ay08 Provide Initial guidance to AMEDDCampS In order to proYide assistance to 07middot55 Betiavloral Health (BH) In tile estabnshment vf a counseDng program In order to
support the Army MedlcaI ActIon Plan (AMAP) phase IV task Establtsh a Training and Counseling Program for WarrIors In Transition (WI) careglve
Provide updated guidance to all AMCs In order to raport status on phase I II m amplVmetrics
Provide updated guidance to all RMCs in reference to WlUs submitting monthly Unit Status Rsports (USR) reports ProvIde Initial guidance to all RMCs in reference to the Human Resources Command (HRC) Memorandum Revised Policy Regarding TransttlonTralnlng for Soidle In WIUs dated 2t APR 08
FRAGO 33 OPORD 2O-Jun-08 ProvIdes Initial guidance to NARMC In order to support additional 07-55 requirement at Fort Drum MEDDAC In support of the Warrior In Transition Units
mission
ProvIdes updat8d guiclanceto MEDCOM RM In order to support additional budget requirements at Fort Drum MEDDAC In support of the Warrior In Transition Units mission
FRAGO 34 OPORD 27JunQ8 ProvIdes Initial guldancs to Army Medicsl Department Center and School In 07-55 support of the Provider ResIliency TreInlng Program
Provides updated guidance to ACS Operations In support of the ProvIder Resfliency Training Program
ProvIdes Inltlalguldance to Health Policy and Servfces In support of the Provider ResfUency Training Program
PlOIIIdes updillt8cl guidance to all RMCs In order to report status on phase I II III aJVmetrtca
ProvIdes Initial guidance to all Rilles In order to uecute SemImiddotAnnual Training Brtefs to the IIIEDCOM Commander
FOR OFFICIAL USE ONLY This dOCtIITIent colltains infellfl8tion EXEMPT FROM MANDATORY OISGlOSURE ~nder the FOIA exemption 5
OlSGemiAatisn 1amp pl9hlblted exeept as euthWed by AR 29 1
A-12
I ProvIda$ Initial guidance to aU RIles In reference to wantor In Transition Units being authortzed to lssueBlackberrles to squad leader cadre In aupport of the WarTlor In Transition Units mlaalon
Provides Initial guidance to all RllCa In rafentnce to the Implementation of the Provider Resmency Training Program
Provfdes updated guidance to all RMCs In orderto Implement the digital profile
FRAG035 ul-08 ProvIde updated guidance to all RMCs In reference to WTUs submitting monthly 07middot55 Unit Status Reports (USR reports
Provide updated guidance to all RMCs Inorder to execute ampemf-Annual Training Briefs to the MEDCOM Commander
FRAGQ 36 OPORD 11Ju1008 Provide updated guidance and clarity to all RMCs on the optImaildantlflC8tion 07-55 screening referral and management of Wounded ID and Injured SoldlerL
Warnor Transition Units (W1U) are designed to meet the needs of Soldlens who were wounded til or InJured In theater andor require complex medkal and case management through the Trtad of Care (primary care manager nurse case manager and squad leader)
Provide updated guidance to all RIICs on the requirements for ellby and exit of Warrlora In Transition (WT) ralnIones cadre manning requirements and clarifies command and control
Provides initial guidance toHeaJth Policy and Servtces In reference to developing a process to track permanent and te~rary profiles
Provides Initial guidance to Health Policy and Servtces In ref1mmce to ImpnMng lhequality validity and rallab1lltyof Medlcal Evaluation Board IntomaJ Tracldng Tool data and developing 8 computeriDd procen to forward Soldier signed MEB results
ProvIcf~ Initial guidance to Human Resources In reference to streamline the reassignment Instructionsrequest for ardors process
Provides initial guidance to Program Analysis and Evaluation In reference to dlrectfng Manpower Division to assist the DCS G-315I1 In the davelopment of TDAs
Provides initial guidance to the Ylanior Transition Office In rvfarence to prcMding command control and expeditious dl8pos1t1on of WT SOldiers awaiting reassignment or aepandlon from the seyenlce
Provides updated guidance to all RMCs on Wanior In Transition definition change
ProvIdes Inldal guidance to all RIICs In reference to MTFsIWTUs coordlnatfng with Installation Senior Command
Provides initial guidance to all RMCs In reference to WTU requirements for the Pb)SlcaI Disability Evaluation System Enhancement
ProvIdes Initial guidance to all RAIIC in refenmce to the establishment a MlC
Provides Initial guidance to all RMCs In reference to UKutlng MEDCOIIJs standardized methods and tools for tracking WTU execution Providea Initial guidance to all RMCa In reference to SpacialDutyAsslgnment Pay
FRAGO 37 OPORD 31Jul-08 PnMdes initial guI~ to the MEDCOM Staff In support of the Warrior In 07-55 Transition (WTU) Seml-Annual Training Brief (SATB) to the MEDCOII
Commander to Include the stafta participation In both a staff rehearsal wtth the MEDCOII Chief of Staff and the actual WTU SATB to the MEDCOM Commander
FOR OFFIGtAL USE ONLY This document contains iliformation EXEMPT FROM MANDATORY DiSClOSURE tinder tfte FOIA Elcemplian 5
Dissemination is prohlbtted exeept as atltheliied by AR 20 1
A-13
Provides updated guIdance to all RMCs to raquest-reasslgnment for active component (AC) and Activa Guard and Reserve (AGR) Warriors In Transition
- (WT) classified 815 Retumed to Duty (RTD) to Include the publicatIon of an RTD Validallon Checldlst
Provides updated guidance to all RMCs In order to execute SemimiddotAnnual Training Briefs to the MEDCOM Commander
Provides initial guIdance to all RMCs to ensure WTUs use the ConsoUdaled RTD Submission Worksheet when submltllng requests for assignment Instructions (AI) to HRC
FRAGO 38 OPORD 15-Sep-08 Provides Initial guidance to th9 MEDCOM Staff in support of the Warrior In 07-55 Transition (WTU) Unit Status Report (USR) to the MEDCOM Commander to
Include the staffs participation In both a staff rehearsal with the MEDCOM Chief of Staff and Director Wanfor Care and Transition OffIce (WCTO) and the actvaI USR brief to the MEDCOM Commander
Provides updated guidance to all RUCs In order to report status on phase I n 01 IV metrlcs
Provides updated guidance on required VA briefings 10 all WTs
Provides Initial guidance to RMCs reference the wru Cadre Resident Course to be conductad by the AMEDDCampS
Provides updated guidance to all RMCs In reference to wru submitting monthly Unit Status Reports (USR) and briefing the USR to the MEDCOM Commander
Provides updated guidance to all RMCs reference acronym change from Community Based Haalthcare Organization (CBHCO) to Community Based Wantor TransiUon Unit (CBWTU)
Provides updated guidance to all RMCa reference CBWTU referrals of WTs from Nebraampka and Kansas
FRAGO 39 OPORD 31()ct-Ga Provides initial guIdance to Health Policy and Services (HPampS) to provide Wli 07-55 HeDP code stamps to MTFa WTUa end CBWTUa In support of the new
TRlCARE enroOment requirements for Warriors In Transition (WT)
Provides updated guidance to all RMCs In order to report status on phase I H III IVmatrlcs
ProYidea updated guidance to all RMCsln reference to the Implementation of the Provider Resiliency Training
Provides Initial guidance to RBIICs on the assignment and use of special Defense Enrollment ERglbility Reporting System (DEERS) enroRment codes known as Health Car Dclllwry Program (HCDP) Plan Coveragecocfes In order to more effIclentry manage the WII population
Provides Initial guidance to AMes and Staff on the execution of Warrior Ca Month
FRAGa 40 OPORD 5-Nov-08 Provides updated guidance to RMCs on the Army Warrior Healthcare Covenant 07middot55
FRAGO 41 OPORD 2oNov-08 Provides updated guidance to RMCs on the assJsJnment and use of special 07middot55 Defense Enrollment Eligibility Reporting System (DEERS) enrollment codes
known as Health Cara Delivery Program (HCDP) Plan Coverage codea In order to more efficiently ~nage the Wounded iii and Injured (WD) population
ProvIdes Initial guidance loRMCs on the required support to the DOD directed - Army Wounded wantOr Program (AW2) Recowry Care CoOrdination (RCC)
Prognun bnplementatlon plan
FOR OFFICiAl USE ONLY This document contains Infonnaflon DEEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemplen 5
Dissemination Is prohibited exeept as autherized by AR 20-1
A-14
FRAGa 42 OPORD Dfeb-09 Provide updated guidance to RMCs on the wru OIP Including the WTU OlP 07-55 FYDt Site VIsit Schedule and regional support requirements In order to facilitate
continuous opendionallmprovements vandate WT program compliance With unifonn standards and to both identify and share best practices among WTUs
FRAGO 43 OPORD 6-Mar(19 ProvIde initial guidance to the AMEDDCampS and HPU on the requlmment to 07s5 update ICCntdH and award continuing education creditS for the MEB Physldans
CoU1$4
Provide Initial guidance to the AMEDDCampS and HPampS on the requirement to dlrYelop a one week resident course for WTU Prfmary Care Managers (PCM)
Provide updated guidance to all RMCs In order to report status on phase I II IU amprv mebtce
Provide updated guidance 10 all RMC8 referance the W1U Cedill Resident Course to be conducted by the AMEODCampS
Provide Inillal guidance to all RIles In reteJ8nce to 0 reqllll1lment to perronn Independent and Impartfal nrvlew of I SoldIers MEB ftndings or narratlw summary when such a review Is requested
Provide Inillal guidance to RMCs reference the DoD ComputerlElectronic Accommodations Program (CAP)
FRAGO 44OPORD 12-Mar-09 Deletes Updated GuIdance on the wru OfP Checklist Erroneously identified In OT-55 Annex K to FRAGO 43
FRAGO 4S OPORD 2T-Apr()9 adCcrn implementation of the ANAP - WTU right-sizing develops 07-amp5 comprahenslve plan to accou~ for WTs and caregivers W1U cadre and GoV1
Equip_ closures and rualignments FRAGO 48 OPORD 2O-May09 RC soldlenl wm move closer to home of record to heal transfers between WTU 07middot$5 and CBWnJ Transition Review Board
As a result of the magnitude of issued guidance the Inspection team noted that individualWTUs execute the guidance in vastly different ways Some leadership teams perceive the guidance as non-prescriptive and open-ended For instance the Consolidated GuIdance issued In late 2007 prescribed that the Triad of Leadership establish a process to review active component Soldiers against the WTU eligibility criteria before determining disposition The DAIG team observed several installations using a review panel to evaluate Soldiers for WTU entry eligibility but the panels aiffered on composition candidate selection and unit notification procedures for Soldiers who were not accepted into the WTU This is just one example of how the enormity of the guidance has caused the lack of standardization across the Army_ In addiUonto a lack of standardization there is conflict between policies In one instance leaders were confused by the fact that a policy Which called for additional support requirements for Warriors in Transition was seemingly in conflict with another policy issued by a different command that required personnel reductions in the upComing years_ Although the Army attempted to field policy guidance via collaborative efforts the unsynchronized issuance of guidance directly impacted the accomplishment of the WTU mission
The Warrior Transition Command began an effort to consoHdate operational requirements into a Field Manuel (FM) for use by all units as a standardizing document however this publication DRAFT FM 4XX- is still ongoing by OTSGIMEDCOM
FOR OFRCIAl USE ONLY This dOCtlment contains lllfollllation EXEMPT FROM MANDATORY DISGU)SURE under the FOIA Exemptieft 5
A-15
Dissemillation Is pmhibltOO eeept as atJthefied 11) AR 29-1
i
RECOMMENDATIONS
a OTSGIMEDCOM Publish a single synchroniZed document to govem the Warrior Care and Transition Program Warrior Transition Command is developing asingle source manual for Warrior Care and Transition Plan
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
STANDARDS NA
FOR OFFICIAL USE ONLY This document colltalns ilifoulistioll EXEMPTFROMMANOAVORY DISClOSURE UAder the FOIA Exemption 6
A-16
(
Dissemination is prohibited mept as auIIefizeEi by AR 29-1
OBSERVATION 12 Warrior Transition Units (WTU) foster I focused environment of healing and transitioning however some WTs abuse the system and manipulate it to maximize entitlements
DISCUSSION Most (720 of 786) WarTiors in Transition (WT) interviewed active and reserve component stated that the Warrior Transition Unit (WTU)lCommunity Based WTU (CBWTU) Is the Ideal organization for them to heal and transition The majority of these WTs are on track with their middotComprehenslve Transition Plan (CTP) yet some cadre and WTs strongly believe that some WTs are not focused on healing or transitioning Rather they are attempting to lengthen their stay in the wru because they have become accustomed to the Armys excellent services and support found In the WTUs above what they wOuld receive in their units or out of the Anny for example with the Veterans Administration At every installation visited cadre made statements in reference to some WTs abusing the system and manipulating it tomiddot maximize entitlements Based upon their observations they expressed frustration with the WTs ability to prolong their length of stay by sequentially bringing forth new medical issues
The inspection team noted a ~ense of entitlemenr among some Warriors in Transition Various programs regulations and poliCies entice Soldiers into a mindset to achieve personal gains The personal motivations to extend length of stay (LOS) may be financial career transition based anxiety or a less than ideal family environment During our interviews we leamed that some WTs are not only seeking to benefit from the system but also to delay the evaluation board process by bringing up additional iIInesseslinjuries at key points during the evaluation process
Once Soldiers enter the WTU they gain access to perks and entitlements that are not available to Soldiers that are not In a WTU Examples include full time education options internship programs and services provided by the Soldier Family Assistance Center (SFAC) These perks and entitlements appear to lead to an actual ormiddot perceived heightened sense of status which is reinforced by senior militarycivilian leaders involvement in WTs concernslissues With the status of Wrt a Soldier has the ability to gain a Top Secret clearance in 45 days when tethered to an intemship Is a notable example These factors may entice some WTslnto a Dmindser of -Im in no hurry to leave
Some WTs also leverage financial inCentives and career concerns to maximize length of stay in the WTU For example WTs attached as opposed to assigned to a WTU allows financial benefits such as combat pay (or other special pays) per diem Basic Allowance for Housing (BAH) and Family Separation Allowance (FSA) to be continued When per diem and BAH based upon the WTs home of recordduty assignment are factored into the equation the financial benefits become prominent and lucrative
FOR OFFICIAL USE ONLY This document coillaillS infolillatiOJl EXEMPT FROM MANDATORY DISOlOSURE tinder the rolA Exemption 5
Diesemlnation Is prohibited exeept as autheltHd by AR 29-1
Additionally some WTs were concerned that they would not be able to return to their previously held civilian occupations due to their military wounds or Injuries and wanted to stay in the WTU until the Army fixed them Although It Is understandable that a Soldier would want to be healthy enough to return to his previously held career it is an unrealistic expectation in some cases that he or she would be able to do so The Army stand~rds for medical fitness for dutY are contained within AR 40-501 and may not match the fitness standards for civilian career fields
Another example of desiring to prolong the stay in a WTU Is the fear of losing health benefits for family members While on active duty all Soldiers and ~ir family members are entitled to health care If eligible the veteran and his family receive benefits from Veterans Administration Some WTs expressed fear of this transition This fear creates a desire to prolong their stay In the WTU
Anotherfactor InfluencingSoldiers motivations is the ubiquitous barracks lawyer A barracks lawyer is another Soldier that has been In the system longer and is perceived by other Soldiers to know more He or she either for nefarious reasons or by genuine concern becomes an adjunct chain of command offering advice to new arrivals into the WTU The majority (237 of 418) cadre members interviewed reqgtgnized this as a serious influencern motivations citing that new anivals often come Into the system motivated to return to duty as soon as possible But after a few months of talking to other WTs change their minds and start to seek ways to prolong their stay and maximize their benefits
Further lengthening the stay of a WT in a WTU is the Medical Evaluation Board (ME B) process and Physical Evaluation Board (PEB) process The MEB is used by the Army to determine medical retention in the Army AR 635-40 chapter 4-10 provides the following
The ~edcalievaluati~n boards (MEB) are convened to document a Soldiers medical status and duty limitations insofar as duty is affected by the Soldiers status A decision is made as to the Soldiers medical qualification for retention based on the criteria in AR 40-501 chapter 3 If the MEB determines the Soldier does not meet retention standards the board will recommend retenal of the Soldier to a PEB [Physical Evaluation Board] For MEBs rUles for documentation recommendations and disposition of the evaluated Soldier See AR40-400 chapter 7
Chapter 4-17 of the same regulation provides the following for PEBs
a Purpose The PEBs are established to evaluate an cases of physl~1 disability equitably for the Soldier and the Army The PEB is not a statutory board Its findings and recomm~ndatlons may be revised It Is a fael-finding board for the following
FOR OFFICIAL USE ONLY This document contains illforlatloll
EXEMPT FROM MANDATORY DISClOSURE tlnder the rOIA Exemption S
A-18
Di9semmstie Is pl8t1ibited exsept as a~oriied by AR 29 1
(1) Investigating the nature cause degree of severity and probable pennanency of the disability of Soldiers whose cases are referred to the board (2) Evaluating the physical condition of the Soldier against the physical requirements of the Soldiers particular office grade rank or rating (3) Providing a full and fair hearing for the Soldier as required by under Title 10 United States Section 1214 (10 USC 1214) (4) Making findings and recommendations required by law to establish the eligibility of a Soldier to be separated or retired because of physical diSability (10 USC 61)
During the process of these boards it is in the Soldiers personal financial interest to ensure that all diagnoses for any ailment are noted for compensation A majority (237 of 418) cadre and case managers said that when some WTs are informed that they will enter the MEB process their mlndset shifts from healing to maximizing disabilities to achieve personal gains (-higher disability rating and social security benefrts) In addition while undergoing this process the WT remains on active duty continuing pay and benefits throughout
The Warrior Care and Transition program Is intended for healing and transition The majority of WTs are on track with the intended purpose of Warrior Care and Transition Program Some WTs are exploiting the intent of the program and are focused on maximizing their entitlements
RECOMMENDATION
OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers retuming to duty ahead of disability-based compensation
STANDARD OTSGMEDCOM Policy Memo 09-011 nComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY This documellt coutaills iurau uation DeMPT FROM MANDATORY DISCLOSURE IAlier the FOIA ampemptieR 6
A-19
Dissemlnatian is pmhibited 8KCept as autherleEi by AR 29 1
OBSERVATION 13 A mixture of combat wounded injured and ill Soldiers in the Warrior Transition Unit has craated perceptions leading to leadership medical management public relations and small unit cohesion challenges
DISCUSSIONmiddot The Wanior Care and Transition program is not just for Soldiers wounded in combat but for all Soldiers with wounds injuries or illnesses EXORD 118-07 HEALING WARRIORS paragraph 3 provides the intent of the program ~It is imperative that the Army provides a continuum of integrated care and services from point of injury illness or disease to return to duty or transition from active duty The Army owes Waniors and their families a quality of care and services that is cOmmensurate with the sacrifices they provide to the Nation
The title of EXORD 118-07 Healing Warriors leads many observers to conclude that all Soldiers cared for within the program were wounded in combat In actuality according to MEDCOM statistics only 10 of Soldiers in the program were physically wounded in combat operations The remainder of the WCTP population includes Soldiers evacuated from combat theaters for diseases or non-battle injuries (37) preshyand post~mobilization Soldiers (20) and Soldiers referred by their commands for various reasons (33) The mispereeption that all Soldiers in the WCTP are wounded waniors leads to leadership medical management public relations and small unit cohesion challenges (Warrior Transition Status PAampE OTSG 21 January 2010)
When interviewed some WTs and cadre stated that they have come to the realization that all WTs are considered battle-injured As a result WTs have subsequently begun creating an informal caste system amongst them that distinguishes the battle-injured and non-battle-injured The caste system appeared to be tiered with the battle-injured Purple Heart recipients at the tOPt followed by the combat~xperienced ill WTs nonshycombat experienced WTs not considered seriously ill or injured followed by all others Both WTs and cadre expressed strong opinions regarding Soldiers who were not seriously injured gaining entrance into the WTU and reaping the benefrts of the WT status Senior level leadership share a similar concem as noted in an excerpt from a recent article written by David Wood published on July 52010 Afghanistan Joumal
Thousands of Soldiers Unfit For War Duty Mixing combat-wounded soldiers with these others has created some tensions Pentagon officials said Another Intemal Pentagon report said that combatshywounded [patients] express concern that they may be associated with those [patients] who stay for long periods of time and milk the system for benefits
To alleviate such concems the WalTior Transition Unit at Fort Hood Texas has built separatefacifities for combat-wounded soldiers BG Cheeks remark regarding Fort Hoods action was that he was kind or in favor of keeping a clear distinction between combat-wounded and the others Because what fdont want to have and what I have had is a guy with acid reflux disease going to ring
FOR OFFiCIAl USE ONLY This document contains om elioll EXEMPT FROM MANDATORY DISClOSURE under the FOIA Exemptio 5
A-20
Dis88miatien is pmhiblte(f elUlept as aliJthellied by~ 20-1
the bell at the opening of the NeW York Stock Exchange and portraying himself to America as a wounded warrior
This article highlights the challenges faced by senior Army leaders regarding public relations If the general public and national Congressional leaders perceive that aU Soldiers in the WCTP are wounded warnorsD then any media stories that inform the public of the Army taking adverse action against a Soldier for non--compliance with Army regulations and standards is viewed negatively against the Army
All Soldiers regardless of wounds Illnesses or injuries are held to standards of behavior and the Uniform Code of Military Justice (UCMJ) Commanders of Warrior Transition Units are charged with ensuring the above stated intent of EXORD 11 amp-07 is achieved while simultaneously upholding the good order and discipline of the SOldiers within their command Intemat and extemal influences (Congress Senior Defense leaders Command Structures and Media) can be disruptive to WTU operations and may hinder the effectiveness of command and control (C2) During interviews some cadre and senior leaders overtly or tactfully made strong reference to the fact that they felt as if they have little or no top cover WTU cadre land senior leaders have the perception that WTs have easy access to military and civman senior officials in order to voice concems Similar channels are not readily apparent and available to Soldiers in the operational forces Leaders share the belief that this allows the NTs in some cases to bypass the chain of commandlNCO support channel with little to no repercussions This factor coupled with the frustration expressed with the disruptive nature of the military and congressional visits and inquiries was consistent during our interviews The wru population as a whole is low density when compared to the balance of the forces yet the high visibility It gamers is due to everyone wanting to do the right thing for Americas Soldiers
Medical managers (nurse case managers and primary care physicians) reported challenges as wetl Most (210 of 249) health care providers interviewed were concerned that many WTs are provided additional medical care unrelated to health reasons that brought them into the WTU All WTs are provided enhanced access to care standards They are sent to the arront of the lineD for initial medical appointments within Anny Medical Treatment Facility (MTF) and have a better chance in securing quick follow-on appointments As WTs meet with providers for these initial and followshyon aPPOintments additional medical issues are broughtuplidentifled which may be unrelated to the primary medical condition These additional and unantiCipated medical concerns consume additional medical resources As some leaders noted if WTs are at the front of the lineD for barracks and healthcare appointments then someone else Is disadvantaged
FOR OFFICtAto USE ONLY This document contains illfQlmslioll EXEMPT FROMMANOAlORY 0I8GLOSURE ttflder he FOIA Exemption 5
A-21
Oi9gemination is prohibited ~ as aidAerimd b) AR 29-1
RECOMMENDATION
OTSGMEDCOM Detennine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
STANDARD NA
FOR OFFICIAL USE ONLY This document contains illfonnation EXEMPT FROM MANDATORY DlSGLOSURE Ufldar h FOIA ampemptien 6
A-22
Oissemillatlofl 19 Jlmhl9iteEi exeept as authefiieG by AR 20 1
OBSERVATION 14 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
DISCUSSION The vision for the Warrior Transition Unit (WTU) is to develop an effective organization that takes care of Warriors in Transition (WT) so they can focus on their mission to heal Immediate goals are providinghigh-quality living conditions and world class health care Ultimately these goals established the conditions that facilitated WTs healing processes physically mentally and spiritually The results of these efforts prevent unnecessary procedural delays and establish conditions that facilitat~ their healing processes
In an effort to provide WTs the highest standards of IMng the Army has committed itself to construct and operate several WTU complexes This action involves constructing new facilities to accommodate the WTs and Soldier and Family Assistance Center (SFAC) These facilities assist WTs housed at the WTU and those residing off post The Army has budgeted $12 billion to construct nine WTU community-based complexes
In a statement by the Secretary and the Chief of Staff of the Army before the House Appropriations Subcommittee on Defense for Fiscal Year 2011 both Army Officials confirmed the Armys commitment to construct -healing environments for the Wounded III and Injured Soldiers (WII) Specifically the Army in Fiscal Year 2011 is budgeting $900 million to continue to operate the 29 WTUs based at Army facilities camps posts and stations and nine Community Based Warrior Transition Units (CBWTUs)
A year of execution funding surge is necessary Some WTU policy changes and updates have been fielded without having been previously submitted through the Program Objective Memorandum (POM) process Most WTUs and installations are currently supporting themselves with local resources which mayor may not be available Some leadership Interviewed stated the follOwing was occurring at installations as a result of demonstrating policy implemented without adequate WTU resourcing
bull A majority of Warrior Transition Units reported their facilities were inadequate to support the mission (enduring verses non-enduring) Non-endunng programs are scheduled to be closed in the future For example Fort Meade MD is nonshyenduring WTU program which is not programmed for resourcing (personnel equipment supplies and facilities) in the out years However Fort Meades WTU continues to receive additional WT Other examples of this are happening In the Massachusetts and Virginia CBWTUs
bull Majority of nurse case managers (NCM) interviewed stated that current office space is inadequate (sharing space with other NCMs (Health Insurance Portability and Accountability Act (HIPM) compliance) separated from WTU and
FOR OFFICIAl USE ONLY This documelltcolltains Infollilation EXEMPT FROM MANDATORY DISCLOSURE UFlderlle FOlA EemptieA 5
A-23
Dissemination is prohibited ueept as atftheflaEj ampy AR 29 1
Physical Evaluation Board Liaison Officer (PEBLOraquo) and possibly unsafe (no panic button and rear exit)
bull The CBWTU Behavioral Health contract employees travel expenses are not included in the contract to enable travel to care for high risk WTs
bull ACS serves a joint community without joint resources
Majority of all leadership teams interviewed stated it was critical that the Army provide simultaneous funding and implementation guidance for all new and future WTU programs and policies
RECOMMENDATION
OTSGIMEDCOM ICW ASA(FMampC) and IMCOM Ensure a cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy req uirements
STANDARD NlA
FOR OFRCIAL USE ONLY This dOCtlment COIItaill$ infOrTuatioli EXEMPT FROM MANDATORY DISCLOSURE under the rOIA Exemllion 5
Di$SCmifletion Is pibited ueept BalMheffmd by AR 20-1
OBSERVATION 15 Subordinate commanders and some healthcare providers consider FRAGO 3f4middotWTU entrance criteria to be vague and inconsistently applied
DISCUSSION The intent of Fragmentary Order (FRAGO) 314 to Execution Order Healing Warriors was to provide prescriptive guidance and clarity on indentifying screening referring and managing Wounded III and Injured Soldiers (WII) Soldiers for both active duty (COMPO 1) and National Guard (COMPO 2) and Army Reserve (COMPO 3) for assignment to Warrior Transition Unit (WTU) The inspection team found that FRAGO 34 vague and Inconsistently applied
FRAGO 3 revised entry and exit criteria for assignmentattachment of Soldiers to a WTU who meet the following requiring complex medical case management Soldier with temporary profile or is antiCipated to recetve a profile for more than 6 months with duty limitations that preclude the Soldier from training for or contributing to unit mission accomplishment the acuity of the wound illness or injury requires clinical case management to ensure appropriate timely and effective utilization and access to healthcare services to support healing and rehabilitation
FRAGO 4 provided clarity on COMPO 2J3 Soldiers assignedattached to Warrior Transition Unit or Community Based Warrior Transition Unit (CBWTU) requiring definitive healthcare Additionally FRAGa 4 provided entry criteria requirements for senior graders Soldiers entry to WTU
However FRAGO 314 failed to define complex medical case managemenr and definitive healthcare which resulted in inconsistent application by leaders This interpretation resulted in ineligible Soldiers entry into WTU
In both FRAGOs the guidance is vague and not cleariy defined FRAGO 3s entry criteria are inconsistently applied from installation to installation For instance not all s(lnior commanders partiCipated in the entry process of a WT candidate into the WTU FRAGO 4 guidance for COMPO 213 focuses on the phases of deployment and the type orders Issued that the WT will fall under therefore allowing COMPO 213 Soldiers entry Into the WTU regardless of the definittve healthcare requirements of their medical condHlon The majority (70 of 106)commanders and senior NCOs interviewed in all COMPOs stated that the entry criterion was unclear and very subJective
The inspection team observed several WTUs using a reviewing panel veraus the Triad of Leadership to ev~luate COMPO 1 Soldiers for eligibility leading to different
interpretations of the reyjeYi process and the panel composition Local poliCies set different requirements for nomination and acceptance into the program which has allowed for an increase ofroutineJnon complex cases gaining admittance into the WTU These routineJnon-complex cases have a direct impact on medical resources available to care for complex and seriouslyseverely wounded ill and Injured (WII) Soldiers
FOR OFFICIAL USEmiddot ONLY This documeiltconlains information EXEMPT FROM MA-NeAleRyen DISCLOSURE tftIder the FOIA Exemption S
Amiddot25
Diasemletion is prehibltsd exeept 89 etflherized by AR 20 1
The inspection team also found Warrior Screening Matrix for WTU Appendix 3 Annex B FRAGO 3 DAEXORD 118-07 (Healing Warriors) to be imprecise subjective and inconsistently applied across several WTU locations The Wan10r Screening Matrix for WTU consideration (assignmentattachment) addresses the potential risk factor and does not consider the medical conditions -that have been identified as pre-existing incurred or aggravated by military service
FRAGO 4 attempted to clarify entry criteria for COMPO 23 Soldiers for entry into a WTUCBWTU FRAGO 4 expands on the types of orders to retainreturn to active duty status for the screening and evaluation process but does not expound on specific evaluation aiteria for entry Additionally FRAGO 4 does not spell out who is responsible for conducting thes~enirig and eValuation for those RC Soldiers that are considered for entry into the WTU
Majority of those interviewees stated that WTU entry criteria must be cleariy defined to prevent different interpretations Clarity of FRAGO 34 ensures only those Soldiers meeting entry criteria are admitted -into WTU resulting in fewer WTs
RECOMMENDATIONS
a OTSGIMEDCOM Define complex medical care extensive and clinical case management definitive healthcare and standardize screening criteria for entry Into the WTU to address medical condition for all COMPOs OTSG is cummtly staffing EXORD that establishes a MEB referral formal reporting system and a General Officer requirement to approve treatment plans for WTUICBWTU WTs with a length of stay greater than 12-months without MEB start date
b ASA(MampRAG1 Consolidate Medical Retention Processing Evaluation (MRP-E) Medical Retention Processing (MRP) Medical ~etention Processing 2 (MRP2) and Active Duty Medical Extension (ADME) into one order similar to COMPO 1
STANDARDS FRAGO 314 to EXORD 118-07 (HEALING WAR~IORS)
FOR OfFICIAL USE ONLY This docilment contains information EXpoundMPT FROM MANDATORY DISCLOSURE Uflder the FOIA Exemptlen 5
A-26
DlesemiAatieFl Is pFElhibited elapt 8S etlthorized by AR 20-1 bull
OBSERVATlON16 MEDCOMs accountability processes for Soldiers evacuated outof theater result in immediate acceptance into the WTU without meeting FRAGO 3 screening criteria
DISCUSSION During the Inspection teams site visits to 17 installations and after interviewing Command and Control (C2) and Medical Management (M2) staffs the teams assessment revealed the Deployed Warrior Medical Management Center (DWMMC) is attaching Soldiers who may not meet entry criteria lAW FRAGO 3 and 4 directly to the wtu Soldiers not meeting eligibilitycriteria should remain in their parent units to receive required care
)
According to the DWMMC Fact Sheet (July 2009 the DWMMC is responsible for the expedient coordination of patient movement and medical care for alFservice members andcMllans who become wounded III or Injured (WI) while serving in support of Operation Enduring Freedom and Operation Iraqi Freedom The DWMMC is led by a US Navy physician and Is staffed by 40 deployed active duty Reserve Sailors 15 civilians and six active duty Soldiers
The traditional Medical Hplding Company was used as the model for the initial development of the DWMMC a non-doctrinal organization In response to new logistical and operation process challenges that arose with the Global War on Terrorism such as the related increase in patient volume multiple teams and sections - celis - were developed Each cell had a unique set of tasks bUt all those tasks were interrelated The need to streamline and improve patient movement led to these
groups being brought together underthe organization that came to be known as the DWMMC The DWMMC was officially established In October 2001 coincident with the beginning of OEF
Soldiers of all components requiring inpatient care greater than 30 days or outpatient recovery greater than 60 days are medical evacuation (MEDEVAC) from theater with
initial movement to an Army Medical TreatmenfFacility (MTF) with capability and capacity closest to the location of patient preference unless the requested facility does not have the capability to care for Soldiers injuries Upon arrival to the WTU a clinical evaluation will be Initiated WTUs will assign a case manager by name for each patient upon arrival
Currentiythe DWMMC utilizes the procedures outlined in OTSGMEDCOM Polley Memo 08-015 apatient Movement from Outside Continental United States and Reception of Warriors in Transition to Military Treatment Facilitie~ dated 13 May 2008 when determining a patienfs final disposition eg retum to duty down range or MEDEVAC to CONUS MTF Paragraph 4p (10) of the above policy requires all Soldiers who arrive at aMTF to be attached to the supported WTU within 24 hours of arrival AR 40-400 chapter8 paragraph 1(e) requires attachment to WTU within24 hours for all Soldiers who report to the MTF for medical evaluation or treatment from off-installation locatons
FOR OFnClAl USE ONLY This document contains information EXEMPT FROM MANDATORY DISGLOSUREtmaer the FOIA EMmpUof fj
Amiddot27
DissemiftatiaA is prehibited eKeept as authorized by AR 20 1
DWMMC is executing OTSGMEDCOM Policy Memo 08-015 however the unintended consequences of the execution of this policy are a few Soldiers that are MEDEVACd gain entry into WTU without meeting the entry criteria lAW FRAGO 3 amp 4 This adds stress and strain on the support and services provided by the WTU Of the 17 WrUlCBWTU units visited 11 of 17 exceeded the C2IM2 to WT ratio as defined in FRAGO 3 to Operations Order 118-07 Annex D Most wrs interviewed perceived that both C2 amp M2 staffs are overburdened with daily administrative duties which slow their
healing and transition process Additionally the WTs stated that the time spent with health care providers was not adequate
As a result of implemented OTSGIMEDCOM Policy Memo 08-015 which directs automatic attachment to the WTU theTriad of Leadership and Triad of Care are removed from the recommendation process when a Soldier Is medically evacuated from theater
The current implementation of OTSGIMEDCOM Policy Memo 08-015 continues to overload an already stressed WTU C2 amp M2 support staff that atmost Installations visited exceeds established approved Army ratios Most C2lM2 staff interviewed stated OTSGMEDCOM Policy Memo 08-015 has allowed Soldiers access into the WTU that should have remained assigned to their rear detachment for out-patient treatment and rehab ilitation
RECOMMENDAnON
OTSGMEDCOM Develop a standardized process to evaluate Soldiers evacuated from theater to determine IT they meet WTU entrance criteria
STANDARDS FRAGO 34 to EXORD 118-07 (HEALING WARRIORS) OTSGIMEDCOM Policy Memo 08-015
FOR OFFICIAL USE ONLY This dOCJlTl8llt oomains infermali8n EXEMPT FROM MANDATORY DISCLOSURE ullder Hie FOtA Exelliption 5
A-28
Dissemination is pmhibited exeElJ3l as authorized by AR 2Q 1
OBSERVATION 17 Most WTU cadres are concerned with Inconsistencies in detennlning the Medical Retention Decision Point (MRDP)
DISCUSSION OTSGMEOCO~ Policy Memo 09-037 Medical Evaluation Board MEB Processing Guidance definesthe Medical Retention Decision Point as
a service member with one or more condition(s) failing to meet medical
retention standards will be referred into the Disability Evaluation System (DES) by competent medical authority at the point of hospitalization or treatment when the memberS progress appears to have medically stabilized the course of further recovery is relatively predictable and where it can be reasonably determined that further treatment wilt not cause the member to meet medical retention standards or render them capable of performing the duties required by their office grade rank or rating This medical retention determination point will be made within one year of being diagnosed with a medical conditions) that does not appear to meet medical retention standards but may be earlier ff the examiner determines that the member will not be capable of retuming to duty within one year
The time it takes the medical community to reacha decision affects when a Soldier is to return to duty (RTO) is released from active duty (REFRAO COMPO 213) or referred to a MEB and subsequently the Physical Evaluation Board (PEB)
leadership teams at most sites visited indicated there are inconsistencies in the execution of the medical retention decision point (MROP) resulting in evaluations for conditions that were beyond the scope of initial WTU entry~ During our visits the inspection team found Soldiers were Initially attached to the WTU for a condition that did not meet the WTUentry criteria However once a Soldier is attached to the WTU heshe is assigned a case manager and a complete systems review is conducted which includes the establishment of the Soldiers master problem list The establishment of the Soldiers master problem list is often when a Soldier will bring forth other medical conditions outside of those that inHially caused the Soldiers to be admitted into the WTU
Physicians must implement treatment plans that optimize medical benefit In order to allow Soldiers to RTD as quickly as possible In 2007 the Optimal Medical Benefit (OMS) was initially defined as
the point during hospitalization or outpatient medical treatment when a SoldierS progress appears to have medically stabilized If return to duty is not possible following an optimal treatment plan the physician must render a decision as early as possible on the need for a penn anent profile and referral to a Military Occupational Specialty (MOS) Medical Retention Board (MMRS) or Medical Evaluation Soard (MES)
FOR OFFICIAl USE ONLY This dOCtlment contail IS illforma60n EXEMPT FROM MANDATORY DISCLOSURE JAder the FOIA ampemHiaA S
A-29
DissemiAatiofl Is pl8t1illited eeept as alllhe~ byAR 20middot1
Deciding when OMB has been reached is difficult This has been interpreted differently by providers Soldiers and legal counsel These varying interpretations have historically Contributed to untimely MEB referrals Also failure to adequately describe the
determinants of the OMS when preparing the MEB Narrative Summary may result in the Physical Evaluation Board (PEB) returning the MEB for clarification or additional clinical care or evaluation Due to difficulty in determining the OMB the Army uses MRDP with the intent to RTD as quickly as possible
Most (195 of 249) healthcare providers perceive the Primary Care Manager (PCM) is reluctant to exercise the MRDP due to lack of clarity regarding elective conditions tendency to view the Soldierpatient holistically and lack of top cover on previous decisions In addition to the above definitions some contributing factors adding to the confusion of when to use MRDP are
bull Drug dependency and addiction (approximated between 25-35 or higher of wr population (based on interviews with health care providers see TAB E Observation 5)
bull Timely access to behavioral healthspecialty appointments delays evaluations and treatment causing further delays to MRDP
bull Lack of accurate processes to identify and stabilize Behavioral Health ~iagnosis issues
bull Missed appointments (one WTU as high as 20 no show rate for appointments) bull No standardized eiective proceduresurgery policy (some WTUs have written a
local policy) DPre-existing conditions not identified prior to mobilization or deployment bull Natali conditions are identified in the Soldiers electronic medical record (AHLTA)
The consensus from the majority of Command and Control (C2) and Medical Management (M2) staff Interviewed is there is a great need for the Army to clearly define the processes and procedures in the effective execution of the Medical Retention Decision Point (MRDP) Failing to clarify the MRDP will continue to add to an already large population of WTs
RECOMMENDATIONS
a OTSGIMEDCOM Redefine the MRDP to be more clear concise and proscriptive develop a standardized metric for assessing the MROP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP OTSGis currentfy staffing EXORD that establishes a MEB referral formal reporting system andmiddot a General Officer requirement to approve treatment plans for WTUCBWTU WTs with a length of stay greater than 12-months without MEB start date
FOR OFRCIAL USE ONLY llds doctlmellt contains btformation
EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemptiaft6
A-30
Oisseminefil is prettiblted exest S9 sIthorized hy AR 29 1
lt
b OTSGlMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGlMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 3
FOR OFFICiAL USE ONLY This doctlment cOntains Information EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA Exemption 5
Dissemination is prohibited Heef)t as autherized b) M 29 1
OBSERVATION 18 Selection ofWTU Cadre shifted from best qualified to good and first available
DISCUSSION ALARACT 21012009 Warrior Transition Unit Personnel ASSignment and utilization Policy provides guidance to force providers and senior commanders for nomination selection approval and assignment of cadre However according to leaders cadre and staff interviewed there needs to be a more effective tool to assess
Soldiers for leadership positions Within the wrus complex environment On several occasions we were informed that the best qualified person is often the firstmost available Also during numerous interviews with WTU cadre and leadership the majority stated that evaluation reports and past performance are not enough to go by when selecting S91diers to fill key positions such as squad leader and platoon sergeant Recruiters and Drill Sergeants require a command recommendation background check and mental health assessment prior to assignment Leaders Interviewed agreed this would be helpful in selecting potential wru cadre members due to the fact Ihat some senior leaders have had to replace cadre due to their inability to perform lead and manage Soldiers within the WTU Consensus by Ihe majority interview~stated that along with a command recommendation background check and mental health assessment Soldiers desiring duties as WTU cadre need to be counseled on the complexities and uniqueness of the job they are seeking to enter
Additionally there are factors that may not be conducive to attracting the best candidates For example Recruiters and Orin Sergeants are rewarded for successful tours by receiving favorable consideration during the centralized promotion board process AlthoughWTU cadre positions are difficuH and challenging most cadremiddot interviewed particularly squad leaders perceived that assignment to a WTU is not career enhancing When queried as to how this belief came about many squad leaders stated that this was information provided to them by HQOA Assignment Managers and senior leaders Specifically the aSSignment was a take a kneew
assignment and not th~ equivalent to Drill Sergeants Recruiters or their peers in the operational forces We also heard this from a Command Sergeant Major and a Company Commander who stated they were informed by their branches that their current positions do not counf as command time therefore they are expected to assume similar level positions in the operational forces in order to have the leadership time counf
Most squad leaders (124 of 149) interviewed stated they lacked an established clear and concise job description Although some WTU senior enlisted advisors have established good job descriptions most have not Squad leaders and platoon sergeants perceived this could be critical to the low number of squad leaders selected for SFC by HQDA selection Poams
FOR OFFICIAl USE ONLY This dOOlment contains information BltpoundMPT FROM IMNDATORY DISCLOSURE tinder the FOIA Exemption 5
A-32
DissemiAatien Is f)R)hibited eept as autheact by AA 2Q 1
Active Component (AC) Soldiers are assigned to a cadre position for 2 years Reserve Component (RC) Soldiers have t~e op~ion for a 2 year Permanent Change of Station (PCS) or a temporary Change of Station (TCS) The overwhelming majority of ARNGUSAR Soldiers are mobilized as cadre for a period of one year Most cadre to include Senior Commanders and their CSMs expressed concem regarding the potential disruptive nature of this practice Many leaders and WTs believe that the organization asa whole benefits when there is continuity of care and leadership
Finally there is no established automated process to volunteer for WTU squad leader and platoon sergeant positions such as the Assignment Satisfaction Key (ASK) on the Human Resources Command (HRC) website This tool allows Soldiers to volunteer for special duty assignments such as Airborne Drill Sergeant and Recruiter The majority of commanders interviewed stated the Army should consider adding WTU squad leader amp platoon sergeant assignments to the HRC ASK module Adding these assignments will provide assignment managers a pool to select NCOs who desire assignment to the WTU
RECOMMENDA nONS
a ASA(MampRA)G1 ICW OTSGIMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Management AR 614-100 Officer
Assignment Policies Details and Transfers
b ASA(MampRA)lG1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
STAt~IDARD ALARACT 21012009 Wanior-Transition Unit Personnel Assignment and Utiliultion Policy
FOR OFFICIAL USE ONLY This documel It contains Infonnatlon DEEMPT FROM MANDATORY DISClOSURE under 1he FOil Exemption 5
A-33
Dlasemination is prohibited e_~ as eulheriiedby AR 20middot1
OBSERVATION 19 The current Wamor Transition Unit (WTU) classroom-centric and theory-based Instruction does not adequately prepare the cadre to perfonn their duties
DISCUSSION After interviewing over 208 WTUlCommunity-based WTU (CBWTU) platoon sergeants and squad leaders most (175 of 208) interviewed stated that the WTU Staff Training for Squad Leaders and Platoon Sergeants course does not adequately prepare them to perform their duties in this unique environment Platoon sergeants and squad leaders alike agreed that the course does provide them with valuable skills and knowledge to help them be successful during their tenure as cadre but it can be improved
The Warrior Transition Unit Staff Training for Squad Leaders and Platoon Sergeants course is conducted 8-10 times per year in San Antonio Texas with an annual student load of more than 700 The majority of Squad Leaders and Platoon Sergeant trained are coming from Military Occupational Specialties (MOS) with no foundation managing Soldiers with complex medical conditions Most (160 of 208) interviewed stated this course does a good job of using lecture demonstration some vignettes and discussion to teach the students However as the numbers of WTs with behavioral health (BH) issues such as traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) rise throughout the WTU population cadre members have expressed the heed for training that includes demonstration on how to deal with Soldiers with BH issues
Cadre members also expre~sed a need for training focused on managing high risk Soldiers Leaders and providers determine a Soldiers risk level by using a Warrior Screening Matrix The Soldier receIves a risk assessment by the Squad Leader (SL) NurSe Case Manager (NCM) Social Worker (SW) and the commander Managing a high risk WT or WT with BH issues can be challenging and sometimes overwhelming for the Inexperienced cadre members Cadre members stated they would like more scenario-based training and lessons learned to help them develop creative and effective ways to deal with Soldiers with these types of conditions Additionally sensitivity training needs to be added with follow on training at the units
WTU cadre expressed the need for additional training to learn the side effects of the various medicaijons prescribed to WTs Knowing which medications make Soldiers drowsy excited irritable or unstable would be beneficial in the management of WTs Platoon sergeants and squad leaders agreed some type of condensed medication smart bookwould be a good take away from the course
Physical training Is still a principal element of most WTs daily routine Cadre members requested more hands on training and not just demonstration when it comes to leaming Adaptive Physical Training Program that a WT can do based upon his or her medical
profile
FOR OFRCIAL USE ONLY This doctlment contains information EXEMPT FROM MANDATORY DISCLOSURE tRcer lIle FOIA EKemptiell 6
Disseminstie Is pralliBiteEI except as lMherized by AR 20 1
CBwrU cadre stated that there is not enough emphasis placed on CBWTU operations Knowing the course is already a full 80 hours a few CBWTU cadre members recommended additional time after regular training hours to discuss best practices resources and lessons learned when managing WTs that are as dispersed as the resources that may be needed to help manage them
Special Outy Assignment Pay (SOAP) is linked to the completion of the Wanior Staff Training Program WT cadre (squad leaders and platoon sergeants) are executing their mission one to three months without the additional pay Cadre attending the training enroute to their assignment could better prepare them for their duties ~nd responsibilities in the WTU Currently cadre members are sent to the course after assignment to the WTU Some squad leaders and platoon sergeants expressed concern that prior to assuming their position they are not able to work alongside their counterpart who they will be replacing Since the Reserve Components do not fill a platoon sergeant or squad leader slot until it is vacant this makes conducting a right seat left seat ride impoSSible As soon as the NCO hits the ground the Soldier is fully engaged learning on the job without any formal training
RECOMMENDATIONS
a OTSGIMEDCOM Implement training for cadre that is scenario-based deals with behavioral health issues side effects of prescription medications and includes sensitMty training
b OTSGIMEOCOM Require cadre training prior to assignment to WTU and implement sustainment training Consider use of computer based training for cadre sustainment training
c OTSGMEDCOM ReqlJire WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGIMEDCOM Provide a leaders guide to address Warrior in Transition p~cesses and policies
STANDARD NlA
FOR OFFiCiAL USE ONLY 1111 document COn1aiIiS informalion EXEMPT FROM MANDATORY DISOLOSURE IiAder the FOlA exemptien 6
A-35
Dissemination is prehibited except amp9 authefimd ~t AR 20 1
OBSERVA fION 110 Most WTUs visited are not meeting the intent and implementation of the Comprehensive Transition Plan (CTP)
DISCUSSION The Comprehensive Transition Plan (CTP) is the cornerstone indMdualized plan of action that guides the recovery of every Warrior In Transition It establishes expectations mixing the desires of the Soldier with the military and medical reality of the individual situation The CTP is mandated by OTSGMEDCOM Policy Memo 09-011 Comprehensive Transition Plan (CTP) Policy dated 10 Mar 09 In paragraph 2 the policy rea~s All Soldiers assigned or attached to a Warrior Transition Unit (WTU) will begin their comprehensive transition plan within the first 30 days of assignment The majority of WTs(442 of 786) stated that they cUd not have a written CTP These WTs further stated that they thought the CTP was just a check- of- theshyblock The inspection team discovered more seniorWTs (Senior NCOs and Officers) embraced CTP and used it as an effective planning tool for their future Of the Soldiers interviewed that had a CTP many expressed dissatisfaction The oft given reason was they did not abuy-in to the plan The junior WTs stated the CTP was ineffective and they only did one to keep their squad leaders off their backs Many expressed that the plan was not theirs to begin with and that th~ chain of command had Influenced decisions with regard to treatment and recovery
The CTP is a life-skill focused plan integrating activities to promote healing in a holistic manner It is interdisciplinary in nature outcome focused and deSigned to optimize function The CTP establishes accountability is goar oriented milestone driven and empowers WTs and Families to transition through the healing process It has four potential outcomes Retum to Dutymiddot(ActiVe Component only) Release from Active Duty (Reserve Component only) New Occupational Specialty Return to Active Duty and Separation from the Army The CTP has a logical progression with a focused end date The plan can and should be updated periodically to reflect condition changes as identified by medical personnel the Soldiers leadership team the Soldier and hislher Family The chain of command must provide accessible responsive and compaSSionate leadership to aid and advise the Soldier through the planning and execution of hislher plan The desired outCome is a Soldier continuing to serve or a Veteran retuming proudly to his community
When asked why so few WTs actually had completed CTPs leadership referred to the impending release and implementation of the automated Comprehensive Transition plan as the reason The expected date of implementation was given as 9 July 2010 (Warrior Transition Command has since implemented the automated version on the expected date of 9 July 2010)
The inspection team also noted that age and maturity of the indMdual WT played a role in plan development implementation and buy_ln More senior Soldiers nonshycommissioned officers and officers tended to grasp the concept behind goal setting
FOR OFFlCfAL USE ONLY This doctInl81lt contaillS infomJation EXEMPT FROM MANDATORY DISClOSURE tinder the FOrA Exemptieft 5
Dl9gemirlatioA is prohlllited except aa atdherized by AR 29-1
meeting milestones and seeking assistance as necessary more readily than did their junior counterparts One very troubling note made by the inspection team was that many CTPs reviewed tended to focus on disability versus ability with an approach towards disability compensation rather than working towards a retum to duty outcome
Overall the Warrior Care and Transition Program is not meeting the intent and Implementation guidance provided in OTSGIMEDCOM Policy Memo 09-011
RECOMMENDATION
OTSGMEDCOM provide policy and guidance to support automated CTP and enforcere-enforce the implementation and executiOn WTU started implementation of the automated CTP and have over 6000 WTs In the program with plan to have all WTs in the automated program in the next six months
STANDARDS OTSGIMEDCOM Policy Memo 09()11 middotComprehensive Transition Plan (CTP) Policy
FOR OFFICIAL USE ONLY nllsdocumsllt contains ilifolilistion EXEMPT FROM MANDATORY DISClOSURE under the FOIA empliell 5
A-37
Dlasemiltetiall is pmhibites exeept as akdheriled by AR 20 1
OBSERVATION 111 Most Warrior Transition Units (WTU) have not Implemented the Transition Review Board (TRB)
DISCUSSION The TRB facilitates communication to effectively manage Warrior in Transition (WT) in a complex medical environment Most (14 of 17) sites visited have not implemente~ the Transition Review Board (TRB) The few (3 of 15) commanders that implemented the TRB stated it is an effective board that incorporates the feedback from multiple disciplines to provide a recommendation to the commander
The TRB is a comprehensive administrative board with medical and command leadership which recommends if a WT should continue care within the program This multi-disciplinary panells purpose is to facilitate dialogue between the WT the Triad of Care the chain of command and other members of the WTs care team as appropriate regarding the Comprehensive Transition Plan (Crp bull strategy for WTs transition) In accordance with the Warrior care and Transition Program (WCrP) Policy memo 09-002 Warnor Transition Unit Transition Review Board Process the Triad of care will review the status of a WTs transition progress in order to validate the transition plan beyond 180 days The TRB is to be conducted no sooner than 180 days ~nd no later than 365 days upon a Soldiers entry Into the program with subsequent reviews by the Triad of care~in 90-day Intervals thereafter
The objective of the TRB is to provide one of three recommendations to the Triad of Leadership
bull Continued assignmentattachment to a WTU or CBWTU (including transfer from a WTU to aCBWTU if appropriate)
bull Retum to duty (RTD)lReleasefrom active duty (REFRAD)lExpiration Term of Service (ETS) as appropriate
bull Referral to a Medical Evaluation Board (MEB) Military Occupational Specialty (M~S)lMedlcai Retention Board (MMRB)
The TRB can be an effective commanders tool to manage wrs progress in WTU The inclusion of the multiple disciplines which impact a WTs treatment and transition allows helghte~d situational awareness of the WTs status This Interaction provides for more effective and efficient command and control and medical management of Soldiers in theprogram
RECOMMENDATIONS
a OTSGlMEDCOM Enforce tho Implementation of the TRB and consider conducting the TRB for everY WT at each 180 day period
FOR OffiCIAL USE ONLY This docullient contains Info illation EXEMPT FROM MANDATORY DlSGLOSURE tmder the FOIA ~ 5
A-36
Dlseemlnatiellls prehihited exeept as aulheFIieEI by AR 20 1
I
b OTSGMEDCOM ICW ASA(MampRA)G1 establish reporting requirements of TRB results
cOTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
STANDARD FRAGO 4 to Army EXORD 118-07 (HEALING WARRIORS)
FOR OFFICIAL USE ONLY This document contains lnfonnation EXEMPT FROM MANDATORY DISCLOSURE tin_the FOIAEKemptieA i
Dissemillation is prelIbited except as suthGr1fed by AR 29 1
OBSERVA orON 112 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapyandcontribute to delays in Soldiers treatment and healing
DISCUSSION The demand for behavioral health (BH) service has increased as more Soldiers are diagnosed with post traumatic stress disorder (PTSD) and traumatic brain injury (TBI) Most Warrior Transition Unit (WTU) cadre and Warriors in Transition (WT) stated speciatty care provider shortages contribute to delays in diagnosis and treatment and thereby increase length of stays With the shortage of specialty care providers military treatment facilities (MTF) refers Soldiers off installation to the TRICARE networK There have been numerous efforts to hire civilians as General Schedule (GS) employees or as contractors to help backfill deployed providers However there is a national shortage of BH providers and hiring efforts have middotbeen met with mixed success To meet its demands the Army hired additional behavioral specialists and is seeking to add more throughout its MTFs The challenges are that GS-Ievel salaries for specialty providers do not correspond with Industry norms (DODshywide)
Table of Distribution and Allowances (TDA) authorizes Occupational The~pists (On at battalions and above leaving the remaining 12 separate WTU companies without OTs OTs are a part of the Comprehensive Transition Plan (CTP) and assist WTs In developing goals in connection with the Triad of Care Their goal is to helpclients have independent productive al)d satisfying lives They help Soldiers improve their ability to pertonn tasks in living and working environments OTs worK with WTs who suffer from a mentally physically developmentally or emotionally disabling condition OTs use treatments to develop recover or maintain the daily living and work skills of their soldiers The therapist helps clients not only to improve their basic motor functions and reasoning abilities but also to compensate for pennanent loss of function Army OTs help optimize Soldier perform~nce and readiness in the field and garrison creating new and innovative applications but not all OT slots are filled on the WTU TDA
Physical Therapists (PT) are not on the WTU TOA MTFs continue to share their PT services between the WTU and hospital This creates delays in access and treatment for both the MTF patients and WTs Army PTs evaluate diagnoses treat WTs with neuromuscular skeletal injuries and optimize Soldier and unit readiness by enhancing functlonallhuman performance PTs serve as the command consultants in areas of injury prevention survelllance physical fitness readiness and health promotion to assist Soldiers transition
RECOMMENDATIONS
a Army G3517 ICW OTSGIMEDCOM validate manpower requirements criteria for healthcare services personnel
FOR OFFICIAL USE ONLY TIils document colltaifls iii formation EXEMPT FROM MAHOATORY DI88lOSURE tinder the FOIA Eqmptiofl 5
A-40
Dissemination Is plehibited except as atJthorfzed by AR 20 1
b ASA(MampRA)lG1 ICW G3I5fl and OTSGIMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRAG1 lew G3I5fl and OTSGMEDCOM confirm salary competitiveness among behaviora1 specialists
STANDARD NA
FOR OFRClALUSE ONLY Tllis dowm811f contains infolr18tion EXEMPT FROM MANDATORY DISCLOSURE tinder ihe FOIA Exemplioo 6
A-41
OIsseminaticn is pRItibitod axcept as atIthCIized b) AR 29-1
OBSERVATION 113 Anny Is failing to properly document Une of Duty (LOD) investigations for Reserve Component Soldiers critical to the follow-on care and transition for the RC Soldier
DISCUSSION All (17 of 17) installations visited had issues wit~ improperly conducted LODs for Army National GuardAnny Reserve Soldiers Most WTU Cadre and healthcare providers interviewed stated that RC WTs were transferred to WTUs with no or incomplete LODs (not in compliance with AR 600-8-4 Line of Duty Policy Procedures and Investigations 4 September 2008) AR 60Q8-4 requires LODs for all Anny National GuardAnny Reserve Soldiers serving on Active Duty for a period of more than thirty days and When an injury illness or disease was incurred or aggravated by duty requirements
Due to a lack of training and understanding on LODs a perception exists within the Active Duty (COMPO 1) that Anny National GuardArmy Reserve Soldiers on mobilization orders (Title 10) do not require an LOD COMPO 1 commanders are unfamiliar with the requirement of Initiating an LOD for Anny National GuardiAnny Reserve Soldiers under their charge
AR 600-8-4para 2~1 states Une of duty detenninations are essential for protecting the interest of both the individual concerned and the US Government where service is interrupted by injury disease or death Soldiers who are on active duty for a period of more than 30 days will not lose their entitlement to medical and dental care even if the injury or disease is found to have been incurred not in line of duty andor because of the Soldiers intentional misconduct or willful negligence Section 1074 Title 10 United States Code (10 USC 1074)
Anny National GuardlReserve Component Soldiers without a completed LOD investigation encounter difficulties obtaining medical treatment through the TRICARE and other non-Military Healthcare Systems once they are no longer In an Active Duty Status They have also experienced a loss of Familysurvivor benefits
An LOD investigation is used to determine whether Army National Guard (ARNG)Army Reserve (USAR) Soldiers aremiddotentitled to follow up medical care pay and allowances and placement on Active Duty Medical Extension (ADME) and Medical Retention Processing (MRP2) when they are injured or become III while In an authOrized duty status The substantiating facts gathered In the LOD investigation will also assist other government agencies such as the Department for Veterans Affairs and Social Security Administration in determining the Soldiers and their Familys entitlement to other benefrts
Both the ARNG and USAR have developed and implemented a web-based LOD Module application In the HQDA Medical Operational Data System (MODS) The Module provides an automated real-time management capability to prepare and
FOR OFFICIAL USE ONLY This document colltaills information EXEMPT FROM MANDATORY DISCLOSURE ttnder thtI FOIA ampemptieR 6
A-42
OEssemifletie is ~ted except as atlthori2ed b) AR 29 1
transmit LOD actions both CONUS and OCONUS Some keyhighlights to the LOD Module Jnclude
bull Common Access Card enabled bull Ability to scan and upload all medical documents in support of LOD bull Regional Military Medical Support Officers (MMSOs) can review authorize
follow-up medical care medical payments and forward the account to TRICARE for payment
bull Allows for electronic signature o Provides leaders and staff full visibility of the LOD process
LODs are essential for follow-on care for Army National GuardArmy Reserve Soldiers AU commanders must ensure the proper documentation of LODs for Army National GuardfArmy Reserve Soldiers in their charge The implications of improperly conducted LODs far exceed the time the Army National GuardArmy Reserve Soldiers spends on Trtle 10 orders and impacts future care of the Soldier and Family members survivors benefits
RECOMMENDATIONS
a~ ASAMampRA)lG1 Publish message to commanders emphasizing required completion of LOD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 ICW ARNG OCAR and T JAG ensure education and trainIng tools for LOD administrators are available to units prior to and during deployment
c ASA(MampRA)lG1 Determine feasibility of presumptive LOD for RC Soldiers on Title 10 active duty orders in support of Contingency Operations
d OTSGMEDCOM Adopt LOD module in MODS as the Armys dedicated line of duty tracking system
STANDARD AR 600-8-4 Personnel-Une of Duty Policy Procedures and Investigations U Chapters 1-2
FOR OFRClAl USE ONLY This doatment ~ntains Infoliilation EXEMPTFROMMANDATeRY DISClOSURE under the FOIA EMmptleA 6
A-43
OissemiRatioR is pmhibited ~pt aamplNlherimd by AR 20 1
OBSERVATION 114 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
DISCUSSION A perception exists among some (316 of 786) Waniors in Transition (WTs) interviewed stated that not all WTs are held to the same standards of discipline as Soldiers in a regular unit They also explained that more often than not its the non-combat wounded Soldiers with the most disciplinary issues Additionally WTs interviewed stated they witnessed WTs displaying disrespect towards noncommissioned officers disobeying direct orders or regUlations and abusing prescription medications and illegal drugs Interviewees further stated the WTs committing these offenses were being punished too leniently or not at all by WTU commanders due to their medical condition and status as a WT They also stated that this middottype of behaVior and lack of appropriate punishment is negatively affecting tlie morale and discipline of others in the unit
WTU platoon sergeants and squad leaders stated they sometimes feel the commander andor higher headquarters do not support them when recommending punishment for WTs for disciplinary problems or other unacceptable or illegal behavior Similarly some WTU commanders interviewed stated they did not always feel they had wrop cover from higher when trying to administer UCMJ punishment which they believed appropriate For example we talked to a WTU commander that attempted to chapter a wounded in combat Soldier out of the Army for illegal drug use but the punishment was reduced by the senior commander to loss of pay and rank It was not until the Soldier failed a second urinalysis that the commander was able to process the WT for separation
On the other hand WTU commanders stated they a~ exercising nonjudicial punishment as permitted by Article 15 Uniform Code of Military Justice to the best of their ability Commanders went on to say they continue to enforce all applicable Army regulations and policies to ensure good order and discipline in accordance with Wanior Care and Transition Program Policy Memo 09-001 4 (b) In deciding appropriate punishment commanders stated they are also seeking the counsel of medical providers before rendering UCMJ action for WTs due to the complexHy of the WTs medical issues some of which may be behavioral health related
Good order and disclpline is critical to the successful performance of any Army organization Despite a Soldiers Injuries and whether or not helshe was wounded in combat it is essential that all Soldiers are held to the same standardsof discipline Not doing so will only degrade the morale and success of the unit Commanders need to support and empower their subordinates when it comes to enforcing standards
FOR OFACIAL USE ONLY This doctln tent ccntains information EXEMPT FROM MANDATORY DISCLOSURE ancter the FOIA Exemption 5
A-44
Oi998ffllrmwn is prohiBited Etl(eept 89 atlthodzed by AR 29 1
RECOMMENDATIONS
a OTSGMEOCOM ICW T JAG Emphasize the importance of maintaining good order and discipline and ~nsure WTs are held to the Army standards of disCipline
b OTSGIMEDCOM Implement cadre training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
STANDARD OTSGIMEDCOM Policy Memo 09-011 Warrior In Transltion (WT) Medical and Military Responsibllfties-
FOR OFFICIAL USE ONlyen This dOCUllient conrail Infolmatlon EXEMPT FROM MANDATORY DISCLOSURE tiMer the FOIA ElIemptiefi 6
A-45
Diss8minati 19 prohibited eceept 88 ellherked by AR2Q 1 bull
TABB
FINDINGS AND OBSERVATIONS
OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers andFamly members
OB~ERVATION 21 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide Warriors in Transition (WTs) with a level of personal service and an environment conducive to their medica f and transitional needs Most SF~Cs encounter near-term resource challenges (facilities funding and staffing)
DISCUSSION One of the highlights ofthe Soldier and Family support systems is the SFAC It is organized under Army Community Service (ACS) but has its own funding challenges through Installation Management Command (IMCOM) It is a Warrior Transition Unit (WTU) - dedicated facility with a collection of services for WTs and their Families AI~hough the services provided by the SFAC can be found in ACS and Soldier Processing Centers the purpose of the SFAC is focused on a smaller population with unique requirements Its mission is to provide a higher level of service with the ability to give more individual time and attention to a smaller and specific population in a tranquil environment All cadre staff providers and Family members interviewed stated WTs with behavioral heatth issues post-traumatic stress disorder andor traumatic brain injury require more time patience and attention when receiving care service or resolution for their issues The SFAC facilitates the delivery of services through a central location and experienced staff WTs their Family members and cadre at all levels report that the SFAC is a valuable resource
The main concern of a few senior leaders is the perceived low usage of the SFAC services A recent Army Audit Agency (AAA) (eport concluded the SFAC workload for many of the services being provided was low and alternative options for providing required services may need to be considered Though the AAA report cited findings similar to ours Concerning the satisfaction with SFAC services AAA concluded that the expense for the facilities and services was too high given the small population and low usage Some leaders and staff stated the SFAC should be open to all or at least to all Soldiers undergoing a Medical Evaluation Board (MEB) Most SFAC directors disagreed that it should be open to all but shared that they provide service to non-WTU Soldiers who find their way into the SFAC if it does not interfere with their main mission
The team observed that SFAC staff consists mainly of personnel who are retired from military service or have extensive experience in or working with the military They provide access to a number of services entitlement and benefits counseling military human resource services educational services employment assistance transition services ACS Family services travel pay for Family members on invitational travel
FOR OFFICIAL USE ONLY ThIs document COiitailiS illformation f3(EMPTFROM MANDATORY DISCLOSURE loIAder the FOlA ampemption 6
B-1
OisseminatioA is prehibiteEI except as aulhEamped by AA 20 1
orders substance abuse information and referral for Family members legal and pastoral services Army Wounded Warrior Program Veterans Affairs representatives Veteran Benefits Administration representatives and Traumatic Service members Group Life Insurance (TSGLI) Most SFAC directors interviewed stated ~he services used most are education finance human resources and military benefits
An additional service provided to the WTU is the ombudsman The ombudsman is an advocate for the wr and hislher Family and ensures a case reaches an individual who can provide resolution Although the program was designed to help resolve medical treatment issues the scope of assistance ombudsmen provide is well beyond the medical arena Assistance often crossed over inspector general and equal opportunity areas The team observed that ombudsmen resolve issues involving legal financial promotion chain of command and disciplinary problems Ombudsmen also assist Soldiers who are not part of the WTU with the same types of issues The majority of the ombudsmen interviewed stated 70-80 of their caseload was from nonshyWTU Soldiers Ombudsmen typically have offices inthe military treatment facility (MTF) on installations and have posters with contact information throughout the MTF but spend much of their time in and around the WTU campus The majority of WT s who used the ombudsman are satisfied with the advocacy heshe provides however most WTs and Soldiers outside the wru are not aware of the ombudsman program
RECOMMENDATIONS
a fMCOM Conduct cost-benefit analysis to determine if SFAC services can be made available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for year of execution policy requirements (zero sum game)
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007~26 2009-08
FOR OFFICIAL USE ONLY This doctllient colltains Information EXEMPT FROM MANDATORY DISCLOSURE tlAder tnt FOIA Exempticn 5
B-2
Dissemination is prehibited exeept as authorized by AR 20-1
OBSERVATION 22 Pro~iding services for COMPO 213 Waniors In Transition (WT) and Families is challenging due to the dispersion of state resources
DISCUSSION Installations (Soldier and Family Assistance Centers (SFAC) and Army Community SelVice (ACS) Centers) are providing the common levels of support (CLS) to WTs and Families per established policy and guidelines For Warrior Transition Units (WTU) how they provide that support varies based on the size anCi geographical situation of the unit and their SFACACS Community-Based WTUs (CBWTU) consist primarily of COMPO 2 and 3 Soldiers These Soldiers are typically remotely located from any installation and present unique challenges to CLS Installation ACSSFAC services are not available to all areas for COMPO 2 and 3 Soldiers and Families on the same scale as those for COMPO 1 Most of the support for these remote Soldiers and Famines is telephonic or web-based (Army OneSource) Military Family Life Consultants (MFLC) fills much of the role of ACSSFAC but cannot provide all of the same services
The same situation exists in Europe In Europe both the WTU and SFAC are very geographically dispersed In some cases the unit is spread out to the squad level Command and control are a great challenge as well as support The SFAC conducts decentralized operations in order to serve the WTU population Most services are telephonic or referral Two providers Veteran Benefits Administration and Army Wounded Warrior Program rotate representatiVes throughout Europe to the WTB companies platoon and squads on a six-month basis
RECOMMENDATION
OTSGIMEDCOM and ASA (MampRA)G1 ICW IMCOM ARNG OCAR and Army PAO Establish a steering committee to determine most effective methods to deliver infonnation and services to COMPO 213 WTs and Families
STANDARDS EXORD 118-07 (HEALING WARRIORS) IMCOM Netca1l2007-26 2009-08
FOR OFRCIAL USE ONLY This document contab IS b om latian EXEMPT FROM MANDATORY 91SCLOSURE tinder the rolA exemption 5
Dieemillatioll is pruhibitod eeept as tNtherized by AR 20-1
lt
OBSERVAnON 23 Communities outside the gate are beginning to selectively support only combat-wounded WTswith incentives resulting in nonshystandardized practices across installations
DISCUSSION The inspection team observed that a caste system has developed in the WTU There is delineation among WTs based on how they came to be a WT hislher motivation or agenda while in the wru and middoteven Army Component Directors and providers stated some comm~nities reach out more fervently than others and the level of support is evident in the types of services provided and events sponsored (sporting events family outings additional counseling and medical services donations)
The initial perception of most people was that theWTU consisted of only combatshywounded Soldiers Now that more people are aware that the wru is home to more than combat-wounded Soldiers SFAC directors and staff informed the inspection team that those who choose to volunteer servicessupport to WTs are specifically qualifying the support for the combat-wounded which is less than 10 of the wru population (Warrior Transition Status PAampE OTSG 21 January 2010) Persons andor organizations making donations andor providing services (recreational outings event tickets social events equipment and facilities) inquire specifically about taking care of wounded warriors
Communities should understand that The Warrior Care and Transition program is not just for combat wounded Soldiers but for all Soldiers with wounds injuries or illnesses requiring complex or comprehensivemedical care Furthermore donations and services provided by communities benefit WTs assigned lattached to WTUs
RECOMMENDATIONS
a OTSGlMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
STANDARD NA
FOR OFFICIAL USE ONLY This document contains information EXEMPT FROM MANDATORY DISCLOSURE Ader the FOIA ampemptioo 6
B--4
OisseminatisA is prohibited exeept as auther-izud by AR 20 1
THIS PAGE INTENTIONALLY LEFTmiddot BLANK
This doetlment contains information EXEMPT FROM MANDATORV DISCLOSURE umler the FOil ExemJ)tieA 6
FOR OFFICIAL USE ONLY Dissemination is prohibited ~ as atlthorizea ~ AR 20 1
TABe
FINDINGS AND OBSERVATIONS
OBJECT1VE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 31 The Anny does not use common terms of reference to accurately determine status of medically not ready medically non-deployable and not availabre Soldiers
DISCUSSION The Army uses numerous terms when discussing Soldier health and fitness for duty The multitud~ of tenns are often used interchangeably and are confusing in discussion or when reporting status of Soldiersmiddot To accurately report unit readiness for overseas deployment while simultaneously managing the health needs of Soldiers commanders need a single term that definitively denotes availability and readiness to deploy
The mixing and mis--usage ofterms such as medically ready or medically not ready deployable or non-deployable and available or not available does not aid commanders in reporting and may even lead to mis-reporting of unit readiness for overseas deployment leaving the Army with a potential false sense of deployability For example a unit commander may count a Soldier as available- on his USR implying that the Soldier is deployable to all potential theaters of operation That same Soldier may require an updated dental panorex making himlher medically not ready according to MEDPROS or that heshe is -not deployable for limitations eXpressed within theater guidance
AR 220-1 Unit Status Reporting is the unit commanders report to the Army detennining overall readiness The medical readiness portion of the report makes use of the terms available- and anot availablemiddot Chapter 4-1 of AR 220-1 states For USR purposes Soldiers are considered to be available if they are attached or assigned to the measured unitlheadquarters are physically present or can be present within the prescribed response time and are not restricted by Army policy from deploying or employing with the unit U By the use of theSe terms it is presumed that this report tells the Army the readin~ss of a unit to deploy overseas This is- however not accurate A Soldier could be available to deploy but not deployable to certain area of operations (AOR) due to more restrictive criteria from a Combatant Command For example the requirements for a Soldier receive an AnthraX vaccination in Central Command (CENTCOM) AOR
AR 40-501 Standards of Medical Fitness provides information on medical fitness standards for induction enlistment appoIntment retention and related policies and procedures e Although this regulation is used as the sole source for detennining medical fttnessfor service in the Army it is not a deployment standard Chapter 5-14
FOR OFRCIAl USE ONLY This dOCtlmellt colltains illfon lIatioli DCpoundMPT FROM MANDATORY DISClOSURE under the FOIA ~mptien S
Dissemination 1amp prehlblted exeept as lMhorimd by AR 2a-
covers medical fitness stan~ards for deployment and certain geographical areas but defers to Army Gl Personnel Policy Guidance (PPG) Message and theater medical guidance for specfficassignment determinations and combat deployments
a All Soldiers considered medically qualifiea for continued military status and medically qualified to serve in al or certain areas of the continental United States (CONUS) are medically qualified to serve in similar or corresponding areas outside the continental United States (OCONUS)
b Some Soldiers because of certain medical conditions may require administrative eonsideration when assignment to combat areas or certain geographic areas is contemplated to ensure that they are used within their medical capabilities without undue hazard to their health and well-being or producing a hazard to the health or weI-being of other Soldiers
c Active duty Soldiers who do not meet the medical retention standards In chapter 3 of this regulationmust be referred to an MEBIPEB for a fitness-forshydutt determination RC Soldiers not on active duty who do not meet medical retention standards are referred for a fitness deteimination in accordance with paragraphs 9---10 (USAR) and 10-26 (NGB) Soldiers (RC or Active Army) with a permanent 3 or 4 in the physical profile who meet or might meet medical retention standards must be referred to an MMRB to determine If they are worldshywide deployable (or be granted a waiver according to AR 600-60) However Soldiers retumedto duty by an MMRB or PES retained in the RC under paragraphs 9-1Ci or 10-26 or Soldiers with temporary medical conditions may stili have some asslgnmenVdeployment limitations that must be considered before a deCision is made to deploy
d Assignment determinations are under the purview of the Deputy Chief of Staff (DCS) G-1 Specific duties in the assignments are under the purview orthe Soldiers commander Medical guidance is criticalin advising commanders and assignment officers of potential problems physical limitations and potential situations that could be harmful to the Soldier andor those with whom the Soldierserves Medical guidance Is provided in the form of physical profiles (permanent and temporary) and occurs during deployment proCessing or dUring the medical revftJw prior to overseas assignment
The Medical Protection Systemor MEDPROSJ Is the primary tool used by commanders and unit medical personnel to track and detennine medical readiness of their unit and individual Soldiers MEDPROS was developed by AMEDD to track all immunization medical readiness and deployability data for all active and reserve components of the Army as well as DA civilians contractors and others The data in MEDPROS Includes aU medical and dental readiness requirements lAW AR 600-8-101 personnel processing (in- out- Soldier readiness mobilization and deployment processing) including immunizations permanent physical profiles and duty limitations
FOR OFFICIAL USE ONLY This doeament contains infomration EJEEMPT FROM MANDATORY DISCLOSURE lIflder ~e FOIA Eempfiefl 6
C-2
DisSemiAatiofl Is prohibited exeept as authorized by AA 21) 1
eyeglasses and insertsmiddot blood type medical warning tags personal deployment medications pregnancy screening DNA and HIV Although MEDPROS is an often used and welcome tool for comm~nders medical providersand unit medical staff it determines readiness not actual deployability often confusing Commanders SoldJers and ultimately the Army as to actual available strength for deployment
The documents that determine deployability of any given Soldier are theater-specific health guidance such as CENTCOMs MOD 10 dated 5 March 2010 When a Soldier and his unit go through Soldier readiness processing (SRP) in preparation for deployment theater specific health guidance is used as the final authority to proscribe to a commander who is and Is not fit to deploy to a given theater of operation Ultimately the commander is the final arbiter but the theater medical guidance is proscriptive in nature and a commander that chooses to ignore it does so at his own peril All in all SRP centers and power projection platforms must check eleven different documents and regulations from 0001 602519 Individual Medical Readiness to theater-specific guidance such as CENTCOMs MOD 10 to determine If a Soldier can or cannot depioy to a given region of the world
RECOMMENDATION
OTSGIMEDCOM ASA(MampRA)lG1 G3I5n ICW FORSCOM Standaroizetenninology for Soldier medical readiness status (eg for standardization data from deployment checklist could be included in MEDPROS)
STANDARDS AR 220-1 Unit Status Reporting chapter 4-1 AR 40-501 Standards of Medical Fitness Chapter 5-14 G1 Personnel Policy Guidance AR 600-8-101 Personnel Processing (In- Out- Soldier Readiness Mobilization and Deployment Processing) Chapter 4 Theater-specific Deployment Guidance
FOR OFACIAL USE ONLY This dOCtlment contains inforTnatlon EXEMPT FROM MANDATORY DISCLOSURE uruter the FOIA EKemptieA 6
C-3
Oissemilletien is pmhibited except 89 author2ed by AR 20-1
OBSERVATION 32 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
DISCUSSION The ARFORGEN cycle is a 30 month cycle broken into three phases reset trainready and available The reset and trainready phases produce combat ready brigade combat teams (BCTs) over an 18 month process During the 18 months of reset and trainready BeTs are filled to 00 strength In personnel At the end of the 18 month period a given BCT is in theory 100 filled with Soldiers that are medically fit to deploy wond-wide
The Army medical fitness detennfnation process [as governed by AR 40-50 Standards of Medical Fitness AR 600-60 Physical Perfonnance Evaluation System and AR 635-40 Physical Evaluation for Retention Retirement or Separation] does not synchronize with the 18 month timeline for reset and trainready in the ARFORGEN cycle AR 40-501 allows for a temporary profile (which may or may not be deployment limiting) for a period of between one and 2 months
Temporary profiles A temporary profile is given if the condition Is considered temporary the correction or treatment of the condition s medically advisable and correction usually will result in a higher physical capacity Soldiers on active duty and RC Soldiers not on active duty with a temporary profile wi be medically evaluated at least once every 3 months at which time the profile may be extended for a maximum of 6 months from the Initial profile start date by the profiling officer
(1) Temporary profiles exceeding 6 months duration for the same medical condition will be referred to a specialist (for that medical condition) for management and consideration for one of the following actions
(a) Continuation middotof a temporary profile for a maximum of 12 months from the initial profile start date
(b) Change the-temporary profile to a permanent profile
(e) Determination If the Soldier meets the medical retention standards of Chapter 3 and If not referral to a MEB
Upon receiving a pennanent profile a Soldier must be referred to either an MMRB (MOS Medical Retention Board) or a MEB (Medical Evaluation Board) Once a Soldier Is referred to an MMRB or aMEBhe or sheJs non-deployable lAW HQDA PPG (Personnel Policy Guidance) published on 1 July 2009 and updated on 15 April 2010 The time standards for the MMRB process are outlined in AR 600-60 Chapter 2-4 page 4-5
FOR OFFICIAL USE ONLY flris document contains infoml8tlon ~EMPT FROM MANDATORY DfSot05URE IInder the FOIA ampemptiefl 6
DissemlMllen 19 prehlbited exeept as aiftheAiBd by AR 20 1
a Soldiers will appear before an MMRB within the tjme standards stated below The time standard will be measured in calendar days from the date the DA Form 3349 s signed by the appropriate approving authority
bull 60 days for Soldiers on active duty and for members of the Active Guard Reserve (AGR) program bull 120 days for Soldiers assigned to USAR TPU or ARNG drilling units (hereafter referred to as drilling reservists) and drilling and nondrilling IMAs bull 180 days for USAR Soldiers assigned to the IRR and ARNG Soldiers assigned to the Inactive NatiOnal Guard (ING)
b The MMRBCA (MOS Medical Retention Board Certifying Authority) will make his or her determination on MMRB recommendations no later than 30 days from the date the MMRB adjourned
By-thls standard a Soldier potentially could be in the MMRB process for a maXimum of 90 days
According to data accumulated by Medical Command (MEDCOM) and the Office of the Surgeon General (OTSG) In 2009 the MEB process coupled with the Physical Evaluation Board process outlined in AR 635-40 takes on average 214 days or just over seven months This number is expected to grow in 2010 It is Important to note that the data collected only Includes the number of days a Soldier is offiCially in the MEB process If a Soldiers individual medical and administrative re~rd Is not sufficient for the board and is -kicked back the Soldiers process starts allover again Thus the 214 day average may In fact be low due to the means in which the data was collected Additionally MEDCOM and OTSG data collected In the first six months of 2010 indicate less than 10 of Soldiers entered into an MEB process are returned to duty (RTD) Said another way in 2010 90 of MEB Soldiers will leave the Army with some level of disability and enter Into the Veterans Affairs disability process All totaled a Soldier that is wounded ill or injured and enters into the medicalmiddotfitness determination process could potentially be In that process for a period of 1 to 24 months or more As stated eartier the average amount of time a brigade combat team (BCT) commander has to fill and train his unit for pending deployment in the ARFORGEN cycle is 18 months (Data collected from PAampE OTSG Briefing 17 June 2010)
Because Soldiers must fill authorized slots on an MTOampE or TDA document for accountability and BCTs cannot request backfill until a slot is empty or coded as a loss senior mission commanders on their own initiative are re-assigning Soldiers within BCTs to ensure BCTs that are preparing for deployment are filled with fit deployable Soldiers A Soldier that is non-deployable Is re-asslgned from one BCT to another il1 order to ensure that theBCT closest to deployment is fully manned prior to deployment This has led to the perception among many medically not ready or non-deployable Soldiers that the chain of command is more interested in obtaining deployable Soldiers than medically fixing the ones they have
FOR OFFICIAL USE ONLY This doclJmenl contains information EXEMPT FROM MANDATORY DISCLOSURE IAder the FOIA 8uilmptieA 6
C-5
DissemiAatieA Is pr-ehibited exeept 8S etltherizaEI by AR 2Q 1
This problem extends to the Reserve components where medically not ready and medically non-deployable Soldiers number roughly 14500 for the National Guard and 14000 for the Army Reserve (data from WCTP briefing to The Surgeon General June 2010) Anecdotal evidence suggests that State National Guards will fill a deploying -BCT with fit Soldiers from across the available units within the State The ARFORGEN cycle with its established timelines forces commanders to make hard calls between the needs of the mission and the needs of the Soldier Rightly so the mission is coming first and commanders are getting creative to ensure Soldiers get the medical attention they deserve
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)G1 G3Sn and FORSCOM Examine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army The Integrated Disability Evaluation System currently in pilot program phase may reduce the amount of time needed to determine fitness for duty and retention or separation from the Army
b ASA(MampRA)lG1 Code Soldiers in MEB process as a loss allowing for replacement requisition
STANDARDS AR 40-501 Standards of Medical Fitness Chapter 7-4 page 74 AR 600-60 Physical Performance Evaluation System Chapter 2-4 page 4-5 AR 635-40 Physical Evaluation for Retention Retirement or Separation Chapter 4 -Section I-VI
fOR OFFICIAL USE ONLY This dOCtlment contains irrfonnation EXEMPT FROM MANDATORY DISCLOSURE fflder the FOIA ampemption 6
0-6
Dissemlft8tlclft Is preh ibiteEI GKeS 8amp alflheFileEl by AR 29 1
OBSERVATION 33 Army medical capabilities do not support the needs of the Medic~1 Not Ready (MNR)Medical Non-Deployable (M~D) tn unitsmiddot
DISCUSSION Theinsp~ction team found that Command~rs personnel staff and medical staff of most units (19 of 22) had very good situational awareness of the medically not ready and medically non-deployable populations within their formations The extensive use of MEDPROS USR reporting and annual Soldier Readiness Processing (SRP) were the principle means of gaining this awareness The Army has large and increasingmiddotnumbets of medically not ready and medically non-deployable personnel The National GJard and Army Reserve report roughly 14500 and 14000 Soldiers respectively in these categories One active component division has organized its medically not ready and medically non-deployable personnel Into five companies to increase the division situational awareness and careot MNRlMND Soldiers
The Vice Chief of Staff recently made a decision establishing Installation Medical Management Centers at Medical Treatment Facilities (MTFs) increasing the number ot Care Coordinators underthe direction of the installation commander to assist unitsmiddot with managing the care of their MNRlMND population Good situational awareness of the population does not equate to caring for the medical needs of Soldiers or determining fitness for duty retention or separation Although most SQldiers (155 of 179) do not feel disadvantaged in access to care most leaders and healthcare providers (411 of 491) are concerned that Soldiers not having enhanced access to care
status as outlined in MEDCOM Policy memo 08-028 are not being seen in a timely manner
As outlined in greater detail in observation 34 the Army places the highest priority for medical care on Warriors in Transition (WTs) giving them enhanced access to care Medically not ready and medically non-deployable Soldiers do not enjoy that same access to care unless they are in a untt that is within 90 days of deployment or 180 days of returning from a deployment The average length of stay for a WTin a WTUthat is not going to return to duty is over 14 months consuming resources that are in short supply across the Army (WTs Length of Stay PAampE OTSG briefing 14 June 2010)
The inspection team also found that most Military Treatment Facilities (MTFs) reported shortages in specialty care providers particularly Occupational and Physical Therapy specialists and Behavioral Health speCialists MEDCOM statistics Indicate that 33 of MTF case load is orthopedic related and 30 Is behavioral health (TBI PTSD Mental health (non-PTSDraquo (Warrior Transition Population PAlE OTSG 13 April 2010) With over 60 of the MTF case load related to these two specialties and shortages in these same specialties the time in which a Soldier gets seen regardless of whether the Soldier is on track for retention or separation is extended
TIme is of the essence not juSt because the Army wants to and must care for its Soldiers but because it needs them or a replacement healthy and fit for deployment If they cannot be retained due to medical fitness standards then they must be
FOR OFRCIAL USE ONLY This document contains infoml8tien EXEMfFf FROM MANDATORY f)fSCLOSURE under the FOIA Exenlption 5
C-7
Dissellib lattan Is prohibited except as authorized by M 26-1
transitioned from the Anny in a timely manner The Medical Retention Decision Point (MRDP) is defined in OTSG Policy Memo 09-037 15 June 2009 as one year of being diagnosed with a medical condition that does not appear to meet medical retention standards but may be earlier If a Soldier simply cannot be seen due to backlog of patients and limited specialty care providers then the time in which he or she Is in the healing MOS Medical Retention Board (MMRB) Medical Evaluation Board (MEB) or Physical Evaluation Board (PEB) process cannot help but be prolonged This situation is exacerbated by a perceived unwillingness or inability of some providers to make a
decision as to wheth~r a case meets retention standards Anny doctors are In a conundrum Their oath as doctors presumes advocacy for patients Their oath as Army officers presumes faithful execution of duties to the Army and Nation Medical professionals at multiple Ievels stated in interviews that they felt bound to error on the side of the individual patient rather than the needs of the Anny as a whole
The on--going increase in the amount of care Coordinators will increase medical situational awareness for the Anny and provide Soldiers more Individualized attention but it will not increase through-put nor will It shrink the amount of time it takes to reach the MRDP Only more doctors to see more patients can do that
RECOMMENDATIONS
a OTSGIMEDCOM ASA(MampRA)lG1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase In medical assets to mitigate current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to assist in managing MNRlMND Sol~iers The Integrated Disability Evaluation System cuffently in pilot program phase may enhance visibility of the system for the Soldier the Army and the Veterans Administration
STANDARD NfA
FOR OFFICIAL USE ONLY This document contains Intormation EXEMPT FROM MANDATORY DISCLOSURE und61 the F01AmiddotExemption 5
DislemiflatieA 18 pmhlblteG except 8S attlhred by AR 29-1
OBSERVATION 34 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
DISCUSSION Most Soldiers (155 of 179) interviewed stated they have adequate access to care Most leaders and healthcare providers (411 of 491) interviewed were concerned that Soldiers lacking enhanced access to care status as outlined in MEDCOM Policy memo 08-028 were not being seen in a timely manner MEDCOM POlicy memo 08-028 MTF Access Standards for Active Duty Service Members enhanced access to care standards applies to Warriors in Transition deploying active duty service members (ADSMs) and Post-deployment ADSMs The standards are
24 hour urgent care - 3 working days routine primary care - 7 wor1dng days initial specialty care (not a consult consuHs have no
access to care standard)
Redeploying Soldiers get 180 days of enhanced access to care status while deploying Soldiers get 90 days
The deploying Soldiers enhanced status provides the opportunity to address medical issues discovered during a unit pre-deployment SRP Whereas Soldiers assigned to non-deploying units or force-generatlng units may enjoy the lUXUry of time to be seen under these priority guidelines a Soldier in a unit within the ARFORGEN cycle does not As mentioned earlier in this report the ARFORGEN provides 18 months of Reset and TrsinlReady time The 6 months of reset time is accounted for in the current priority guidelines with the 180 days of post deployment care but the 12 months of trainready time is not A commander deciding between healing a Soldier for impending deployment or deciding to separate him or her has a very short amount of time The access to care standards does not support the commanders need to get his unit ready for the next deployment
RECOMMENDA 110N
OTSGMEDCOM ASAMampRA)lG1 and G3517 Conduct a comprehensive MNRlMND support needs study to detennine if medical priorities are correctly synchronized and applied Installation Medical Management Centers recently instffuted by the Army may assist commanders in managing their MNRlMND Soldiers
S1 ANDARD MEDCOM POlicy memorandum 08-028
FOR OFfiCIAL USE ONLY This dom conlaiils information B(EMPf FROM MANDATORY DISClOSURE tinder the FOIA Exemlltien 6
C-9
Ois88minatien i9 ptehlblted eKOept 88 authorized by AR 29-1
OBSERVATION 35 Leaders are concerned about Soldiers that pes with known or unknown medical issues particularly behavioral health Issues (Traumatic Brain Injury and Post-Traumatic Stress Disorder)
DISCUSSION The ARFORGEN Reset phase is when Penn anent Change of Station (PCS) moves are most likely to occur Units of all types (Operatlng Force and Generating Force) inherit Soldiers with unresolved medi~1 issues from past deployments affecting unit mission and readiness
AR 40-501114 a (3) states Pointof Service (POS) must update MEDPROS to reflect temporary and permanent profiles However the inspection team found that a few leaders perceive that some Soldiers are not bringing injuries to the attention of the chain of command in order to expedite a PCS move or in some cases to deploy with their oo~
Most health care providers (199 of249) interviewed stated that behavioral health issues traumatic brain injury and post traumatic stress disorder do not often manifest until six months after returning from a deployment A concern among hearth care providers was that a PCSlng Soldier is under the observation and accountability of a new chain of command that is not familiar with the individuals behavioral patterns Thus-the new chain of command may not notice a change in behavior and miss vital early warning siQns of impending problems -
Similar issues were identified In the Department of the Army Inspector General Inspection of the Army Medical Deployment Process completed In January 2009 Specifically Findings 23 24 and 26 address inaccuracies in MEDPROS and the practice of Soldiers middothand carrying profiles to new duty stations in violation of AR 4CJS01
RECOMMENDATION
ASA(MampRA)lG1 ICW OTSGMEDCOM FORSCOM TRADOC Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
STANDARD AR 40-S01 Standards of Medical Fitness para 11-4 a (3)
FOR OFFICIAL USE ONLY This doctlnl8Tlt contains Information EXEMPT FROM MANDATORV
_ DISCLOSURE looerttle FOIA ampempUeA 6 C-10
Dissemination is pmhieited EtlCeept 88 autheriiBd by AR 2t) 1
OBSERVATION 36 Soldiers in the MEBIPEB process that are not assigned to a WTU are disadvantaged from a lack of Information lower priority in access to care and length of MEBPEB process
DISCUSSION As stated above in Observation 34 most leadership and healthcare providers areconcemed that Medically Not Ready (MNR)Medically Non-deployable (MND) Soldiers are disadvantaged In access to care Soldiers in the Medical Evaluation Board (MEBVPhysical Evaluation Board (PEB) process are Included in the MNRlMND population
Soldiers that are assigned to a WTU in addition to receiving enhanced access to care also receive one--on-one focused Individualized infonnaticm and assistance via the Soldier and Family Assistance Center (SFAC) Soldiers in the MEBPEB process receive information in large forums often via Anny Community Services ACS In Observations 32 and 33 of this report the inspection team noted that Soldiers in the MEBIPEB process experience delays in reaching the medical retention decision point Not only Is this bad for the Army tt also bad for the individual Soldier He or she languishes in a system that despite the best efforts of commanders medical providers and social YOrkers delays their return to civilian life
RECOMMENDATIONS
a IMCOM Conduct cost-benefit analysis to detennine if SFACservicesshould be available to aU Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable the MEBPEB process to begin sooner Installation Medical Management Centers recently instituted by the Army will assist in providing infonnation to MNRlMND Soldiers undergoing the MEBIPEB process
STANDARD NA
FOR OFFICIAL USE ONLY TIde downtellt COl dains Information BEEMPT FROM MANDATORY DISGLOSURE under the FOIA ampemptiofl S
C11
Dissemlrtatiorl is pRlhihited ~pt 8$ 8IJtherized by AR 2Q 1
_ OBSERVATION 37 IRR Soldiers are often not Identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
DISCUSSION Recalled Individual Ready_ Reserve (IRR) Soldiers attend an average of 35 days of administrative accessions and training before linking up with their assigned unit (wwwhrcannymIVsiteiprotectlReserveisokiierservicemobilizationlirrmiddotmobshyinfohtm) The goal of Human Resources Command (HRC) is to link the Soldier up with -his or her unit of assignment at the mobilization station so they can participate in unit mobilization administration and training to include deployment-specific Soldier Readiness Processing (SRP) Army Personnel Policy Guidance (PPG) for Overseas Contingency Operations dated 1 July 2009 and updated on 14 July 2010 states
RC Soldiers identified within the first 25-days as having a pre-existing medical condition that renders the individual non-deployable may be r~reased from active duty (REFRAO) immediately Disqualifying conditions include temporary and permanent conditions that do not meet medical retention standards (Reference AR 40501 Chapter 3)
The PPG further states that an RC Soldier retained on active duty for more than 30 days must be retained on active duty for appropriate medical processing This is commonly referred to as the 25-day rule and is used to determine Army ~ownershlp of Soldier medical Issues
When undergoing accessions at one of four locations (Fort Benning GA Fort Leonard Wood MO Fort Jackson SC or Fort Sill OK) the Soldier receives medical and dental screening according to the standards in AR 4Q501 This process normally tak~s 3 toAshydays Following accession the Soldier conducts 7-10 days of Warrior Task Training WTT)and two to four weeks of MOS training prior to jOining his or her unit of aSSignment at the mobilization station At the mobilization station the same IRR Soldier will accompany hislher unit of assignment throughSRP which includes medical -screening for deployment to the specific geographic location of assignment
I
At one inspection I~tion the team learned that some IRR Soldiers (5 of 14) did not - meet deployment criteria at the mobilization station when going through deploymentmiddot
specific SRP These Soldiers had passed-their accessions frtness standards lAW AR - 40-501 MobiliZation station leadership inferred that a-Soldier maybe fit for service by
AR 40-501 standards but deemed non-ltleployable when screened against theater specific medical deployabilityguidance such as CENTCOM MOD 10 The resuH for the -Army is that these Soldiers are retained on active duty for medical treatment aHhough the medical issue was a pre-existing condition that rendered them non-deployable to the CENTCOM area of operations
FOR OFACIAL USE ONLY - This doctJment contains information
EXEMPT FROM MANDATORY DISeLOSURE under the FOlA Exemption 6
C-12
Dias9lflinatieR 1amp prohibited exeept 89 eutheFlz8d by AR 201
RECOMMENDATION
ASA(MampRAJG1 HRCICW ARNG and OCAR Ensure that IRR Soldiers receive a theater-specifIC SRP within 25 days of mobilization prior to attending WTT MOS training and assignment toa deploying unit
STANDARD NlA
FOR OFFICIAL USE ONLY This doctln IGIiI COIltailiB Infonnation BEEMPT FROM MANDATORY DISCLOSURE tinder ttle FOlA ElEemlflEm 6
013
OisaeminatieA is plElhibiled exeept 89 euItIorizeiJ by AA 2)1
TAB 0
OTHER MAnERS
OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBIPEB Inefficiencies affect the Armys ablUty to meet the needs of Soldiers and the Army in a timely manner
DISCUSSION Currently a separate study regarding MediCal Evaluation Board(MEB) Physical Evaluation Board (PEB) is ongoing by Task Force Franks Most health Care providers nurse case managers (NCM) Warriors in Transition (WTs) and other cadre interviewed identified specific problems of the currentsystem along with the Implementation of the Disability Evaluation System (DES) board processes
There are not enough Physical Evaluation Board Liaison Officers (PEBlO) to meet MEB caseloads in most locations For example at one WTU location the PEBlO to WT ratio was 1 to 52 the standard is 1 to 30
Most health care provider (212 of 249) Interviewed stated DES Pilot Program lengthens the MEBIPEB process This Increase in proceSSing time was due to the following shortage of key administrative personnel (PEBlOs) lack of certified VA examiners differences In the 000 and VA medical examiners credentialing and coordinating physi~1 examination and specialty appointments For example the OES Pilot Program schedules one appointment at a time and requires multiple TOY travel exceeding the 45 days to complete a physical examination In contrast the legacy system scheduled appointments over a 2 week block to complete all evaluations and testing nonnally within the 45 day requirement to complete a physical examination on a Soldier is in MEBIPEB processes Delays in the board process can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources in many locations
The majority of those interviewed stated that these MEBIPEB processes are complex disjOinted hard to understand and take approximately 7 to 24 months In Gen(R) Franks Task Force report April 2009 WTs stated the board process Is slow reportedly taking one year plus to initiate the board and 18-24 months to complete it The fact that less than 10 of Soldiers in the MEBIPEB processes will return to duty also impacts unit readiness Delays in the bOard processes can cause previous evaluations to expire resulting in repeated evaluations drawing on already limited resources inmany locations Measurement of the board time line is difficult at best when health care providers can stoP start and tenninate boardadions Soldiers identify anew conditions requiring Initial evaluation(s) or assessment(s) this continues as mentioned In Gen(R) Franks Task Force report April 2009 Additionally most interviewed were concemed that medical staffing is insufficient to support timely MEBPEB processing
FOR OFFICIAL USE ONlY flos cfowflerit colitailiS illfarmstion EXEMPT FROM MAflDATORY DISCLOSURE urujerthe FOil ExemJHisA 6
0-1
DissemiAatieA is plQhibited except 8S Stlthorfzed ~ AR 2()1
The majortty of providers stated th~ current system encourages focus on disability rather than ability ThIs also coincides with GenR) Franks recommendations to switch focus to rehabilitation and transition
According to AR 635-40 the MEBIPEB process may be stopped or tenninated if elective procedure or surgery is performed as Soldier needs time to stabilize condition Some WTs have completed elective surgeries through civilian providers without discussing them with their primary care manager (PCM) or NCM Currently there is no standardized elective proceduresurgery policy In place for the WTU Program
Most PCMs (31 of 34) interviewed stated current PCM to WT ratios (1 200) are too high and Impacts the quality of cars to WTs Recently added complexity and responsibilities (ie Comprehensive Transition Plans Transttlon Review Boards increase in behavioral health issues complex patients with multiple diagnoses etc) make it difficult to maintain direct cont~ct with specialty providers calJslng delays in recommending Soldiers for MEB initiation Most PCMs (31 of 34) interviewed stated PCM to WT ratios of 1 150 are manageable
RECOMMENDATIONS
a OTSGMEDCOM Continue implementation of recommendatIons provided by GEN(R) Franks Task Force
b OTSGIMEDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet reqUirements
d OTSGMEDCOM Detennine the laws that need to be changed in order to expedite theMEBPEB processes and improve efficiencies between the Army-and VA
STANDARD
FRAGO 3 to EXORO 118-07 (HEAliNG WARRIORS) Annex D WTU Force Structure Appendix 1 Ratios
OBSERVATION 2 Limited andor no interoperability between 000 (AHLTA) VA (VISTA)TRICARE network and civilian provider infonnatlon syStems
FOR OFFICIAL USE ONlY This dOCllment contains InforTllation EXEMPf FROM MANDATORY DISCLOSURE 1IlEief the FOIA EKemptioo 6
0-2
Dissemifletiofl is pOMltted eJleept as autAeFked by AR 29 1
DISCUSSION Soldiers in Community Based Warrior Transition Units (CBWTU) stated -that sister service MTFs do not recognize the Armys accessto care standards However most Warriors In Transition (WT) stated they are receMog excellent medical
care from sister service areas Most healtrl care professionals interviewed stated there is a lack of TRICARE medical management standardization between regions Regions do not use the same criteria for referral procedures surgical and medication authorizations Reports from the CBwrU noted TRICARE is not covering costs of some medications and WTs have to payout of pocket Some healthcare professionals stated TRICARE authorized different (generic) medication for WTs other than what the primary care manager (PCM) prescribed Some of the primary care managers interviewed were concerned that in some cases the generic medication caused decompensation in the WTs condition
Nurse Case Managers reported TRICARE contact listings for providers were not forthshycoming The provider listings are outdated Moreover a provider may no longer accept TRICARE because of the following reasons less money for the providers when compared to other paym~nt programs increased administrative costs to maintain participatloo in the program andor simple failure to renew TRICARE participation
Provider qualification for TRICARE may take up to nIne months
Most WTs (598 of 786) stated referrals to the TRICARE networks result in medical treatment obstacles and administrative errors Additional issues voiced were that different TRJCARE regions reQuire different information and delays in obtaining copies of medical treatment back from TRiCARE providers delays WTs treatment and transItion CBwru health care providers were concerned with TRICARE standardization of care due to croSSing of the servicing networks (NORTH SOUTH and WEST)
Providers at CaWTUs stated that bridging capabilities to improve the interoperability between DrgtD Armed Forces Health Longitudinal Technology Application (AHLTA) VA Veterans Health Information Systems and Technology Architecture (VISTA) and civilian medical systems would provide continuity and communication of care Currently Army medical and TRICARE interoperability issues hinder medical management ofWTs referred to the TRICARE provider network
RECOMMENDATION
OTSGMEDCOM Improve the interoperabillty between DoD (AHLTA) VA (VISTA) and TRICARE network Information systems
STANDARD NA
FOR OFfiCIAL USE ONLY This deetlment eeAtaiAs iflfermatien EXEMPT FROM MANDATOf1tY DISCLOSURE tinder the raJA rx8mption 5
D-3
DissefIIlAfltioo is pmhibited ellaquol8pt a9 authorized by AR 20-1
OBSERVATION 3 COMPO 213 are no longer a strategic reserve current Army resources appear to be Insufficient to medically sustain RC in an operational environment
DISCUSSION The last major reform of the Reserve Components took place after the Korean War for which the nation was poorly prepared The Vietnam War was the last conflict fought with a draft and without a largemiddot reserve mobilization It was followed by the Total Force concept and a significant shift In the mld~1970s to an all volunteer force However the Reserve Components remained a strategic force to be used only for extraordinary contingencies with the assumption that they would have the benefit of lengthy mobilization periods Since employing the reserves in Desert Shield and Desert Storm Department of Defense (000) has increased theoperational tempo of the Reserve Components to sustain global oommitments Acoording to the Commission on the National Guard and Reserves 31 January 2008 the contribution of the National Guard and Reserves to our nations defense efforts has risen to almost fIVe times the level it was before 911 the Army National Guard and Army Reserve workload has increased more than seven times
In January 2008 after releasing two interim reports the Commission on the National Guard and Reserves submitteq its final report to Congress The Commission concluded The reliance (on the Reserve Components) should grow even after the demands for forces associated with current operations are reduced The report noted that -ueir service In the operational force will be required in peacetime and they will continue to provide a cost-effective means of ensuring that strategic requirements to meet a large wartime threat are also available Employing the Reserves in this fashion has proven necessary and effective and they have been relied on in every major military operation since Operation Desert Storm yet the structural foundations of Reserve Component organization have been changed little to facilitate this employmenf
In October 2008 in recognition of this increased reliance on the Reserve Components to support the nations defense the Secretary of Defense published a directive for management of the Reserve Components The Secretary of Defense now requires the Secretaries of the Mili1ary Departments -to manage their respective Res as an operational force to meet US military requirements across the full spectrum of conflict as Identified by the President and the Secretary of Defense
The Secretary of Defenses directive further explains what is meant by the term RC as an operational force II The RCs provide operational capabilities and strategic depth to meet US defense roles RCs participate in a full range of missions according to their Services force generation plans Units and IndIviduals patficlpate In missions in an established cyclic or periodic manner that provides prampdictability for the combatant commands the Services Service members their families and employers In their strategic roies RC ~nlts and indMduas traIn or are available for missions in accordance
FOR OFFICIAL USE ONLY This document contains illfom l8tiou EXEMPT FROM MANDATORY DISCLOSURE tinder the FOIA ampemptieR 5
Dissemimdio is j)Fehlbited elteept as autheriHd by AR 29 1
wffh the national defense strategy As SUehl the Res provide strategic depth and are avaJ1abie to transition to operational roJes as needed~
Thus the primary rationale for transforming the Armys Reserve Components is to ensure the Army is complying with the Secretary of Defenses policy for managing the Reserve Components as an operationalforce Policies legislative proposals and prograrnming decisions are required to ensure the Army can comply with the Secretary of Defenses guidance to achieve an Operational Reserve Force for full spectrum conflict
RECOMMENDATIONS
a OTSGIMEDCOM and ASA(MampRA)lG1 ICW IMCOM ARNG and OCAR and Army PAO Establish a steering committee to conduct gap analysis and provide recommendations to address RC medical care requirements as an operational force
b OTSGMEDCOM ICW ASA(MampRA)G1 G35n ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified for deployment
STANDARD NA
OBSERVA nON 4 The majority of medicalmanagement staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
DISCUSSION The majority of Command and Control (C2) andMedical Management (M2) staff (348 of 457) stated they had concems when tending high-risk and volatile Soldiers (eg WTs MNbs in Medical Evaluation Board (MEB) process) They informed the team that some Soldiers who may have behavioral health (BH) issues andor may be frustrated with perceived lengthy process of hislher MEB often become irate and threaten or physically assault M2 staff For example some of the PEBLOs interviewed reported theywere assaulted in their offices and also threatened with violence Some medical providers (MEB physicians and Primary Care Managers (PCMraquo (36 of 134) reported they were threatened and incurred personal property damage in the forms of flat tires and damage to prlvately-owned vehicles A few Nurse Case Managers (12 of 115) (NCM) reported receiving threatening phone calls andor threats during sessions
Compounding the safety concems was the lack of safety measures in some of the facilities the team visited Staff members on four installations complained there were no means to alert authorities immediately should a problem arise They referred to panic buttons like those in banking centers which would be direct lines to installation security
FOR OFFICIAL USE ONLY This docun lent contains Infcrrnatlon OissemlAatieA is prehibitee EXEMPT FROM MANDATORY exeept 8S alileriee tty AR 29 1 DISCLOSURE tinder the FOIA ExemptieA 5
forces Some facilities although brand new had only one way in and out that was easily accessible The team also interviewed C2 and M2 staff who devised their own personal safety measures They used buddy teamsa when providing services and carried whistles and pepper spray or mace Some coordinated for other staff to be present during a Soldiers appointment Eisenhower Army Medical Center Fort Gordon GA has anned security guards within the hospital All of these ideas worked for the staff we Interviewed but do not address the central issue of a lack of personal security measures
RECOMMENDATION
IMCOM ICW OTSGIMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
STANDARD NA
OBSERVA noN 5 Most healthcare provide~ interviewed (Primary Care Managers Nurse Case Managers) estimate 25 35 of WTs are dependent on or addicted to drugs
DISCUSSION The majority of health care providers and NCMs (126 of 249) interviewed stated most WTs ariive at the WTU with prescriptions of controlled s~bstances that were provided in theater or from the demobilization site Most PCMs and NCMs (113 of 149) interviewed stated some (25-35) WTs are over medicated abuse presCliptions and have access to Dlegal drugs Health care providers intervieWed stated a few WTs are paying out of pocket for narcotics These health care providers are concerned a few WTs are mixing I~al and illegal drugs
TRICARE representatives and pharmacists stated there is a TRlCARElcivilian provider prescription automation gap (1-4 days may pass before military systems account for civilian filled prescriptions) allOwing WTs to request refills or renew prescriptions before PCMs are aware
PCMs are responsible for medication reconciliation at each apPOintment Constant proactive communication between the Triad of Care specialty heaHhcare providers and the chain of command Is required to maintain a semblance of control Not all WTUs have a pharmacist available or dedicated to review WTs medication histories This is especially apparent for separate WTU Companies PCMs are required to follow up monthly with high-risk WTs on the sole provider program
FOR OFFICIAL USE ONLY Tlds dUCClll1811t COlltains infonnalion EXEMPT FROM MANDATORY DI$ClOSURE under the rOIA exefflJtien 5
Oissemifleioo is prehiblted exeept as eutAoFlied by AR w 1
The majority of providers (138 of 249) Interviewed stated the current military health system is not resdurced appropriately to treat drug dependence or abusers These same providers who refer Soldiers to civilian Inpatient drug rehabilitation programs stated these programs are not as effective as the fonner residential military drug programs and their preference is for the Army to re-established inpatient treatment Most psychologists (19 of 21) interviewed stated that WTs referred to a civilian drug rehabilitation program do not continue on active duty They are normally discharged from the Army
Additionally the majority of health care providers (138 of 249) interviewed stated that additional resourcing is necessary to treat an increase in demand for pain management therapy among WTs Some WTUs implemented pain management programs (acupuncture and bo-feedback) have resulted in reduction of the usage of medication byWTs
RECOMMENDATIONS
a OTSGlMEDCOM Evaluate p~cedures for prescribing medication and consider expansion of alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
STANDARD NA
FOR OFFICIAL USE ONLY TIds document contains infonnation BeMPT FROM MANDATORY DISCLOSURE Ilfldet the FOIA ampemptieR 5
0-1
Dissemination Is prehibited eeef)t as authorized by AR 2Q 1
lABE
INSPECTION OBSERVATIONS - POSITIVE NorES
Positive Note 1 Some Warrior Transition Units imple~ented pain and prescription management programs to assist in the reduction of medication dependency (eg Walter Reed Army Medical Center DC Fort Sam Houston TX Fort Bragg NC and Fort Gordon GA) Military Treatment Facility (MTF) pain management providers offer Warriors in Transition (NT) the option of alternative medicine such as acupuncture and biofeedback 1Jiese options enable WTs to reduce their dependency on pain medication and prescription drugs
Positive Note 2 Focused Transition Review (FTR) Fort Bragg NC is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB) The intent of the FTR is to ensure the leaders and providers of a WT are able to collectively assess and provide feedback as to the WTs progress in all areas This comprehensive review provides the opportunity to also set or adjust the transition timeline for the WT
Positive Note 3 Eisenhower Substance Addiction Program (ESAP) Fort Gordon GA is a partial hospitalization program between the Army Substance Abuse Program (ASAP) and Residential Treatment ProglClms Operated from Eisenhower Army Medical Center ESAP is an tlin-patienf substance addiction program that provides for more effective command and control (C2) and medical management (M2) of Soldiers with addiction diagnoses The ESAP program serves all active duty personnel Army Navy Marine Air Force Coast Guard and Activated Service members in all branches of the military addicted to alcohol andor drugs Partial hospitalization patients participate in group therapYeducational sessions and daily counseling sessions ESAP has a range of program initiatives to work with the service member intensivetherapeutic group sessions relapse prevention risk management sessions therapeutic autobiography group sessions nutrition class occupational therapy recreational therapy and much
more
Positive Note 4 The 4th 10 Building The Soldier Athlete fitness program Fort Carson CO motivates Medically Non-Deployable (MNO) Soldiers and focuses on abilities instead of disabilities The program helps to provide tailored fitness routines for Soldiers with medical profiles It has taken the role of the Master Fitness Trainer to the next level enabling MND Soldiers to maintain or improve physical fitness while on profile It includes color-coded gymnasium workout equipment and a legend to guide Soldiers to the right equipment based on hisher condition A Master Fitness Trainer tracks Soldiers physical fitness needs and progress adVising the Soldier and making adjustments as necessary
middotPosiUve Note 5 Evans Army Community Hospital (EACH) Fort Carson CO established robust Behavior Health Teams (BHl) as a single point of contact to improve
FOR OFFICIAl USE ONLY This document contains informatiOIl EXEMPT FROM MANDATORY DISCLOSURE under the FOIA Exemption 5
E-l
Dissemination Is hbited elEoept as aulheFiied by ltampR 20-1
mission readiness Key leaders at EACH created the initial BHT formel1y called Mobile BHT in December 200 after identifying major issues in the delivery of-behavjoral health (BH) care on Fort Carson The leaders designed the team to address the stigma to BH care poor mission readiness of depl9ying BCTs deficiencies in access to and continuity of BH care and gaps in communication between BH providers and key FORSCOM leaders At full strength a BHT is has 13 personnel and supports a full Brigade Combat Team At the core of the team are six BH providers (mixed skill-set of three psychologists and three Licensed Clinical Social Workers) Each provider exclusively supports a single battalion for the duration of its ARFORGEN cycle in garrison Seven additional personnel support the six BH providers one nurse care manager two social service assistants or BH technicians one medtcal support assistant one LPN and one psychiat~st The team operates in a facility within the BCTs footprint collocated with the supported BCTs medical personnel wherever possible
FOR OFFIGIAL USE ONLY This document contains infolillatlcn EXEMPT FROM MANDATORY DISCLOSURE HAder the FOIA ExemptieA Iii
E-2
Disselftinetioll is pIOhibited BKeept as authorized by M 20-1
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains inforlllationmiddot EXEMPT FROM MANOATQft( DISCLOSURE undet the rOJA Exemption 5
FOR OFFICIAL USE ONLY DissemiAatieA is pFehibited exes as autherized by R 20-1
TABF
QBJECTIVES AND METHODOLOGY
1 Objectives (Reference Appendix 1middotlnspection Directive)
a Assess implementation and oversight of policies and procedures for the Warrior Care and Transition Program
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers who are MedicaltyNot Ready
Spe~iallnterest Item Assess effectiveness and understanding of the Comprehensive Soldier Fitness program
2 Inspection Team The inspection team consisted of sixteen members nine assigned within the US Army Inspector General Agency (USAIGA) Inspections Division and seven IG Augmenteesl subject matt~r experts (SMEs) from the US Army Medical Command (MEDCOM) Assistant Secretary of the Army-Manpower and Reserve Affairs (ASA (MampRAraquo bull
middotArmy Reserve and Army National Guard
3 Scope
Team Chief Deputy Team Chief Inspector Operations Officer Inspector Inspector Inspector Inspector Inspector Inspector Health Policy Army Reserve Policy National Gu~rd Policy amp Operations Nurse Case Management Nurse Case Management WTU Operations WTU Operations
USAIGA USArGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA USAIGA ASA (MampRA) USAR ARNG MEDCOM MEDCOM MEDCOM MEDCOM
FOR OFFICIAL USE ONLY This doament coutains illformatiol1 EXEMPT FROM MANDATORY DISCLOSURE IAEfer the FOIA ampemptioA 6
F-1
DlssemiAationls pmlliblted except as au81BiUed by AR 20 1
a The inspection assessed
(1) Th~ effectiveness compliance and underStanding of policies processes and procedures that apply to the Warrior Care and Transition Program and the implementation of directed changes to policy procedures programs and systems
(2) The effectiveness of support systems soch as Soldier Family Assistance Centers (SFAC) Army Community Service (ACS) and Ombudsman in meeting the needs of our Wounded Warriors and their families
(3) The use and effectiveness of tools and processes (Unit Status Report (USR) transitional companies) by commanders to manage their Medically Not Ready (MNR) populations
(4) Leaders and Soldiers understanding and the effectiveness of the Comprehensive Soldier Fitness Program (results provided under separate correspondence)
4 Methodology
a The DAIG team organized into two inspections teams to conduct simultaneous inspections of multiple installationsuilits and formed one team for large inspection sitesmiddotwhen appropriate This concept allowed the inspedion team to assess a wider range of installations and units within the given inspection timeline The inspection team visited 17 locations in CONUS and OCONUS and contacted 2122 personnel through individual and group interviews and senSing s~ssions
b Document Review The inspedion team reviewed applicable DOD Army and Army subordinate headquarters directives regulations policies guidance and standing operating procedures Additionally it anCllyzed the April 06-07 Inspector General report of the Army
Physical Disability Evaluation System (APDES) and the June 07 -April 08 APDES Follow-up Inspection the GEN(R) Franks Task Force report on the Medical Evaluation Board (MEB)I Physical Evaluation Board (PEB) Process July 08 - April 09 the Inspector General SoldiershyFamily Action Plan report September 09 and several press releases relating to Wounded Warrior issues The team also reviewed approximately 95 Warrior Transition Unit (WTU)Community Based Warrior Transition Unit (CBwru) policies guidance standing operating procedures and other documentation developed locally to helpmiddotthese units manage and care for their W04nded Warriors and families
c EventsProcesses Observed The observation opportunities listed below represent some of the events that were observed by the team when available during a scheduled visit In total the team observed over 52 various eventsprocesses throughout this inspection
bull wru barracks walk-thru
This dactlment contains information EXEMPT FROM MANDATORY DISCLOSURE tlnll the FOIA Exemption 5
FOR OFFICIAL USE ONLY
F-2
Disseminetioll Is prohibited eJEGept as autherized by AR 20-1
bull SFAC walk-thn bull Access to the Wounded Warrior Automation System bull Triad of Leadership Decision Board for Soldiers nominated for assignment to a WTU
0 Access to the Warrior Transition Module in the Medical Operational Data System (MODS)
e Personnel proce~sing of Soldiers arrivaldeparture from a Wru bull Deployed Warrior Medical Management Center (DWMMC) Walk thru
dln Progress Reviews To examine inspection trends and progress and to receive updated guidance from senior leadership the team cOnducted in-progress reviews throughout the inspection timeline with The Inspector General and other stakeholders including the Warrior Transition Command
5 LocationsUri its
Washington DC- WaRer Reed Army Medical Center and Warrior Transition Brigade Fort Meade MD-Kimbrough Ambulatory Care Center Warrior Transition Company amp Tenant Units Fort Sam Houston TX-Brooke Army Medical Center and Warrior Transition Battalion Fort Bliss TX-William Beaumont Army Medical Center Warrior Transition Battalion amp Tenant Units Fdrt Benning GA-Martin Army Community Hospital Warrior Transition Battalion amp Tenant Units Camp Robinson AR- Community Based Warrior Transition Unit Fort Dix NJmiddot Warrior Transition Company amp Tenant Units Fort Eustis VA- McDonald Army Community Hospital Warrior Transition Company amp Tenant Units Fort Jackson SC-Moncrief Army Community Hospital Warrior Transition Company amp Tenant Units Fort Bragg NC-Womack Army Medical Center Warrior Transition Battalion amp Tenant Units Fort Gordon Dwight David Eisenhower Army Medical Center Warrior Transition Battalion amp Tenant Units Concord MA- Community Based Warrior Transition Unit Fort Carson CO-Evans Army Community Hospital Warrior Transition Battalion amp Tenant Units Landstuhl GE-Landstuhl Regional Medical Center amp Deployed Warnor Medical Management Center Virginia Beach VA- Community Based Warrior Transition Unit
Camp Shelby MS-Joint Force Training Center Medical Task Force Shelby
6 Observation Format
This docoment COlltains infonuatlon EXEMPT FROM MANDATORY DISCLOSURE tmder DIe FOIA ExeMption 5
FOR OFFICIAL USE ONLY
F-3
DlssRnatioA is plOhibited ecept BS aulonzes by AR 20 1
The inspection team addressed its findings in this report using the following format
Observation I Root Cause I Recommendation(s) I Discussion I Standard(s)
7 In the report quantitative terms such as few some many and mosf are used to describe percentile ranges of personnel interviewed and sensed The terms also represent a percentile of units organizations inspected linked to specific findings or observations The team used the following thresholds throughout the report
None Few Some Half Majority Most All
0 1 - 25 26 -49 50 51 - 75 76 - 99 100
This doctlmerrt contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ElEempliefl 6
FOR OFFICIAL USE ONLY
F-4
DlssemiAstioo is prohibited eJfGept as authoFRed by AR 2Q 1
THIS PAGE INTENTIONALLY LEFT BLANK
This document cClfttains iflfelmatieA EXEMPT FROM MANDATORV DISCLOSURE under theFOIA Exempti()fI 6
FOR OFFICIAL USE ONLY Dissemindafl is pmhibiled
exeept as autheri2ed by AR2()1
F-5
THIS PAGE INTENTIONALLY LEFT BLANK
This document contains information EXEMPT FROM MANDATORY DISCLOSURE under the FOIA ampemptioo 6
FOR OFFICIAL USE ONLY OiseemiAatian is prohibited elCeep 8S atfthCriEed by AR 29-1
Appendix 1
SAlG--ZX
DEPARTMENT OF THE ARMY OFFIce OF THE INSPECTOR GENERAL
1700 AfWI PENTAGON WASHINGTON DC 203101700
MEMORANDUM FOR CHIEF INSPECTlONS DIVISION DAIG
JAN 27 2Dl0
SUBJECT Directive Inspection of the Warrior Care and Transition Prog~am
1 You are directed to conduct an inspection of the Warrior Care and Transition Program
2 This Inspection will focus on the following objectives
a Assess implementationand oversight of policies and procedures for the US Army Warrior Care and Transition PrOgram
b Assess Warrior Care and Transition support systems for Soldiers and Family members
c Assess tools and processes implemented by Commanders to manage Soldiers
who are Medically Not Ready
3 YQIJ arealsO directed to conduct a special interest item (811) inspection of the Comprehensive ~ldier Fijness PrOgram The 811 will discusS the effectiveness and understanding of ttle program at the unit level This teport will be provided in a separate memorandum
4 By direction of the Secretary of the Army you are authorized unlimited access to Army activities and ~rsonnel locations organizations and documents to ensure the successful accomplishment oftf)is assessment Additionally you are authorized to coordinate with o1her services and Joint Staff for assistance documentatiOn and Infomiadon that may assist in completing thi~ asse$Sment
5 Byairedion ofSecretaryofthe Army you are autl1orized to task the PJrrY Staff and subordinate headquarterS as an approved exception to the HQDA Short Notice Tasking Policy dated 031353Z Jan 01
middot6 You will provide me a report at the conclusion of the inspection
Q~~ R STEVEN WHITCOMB Lieutenant General USA Thel~rGenend
Appendix 2
- fljeWS
Depatftent of the Army Inspector General- INSPECTIONS OSION
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
=============================-=============================== 1 FOROFFICtAL tf9E ON LV
Thl8 ecumet eomaln nfofItIon wt1lch Is EllS M8ndatoty Dlsclostlre tinder the Freedom of 1108110 Aot Dlssemlnatlon8 prohibited Gee Btl authorlnd by AR 20 1
j m f _ bullbullbull 44
Deparlflent of the Army Inspector General INSPECTIONS DhllSION
Purpose
To provide an overview of observations and recommendations from the in$pection of the
Warrior Care and Transition Program
FOR OFFICIAL IJSE ONLY bull
2
This eeUlfteM eentllline Infenftation which Is Exempt fro Mandatory Dlscloaure uncler the Freedom of Information Act DlslRlmlnation Is p~hlbllecl except illS authorlnd b AR-fO+-
4yenW6ampMi
MS ampI M yenMO- 5MlsectiMF 3yenW
Depsrtillent of the Army Inspector General- INSPECTIONS iJntSION r
Agenda
bull Inspection Objectives
bull Inspection Data and D~mographics
bull Inspection Timeline
bull Bottom Line Up Front bull Objective 1 Observations (14) bull Objective 2 Observations (3) bull Objective 3 Observations (7)
bull Other Matters (5)
bull Positive Notes
=======================================================1 3 FOR OFFIGIAL USE ONLY
rhla deGllme GEI_I_ Infermlltlon which I Exempt from Mandatory Olaclosure under the F dom of Iro mallol Act Dissemlilatlon Is prohibited except 88 8l1ttOl Ibid bV AR 20middot1
Departent of the Anny Inapector Generalmiddot INSPECTIONS OnISION
Inspection Objectives 1 Assess implementation and oversight of pOlicies a~d procedures for the US ArmyWarrlor Care and Transition Program
2 Assess Warrior Care and Transition support systemsfofSoldiers and Family members
3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not ~eady
4 Synchronized the Inspection of Warrior Care and Transition Program with GEN(R) Franks RC Medical Process Review TF (VOCO)
Total Contacted
bull Contacted 2122 Service Members Family members civilians and leaders through interviews and sensing session
Agencies Coordinated
bull GEN(R) Franks RC Medical Process Review TF bull Warrior Transition Command bull Northern Regional Medical Command bull Southern Regional Medical Command bull Western Regional Medical Command bull European Regional Medical Command bull Forces Command bull G1 I Human Resources Command
Sites Visited
bull Walter Reed Army Medical Center DC o Fort Sam Houston TX bull Fort Bliss TX bull Fort Benning GA bull Fort Ja~kson se bull Fort Eustis VA bull Fort Meade MD bull Fort Dix NJ bull Camp-Robinson AR - CBWTU
FOR OFFIOIAL liSE ONLY
bull Fort Gordon GA bull Fort Bragg NC bull Fort Carson CO bull Concord MA - CBwrU bull Fort Sill OK bull Landstuhl GE bull Virginia Beach VA - CBwrU bull Camp Shelby MS
4
This tOtacwmet G8AampaIRIIlnfermatien whle 1amp sempt from Mandate Disclosure under the Freedom of Informatton Act Diseerninatlan 18 profollblted except a~ortzed by AR 11
Depllrtrllent qf the Anny Inspector General-INSPECTIONS )nIISION
WTU Inspection Data and D~mographics Total Contacted 2122
Interviews 405
Sensing Sessions 114
Documents Reviewed
Comprehensive Transition PlansAutomated CTP WTUSOP WTB Enhanced Discharge Plan USRlMEDPROS DATA Draft Squad Leader Handbook Cadre Training ScheduleClass Surveys Warrior Handbook SFAC SOPAW2 PacketUsage Local Draft Elective Surgery Policy
Observations
Rank E1-4 E56 E7 E8 E9 WOi
Peonnel 397 462 208 109 52 5
CBwrU Command and ControlSOP WT Intake Packet PEBLO Soldier Briefing Centralized Wru Transfer Process SOP Behavioral Health Care Management SOP CBWTU Patient Administration Discharge SOP 4th 10 Master ResilienceTraining Program WTB Spouse Orientation Guide DWMMC Movement and Orders SOP
Cadre Training Center for the Intrepid SFACslWarrior and Family Support Center CTP Approval ProcessAutomated CTP TRIAD of Care Meeting WTU Barracks
CW3 ew~ 012 06 elv
8 6 35 65 371
FAM Total
10 85 2122
==========================================================~======~==========I 5 FOR ClFRGIAl USE eNLV
1hl8 aolilumem lila_IRs Information ~Ieft Is amp fteftt MnfJatert Dlacloaur under the Freedom of InfonnatJon Act Dissemination Is prohibited except alii etfthorllllld br AR21M
Departrllent of theAmJy Inspector General-INSPECTIONS OnSON
Historical Timeline of Warrior Care and Transition
Oct 2009 - NOAA 10 Continuation an AD for RC Service Members during POES following MOB and Deploymen
Oct 2009 - WCTP Policy Memo 09-002 Warrior Transition Review Board CTRB) Procesa
Mar 2009 - MEOCOM Policy 09-011 Comprehensive Transition Plan Policy
July 2009-ALARACT 2102009 SCa approve all cadre assignments
May 2009 - FRAGO 4 published (Triad of Leadership transfers to CBWTU and created the Transition Review Board (TRB))
Jul 2008 bull FRAGO 3 published revised entry crltsrla
Jul 2008 - OTSGlMEOCOM Policy 08-028 i Access to Care $tandards for AD Service Members
Dec 2001 - FRAGO 2 publlshedj directed SCs to meet FOC requirements forWTU
Oct 2007 - G1 publishes Consolidated Guidance
FY 2007 - FY 2008 WTU population grew from 6K to 12K (steady state now 9K plus) Aug 2007 - FRAGO 1 published eetabllshed WTU C2 functions and Institutionalized structure
Findings by Internal Review Group TSG strengthens managed ca
Jun 2007 ~ OPORD 07-65 Army Medical Action Plan (AMAP) published
Jun 2007 - WalTior Transition Units created to replace MRPUs
Jun 2007 - EXORO Healing Warrtore publlehed
Feb 2007 - Washington Post Arllclej InSignificant management of wounded and III at WRAMC
Dec 2003 - SECARMY created Community Based Health Care Organlzations (CBHCO) FORSCOM Is Executive Agent
FY 2004 - MHOs evolve to Medical Retention Processing Units (MRPU)
FY 2004middot ASA(MRampA assumed oversight of MHO
FY 2004 - Media outraged by care provided by Medical Holdover Operations (MHOs) at FortsStewart and Knox
FOR OFRGIAL USE ONI-
6
This dIMlY 8antaiM 11Ifeffft8tlon which e Exempt om Mandatory Disclosul tinder the Freedom of Information Act Dissemination Is plohlbltad except as authollud by Aft 20-1
H bull +w A
Departent of the Anspector General- INSPECTIONS D~tlISIOf1
Timeline of IG Inspection of Warrior Care and Transition
30 JUL - Report Approval -
19middot29 JULmiddot Finalize Report~ 19-29 JUL - Brief Stakeholders
27=30 JUN - Camp Shelby MS (DEMO 23-24 JUNmiddot Virginia Community Baaed WT Virginia Beach VA (CO)
21 JUL - Brief TlG
9middot14 MAY - Fort Cal8on CO (SN)
15middot19 MAR - Fort Sam Houston TX (BN
2-amp MAR -Walter Reed DC (BDE
3-7 MAY - Massachusetts Community Based WTU Concord MA (CO)
26middot30 APR - Fort Gordon GA (BN)
19-23 APR - Fort Bragg NC (BN)
5-9 APR - Fort Jackson SC (CO)
29 MAR - 2 APR - Fort Eustis VA (CO)
22-28 MAR- Arkaneas Community Based WTU Camp Robinson AR (CO)
15middot19 MAR bull Fort Bllas TX (BN)
2-6 MAR - Fort Meade MD (CO)
29 JAN -19 FEB - Final Coordination with DA Staff ACOMa DRUs amp Inatallatlons
2T JAN - Approved Inspector Generallnpectlon Directive
~ - Coordinating Site Visit to Fort Drum NY
22 DEC - Coordination Brief with Warrior Transition Command
FOR OFRGbL use ONLY Thla ~eellmAt eontaln81nformatlon which Is Exempt from Mandatory elcloBtll wilder the Freedoih of l fullliatJon Act Osemlnatlon II plohlblted except as authodzed by AR 28=1
f
Deparlrtent of the Army Inspector Genera- INSPECTIONS bnllSON
I
Bottom Line Up Front bull The concept of WTU works ~ operations are complicated by internal and external influences
bull This is a low-density high-visibility unit - every one wants to do the right thing for wounded Soldiers but o The mission is larger than just wounded Soldiers it includes ill and injured bull CongressionalMediaPublic misunderstanding of the population and mission bull Individual WT issues raised directly to Senior Leaders - marginalizes chain of command
bull The mixing of different populations of WTs has created leadership medical management public relations and small unit cohesion challenges
bull Soldiers are combat wounded (1000) evacuated diseasenon-battle injured (3700) command referred (33) and prepost-mobilization (20) - all are considered IIwounded warriors bull Combat wounded are easier to manage media misunderstanding of the pop~lation self segregating -population (caste system)
-Most Soldiers are receiving the best care and generally feel that the WTU Is the best place for themto heal and transition HOWEVER some Soldiers personal motivations are the driving factor
bull The program is focused on supporting the healing and transition of Soldiers o There isa noticeable sense of entitlement among some Warriors in Transition bull Reception processes entice some Soldiers into an unhealthy mindset to achieve personal gains
- No single synchronized source document outlining governing policies guidance and regulatory requirements -- DA EXORD w4 FRAGOs MEDCOM OPORD w46 FRAGOs Consolidated Guidance (Admin) 22ALARACTs 29 Policy Memos and 5 MllPEH messages
FOR OFFIGIAL USE ONLY
8
Ttl document eantel IAfarmatfon which I Exempt from Mandatory Ollllclosure under the Fu)edom of IlIfoliliatloll Act Dls lnatlon 111 prohibited except as authortZlld b AR 20middot1
Mt bullbull se bull fW
Department of the Army Inspector General-INSPECTIONS DnllSION
Bottom Line UmiddotpFront
bull FRAGO 3 and 4 WTU entrance c~iteria is vague and inconsistently applied bull Varied interpretation of complex medical case management leads to widely different entrance standqrds Entrance criteria for Reserve Component is a medical recommendationofdefini~ive healthcarefl
bull Army is faiiing to properly document line of Duty (LOD) for Reserve ComPonent Soldiers ~ critical to the follow-on care and transition for the RC Soldier
bull The intent and Implementation of the Comprehensive Transition Plan (CTP) is not being met bull Most WTs did not have a written transition plan (8000) bull Cornerstone of the Warrior Care and Transition program - roadmap to RTD or transition bull Expectation management - blending what the WT desires with the medical and military reality bull WTC implementing automated version since 9 July 2010
bull The ARFORGEN cycle exposes medical management challenges for units and MTFs bull The Army does not use common terms of reference to accurately describe Soldier status (availability vs deployability vs ready) o Profiling periods and medical boarding actions (MEBPES) are not synched with ARFORGEN cycle bull Army medical capabilities do not support the needs of the increasing MNRlMND population
FOR OFFlGbL use ONtO
9
11119 document contains Informatioll which I exempt fio1I Mandalol Disclosure allda Hie F_doIn of llifoilhatioil Act DeellllnaUOtIIB proldbll8d except bullbull autllollmd bp Aft2Ot
Depanment of the Army Inspector Genera- INSPECTIONS bftSION _ 1 bull bull
Bottom Line Up Front - Soldiers are disadvantaged by medical care priorities
- Enhanced access to care standards are forWTs and deploying and redeploying Soldiers - The numbers of medically not ready and medically non-deployable Soldiers are increasing in all components - The average stay for a Soldier who is return to duty from a WTU is just over 6 months however the average length of stay for all Soldiers who are medically released is over one year - Medical resources tied up for SoldierS who will not be returning to the fight
- Leaders are concerned about Soldiers that pes with known or unknown medical Issues bull Behavior Health Traumatic Brain Injury Post-Traumatic Stress Disorder often do not manifest for up to six months post deployment - Gaining units inherit Soldiers with unresolved medical issues from past deployments effecting unit readiness
- MEBPEB ineffiCiencies affect the Armys ability to meet the needs of Soldiers and the Army in a timely manner
-The majority of those interviewed stated that the MEB process is complex disjointed and hard to understand bull MEBPEB process average of 214 days (stats from 2009) bull Less than 10 of Soldiers in the MEBPEB process will RTD bull Medical staffing is insufficient to support timely MEBPEB processing
- Most healthcare providers estimate 25-35 of WTs are dependent on or addicted to drugs -over medicated abuse of prescriptions medication self medication and abuse of illegal drugs
FOR OFFIGIAL USE ONLY
10
Thte deeument ee_lna Infomlatlon which Is Exampt fronl Mandatory Dlsclo undat the FIHdam of Infonnatlon Act 0188emlnatlon 18 prohibited except 88 eUlhortl8d by AR H 1
~
G) t gt 0 Cii 11-
S ~ - Umiddot Q (I) ~ (f) 0 ~ i c u ~ 0 ~ -I
e til r II
() ~ e 0 GI
~ s -~ ~
q CD ~ a Got
i middotE i t Q
Eepartment of theAnny Inspector General ~ INSPECTIONS PHIISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 1 No single synchronized source document outlining governing policies guidance and regulatory requirements
RECOMMENDATIONS a OTSGMEDCOM Publish a single synchronized document to govern the Warrior Care and Transition Program
b MEDCOM Publish DA PAM in support of single source document standardizing WTU procedures
FOR OFFICIAL USE ONLY
12
nla ci8GllmeRt santalns IAfermatOA whleh 18 Exempt M~ underthe Freedom of InfcrmllUon Acto a mlnatlon Ie prohibited except 88 authorized bV AR 10 1
bull I ~ _ _ ~ ~ ~ bull bull bull ~ bull bullbull bullbullbullbull bull bull t I ~ _ bullbull ~ bull ~ bull ~ bull ~ bullbull ~
Department of the Army Inspector Genera- INSPECTIONS DIVISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of pollcies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 2 WTU fosters a focused environment of healing and transitioning however WT personal motivations may drive transition decisions
RECOMMENDATION OTSGMEDCOM Revise Warrior Care and Transition Program procedures to incorporate a sequential approach initially focusing on strengthening the incentives for Soldiers returning to duty ahead of disability-based compensati9n
-fOR OFFl61AL USE ONtf
13
1hl8 dOGumant aontal 18110 which I txmpt from Maridatcry Blscl08UIII allOOI the Feedom of Informatiu Act a lilatlon Is pi ohlbltad except as auttlOlred by AR 20-1
~ ~ _ lt _ ~ - bull - bull ~ bullbull ~ bullbull ~ ~~ ltI rmiddot - ~ ~~gt - lt - - - _ I - r bullbull
Department of the Army Inspector General INSPECTIONS DIlIISION ~ 5 to j bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 3 A mixture of combat wounded injured and ill Soldiers in the WTU has created perceptions leading to leadership medical management public relations and small unit cohesion challenges
RECOMMENDATION OTSGMEDCOM Determine messages and strategies to educate the Army and public on the Warrior Care and Transition Program
FOR OFFICIAL U8E ONIyen
14
This daGtlmeAt BBAtalM IAformatlen which Is Exemptfromlllandatocraquo 91sclo91i18 under the Feedom of Ifomtion Act BIs88mlnaiton 1amp prahlbltBd except as authorized by AR 29-1
M 11 SA
lit
Departlent of the Army Inspector Generalmiddot INSPECTIONS Oi 1fISION INSPECTION OBJECTIVE 1 Assess Implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
rtM~
OBSERVATION 4 Challenges exist to implement rapidly issuedchanging policy without the requisite resources
RECOMMENDATION OTSGMEDCOM lew ASA(FMampC) and IMCOM Ensure cost benefit analysis is conducted and appropriate resources are available for year of execution for WT policy requirements
-================================================================= 15 bill
FOR OFFICIAL USE ONLY This deGumltt eOReablnfermatlen which 8 Exempt -om Mandatory Disclosure unde the Freedom of Information Act DI8semination Is prohibited ICC_ _ authorized AR 28-1
Deparltrnt of the Army Inspector General- INSPECTIONS OnllSON 3
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program iBE~ BI
OBSERVATION 5 Subordinate commanders and some healthcare providers consider FRAGO 3 WTU entrance criteria to be vague and inconsistently applied
RECOMMENDATIONS a OTSGMEDCOM Define complex medical care extensive and clinical case _ management definitive healthcare and standardize screening criteria for entry into the WTU to address medical condition for all COMPOs
b ASA(MampRA)G1 Consolidate MRP-E MRP MRP2 and ADME into one order similar to COMPO 1
-FOR OFFICIAL USE ONLY
16
This document caRtaI iRkImutUen which 18 eMptM Mandatory Disclosure under the Freedom of Illfonnation Acplusmn-DInandnation 18 prohibited except I authorbed ~ AR 29-1
Departnent of the Army Inspector General- INSPECTIONS D IfISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 6 MEDCOMJs accountability processes for Soldiers evacuated out of theater result in immediate acceptance into the wru without meeting FRAGO 3 screening criteria
RECOMMENDATION OTSGMEDCOM Develop a standardized processto evaluate Soldiers evacuated from theater to determine if they meet WTU entrance criteria
f~ ~ ==================================================================17 (~~Imiddot ~It~
Q~0 ~ltj- I
FOR OFFIClALU9E ONLY 1lI1 document contains Information whloh Is Eu lram Mandatory OIcl08t1~ unde the Fraadom of IAfermeUoft Act OlaaemlfteUoft I prohibited 8xeept 89 8utholind by AR 29 1
Deparfnent of the Army Inspector General-INSPECTIONS DIviSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of PQlicies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 1 Most WTU cadre are concerned with inconsistencies in determining the Medical Retention Decision Point (MRDP)
RECOMMENDATIONS a OTSGMEDCOM Redefine the MRDP to be more clear concise and proscript~ve develop a standardized metric for assessing the MRDP establish reporting requirements for Soldiers being treated for more than one year without reaching the MRDP
bOTSGMEDCOM Develop and publish standardized elective proceduresurgery policy
cOTSGMEDCOM Develop and publish policy regarding treatment of additional medical conditions subsequent to admittance into the Warrior Care and Transition Program (WCTP)
=============================================================1 18 FOR OFFICIAL USE ONLV
~ ~OCNmnt eOlllell I etlon which Ie E bullbull mpt ffem laquolatelY Dl9olOGlIf8 under the Freedom of Information Aet Dlnemlation Ie prohibited IIJlcapt 88 eutholl2ed by AR 29middot1
Deparlment of the Anny Inspector Generalmiddot INSPECTIONS D viSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 8 Selection of WTU Cadre shifted from best qualified to 4good and first available
RECOMMENDATIONS a ASA(MampRA)G1 ICW OTSGMEDCOM Add WTU Cadre eligibility requirements to AR 614-200 Enlisted Assignment and Utilization Ma~agement AR 614-100 Officer Assignment Policies Details and Transfers
b ASA(MampRA)G1 Implement a selection process for WTU cadre commensurate with other Special Duty assignments (Recruiter Drill Sergeant) for all COMPOs
============================================================= 19 FOR OFFlelAL USE ONLY
ThIe deeum aentalslfemletlon which I Exempt flom Mandato Blactostlle under tfle Ffeedom of Information Act Dlaaaminalfon Is pnOll blled except as authorlmd by AR tomiddot1
Departluent of the Army Inspector General- INSPECTIONS InflSON
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 9 The current WTU classroom-centric and theory-based instruction does not adequately prepare the cadre to perform their duties
RECOMMENDATIONS a OTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of prescription medications
b OTSG(MEDCOM Require cadre training prior to assignment to WTU and implement sustainment training
c OTSGMEDCOM Require WTU Primary Care Managers to attend cadre training within 30 days of assignment
d OTSGMEDCOM Provide a leaders guide to address Warrior in Transition processes and policies
FOR OFFIOIAL tl9E ONLV
20
This document cOlltallllllllfoliilulion which 18 Exempt flom Mandatory DISC_UN udertlle Freedom of Iormlltlon Act Dlaaamlotion Ie rohlblted exoept as autherlzed ~ leR 20 1
_-----------
Department of the Army Inspector Generalmiddot INSPECTIONS DnllSION bull bull
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedUlres for the United States Anny Warrior Care and Transition Program
OBSERVATION 10 Most WTUs visited are not meeting the intent and
implementation of the Comprehensiv~ Transition Plan (CTP)
RECOMMENDATION OTSGIMEDCOM Provide policy and guidance to support automated CTP and enforce the implementation and execution
FOR OFFIOIAL USE ONLY
21
s laquotoGument G811IAa IRfGrmatien whletl 1amp EQmpt from Mandatory Disclosure tinder the Freedam af InformatlCln-Act--pound)lIaemlnatJon Is prahlbHlad ~Pt as atdtoorlzad by AR 20
Deparlnltmt of the Army Inspector General- INSPECTIONS Dr tYSION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of P9licies and procedures for the United States Anny Warrior Care and Transition Program
OBSERVATION 11 Most Warrior Transition Units have not implemented the Transition Review Board (TRB)
RECOM~ENDATIONS
aOTSGMEDCOM Enforce the implementation of the TRB and consider conducting the TRB for every WT at each 180 day period
b OTSGMEDCOM ICW ASAMampRA)G1 establish reporting requirements of TRB results
c OTSGMEDCOM Assess the feasibility of combining the TRB and the CTP
============================================================= 22 FOR OFFIOIAL USE ONLV
This deGumeAt Gentsl InyenollllMioft which Is eaempt from Mandato Dhltl08ura under ttle Freedom of 1lomlaHo Act Dissemination Is prohibited except as Authollmd by AR Ie-i
Department of the Army Inspector Genel8- INSPECTIONS DnISION
INSPECTION OBJECTIVE 1 Assess implementation and Qversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 12 Army-wide specialty care shortages exist in Behavioral Health Occupational Therapy and Physical Therapy and contribute to delays in
Soldiers treatment and healing
RECOMMENDATIONS
a Army G3517 lew OTSGMEDCOM validate Manpower Requirements Criteria for healthcare services personnel
b ASA(MampRA)G 1 ICW G357 and OTSGMEDCOM review TDA structurestaffing requirements for the specialty care providers (BH OT PT) and develop staffing actions to address shortages
c ASA (MampRA)G1 ICW G3517 and OTSGMEOCOM confirm salary competitiveness among behavioral specialists
=========================================================== 23 FOR OFFICIAL USE ONlf
Tille deewm aentalna Infemlatfon wtllch Is Emn Ipt from Manaatoty Disclostira tinder the rreedcn of Ifalinallol I Act DI88111111allon Is pi ohlbltad bullbull capl as autilollDld b AR 20middot1
bull Department of the Army Inspector Geeramiddot INSPECTIONS DivISION
INSPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 13 Army is failing to properly document Line of Duty (LD) for Reserve Component Soldiers - critical to the follow-on care and transition for the RC Soldier
RECOMMENDATIONS a ASA(MampRA)G1 Publish message to commanders emphasizing required completion of LD for RC Soldiers prior to REFRAD
b ASA(MampRA)G1 lew ARNGOCAR and T JAG ensure education and training tools for LD administrators are available to units prior to and during deployment
c OTSGMEDCOM Adopt LD module in MODS as the Armys dedicated line of duty tracking system
=========================================================== ~ FOR OFFIGIAL USE ONLY
This deeU8l8M contains Informatloll which Is Exen1pt from Mandato Disclosure unclel the Freedom of Iromtlon Act Dla_mlnden la prohibited except a authorized b AR 20-1
Departnnt of the Army Inspector General- IN$PECTIONS OnSON
I~SPECTION OBJECTIVE 1 Assess implementation and oversight of policies and procedures for the United States Army Warrior Care and Transition Program
OBSERVATION 14 Perception that Warriors in Transition are not held to same standards of discipline as required of other Soldiers
RECOMMENDATIONS a OTSGMEDCOM ICW T JAG emphasize the importance of maintaining good order and discipline and ensure WTs are held to the Army standards of discipline
bOTSGMEDCOM Implement training that is scenario-based deals with behavioral health issues and includes side effects of commonly prescribed prescription medications
_===============================================================1 25 FOR OfFlGIAL use ONLf
ThIs doeumeftt eontalns Infonnatlon which I Exeiiipt IOiil Plandatoly Oludo_u blldai the FntedOIh or ItifOliliatlon Act Ollsamlnation prohibited bull capt atithOltHd by AR 10-1
N (J)
gt (J CD ~
Q
0
Department of the Amrylnspector Generalmiddot INSPECTIONsqlllS9N
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 1 Soldier and Family Assistance Centers (SFAC) are underutilized however they provide WTs with a level of personal service and an environment conducive to their medical and transitional needs Most SFACs encounter near-term resource challenges (facilities funding and staffing)
RECOMMENDATIONS a IMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b IMCOM ICW OTSGMEDCOM and ASA(FMampC) Ensure resources are provided for-year of execution policy requirements (zero sum game)
FOR OFFIelAL USE aNt
27
Thle deOtlmeAt aORtal Infolmfllloll which Is Eltempt from Mandetoty Olcto8ul8 under Fredam of InfonnlltJon Ad DI8emRBtIeA I prehlblted GlCe_1tt 8IJ authertnd by AR 28 1
M
Department of the Army Inspector General INSPECTIONS DnllSON
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION -2 Providing services for COMPO 23 WTs and Families is challenging due to the dispersion of state resources
RECOMMENDATION OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG OCARand Army PAO Establish a steering committee to determine most effective methods to deliver information and services to COMPO 23 WTs and Families
================================-================================ 28 bull FOR OFFICIAL lISE ONLV_
l18 deGumAt malna IAfatlen-whieh Exempt from Mandetaroy Discl08ure under the Freedom of Information Act Dissemination Is prchtbltad except liS authorized by AR 20middot1
Depattnent of the Army Inspector Gene INSPECTIONS poundIIl11SION
INSPECTION OBJECTIVE 2 Assess Warrior Care and Transition support systems for Soldiers and Family members
OBSERVATION 3 Communities outside the gate are beginning to selectively support only combat-wounded WTs with incentives resulting in non-standardized practices across installations
RECOMMENDATIONS a OTSGMEDCOM Determine messages and strategies to educate the Army and public on the War~ior Care and Transition Prog ram
b OTSGMEDCOM Establish policy standardizing acceptance of community incentives
FOR OFFielAL USE eNLV
29
This documeAt contains Infomlatlen willa I ampKmp from Manllaterv Oleclosul8 uncler ttl Freedom of Information Ad Olumlnatlon Ie prohibited except as aathotzed by AR 2CP1
fI)
CD c gt 0 - _ CI) +If ~ () Q CI) (I) c 0 0 i ()
~ 0 ~ -I -e
CD c CD
() ~ s Co) CD
t s ~
oct ~
E 0 -c CD
~ ca B-tl
Departint of the Army Inspector General- INSPECTIONS iJnIISON
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 1 The Army does not use common terms of reference to accurately determine stat~s of medically not ready medically non-deployable and not available Soldiers
RECOMMENDATION OTSGMEDCOM ASA(MampRA)G1 f G357 ICW FORSCOM Standardize terminology for Soldier medical readiness status
FOR OFFICIAL USE ONLY
31
This doculMnt eo_ Information wtllch 18 Exempt 0111 Mandatory Dlsctoeu under the Freedon of Information Act Blasendllation 18 prot1lblted except aa 8oUIOrzed bJ AR 20middot1
Depnent of the Army Inspector General - INSfECTIONS 1)(~lRN II
INSPECTION OBJECTIVE 3 Assess tools and processes Implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 2 Army medical fitness determination processes have not kept pace with ARFORGEN requirements
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 G357 and FORSCOMExamine medical support needs of the ARFORGEN cycle to determine processes that can best support the needs of the Army
b ASA(MampRA)G1 Code Soldiers in MEB process as a Iossn allowing for replacement requisition
cg
FOR OFFfGlAL liSE ONlV
32
-lbl dOGyment eontalna-informaton Which Is ElCelftit 1ft Mandatory Disclosure under the Fntedom of Information Act DIsemlnatlon Is ISrohlblted ampXCelSt lUll atfthlllrlnd by AR 20+-
r
Department of the Army Inspector General- INSPECTIONS D (fISION
ARFORGEN (AC) Timellne Compared to Hypothetical Administrative TImeline In AR 40-501
Reset Pool
o RSRP o Soldier-family reintegration o Block Leave o Unit Reconstitution o Individual Training o Institutional Training o Receive New Personnel and Equipment 6 m nths
Train I Ready Pool
o Individual Training o Collective Training
12 months
ent Profile
o Deploy o Exercises lt) Available for World-wid deployment
RTD or Discharge
Temporary Profile (1- 2 Months) MMRB (3 Months) M IPEB Average (7+ Months)
Temporary Profile MEBIPEB
Temporary Profile
Temporary Profile MMRB
MEBIPEB
FOR OFFICIAL IJSE ONLV
33
1=hle document centellnformattofl which Is Exempt from Mandatory Bleclosule alider the Fleedo of Information Act Dlasemlnattonla prohibited except as authorized by AR 2Gw1
Department of the Anny Inspector Generalmiddot INSPECTIONS DlfIISION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 3 Army medical capabilities do not support the needs of the MNRlMND in units
RECOMMENDATIONS a OTSGMEDCOM ASA(MampRA)G1 and OCAR Conduct feasibility assessment to determine requirements and implementation strategies for a temporary increase in medical assets to mitigte current limitations
b OTSGMEDCOM Establish Installation Medical Management Center (IMMC) pilot site for a next deploying RC brigade to as~ist i~ managing MNRlMND Soldiers
-FOR OFFl91AL ~6E 9NLY
34
TRIG document eon Informe60n which Is Exllmpt from Mandatory DIsclollure under the Freedom of Information Ael 018180011 IG prohibited eWieept 8S auttlorlred by AR 20 1
bull Wi BM
Departillentof the Army Inspector General - INSPECTIONS u)tlSON
INSPECTiON OBJECTIVE 3 Assess tools and processes implemented by Com~and~rS to manage Soldiers who are Medically Not Ready
OBSERVATION 4 Current medical priorities do not assist commanders in maintaining a fit fighting force that is medically ready to deploy
RECOMMENDATION OTSGMEDCOM ASA(MampRA)IG1 and G357 Conduct a comprehensive MNRMND support needs study to determine if medical priorities are correctly synchronized and applied
FOR OFFICIAL USE ONLY
35
This deetlmant eantaiHII Inomatio which Is Exempt from Mandatory Disclosure und8r the Freedom or Iilformatlon Act 0101l8mllo Is prohibited el(~8pt 811 authorized by AR 20middot1
yenfi bull
Department of the Army Inspector General-INSPECTIONS OUhSION
INSPECTION OBJECTIVE 3 Asse~s tools and processes Implemented by Commanders to mflnage Soldiers who are Medically Not Ready
FMW
OBSERVATION 5 Leaders are concemed about Soldiers that pes with known or unknown medical issues particularly behavioral health issues (TraumatiC Brain Injury and Post-Traumatic Stress Disorder)
RECOMMENDATION ASA(Mamp RA)G1 lew OTSGMEDCOM Enforce compliance with AR 40-501 11-4a (3) updating of MEDPROS commanders must
emphasize medical in-processing to capture profile limitations and acknowledge Soldiers recent past deployment history
FOR OFFIOIAL USE ONLY
36
Thle GlGllum eGRtalBlnformatto hleili Exempt from Mlmctatory OIeol tinder the Freedom of Informatloll Act 01 ml8tlo 8ptohlblted alCCapte IltIttlortlNd by AR 20-1
bull
Department o~ the Army Inspector General-INSPECTIONS DlfllSION
INSPECTION OBJECTftVE3 Assess tools and processes implemented bymiddot Commanders to manage Soldiers who are Medically Not Ready
iii -
OBSERVATION 6 Soldiers in the MEBPEB process that are not assigned to a WTU are disadvantaged from a lack of information lower priority in access to care and length of MEB I PES process
RECOMMENDATION~ aIMCOM Conduct cost-benefit analysis to determine if SFAC services can be available to all Soldiers in the MEB process
b OTSGMEDCOM Make all MEB Soldiers same priority in access to care as WTs
c OTSGMEDCOM Clarify the Medical Retention Decision Point (MRDP) in order to enable to the MEBPES process to begin sooner
FOR OFFICtAL USE ONL
37
This deeument contains fonnalon whldl Is Emrnpl flom Mandaluiy Disclosure undar the Feadom of Infolillattoll Act Dissemination Is protllbibiJd except aa authorized by AR 20-1
Nt
Department of the Army Inspector Genera- INSPECTIO~S unliSION
INSPECTION OBJECTIVE 3 Assess tools and processes implemented by Commanders to manage Soldiers who are Medically Not Ready
OBSERVATION 7 IRR Soldiers are often not identified as non-deployable until they reach a mobilization platform approximately 42 days or more after recalled to active duty
RECOMMENDATION ASA(Mamp RA)G 1 HRC ICW ARN~ and aCAR Ensure that IRR Soldiers receive a theater-specific SRP during mobilization prior to attending WIT MaS training and assignment to a deploying unit
==================================~======================== ~ FOR OFFIOIAl USE ONLY
Thle deellmanl eSIMI_lnformatlon whichs Exempt fro Mandelory Disclosure under the FlGGdolh of luforma1Jon Act 018semlnatlon 18 prohibited Idcep a8 ItCthorized by AR 2amp-1
Department of the Army Inspector Genera- INSPECTIONS DlfiSION
Inspection Observations - Other Matters OBSERVATION 1 Leaders health care professionals and Soldiers stated that MEBPEB inefficiencies affect the Armys ability to meet the needs of Soldiers and
the Army in a timely manner
RECOMMENDATIONS a OTSGMEDCOM Continue implementation of recommendations provided by GENR) Franks Task Force
b OTSG~EDCOM Develop and publish standardized elective proceduresurgery policy
c OTSGMEDCOM Re-evaluate MEB physician ratios and ensure local MTF recruits hires and trains new PEBLOs to meet requirements
d OTSGMEDCOM Coordinate with VA (DES) to reduce amount of time between final appointments and return of medical findings report to the MEB
~ ~ 7 __ 1
========================================================== 38 FOR OFFICIAl leE ONLyen
TN9 document contain Intonnation which Is Exvrnpt flol1l Mandatory DlsclosQu ande the Freedolll of olillalion Act D8semllalOft 18 prohibited eCGIt8 authOrized by AR 21)1
Department of the Anny Inspector General- INSPECTIONS DIfIlSION
Inspection Observations - Other Matters
OBSERVATION 2 Limited andor no interoperability between DoD (AHLTA) VA (VISTA) TRICARE network and civilian provider information systems
RECOMMENDATION OTSGMEDCOM Improve the interoperability between DoD (AHLTA) VA (VISTA) and TRICARE network information systems
============================================================= 40 FOR OFFICIAL USE ONLY
Thll docYmen oentaln InformaUan which 18 EMlftpt 1ft Mend_IV Dlllcl09l1N lInder the FlIII8dam eflnfellllatien AM DlatJemlnation 18 prohibited oeept eutholfnd bv AR 20-1
aMmiddot
Department of the Army Inspector Generalmiddot INSPECTIONS DnIlSON bull
Inspection Observations -Other Matters
OBSERVATION 3 COMPO 23 are not longer a strategic reserve current Army resources appear to-be insufficient to medically sustain RC in an operational environment
RECOMMENDATIONS a OTSGMEDCOM and ASA(MampRA)G1 ICW IMCOM ARNG and OCAR and Army PAO EstsQlish a steering committee to conduct gap analysis and provide recommendations to address RC medicalmiddotcare requirements as an operational force-
b OTSGMEDCOM ICW ASA(MampRA)G1 G357 ARNG and OCAR Resource annual medical screening for National Guard and Army Reserve Soldiers identified
for deployment
========================================================== ~ rOA ornCIAl USE ONLY
This dooumant lIeltal Infonnation which I Exempt from MandateI) DIsclosure under the Freedom of Information Act Blnemlnatlon Ie titbit Bcapt bullbull etithortHcl _ AA 2G t
amp
Department of the Army Inspector General-INSPECTIONS DlfIISION
Inspection Observations - Other Matters
OBSERVATION 4 The majority of medical management staff have some level of concern for personal safety in managing increasing numbers of Soldiers with behavioral health issues
RECOMMENDATION IMCOM ICW OTSGMEDCOM OPMG and USACE Identify threats to personnel safety (facilities and operations) and implement safeguards as necessary including awareness training
FOA OFFIGlAL USE ONLY
42
Thill doeumeltt contains Information which I Exempt fmn Mandatory DIclasa und bullbull tlMil Freedom 0 Information Act Dissemination II protllbltad exceplas atlthorlzed by AA 2emiddot1
Department of the Anny Inspector Genera- INSPECTIONS DlrtlSION
I~spection Observations - Other Matters
OBSERVATION 5 Most healthcare providers interviewed (Primary Care
Managers Nurse Case Managers) estimate 25-35 of WTs are dependent on or addicted to drugs
RECOMMENDATIONS aOTSGMEDCOM Evaluate procedures for prescribing medication and consider expansion of the alternative medicine programs
b OTSGMEDCOM Expand residential dependencyaddiction programs and pain management programs to MTFs
c OTSGM EDCOM Assess the feasibility of providing a dedicated pharmacist at the WTU battalion and separate company level
=-===================-============================-=====-===== 4~ FOR OFFICIAL USE ONIoyen-
This document contains Information which Is Exempt fl 0111 Mandato Disclosue Illlder ttl Fleedom of Information Act Dissemination Is pt ohlblted except as atlthorlnd by AR 28-1
__ bull _---------------------------bull
Depanment of the Army Inspector General- INSPECTIONS DIVISION 7
Inspection Observations - Positive Notes
Positive Note 1 Some units impleme~ted pain and prescription management programs to assist in the reduction of medication dependency (eg Valter Reed Army Medical Center Fort Sam Houston Fort Bragg Fort Gordon)
Positive Note 2 Fort Braggs Focused Trarisition Review (FTR) is a multidisciplinary platform that combines features of the Comprehensive Transition Plan (CTP) with the Transition Review Board (TRB)
Positive Note 3 Fort Gordons Eisenhower Army Medical Centers in-patient subst~nce addiction program provides for more effective C2 and M2 of Soldiers with addiction diagnoses
Positive Note 4 4th ID Building The Soldier Athlete fitness program motivates MNDs focuses on abilities instead of disabilities
Positive Note 5 Fort Carsons Evans Army Community Hospital established robust Mobile Behavior Health Team (MBHT) as a single point of contact to improve mission readiness
========================================================= FOR OFAGIAL USE ONLY
=lhll document contains I fo iii_tim which t Exeliipt 0111 Mandator 51closare allder the Freedom of Information Act 51S bullbull mlltaUon Is pi ohlblbld except a aulftortmd by AR 21)oot
M
tHE bull r rWAessabee FPE Crt _ H middotNW-middotewelWfj
Department of the Army Inspector General INSPECTIONS DlfllSION ~ Of e
Final Brief to The Inspector General
Inspection of the Warrior Care and Transition Program
as of 21 July 10
==================================================================~ ~ 1middot FOR OFFle~ USE ONLY
Tilts dGGUlftanteeNaIllnformaUon which Is Exempt om Mandato 0110111 tinder the FI8edOl1l 0 IlItonatioll Act 01 118110 Is ptohtbtled except bullbull 8uthoriHd by Aft JOy I
App ndix 3
I
Warrior Care and Transition Program ABBREVIATIONS AND ACRONYMS
AM ADT ARNG Army Audit Agency Active Duty for Army National Guard
Training AC ASA(FMampC) Active Component AGR Assistant Secretary of the
Active Guard and Army for Financial ACAP Reserve Management and Army Career and Alumni Comptroller
Program AHLTA Armed Forces Health ASA (IampE)
ACEP Longitudinal Assistant Secretary of the Army Center formiddot Technology Army for Installation and Enhanced Performance Application Environment
ACOM ALARACT ASA (MampRA) Army Command All Army Activity Assistant Secretary of the
Army for Manpower and ACS AMAP Reserve Affairs Army Community Service Army Medical Action
Plan ASCC ACSIM Army Service Component Assistant Chief of Staff AIIIC Command for Installation Army Medical Center Management ASK
AMEDD(CampS) Army Satisfaction Key AD Army Medical Active Duty Department ATTRS
(CenterampSchool) Army Training ACME Requirements and Activemiddot Duty Medical APDES Resources System Extension Army Physical
Disability Evaluation BCT ADSM System Brigade Combat Team Active Duty Service Member APFT BH
Army Physical Fitness Behavioral Health ADSW Test Active Duty for Support BMM Work AR Borrowed Military
Army Regulation Manpower
C2 Command and Control
App3-1
CBHCO eTP DNBI Community Based Health Comprehensive DiseaseNon-BaitJe Injury Care Organizations Transition Plan
DOD eBwru DA Depa rtment of Defense Community Based Department of the Warrior Transition Unit Army DODD
Department of Defense CCIR DAIG Directive Commanders Critical Department of the Information Requirement Army Inspector 0001
General Department of Defense CLS Initiative Common levels of DAMEMO Support Department of the DRU
Army Memorandum Direct Reporting Unit COAD Continuations on Active DAMPS DWMMC Duty Department of ~he Deployed Warrior
Army Mobilization Medical Management CO-ADOS Processing System Center Contingency Operations Active Duty for DARNG EeT Operational Support Director Army Extended Combat
National Guard Training COAR Continuations on Active DeeS EPTS Reserve Deputy Commander Existed Prior To Service
for Clinical Services COTA ETS Certified Occupational DCG Expiration r Term of Therapy Assistants Deputy Commanding Service
General CONUS EXORD Continental US DCS Execution Order
Deputy Chief of Staff eSA FM Chief of Staff of the Army DEERS Field Manual
Defense Enrollment CSFP Eligibility Reporting FOC Comprehensive Soldier System Full Operational Fitness Program Capabilities
DES CSM Disability Evaluation FOIA Command Sergeant System Freedom Of Information Major Act
App3-2
FORSCOM IMA MACOM US Army Forces Installation Major Area Command Command Management Agency
MaDD FRAGO IMCOM Mobilization and Fragmentary Order Installation Deployment
Management Demobilization Gmiddot1 Command Division or higher MBHT personnel staffofficer IMMC Mobile Behavior Health
Installation Medical Team G-3 Management Center Division or higher MDMP operations staffofficer ING Military Decision Making
Inactive National Process G4 Guard Division or higher MEB logistics staffofficer IOC Medical Evaluation Board
Initial operational GS capabilities MEBITT General Schedule Medical Evaluation Board
IRR Internal Tracking Tool GWOT Individual Ready Global War on Terrorism Reserve MEDCOM
US Army Medical HIPAA ITO Command Health Insurance Invitational Travel _ Portability and Orders MEDIVAC Accountability Act Medical evacuation
JAG -HQDA Judge Advocate MEDPROS Headquarters General Medical Protection Department of the Army System
LD -HR Line of Duty MFLC Human Resources Military Family Life
LOS Consultants HRC Length of Stay Human Resources middotMILPER Command LPTA Military Personnel
Licensed Physical lAW Therapy Assistants MHO I n accordance with Metfical Holdovers
M2 ICW Medical Management In conjunction with
App 3-3
MMRB MRPU NMA MOSlMedical Retention Medical Retention Non Medical Attendee Board Processing Units
OCAR MMSO MTF Office of the Chief Army Military Medical Support MediCal Treatment Reserve OffICer Facility
OCONUS MNO MTOE Outside-of-Continental Medically Non Modification Tables of US Deployable Organization and
Equipment OEF MNR Operation Enduring Medically Not Ready NARMC Freedom
North Atlantic MOA Regional Medical OER Memorandum of Center Officer Evaluation Report Agreementmiddot
NARSUM OES MODS Medical Operational Data
Narrative SUf1mary Officer Education System
System NCM OIF Nurse Case Manager Operatio~ Iraqi Freedom
MOS Military Occupational NCO OJT Specialty Non-Commissioned On the Job Training
Officer MOU OMB Memorandum of NCOER Optimal Medical Benefit Understanding Non-Commissioned
Officer Evaluation OPORD MRDP Report Operations Order Medical Readiness Determination Point NCOES aT
Non-Commissioned Occupational MRP Officer Education TherapylTherapist Medical Retention System Processing (orders) OTSG
NCOIC Office of The Surgeon MRP-E Non-Commissioned General Medical Retention Officer in Charge Processing Evaluation PAC Pay (orders) NGB Pay amp Allowance
National Guard Continuation Pay Bureau
App 3-4
PAD PSG SOAP Patient Administration Platoon Sergeant Special Duty Assignment Directorate Pay
PTSO PAO Post Traumatic Stress SFAC Public Affairs Office Disorder SolQier and Family
Assistance Center PCM PT Primary Care Manager Physical 5l
TherapyfTherapist Squad Leader pes PennanentChangem RC SMC Station Reserve Component Senior Mission
Commander PO RD Position Description Rear Detachment SOP
Standing Operating POES REFRAO Procedure Physical Disability Release From Active Evaluation System Duty 5RP
Soldier Readiness POHRA RMC Processing Post Deployment Health Regional Medical Re-Assessment Command SW
Social Worker PES RRe Physical Evaluation Regional Readiness TBI Board Command Traumatic Brain Injury
PEBlO RTD TeS Physical Evaluation Return to Duty Temporary Change of Board Liaison Officer Station
5-1 POC Battalion or brigade TOA Point of Contact personnel staff officer Table of Distribution and
Allowances POM 5-3 TOY Program Objective Battalion or brigade Temporary Duty Memorandum operations staff officer
llTLE 10 POS S-4 Full-TIme Active Duty Point of Service Battalion or brigade (may be AC or RC)
logistics staff officer PPG MlE32 Personnel Policy Full-time Active Duty Guidance (ARNG only)
App3-5
~
TJAG USR WTe The Judge Advocate Unit Status Report Warrior Transition General Command
VA I TOA Department of WIT
Transfer of Authority Veterans Affairs Warrior Task Training
TPU VBA WTU Troop Program ~nit Veterans Benefits Warrior Transition Unit
Administration TRADOe US Army Training and VeSA Doctrine Command Vice Chief of Staff of
the Army TRB Transition Review Board VISTA
Veterans Health TSGLI Information Systems Traumatic and Technology Servicemembers Group Architecture Life Insurance
WCfP UtC Warrior Care and Unit Identification Code Transition Program
USARC Wli US Army Reserve Wounded ill and Commander injured
USAREUR WRAMC US Army Europe Walter Reed Army
Medical Center UCMJ Uniform Code of Military WRMC
Justice Western Regional Medical Command
USAMAA US Army Manpower wr Analysis Agency Warrior in Transition
USARC WTe US Army Reserve Warrior Transition Command Brigade
use United States Code
App3-6