universal adhesives universal adhesives: the next ... session/2019/ha… · demineralized enamel.2...
TRANSCRIPT

15www.compendiumlive.com January 2015 compendium
T he development of practical adhesive dentistry can be traced to Dr. Michael Buonocore who, in 1955, discov-ered he could increase the retention of acrylic-based restoratives by first treating the enamel with phosphoric acid.1 Subsequent research by Buonocore, Gwinnett, and
Matsui elucidated the mechanism of adhesion as micromechanical attachment via resin infiltration and tag formation within the acid-demineralized enamel.2 While long-term bonding to phosphoric-acid–etched enamel surfaces has proven to be highly reliable and predictable, long-term bonding to dentin has been considerably more problematic. This is largely due to morphologic, histologic, and compositional differences between the two substrates.3 For one thing, dentin is a vital, dynamic, and highly variable substrate. Superficial, middle, and deep dentin can vary significantly in structural, physi-cal, and chemical composition. Enamel, conversely, is quite con-sistent throughout and is also considerably more mineralized than
dentin. The inorganic content of mature enamel is approximately 96% hydroxyapatite by weight; the remainder consists of water and organic material. Dentin, on the other hand, is approximately 70% hydroxyapatite by weight, 18% organic material (predominantly type I collagen), and 12% water.4,5 These percentages are not consistent and can vary significantly depending on several factors, including dentin depth, age of the teeth, and history of tooth trauma and/or pathology. This, coupled with the relatively high water content of dentin, presents a significant challenge for consistent and reliable long-term adhesion.
The few available adhesive systems of the 1970s and early 1980s were relatively hydrophobic in nature and unable to adequately pen-etrate the dentin smear layer, thus limiting their direct interaction with the tooth tissues. The smear layer is the residue that is left on the surface of the dentin after rotary instrumentation with diamond or carbide burs (Figure 1). It is a thin amorphous layer largely composed
Abstract: Every so often a new material, technique, or technological breakthrough spurs a paradigm shift in the way dentistry is practiced. The development and evolu-tion of reliable enamel and dentin bonding agents is one such example. Indeed, the so-called “cosmetic revolution” in dentistry blossomed in large part due to dramatic advances in adhesive technology. It is the ability to bond various materials in a reasonably predictable fashion to both enamel and dentin substrates that enables dentists to routinely place porcelain veneers, direct and indirect composites, and a plethora of other restorative and esthetic materials. In fact, the longevity and pre-dictability of many (if not most) current restorative procedures is wholly predicated on the dentist’s ability to bond various materials to tooth tissues. Adhesive systems have progressed from the largely ineffective systems of the 1970s and early 1980s to the relatively successful total- and self-etching systems of today. The latest players in the adhesive marketplace are the so-called “universal adhesives.” In theory, these systems have the potential to significantly simplify and expedite adhesive protocols and may indeed represent the next evolution in adhesive dentistry. But what defines a univer-sal system, and are all these new systems truly “universal” and everything they are claimed to be? This article will examine the origin, chemistry, strengths, weaknesses, and clinical relevance of this new genre of dental adhesives.
Universal Adhesives: The Next Evolution in Adhesive Dentistry?Gary Alex, DMD
• discuss the history of the
development of adhesive
dentistry
• define what constitutes a
universal dental adhesive
• describe the chemical
makeup of this new cat-
egory of universal dental
adhesives
• identify clinical issues
that need to be con-
sidered when using a
universal adhesive
leArninG objectives
continuing education 1UniversAl ADhesives
16 Volume 36, Number 1compendium January 2015
continuing education 1 | Universal adhesives
of degraded collagen, bacteria, and various inorganic dentin and enamel debris.6,7 Early adhesive systems were extremely limited and generally ineffective, in part because they bonded directly to the smear layer and were, thus, limited by the smear layer’s low intrinsic cohesive strength.8 Eventually, it was recognized that the smear layer needed to be removed and/or modified and bypassed in some fashion so that adhesive primers and resins could interact directly with the dentin. In the case of total-etch adhesive systems, the smear layer is essentially dissolved with phosphoric acid (H3PO4) and subsequently washed away during the rinsing step (Figure 2 and Figure 3). With self-etching systems, various acidic primers are used to modify, dis-rupt, and/or solubilize the smear layer and, although the remnants are not washed away as with total-etch systems, still permit direct adhesive interaction with the dentin substrate.9
The acids and/or acidic primers and conditioners used with ei-ther total- or self-etching bonding systems do not just remove and/or disrupt the smear layer but create a thin zone of demineraliza-tion, exposing collagen fibrils that are either subsequently (total-etch) or concurrently (self-etch) infiltrated with various functional and cross-linking primers and resins. One of the goals in developing a successful adhesive interface is the infiltration and penetration through this acid-demineralized zone with various primers and/or resins that can be subsequently polymerized by light and/or chemical curing mechanisms. It is this thin layer of resin-infiltrated dentin, first described in a classic 1982 paper by Nakabayashi and
colleagues,10 that is called the hybrid layer (Figure 4). Although micromechanical resin infiltration and entanglement with the tooth tissues appears to be the primary attachment mechanism to both enamel and dentin, strong evidence suggests that certain monomers (such as 10-MDP) chemically interact, via ionic bond-ing, to calcium in hydroxyapatite as well.11,12 The hybrid layer and associated resin tags form a thin polymerized micromechanically, and in some cases chemically, attached resinous surface layer that acts as the foundation for subsequently placed chemically compat-ible restorative materials and resin-based cements.
While an in-depth discussion of the imperfect, and sometimes confusing, classification categories typically used to describe adhe-sive systems (etch-and-rinse, etch-and-no rinse, three-bottle, two-bottle, one-bottle, all-in-one, various generations, etc.) is beyond the scope of this article, it is reasonably safe to say that all adhesive systems, regardless of classification category, contain some type of acidic conditioner, dentin primer, and bonding resin. For example, the basic protocol when using a three-step total-etch system (4th generation) is the sequential placement of the three primary com-ponents (acidic conditioner, hydrophilic primer typically consisting of HEMA and adhesive functional monomer(s), and hydrophobic resin). In the case of 4th generation systems the components are packaged in separate containers and applied sequentially. Typically, phosphoric acid is first placed on enamel and dentin for a period of time, rinsed off with water, then a hydrophilic primer is placed and
tAble 1
Universal Adhesives and Their Basic Chemistries
ADhese UniversAl (ivoclAr vivADent)
All-bonD UniversAl (bisco, inc.)
cleArfil UniversAl bonD (KUrArAy)
fUtUrAbonD U (voco)
optibonD Xtr (Kerr corp.)
relUDe one (DAnville
MAteriAls)
priMe&bonD elect (Dentsply cAUlK)
scotchbonD UniversAl (3M espe)
Primer Adhesive
phosphate ester 10-MDP 10-MDP 10-MDP “Modified” 10-MDP GPDM GPDM 10-MDP PENTA-P 10-MDP
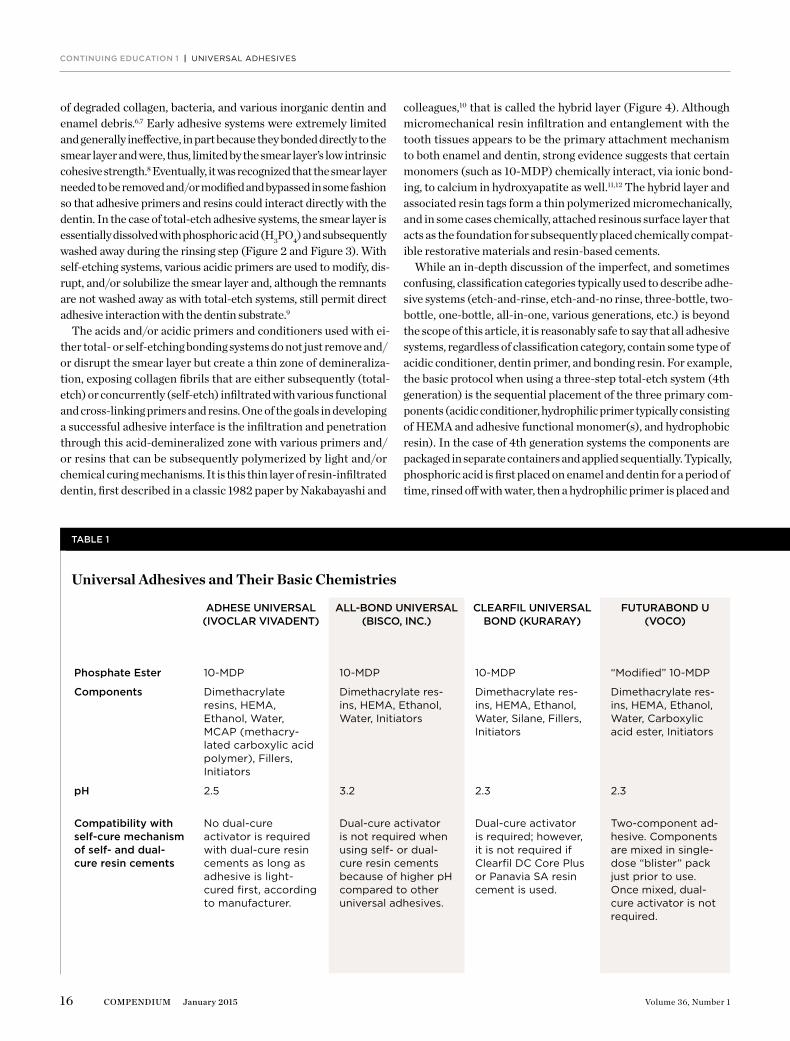
components Dimethacrylate resins, HEMA, Ethanol, Water, MCAP (methacry-lated carboxylic acid polymer), Fillers, Initiators
Dimethacrylate res-ins, HEMA, Ethanol, Water, Initiators
Dimethacrylate res-ins, HEMA, Ethanol, Water, Silane, Fillers, Initiators
Dimethacrylate res-ins, HEMA, Ethanol, Water, Carboxylic acid ester, Initiators
Various methacrylate monomers, HEMA, Acetone, Ethanol, Water, CQ Initiator
Tri-functional monomer, HEMA, Ethanol, Disodium hexafluorosilicate, Methoxyphenol (MEHQ)
Dimethacrylate res-ins, HEMA, Ethanol, Water, Initiators
Dimethacrylate res-ins, HEMA, Acetone, Water, Initiators
Dimethacrylate resins, HEMA, Ethanol, Water, Polyacrylic acid copolymer, Silane, Fillers, Initiators
ph 2.5 3.2 2.3 2.3 2.4 (drops to 1.6 when applied)*
3.4 2.8 2.5 2.7
compatibility with self-cure mechanism of self- and dual-cure resin cements
No dual-cure activator is required with dual-cure resin cements as long as adhesive is light-cured first, according to manufacturer.
Dual-cure activator is not required when using self- or dual-cure resin cements because of higher pH compared to other universal adhesives.
Dual-cure activator is required; however, it is not required if Clearfil DC Core Plus or Panavia SA resin cement is used.
Two-component ad-hesive. Components are mixed in single-dose “blister” pack just prior to use. Once mixed, dual-cure activator is not required.
Two-bottle system, marketed as self-etching system. No DC activator is required for self- and dual-cure resin cements if primer, followed by adhesive, is used on tooth. Only the adhe-sive is used as primer for porcelain and zirconia.
* information provided by Eugene Qiane (Kerr)
No dual-cure activa-tor is required with dual-cure resin cements if adhesive is light-cured first, according to manu-facturer. Product is marketed as self-etch only, but can be used as total-etch, accord-ing to manufacturer.
Dual-cure activator is required whenever self- or dual-cure resin cements are used.
Dual-cure activator is required; however, it is not required if RelyX Ultimate resin cement is used.

17www.compendiumlive.com January 2015 compendium
tAble 1
Universal Adhesives and Their Basic Chemistries
ADhese UniversAl (ivoclAr vivADent)
All-bonD UniversAl (bisco, inc.)
cleArfil UniversAl bonD (KUrArAy)
fUtUrAbonD U (voco)
optibonD Xtr (Kerr corp.)
relUDe one (DAnville
MAteriAls)
priMe&bonD elect (Dentsply cAUlK)
scotchbonD UniversAl (3M espe)
Primer Adhesive
phosphate ester 10-MDP 10-MDP 10-MDP “Modified” 10-MDP GPDM GPDM 10-MDP PENTA-P 10-MDP
components Dimethacrylate resins, HEMA, Ethanol, Water, MCAP (methacry-lated carboxylic acid polymer), Fillers, Initiators
Dimethacrylate res-ins, HEMA, Ethanol, Water, Initiators
Dimethacrylate res-ins, HEMA, Ethanol, Water, Silane, Fillers, Initiators
Dimethacrylate res-ins, HEMA, Ethanol, Water, Carboxylic acid ester, Initiators
Various methacrylate monomers, HEMA, Acetone, Ethanol, Water, CQ Initiator
Tri-functional monomer, HEMA, Ethanol, Disodium hexafluorosilicate, Methoxyphenol (MEHQ)
Dimethacrylate res-ins, HEMA, Ethanol, Water, Initiators
Dimethacrylate res-ins, HEMA, Acetone, Water, Initiators
Dimethacrylate resins, HEMA, Ethanol, Water, Polyacrylic acid copolymer, Silane, Fillers, Initiators
ph 2.5 3.2 2.3 2.3 2.4 (drops to 1.6 when applied)*
3.4 2.8 2.5 2.7
compatibility with self-cure mechanism of self- and dual-cure resin cements
No dual-cure activator is required with dual-cure resin cements as long as adhesive is light-cured first, according to manufacturer.
Dual-cure activator is not required when using self- or dual-cure resin cements because of higher pH compared to other universal adhesives.
Dual-cure activator is required; however, it is not required if Clearfil DC Core Plus or Panavia SA resin cement is used.
Two-component ad-hesive. Components are mixed in single-dose “blister” pack just prior to use. Once mixed, dual-cure activator is not required.
Two-bottle system, marketed as self-etching system. No DC activator is required for self- and dual-cure resin cements if primer, followed by adhesive, is used on tooth. Only the adhe-sive is used as primer for porcelain and zirconia.
* information provided by Eugene Qiane (Kerr)
No dual-cure activa-tor is required with dual-cure resin cements if adhesive is light-cured first, according to manu-facturer. Product is marketed as self-etch only, but can be used as total-etch, accord-ing to manufacturer.
Dual-cure activator is required whenever self- or dual-cure resin cements are used.
Dual-cure activator is required; however, it is not required if RelyX Ultimate resin cement is used.
air-dried, followed by the placement of a separate, relatively hydro-phobic bonding resin. The simplified two- and one-bottle systems still contain the aforementioned three primary components, but the components are consolidated and combined in various configura-tions depending on the specific system. In any case, as most dentists know, the trend in recent years has been toward not just the sim-plification of adhesive systems, but making them universal as well.
Table 1 lists eight products that are marketed as universal adhe-sives, along with their basic chemistries.
What is a “Universal” Adhesive?There does not appear to be any “official” definition as to what quali-fies as a universal adhesive. In any case, universal adhesives should not be confused with 7th generation self-etching single-bottle or
“all-in-one” systems such as iBond® (Heraeus Kulzer), Xeno® IV (DENTSPLY Caulk), Clearfil™ S3 Bond (Kuraray), and OptiBond® All-In-One (Kerr Corporation). For one thing, universal adhesives are said to have much broader applications than 7th generation sys-tems. Universal adhesives have been described by some manufactur-ers and opinion leaders as: ideally a single-bottle, no-mix, adhesive system that can be used in total-etch, self-etch, or selective-etch mode depending on the specific clinical situation and personal pref-erences of the operator.13,14 Additionally, manufacturers typically state that universal adhesives can be used for the placement of both direct and indirect restorations and are compatible with self-cure,
light-cure, and dual-cure resin-based cements. It is further stated that universal adhesives can be used not only to bond to dentin and enamel, but as adhesive primers on substrates such as zirconia, noble and non-precious metals, composites, and various silica-based ce-ramics. In principle, this would enable bonding to these surfaces without the need for dedicated and separately placed primers such as silane and various products marketed as metal and zirconia primers.
If this unofficial definition as to what constitutes a universal ad-hesive is accepted, it becomes apparent that a degree of ambiguity exists as to where certain products that are sometimes marketed as universal adhesives actually fit in. For example, OptiBond™ XTR (Kerr Corp.) is a two-bottle system that the manufacturer describes on its website as a “self-etch, light-cure, universal dental adhesive” that can be used for direct and indirect restorations, is compatible with light-, self-, and dual-cure resin cements, and bonds to metals, zirconia, porcelain, and composite. While this may all be true, as a two-bottle self-etching system with individual components that are applied separately and in a sequential fashion when bonding to tooth tissues, would OptiBond XTR be better described as a 6th generation self-etching system with expanded functions? Some products marketed as universal adhesives, such as Futurabond Universal Bond (VOCO), require the mixing of two separate com-ponents prior to use. This product comes in individual disposable blister packs that are easily activated just prior to use. There may be very sound reasons for keeping the chemistry of an adhesive

18 Volume 36, Number 1compendium January 2015
continuing education 1 | Universal adhesives
separate until just prior to use in terms of stability and product performance, but where does this mixing requirement fit into the definition of a universal adhesive? Prelude One™ (Danville Materials) is marketed on the company’s website as a “self-etch bonding system” yet the manufacturer claims it’s not contradictory to also use it in total-etch capacity (S. Chen, Danville Materials, per-sonal conversation/e-mail). Scotchbond™ Universal (3M ESPE) and Clearfil™ Universal (Kuraray) require a separate “activator” be added to the adhesive if another manufacturer’s self- or dual-cure resin cement is used during placement of indirect restorations, while Prime&Bond Elect® (DENTSPLY Caulk) requires the addi-tion of a separate activator for all self- and dual-cure resin cements. In addition, the manufacturers of some universal adhesives still recommend the use of separate and dedicated primers to optimize bond strength to substrates such as porcelain and zirconia.
Thus, it appears, at least in certain situations and with some products, that universal adhesives actually consist of two bottles, or require the use of an additional activator, or have chemistries that must be mixed prior to use, or bond most optimally to porcelain and zirconia with separately applied and dedicated primers, or are not compatible with a total-etch protocol. Suddenly, the definition of what qualifies as a universal adhesive becomes a bit muddled. Does this mean some products should not be classified as universal adhesives, or does the definition of exactly what a universal adhe-sive is need to be broadened? In any case, can universal adhesives, however they are defined, really do all of the things they are said to be able to do? Clearly, there must be significant practical and chemical challenges in developing such a versatile product, plac-ing all the chemistry required into one or even two bottles, have it perform as claimed, and have it remain stable for a reasonable period of time. So, how is it done?
It’s All About the ChemistryIn order to develop a truly universal adhesive, very specific and synergistic functional and cross-linking monomers that are multi-functional in nature are required. They must be capable of reacting
with a number of different substrates, be able to copolymerize with chemically compatible resin-based restoratives and cements, and have some hydrophilic character in order to properly “wet” dentin that has a significant water content, yet at the same time be as hy-drophobic as possible once polymerized to discourage hydrolysis and water sorption over time. Film thickness of the polymerized adhesive must also be thin enough as to not interfere with the seat-ing of indirect restorations. In addition, universal adhesives ideally should be acidic enough to be effective in a self-etching mode but not so acidic that they breakdown initiators needed for the polym-erization of self- and dual-cure resin cements.15
Universal adhesives must also contain water, as it is required for dissociation of the acidic functional monomers, inherent in all these systems, that makes self-etching possible. One of many dilemmas faced by chemists developing universal adhesives is that while some water is needed, too much can degrade the chemistry of these systems, contribute to phase separation of monomers, de-crease shelf-life, and be difficult to completely evaporate during the air-drying step.16,17 Residual water after air-drying could result in incomplete adhesive polymerization, increased hydrolysis after polymerization, and a generally compromised adhesive interface. Adding ethanol or acetone into universal adhesive formulations enhances resin wetting and infiltration of tooth tissues and also aids in water removal and evaporation during the air-drying step. There are many other important subtle factors and nuances that vary from manufacturer to manufacturer, such as pH, initiator and solvent chemistry, and specific monomer types and ratios, that also play a vital role in the viability of these systems and, in some situations, give certain products advantages over others. An examination of the chemistry of the systems listed in Table 1 shows some remark-able similarities, as well as some subtle and important differences.
The 10-MDP Adhesive Functional MonomerAll of the universal adhesives listed in Table 1 use phosphate esters (R-O-PO3H2) as their primary adhesive functional monomer. In fact, phosphate esters form the backbone of virtually all current
fig 3. fig 2. fig 1.
fig 1. Typical “peanut butter spread on toast” appearance of the dentin smear layer. (SEM courtesy of Jenny Wang.) fig 2. Dentin treated with 37% phosphoric acid for 15 seconds, rinsed, and blot dried. The smear layer has been removed and a thin zone of demineralization created. Collagen fibrils, which are inherent in dentin, are now exposed as they are no longer supported and surrounded by their inorganic hydroxyapatite scaffolding, which has essentially been “dissolved” away by the acid. It is important to penetrate this “collagen network” as completely as pos-sible with subsequently placed primers and adhesives in order to achieve good bonding. (See Fig 3.) fig 3. This SEM is basically the same as Fig 2 except the collagen seen in Fig 2 has been removed with collagenase enzymes exposing the dentin underneath that has not been, or has been minimally, demineralized by acidic pretreatment. It is this interface that is important to engage, via hybrid layer formation, to achieve good bond-ing and a well-sealed interface. (SEM courtesy of the late Dr. John Gwinnett.)

19www.compendiumlive.com January 2015 compendium
bonding between the 10-MDP in Z-Prime and zirconia19 and the product received very favorable reviews for use as a dedicated zir-conia primer25 (Figure 6 through Figure 11). Two years after the introduction of Z-Prime, 3M ESPE introduced the first “universal” adhesive (Scotchbond Universal), which also utilized 10-MDP in its formulation (J. Fundingsland, 3M ESPE, personal communi-cation). This product was followed shortly thereafter by Bisco’s
fig 5.
fig 4. The hybrid layer and associated resin tags form the foundation of the adhesive interface and represents the first in a series of links that to-gether form a bonded assembly between the tooth tissues and resin-based restoratives and cements. fig 5. The 10-MDP monomer used in many universal adhesive systems consists of a versatile phosphate group (red) on one end capable of bonding to tooth tissues and a variety of restorative substrates, and a methacrylate group (gold) on the other end capable of bonding to methacrylate-based restorative materials and cements.
universal adhesive systems and enable them to do much of what they do. These monomers have many positive attributes, including the potential to bond chemically to metals,18 zirconia,19 and to tooth tissues through the formation of non-soluble Ca++ salts.11,12 In addi-tion, their acidic nature (they are esters of phosphoric acid) gives them the potential to etch and demineralize tooth tissues, which makes them good candidates for use in adhesives that require self-, selective-, and total-etching options.
A very practical and proven phosphate ester, which also happens to be the one used in the formulations of many current universal adhesives, was actually synthesized more than 30 years ago. In the early 1980s chemists at Kuraray (Osaka, Japan) synthesized the adhesive functional monomer 10-MDP (methacryloyloxy-decyl-dihydrogen-phosphate) (Figure 5). One of the first practi-cal applications of this new monomer was its use in the company’s Panavia™ adhesive resin cement. Panavia proved to be especially adept at bonding to metals, and its success led to the use of the MDP monomer in virtually all subsequent Kuraray adhesives. The 10-MDP monomer has many positive attributes that make it prac-tical for use in a universal adhesive. It is a versatile amphiphilic functional monomer with a hydrophobic methacrylate group on one end (capable of chemical bonding to methacrylate-based re-storatives and cements) and a hydrophilic polar phosphate group on the other (capable of chemical bonding to tooth tissues, metals, and zirconia). This attribute alone makes it desirable for use in a
“universal” adhesive. Moreover, the long carbon chain backbone of the monomer renders it fairly hydrophobic. In fact, with a partition coefficient of 4.1 (partition coefficient is essentially a measure of how hydrophilic or hydrophobic a chemical substance is) 10-MDP is the most hydrophobic of all the functional monomers typically used in dental adhesives.20 This may be important in terms of du-rability, as water sorption and hydrolytic breakdown of the adhe-sive interface over time has been implicated as one of the primary causes of bond failure.21,22 It makes sense that, once they are placed and polymerized, adhesive monomers that discourage water sorp-tion are desirable. The hydrophobic nature of 10-MDP also makes it relatively stable in solution, which is important in terms of shelf-life. Additionally, 10-MDP is one of the few monomers used in adhesive dentistry that has been shown to actually bond chemically to the tooth tissues via ionic bonding to calcium found in hydroxyapatite (Ca10[PO4]6[OH]2).11,12 Stable MDP-calcium salts are formed during this reaction and deposited in self-assembled nano-layers of vary-ing degrees and quality depending on the adhesive system.23,24 This type of molecular interaction and self-organization, coupled with the relatively hydrophobic nature of polymerized 10-MDP, helps explain why this monomer appears to be so effective in creating adhesive interfaces that are resistant to biodegradation23 (J. Oxman, chemist, 3M ESPE, personal communication).
When Kuraray’s patent on 10-MDP expired (around 2003) other manufacturers began to explore its potential. In October 2009, Bisco, Inc. introduced a dedicated zirconia primer, Z-Prime™, that utilized a combination of 10-MDP and biphenyl dimethacrylate (BPDM) in its formulation (C. Suh, Bisco, Inc., personal commu-nication). The use of secondary ion mass spectrometry (SIMS) at Northwestern University showed evidence of actual chemical
resin-based restorative or cement
Adhesive Agent
hybrid layer
resin tags
fig 4.

20 Volume 36, Number 1compendium January 2015
continuing education 1 | Universal adhesives
which is then overlaid by a relatively hydrophobic bonding resin. Chemists developing single-bottle universal adhesives had to for-
mulate an optimized blend of chemically compatible hydrophobic, adhesive functional, and hydrophilic monomers that would work in a synergistic fashion and when polymerized form a durable, and hopefully hydrophobic, bonded interface. In this regard, the different monomers employed in universal adhesives each have their own spe-cific functions. Generally, the hydrophilic ends of monomers interact with the tooth tissues, while the hydrophobic ends interact with methacrylate-based restorative materials or cross-link with other functional and structural monomers. The terminal ends of some adhesive functional monomers are hydrophilic initially (such as the ionic phosphate group in 10-MDP) but become more hydrophobic once they chemically react with tooth tissues and are polymerized.
There are significant challenges in striking just the right balance between hydrophilic and hydrophobic character when developing a universal adhesive, as the monomers need to initially be hydrophilic enough to wet, infiltrate, and interact with the dentin substrate, but once they are polymerized, not so hydrophilic that they encourage water sorption that could lead to hydrolysis and breakdown of the adhesive interface over time. Manufacturers of universal adhesives address these issues by blending some well known and widely used monomers such as bis-GMA (hydrophobic) and hydroxyethyl meth-acrylate (HEMA) (hydrophilic) along with proprietary and various adhesive functional monomers that vary from manufacturer to manu-facturer. One of the goals after placing, drying, and curing a universal adhesive should be the creation of a highly cross-linked hydrophobic polymer matrix29 that is well bonded to the tooth tissues on one end and to restorative materials, such as composites, on the other. Some manufacturers may have advantages over others in this regard.
Almost all adhesive systems, including universal systems, utilize HEMA in their formulations (Figure 12). HEMA is a versatile low molecular weight hydrophilic monomer that is particularly adept at infiltrating and “wetting” dentin substrates. It is extremely soluble in water, ethanol, and acetone, and thus easy to incorporate into adhesive formulations. The hydrophilicity of HEMA makes it an excellent adhesion-promoting monomer that has been shown to
fig 6. fig 7.
fig 6. Two zirconia winged resin bonded bridges replacing Nos. 7 and 10. The wings and frame are 100% zirconia. Porcelain has been pressed over the frame, creating the veneers Nos. 7 and 10. fig 7. After the bridges were tried in and the intaglio surface of the zirconia wings were sandblasted with 50-µm aluminum oxide at 30 PSI to 40 PSI of air pressure, a 10-MDP dedicated primer was placed and warm-air–dried for 30 seconds.
All-Bond Universal®, also featuring the 10-MDP monomer. In fact, six of the eight universal adhesives listed in Table 1 use 10-MDP in their formulations (including one that uses a modified 10-MDP [in-formation provided by G. Connell, Director of Clinical Education & North American Training, VOCO Canada]). In addition to 10-MDP, other phosphate esters such as PENTA-P (dipentaerythritol penta acrylate monophosphate) and GPDM (glycero-phosphate dimethacrylate) also appear to be viable alternatives. In any case, it is apparent that the use of phosphate esters is an important part of the universal adhesive story, but it’s only part of the story.
The Delicate Balance Between Hydrophilic, Hydrophobic, And Adhesive Functional MonomersA great paradox of adhesive dentistry is that the chemistry that helps make adhesive systems so effective initially can also con-tribute to their eventual breakdown. One reason for the success of current adhesive systems is the use of hydrophilic monomers that are able to interact with and “wet” tooth tissues that are, to some degree, inherently moist. The problem is that the same hydrophilic groups that initially facilitate primer/resin interac-tion with the tooth tissues can become a liability in the long term by encouraging water sorption and hydrolysis of the adhesive interface.26 Indeed, one of the major problems with 7th generation single-bottle self-etching systems is that the inherently hydro-philic nature of the polymerized adhesive, coupled with residual water that may remain, has been shown to act as a semi-permeable membrane permitting water diffusion that, over time, could lead to hydrolysis and breakdown of the adhesive interface.27 One could argue that an “ideal” dentin bonding agent would be one that is hydrophilic when first placed (to facilitate interaction with the tooth tissues) but then becomes hydrophobic once polymer-ized (to discourage water sorption). The next best thing would be gradation from hydrophilic to hydrophobic as one moves from the tooth surface to the restorative interface.28 Indeed, this is the strategy employed by the original three-step total-etch (4th generation) and two-step self-etch (6th generation) adhesive systems—that is, the initial placement of a hydrophilic primer,

21www.compendiumlive.com January 2015 compendium
improve immediate bond strengths of adhesive systems by enhanc-ing monomer diffusion into dentin and facilitating the formation of the “hybrid” layer.30-32 HEMA is frequently added to adhesives, not only to ensure good wetting, but also because of its solvent-like nature. This improves stability and helps keep hydrophobic and hydrophilic monomers in solution by minimizing phase separation in the presence of water (HEMA-free adhesives can have issues with phase separation).30,33,34
While HEMA has many positive attributes there is also a down-side. HEMA in both the uncured and polymerized state readily absorbs water. Once polymerized it can swell, discolor, and con-tribute to hydrolysis of the adhesive interface.29,32,35 High amounts of HEMA can also decrease mechanical properties of the resulting polymer. Uncured HEMA also has the potential to lower the vapor pressure of water and may make it more difficult to evaporate dur-ing the air-drying step.36 While the concentration of HEMA used in universal adhesives varies from manufacturer to manufacturer, the goal should be to optimize the HEMA concentration (use least amount possible) to take advantage of the benefits of this monomer while concurrently minimizing its undesirable properties.
The pH PuzzleThe pH of current universal adhesives varies from about 2.2 to 3.2 depending on the product. Universal adhesives are generally con-sidered to have “mild” (pH > 2) or “extra-mild” (pH > 2.5) etching capabilities.37,38 Adhesives in this pH range can be very effective in terms of bonding to dentin. The concern is that they may not be as effective when it comes to bonding to enamel (especially to uncut enamel).39-41 As an example, a popular two-bottle 6th generation self-etching system (Clearfil™ SE Bond, Kuraray) with a pH in the range of current universal adhesives and which also contains the 10-MDP monomer has been shown to bond more predictably to enamel in some clinical studies when the enamel is first etched with phosphoric acid.42-44 In fact, a common clinical technique when using this product is to first etch the enamel with traditional phos-phoric acid gel (selective-etch technique). While there are in-vitro studies that do demonstrate acceptable bond strength values to enamel using the self-etching mode of some universal adhesives,45,46 caution is urged as there is equivocation in the literature47-50 and some systems may perform significantly better (or worse) than others when it comes to enamel bonding.51 The author’s personal preference, and recommendation, is to use universal adhesives only in the selective- or total-etching modes when enamel is present to ensure predictable long-term bonding to this substrate. In the case of bonding in full-coverage restorations, where there is little or no enamel remaining, then universal adhesives used in the self-etching mode is a viable, and perhaps even preferred, option.
There is also a direct correlation between pH and the compat-ibility of universal adhesives with self- and dual-cure resin cements and composites. As a generalization, the more acidic the adhesive the less compatible it is with the self-cure mode of dual-cure resin-based materials.52,53 This is primarily due to acid deactivation of the aromatic tertiary amines that play a crucial role in chemical curing mechanisms of most of these materials.20 To overcome this issue, several universal adhesives, when used in conjunction with self- and
fig 10.
fig 11.
fig 8. fig 9.
dual-cure resin cements, require the addition of a separate “activa-tor” (typically arylsulfinate salts) either all of the time (Prime&Bond Elect) or unless specific dedicated amine-free resin cements are used (Scotchbond Universal, Clearfil Universal). At least one universal adhesive (All-Bond Universal) is compatible with most common self- and dual-cure resin cements without the use of a separately applied activator. This is because this adhesive is less acidic, with a pH of 3.2, than other universal adhesives that have pHs ranging be-tween 2.0 and 3.0. This is enough of a difference to allow the reactions necessary for chemical curing of self- and dual-cure resin cements
fig 8 through fig 11. Preoperative and postoperative views. At the time of this writing, the case has been in place 4 years and 10 months. fig 12. HEMA monomer consisting of a methacrylate group on one end (gold) and a hydroxyl (-OH) group capable of hydrogen bonding on the other.
fig 12.

22 Volume 36, Number 1compendium January 2015
continuing education 1 | Universal adhesives
and composites when using All-Bond Universal.54 Likewise, the two-component systems that are also marketed as universal adhesives (OptiBond XTR, Futurabond Universal) do not require the use of a separate activator, because the activator is already incorporated into one of the components of these systems. The manufacturers of some universal adhesives with pH less than 3.0 (Adhese® Universal, Ivoclar Vivadent; Prelude One) suggest that bonding to dual-cure resin cements is acceptable as long as the adhesive is light-cured first. In the author’s opinion the use of a universal adhesive with a pH less than 3.0 is risky if the dentist is relying on the self-cure mechanism of a dual-cure resin cement (which may be the case when light penetra-tion is an issue) unless an additional activator is used.
Will Universal Adhesives Replace Dedicated Primers?The manufacturers of most universal adhesives state they can be used not only for bonding to dentin and enamel, but as adhesive primers on substrates such as zirconia, noble and non-precious metals, composites, and silica-based ceramics. The question isn’t
fig 13.
fig 14.
whether universal adhesives are capable of bonding to these sub-strates (they are), but are they as effective, both initially and, more importantly, over time, as separately placed dedicated primers? There is some controversy surrounding this question. Opinions differ from manufacturer to manufacturer, and, in the author’s view, additional objective independent research is needed before making definitive recommendations.
In terms of bonding to zirconia, there are studies that demon-strate some universal adhesives are very effective as zirconia prim-ers.51,55-57 However, at least two studies also found that the bond strength values of some universal adhesives to zirconia decreased significantly after thermocycling or 6 months of water storage.57,58 There are also respected chemists and researchers who feel that the most durable bond to zirconia is attained when separate and dedi-cated primers are employed.19 One such primer (Z-Prime), consist-ing of a phosphate ester (10-MDP) and carboxylic acid monomer (BPDM), has proven to be especially effective in this regard59-63 and does not require light-curing, which alleviates concerns some may have regarding film thickness (universal adhesives used as zirconia primers should be air-thinned and light-cured). Some self-etching 10-MDP-containing resin cements, such as Panavia SA Cement (Kuraray), have also shown promise bonding to both tooth tissues and substrates such as zirconia without the use of separately placed adhesives or primers.64 It is possible that products of this nature would perform even better if the zirconia surface were first treated with a universal adhesive or dedicated zirconia primer (the author is unaware of any research that has specifically examined this).
Another issue is how the dentist should treat the zirconia surface prior to placing a universal adhesive or dedicated zirconia primer. It is the author’s strong opinion that the zirconia surface should be sandblasted prior to utilizing any adhesive, primer, or resin-based cement. There is significant support in the literature for this recom-mendation.55,61-63,65-67 While there is some concern that sandblasting has the potential to induce surface and subsurface cracks and/or de-fects that could reduce physical properties,68,69 the author is unaware of any studies or anecdotal evidence that demonstrates this to be a clinical problem. Sandblasting zirconia is useful in terms of cleaning the target surface of impurities, increasing surface roughness, raising surface energy, improving the bond to primers and adhesives, and generally optimizing the surface prior to bonding or cementation. The author recommends using a sandblaster (eg, Microetcher™ II, Danville Materials) with 30-µm to 50-µm aluminum oxide (Al2O3) at 30 PSI to 40 PSI of air pressure (2.0 to 2.8 bar). The intaglio surface of the restoration is sandblasted after it has been tried in and just prior to dedicated primer or universal adhesive application. If the dentist does not have a sandblaster then the author recommends the dentist have the laboratory sandblast the restoration and then use a product such as Ivoclean (Ivoclar Vivadent), which is a solution of sodium hydroxide, polyethylene glycol, water, and zirconia oxide, after the restoration has been tried in and prior to primer application. While the use of phosphoric acid (H3PO4) can be an effective cleaning agent for saliva-contaminated silica-based ceramics (such as lithium disilicate)70 it is contraindicated for cleaning zirconia surfaces. This is because phosphate ions from the phosphoric acid remain bound to the zirconia surface (even after rinsing) and compete with phosphate
fig 13. The silane most often used in dentistry is 3-methacryloxyprop-yltrimethoxysilane. The left side of this molecule is nothing more than a methacrylate group capable of copolymerization with methacrylate-based resin cements and adhesives. The right side, after hydrolysis, has the potential to form chemical bonds to the porcelain surface. fig 14. This diagram shows unhydrolyzed silane on the left. To be able to function as a coupling agent and interact chemically with porcelain surfaces, silane must first be hydrolyzed. Acetic acid is commonly used to “activate” or hydrolyze silane by reacting with the three methoxy (-OCH3) groups located at one end of the silane molecule and replac-ing them with hydroxyl (-OH) groups. Silane in the active hydrolyzed form is shown on the right.

23www.compendiumlive.com January 2015 compendium
dedicated silane solution. This makes sense as long as all the other chemistry found in universal adhesives does not interfere with silane stability and performance. The manufacturers of other universal ad-hesives have chosen not to add silane into their formulations because they question the stability of silane in the acidic environment of a universal adhesive and/or believe the chemical interaction of silane with silica-based ceramics is significantly inhibited when combined with all the other monomers found in universal adhesives. Indeed, contact angle studies have found that the incorporation of bis-GMA resin or MDP (both of which are used in universal adhesives) into silane solutions substantially reduced the priming efficiency and chemical interaction of the silane with silica-based lithium disilicate compared to pure silane controls.75,76 Once again, in the author’s opin-ion, the efficacy and wisdom of incorporating silane into universal adhesives is an area that requires further study and clarification. When bonding to silicate-based ceramics, the author’s personal pref-erence, at least at this time, is to etch the porcelain with HF followed by the use of a dedicated pre-hydrolyzed silane primer (eg, RelyX™ Ceramic Primer, 3M ESPE; Porcelain Primer, Bisco, Inc.; Ultradent® Silane, Ultradent Products, Inc.) that is free of any added monomers or resins (pure silane).
ions from zirconia primers for reaction sites on the surface (zirconia has a strong affinity for phosphate ions). Likewise, the phosphate ions in saliva can tie-up reactive sites on the zirconia surface. Studies show that the best way to treat saliva-contaminated sandblasted zirconia surfaces is by re-sandblasting or using a strongly alkaline cleaning solution such as Ivoclean.71-73
Some universal adhesives also claim they can be used in lieu of dedicated silane coupling agents when bonding to silica-based ce-ramics (feldspathic, lithium disilicate, etc.). Historically, the use of hydrofluoric acid (HF) followed by the application of a dedicated silane coupling agent has been the treatment of choice in this regard, and the author has previously discussed this topic in great detail.74 Silanes are a class of organic molecules that contain one or more sili-con atoms. Dozens of different silane compounds exist and are used extensively in industry and manufacturing. The silane typically used in dentistry, for both intraoral repair and the priming of silica-based ceramic restorations prior to placement, is 3-methacryloxypropyl-trimethoxysilane (Figure 13 through Figure 16). The manufacturers of some universal adhesives have incorporated silane directly into their adhesive formulations, as noted in Table 1, with the idea that the universal adhesive can now be used instead of a separately applied
fig 15. The hydroxyl groups on the activated silane molecule are now capable of reacting directly with corresponding hydroxyl groups present on the surface of silica-based ceramics. The opposing hydroxyl groups first interact with one another via hydrogen bonding. As water is lost, a condensation polymerization reaction occurs and covalent bonds are formed. Warm, dry air encourages this reaction. fig 16. In this illustration, the individual silane molecules have covalently bonded not just to the porcelain surface, but to adjacent silane molecules, essentially forming a polymer “network” on the surface. The methacrylate group on the other end of the silane molecule can now react—via free radical addition polymerization—with methacrylate groups in subsequently placed adhesives and methacrylate-based resin cements.
fig 15. fig 16.

24 Volume 36, Number 1compendium January 2015
continuing education 1 | Universal adhesives
Is It Time to Switch to a Universal Adhesive?In August 2014, at a “key opinion leader” meeting comprised of 32 dentists, academicians, researchers, and chemists, the author con-ducted a written survey that included several questions,14 some of which, along with responses and attendee comments, are listed below:• Question: “Do you, or have you, used any of the new universal
adhesive systems?” Of the 32 responses, 30 answered “yes.” • Question: “At this time what is your ‘go-to’ adhesive, ie, the one you
use, or would recommend, most often?” There were 19 responses answering universal adhesives (two such products in particular were mentioned). Nine respondents answered either 4th or 5th generation total-etch systems, and four answered 6th generation self-etching systems.
• Question: “Even though universal adhesives are supposed to bond to a variety of substrates, do you still feel separate dedicated metal, zirconia, and porcelain primers should be used? If yes, why do you feel that way?”
Most interestingly, 29 of the 32 respondents to the last question said they would still use a dedicated primer. Comments included: not trusting that universal adhesives would work as well as a separate primer; stability being an issue; Z-Prime Plus giving the best bond strength to zirconia; longer-range research data existed for dedicated primers; more steps still proves to be more durable, reliable, and lon-ger lasting. Another concern was “never felt comfortable with silane being contaminated.” It should be pointed out that comments such as these are sometimes visceral in nature and not necessarily based on science. In any case, it is clear that there are some concerns about the ability of universal adhesives to perform as predictably as dedicated primers (especially when stressed by aging or thermocycling), and more research is needed that directly compares the two.
So, is it time to make the switch to a universal adhesive? Certainly, the versatility, simplicity, potential to reduce product inventory, chemistry, and relatively hydrophobic nature of polymerized uni-versal adhesives do make them an attractive option. The author has been using a 10-MDP-containing universal adhesive system, most often in total- or selective-etching mode, almost exclusively now for just over 2 years with excellent clinical success. There are certain points to keep in mind that will optimize the performance of universal adhesive systems (as well as all adhesive systems):
1) Make sure to evaporate the solvents. All adhesive systems employ acetone, ethanol, water, or a combination of these as sol-vents for their particular monomers. It is extremely important to evaporate these solvents as completely as possible by air-drying for an adequate period of time prior to polymerization. Inadequate solvent evaporation has been associated with incomplete resin polymerization, nanoleakage, and decreased bond strength.77,78 Increasing the manufacturer’s recommended air-drying times and/or the use of warm air dryers may be prudent in this regard.
2) Even good chemistry will not overcome poor clinical technique. For example, all universal adhesives recommend “rubbing” or
“scrubbing” the tooth preparation with adhesive for at least 20 sec-onds, drying, and then light-curing for an adequate period of time with a quality bonding light. Dentists should critically examine their own technique to make sure these guidelines are being followed.
3) Check the expiration date. All bonding agents utilize chemistries that can deteriorate significantly over time. This is especially true when they are subjected to high temperatures. Refrigeration may be useful in this regard, but adhesives should be removed and allowed to warm up to room temperature at least 30 minutes prior to use.79
4) Be sure to read the directions. All adhesive systems tend to have their own specific placement and handling idiosyncrasies that must be followed precisely for optimal results. What works well for one system may not be applicable for another.
ConclusionProper management of the adhesive interface is crucial for the pre-dictable placement of many current dental restorations. This requires an understanding of the materials being utilized, the substrate being bonded to, and a correct and precise clinical protocol. It is incumbent on every dentist to learn about the specific adhesive system being used, its idiosyncrasies, strengths, and weaknesses, and how to maximize its performance. While clinical trials and clinical experience remains the ultimate test for all dental materials, universal adhesives represent an exciting and promising new class of dental adhesives that the author suspects will soon dominate the adhesive marketplace.
AcKnoWleDGMents
During the preparation of this article the author spoke or corre-sponded with dozens of individuals from many different dental companies. He would especially like to thank the following individu-als for their input, advice, and general support: Dr. Byoung Suh and Dr. Liang Chen (Bisco, Inc.); Dr. Joe Oxman and Jon Fundingsland (3M ESPE); Gregor Connell (VOCO Canada); Dr. Shashikant Singal (Ivoclar Vivadent); Dr. Xiangxu (Sean) Chen and Dr. Patrick Roetzer (Danville Materials); Dr. Xuejun (Eugene) Qiane (Kerr Corpora-tion); and Dr. John Burgess (University of Alabama Birmingham).
DisclosUre
The author has no affiliation with any of the companies mentioned in this article.
AboUt the AUthor
Gary Alex, DMDPrivate Practice, Huntington, New York
Queries to the author regarding this course may be submitted to [email protected].
references
1. Buonocore MG. A simple method of increasing the adhesion of acrylic filling to enamel surfaces. J Dent Res. 1955;34(6):849-853.2. Buonocore MG, Matsui A, Gwinnett AJ. Penetration of resin dental materials into enamel surfaces with reference to bonding. Arch Oral Biol. 1968;13(1):61-70.3. Alex G. Adhesive dentistry in the new millennium. Oral Health. 2000;59-64.4. Gwinnett AJ. Bonding basics: What every clinician should know.

25www.compendiumlive.com January 2015 compendium
Esthetic Dent Update. 1994;5:35-41.5. Van Meerbeek B, Lambrechts P, Inokoshi S, et al. Factors affecting adhesion to mineralized tissues. Oper Dent. 1992;(suppl 5):111-124.6. Gwinnett AJ. Smear layer: morphological considerations. Oper Dent Suppl. 1984;3:2-12.7. Brännström M. Smear layer: pathological and treatment considerations. Oper Dent Suppl. 1984;3:35-42.8. Pashley DH. Smear layer: overview of structure and function. Proc Finn Dent Soc. 1992;88(suppl 1):215-224.9. Alex G. Is total-etch dead? Evidence suggests otherwise. Compend Contin Educ Dent. 2012;33(1):12-26.10. Nakabayashi N, Kojima K, Masuhara E. The promotion of adhesion by the infiltration of monomers into tooth substrates. J Biomed Mater Res. 1982;16(3):265-273.11. Fukegawa D, Hayakawa S, Yoshida Y, et al. Chemical interaction of phos-phoric acid ester with hydroxyapatite. J Dent Res. 2006;85(10):941-944.12. Van Landuyt KL, Yoshida Y, Hirata I, et al. Influence of the chemical structure of functional monomers on their adhesive performance. J Dent Res. 2008;87(8):757-761.13. Key opinion leader symposium held at 3M ESPE; July 2014; Wonewok, MN. 14. Key opinion leader symposium held at Bisco, Inc.; August 2014; Chicago, IL. 15. Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the in-compatibility between simplified-step adhesives and chemically-cured or dual-cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent. 2003;5(4):267-282.16. Nishiyama N, Tay FR, Fujita K, et al. Hydrolysis of functional mono-mers in single-bottle self-etching primer-correlation of 13C NMR and TEM findings. J Dent Res. 2006;85(5):422-426.17. Moszner N, Salz U, Zimmermann J. Chemical aspects of self-etching enamel-dentin adhesives: a systematic review. Dent Mater. 2005;21(10):895-910.18. Kadoma Y. Surface treatment agent for dental metals using a thiirane monomer and a phosphoric acid monomer. Dent Mater J. 2002;21(2):156-159. 19. Chen L, Suh BI, Brown D, Chen X. Bonding of primed zirconia ceram-ics: evidence of chemical bonding and improved bond strengths. Am J Dent. 2012;25(2):103-108.20. Suh BI. Principles of Adhesive Dentistry: A Theoretical and Clinical Guide for Dentists. Newtown, PA: Aegis Publications LLC; 2013.21. De Munck J, Van Meerbeek B, Yoshida Y, et al. Four-year water degradation of total-etch adhesives bonded to dentin. J Dent Res. 2003;82(2):136-140.22. Hashimoto M, Ito S, Tay FR, et al. Fluid movement across the resin-den-tin interface during and after bonding. J Dent Res. 2004;83(11):843-848.23. Yoshida Y, Yoshihara K, Nagaoka N, et al. Self-assembled Nano-layer-ing at the Adhesive interface. J Dent Res. 2012;91(4):376-381. 24. Yoshihara K, Yoshida Y, Hayakawa S, et al. Novel fluoro-carbon func-tional monomer for dental bonding. J Dent Res. 2014;93(2):189-194.25. Z-PRIME Plus evaluation. The Dental Advisor. December 2010;27(10). 26. Tay FR, Pashley DH. Have dental resins become too hydrophilic? J Can Dent Assoc. 2003;69(11):726-731.27. Tay FR, Pashley DH, Suh BI, et al. Single-step adhesives are permeable membranes. J Dent. 2002;30(7-8):371-382.28. De Munck J, Van Landuyt K, Peumans M, et al. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res. 2005;84(2):118-132.29. Suh BI, Chen L, Brown DJ. A novel concept: the introduction of cross linking monomers into a self-etch adhesive to create a more hydrophobic and durable bond. Oral Health. 2011;March:62-66,94. 30. Van Landuyt KL, Snauwaert J, De Munck J, et al. Systematic review of the chemical composition of contemporary dental adhesives. Biomateri-als. 2007;28(26)3757-3785.31. Nakaoki Y, Nikaido T, Pereira PN, et al. Dimensional changes of deminer-alized dentin treated with HEMA primers. Dent Mater. 2000;16(6):441-446.32. Nakabayashi N, Takarada K. Effect of HEMA on bonding to dentin.
Dent Mater. 1992;8(2):125-130.33. Jacobsen T, Soderholm KJ. Some effects of water on dentin bonding. Dent Mater. 1995;11(2):132-136.34. Van Landuyt KL, De Munck J, Snauwaert J, et al. Monomer-solvent phase separation in one-step self-etch adhesives. J Dent Res. 2005;84(2):183-188.35. Burrow MF, Inokoshi S, Tagami J. Water sorption of several bonding resins. Am J Dent. 1999;12(6):295-298.36. Pashley EL, Zhang Y, Lockwood PE, et al. Effects of HEMA on water evaporation from water–HEMA mixtures. Dent Mater. 1998;14(1):6-10.37. Van Meerbeek B, De Munck J, Yoshida Y, et al. Buonocore memorial lecture. Adhesion to enamel and dentin: Current status and future chal-lenges. Oper Dent. 2003;28(3):215-235.38. Van Meerbeek B, Yoshihara K, Yoshida Y, et al. State of the art of self-etch adhesives. Dent Mater. 2011;27(1):17-28. 39. Perdigao J, Lopes L, Lambrechts P, et al. Effects of a self-etching primer on enamel shear bond strengths and SEM morphology. Am J Dent. 1997;10(3):141-146.40. Miyazaki M, Sato M, Onose H. Durability of enamel bond strength of simplified bonding systems. Oper Dent. 2000;25(2):75-80.41. El-Askary FS, Anwar MN, Munoz MA, et al. Micro-shear bond strength of universal adhesives to uncut enamel [abstract]. J Dent Res. 2014;93(spec iss B). Abstract 1139.42. Peumans M, De Munck J, Van Landuyt K, et al. Five-year clinical effec-tiveness of a two-step self-etching adhesive. J Adhes Dent. 2007;9(1):7-10.43. Abdalla AI, El Sayed HY. Clinical evaluation of a self-etch adhesive in non-carious cervical lesions. Am J Dent. 2008;21(5):327-330.44. Ermis RB, Temel UB, Cellik EU, Kam O. Clinical performance of a two-step self-etch adhesive with additional enamel etching in Class III cavities. Oper Dent. 2010;35(2):147-155.45. Understanding the newest generation of adhesives: universal bonding agents. The Dental Advisor. March 2013;30(2).46. Wagner A, Wendler M, Petschelt A, et al. Bonding performance of uni-versal adhesives in different etching modes. J Dent. 2014;42(7):800-807.47. Perdigao J, Sezinando A. Evaluation of a new universal adhesive using different bonding strategies [abstract]. J Dent Res. 2012;91(spec iss A). Abstract 18.48. de Goes MF, Shinohara MS, Freitas MS. Performance of a new one-step multi-mode adhesive on etched vs non-etched enamel on bond strength and interfacial morphology. J Adhes Dent. 2014;16(3):243-250.49. McLean D. Enamel Bond Strength of New Universal Adhesive Bonding Agents [master’s thesis]. Bethesda, MD: Uniformed Services University of the Health Sciences; 2013. 50. Perdigao J, Munoz MA, Luque-Martinez IV, et al. Enamel Etching Pat-terns of Universal Adhesives — FESEM Analyses [abstract]. J Dent Res. 2014;93(spec iss B). Abstract 474.51. New Universal Adhesives (Part II): Faster, Easier, Better? Clinicians Report. 2012;5(8):1-3. 52. Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and self-cured or dual-cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent. 2003;5(4):267-282.53. Schittly E, Bouter D, Le Goff S, et al. Compatibility of five self-etching adhesive systems with two resin luting cements. J Adhes Dent. 2010;12(2):137-142.54. Suh BI. Universal adhesives: The evolution of adhesive solutions con-tinues. Compend Contin Educ Dent. 2014;35(4):278.55. Amaral M, Belli R, Cesar PF, et al. The potential of novel primers and universal adhesives to bond to zirconia. J Dent. 2014;42(1):90-98.56. Seabra B, Arantes-Oliveira S, Portugal J. Influence of multimode uni-versal adhesives and zirconia primer application techniques on zirconia repair. J Prosthet Dent. 2014;112(2):182-187.57. Kim JH, Chae SY, Lee Y, et al. Effects of multipurpose, universal adhesives on resin bonding to zirconia ceramic. Oper Dent. 2014 Aug 1. [Epub ahead of print]58. de Souza G, Hennig D, Aggarwal A, Tam LE. The use of MDP-based

26 Volume 36, Number 1compendium January 2015
continuing education 1 | Universal adhesives
materials for bonding to zirconia. J Prosthet Dent. 2014;112(4):895-902.59. Kobes KG, Vandewalle KS. Bond strength of resin cements to zirconia conditioned with primers. Gen Dent. 2013;61(6):73-76. 60. Inokoshi M, Poitevin A, De Munck J, et al. Bonding effectiveness to different chemically pre-treated dental zirconia. Clin Oral Investig. 2014;18(7):1803-1812. 61. Yi YA, Ahn JS, Park YJ, et al. The effect of sandblasting and different primers on shear bond strength between yttria-tetragonal zirconia polycrystal ceramic and a self-adhesive resin cement. Oper Dent. 2014 Aug 1. [Epub ahead of print]62. Barragan G, Chasqueira F, Arantes-Oliveria S, Portugal J. Ceramic repair: influence of chemical and mechanical surface conditioning on adhesion to zirconia. Oral Health Dent Manag. 2014;13(2)155-158. 63. Zandparsa R, Talua NA, Finkelman MD, Schaus SE. An in-vitro comparison of shear bond strength of zirconia to enamel using different surface treatments. J Prosthodont. 2014;23(2):117-123. 64. Koizumi H, Nakayama D, Komine F, et al. Bonding of resin-based luting cements to zirconia with and without the use of ceramic priming agents. J Adhes Dent. 2012;14(4):385-392.65. Sahabi M, Yaghmaie K, Fayaz A. Effect of air-abrasion on microshear bond strength of two resin cements to Cercon porcelain. J Res Med Sci. 2010;4(3):142-145.66. Yun JY, Ha SR, Lee JB, Kim SH. Effect of sandblasting and various metal primers on the shear bond strength of resin cement to Y-TZP ceramic. Dent Mater. 2010;26(7):650-658.67. Wolfart M, Lehman F, Wolfart S, Kern M. Durability of the resin bond strength to zirconia ceramic after using different surface conditioning methods. Dent Mater. 2007;23(1):45-50.68. Zhang Y, Lawn BR, Rekow DE, Thompson VP. Effect of sandblasting on long-term performance of dental ceramics. J Biomed Mater Res B
Appl Biomater. 2004;71(2):381-386.69. Chintapalli RK, Marro FG, Jimenez-Pique E, Anglada M. Phase trans-formation and subsurface damage in 3Y-TZP after sandblasting. Dent Mater. 2013;29(5):566-572.70. Klosa K, Wolfart S, Lehmann F, et al. The effect of storage condi-tions, contamination modes, and cleaning procedures on the resin bond strength too lithium disilicate ceramic. J Adhes Dent. 2009;11(2):127-135. 71. Yang B, Lange-Jansen HC, Scharnberg M, et al. Influence of saliva con-tamination on zirconia ceramic bonding. Dent Mater. 2008;24(4):508-513. 72. Chen L, Suh BI, Shen H. Minimize the contamination of zirconia restoration surface with saliva [abstract]. J Dent Res. 2013;92(spec iss A). Abstract 1654.73. Feitosa SA, Patel D, Borges A, et al. Effect of cleaning methods on saliva-contaminated zirconia–An evaluation of resin bond durability. Oper Dent. 2014 Aug 19. [Epub ahead of print]74. Alex G. Preparing porcelain surfaces for optimal bonding. Compend Contin Educ Dent. 2008;29(6):324-336.75. Chen L, Shen H, Suh BI. Effect of incorporating BisGMA resin on the bonding properties of silane and zirconia primers. J Prosthet Dent. 2013;110(5):402-407.76. Suh BI, Shah M, Chen L. Additional resin or acidic monomer inhibits silane primer [abstract]. J Dent Res. 2014;93(spec iss A). Abstract 792.77. Hashimoto M, Tay FR, Svizero NR, et al. The effects of common errors on sealing ability of total-etch adhesives. Dent Mater. 2006;22(6):560-568.78. Luque-Martinez IV, Perdigao J, Munoz MA, et al. Effects of solvent evaporation time on immediate adhesive properties of universal adhe-sives to dentin. Dent Mater. 2014;30(10):1126-1135.79. Sundfeld RH, da Silva AM, Croll TP, et al. The effect of temperature on self-etching adhesive penetration. Compend Contin Educ Dent. 2006;27(10):552-557.

34 inside dentistry | August 2013 | www.insidedentistry.net
Larry BormanPresident, Tetra Dynamics, Inc.Full-Service Dental LabWest Babylon, New York
Gary aLex, DmDCo-director, The Long Island Center for advanced DentistryHuntington, New York
G-CeM™, GC America); and dual-cure resin cements that are used with a separate dBA (eg, relyX™ Ultimate Adhesive resin Cement, 3M esPe; dUO-LinK™, BisCO, inc., www.bisco.com; Multilink®, ivoclar Vivadent, www.ivoclarvivident.com).
it can be argued that the two classes of resin cements have a distinct advantage over rMGi cements when it comes to bonding restora-tions on or in minimally retentive preparations, because resin cements have the potential to bond more durably to both the tooth structures and the restorative material. they are also gen-erally the best choice when placing porcelain restorations that can be etched with hydroflu-oric acid and silane treated, as resin cements bond extremely well to etched porcelain and optimize overall assembly strength. the resin cements are also often the best choice for res-torations placed in the esthetic zone, because rMGi cements tend to be opaque and whitish in color and can “show through” many restora-tions, creating unacceptable esthetics.
Although self-etching/priming resin ce-ments have the obvious advantage of not
Due to the upsurge of new and innovative indirect ceramic, zirconia, and composite-based ma-terials, it is understand-able that dentists and laboratory technicians
are sometimes confused regarding optimal placement protocols. Questions often arise about whether the dentist’s current cementa-tion products and protocols are acceptable and compatible with these new materials, or whether an entirely new cementation system and protocol are required.
Understandably, most dentists prefer stick-ing with materials they already know, have, and trust. no dentist wants to have to pur-chase another cementation kit just to place a new prosthetic or restorative material they may use only occasionally or even abandon en-tirely. it is helpful to briefly examine the types of cements and resin adhesives currently in
use and determine their applicability when using these newer materials.
exploring the options Cementation options for indirect restorations usually entail the use of one of three distinct classes of materials: resin-modified glass iono-mers (rMGi) (eg, relyX™ Luting Plus Automix resin Modified Glass ionomer Cement, 3M esPe, www.3mespe.com; FujiCeM™ 2, GC America, www.gcamerica.com); self-etching/priming dual-cure resin cements that are used without a separate dentin bonding agent (dBA) (eg, relyX™ Unicem self-Adhesive Universal resin Cement, 3M esPe; Maxcem, Kerr Corporation, www.kerrdental.com;
New Material Options, New Cement SelectionsLabs share valuable insight and perspective when it comes to adhesionGary Alex, DMD, AAACD | Larry Borman
prACtiCe BuiLDinG LAB tALk
Exchange
Table 1
What to Look for in a Dual-Cure resin Cement
• Lowsolubility
• Lowfilmthickness(the current ISO standard for combined film thickness of the adhesive/cement is ≤25 μm; however, a film thickness ≤20 μm is much more ideal)
• Highcompressivestrength
• Highfracturetoughness
• Highflexuralstrength
• Easydeliveryandself-mixingcapability
• Easycleanup
• Nopostoperativesensitivity
• Predictableself-curemechanism(When light can’t reach an area of the restoration, it is still very important for the cement to cure predictably. Some “dual cure” materials actually do not self-cure nearly as well as they light cure. Ideally, a resin-based cement will self-cure as well as it light cures)

36 inside dentistry | August 2013 | www.insidedentistry.net
priming product to increase bond strength, but if a dentist is going to use a separate dBA, then it seems to make sense to pair it with a dual-cure cement for which it is specifically designed. Guidelines for choosing a dual-cure resin cement are found in table 1.
Guidance for new restorative materialsWith the introduction of any new restorative material, dentists and labs should carefully consider placement recommendations of the manufacturer. For example, one recent-ly introduced product—3M™ esPe™ Lava™ Ultimate restorative—is a resin nanoceramic, representing a new class of materials. As such, dentists may be unsure about the optimal placement protocol. Labs will often advise dentists to stay within the manufacturer’s product line when placing indirect restora-tions, and this logic is applicable when using this material. Lava Ultimate restorations can be placed using scotchbond™ Universal Adhesive (3M esPe) along with relyX Ultimate cement (a dual-cure resin cement). these three products are designed to work together. the resin cement has an integrated dark-cure activator that works in conjunc-tion with the adhesive to ensure complete curing even in the absence of light. the ce-ment was developed to work especially well with glass ceramics, but it is also indicated for composite and metal materials.
One additional feature of this cement that labs may find helpful to relay to dentists is that it is offered with try-in pastes in match-ing shades. these try-in pastes can be very useful during shade selection for final cemen-tation, and their water solubility allows them to be cleaned up easily from both the tooth and the restoration.
requiring a separate dBA, the highest bond strengths are generally achieved when a dual-cure resin cement is used in conjunction with a separate dBA. in fact, some studies have showed that even the self-etching/priming
“Cem” type cements perform better (in terms of bond strength) when a separate dBA is placed first.1-3 this extra bond strength may be important in some clinical situations, such as minimally retentive crown preparations.
Many dentists, when faced with the choice between using a self-etching/priming dual-cure resin cement or a dual-cure resin cement that requires a separate dBA, will be tempted to choose the self-etching product simply be-cause it is easier to use. the elimination of the dBA and the time savings that go with this are very appealing. However, if bond strength is truly a priority, the truth of the matter is that using a separate dBA first will optimize adhesion. As previously mentioned, a sepa-rate dBA can even be used with a self-etch/
exchange LAB tALk
this integrated system of cement, adhesive, and restorative material serves as a strong example of the benefits that can be achieved with new material options. to ensure maxi-mum efficiency and optimal results, even experienced dentists can gain from commu-nicating closely with their lab when a new restorative is introduced.
Cementation may not be one of the most frequent topics of conversation between the dentist and the lab, but that doesn’t mean that labs don’t have good advice to offer dentists when it comes to this important step. A lab expert’s advice on general topics, including reliable manufacturers and combinations and specific product recommendations, can help dentists shave time off the cementation procedure and achieve optimal results. Open lines of communication can help both parties keep each other apprised of their own expe-riences with new cements and materials, as well as news from trade shows and continut-ing education opportunities.
reliability and Simplification Both dentists and labs can appreciate the importance of simplified and time-saving systems, and both partners obviously have a strong interest in providing patients with restorations that will look natural and last for the long term. new material options can throw many established procedures into question, but by recommending and choos-ing cements from proven and reliable manu-facturers, labs and dentists can take much of the guesswork out of the process.
References1. Barcellos dC, Batista Gr, silva MA, et al. evaluation of bond strength of self-adhesive cements to dentin with or wihout application of adhesive systems. J Adhes Dent. 2011;13(3):261-265.2. Chen C, He F, Burrow MF, et al. Bond strengths of two self-adhesive resin cements to dentin with dif-ferent treatments. J Med Biol Eng. 2011;31(1):73-77.3. Pisani-Proença J, erhardt MC, Amaral r, et al. in fluence of different surface conditioning proto-cols on microtensile bond strength of self-adhesive resin cements to dentin. J Prosthet Dent. 2011;105 (4):227-235.
“Even experienced dentists can gain from communicating closely with their lab.”
Is someone on your staff the
2013 Dental Assistant of
the Year?
If you think so, learn more here:
www.dentalassistantoftheyear.com
2013 Dental assistant
of the Year
Dedication. Passion. Skill.

2 Compendium July | August 2008—Volume 29, Number 6
Abstract: When placing an indirect restoration such as a
porcelain veneer, inlay, or onlay, the intaglio surface is
typically treated in some fashion to ensure optimal bond-
ing to the resin-based adhesives and luting cements re-
quired to affix it to the tooth tissues. A variety of surface
preparation techniques have been advocated, including
the use of acids, particle abrasion, various adhesives, and
chemical couplers such as silane. There is often equivoca-
tion in the literature regarding the effectiveness of these
materials and surface preparation techniques. This article
will attempt to make some sense of the various method-
ologies currently advocated for the treatment of porce-
lain surfaces before placement.
Optimal surface preparation techniques for chemicaland/or mechanical bonding to porcelain substrates are cru-cial to ensure clinical success when placing indirect porcelainrestorations and, when required, repairing them intraorally.Clinicians are often confused regarding the most effective
way to treat the intaglio surfaces of indirect porcelain res-torations before placement with various adhesives and lut-ing resins. They are often equally perplexed about the “ideal”surface treatment for the intraoral repair of preexisting por-celain restorations. This is not surprising, as there appearsto be no clear consensus in the dental literature, among“opinion leaders,” or from dental manufacturers on exactlywhat the optimal surface treatment should, in fact, be. Den-tal laboratory technicians also appear to lack standardizedprotocols on how they should treat the surface of finishedporcelain. For example, in 2007, the author spoke with theowners and/or ceramists from 11 different dental laborato-ries regarding their specific surface treatment protocol beforesending out finished feldspathic porcelain veneers. All treat-ed the inner surface of the veneers with hydrofluoric acid(HF). Only two knew the actual concentration of the HFthey were using. Application times varied from as short as 30seconds to as long as 10 minutes. Several laboratory techni-cians stated they simply etched the veneers until the surfacelooked “frosty.” Some laboratories sandblasted the veneersbefore HF treatment and some did not. After etching, somelaboratories placed the veneers in an ultrasonic cleaner, some“steam” cleaned the veneers, some placed the veneers back inthe oven at a low temperature to “burn off ” any white “res-idue” left over from etching, and others merely rinsed themwith tap water. Three laboratories stated they “sometimes”used a basic solution to “neutralize the acid” after HF treat-ment, although they were not sure if this was a necessarystep. This author also questioned approximately 24 “opin-ion leaders” at a recent symposium1 regarding their recom-mendations for the intraoral repair of both composite andporcelain restorations. While there were many similarities,there were also significant differences, and no treatmentprotocols were exactly the same.
Preparing Porcelain Surfaces for Optimal Bonding
Gary Alex, DMD*
Learning Objectives:
After reading this article, the reader should be able to:
n discuss how hydrofluoric acid etching affects thebonding potential of porcelain materials.
n describe how silane reacts with porcelain and creates a bond.
n explain the approach required to bond high-contentalumina and zirconia core-based ceramics.
n compare the general treatment protocols for porcelain veneers that have been etched and havenot been etched in the dental laboratory.
*Co-director, Long Island Center for Dental Esthetics and Occlusion; Private Practice, Huntington, New York
Continuing Education 1

Alex
www.compendiumlive.com Compendium 3
The lack of clear and consistent guidelines regarding thetreatment of composite and porcelain surfaces raises severalsignificant questions. Is there, in fact, an optimal surfacetreatment protocol for porcelain restorations before place-ment and for intraoral repair? Is it possible that several viablesurface treatment options exist? Is it even practical to recom-mend a specific “universal” treatment protocol because ofmaterial differences (eg, not all porcelains are the same)?
This article will attempt to address these questions, pro-vide some general guidelines, and no doubt raise additionalquestions regarding the management of porcelain surfaces. Agood place to start is by examining what we “think” we know.
BONDING TO PORCELAIN—USE OF HFHF is an inorganic acid capable of etching glass surfaces. Ithas been used for hundreds of years to create decorativedesigns and patterns on glass and various ceramic materi-als.2 It is also used as a precursor in the manufacturing ofnumerous pharmaceuticals, various polymers (eg, Teflon),and many other synthetic materials that contain fluorine.3
Contrary to what most dentists believe, because of its lowtendency to dissociate into H+ and F- ions, HF is consid-ered to be a relatively weak acid from a chemical stand-point. This doesn’t mean HF is not dangerous. Quite thecontrary; due to its low dissociation potential, HF has theability to readily penetrate skin tissues (often without caus-ing an external burn),where it can cause extensive internaltissue damage, as well as alter blood calcium levels (due tothe formation of CaF2), which can lead to dangerous heartarrythmias.4 There have been industrial accidents wheredeath has occurred from accidental skin exposure to HF.5
The duration of exposure, the concentration of HF, and thetotal surface area affected will obviously have an effect onclinical outcomes relating to accidental dermal exposure.6
In typical dental applications (eg, the etching of porcelainveneers and the intraoral repair of fractured porcelain res-torations), concentrations of 4% to 10% HF are typicallyused. In this author’s opinion, HF in this concentrationrange can be used safely for dental procedures, includingintraoral repair, provided caution and common sense areemployed. Whenever HF acid is used for intraoral repair,the use of appropriate barrier techniques, viscous HF gelformulations (ie, that stay where you put them), and con-tinual visual observation during the application period aremandatory. For those dentists not comfortable with the in-traoral use of HF, acidulated phosphate fluoride gel (APF)
has been shown to have the ability to etch porcelain, al-though the application time must be considerably longerthan for HF etching. One recent study showed that a 7- to10-minute application of 1.23% APF gel on a leucite-containing porcelain (IPS Empress®, Ivoclar Vivadent, Inc,Amherst, NY) produced a shear bond strength to compos-ite (Filtek™ Z250 Universal Restorative, 3M ESPE, St.Paul, MN) similar to a 4-minute etch with 9.6% HF.7 Itshould be pointed out that this same study showed thatetching with 9.6% HF for 4 minutes resulted in a very def-initive microscopic etching pattern, while etching for 7 to10 minutes with 1.23% APF resulted in a pitted, but muchsmoother-appearing surface. This difference in surface mor-phology could be significant over the long term, and it wouldhave been interesting to see what effect thermocyling ofthe samples, which was not done, would have had on bondstrength. Also, it is unclear why the investigators used 9.6%HF for 4 minutes when the manufacturer of the porcelaintested recommends that 5% HF acid be used for only 60 sec-onds. It is possible that the bond strength to the HF-treatedporcelain samples would have been even higher had the man-ufacturer’s recommended protocol been followed. Otherstudies have also shown that etching with APF, even withprolonged application times, results in very shallow etchingpatterns when compared with HF etching for much shortertime periods.8 Silica coating, followed by silane application,has also been explored as an alternative to HF etching offeldspathic-based porcelains. The authors of one study foundthat both the high and low leucite-containing feldspathicporcelains they tested had significantly higher tensile bondstrength to composite when samples were first etched withHF followed by silane treatment, vs just silica coating fol-lowed by the application of silane.9 Still another study look-ing at alternatives to HF etching found that simply rough-ening porcelain surfaces, followed by treatment with 35%phosphoric acid gel and silane priming, was as effective as HFtreated samples to bonded composite.10 Once again, thermo-cyling of the samples, which was not done, might have had asignificant effect on the results. Other products also exist andare marketed as alternatives to HF etching of porcelain.
In this author’s opinion, while other alternatives do exist,they are less predictable, especially over the long term, whencompared with HF-etched porcelain. Numerous in vitrostudies clearly demonstrate that etching feldspathic-basedporcelain with HF has the potential to significantly increaseits bond strength to composite resin.10-16 Dental porcelain

generally consists of an amorphous glassy phase or matrix anda crystalline phase. Treating porcelain with HF tends to selec-tively dissolve the glassy matrix, resulting in a microscopical-ly porous, high-energy, and microretentive surface12,17,18
(Figure 1). In principle, this is similar to what happens toenamel surfaces after etching with phosphoric acid.
Several important questions arise when using HF to etchporcelain. Is there an optimal etching time and concen-tration of HF that should be used? Can porcelain be over-etched? What is the white “residue” often seen on the surfaceof the porcelain after etching with HF, and how should it behandled? The first question is not easily answered. This isbecause the chemical and physical makeup of dental porce-lain is variable, depending on the type of ceramic beingused. Years ago, Calamia recommended adjusting the etch-ing times and concentration of HF depending on the specif-ic porcelain being treated.19 While all feldspathic porcelainscontain silica dioxide (SiO2), aluminum oxide (Al2O3), andpotassium oxide (K2O), the relative amount of each can varyconsiderably depending on the specific porcelain used. Alu-mina content, crystalline microstructure, size, and concen-tration can all influence HF etching times and concentra-tions.11,20,21 As an example, leucite crystals, which affectoptical, thermal, and physical properties, are incorporatedinto the matrix of many dental porcelains.22,23 A study byBarghi showed a 50% leucite content porcelain (Fortress™,
Chameleon Dental Products, Inc, Kansas City, KS) requireda longer etching time (ie, 150 to 180 seconds) with 10% HFwhen compared with a 27% leucite content ceramic (Ce-ramco® II, DENTSPLY Ceramco, Burlington, NJ) that onlyrequired a 60-second etch with 10% HF.24 Some manufac-turers recommend very specific HF concentrations and etch-ing times for their ceramics. The manufacturer of one pop-ular pressable ceramic (IPS Empress), which has a reportedleucite concentration of 35% to 40%, recommends etchingfor 60 seconds with 5% HF.25,26 Longer etching times orhigher concentrations of HF with this particular ceramicmay actually result in “overetching” and weakening of theporcelain substrate by excessively degrading the surface.26 Atleast one study supports this contention and found that ex-tending the etching time of this particular ceramic’s ingotsfrom 1 to 2 minutes with 5% HF significantly decreased thebiaxial flexure strength of the ceramic.27 The manufacturerof another popular pressable leucite reinforced ceramic (Au-thentic®, Jensen Industries, Inc, North Haven, CT) recom-mends “lightly sandblasting the internal surface with 50 µmAl2O3 at a maximum of 20 PSI and then placing 5% to 12%HF for 90 seconds to 5 minutes.”28 One logical interpreta-tion of this is that dentists could use 12% HF for 90 secondsor 5% HF for 5 minutes. So, one manufacturer (IvoclarVivadent, Inc) recommends etching with 5% HF for 1 mi-nute when treating the inner surface of its leucite containingpressable ceramic, and another manufacturer (Jensen Indus-tries, Inc) appears to recommend etching with 5% HF for5 minutes when treating its leucite containing pressable ce-ramic. Why there is such a difference in recommended 5%HF application times between these two ceramics is difficultto understand. It is certainly possible that a difference inleucite concentration, size/orientation of crystals, or mi-crostructure might affect etching times. According to onesource,29 the leucite concentration for the aforementionedpopular pressable ceramic (Authentic) is approximately 8%,depending on the shade. This author was unable to corrob-orate this information despite an extensive Internet searchand several phone and e-mail contacts with representativesof the manufacturer. At least one company representativesuggested etching the ceramic with 7% HF for 1 to 2 min-utes, although it was unclear on what this recommenda-tion was based.30
Two lithium disilicate-based ceramics (IPS e.max® CAD,IPS e.max® Press, Ivoclar Vivadent, Inc) replaced the manu-facturer’s now defunct product (IPS Empress® II).26 The
Continuing Education 1
4 Compendium July | August 2008—Volume 29, Number 6
Figure 1 Typical “honeycomb” pattern seen in a scanning
electron micrograph of a stackable (ie, powder/liquid) felds-
pathic porcelain etched, in this case, for 5 minutes with 4%
HF. A similar etching pattern is observed when 9% to 10%
HF is applied for 90 seconds. Etching with HF creates a high-
energy, retentive, and hydrophilic surface.

Alex
www.compendiumlive.com Compendium 5
manufacturer of these products recommends a very specificetching time of only 20 seconds with 5% HF,25,26 and stud-ies exist supporting this protocol.17,31 Powder/liquid or“stackable” porcelains (Ceramco® 3 and Duceram® Plus,DENTSPLY Ceramco; Omega® 900 and VMK-68, Vident,Brea, CA; EX-3, Noritake Dental Supply Co, Ltd, Aichi,Japan; IPS d.SIGN®, Ivoclar Vivadent, Inc; Creation®, JensenIndustries, Inc) are used extensively in the fabrication of ce-ramic restorations. Some opinion leaders/studies recom-mend 90 seconds of etching with 10% HF for stackablefeldspathic porcelains,32 while others recommend a 120- to150-second etch with 9.5% HF.33 The manufacturers oftwo popular 9.5% HF etching gels (HF etching gel, Bisco,Inc, Schaumburg, IL; HF etching gel, Ultradent Products,Inc, South Jordan, UT) recommend etching times of 90 sec-onds (ie, the former manufacturer) and 60 seconds (ie, thelatter manufacturer).34
In an unpublished study, Byoung Suh tested 10 differentfeldspathic porcelains (Synspar® and OPC®, Pentron Clin-ical Technologies, LLC, Wallingford, CT; IPS d.SIGN;CZR Press, Noritake Dental Supply Co, Ltd; Vintage™,Shofu Dental Corp, San Marcos, CA; Vita®, Vident; Initial,GC America, Inc, Alsip, IL; Ceramco® II and Duracem®,DENTSPLY Ceramco; and Creation, Jensen Industries,Inc) by HF etching (ie, 9.5% and 4%), followed by con-tact angle analysis and microscopic evaluation. He firstparticle-abraded the samples (ie, sandblasting) and foundthey all showed an acceptable microscopic etching patternafter a 4- to 5-minute etch with 4% HF. These same porce-lains showed a similar etching pattern when 9.5% HF wasused for 90 seconds.35 The authors of another study foundstatistically higher composite shear bond strength to severalstackable porcelain disks when they were etched with 10%HF for 2 minutes as opposed to a longer etch of 4 minutesat the same HF concentration. They attributed the lowerbond strength with the longer etching time of 4 minutes to“overetching” and actual weakening of the porcelain sur-face.36 The manufacturer of a popular laboratory ceramicetching gel sells a 12% to 13% HF etching gel for stackableporcelains (Etch-It Kit, American Dental Supply, Inc, Al-lentown, PA) and recommends what, to this author, ap-pears to be a rather long etching time of 10 to 15 minutes.According to the manufacturer, this application time wasbased on observation of the contact angle of water dropletsplaced on ceramic surfaces and the microscopic appearanceof the porcelain surface after etching for different time periods
(no shear or tensile bond testing was performed).37 Inter-estingly, this same manufacturer sells another product mar-keted for pressed ceramics (Etch-It Kit for pressable por-celain, American Dental Supply, Inc) that uses 5% HF witha recommended etching time of only 30 to 60 seconds.
Most dentists and ceramists have noticed that a white“residue” sometimes remains on the surface of HF-etchedporcelain restorations. At times this residue can be quiteextensive and cover virtually the entire etched porcelain sur-face. The extent of this precipitate is no doubt related to thetype of porcelain, concentration of HF, and the time of ap-plication. One study, through energy dispersive spectrometeranalysis, determined this residue to consist of the re-action products of porcelain and HF.38 Basic chemistry hasshown that when an acid and base react, various salts are pro-duced as byproducts of the reaction. In the case of HF etch-ing, the porcelain acts as a base, and when it reacts with HF,various insoluble metallic salts are formed.31 In this author’sopinion, the white residue consists not merely of “porcelainsalts,” but also of numerous microscopic crystalline fragmentsexposed, possibly weakened by HF exposure, and displacedafter the glassy matrix supporting them has been dissolved byHF and the porcelain surface washed and dried. This waterinsoluble “crystalline residue/salt mix” rather tenaciously
Figure 2 In this example, the intaglio surface of a porcelain
veneer was purposely overetched by the author with 9.5%
HF placed for 15 minutes. Much of the clearly visible “white
residue,” a combination of porcelain salts and porcelain
debris, could not be removed even after an aggressive air/
water spray for 2 minutes and wiping with cotton pellets
soaked in acetone.

Continuing Education 1
6 Compendium July | August 2008—Volume 29, Number 6
adheres to the porcelain surface and is often difficult toremove. While many believe this white “frosting” to be indica-tive of a “good etch” of the porcelain, this is probably an inac-curate assessment. In fact, in this author’s opinion, if the whiteprecipitate is excessive, this may be indicative of overetchedporcelain (Figure 2). Several authors have discussed the poten-tial for overetching porcelain and how this could adverselyaffect porcelain physical properties and/or bond strength tocomposite.15,27,36,39-42 In any case, this surface residue is apotential contaminant, and it makes sense to remove it beforeproceeding to the bonding phase of treatment.
In this author’s experience, removal of this material withwater alone is usually not effective, even after a vigorous air/water spray. Acetone or alcohol rubbing is only slightly moreeffective. This author has found that placing the etched restora-tions in an ethanol solution followed by ultrasonication for5 minutes is usually, but not always, effective in removing anyresidue (Figure 3A through Figure 3C). Sometimes light brush-ing with a toothbrush and/or longer ultrasonication times arealso required. Other authors have recommended a similarprotocol using distilled water.32 This author prefers an alcoholsolution because it evaporates more easily than water and isprobably a better solvent when it comes to removing poten-tial contaminates (eg, grease and oils from handling, surfac-tants from acid gels, saliva, try-in paste residue, etc). Otherauthors have recommended the use of steam cleaning to re-move any residue/salts left after HF etching of porcelain.43
In any case, the idea is to have an etched, clean, reactive, andhigh-energy surface before the next phase of porcelain surfacepreparation (ie, treatment with a silane coupling agent).
BONDING TO PORCELAIN—USE OF SILANESilanes are a class of organic molecules that contain one ormore silicon atoms. Dozens of different silane compoundsexist, and they are used extensively in industry and manu-facturing. The specific silane typically used in dentistry forboth intraoral repair and treatment of ceramic restorationsbefore placement is 3-methacryloxypropyltrimethoxysilane.(Note: all other use of the term “silane” in this article willrefer specifically to this monomer.)
In dentistry, silane is potentially useful as a chemicalcoupler linking organics (ie, resin-based materials) to inor-ganics (eg, porcelain, some oxidized metals, and glass fillersin resin-based composites). A number of theories—rangingfrom its ability to simply act as a good wetting agent to theactual formation of covalent chemical bonds at the involved
Figure 3A through Figure 3C A useful technique for cleaning veneers is to place them in ethanol followed by ultrasonication.
In this case, a full 15 minutes of ultrasonication was required to remove the white residue on the veneer depicted in Figure 2.
The silane most often used in dentistry is the 3-methacryloxy-
propyltrimethoxysilane, which is a difunctional molecule. The
left side of this molecule is nothing more than a methacrylate
group capable of copolymerization with methacrylate-based
adhesives and resins routinely used for dental procedures. The
right side, after hydrolysis, has the potential to form chemical
bonds to the porcelain surface.

Alex
interfaces—exist regarding how silane actually functions.44-46
(This author highly recommends an excellent paper on silanechemistry and interactions written by Meyer Rosen in 1978while working for Union Carbide.44) Infrared spectroscopyhas shown that silane has the potential to react with hydrox-yl (-OH) groups present on the surface of porcelain and metalsubstrates.46-48 To be able to function as a coupling agent andinteract chemically with porcelain surfaces, silane must first behydrolyzed.45 Acetic acid is commonly used to “activate” orhydrolyze silane by reacting with the three methoxy (-OCH3)groups located at one end of the silane molecule (Figure 4).Ideally, all three of the terminal methoxy groups will con-vert to -OH groups, although only one or two may actuallyreact, resulting in incomplete hydrolysis and a potentiallyless effective silane.46,47
Single-bottle silanes are prehydrolyzed by the manufac-turer and, while variations in chemistry exist, typically con-sist of 1% to 5% silane in a water/ethanol solution with anacetic acid adjusted pH of 4 to 5.44,45 Once hydrolyzed,silane molecules have a tendency to react with one another,forming high-molecular-weight oligomers44,47 (ie, poly-siloxanes) that can actually function as a lubricant49-51 andpotentially decrease bond strength to porcelain. It is impor-tant to remember that one-bottle prehydrolyzed silane solu-tions have a limited shelf life, and this author recommendsrefrigerated storage and replacement after 1 year, as well asbringing refrigerated silane to room temperature before use.If the silane solution appears at all cloudy or “milky” inappearance, or any type of precipitate is noticed, it shouldbe discarded.
Two-bottle silane systems typically consist of an unhy-drolyzed silane/ethanol solution in one container and anacetic acid/water solution in the other.35 These are mixedtogether by the clinician to hydrolyze the silane before ap-plication. It is unclear to this author precisely how muchtime is required for an acceptable degree of hydrolysis to oc-cur once the solutions of two-part silane systems are mixed.The authors of one paper state “0.5 to 2 hours should besufficient,”45 while another author cites a study showinghydrolysis was “complete 10 minutes after mixing with0.1% acetic acid.”44 The authors of another study deter-mined the hydrolysis rate of silane by the use of Ramanspectroscopy and determined that 30 to 50 minutes wasrequired.52 Still another study found that the two-part sys-tem (Silanit, Ivoclar Vivadent, Inc) they tested did not havethe same degree of hydrolysis 20 minutes after activation
when compared with the two prehydrolyzed systems theytested.47 One reputable manufacturer and respected research-er stated to this author that, based on contact angle analysisand in-house testing, its two-part silane was effective immedi-ately after mixing, but performed optimally if left alone on theporcelain surface for 5 minutes after it was applied.35 This isprobably an indication of further hydrolysis of the silaneand/or increased chemical interaction with the porcelain dur-ing the waiting period. Two-bottle systems should have alonger shelf life than premixed systems and might be a betterchoice for dentists whose use of silane is infrequent.
The important point to remember is that the goal of sil-ane hydrolysis is to create terminal hydroxyl groups on eachsilane molecule. These hydroxyl groups are then capable ofreacting directly with corresponding hydroxyl groups pres-ent on the surface of feldspathic porcelain (through oxida-tion of SiO2). The opposing hydroxyl groups interact withone another (via hydrogen bonding) and then, through acondensation polymerization (ie, loss of water) reaction,covalent bonds are formed between the silane and porce-lain. Not only does the silane bond directly to the porcelainin this fashion, but also the individual silane moleculesbond to one another, forming a polymer “network” on theporcelain surface44 (Figure 5 and Figure 6). In theory, theideal situation would be one in which a “monolayer” of sil-ane molecules lines the surface of the porcelain.45 Clinically,
www.compendiumlive.com Compendium 7
Figure 4 This diagram demonstrates unhydrolyzed silane
(ie, 3-methacryloxypropyltrimethoxysilane) on the left. To
be able to function as a coupling agent and interact chemi-
cally with porcelain surfaces, silane must first be hydrolyzed.
Acetic acid is commonly used to “activate” or hydrolyze
silane by reacting with the three methoxy (-OCH3) groups
located at one end of the silane molecule and replacing
them with hydroxyl (-OH) groups. Silane in the active form
is shown on the right.
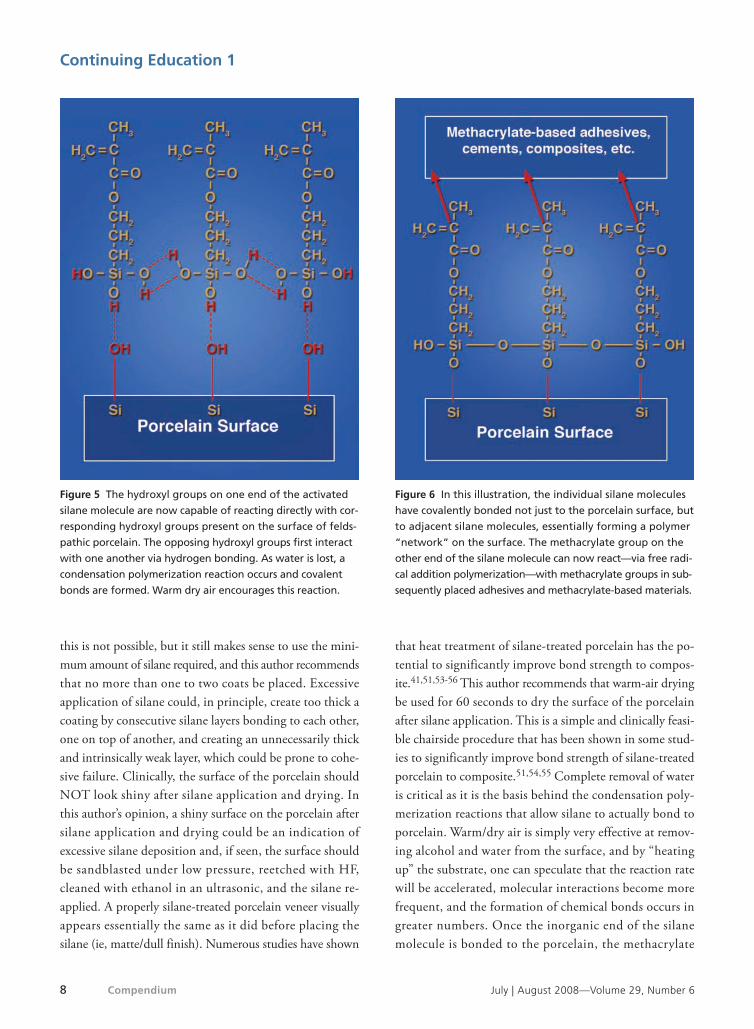
this is not possible, but it still makes sense to use the mini-mum amount of silane required, and this author recommendsthat no more than one to two coats be placed. Excessiveapplication of silane could, in principle, create too thick acoating by consecutive silane layers bonding to each other,one on top of another, and creating an unnecessarily thickand intrinsically weak layer, which could be prone to cohe-sive failure. Clinically, the surface of the porcelain shouldNOT look shiny after silane application and drying. Inthis author’s opinion, a shiny surface on the porcelain aftersilane application and drying could be an indication ofexcessive silane deposition and, if seen, the surface shouldbe sandblasted under low pressure, reetched with HF,cleaned with ethanol in an ultrasonic, and the silane re-applied. A properly silane-treated porcelain veneer visuallyappears essentially the same as it did before placing thesilane (ie, matte/dull finish). Numerous studies have shown
that heat treatment of silane-treated porcelain has the po-tential to significantly improve bond strength to compos-ite.41,51,53-56 This author recommends that warm-air dryingbe used for 60 seconds to dry the surface of the porcelainafter silane application. This is a simple and clinically feasi-ble chairside procedure that has been shown in some stud-ies to significantly improve bond strength of silane-treatedporcelain to composite.51,54,55 Complete removal of wateris critical as it is the basis behind the condensation poly-merization reactions that allow silane to actually bond toporcelain. Warm/dry air is simply very effective at remov-ing alcohol and water from the surface, and by “heatingup” the substrate, one can speculate that the reaction ratewill be accelerated, molecular interactions become morefrequent, and the formation of chemical bonds occurs ingreater numbers. Once the inorganic end of the silanemolecule is bonded to the porcelain, the methacrylate
Continuing Education 1
8 Compendium July | August 2008—Volume 29, Number 6
Figure 5 The hydroxyl groups on one end of the activated
silane molecule are now capable of reacting directly with cor-
responding hydroxyl groups present on the surface of felds-
pathic porcelain. The opposing hydroxyl groups first interact
with one another via hydrogen bonding. As water is lost, a
condensation polymerization reaction occurs and covalent
bonds are formed. Warm dry air encourages this reaction.
Figure 6 In this illustration, the individual silane molecules
have covalently bonded not just to the porcelain surface, but
to adjacent silane molecules, essentially forming a polymer
“network” on the surface. The methacrylate group on the
other end of the silane molecule can now react—via free radi-
cal addition polymerization—with methacrylate groups in sub-
sequently placed adhesives and methacrylate-based materials.

group on the other end is free to bond (via free radical ad-dition polymerization) with methacrylate groups in resin-based dental materials and adhesives (Figure 6).Whilethere is equivocation in the literature,11 it appears thatmost studies find proper use of silane significantly im-proves the bond strength of resin-based composites toporcelain.10,15,57-60
BONDING TO PORCELAIN: HIGH-CONTENT ALUMINA ANDZIRCONIA CORE-BASED CERAMICS High-content alumina and zirconia core-based ceramics (In-Ceram®, Vident; Procera® All-Ceram, Nobel Biocare USA,LLC, Yorba Linda, CA; LAVA™, 3M ESPE; Wol-Ceram®,Wolz Dental-Technik GmbH, Ludwigshafen, Germany;Cercon®, DENTSPLY Ceramco; CEREC® InLab, SironaDental Systems USA, Charlotte, NC; Everest®, KaVo Den-tal Corp, Lake Zurich, IL) are highly resistant to chemicalattack from HF,11,61-63 and a different approach is requiredif the clinician elects to bond these restorations into placeusing resin-based adhesives and luting cements (as opposedto conventional cementation). One method that has beenshown to be quite effective in increasing bond strength tothese materials is the technique of silica coating followed bysilane application.61-63 One simple and effective techniqueuses silica-coated 30-µm aluminum oxide particles (CoJet™Sand, 3M ESPE) followed by the application of silane. Ac-cording to the manufacturer, sandblasting with this materialuses “impact energy to apply a silica coating to the targetsurface.”64 Whether this transfer of silica is caused by parti-cles actually becoming embedded in the target surface, actu-al mechanical/chemical transference (ie, tribochemistry), orboth, is unclear to this author. In this author’s opinion, it isunlikely that, in the case of high alumina or zirconia cores,there is actual imbedding of silica-coated particles because ofthe intrinsic hardness of the target material. It may be morefeasible that the silica-coated particles actually “bounce off”these ceramics, but before doing so there is an actual trans-ference of silica from the particles to the target substrate (ie,tribochemistry). In any case, this technique has proven to beeffective (more so than conventional sandblasting) not justwith high-strength alumina and zirconia-based ceramics,but also when bonding to composite65,66 and metal sur-faces.67-69 One can speculate that by silica-coating metal orcomposite substrates, not only is the surface mechanically
roughened, but the number of available hydroxyl groups forsurface silane coupling is significantly increased. Silica coat-ing is not effective, or required, with conventional feldspath-ic porcelains simply because significant amounts of SiO2
and free hydroxyl groups are already present (much more sothan metals and composites). If the dentist opts to conven-tionally cement zirconia or high alumina core-based crowns/bridges, silane is not required. However, this author stillrecommends briefly sandblasting the inner surface of therestoration under low pressure (ie, approximately 20 PSI),followed by placement with whatever conventional ce-ment is chosen by the dentist. (This author prefers resin-modified glass ionomer cements [RelyX™ Luting Plus,3M ESPE; FujiCEM, GC America, Inc]). Care should betaken when sandblasting these restorations, making sureto use low pressure for short time periods, as at least onestudy has found that sandblasting with 50-µm AL2O3 (at40 PSI) had the potential to induce flaws in dense alu-mina and zirconia ceramic plates, resulting in decreasedphysical properties.70
UNDERSTANDING ALL OF THISAfter a fairly extensive literature review, numerous discus-sions with manufacturers, laboratory technicians, and re-searchers, it is apparent to this author that no single specificHF concentration and application time exists that is opti-mal for etching all porcelains. As a consequence, it is notsurprising that currently recommended HF concentrationsand application times vary significantly. It also appears thatthere is potential to both underetch and overetch porcelain.As Calamia suggested years ago,19 HF concentrations andapplication times should, ideally, be adjusted depending onthe specific nature of the porcelain being treated. In thisregard, dentists are somewhat at the mercy of manufacturers,and it should be incumbent on them to provide accurateand scientifically supported recommendations on preciselyhow to optimally treat and place their specific product(s). Itis then incumbent on dentists and ceramists to actually followthese protocols. As it is, even when specific protocols do exist,this author suspects they all too often are ignored, not under-stood, or dentists and ceramists are simply not aware of them.In regards to etching porcelain, one goal should be to deter-mine the time frame required, at a very specific HF concentra-tion that will adequately etch various porcelains without ex-cessively degrading and/or weakening the substrate.
Alex
www.compendiumlive.com Compendium 9

In any case, while recognizing that exceptions are likelyto exist, it is probably safe to make some generalizations re-garding porcelain surface treatment.
1. It appears that low-pressure sandblasting, followed by60 to 120 seconds of etching with 9% to 10% HF, hasscientific support and validity when treating conven-tional powder/liquid stackable porcelains. A variationthat also appears effective is sandblasting followed by4% to 5% HF applied for 4 to 5 minutes.
2. In the case of a popular pressable ceramic (IPS Em-press), the recommended treatment protocol of 5% HFapplied for 60 seconds has scientific support and shouldbe followed. The manufacturer of this particular prod-uct is one of the few that this author found to have veryspecific recommendations, as far as HF concentrationsand application times, for a number of its bondable ce-ramics. Specific manufacturer recommendations formany of the other pressable and/or high leucite con-taining ceramics are vague, do not exist, or could not befound and/or verified by this author. Some ceramicmanufacturers shift responsibility by simply recom-mending following the directions of the manufacturerof whatever HF-etching gel or liquid is being used. As aresult, specific treatment protocols appear to be largelyspeculative. Perhaps these are the restorations manyceramists stated (to this author) that they simply etchuntil the “surface looks frosty.” While this is certainlynot very scientific, and likely not optimal, in the ab-sence of specific guidelines, it may be the best ceramistsand dentists have in some situations.
3. High-strength alumina and zirconia core-based crownscannot be etched with HF. As a result, it is not possibleto “bond” these restorations with conventional HF/silane treatment. Silica coating, followed by silane ap-plication, has been shown to be a viable alternative.
4. Proper use of hydrolyzed silane, in conjunction withwarm-air drying, has scientific support and is advisableafter HF etching of feldspathic porcelains or silica coatingof high alumina, zirconia, metal, and composite surfaces.
TREATMENT PROTOCOLSTwo general treatment protocols successfully used by the au-thor for surface treatment of stacked (powder/liquid) porce-lain veneers before placement are presented below. Theseprotocols may not be valid for all stacked porcelains and
when available, manufacturer recommendations regardingetching times and HF concentrations should be followed.The first protocol assumes that the veneers are not etched atthe dental laboratory. The advantage of this protocol is thatthe dentist has complete control over the surface prepara-tion. In the second protocol, the veneers have been etched atthe dental laboratory. This requires a certain degree of faithin the laboratory technician and assumes he or she has prop-erly etched the porcelain. The author recognizes other pro-tocols exist, are valid, and are clinically successful.
Protocol 1—Veneers NOT Etched by the Dental Laboratory
1. Try in case for fit and esthetics. Once the decision toplace the veneers is made, proceed to Step 2.
2. Briefly sandblast veneers under low pressure (ie, 20 PSI)with 50-µm Al2O3 or 30-µm aluminum oxide particles.
3. Etch with 9% to 10% HF gel for 90 seconds, wash,and dry.
4. Ultrasonicate for 5 minutes in ethanol; dry well.5. Apply one to two coats of prehydrolyzed silane and
warm-air dry for 60 seconds.6. Place a thin layer of hydroxyethylmethacrylate (HEMA)-
free unfilled resin (Porcelain Bonding Resin, Bisco, Inc).Do not cure. HEMA-free resins are less hydrophilicthan HEMA-containing resins and may be less prone towater sorption.
7. Fill veneers with a light-cure only resin veneer cement(RelyX™ Veneer Cement, 3M ESPE; Choice™ 2, Bis-co, Inc) and bond in place. Veneer cements that have adual-cure capacity contain tertiary aromatic aminesthat may discolor with time, potentially altering theshade of the veneers.71-73
Protocol 2—Veneers Etched by the Dental Laboratory
1. After receiving the veneers from the dental laboratory,inspect the inner surface. Properly etched veneers shouldhave a dull/matt finish and no shiny areas. If the veneershave shiny areas, briefly sandblast and reetch with 9%to 10% HF for 90 seconds. If the veneers appear welletched, proceed to Step 2.
2. Ultrasonicate for 5 minutes in ethanol; dry well. (Note:an alternative to using an ultrasonic is to clean the ve-neers with phosphoric acid, wash, and dry.) The basicidea is to ensure a clean, fresh, high-energy surface before
Continuing Education 1
10 Compendium July | August 2008—Volume 29, Number 6

applying silane, as it may be possible the veneers were con-taminated from normal handling and exposure at somepoint between the laboratory and the time of placement.
3. Before the veneers are tried in, apply one to two coats ofprehydrolyzed silane and warm-air dry for 60 seconds.
4. Try in veneers to access fit and esthetics. (Note: this au-thor rarely uses try-in pastes.) After approval, place theveneers back in the ultrasonic to remove any surfacecontaminates. Silane does not need to be reapplied.
5. The cleaned veneers should be dried thoroughly andbrushed with a thin coat of HEMA-free bonding resin.(Note: See Step 6, Protocol 1.)
6. Perform the same as Step 7, Protocol 1.
An acceptable variation in this protocol is to try in theveneers before cleaning with phosphoric acid, ultrasonica-tion, and application of silane.
CONCLUSIONOptimizing porcelain surfaces before treatment with vari-ous adhesives and luting resins requires an understandingof the involved substrates and materials, as well as a logicaland systematic methodology in their manipulation. It isclear that while much is known, even more remains to belearned. It is hoped that this article has answered some ques-tions, raised others, and provided greater insight into the na-ture of bonding to porcelain.
ACKNOWLEDGEMENTThe author would like to thank Byoung Suh of Bisco, Incfor allowing the author unfettered use of his scientific facili-ties for personal testing of materials, as well as many years ofmentorship, encouragement, insight, advice, and friendship.
REFERENCES1. 3M ESPE Symposium. July 2007;Wonewok, Minnesota.2. Matcham J, Dreiser P. The Techniques of Glass Engraving. 1982;
London, England: Larousse Art Craft Series, B.T. Bratsford LTD.3. Wikipedia. Available at: http://en.wikipedia.org/wiki/Hydro
fluoric_acid. Accessed Dec 21, 2007.4. Rich WM. By what mechanism does hydrofluoric acid cause
death? Posted May 19, 1998. Available at: http://www.madsci.org/posts/archives/1998-05/895674112.ME.R.HTML. Ac-cessed Dec 21, 2007.
5. Muriale L, Lee E, Genovese J, et al. Fatality due to acute fluo-ride poisoning following dermal contact with hydrofluoric
acid in a palynology laboratory. Ann Occup Hyg. 1996;40:705-710.
6. Sullivan JB, Krieger GR. Hydrofluoric acid. In: Hazardous Ma-terials Toxicology: Clinical Principles of Environmental Health.Baltimore, MD: Williams & Wilkins; 1992.
7. Kukiattrakoon B, Thammasitboon K. The effect of differentetching times of acidulated phosphate fluoride gel on the shearbond strength of high-leucite ceramics bonded to compositeresin. J Prosthet Dent. 2007;98:17-23.
8. Canay S, Hersek N, Ertan A. Effect of different acid treat-ments on a porcelain surface. J Oral Rehabil. 2001;28:95-101.
9. Boscato N, Della Bona A, Del Bel Cury AA. Influence of ceram-ic pre-treatments on tensile bond strength and mode of failure ofresin bonded to ceramics. Am J Dent. 2007;20:103-108.
10.Kussano CM, Bonfante G, Batista JG, et al. Evaluation of shearbond strength of composite to porcelain according to surfacetreatment. Braz Dent J. 2003;14: 132-135.
11 Sorensen JA, Engelman MJ, Torres TJ, et al. Shear bond strengthof composite resin to porcelain. Int J Prosthodont. 1991;4:17-23.
12.Hussain MA, Bradford EW, Charlton G. Effect of etching onthe strength of aluminous porcelain jacket crowns. Br Dent J.1979;147:89-90.
13.Suliman AH, Swift EJ Jr, Perdiago J. Effects of surface treat-ment and bonding agents on bond strength of composite resinto porcelain. J Prosthet Dent. 1993; 70:118-120.
14.Della Bona A. Characterizing ceramics and the interfacial ad-hesion to resin: the relationship of surface treatment, bondstrength, interfacial toughness and fractography. J Appl OralSci. 2005;13(2):101-109.
15.Chen JH, Matsumura H, Atsuta M. Effect of etchant, etchingperiod, and silane priming on bond strength to porcelain ofcomposite resin. Oper Dent. 1998; 23:250-257.
16.Kondo M, Ikeda M, Takeuchi N, et al. [Study on the porcelainveneer restoration. 3. Effect of various treatments of porcelainsurface on the bonding strength at porcelain-resin interface].Aichi Gakuin Daigaku Shigakkai Shi. 1990;28:631-638.
17.Pisani-Proenca J, Erhardt MC,Valandro LF, et al. Influence ofceramic surface conditioning and resin cements on microten-sile bond strength to a glass ceramic. J Prosthet Dent. 2006;96:412-417.
18.Olorunfemi BO. Hydrofluoric acid etching of Flexoceram in-lay porcelain: A microscopic study. Saudi Dental J. 1995;7:82-86.
19.Calamia JR, Simonsen RJ. Effects of coupling agents on bondstrength of etched porcelain. J Dent Res. 1985;64:296.
Alex
www.compendiumlive.com Compendium 11

20.Della Bona A, Anusavice KJ, Mecholsky JJ Jr. Apparent inter-
facial fracture toughness or resin/ceramic systems. J Dent Res.
2006;85:1037-1041.
21.Ozcan M. Evaluation of alternative intra-oral repair techniques
for fractured ceramic-fused-to-metal restorations. J Oral Re-
habil. 2003;30:194-203.
22.Rosenblum MA, Schulman A. A review of all-ceramic restora-
tions. J Am Dent Assoc. 1997;128:297-307.
23.Westbrook PH. Bonded esthetic onlay. Contemporary Esthetics
and Restorative Practice. Jul/Aug 1999;52-54.
24.Barghi N, Fischer DE, Vatani L. Effects of porcelain leucite con-
tent, types of etchants, and etching time on porcelain-composite
bond. J Esthet Restor Dent. 2006;18:47-52.
25.www.ivoclarvivadent.us.com
26.Tysowsky G. Ivoclar Vivadent. Personal communication. Au-
gust 28, 2007.
27.Mona H, Abou-Daya M. Effect of ceramic surface treatments
on the biaxial flexural strength of heat-pressed glass ceramic.
J Egyptian Dent Assoc. 2000;46:1477.
28.www.jensenindustries.com
29.Jensen C. Jensen Industries. Indirect personal communication
via West B, Frontier Dental Lab.
30.Chevalier S. Jensen Industries. Personal communication.
31.Kim JS, Hwang HS, Jeong CM, et al. A study on the bond
strength of resin cements to Empress 2 ceramic. J Korean Acad
Prost. 2001;39:184-196.
32.Magne P, Magne M. Treatment of extended anterior crown
fractures using Type IIIA bonded porcelain restorations. J Calif
Dent Assoc. 2005;33:387-396.
33.Soares CJ, Soares PV, Pereira JC, et al. Surface treatment pro-
tocols in the cementation process of ceramic and laboratory-
processed composite restorations: a literature review. J Esthet
Restor Dent. 2005;17:224-235.
34.www.bisco.com and www.ultradent.com
35.Suh B. Bisco Dental. Personal communication.
36.Nagayassu PM, Shintome LK, Uemura ES, et al. Effect of sur-
face treatment on the shear bond strength of a resin-based ce-
ment to porcelain. Braz Dent J. 2006;17:290-295.
37.Hochhauser L. American Dental Supply, Allentown Pa. In-
formation supplied.
38.Bailey LF, Bennett RJ. DICOR surface treatments for en-
hanced bonding. J Dent Res. 1988;67:925-931.
39.Addison O, Marquis PM, Fleming GJ. The impact of hydro-
fluoric acid surface treatments on the performance of a porcelain
laminate restorative material. Dent Mater. 2007;23:461-468.
40.Shimada Y, Yamaguchi S, Tagami J. Micro-shear bond strengthof dual-cured resin cement to glass ceramics. Dent Mater. 2002;18:380-388.
41.Roulet JF, Söderholm KJ, Longmate J. Effects of treatment andstorage conditions on ceramic/composite bond strength. J DentRes. 1995;74:381-387.
42.Suh B. Bisco Dental. Unpublished data from contact angleanalysis. 2007.
43.Barghi N. To silanate or not to silanate: making a clinical de-cision. Compend Contin Educ Dent. 2000;21:659-662, 664.
44.Rosen RR. From treating solution to filler surface and beyond—the life history of a silane coupling agent. J Coatings Technology.1978;50:70-82.
45.Matinlinna JP, Lassila LV, Ozcan M, et al. An introduction tosilanes and their clinical applications in dentistry. Int J Pros-thodont. 2004;17:155-164.
46.Culler S. ScotchPrime Ceramic Primer Product Profile. 3MDental Products. 1985. Also personal communication.
47.Anagnostopoulos T, Eliades G, Palaghias G. Composition, re-activity and surface interactions of three dental silane primers.Dent Mater. 1993;9:182-190.
48.Söderholm KJ, Shang SW. Molecular orientation of silane atthe surface of colloidal silica. J Dent Res. 1993;72:1050-1054.
49.Daniels MW, Francis LF. Silane adsorption behavior, micro-structure, and properties of glycidoxypropyltrimethoxysilane-modified colloidal silica coatings. J Colloid Interface Sci. 1998;205:191-200.
50.Liu Q, Ding J, Chambers DE, et al. Filler-coupling agent-matrixinteractions in silica/polymethylmethacrylate composites. J Bio-med Mater Res. 2001;57:384-393.
51.Monticelli F, Toledano M, Osorio R, et al. Effect of temperatureon the silane coupling agents when bonding core resin to quartzfiber posts. Dent Mater. 2006;22:1024-1028.
52.Shih PTK, Koenig JL. Mater Sci Eng. 1975;20:137.53.Wood WE, Johnson DL, Duncanson MG. Variables affecting
silicone-polymethyl methacrylate interfacial bond strengths.J Prosthodont. 1993;2:13-18.
54.Shen C, Oh WS, Williams JR. Effect of post-silanization dry-ing on the bond strength of composite to ceramic. J ProsthetDent. 2004;5:453-458.
55.Papacchini F, Monticelli F, Hasa I, et al. Effect of air-dryingtemperature on the effectiveness of silane primers and couplingblends in the repair of a microhybrid resin composite. J AdhesDent. 2007;9:391-397.
56.Barghi N, Berry T, Chung K. Effects of timing and heat treat-ment of silanated porcelain on the bond strength. J Oral Re-habil. 2000;27:407-412.
Continuing Education 1
12 Compendium July | August 2008—Volume 29, Number 6

57.Kupiec KA, Wuertz KM, Barkmeier WW, et al. Evaluation ofporcelain surface treatments and agents for composite-to-porcelain repair. J Prosthet Dent. 1996; 76:119-124.
58.Hayakawa T, Horie K, Aida M, et al. The influence of surfaceconditions and silane agents on the bond of resin to dental por-celain. Dent Mater. 1992;8:238-240.
59.Spohr AM, Sobrinho LC, Consani S, et al. Influence of sur-face conditions and silane agent on the bond of resin to IPSEmpress 2 ceramic. Int J Prosthodont. 2003;16:277-282.
60.Thurmond JW, Barkmeier WW, Wilwerding TM. Effect ofporcelain surface treatments on bond strengths of compositeresin bonded to porcelain. J Prosthet Dent. 1994;72:355-359.
61.Valandro LF, Della Bona A, Antonio Bottino M, et al. The ef-fect of ceramic surface treatment on bonding to densely sin-tered alumina ceramic. J Prosthet Dent. 2005;93:253-259.
62.Kern M, Thompson VP. Bonding to glass infiltrated aluminaceramic: adhesive methods and their durability. J Prosthet Dent.1995;73:240-249.
63.Ozcan M, Vallittu PK. Effect of surface conditioning meth-ods on the bond strength of luting cements to ceramics. DentMater. 2003;19(8):725-731.
64.www.3mespe.com 65.Bouschlicher MR, Reinhardt JW, Vargas MA. Surface treat-
ment techniques for resin composite repair. Am J Dent. 1997;10:279-283.
66.Tezvergil A, Lassila LV, Yli-Urpo A, et al. Repair bond strengthof restorative resin composite applied to fiber-reinforced com-posite substrate. Acta Odontol Scand. 2004;62:51-60.
67.dos Santos JG, Fonseca RG, Adabo GL, et al. Shear bondstrength of metal-ceramic repair systems. J Prosthet Dent. 2006;96:165-173.
68.Frankenberger R, Krämer N, Sindel J. Repair strength of etchedvs silica-coated metal-ceramic and all-ceramic restorations. OperDent. 2000;25:209-215.
69.Cobb DS, Vargas MA, Fridrich TA, et al. Metal surface treat-ment: characterization and effect on composite-to-metal bondstrength. Oper Dent. 2000;25:427-433.
70.Zhang Y, Lawn BR, Rekow ED, et al. Effect of sandblastingon the long-term performance of dental ceramics. J BiomedMater Res B Appl Biomater. 2004;71:381-386.
71.Schulze KA, Marshall SJ, Gansky SA, et al. Color stability andhardness in dental composites after accelerated aging. DentMater. 2003;19:612-619.
72.Nathanson D, Banasr F. Color stability of resin cements—anin vitro study. Pract Proced Aesthet Dent. 2002;14:449-455.
73.Lu H, Powers JM. Color stability of resin cements after accel-erated aging. Am J Dent. 2004;17:354-358.
Alex
www.compendiumlive.com Compendium 13

www.compendiumlive.com Compendium 14
Continuing Education Quiz 1
This article provides 1 hour of CE credit from Ascend Dental Media, now operated by AEGIS Communications. Record youranswers on the enclosed answer sheet or submit them on a separate sheet of paper. You may also phone your answers in to(888) 596-4605 or fax them to (703) 404-1801. Be sure to include your name, address, telephone number, and last 4 digits ofyour Social Security number.
Please see tester form on page xxx.
1. Hydrofluoric acid (HF) is:a. a strong organic acid.b. a relatively weak organic acid.c. a strong inorganic acid.d. a relatively weak inorganic acid.
2. Because of its low dissociation potential, HF:a. has the ability to readily penetrate skin tissues.b. can cause extensive internal tissue damage.c. has caused death from accidental skin exposure.d. all of the above
3. Acidulated phosphate fluoride gel (APF) has been shown:a. to have the ability to etch porcelain.b. to require considerably shorter application
times than HF etching.c. to result in a rougher-appearing surface than
HF etching.d. all of the above
4. All feldspathic based porcelains contain:a. silica dioxide (SiO2).b. aluminum oxide (AL2O3).c. potassium oxide (K2O).d. all of the above
5. The manufacturer of the pressable ceramic IPSEmpress recommends an etching protocol using:
a. 5% HF for 60 seconds.b. 5% HF for 2 minutes.c. 9% HF for 60 seconds.d. 9% HF for 2 minutes.
6. Some opinion leaders/studies recommend an etchingprotocol for powder/liquid or “stackable” porcelains of:
a. 4 minutes with 10% HF or 5 minutes with9.5% HF.
b. 2 minutes with 10% HF or 2.5 minutes with9.5% HF.
c. 90 seconds with 10% HF or 120 to 150 sec-onds with 9.5% HF.
d. 60 seconds with 10% HF or 90 to 120 sec-onds with 9.5% HF.
7. To remove the white “residue” from an etched porcelainsurface, the author has found what protocol usually, butnot always, effective?
a. rinsing the etched restoration with water followed by a vigorous air spray
b. placing the etched restoration in an ethanolsolution followed by ultrasonication for 5 minutes
c. scrubbing the etched restoration with alcoholfollowed by air drying
d. all of the above
8. Silanes are:a. a class of organic molecules that contain one
or more silicon atoms.b. potentially useful as chemical couplers linking
organics to inorganics.c. able to interact chemically with porcelain sur-
faces only if they are hydrolyzed before use.d. all of the above
9. The terminal hydroxyl groups on each silane molecule interact with the opposing hydroxyl groupson the surface of feldspathic porcelain through:
a. hydrogen bonding.b. anionic addition polymerization.c. formation of ionic bonds.d. formation of aromatic bonds.
10. One method that has been shown to be quite effec-tive in increasing bond strength to high-content alu-mina and zirconia core-based ceramics is:
a. etching with 9% to 10% HF.b. silica coating followed by silane application.c. ultrasonic brushing.d. applying 1.23% APF.