university-based design of developing world healthcare technologies: what’s wrong, what’s...
DESCRIPTION
Robert Malkin’s Developing World Healthcare Technology Laboratory at Duke. University-Based Design of Developing World Healthcare Technologies: What’s Wrong, What’s Right, What’s Next?. Robert Malkin, PhD, PE Professor of the Practice, Biomedical Engineering Director, DHT-Lab - PowerPoint PPT PresentationTRANSCRIPT

University-Based Design of Developing World Healthcare Technologies:
What’s Wrong, What’s Right, What’s Next?
Robert Malkin, PhD, PEProfessor of the Practice, Biomedical Engineering
Director, DHT-LabDirector, Duke-EWH Summer Institute
Director, Global Public Service Academies
Robert Malkin’sDeveloping World Healthcare Technology Laboratoryat Duke

• What is Global Health?• Developing World
– Medical Equipment Landscape– Why Equipment Doesn’t Work
• University-based Design– What’s Right– What’s Wrong– What’s Next
Robert Malkin’sDeveloping World Healthcare Technology Laboratoryat Duke
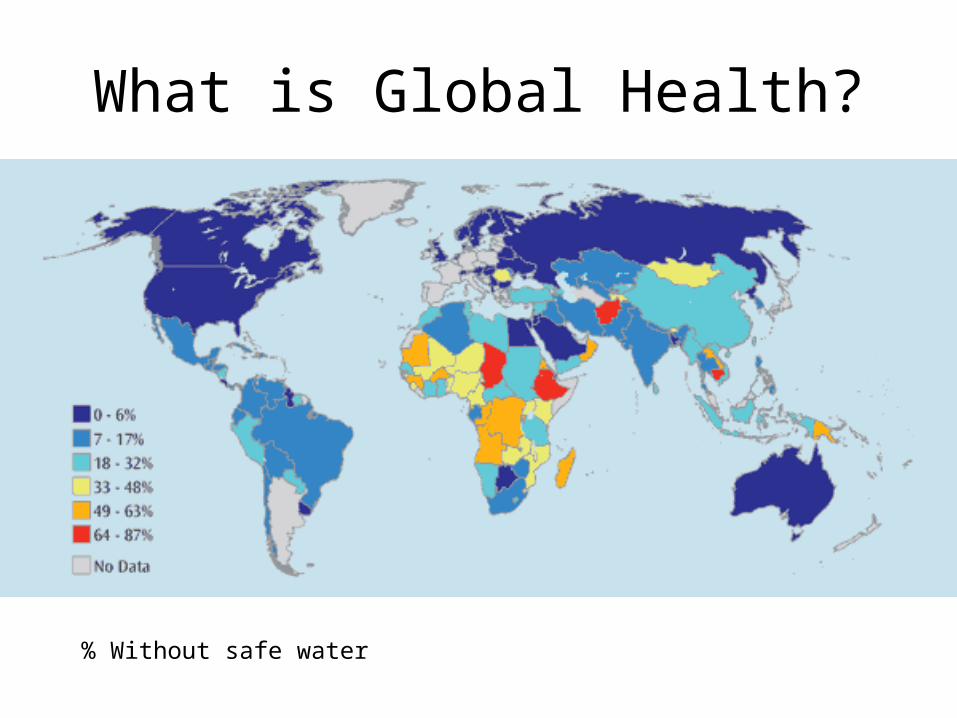
% Without safe water
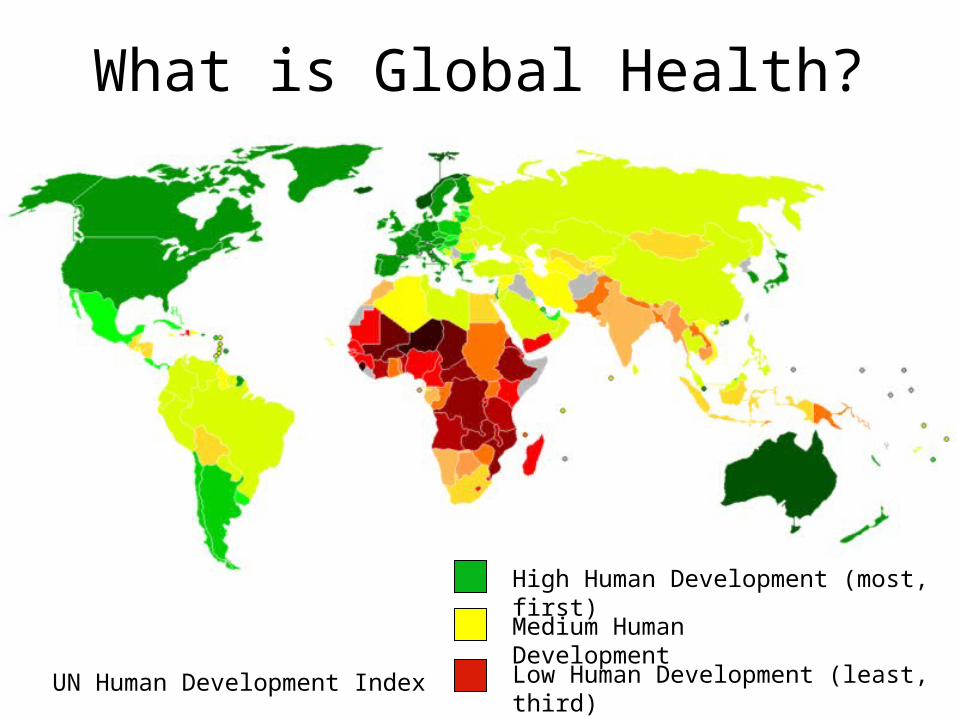
What is Global Health?
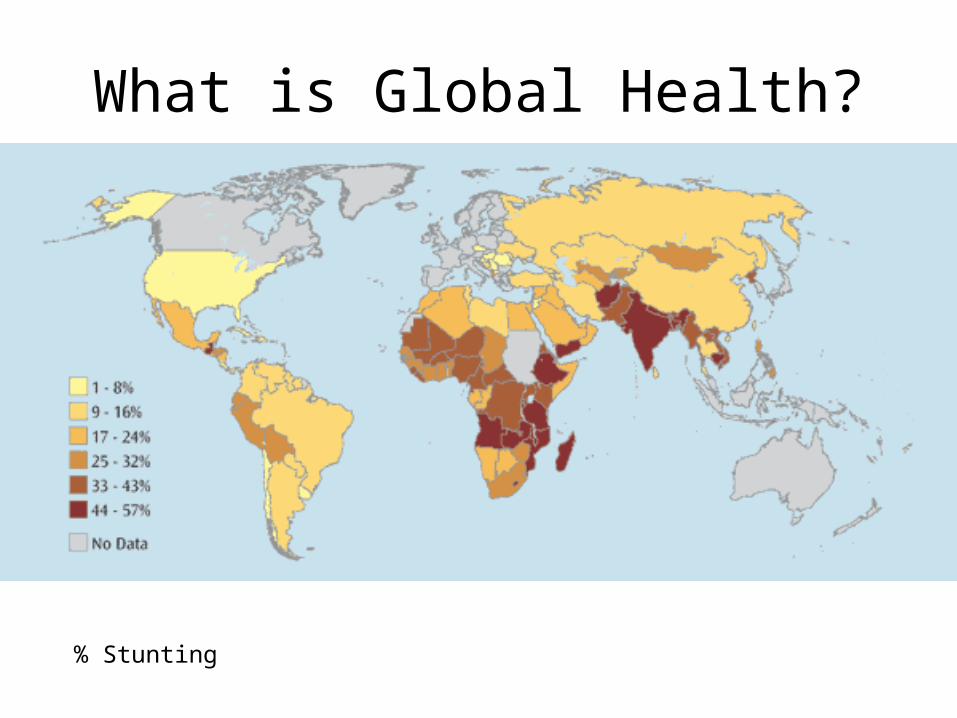
What is Global Health?
% Stunting
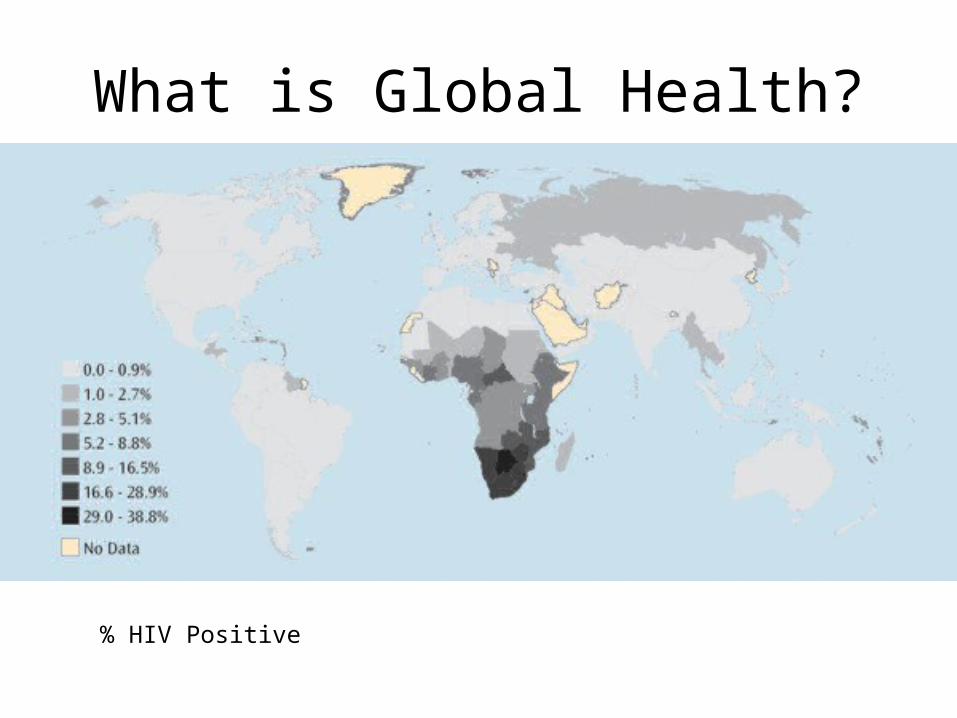
What is Global Health?
% HIV Positive
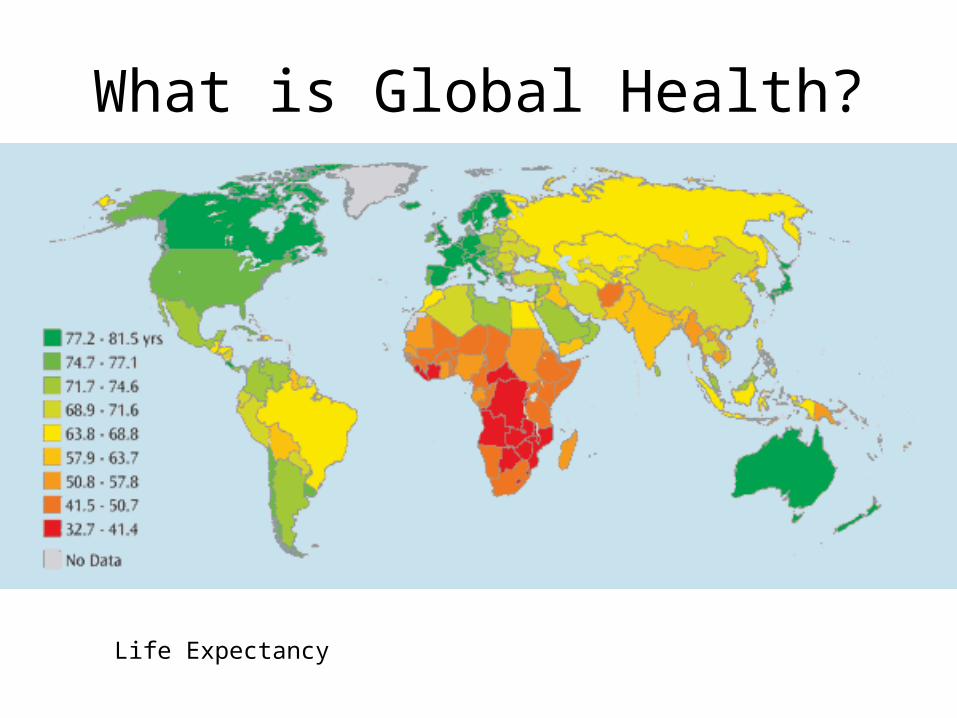
What is Global Health?
Life Expectancy
What is Global Health?
UN Human Development Index Low Human Development (least, third)
High Human Development (most, first)
Medium Human Development
Why should you care?
US$60 billion
Buffet and Gates have put in …
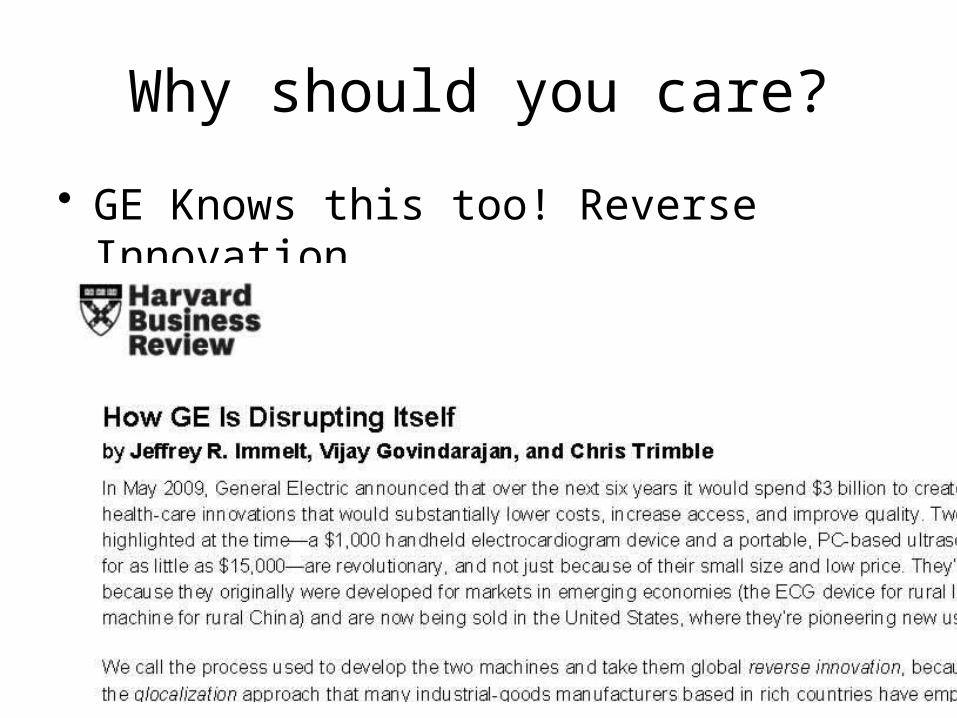
Why should you care?
• GE Knows this too! Reverse Innovation
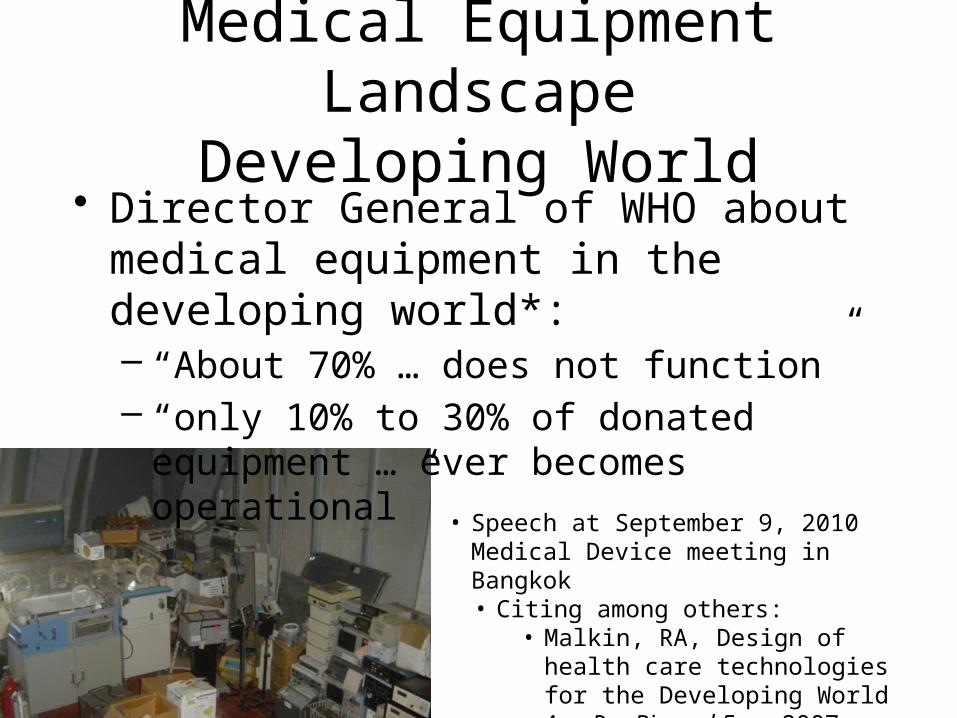
Medical Equipment LandscapeDeveloping World
• Director General of WHO about medical equipment in the developing world*:– “About 70% … does not function” – “only 10% to 30% of donated equipment …
ever becomes operational”
• Speech at September 9, 2010 Medical Device meeting in Bangkok• Citing among others:
• Malkin, RA, Design of health care technologies for the Developing World Ann Rev Biomed Eng, 2007
Medical Equipment LandscapeDeveloping World
• 112,000 pieces, 16 developing countries [1]– 38.3% (42,925 pieces) out of service
• Range: 1% (Costa Rica) to 47% (Venezuela)• Highest: X-ray (48%) and Sterilizers (43%)
– 95.8% imported• Wheelchairs, lighting devices locally produced
[1] Perry, L, Malkin, RA, How much equipment is broken?, accepted and in print MBEC
Why Current Equipment Doesn’t Work
• Most common hypotheses are:– Capital Cost (one-time cost)– Infrastructure
• electricity, water …– Spare Parts (cost and availability)– Too complicated
• training– Consumables (recurring cost)
Why It Doesn’t Work• Capital Cost – No evidence [1]
– Interviewed 54 hospitals, 16 Countries• Most common complaint: TOO MUCH equipment
– Large pieces with govt investment• Significant donation stream [2]
• 90% donate expired supplies• 60% admit donating broken equipment• 8% donate through non-BME MSRO
[1] Malkin, RA, Design of health care technologies for the Developing World Ann Rev, 2007[2] CHA Medical Surplus Donation Study, April 2011
Why It Doesn’t Work• Infrastructure – Limited [1]
– Electricity limited– Gasses– Not water
[1] Malkin, RA, Design of health care technologies for the Developing World Ann Rev, 2007
Why It Doesn’t Work• Spare Parts – Partial Evidence [1], [2]
– Retrospective • 2849 Work Tickets [1]• 11 countries, 60 hospitals
– 66% without importing spare parts, <$50– Prospective
• 106 work tickets Rwanda [2]– 68.9% without importing spare parts, <$50
• Too complicated – No Evidence [1]– 25% Training, >400 documented– No training failures
[1] Malkin, Keane, Evidence-based approach to the maintenance of laboratory and medical equipment in resource-poor settings MBEC, 2010 v48, 721-726[2] Finley, Malkin, BMET in Rwanda, Internal DHTLab Report, 2011
Why It Doesn’t Work• Consumables- YES – sort of
– 42,925 out of services pieces [1]• Top three non-personnel reasons
– Consumables, accessories, spare parts
– Interview in 54 hospitals in 16 hospitals [2]• 133 interviews (50% MD: rest nurse, staff, BMET)• 0 cited consumables
[1] Perry, Malkin, MBEC 2011[2] Malkin, Annals of BME, 2007
Why Medical Equipment in the Developing World Doesn’t Work
• Design Constraints:– Spare Parts – Partial: 30-35% – Too complicated – No evidence
• Caveat: Training ~= task shifting– Infrastructure (Electricity, gas …)
– Capital Cost – No evidence– Consumables – YES – sort of
• Caveat: Iceburg
NurseMD
PA
CHW
University-Based Design
• What’s Right?• What’s Wrong?• What’s Next?

What’s Right?
• Students are Getting Involved• Product is Reaching Patients
University-Based BME Trips
• UPenn Global Biomedical Service Program• U Penn International Development Summer Institute • Rice Beyond Traditional Borders • Vanderbilt VISAGE• Northwestern Global Engagement Summer Institute• Duke EWH Summer Institute• U Michigan Global Course Connections• U Michigan Global Intercultural Experience for Undergraduates
> 100 US students per year traveling to resource poor settings focusing on medical equipment

Engineering World HealthSummer Institute
~50 Participants in 2012
1 Month Training in Costa Rica/Tanzania
1 Month in a poor HospitalNicaragua, Honduras, Tanzania
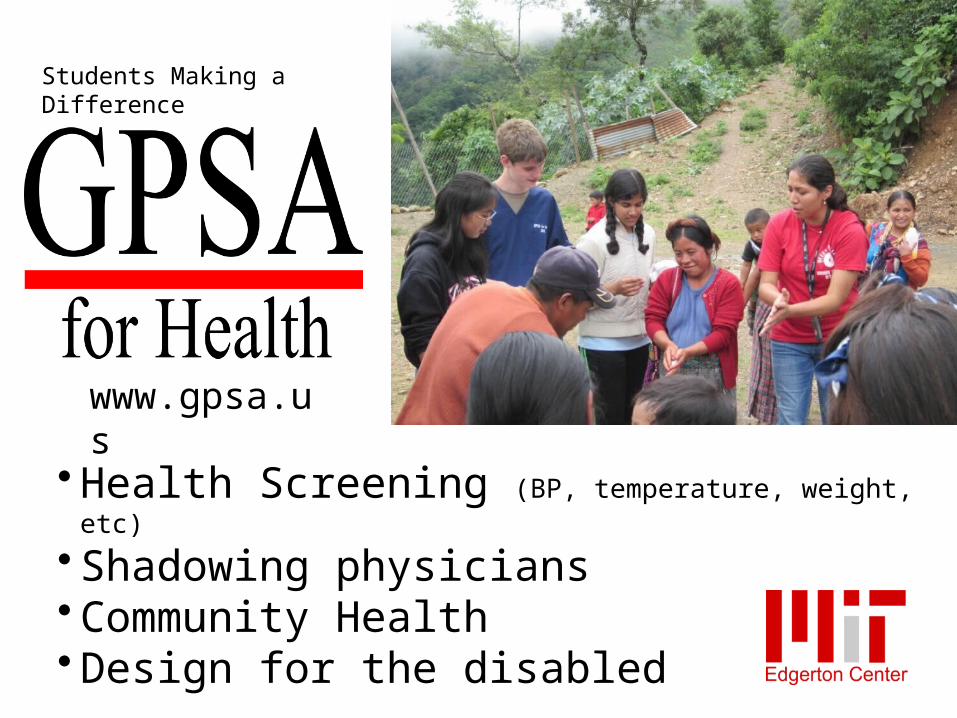
Students Making a Difference
• Health Screening (BP, temperature, weight, etc)
• Shadowing physicians• Community Health• Design for the disabled
www.gpsa.us
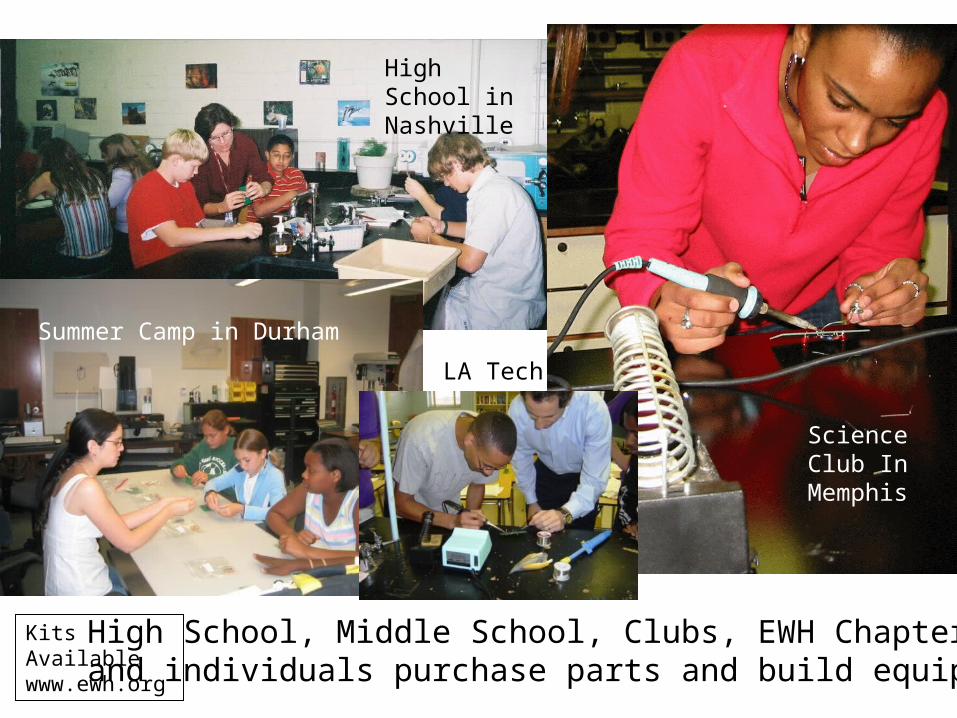
High School, Middle School, Clubs, EWH Chaptersand individuals purchase parts and build equipment
High School in Nashville
Science Club In Memphis
Summer Camp in Durham
LA Tech
Kits Availablewww.ewh.org

Sudan
Nicaragua
• ESU, ECG, Defib Tester• O2 Tester, ECG pads• >$1 Million (replacement value)
El Salvador
PhilippinesTanzania
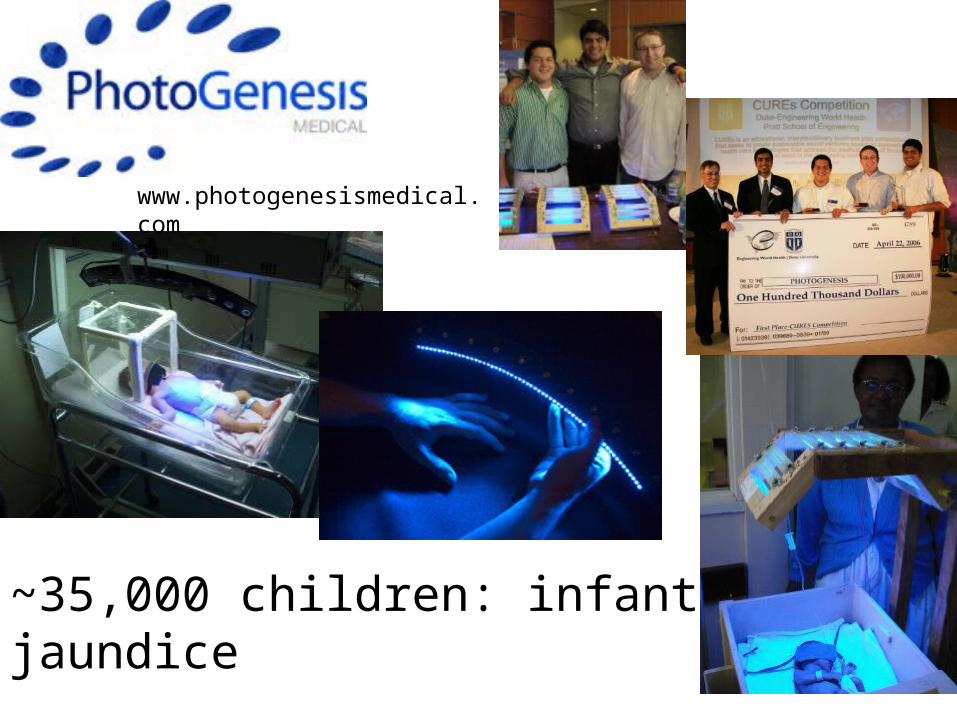
~35,000 children: infant jaundice
www.photogenesismedical.com
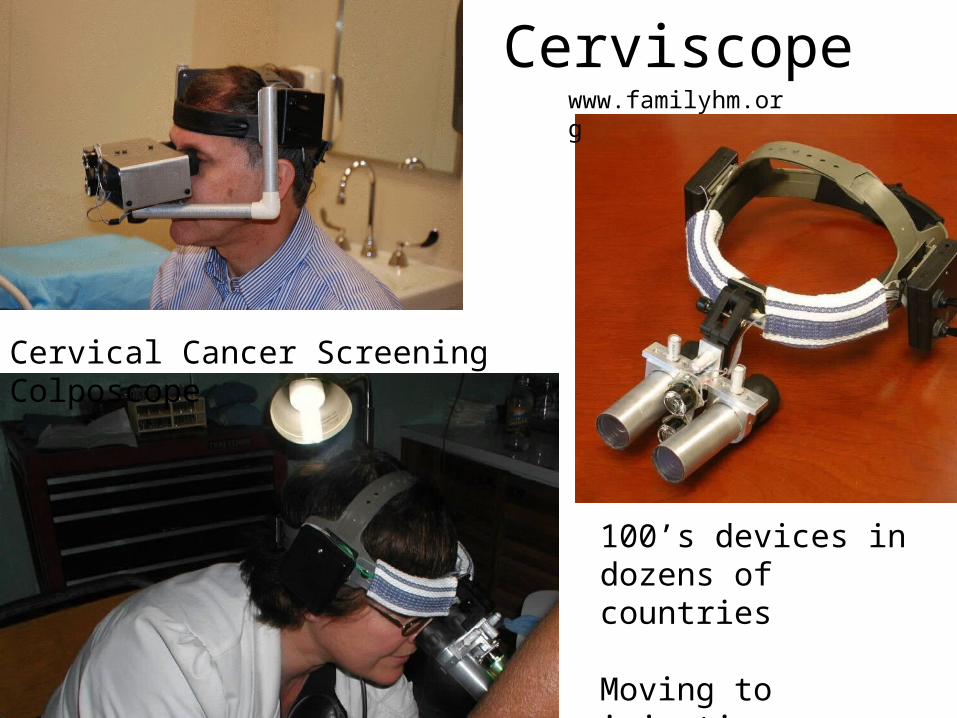
Cerviscope
Cervical Cancer Screening Colposcope
100’s devices in dozens of countries
Moving to injection molding in 2012
www.familyhm.org
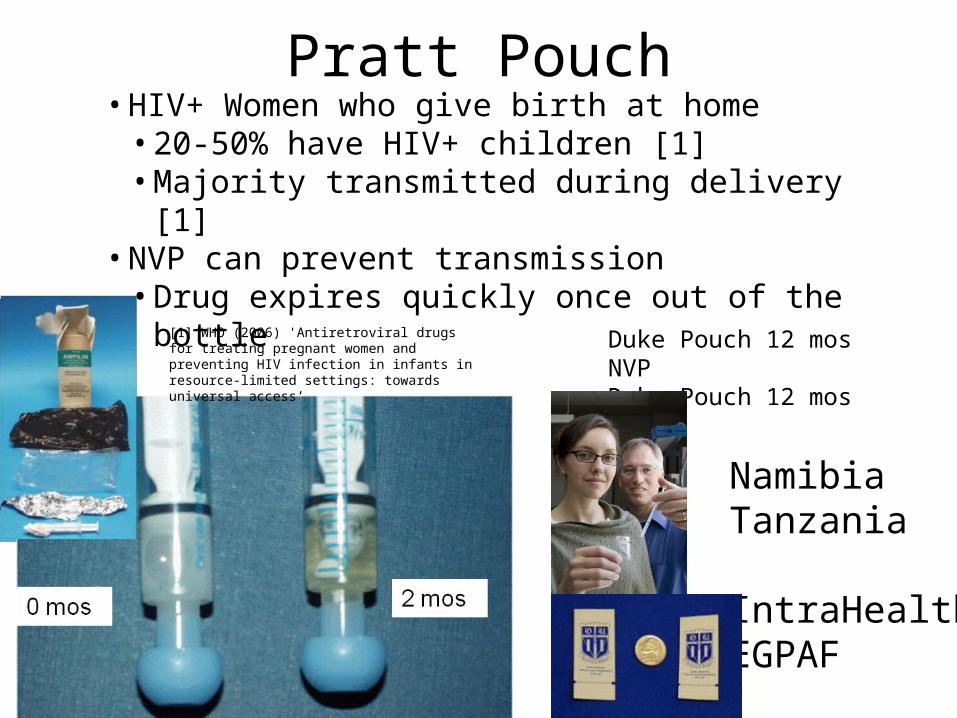
Pratt Pouch• HIV+ Women who give birth at home
• 20-50% have HIV+ children [1]• Majority transmitted during delivery [1]
• NVP can prevent transmission• Drug expires quickly once out of the bottle
2 mos0 mos
Duke Pouch 12 mos NVPDuke Pouch 12 mos AZT
NamibiaTanzania
IntraHealthEGPAF
[1] WHO (2006) 'Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants in resource-limited settings: towards universal access’

What’s Wrong?
• Product Success Rate is Terrible!– But why?
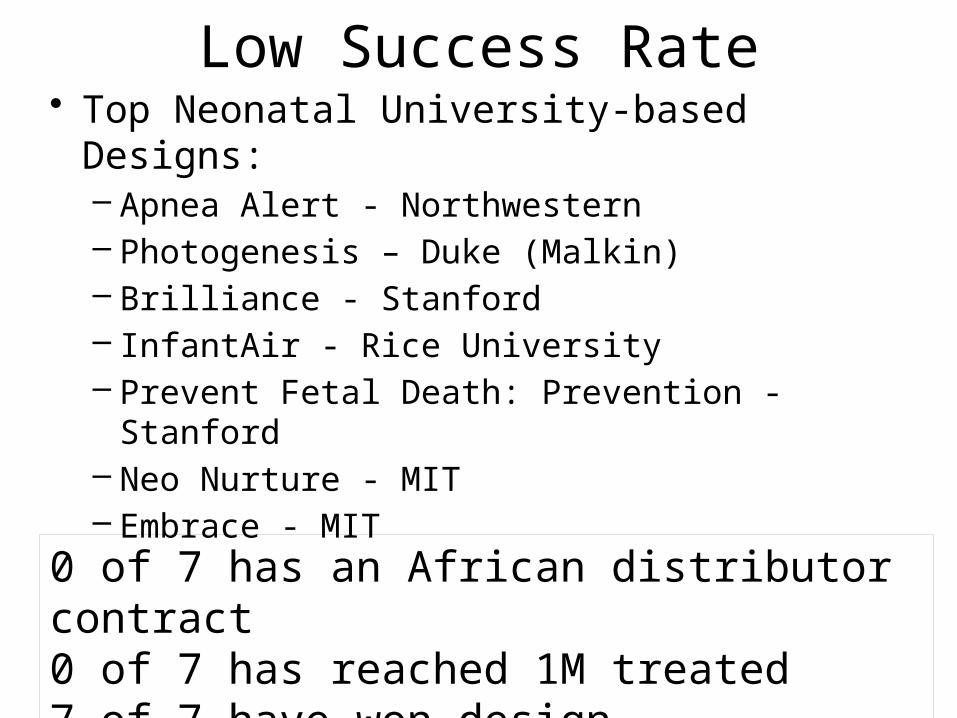
Low Success Rate• Top Neonatal University-based Designs:
– Apnea Alert - Northwestern– Photogenesis – Duke (Malkin)– Brilliance - Stanford– InfantAir - Rice University– Prevent Fetal Death: Prevention - Stanford– Neo Nurture - MIT– Embrace - MIT
0 of 7 has an African distributor contract0 of 7 has reached 1M treated7 of 7 have won design competitions
Success Rate Comparison
• My Industrial Experience– Cordis (now St. Jude Medical) – 2 for 2– Sarns (now 3M Sarns) – 1 for 1– EM Microelectronics – 1 for 5 (I quit)
• University-based design– US Universities charge $:
• some achieve >90% deliver– BME – interviewed some colleagues
• Some achieve >30% deliver
But Why?A Few Untested Hypotheses
• Rapidly Changing Field• Design Approach Wrong
– Consensus– NGO Donation– Low Feature
• Manufacturing Missing– Capital/Process– Distributors missing
Rapidly Changing Field• Avg manufacturing cycle is 18 months [1]
– Very small manufacturing runs (~1000’s)• Huge innovation volume
– FDA approved• 260 medical devices/month (510k, 1/2011)
• 72 new drugs/year (2009)
• Life Expectancy of Medical Device – 5-8 years in US hospital [2]
• Note: much longer in developing world
[1] AdvaMed, Raalph Ives, WHO Second Meeting of Technical Advisory Group on Healthcare Technology, Rio de Janeiro, 2009[2] Veteran’s Administration, Rob Campbell, BME at VAMC Ashville
Design Approach: Consensus• 2003 WHO convenes BP committee
– specify NIBP for resource poor settings• 2005 WHO committee releases specifications• 5 manufacturers entered discussions• 3 manufacturers submitted a device• 1 Manufacturer met specs
– Omron HEM-SOLAR• only for systolic (not diastolic)
• Dec 2010, first published data– Manufacturer will sell at a loss for 25 Euros each
But, uniject …
Design Approach: NGO/Donation
Donating imported medical equipment– Design to be donated via NGO
• Solves a non-problem – capital (buy-in)• Donation moves country backwards
• Donate bed nets [1]– Local bed net manufacturer out of business
• Donate scales, beds and lighting devices [2]– Top three locally manufactured devices– Large fraction of some donor/university portfolios
[1] Dambisa Moyo: Dead Aid[2] Perry, Malkin, MBEC 2011
Design Approach: Low Features
Lower cost by removing features• Solves a non-problem – capital (buy-in)• Customer Acceptance low
– Most trained in US/UK– Double Standard - Rotavirus vaccine [1]
• Rotashield and intussusception
[1] Bines: 2006 Vaccine, e.g., Weijer, BMJ, 2000
Manufacturing Missing• Survey Data from 8 companies (visited 3)
– Cameroon (incubators)– Cameroon (sterile fluids)– Namibia (sterile fluids, distributor)– Nigeria (distributor)– Cote D’Ivoire (beds, exam and OR tables)– Tanzania (wheelchairs)– Tanzania (tables, lamps, wheelchairs)– Tanzania (tables, lamps, wheelchairs)
Product line, challenges, processes
Manufacturing Missing• No Capital to Expand Production
– NO LACK of entrepreneurship– No African manufacturer reported access
• Even to small amounts of capital– Three request for powder coat painting capital– TZ: Jafry, Palray: No stick welding
» but >80% of line is welded
Opportunity: Design for low production capital

What’s Next?
What’s Next?• Capacity Building• Manufacturing Partnerships
El Progresso, Honduras
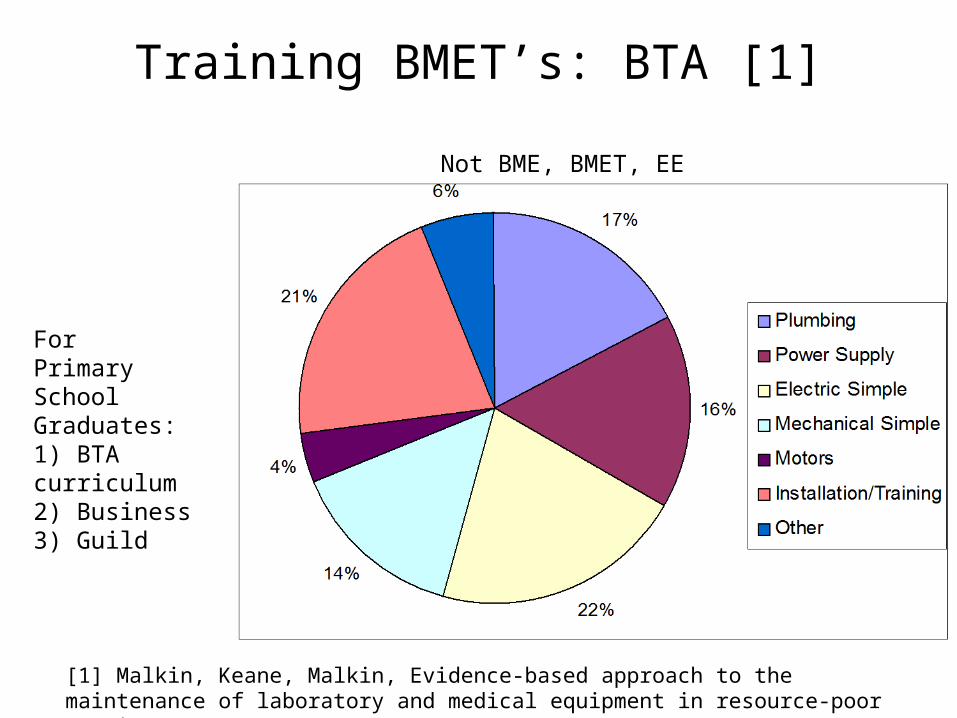
Training BMET’s: BTA [1]
For Primary School Graduates:1) BTA curriculum2) Business3) Guild
Not BME, BMET, EE etc.
[1] Malkin, Keane, Malkin, Evidence-based approach to the maintenance of laboratory and medical equipment in resource-poor settings MBEC, 2010 v48, 721-726
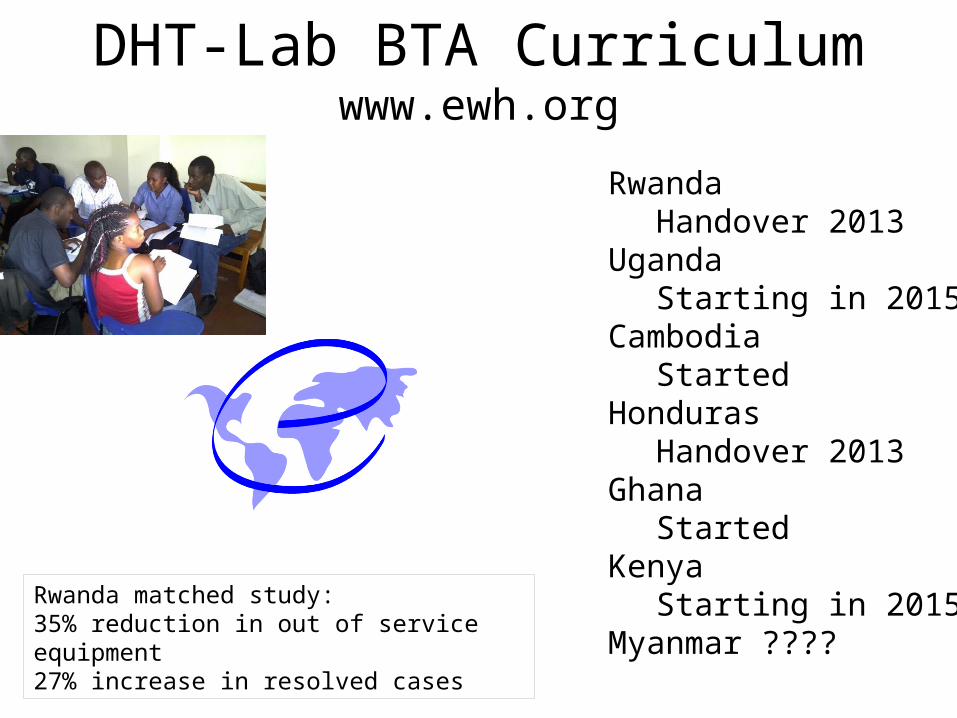
DHT-Lab BTA Curriculumwww.ewh.org
RwandaHandover 2013
UgandaStarting in 2015?
CambodiaStarted
HondurasHandover 2013
Ghana Started
KenyaStarting in 2015?
Myanmar ????Rwanda matched study:35% reduction in out of service equipment27% increase in resolved cases

Manufacturing Partnerships• Historical role
– University of Michigan/Car– Incremental improvements
• STTR/SBIR funding model• Current products redesigned for
– Low production capital– Low training– Low consumables– Low infrastructure– Local spare parts
• Mirror Manufacturing– Mirror a local med device manufacturer
Personnel at DHT-Lab• 5 full-time staff
– Pegeen Ryan Murry, Robert Malkin– Alex Dahinten, Dane Emmerling
• >5 part-time staff– Joy, Chelsea, Jessie, Judy
• 2 summer faculty (2013)– Alex, Daria and many, many more
• DHT-Lab Fellows +: – Caroline, Alexa, Bianca– Fuqua students?
Thank you
dhtlab.pratt.duke.eduwww.ewh.orgwww.gpsa.org
Robert Malkin’sDeveloping World Healthcare Technology Laboratoryat Duke