universal health coverage models from developing countries by dr snehal moderator dr subodh s gupta
TRANSCRIPT

Universal Health CoverageModels from developing countries
By Dr SnehalModerator Dr Subodh S Gupta

Frame work• What is Universal Health Coverage?• Historical Perspective• Need of UHC• Dimensions of UHC• Principles of UHC• Indian Scenario• India’s path to UHC• High level Expert Group India (HLEG Report 2011)• Models of UHC from developing countries Sri Lanka Thailand Turkey Brazil• Challenges for these countries

Universal Health Coverage:
“Ensuring that all people have access to needed Promotive, preventive, curative and rehabilitative health services, of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user to financial hardship”.
World Health Organization
“Ensuring equitable access for all Indian citizens, resident in any part of the country, regardless of income level, social status, gender, caste or religion, to affordable, accountable, appropriate health services of assured quality ( Promotive, preventive, curative and rehabilitative) as well as public health services addressing the wider determinants of health delivered to individuals and populations, with the government being the guarantor and enabler, although not necessarily the only provider, of health and related services”. HLEG on UHC, Planning Commission

Historical Perspectives
1883 Health Insurance Bill, Germany became the first country to make nationwide health insurance mandatory.
1948 In U. K. Enactment of the National Insurance Act in 1911 and the National Health Service (NHS)
1948 ; Article 25.1 of the Universal Declaration of Human Rights states right to health as an important fundamental right.
1966, The International Convention on Economic, Social and Cultural Rights recognized "the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.
1978: Alma-Ata declaration & the vision of "health for all” 2005 World Health Assembly resolution 58.33 adopted 'Universal
Health Coverage' 201 1 :High Level Expert Group Committee Report India

Need of Universal Health Coverage
Promoting and protecting health is essential to human welfare
and sustained economic and social development.
Many ways to promote and sustain health : Education, housing,
food and Employment.
Redressing inequalities
Timely access to health services
Well-functioning health financing system
Use of health services when people need them.

Principles of UHC• Universality• Equity• Empowerment• Comprehensiveness of care• Non-exclusion and non-discrimination• Financial Protection• Quality and rationality of care• Protection of patients’ rights, appropriate care, patient choice• Portability and continuity of care• Pivotal role of public financing, substantial contribution of tax based
funds, single payer System• Consolidated and strengthened public health provisioning as a key
component of UHC• Accountability, transparency and participation

Three Dimensions of Universal Health Coverage:

Expected Outcomes From UHC…

India’s path to UHC…..• India’s economic growth is much more rapid than that
in any other country.• India’s greatest demographic asset is its young people .• The ability of these individuals to fully participate in
the country’s future is seriously undermined by the inability of the health-care system to address their needs.
• Global experience shows that universal health care is affordable and feasible; when there is
a. Sustained public finance b. Strong leadership c. Improved health.
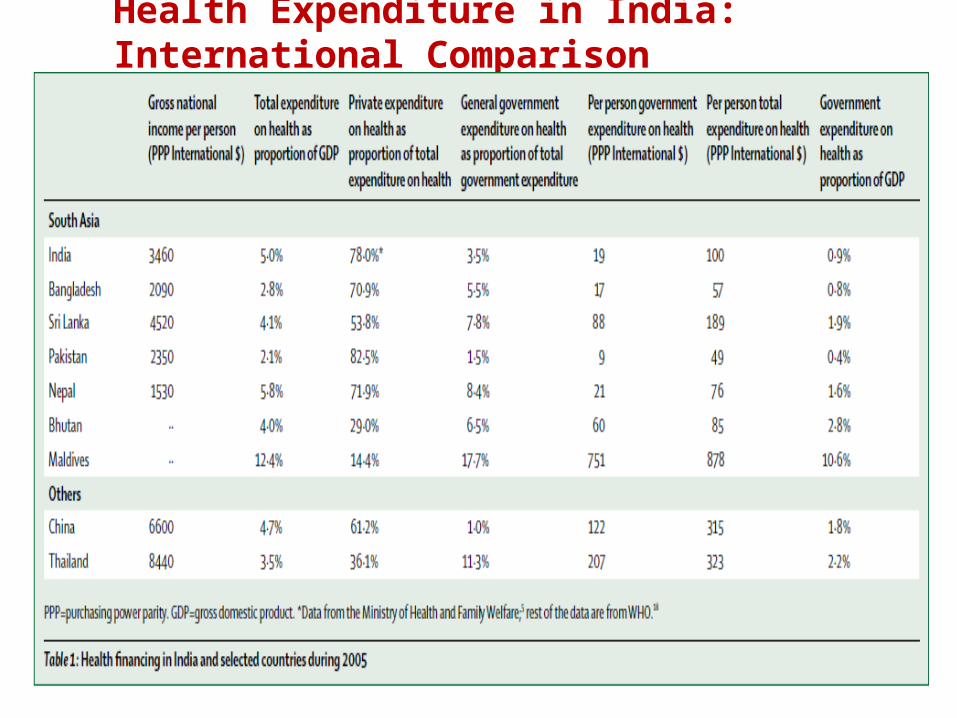
Health Expenditure in India: International Comparison

Where we are?

High Level Expert Group Report India
• CONSTITUTED IN OCTOBER 2010• REPORT IN NOVEMBER 2011

WHY IS HEALTH SYSTEM REFORM NEEDED?• 18% of all episodes in rural areas and 10% in urban areas received
no health care at all• 12% of people living in rural areas and 1% in urban areas had no
access to a health facility• 28% of rural residents and 20% of urban residents had no funds for
health care• Over 40% of hospitalised persons had to borrow money or sell
assets to pay for their care• Over 35% of hospitalised persons fell below the poverty line
because of hospital expenses• Over 2.2% of the population may be impoverished because of
hospital expenses• The majority of the citizens who did not access the health system
were from the lowest income quintiles

Recommendation OF HLEG
• Government (Central government and states combined) should increase public expenditures on health from the current level of 1.2% of GDP to at least 2.5% by the end of 12th plan (2012-17) and to at least 3% of GDP by 2022
• Use general taxation as the principal source of health care financing
• Eliminate user fees for essential health services• Avoid insurance schemes, as they fragment health care, do
not provide full coverage of needed services and fail to cover the whole population.
• Expenditures on primary health care, should account for at least 70% of all health care expenditures
• Ensure availability of free essential medicines by increasing public spending on drug procurement

Universal Health Coverage By 2022:The vision

Schemes to promote universal health coverage in India
• NRHM• Janani Suraksha Yojana• The Rashtriya Swasthya Bima Yojna• Chiranjeevi Yojana in Gujarat• The Jan Aushadhi programme
Source: Towards achievement of universal health care in Indiaby 2020: a call to action ; Lancet 2011; 377: 760–68

NRHM• Main focus on Maternal & Child Health• Accredited Social Health Activists (ASHAs)• Conditional cash transfers (institutional deliveries)• Infrastructure strengthening (Primary Health
Centers)• Increased fund flow to States (flexible funding• mechanisms)• Decentralized planning• Proposed platform for operational integration of
multiple national health programs

Janani Suraksha Yojana
• The Janani Suraksha Yojana launched in 2005 encourages women to deliver in government health facilities or accredited private facilities by providing fi nancial incentives.
• This conditional cash transfer scheme has the largest number of beneficiaries for any such programme in the world, estimated to be 9·5 million women giving birth in 2010.
• This scheme is complemented by a public-partnership programme, initially started as the Chiranjeevi Yojana in Gujarat and now being tested in other states in which private obstetricians are paid to assist women who are poor with their deliveries.
• Another complementary programme is the Muthulakshmi Scheme in Tamil Nadu that provides fi nancial support before and after the delivery period.
• Assessments of Janani Suraksha Yojana and Chiranjeevi Yojana have suggested benefi cial outcomes and ideas for improvements.

Rashtriya Swasthya Bima Yojna scheme
• The Rashtriya Swasthya Bima Yojna scheme was launched in 2007 by the Ministry of Labour and Employment to provide insurance coverage for treatment in hospital to families below the poverty line.
• Each eligible family is given a smart card that allows the members coverage up to a limit at either public or private hospitals at a nominal yearly fee that is paid by the beneficiary.
• 75% of the yearly insurance premium is contributed by the central government and 25% by the state governments.
• The scheme includes cashless care in hospital, coverage of pre-existing diseases, and transportation costs.

Jan Aushadhi Programme
• The Jan Aushadhi programme is a public-private partnership, which aims to set up pharmacies in every district to provide quality generic drugs and surgical products at affordable prices 24 h a day.
• The first store opened under this programme was started in late 2008, and 44 stores were functioning throughout India by March, 2010.
• This programme, involving several stakeholders, has great promise because it aims to provide quality generic drugs at very low cost to individuals who might otherwise not be able to afford them

Aspects of health system affecting coverage

Models of UHC From developing countries…
Sri Lanka
Brazil
Thailand

SRI LANKA

Sri LankaHealth Financing Health ServicesBy relying on tax-financed and government-operated health services, Sri Lanka achieved universal health coverage
In 2005, total expenditure on health in Sri Lanka accounted for 4.2 % of GDP and neared Rs. 100 billion (US$1 billion).
OPD,IPD services are free. All citizens live within one or two kilometers of a clinic.Emphasis on Primary Health CareSri Lanka’s system encourages richer patients to choose private care, which opens up facilities for the poor and reduces the burden on the government.All public hospitals are able to accept all patients without restriction, and no referral system is enforced.most private doctors are typically government medical employees who are permitted to practice privately during their free time.health system bulk-purchases only generic medicines.strong health infrastructure in rural areas, which has encouraged usage of health services by the poor.

BRAZIL

BrazilHealth Financing Health Services
Brazil integrated its multiple programs into a single publicly funded Unified Health System (SUS) covering the whole population, financed through general taxation.
A subsidized health care system is available to all citizens, but some implicit targeting occurs as wealthier individuals choose additional private coverage.
They have attained significant coverage expansion through a strong emphasis on primary health care, redistribution of resources to reduce inequities in coverage,and efforts to recruit and retain health workers in underserved communities.
The Unified Health System emphasizes primary care
Provides free primary health care
Basic dental care
A range of hospital services including diagnostics and surgeries through a network of public and private providers
Financial protection against costly drugs
Negotiate low drug prices with pharmaceutical companies.

THAILAND

ThailandHealth Financing Health ServicesIncreased payroll taxes and their allocation thruogh general revenues.The UCS works alongside two other public health insurance programs The Compulsory Social Security Scheme (SSS), created for government employees and dependents and covers 13% of the populationThe Civil Servant Medical Benefit Scheme (CSMBS), which serves private employees and temporary public employees and covers 8% of the population.All together, the UCS, SSS and CSMBS represent a strong government-run health insurance system that covers nearly 100% of Thailand’s population.
Marked shift towards primary careCompletely free IPD servicesA comprehensive package of curative and preventive care Universal access to antiretroviral drugs.Public health advocates are present in the senior levels of Thailand’s bureaucracyTough negotiations with pharmaceutical companies Priority setting for expanding the benefits package Redistribution of resources to reduce inequities in coverage,and Efforts to recruit and retain health workers in underserved communities.

Challenges for Countries achieved UHC• Managing expenditures to meet the growing demand from the
population for more comprehensive coverage and higher quality care
• They face accelerating cost pressures.
• The consequences of aging populations with a higher burden of chronic diseases regulating the role of the private sector in UHC.
• Pressure on their government budgets.
• Shortage of doctors to staff primary care units
• The main challenge for the provision of health care services in Sri Lanka relates to the government’s ability to continue to provide health services free at the point of delivery.

Refferrences
• Gina Lagomarsino, Alice Garabrant, Atikah Adyas, Richard Muga, Nathaniel Otoo ;Moving towards universal health coverage: health insurance reforms in nine developing countries in Africa and Asia; Lancet 2012; 380: 933–43;
• High Level Expert Group Report on Universal Health Coverage for India;Instituted by Planning Commission of India; New Delhi,November, 2011
• K Srinath Reddy, Vikram Patel, Prabhat Jha, Vinod K Paul, A K Shiva Kumar, Lalit Dandona, for The Lancet India Group for Universal Healthcare; Towards achievement of universal health care in India by 2020: a call to action; Lancet 2011; 377: 760–68
• Universal Health Coverage for Inclusive and Sustainable Development http://dx.doi.org/10.1596/978-1-4648-0297-3• Tracking universal health coverage: first global monitoring report; World Health
Organization 2015