update on 2022 outpatient pps and physician fee schedule
TRANSCRIPT

8/25/2021
1
Update on 2022 Outpatient PPS and Physician Fee Schedule Proposed Rules
August 26, 2021
Welcome
Jaime Welcher
Education Program Manager
California Hospital Association
1
2
8/25/2021
2
Questions
CALIFORNIA HOSPITAL ASSOCIATION 3
There will be time at the end to address questions.
Please submit them throughout the presentation in the Q & A box usually found at the bottom of your Zoom screen.
Welcome! Today’s Speakers
4
Chad MulvanyVice President, Federal Policy
Chad Mulvany is responsible for providing leadership on federal hospital reimbursement issues and contributes on other federal regulatory matters. Based in CHA’s Washington, DC Office, Chad collaborates with CHA’s vice president, federal policy, CHA’s senior vice president, federal relations, CHA issue managers and national hospital associations on analysis and policy development for advocacy purposes.
3
4
8/25/2021
3
Welcome! Today’s Speakers
5
Megan HowardVice President, Federal Policy
As Vice President, Federal Policy for CHA, Megan Howard is responsible for providing leadership on federal regulatory issues related to health care finance, quality and patient safety, and hospital and post-acute provider related issues. Also based in CHA’s Washington, DC office, Megan works with Chad, CHA issue managers and national hospital associations on analysis and policy development for advocacy purposes.
Agenda
CALIFORNIA HOSPITAL ASSOCIATION 6
Outpatient Prospective Payment System (OPPS) Proposed Rule
• OPPS Payment and Policy Updates
• 340B Updates
• Inpatient-Only (IPO) List
• Rural Emergency Hospital
• Radiation Oncology Model
• Price Transparency
• Outpatient Quality Reporting Program
• Additional Requests for Comment
Physician Fee Schedule (PFS) Proposed Rule
• PFS Conversion Factor• Rural Health Clinic (RHC)
Payment• Evaluation/Management Services• Medicare Shared Savings
Program• Telehealth• Appropriate Use Criteria (AUC)• Quality Payment Program
5
6
8/25/2021
4
Overview/How to Comment
CALIFORNIA HOSPITAL ASSOCIATION 7
• On July 23, the Centers for Medicare & Medicaid Services (CMS) published the calendar year (CY) 2022 PFS proposed rule.
• On August 4, CMS published the CY 2022 OPPS proposed rule.
• Comments due to CMS by 2 p.m. (PT) on:
✓ September 13 for the PFS proposed rule
✓ September 17 for the OPPS proposed rule
• Submit comments online at regulations.gov
✓ Search “CMS-1751-P” for PFS
✓ Search “CMS-1753-P” for OPPS
• CHA summaries are available: PFS and OPPS
8
Outpatient Prospective Payment SystemKey Provisions
7
8
8/25/2021
5
OPPS: Key Proposed Changes
CALIFORNIA HOSPITAL ASSOCIATION 9
• Use CY 2019 claims and fiscal year (FY) 2018 cost report data to set the CY 2022 payment rates due to the effect of the COVID–19 public health emergency (PHE).
• Reverse the elimination of the IPO list and add back in services removed in CY 2021.
• Create a universal low volume Ambulatory Payment Classification (APC) policy.
• Continue the reduction in payment to 340B hospitals for separately payable Part B drugs.
• Amend price transparency requirements, increasing penalties for non-compliance.• Make changes to the radiation oncology model.
• Update the requirements for the Hospital Outpatient Quality Reporting (OQR) Program.
The proposed rule includes policies that will:
The increase in OPPS spending due only to changes in the 2022 OPPS proposed rule is estimated to be approximately $1.35 billion.
Proposed OPPS Conversion Factor update
CALIFORNIA HOSPITAL ASSOCIATION 10
The proposed OPPS conversion factor increases 2% over the prior year.
Final
CY 2021
Proposed
CY 2022
Percent
Change
OPPS Conversion Factor $82.797 $84.457 +2.00%
Proposed CY 2022 Update Factor Component Value
Market Basket (MB) Update +2.5%
Affordable Care Act (ACA)–Mandated Productivity MB
Reduction–0.2 percentage points (PPT)
Wage Index BN Adjustment +0.12%
Pass–through Spending/Outlier BN Adjustment –0.38%
Cancer Hospital BN Adjustment +0.00%
Overall Proposed Rate Update +2.04%
9
10
8/25/2021
6
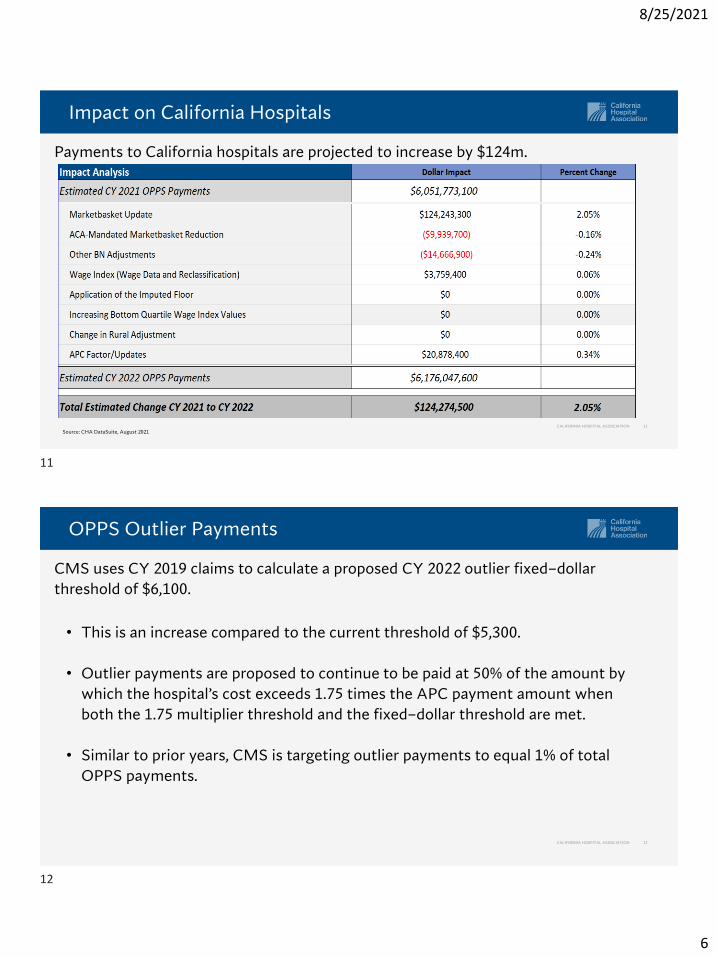
Impact on California Hospitals
CALIFORNIA HOSPITAL ASSOCIATION 11
Payments to California hospitals are projected to increase by $124m.
Source: CHA DataSuite, August 2021
OPPS Outlier Payments
CALIFORNIA HOSPITAL ASSOCIATION 12
• This is an increase compared to the current threshold of $5,300.
• Outlier payments are proposed to continue to be paid at 50% of the amount by
which the hospital’s cost exceeds 1.75 times the APC payment amount when
both the 1.75 multiplier threshold and the fixed–dollar threshold are met.
• Similar to prior years, CMS is targeting outlier payments to equal 1% of total
OPPS payments.
CMS uses CY 2019 claims to calculate a proposed CY 2022 outlier fixed–dollar
threshold of $6,100.
11
12
8/25/2021
7
Claims Used for Rate-Setting
CALIFORNIA HOSPITAL ASSOCIATION 13
• CMS believes 2020 outpatient utilization has been significantly affected by the
COVID-19 PHE, as it did for the FY 2022 inpatient prospective payment system
(IPPS) proposed rule.
• CMS’ analysis of the issue in the CY 2022 OPPS proposed rule is nearly identical
to the analysis provided in the FY 2022 IPPS proposed rule.
• CMS also proposes to extend pass-through payment for up to four quarters for 21 drugs, and one device whose pass-through status was scheduled to expire in CY 2022 (Table 38, pg. 42192).
CMS proposes using 2019 outpatient claims and FY 2018 hospital cost report data to set the OPPS relative weights for 2022.
Wage Index
CALIFORNIA HOSPITAL ASSOCIATION 14
• Labor related share remains at 60%.
• For non-IPPS hospitals paid under the OPPS for 2022, CMS proposes continuing its past policies of assigning the wage index that would be applicable if the hospital were paid under the IPPS and allowing the hospital to qualify for the out-migration adjustment.
• For Community Mental Health Centers (CMHC), CMS proposes continuing to calculate the wage index by using the post-reclassification IPPS wage index based on the core-based statistical area (CBSA) where the CMHC is located.
Similar to prior years, CMS proposes to use the FY 2022 IPPS post-reclassified wage index for the CY 2022 OPPS.
13
14
8/25/2021
8
Comprehensive Ambulatory Payment Classification (C-APC)
CALIFORNIA HOSPITAL ASSOCIATION 15
• The treatment is a Food and Drug Administration (FDA)-approved (or indicated in the
“Criteria for Issuance of Authorization”) drug or biological product (which could include
a blood product) authorized to treat COVID–19.
• The emergency use authorization for the drug or biological product must authorize the
use of the product in the outpatient setting or not limit its use to the inpatient setting
or be approved by the FDA to treat COVID–19 disease and not limit its use to the
inpatient setting.
This is in effect from the effective date of the interim final rule (November 2, 2020) with
comment period (IFC) until the end of the pandemic.
CMS continues its exclusion for new COVID–19 treatments meeting certain criteria from C-APC packaging.
Any New COVID–19 Treatment Meeting the Following Criteria Is Separately Payable:
Payment for Drugs, Biologicals, and Radiopharmaceuticals
CALIFORNIA HOSPITAL ASSOCIATION 16
• CMS proposes a packaging threshold of $130.
• Separately payable drugs and biological products without pass–through status and not acquired under the 340B program are paid wholesale acquisition cost (WAC) plus 3% instead of WAC plus 6%.
• CMS proposes to continue to pay for therapeutic radiopharmaceuticals with pass–through payments status as well as blood clotting factors, based on ASP plus 6%.
• Pass–through status will expire by December 31, 2021, for 25 drugs and biologicals listed in Table 27 (page 42118 of the proposed rule) and by December 31, 2022, for 26 drugs and biologicals listed in Table 28 (page 42121 of the proposed rule).
• CMS also proposed to continue/establish pass–through status in CY 2022 to 46 others, shown in Table 29 (page 42124 of the proposed rule).
Drugs, biologicals, and radiopharmaceuticals above the packaging threshold will continue to be paid at average sales price (ASP) plus 6%.
15
16
8/25/2021
9
Drugs Acquired Under 340B
CALIFORNIA HOSPITAL ASSOCIATION 17
• The 340B adjustment applies to drugs priced based on WAC and average wholesale price.
• CMS proposes to continue paying for drugs priced under WAC at WAC minus 22.5%, while those acquired under average wholesale price (AWP) pricing are paid at 69.46% of AWP.
• Proposed Exemptions: Critical access hospitals (CAHs), sole community hospitals (SCHs), children’s hospitals, and PPS–exempt cancer hospitals will receive drug payments based on ASP plus 6% if finalized.
• Modifier “JG” is used by non–exempt hospitals to report separately payable drugs that were acquired through the 340B program, and thus paid the reduced rate.
• Modifier “TB” is used by hospitals exempt from the 340B payment adjustment to report separately payable drugs that were acquired through the 340B program.
CMS proposes continuing to pay ASP minus 22.5% for separately payable drugs and biologicals acquired under the 340B program.
Payment for Off-Campus PBD Clinic Visits
CALIFORNIA HOSPITAL ASSOCIATION 18
• These excepted PBDs continue to bill HCPCS code G0463 with modifier “PO”.
CMS is proposing to continue to apply a 60% reduction to the OPPS rate for excepted off–campus provider-based departments (PBDs) for basic clinic services in CY 2022.
17
18
8/25/2021
10
Inpatient-Only (IPO) List
CALIFORNIA HOSPITAL ASSOCIATION 19
• CMS proposes reinstating the 266 musculoskeletal services and 32 other Healthcare Common Procedure Coding System (HCPCS) codes that were removed in CY 2021.
• CMS proposes codifying in regulation the five criteria to determine if a procedure or service should be removed from the IPO list.
• CMS solicits comments on services that were removed in CY 2021 and should remain off the list but are proposed to be reinstated for CY 2022.
CMS proposes to halt the elimination of the IPO list.
2-Midnight Rule for IPO List
CALIFORNIA HOSPITAL ASSOCIATION 20
• In the CY 2020 OPPS final rule, CMS established a two–year exemption from
medical review activities, including referrals to recovery audit contractors
(RACs), site–of–service claim denials, and RAC reviews for “patient status” for
procedures removed from the IPO list for CY 2020 and forward.
• In the CY 2021 OPPS rule, CMS finalized an indefinite exemption from medical
review activities for procedures removed from the IPO list on or after
January 1, 2021.
CMS proposes rescinding the indefinite exemption period and reinstating the two–year exemption from medical review activities for procedures removed from the IPO list beginning on or after January 1, 2021.
19
20
8/25/2021
11
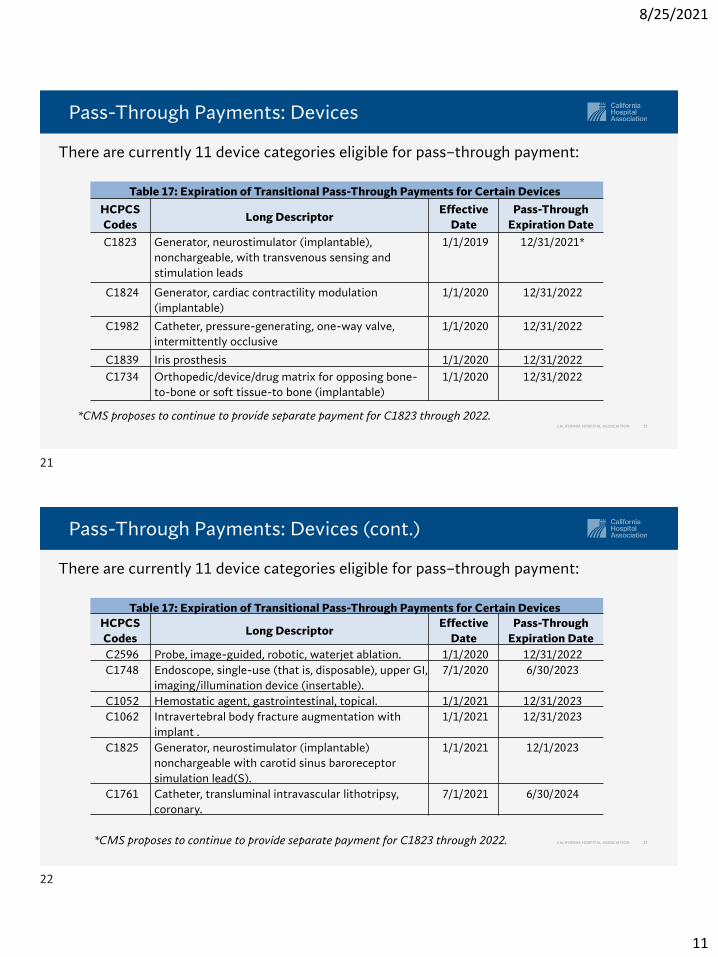
Pass-Through Payments: Devices
CALIFORNIA HOSPITAL ASSOCIATION 21
There are currently 11 device categories eligible for pass–through payment:
*CMS proposes to continue to provide separate payment for C1823 through 2022.
Table 17: Expiration of Transitional Pass-Through Payments for Certain Devices
HCPCS
CodesLong Descriptor
Effective
Date
Pass-Through
Expiration Date
C1823 Generator, neurostimulator (implantable),
nonchargeable, with transvenous sensing and
stimulation leads
1/1/2019 12/31/2021*
C1824 Generator, cardiac contractility modulation
(implantable)
1/1/2020 12/31/2022
C1982 Catheter, pressure-generating, one-way valve,
intermittently occlusive
1/1/2020 12/31/2022
C1839 Iris prosthesis 1/1/2020 12/31/2022
C1734 Orthopedic/device/drug matrix for opposing bone-
to-bone or soft tissue-to bone (implantable)
1/1/2020 12/31/2022
Pass-Through Payments: Devices (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 22
There are currently 11 device categories eligible for pass–through payment:
Table 17: Expiration of Transitional Pass-Through Payments for Certain Devices
HCPCS
CodesLong Descriptor
Effective
Date
Pass-Through
Expiration Date
C2596 Probe, image-guided, robotic, waterjet ablation. 1/1/2020 12/31/2022
C1748 Endoscope, single-use (that is, disposable), upper GI,
imaging/illumination device (insertable).
7/1/2020 6/30/2023
C1052 Hemostatic agent, gastrointestinal, topical. 1/1/2021 12/31/2023
C1062 Intravertebral body fracture augmentation with
implant .
1/1/2021 12/31/2023
C1825 Generator, neurostimulator (implantable)
nonchargeable with carotid sinus baroreceptor
simulation lead(S).
1/1/2021 12/1/2023
C1761 Catheter, transluminal intravascular lithotripsy,
coronary.
7/1/2021 6/30/2024
*CMS proposes to continue to provide separate payment for C1823 through 2022.
21
22
8/25/2021
12
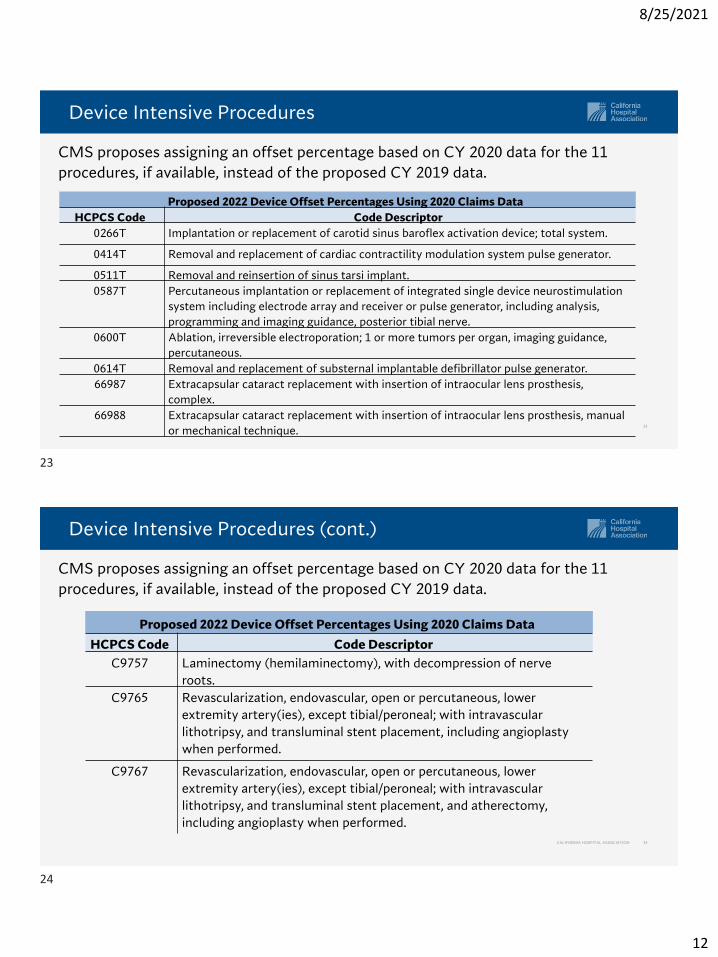
Device Intensive Procedures
23
CMS proposes assigning an offset percentage based on CY 2020 data for the 11
procedures, if available, instead of the proposed CY 2019 data.
Proposed 2022 Device Offset Percentages Using 2020 Claims Data
HCPCS Code Code Descriptor
0266T Implantation or replacement of carotid sinus baroflex activation device; total system.
0414T Removal and replacement of cardiac contractility modulation system pulse generator.
0511T Removal and reinsertion of sinus tarsi implant.
0587T Percutaneous implantation or replacement of integrated single device neurostimulation
system including electrode array and receiver or pulse generator, including analysis,
programming and imaging guidance, posterior tibial nerve.
0600T Ablation, irreversible electroporation; 1 or more tumors per organ, imaging guidance,
percutaneous.
0614T Removal and replacement of substernal implantable defibrillator pulse generator.
66987 Extracapsular cataract replacement with insertion of intraocular lens prosthesis,
complex.
66988 Extracapsular cataract replacement with insertion of intraocular lens prosthesis, manual
or mechanical technique.
Device Intensive Procedures (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 24
CMS proposes assigning an offset percentage based on CY 2020 data for the 11
procedures, if available, instead of the proposed CY 2019 data.
Proposed 2022 Device Offset Percentages Using 2020 Claims Data
HCPCS Code Code Descriptor
C9757 Laminectomy (hemilaminectomy), with decompression of nerve
roots.
C9765 Revascularization, endovascular, open or percutaneous, lower
extremity artery(ies), except tibial/peroneal; with intravascular
lithotripsy, and transluminal stent placement, including angioplasty
when performed.
C9767 Revascularization, endovascular, open or percutaneous, lower
extremity artery(ies), except tibial/peroneal; with intravascular
lithotripsy, and transluminal stent placement, and atherectomy,
including angioplasty when performed.
23
24
8/25/2021
13
Sole Community Hospital (SCH) Adjustment
CALIFORNIA HOSPITAL ASSOCIATION 25
• This includes services and procedures paid under the OPPS, excluding separately payable drugs and biologicals, devices paid under the pass-through payment policy, and items paid at charges reduced to costs.
• The adjustment is budget neutral and is applied before calculating outliers and copayments.
• CMS is proposing to maintain this for future years until data supports a change to the adjustment.
CMS proposes to continue applying a 7.1% payment adjustment to all SCHs.
Cancer Hospital Adjustment
CALIFORNIA HOSPITAL ASSOCIATION 26
• CMS adjusts payments so the hospital’s target payment–to–cost ratio (PCR) after the additional payments is equal to the weighted average PCR for the other OPPS hospitals.
• Due to the COVID–19 PHE, CMS is holding the target PCR equal to that of CY 2021.
• Since this is the same target PCR as CY 2021, CMS proposed a 0% adjustment to the CY 2022 conversion factor to account for this policy.
CMS proposes continuing providing payment increases to the 11 hospitals
identified as exempt cancer hospitals.
25
26
8/25/2021
14
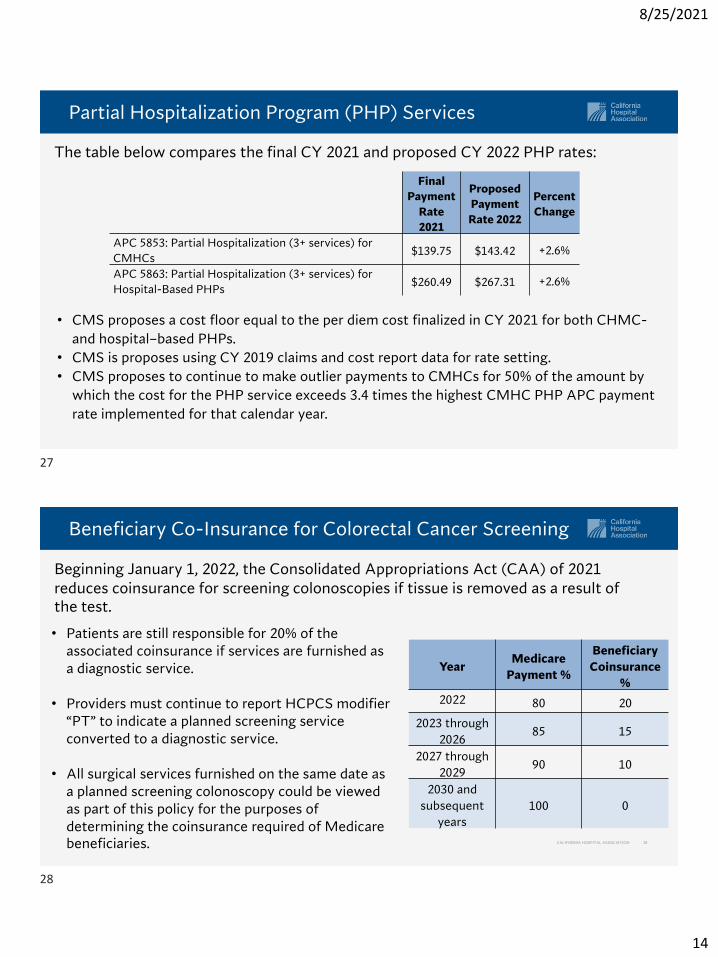
Partial Hospitalization Program (PHP) Services
27
• CMS proposes a cost floor equal to the per diem cost finalized in CY 2021 for both CHMC-
and hospital–based PHPs.
• CMS is proposes using CY 2019 claims and cost report data for rate setting.
• CMS proposes to continue to make outlier payments to CMHCs for 50% of the amount by
which the cost for the PHP service exceeds 3.4 times the highest CMHC PHP APC payment
rate implemented for that calendar year.
The table below compares the final CY 2021 and proposed CY 2022 PHP rates:
Final
Payment
Rate
2021
Proposed
Payment
Rate 2022
Percent
Change
APC 5853: Partial Hospitalization (3+ services) for
CMHCs$139.75 $143.42 +2.6%
APC 5863: Partial Hospitalization (3+ services) for
Hospital-Based PHPs$260.49 $267.31 +2.6%
Beneficiary Co-Insurance for Colorectal Cancer Screening
CALIFORNIA HOSPITAL ASSOCIATION 28
Beginning January 1, 2022, the Consolidated Appropriations Act (CAA) of 2021 reduces coinsurance for screening colonoscopies if tissue is removed as a result of the test.
• Patients are still responsible for 20% of the associated coinsurance if services are furnished as a diagnostic service.
• Providers must continue to report HCPCS modifier “PT” to indicate a planned screening service converted to a diagnostic service.
• All surgical services furnished on the same date as a planned screening colonoscopy could be viewed as part of this policy for the purposes of determining the coinsurance required of Medicare beneficiaries.
YearMedicare
Payment %
Beneficiary
Coinsurance
%
2022 80 20
2023 through
202685 15
2027 through
202990 10
2030 and
subsequent
years
100 0
27
28
8/25/2021
15
Rural Emergency Hospital (REH)- Background
CALIFORNIA HOSPITAL ASSOCIATION 29
The CAA of 2021 establishes REHs as a new provider type starting January 1, 2023.
• REHs provide emergency department services, observation care, and potentially other medical and health services on an outpatient basis.
• REHs must not provide inpatient services (except skilled-nursing facility services in a distinct unit).
• CAHs and rural hospitals with fewer than 50 beds are eligible to convert to an REH.
• REHs will be paid at the OPPS rate plus 5%.
• REHs will also receive a monthly payment based on the excess of the total amount paid to all CAHs in 2019 over the estimated total amount that would have been paid to CAHs in 2019 if payment were made for inpatient, outpatient, and SNF services under the PPS.
REH – Request For Information
CALIFORNIA HOSPITAL ASSOCIATION 30
CMS seeks comment on the health and safety standards, payment policies, enrollment, health equity, and quality measures and reporting requirements.
• Type and scope of services offered, including what outpatient medical and health
services should be considered as eligible services.
• Health and safety standards, including licensure and conditions of participation.
• How REHs can help address social needs in rural areas and if there are additional
factors to consider for specific populations.
• Quality measures, including quality reporting requirements, specification of measures,
and public reporting of data.
• Payment provisions, including what payment reporting issues should be considered
when estimating payments under prospective payment systems for service furnished.
• Enrollment process, such as the steps and timing for conversion to an REH.
29
30
8/25/2021
16
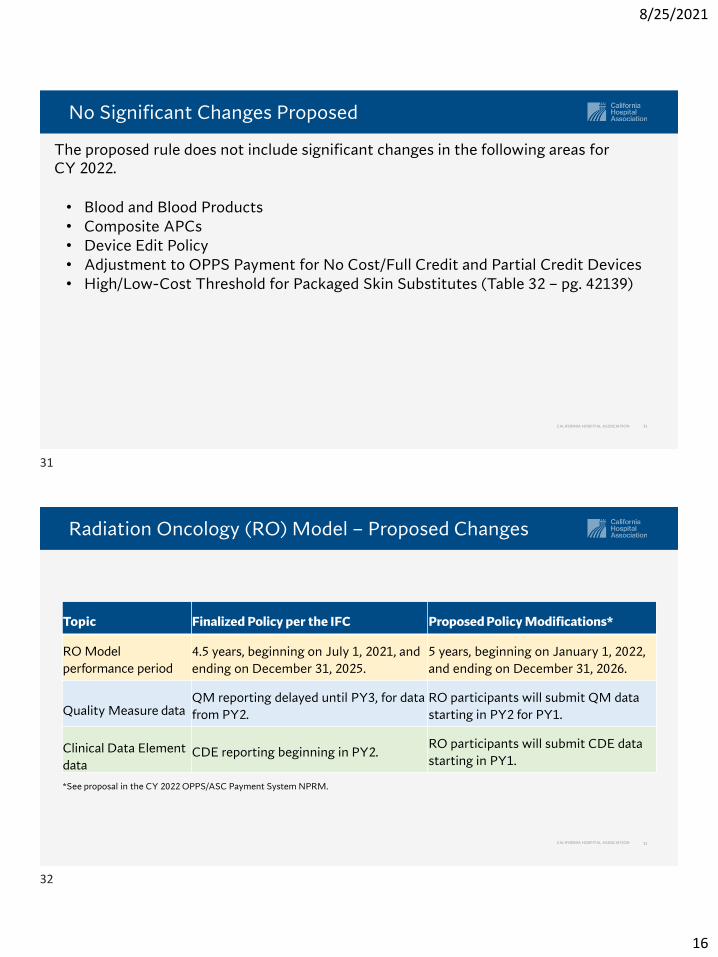
No Significant Changes Proposed
CALIFORNIA HOSPITAL ASSOCIATION 31
• Blood and Blood Products• Composite APCs• Device Edit Policy• Adjustment to OPPS Payment for No Cost/Full Credit and Partial Credit Devices• High/Low-Cost Threshold for Packaged Skin Substitutes (Table 32 – pg. 42139)
The proposed rule does not include significant changes in the following areas for CY 2022.
Radiation Oncology (RO) Model – Proposed Changes
32
Topic Finalized Policy per the IFC Proposed Policy Modifications*
RO Model
performance period
4.5 years, beginning on July 1, 2021, and
ending on December 31, 2025.
5 years, beginning on January 1, 2022,
and ending on December 31, 2026.
Quality Measure dataQM reporting delayed until PY3, for data
from PY2.
RO participants will submit QM data
starting in PY2 for PY1.
Clinical Data Element
dataCDE reporting beginning in PY2.
RO participants will submit CDE data
starting in PY1.
*See proposal in the CY 2022 OPPS/ASC Payment System NPRM.
CALIFORNIA HOSPITAL ASSOCIATION
31
32
8/25/2021
17
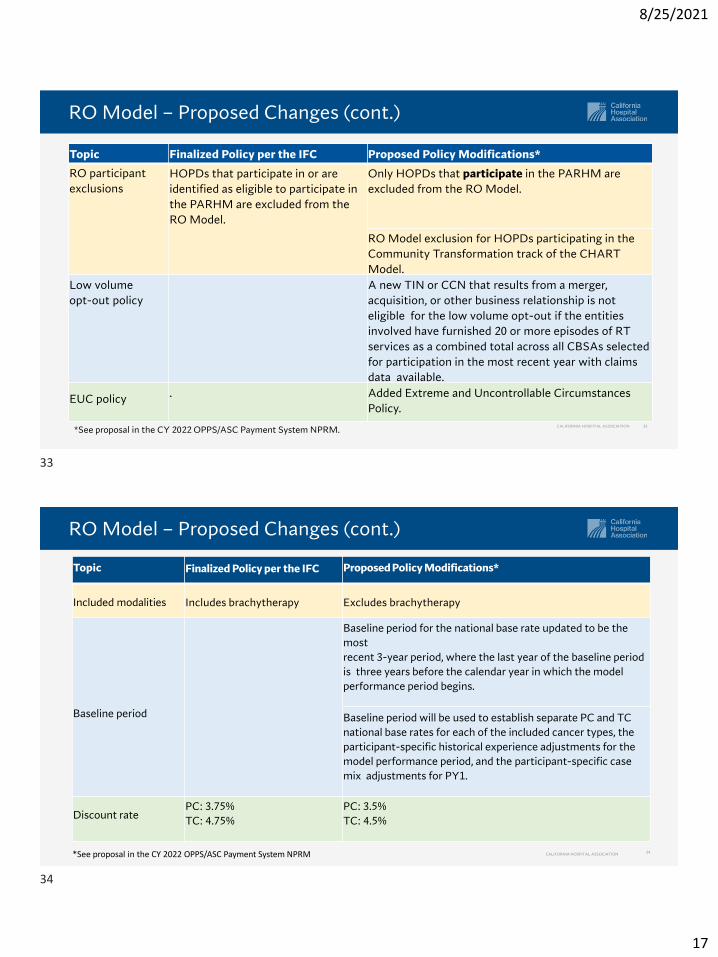
RO Model – Proposed Changes (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 33
Topic Finalized Policy per the IFC Proposed Policy Modifications*
RO participant
exclusions
HOPDs that participate in or are
identified as eligible to participate in
the PARHM are excluded from the
RO Model.
Only HOPDs that participate in the PARHM are
excluded from the RO Model.
RO Model exclusion for HOPDs participating in the
Community Transformation track of the CHART
Model.
Low volume
opt-out policy
A new TIN or CCN that results from a merger,
acquisition, or other business relationship is not
eligible for the low volume opt-out if the entities
involved have furnished 20 or more episodes of RT
services as a combined total across all CBSAs selected
for participation in the most recent year with claims
data available.
EUC policy . Added Extreme and Uncontrollable Circumstances
Policy.
*See proposal in the CY 2022 OPPS/ASC Payment System NPRM.
RO Model – Proposed Changes (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 34*See proposal in the CY 2022 OPPS/ASC Payment System NPRM
Topic Finalized Policy per the IFC Proposed Policy Modifications*
Included modalities Includes brachytherapy Excludes brachytherapy
Baseline period
Baseline period for the national base rate updated to be the
most
recent 3-year period, where the last year of the baseline period
is three years before the calendar year in which the model
performance period begins.
Baseline period will be used to establish separate PC and TC
national base rates for each of the included cancer types, the
participant-specific historical experience adjustments for the
model performance period, and the participant-specific case
mix adjustments for PY1.
Discount ratePC: 3.75%
TC: 4.75%
PC: 3.5%
TC: 4.5%
33
34
8/25/2021
18
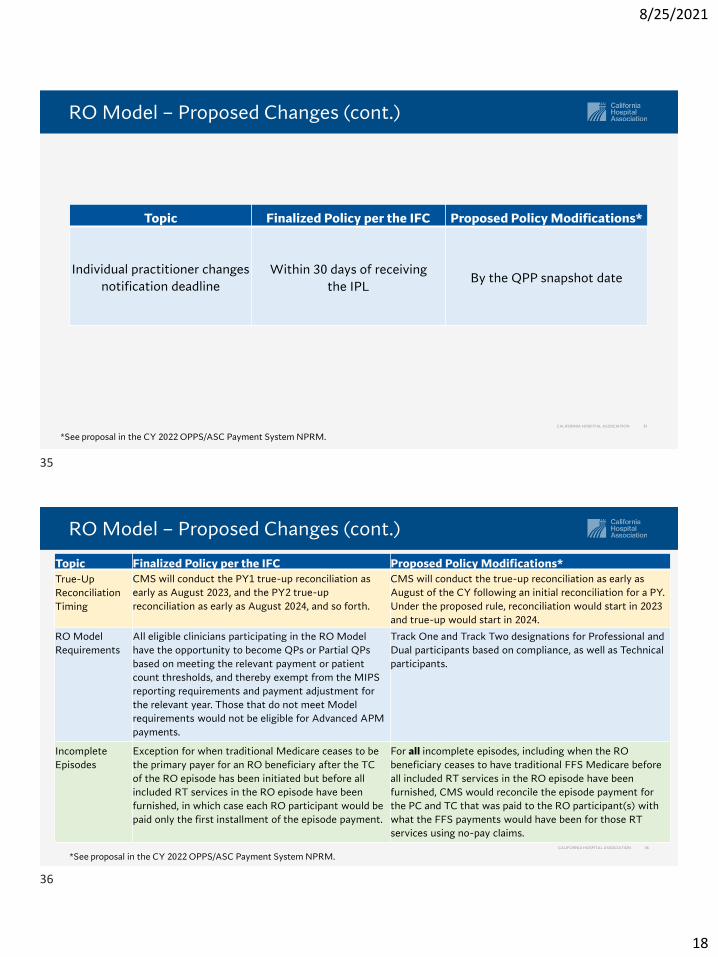
RO Model – Proposed Changes (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 35
Topic Finalized Policy per the IFC Proposed Policy Modifications*
Individual practitioner changes
notification deadline
Within 30 days of receiving
the IPLBy the QPP snapshot date
*See proposal in the CY 2022 OPPS/ASC Payment System NPRM.
RO Model – Proposed Changes (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 36
Topic Finalized Policy per the IFC Proposed Policy Modifications*
True-Up
Reconciliation
Timing
CMS will conduct the PY1 true-up reconciliation as
early as August 2023, and the PY2 true-up
reconciliation as early as August 2024, and so forth.
CMS will conduct the true-up reconciliation as early as
August of the CY following an initial reconciliation for a PY.
Under the proposed rule, reconciliation would start in 2023
and true-up would start in 2024.
RO Model
Requirements
All eligible clinicians participating in the RO Model
have the opportunity to become QPs or Partial QPs
based on meeting the relevant payment or patient
count thresholds, and thereby exempt from the MIPS
reporting requirements and payment adjustment for
the relevant year. Those that do not meet Model
requirements would not be eligible for Advanced APM
payments.
Track One and Track Two designations for Professional and
Dual participants based on compliance, as well as Technical
participants.
Incomplete
Episodes
Exception for when traditional Medicare ceases to be
the primary payer for an RO beneficiary after the TC
of the RO episode has been initiated but before all
included RT services in the RO episode have been
furnished, in which case each RO participant would be
paid only the first installment of the episode payment.
For all incomplete episodes, including when the RO
beneficiary ceases to have traditional FFS Medicare before
all included RT services in the RO episode have been
furnished, CMS would reconcile the episode payment for
the PC and TC that was paid to the RO participant(s) with
what the FFS payments would have been for those RT
services using no-pay claims.
*See proposal in the CY 2022 OPPS/ASC Payment System NPRM.
35
36
8/25/2021
19
Hospital Price Transparency
CALIFORNIA HOSPITAL ASSOCIATION 37
• Under the Hospital Price Transparency final rule, CMS requires all hospitals post price information on their website to comply with two specific requirements:
✓ Post gross charges, payer-specific negotiated rates, the de-identified minimum and maximum negotiated rates, and the cash discount price for all items and services on a website in a machine-readable format.
✓ Post information for 300 “shoppable” services (70 CMS-specified and 230 hospital-selected) in a “consumer-friendly manner,” OR provide an Internet-based price estimator tool for common shoppable services.
• In response to what CMS deems as high rates of noncompliance with the requirements — which were effective January 1, 2021 — CMS proposes to increase the maximum civil monetary penalty (CMP) (currently $300/day) using a scaling factor to establish the CMP amount for a noncompliant hospital.
• CMS proposes to use the noncompliant hospital’s number of beds as specified in hospital cost report data as the scaling factor to establish CMP amounts.
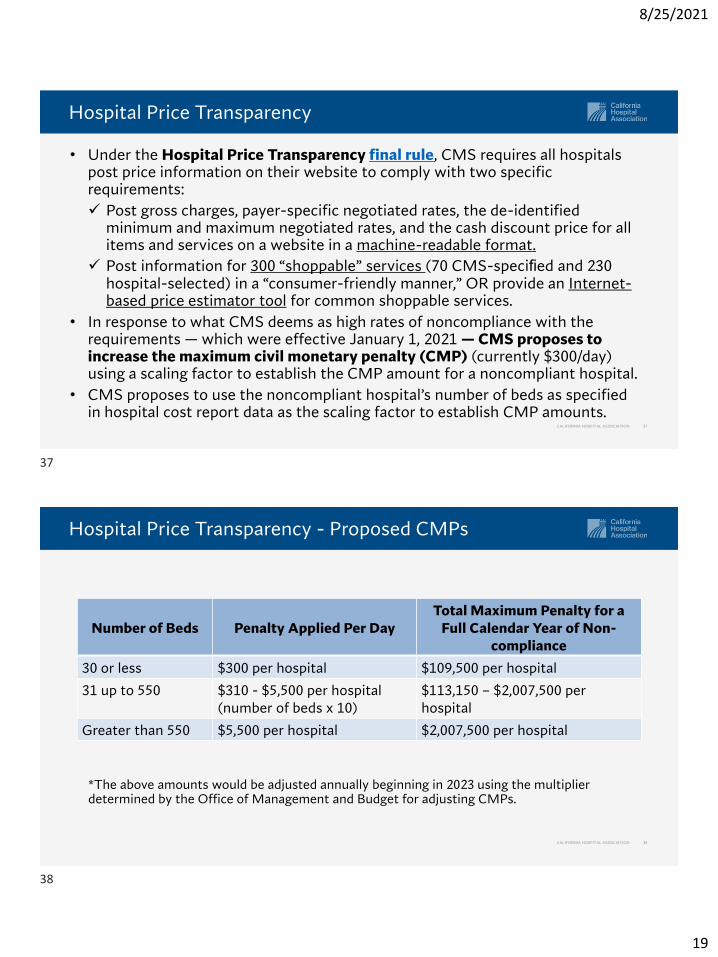
Hospital Price Transparency - Proposed CMPs
CALIFORNIA HOSPITAL ASSOCIATION 38
*The above amounts would be adjusted annually beginning in 2023 using the multiplier determined by the Office of Management and Budget for adjusting CMPs.
Number of Beds Penalty Applied Per DayTotal Maximum Penalty for a
Full Calendar Year of Non-compliance
30 or less $300 per hospital $109,500 per hospital
31 up to 550 $310 - $5,500 per hospital (number of beds x 10)
$113,150 – $2,007,500 per hospital
Greater than 550 $5,500 per hospital $2,007,500 per hospital
37
38
8/25/2021
20
Hospital Price Transparency
CALIFORNIA HOSPITAL ASSOCIATION 39
• Machine-Readable File: CMS proposes to specify that the hospital must ensure that standard charge information is easily accessible, without barriers, including but not limited to ensuring the information is accessible to automated searches and direct file downloads through a link posted on a publicly available website.
• Shoppable Services and Price Estimator Tool: CMS clarifies that price estimator tools must be “tailored to individuals’ circumstances” to satisfy requirements as an alternative to posting shoppable services price information.
✓ Hospital must provide real-time individualized out-of-pocket estimates that combine hospital standard charge information with the individual’s benefit information directly from the insurer or provide the self-pay amount.
• Requests for Comment for Future Rulemaking:
✓ Best practices for price estimators
✓ Standardization of machine-readable file
✓ Expectations for plain language descriptions of shoppable services
✓ Recognizing “exemplar” hospitals
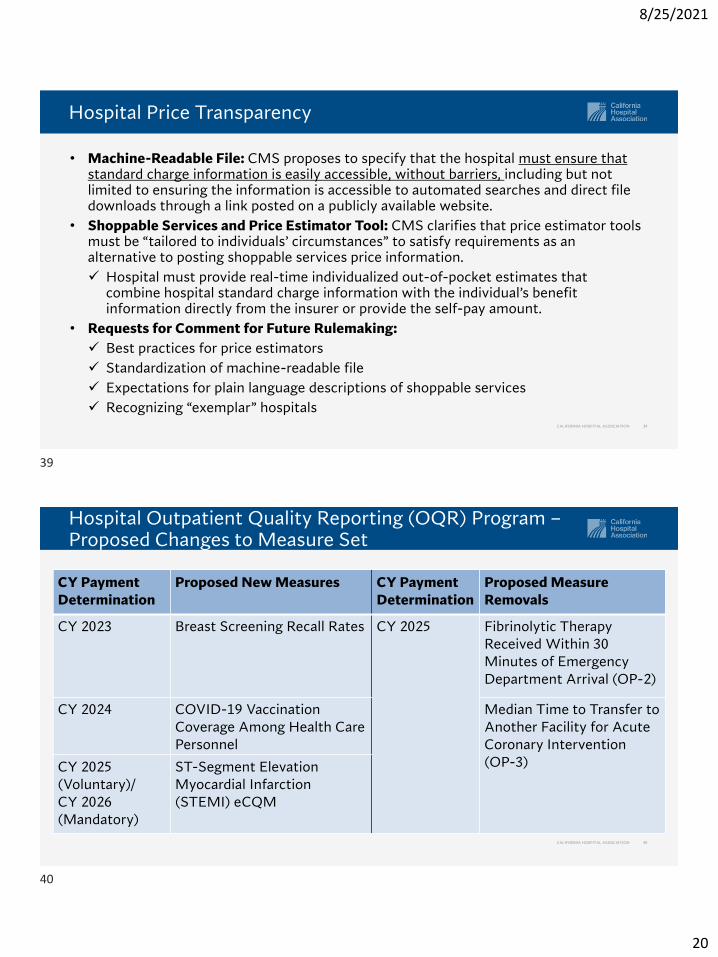
Hospital Outpatient Quality Reporting (OQR) Program –Proposed Changes to Measure Set
CALIFORNIA HOSPITAL ASSOCIATION 40
CY Payment Determination
Proposed New Measures CY Payment Determination
Proposed Measure Removals
CY 2023 Breast Screening Recall Rates CY 2025 Fibrinolytic Therapy Received Within 30 Minutes of Emergency Department Arrival (OP-2)
CY 2024 COVID-19 Vaccination Coverage Among Health Care Personnel
Median Time to Transfer to Another Facility for Acute Coronary Intervention (OP-3)CY 2025
(Voluntary)/CY 2026 (Mandatory)
ST-Segment Elevation Myocardial Infarction (STEMI) eCQM
39
40
8/25/2021
21
COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) Measure
CALIFORNIA HOSPITAL ASSOCIATION 41
• Proposed measure would track the percentage of healthcare personnel (HCP) who receive a complete COVID-19 vaccination.✓ Detailed measure specifications available on CDC’s website
✓ For OQR Program, CMS clarifies that acute care facilities would count all HCP working in all inpatient or outpatient units that share a hospital’s CMS Certification Number (CCN), regardless of a unit’s size or type.
• CMS proposes to require an initial data reporting of January 1, 2022, through December 31, 2021, for the CY 2024 payment year.
• Hospitals would submit measure data using the National Health Safety Network’s (NHSN) standard data submission requirements via the CDC/NHSN web-based surveillance system.
• CMS would publicly report the CDC-calculated vaccination coverage rates on a quarterly basis on Care Compare.
• CMS has finalized this measure for the inpatient quality reporting (IQR) program, SNF QRP, and inpatient rehabilitation facility QRP beginning with FFY 2023 payment determination.
Hospital OQR Program – Modifications to Previously Adopted Measures
CALIFORNIA HOSPITAL ASSOCIATION 42
CMS also proposes modifications to two previously adopted – but delayed – measures:
• Cataracts: Improvement in Patient’s Visual Function within 90 Days Following Cataract Surgery (OP-31): CMS proposes to require mandatory reporting through the CMS web-based tool beginning with the 2023 reporting year/2025 payment determination.
• Outpatient and Ambulatory Surgery Consumer Assessment of Healthcare Providers and Systems (OAS CAHPS) Survey-Based Measures (OP-37a-e): CMS proposes a voluntary reporting for the 2023 reporting period/2025 payment determination, and mandatory reporting beginning with the 2024 reporting period/2026 payment determination.
✓ CMS proposes to add two web-based data collection modes for the 2023 reporting period/2025 payment determination.
✓ CMS proposes a low-volume exception that would apply to hospitals with fewer than 60 survey-eligible patients during the calendar year just prior to the data collection period.
41
42
8/25/2021
22
Additional OQR Program Proposals
CALIFORNIA HOSPITAL ASSOCIATION 43
• CMS proposes several changes to electronic clinical quality measures (eCQMs) reporting to align with IQR and Promoting Interoperability Program requirements.
• CMS proposes changes to the OQR data validation process beginning with the 2022 reporting period/2024 payment to further align the OQR Program with the hospital IQR Program.
• CMS seeks comments for future rulemaking:
✓ Measures to assess quality of care for services whose delivery is shifting from inpatient to outpatient settings.
✓ Adoption of a Hospital-Level Risk-Standardized Patient Reported Outcomes Measure Following Elective Primary Total Hip and/or Total Knee Arthroplasty specified for the outpatient setting.
• CMS continues its focus on health equity seeking comment on:
✓ Stratification of certain measure hospital-specific reports by dual eligibility and race and ethnicity.
✓ Hospital collection of standardized demographic information.
Requests for Information: dQMs and Safe Use of Opioids eCQM
CALIFORNIA HOSPITAL ASSOCIATION 44
• CMS continues to requests input into the agency’s planning for transformation to a fully digital quality enterprise by 2025, posing numerous questions grouped into three categories:
✓ Definition of digital quality measures (dQMs).
✓ Potential role of Fast Healthcare Interoperability Resources (FHIR)-based standards, including transitioning to FHIR-based quality reporting through APIs for existing eCQMs.
✓ How dQMs could support alignment across public and private quality measurement efforts.
• Under both the hospital IQR and Promoting Interoperability programs, hospitals are required to report three self–select eCQMs and the Safe Use of Opioids eCQM beginning with the 2022 reporting period.
✓ CMS seeks feedback on whether reporting the Safe Use of Opioids eCQM should be required or self–selected by hospitals as part of the available eCQM measure set.
43
44
8/25/2021
23
Request for Comment on Maintaining COVID-19 PHE Flexibilities
CALIFORNIA HOSPITAL ASSOCIATION 45
CMS seeks comment on permanently extending several temporary policies intended to address the COVID-19 PHE:
• Mental Health Services Furnished Remotely by Hospital Staff to Beneficiaries in their homes.
• Direct Supervision by Interactive Communications Technology.
• Payment for COVID-19 Specimen Collection in HOPDs.
Questions
CALIFORNIA HOSPITAL ASSOCIATION 46
45
46
8/25/2021
24
47
Physician Fee ScheduleKey Provisions
Physician Fee Schedule – Conversion Factor
CALIFORNIA HOSPITAL ASSOCIATION 48
CMS proposes a slight decrease in PFS payment rates of 0.14% in CY 2022 .
• The actual change from the final CY 2021 conversion factor of $34.89 to the proposed CY 2022 conversion factor of $33.58 is a decrease of $1.31, or 3.89%.
• This reflects the expiration of the one-time 3.75% payment increase to the conversion factor included in the CAA of 2021, a zero-percent update factor as required by MACRA and a budget-neutrality adjustment.
47
48

8/25/2021
25
RHC Modernization Act
CALIFORNIA HOSPITAL ASSOCIATION 49
• Definition of Existing RHCs: “Existing” RHCs that are provider-based to hospitals under 50 beds must have either:
1. Been enrolled in Medicare as of December 31, 2020; or2. Submitted an application for enrollment in Medicare that was received no
later than December 31, 2020.
• Medical economic index: the proposed inflation factor for 2022 is 1.8 precent. CMS will likely update this in the final rule based on more recent data if it is available.
• Base year: The proposed rule clarified that if an RHC does not have a calendar year cost report, the 2020 reasonable cost per visit will be from the cost report that ends in 2020.
The CAA of 2021 capped the all-inclusive rate for existing RHCs that are provider-based to hospitals with less than 50 beds for services provided after April 1, 2021.
Payment for Therapy Services
CALIFORNIA HOSPITAL ASSOCIATION 50
• CMS proposes polices to implement requirements that the agency identifies and pays 85% of the otherwise applicable Part B payment amount for physical therapy and occupational therapy services furnished in whole or in part by physical therapist assistants (PTAs) and occupational therapy assistants (OTAs), for dates of service on and after Jan. 1, 2022.
• In previous rulemaking, CMS defined “in whole or in part” via de minimis standard and established modifiers (CQ/CO) to identify these claims.
• CMS proposes to clarify:
✓ Modifiers would apply if PTA /OTA furnishes 8 or more minutes of a timed unit of service, regardless of the minutes of service provided by the PT/OT.
✓ Modifiers would NOT apply if PT/OT provides 8 or more minutes of service, regardless of the minutes of service provided by the PTA/OTA.
49
50
8/25/2021
26
Evaluation & Management (E/M) Split Billing
CALIFORNIA HOSPITAL ASSOCIATION 51
• Definition: CMS proposes to define a split (or shared) visit as an E/M visit in the
facility setting that is performed in part by both a physician and a non-physician
practitioner (NPP) who are in the same group. CMS proposes to define facility
setting as an institutional setting in which “incident to” payment is prohibited.
• New and established patients; initial and subsequent visits: CMS proposes to modify
existing policy to allow physicians and NPPs to bill for split (or shared) visits for
both new and established patients and for both initial and subsequent visits.
• Substantive portion: CMS proposes to define the “substantive portion” of the split
(or shared) visit as more than half of the total time spent by the physician and non-
physician practitioner performing the visit.
CMS includes the following proposals related to split (or shared) visits:
E/M Split Billing (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 52
• Qualifying activities: CMS includes in the rule a list of activities that it proposes
to count toward total time for purposes of determining the substantive portion
of the visit.
• Claim identification: CMS proposes to create a modifier to describe split (or
shared) visits that providers would be required to append to claims for these
visits.
• Critical care services: The agency proposes to allow critical care visits to be
furnished as split (or shared) visits and delineates a unique list of qualifying
activities as well as other policies specific to split (or shared) critical care.
CMS includes the following proposals related to split (or shared) visits:
51
52

8/25/2021
27
Critical Care Split Billing
CALIFORNIA HOSPITAL ASSOCIATION 53
• Concurrent Care: CMS proposes to allow critical care services to be furnished as
concurrent care if medically necessary and not duplicative. Concurrent care is
defined as more than one physician or qualified NPP furnishing services to the
same patient on the same day.
• Global Surgical Period: CMS also proposes to bundle critical care visits with
procedure codes that have a global surgical period.
CMS proposes to adopt the Current Procedural Terminology (CPT) Professional Codebook definition of critical care that delineates where, when and by whom critical care services may be delivered.
Physician Self Referral - Clarifications
CALIFORNIA HOSPITAL ASSOCIATION 54
• The two-step analysis will apply to any unbroken chain of financial relationships in
which the compensation paid under the arrangement closest to the physician (or
immediate family member) is for anything other than services personally performed by
the physician.
• CMS proposes to define personally performed services to “not include services that are
performed by any person other than the physician (or immediate family member),
including, but not limited to, the referring physician’s (or immediate family member’s)
employees, independent contractors, group practice members, or persons supervised
by the physician (or the immediate family member).”
• CMS views all compensation as unit-based; as such, an underlying unit may be a
discrete item, a unit of service, a unit of time or a unit that results from combining
different types of units into a single unit used to calculate the compensation.
CMS proposes to clarify the “streamlined” two-step analysis of physician compensation
arrangements that was finalized in 2020.
53
54
8/25/2021
28
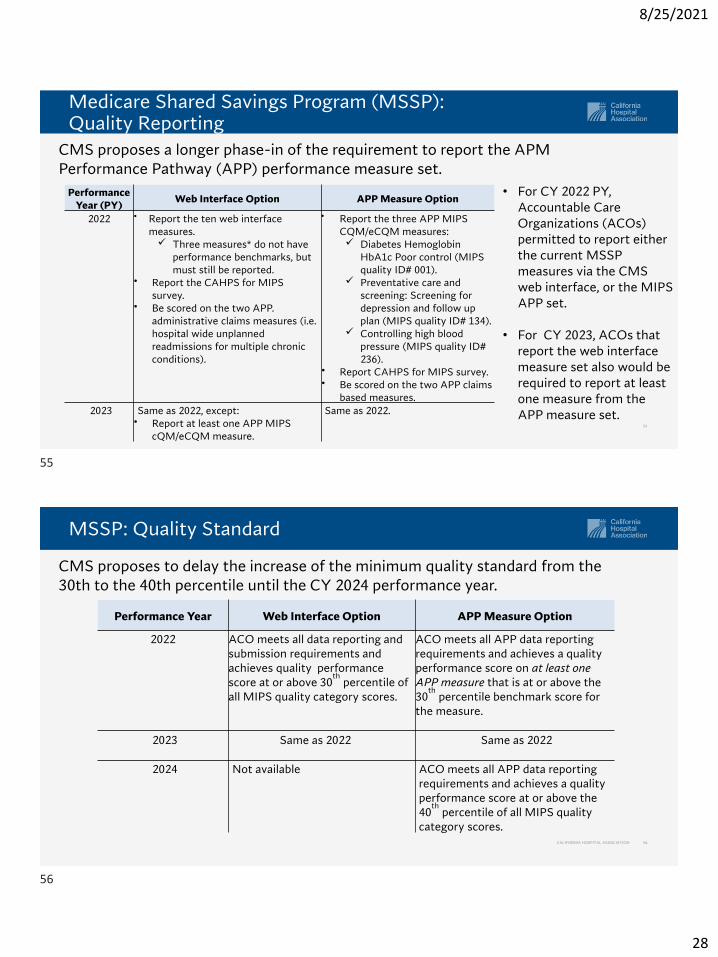
Medicare Shared Savings Program (MSSP): Quality Reporting
55
CMS proposes a longer phase-in of the requirement to report the APM Performance Pathway (APP) performance measure set.
• For CY 2022 PY, Accountable Care Organizations (ACOs) permitted to report either the current MSSP measures via the CMS web interface, or the MIPS APP set.
• For CY 2023, ACOs that report the web interface measure set also would be required to report at least one measure from the APP measure set.
Performance Year (PY)
Web Interface Option APP Measure Option
2022 • Report the ten web interface measures.✓ Three measures* do not have
performance benchmarks, but must still be reported.
• Report the CAHPS for MIPS survey.
• Be scored on the two APP. administrative claims measures (i.e. hospital wide unplanned readmissions for multiple chronic conditions).
• Report the three APP MIPS CQM/eCQM measures:✓ Diabetes Hemoglobin
HbA1c Poor control (MIPS quality ID# 001).
✓ Preventative care and screening: Screening for depression and follow up plan (MIPS quality ID# 134).
✓ Controlling high blood pressure (MIPS quality ID# 236).
• Report CAHPS for MIPS survey.• Be scored on the two APP claims
based measures.2023 Same as 2022, except:
• Report at least one APP MIPS cQM/eCQM measure.
Same as 2022.
MSSP: Quality Standard
CALIFORNIA HOSPITAL ASSOCIATION 56
CMS proposes to delay the increase of the minimum quality standard from the 30th to the 40th percentile until the CY 2024 performance year.
Performance Year Web Interface Option APP Measure Option
2022 ACO meets all data reporting and submission requirements and achieves quality performance score at or above 30
thpercentile of
all MIPS quality category scores.
ACO meets all APP data reporting requirements and achieves a quality performance score on at least one APP measure that is at or above the 30
thpercentile benchmark score for
the measure.
2023 Same as 2022 Same as 2022
2024 Not available ACO meets all APP data reporting requirements and achieves a quality performance score at or above the 40
thpercentile of all MIPS quality
category scores.
55
56
8/25/2021
29
MSSP: Beneficiary Attribution
CALIFORNIA HOSPITAL ASSOCIATION 57
CMS proposes adding the following additional codes to the definition of primary care services for Performance Year 2022:
• Chronic care management code 99X21*.
• Principal care management codes 99X22, 99X23, 99X24 and 99X25*.
• Prolonged office or other E/M service HCPCS code G2212.
• Communication Technology-Based Service (CTBS) HCPCS code G2252 (for a prolonged virtual check-in that can be provided via audio-only connection)*.
CMS also proposes to continue allowing telephone E/M codes (99441 through 99443) to be used for beneficiary assignment until they are no longer be payable under Medicare telehealth policies.
* If CPT/HCPCS codes in question are finalized through this rule as proposed.
MSSP: Reduced Repayment Mechanism
CALIFORNIA HOSPITAL ASSOCIATION 58
CMS believes repayment mechanisms are larger than necessary and makes the following proposals to reduce them.
• Changing the methodology used to calculate the repayment mechanism amount, lowering the required amount.
• Changing the methodology to more clearly specify the assigned population used as a multiplier in annually recalculating the repayment mechanism amount.
• Allowing ACOs already in two-sided participation agreements a one-time opportunity to decrease the amount of their repayment mechanism.
57
58
8/25/2021
30
MSSP: Reduced Application Burden
CALIFORNIA HOSPITAL ASSOCIATION 59
CMS proposes to modify three provisions of its application requirements.
• Instead of being mandatory, CMS proposes that prior participation disclosure requirements are required only at the request of the agency during the application process.
• CMS proposes removing provisions requiring an ACO to submit sample ACO participant agreements during the application process.
• CMS proposes removing provisions requiring an ACO to submit an executed agreement for each ACO participant at the time of its initial application or participation agreement renewal process.
MSSP: Benchmark Request for Information (RFI)
CALIFORNIA HOSPITAL ASSOCIATION 60
Stakeholders have expressed concerns that the MSSP benchmarking methodology penalizes efficient ACOs. The proposed rule discusses ideas to respond to those concerns and requests feedback.
• CMS describes an approach to benchmarking per-capita risk-adjusted regional fee-for-service (FFS) expenditures for all assignable beneficiaries in an ACO’s regional service area (a) as a weighted average of the FFS expenditures for the ACO’s assigned beneficiaries (b) and the assignable beneficiaries in the region who are not actually assigned to the ACO (c).
• A simulation of this approach found that the average increase in the updated benchmark by quintile ranged from 0.1% to 1.4%, although some ACOs saw decreases in their benchmarking amounts.
59
60
8/25/2021
31
MSSP: Benchmark RFI (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 61
CMS seeks comment on several issues related to the use of regional FFS expenditures in benchmarks, including:
• CMS’ approach or alternative approaches to calculating regional FFS expenditures without including an ACO’s assigned beneficiaries.
• Whether market penetration should be considered in benchmark calculations and what constitutes heavy penetration in the ACO’s regional service area.
• Possible unintended consequences that could result from removing an individual ACO’s assigned beneficiaries from regional calculations.
• Whether removal of an ACO’s assigned beneficiaries from regional FFS calculations brings about a need to remove ACO assigned beneficiaries from other MSSP financial calculations.
• Other approaches to calculating benchmarks that would reduce the influence of an ACO’s assigned beneficiaries on regional expenditure calculations.
MSSP: Risk Adjustment RFI
CALIFORNIA HOSPITAL ASSOCIATION 62
CMS also requests comment on issues related to its risk adjustment methodology, including:
• Approaches to improving the risk adjustment methodology and specifically for ACOs with medically-complex, high-cost beneficiaries.
• Approaches to risk adjustment that would balance the need for accurate and complete coding, while protecting against incentivizing coding intensity initiatives by ACO participants and ACO providers/suppliers.
• Alternate approaches that would increase the cap on an ACO’s risk score growth in relation to risk score growth in the ACO’s regional service area.
• Potential interactions between policies to remove assigned beneficiaries from the assignable beneficiary population used to calculate regional FFS expenditures and growth rates and policies addressing regional risk score growth.
61
62
8/25/2021
32
Medicare Telehealth Services
CALIFORNIA HOSPITAL ASSOCIATION 63
• In CY 2021, CMS finalized a new “Category 3” list of Medicare telehealth services to describe services added temporarily during the COVID-19 PHE for which there is clinical benefit when furnished via telehealth, but for which there is not yet sufficient evidence to consider the services as permanent additions under Category 1 or Category 2 criteria.
• CMS proposes to retain all services added to the Medicare telehealth services list on a Category 3 basis until the end of CY 2023.
• CMS also seeks comment on whether any of the services added to the Medicare telehealth list for coverage and payment during the PHE that were not extended on a temporary Category 3 basis in the CY 2021 PFS final rule should now be added to the Medicare telehealth list under Category 3.
✓ These services are identified in Table 11 of the proposed rule.
Medicare Telehealth Services – Table 11 Services
CALIFORNIA HOSPITAL ASSOCIATION 64
63
64
8/25/2021
33
Medicare Telehealth – Mental Health Services
CALIFORNIA HOSPITAL ASSOCIATION 65
• The Consolidated Appropriations Act (CAA) waived the Medicare geographic restrictions and added the patient’s home as a permissible originating site for telehealth services furnished for the purpose of diagnosis, evaluation or treatment of a mental health disorder, effective for services furnished on or after the end of the COVID-19 PHE.
• CMS proposes to require providers conduct an in-person, non-telehealth service within six months prior to initial mental health telehealth service, and at least once every six months thereafter.
✓ CMS seeks comment on whether the required in-person, non-telehealth service could be furnished by another physician or practitioner of the same specialty and same subspecialty within the same group as the physician or practitioner who furnishes the telehealth service.
• CMS proposes to revise its regulatory definition of “interactive. telecommunications system” to permit the use of audio-only communications technology for mental health services under certain conditions when provided to beneficiaries located in their home.
Medicare Telehealth Services and Other Communications Technology-Based Services
CALIFORNIA HOSPITAL ASSOCIATION 66
• Direct Supervision: During the COVID-19 PHE, CMS allowed providers to satisfy “direct supervision” requirements for diagnostic tests, physicians’ services and some hospital outpatient services through virtual presence, using real-time audio/video technology, and finalized this policy through the later of the end of the calendar year in which the PHE ends or Dec. 31, 2021. CMS seeks comment on whether it should make this flexibility permanent or if it should temporarily continue it beyond the current timeframe.
• Extended Virtual Check-in: CMS proposes to permanently adopt coding and payment for HCPCS code G2252, extended virtual check-in provided using any form of synchronous communication technology, including audio-only communication.
• Remote Therapeutic Monitoring (RTM): CMS provides several clarifications on RTM services, including that it believes RTM codes are “incident to” services and therefore cannot be billed independently by physical therapists and other practitioners who are not physicians or NPPs.
65
66
8/25/2021
34
Appropriate Use Criteria (AUC) for Advanced Diagnostic Imaging Services
CALIFORNIA HOSPITAL ASSOCIATION 67
• The Protecting Access to Medicare Act (PAMA) of 2014 required CMS to create a program promoting use of AUC for advanced diagnostic imaging.
• Restricts payment to furnishing professional for claims that indicate that ordering professional consulted with qualified a clinical decision support mechanism (CDSM).
• Applies only in “applicable settings”: Hospital outpatient departments, physician offices, ambulatory surgical centers, and independent diagnostic testing facilities.
✓ Outpatient department of a critical access hospital is not an applicable setting.
• The AUC program has operated under an “educational and testing” period since Jan. 1, 2020.
✓ In response to the COVID-19 PHE, CMS extended the educational and operational testing period through 2021.
AUC for Advanced Diagnostic Imaging Services (cont.)
CALIFORNIA HOSPITAL ASSOCIATION 68
• CMS proposes to delay the payment penalty phase of the AUC program to Jan. 1, 2023 — or the first of the January that follows the end of the PHE —whichever is later.
✓ CMS clarifies that stakeholders may continue to attest to a significant hardship under the AUC program due to extreme and uncontrollable circumstances related to the PHE and that such an attestation may be used as needed throughout the PHE.
• CMS proposes and seeks comment on several additional policies related to implementation of the AUC payment penalty phase.
✓ Modified orders
✓ Claims processing edits and modifiers
✓ Denial vs return of claims that fail AUC processing edits
67
68
8/25/2021
35
Additional PFS COVID-19 PHE Related Policies
CALIFORNIA HOSPITAL ASSOCIATION 69
• Clinical Lab Fee Schedule: Lab Specimen Collection and Travel Allowance
✓ During COVID-19 PHE, CMS established a revised policy to pay independent labs for specimen collection for COVID-19 testing at an increased rate of $23-$25 (from the current rate of $3-$5).
✓ CMS expects this policy to end with the PHE but seeks comment on considerations for specimen collection for COVID testing beyond the PHE.
• Expansion of Coverage for Pulmonary Rehabilitation
✓ CMS proposes to expand coverage of outpatient pulmonary rehab services to beneficiaries with “severe manifestations” of COVID-19.
o CMS proposes to define “severe manifestations” as patients requiring hospitalization in the ICU or otherwise who experience continuing symptomatology, including respiratory dysfunction, for at least 4 weeks post discharge.
Quality Payment Program
CALIFORNIA HOSPITAL ASSOCIATION 70
• CMS proposes several changes to Merit-based Incentive Payment System (MIPS) thresholds and categories:✓ Performance threshold
✓ Quality data completeness threshold
✓ Removal of 3-point floor for certain measures
✓ Five new episode-based cost measures
✓ Updated Improvement Activities inventory
✓ Changes to complex patient bonus
✓ Changes to Promoting Interoperability program generally aligned with hospital program
• CMS proposes to implement 7 voluntary MIPS Value Pathways beginning CY 2023:✓ Rheumatology, stroke care and prevention, heart disease, chronic disease management,
lower extremity joint repair, emergency medicine, anesthesia.
✓ Organizes each MIPS category’s reporting requirements around particular treatments, specialties or other priorities.
Additional information available in CMS Fact Sheet
69
70

8/25/2021
36
Questions
CALIFORNIA HOSPITAL ASSOCIATION 71
Closing Comments and Next Steps
72
71
72

8/25/2021
37
Contact
73
Please contact us if you have questions we were not able to address today.
Chad MulvanyVP, Federal Policy(202) [email protected]
Megan HowardVP, Federal Policy(202) [email protected]
Thank You
CALIFORNIA HOSPITAL ASSOCIATION 74
Thank you for participating in today’s webinar.
A recording of the program will be sent to each attendee within two weeks.
For education questions, contact:
73
74