update on agents for type 2...
TRANSCRIPT

Update on Agents for Type 2 Diabetes
This presentation will:
• Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific concerns, adverse drug reactions, and contraindications
• Discuss the role and timing of combination therapy in achieving A1C goals
• Explain the implications of recent, large randomized clinical trials on clinical decision-making

Estimated Prevalence and Costs of Diabetes in the U.S., 2002-2012
Medical expenditures for people with DM are 2.3 times higher than those without DM
The primary driver of increased cost is the increasing prevalence of DM
Despite the introduction of new classes of medications for DM treatment, anti-diabetic agents and supplies only account for 12% of medical expenditures
Number of People with Diagnosed Diabetes, Millions
Estimated Cost of Diabetes Care,Billions, US Dollars
DM = diabetes mellitus.
American Diabetes Association. Diabetes Care, 2014.

AACE Diabetes Algorithm• Guide therapy based on A1C level
– Focus on lifestyle intensification at all levels
• Important tenets:– Target A1C is <6.5%
• Based on associated lower risk of micro- and macrovascular complications
• Recommend monitoring A1C quarterly, along with fasting and postprandial blood glucose, with intensification of therapy until goal A1C is achieved
• Individualize A1C target based on comorbidities
• Patient should monitor fasting and postprandial blood glucose levels
– Use agents with maximal efficacy, associated with lowest risk of hypoglycemia
• Sulfonylureas are therefore much lower in algorithm
• Earlier use of incretin mimetics and DPP-4 inhibitors to stimulate insulin secretion without hypoglycemia
AACE Comprehensive Diabetes Management Algorithm 2013. Endocr Pract. 2017,doi:10.4158/EP161682.CS.
A1C = glycated hemoglobin; DPP-4 = dipeptidyl-peptidase 4

Approach to Management of Hyperglycemia
ADA. V. Diabetes Care. Diabetes Care. 2014;37(suppl 1):S25. Figure 1.
Adapted with permission from Ismail-Beigi F, et al. Ann Intern Med 2011;154:554-559

Main Pathophysiological Defects in T2DM “The Ominous Octet”
Islet b-cell
Impaired
insulin secretion
Neurotransmitter
dysfunction
Decreased glucose
uptake
Islet a-cell
Increased
glucagon secretion
Increasedlipolysis
Increased glucose
reabsorption
Increased
hepatic
glucose
production
Decreasedincretin effect
Defronzo RA. Diabetes. 2009 Apr;58(4):773-95.

Current Antihyperglycemic Medications
Sulfonylureas
Generalized insulin
secretagogue
12 groups with different mechanisms of action
a-Glucosidaseinhibitors
Delay CHO absorption
Biguanide
Reduces hepaticinsulin
resistance
TZDs
Reduce peripheral insulin
resistance
Amylin analog
Suppressesglucagon
GLP-1 analogs
Stimulate beta-cellsSuppress glucagon
Colesevelam
Bile acid sequestrant
Bromocriptine
Hypothalamicpituitary reset
Insulinreplacement
therapy
SGLT-2 inhibitors
Block renal glucose
reabsorption
Glinides
Restore postprandial
insulin patterns
DPP-4 inhibitors
RestoreGLP-1 Levels
CHO = carbohydrate; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2 = sodium-dependent glucose cotransporters-2; TZD = thiazolidinedione.


Algorithm to Achieve Glycemic GoalsBaseline A1C 6.5% - 7.5%
• Monotherapy may be effective in this range– Metformin first choice for monotherapy if no
contraindications
– Consider DPP-4 if PP and FPG, GLP-1 if PP, TZD if metabolic syndrome or NAFLD, AGI if PP
– Do not recommend secretagogue (SU or glinide) in this range due to risk of hypoglycemia; short-lived effect
• If monotherapy is unsuccessful, move on to dual oral rx; often need to augment reduction in PP BG to get to goal in this A1C range
DPP-4 = dipeptidyl peptidase-4; PP = post-prandial; FPG = fasting plasma glucose; GLP-1 = glucagon-like peptide-1; TZD = thiazolidinedione; NAFLD = non-alcoholic fatty liver disease; AGI = alpha-glucosidase inhibitor; SU = sulfonylurea; A1C = glycated hemoglobin; SGLT-2 = sodium glucose transport-2
AACE Comprehensive Diabetes Management Algorithm 2017. Endocr Pract. 2017,doi:10.4158/EP161682.CS.
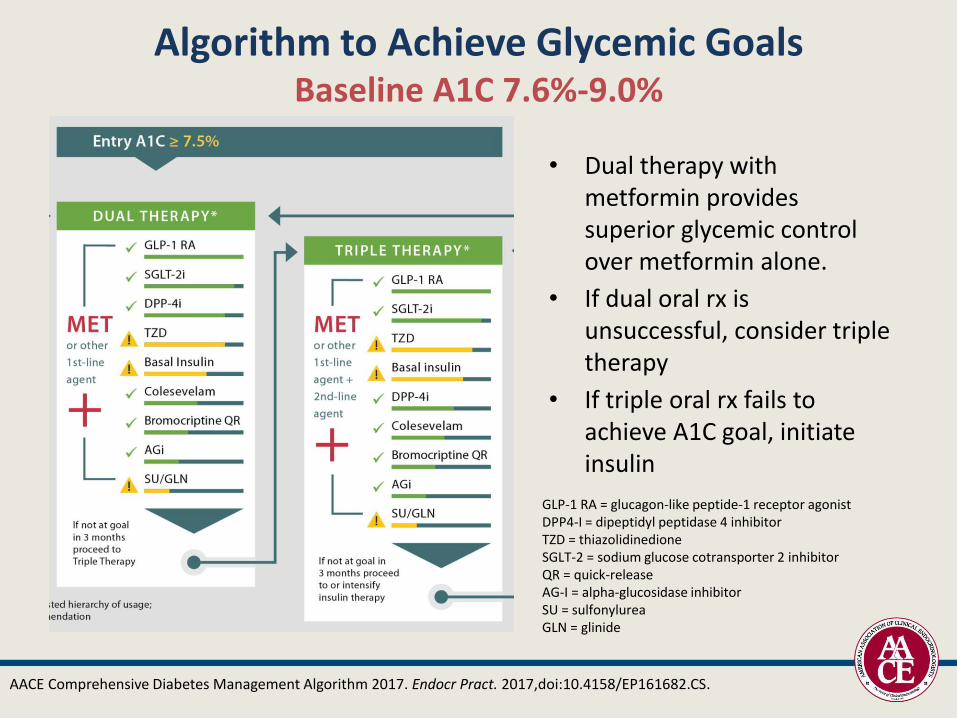
Algorithm to Achieve Glycemic Goals Baseline A1C 7.6%-9.0%
• Dual therapy with metformin provides superior glycemic control over metformin alone.
• If dual oral rx is unsuccessful, consider triple therapy
• If triple oral rx fails to achieve A1C goal, initiate insulin
AACE Comprehensive Diabetes Management Algorithm 2017. Endocr Pract. 2017,doi:10.4158/EP161682.CS.
GLP-1 RA = glucagon-like peptide-1 receptor agonistDPP4-I = dipeptidyl peptidase 4 inhibitorTZD = thiazolidinedioneSGLT-2 = sodium glucose cotransporter 2 inhibitorQR = quick-releaseAG-I = alpha-glucosidase inhibitorSU = sulfonylureaGLN = glinide

If patient is asymptomatic with recent onset of disease and drug naïve, may consider starting with dual or triple oral regimens
Once A1C has improved to <7.5%, consider initiation of dual oral therapy with tapering
and possible discontinuation of insulin rx
If symptomatic, start insulin
Algorithm to Achieve Glycemic Goals Baseline A1C >9.0%
AACE Comprehensive Diabetes Management Algorithm 2017. Endocr Pract. 2017,doi:10.4158/EP161682.CS.

Targeted Sites of Action ofOral Anti-Hyperglycemic Drug Classes
DPP = dipeptidyl peptidase; SGLT-2 = Sodium-glucose co-transporter 2; TZD = thiazolidinediones
.Fonseca V. Clin Ther. 2014;36:477-484. Sonne DP. Eur J Endocrinol. 2014. Inzucchi S, et al. Diabetes Care. 2012;35:1364–1379; Diabetologia. 2012;55:1577–1596.
Liver Skeletal Muscle Pancreas Gut Fat Kidney Brain
• Biguanides
• TZDs
• DPP-IV
inhibitors
• Sulfonylureas
• TZDs
• Insulin
• DPP-IV
Inhibitors
• Sulfonylureas
• Glinides
• TZDs
• Amylin
• α-Glucosidase
inhibitors
• Biguanides
• Colesevelam
• GLP-1 RA
• TZDs • SGLT-2
inhibitors
• Bromocriptine
Glucose
production
Glucose
uptake
Insulin
release
Glucose
absorption
Insulin
sensitivity
Glucose
reabsorption
Glucose
production

Clinical Considerations
• Combining therapeutic agents with different modes of action may be advantageous
• In many if not most patients (unless contraindicated or intolerance has been demonstrated), use metformin, which increases insulin sensitivity, and/or insulin sensitizers such as TZDs, as part of the therapeutic regimen
• Dosage of secretagogues or insulin should be adjusted as blood glucose levels decline when used in combination with metformin, TZD, DPP-4 inhibitors, and/or incretin mimetics (GLP-1 agonists)
AACE Comprehensive Diabetes Management Algorithm 2013. Endocr Pract. 2013;19(3):536-557.
Sitagliptin [package insert]. Whitehouse Station, NJ; Merck Co. Inc.; 2010. Saxagliptin [package insert]. Princeton, NJ; Bristol Meyers Squibb;
2009; Linagliptin [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals. 2011.
TZD = thiazolidinediones; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1

• The weight gain associated with thiazolidinediones in some patients may be partly offset by combination therapy with metformin
• If A1C is elevated and preprandial blood glucose measurements are at target levels, carefully assess postprandial glucose levels
• Individualize treatment regimens!
AACE Comprehensive Diabetes Management Algorithm 2013. Endocr Pract. 2013;19(3):536-557;
Clinical Considerations

Effect of Glucose-lowering Drugs on Patient Weight
1. Malone M. Ann Pharmacother. 2005;39:2046-2055. 2. Glipizide [package insert]. New York, NY; Pfizer; 2006. 3. Pioglitazone [package insert]. Deerfield, IL: Takeda Pharmaceuticals America; 2007. 4. Rosiglitazone [package insert]. Research Triangle Park, NC; GlaxoSmithKline; 2007. 5. Nathan DM, et al. Diabetes Care. 2008;31(1):173-175. 6. Holman RR. NEJM. 2007;357(17):1716-1730. 7. Metformin[package insert]. Princeton NJ; Bristol Meyers Squibb; 2009. 8. Sitagliptin [package insert]. Whitehouse Station, NJ; Merck and Co.; 2009. 9. Drucker DJ, et al. J Clin Invest.2007;117(1):24-32. 10. Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ
SGLT-2 Inhibitors10
Therapeutic Options
GLP-1 receptor agonist9
Insulin5,6
DPP-4 inhibitor8
TZD3,4
Sulfonylurea1,2
Weight
Metformin7
A1C = glycated hemoglobin; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2 = sodium glucose co-transporter-2; TZD = thiazolidinedione

Risk of Hypoglycemia
• Plays a significant role in choice of agents in AACE algorithm
• For patients at highest risk of hypoglycemia, may consider close evaluation of agents chosen as well as therapeutic goal
• Patients with type 2 diabetes at highest risk of low blood glucose include those with:– Diabetes duration >15 years
– Advanced macrovascular disease
– Hypoglycemia unawareness
– Limited life expectancy
– Severe comorbidities
AACE Comprehensive Diabetes Management Algorithm 2013. Endocr Pract. 2013;19(3):536-557;AACE Algorithm for Glycemic Control, Endocr Pract. 2009;15(6):540-59.

Mechanism Insulin sensitivity Hepatic glucose production FPG more than PPG
Efficacy A1C 1%-2%
AdvantagesNo weight gain or hypoglycemia, potential weight loss
DisadvantagesGI side effectsLactic acidosis (rare)
Contraindications Renal disease; CHF
Combinations available with SU, TZD, repaglinide, and DPP-4 inhibitors
BiguanidesMetformin
Metformin [package insert]. Princeton NJ; Bristol Myers Squibb; 2009.
A1C = glycated hemoglobin; CHF = congestive heart failure; DPP-4 = dipeptidyl peptidase-4; FPG = fasting plasma glucose; GI = gastrointestinal; PPG = post-prandial glucose; SU = sulfonylurea; TZD = thiazolidinedione

Sulfonylureas and GlinidesGlipizide, Glimepiride, Glyburide
Repaglinide, Nateglinide
Mechanism
Insulin secretion FPG PPG
Efficacy Moderate
Advantages Strong short term efficacy
DisadvantagesWeight gain, hypoglycemia, tend to lose efficacy after several years
ContraindicationsAvoid in severe hepatic and renal impairment
Combinations available with metformin, TZD
Glyburide [package insert]. New York, NY; Pfizer; 2010. Glipizide [package insert]. New York, NY; Pfizer; 2010. Glimepiride [package insert]. Scoppito, Italy; Aventis Pharma S.p.A; 2001. Kahn SE, et al. NEJM. 2006;355:23.
FPG = fasting plasma glucose; PPG = post-prandial glucose; TZD = thiazolidinedione

Higher Mortality Is Associated with Greater Exposure to Sulfonylureas
Simpson SH, et al. CMAJ. 2006;174:169-174.
A retrospective, inception cohort study conducted in 5795 new users of oral glucose-lowering medications
- Insulin or combination therapy were excluded
- Mean age: 66.3 years
- Mean follow-up: 4.6 years
- Main outcomes: all-cause mortality, death fromacute ischemic event
There was a greater risk of death associated with higher daily doses and better adherence for patients who used glyburide (HR = 1.3; 95% CI, 1.2-1.4),
but not metformin (HR = 0.8; 95% CI, 0.7-1.1)
0 1 2
Glyburide(n = 4138)
Metformin(n = 1537)
1.321.291.29
0.920.960.84
41.5 (37.6)
53.4 (70.2)
Daily Dose
Hazard ratio
Monotherapygroup
Deaths/1000 person-years
Lower (higher)
0 1 2
Glyburide(n = 4138)
Metformin(n = 1537)
1.551.341.33
1.101.090.98
49.0 (75.8)
37.7 (41.3)
Poor (good)
Adherence
Hazard ratio
Monotherapygroup
Deaths/1000 person-years
UnadjustedAdjusted for age, sex, chronic disease score (CDS), and nitrate useAdjusted for age, sex, CDS, nitrate use, physician visits, and hospital admissions

Thiazolidinediones
Mechanism Insulin sensitivity, especially at muscle, lowers both FPG and PPG, but effect may be delayed
Efficacy Moderate ( A1C 1.0%-1.5%)
Advantages No hypoglycemia, no reliance on renal excretion
Disadvantages
Fluid retention, edema, heart failure, weight gain, slow onset of action, bone fractures, macular edema, osteoporosis, anemia, and bladder cancer
ContraindicationsClass III or IV CHF or hepatic impairment w/ALT >2.5 times upper normal limits
Combinations available with metformin and sulfonylurea
Pioglitazone, Rosiglitazone
Pioglitazone [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, 2011.Rosiglitazone Prescribing Information. Research Triangle Park, NC: GlaxoSmithKline, 2013.
A1C = glycated hemoglobin; ALT = alanine aminotransferase; CHF = congestive heart failure; FPG = fasting plasma glucose; PPG = postprandial plasma glucose.

Alpha-Glucosidase InhibitorsAcarbose, Miglitol
Mechanism Rate of gut polysaccharide breakdown, thereby slowing absorption
Efficacy Modest ( A1C 0.5%-1.0%), PPG lowering
AdvantagesWeight-neutral, non-systemic drug, targets post-prandial glucose
DisadvantagesBloating, flatulence, diarrhea – w/slow titration, frequent dosing
ContraindicationsSevere renal impairment, diabetic ketoacidosis, malabsorption, obstruction, inflammatory bowel, or conditions aggravated by gas production
Combinations available with sulfonylureas
Acarbose [package insert]. Wayne, NJ; Bayer HealthCare Pharmaceuticals Inc.; 2009. Miglitol [package insert]. Wayne, NJ; Bayer HealthCare Pharmaceuticals Inc.; 2010.
A1C = glycated hemoglobin; PPG = post-prandial glucose

Dopamine Receptor AgonistBromocriptine QR
Cincotta et al. Taylor and Francis, Eds Hansen, B Shafrir, E London, 2002. 271-312. Defronzo RA et al. Diabetes Care. 2011 Apr;34(4):789-94.
MechanismExact mechanism of action unclear, believed to reduce sympathetic tone, inflammation, and insulin resistance
Efficacy Modest ( A1C 0.5%)
AdvantagesMay decrease cardiovascular risk
DisadvantagesHypotension, syncope, hypoglycemia, nausea
ContraindicationsHistory of psychosis or during breastfeeding.Use caution with renal or hepatic impairment.
A1C = glycated hemoglobin; QR = quick-release

Bile Acid SequestrantsColesevelam
Bays HE, et al. Arch Intern Med. 2008;168:1975-83. Fonseca VA, et al. Diabetes Care. 2008; 31:1479-1484. Fonseca V, et al. Diabetes ObesMetab. 2010;12(5);384-392. Goldberg RB, et al. Arch Intern Med. 2008;168:1531-1540; Colesevelam [package insert]. Parsippany, NJ; Daiichi Sankyo, 2011.
Mechanism
Raises cholecystokinin, which slows gastric emptying and post-prandial glucoseExact mechanism unknown, may be mediated via TGR5, and/or farnesoid X receptor (FXR/bile acid receptor) effects on intestinal glucose
Efficacy Modest ( A1C 0.5%)
Advantages
LDL-C (also FDA approved for LDL-C reduction)weight neutral, no hypoglycemia, can complement statin treatment in lowering LDL and cardiac event risk
Disadvantages Constipation, nausea, dyspepsia, myalgia, pharyngitis, triglycerides, drug interactions
ContraindicationsHistory of bowel obstruction, TGs >500 mg/dL; history of hypertriglyceridemia-induced pancreatitis
A1C = glycated hemoglobin; LDL-C = low-density lipoprotein cholesterol; TG = triglyceride

GLP-1 Modulates Numerous Functions in
Humans
GLP-1: Secreted upon
the ingestion of food
Beta-cells:Enhances glucose-dependent
insulin secretion
Brain promotes satiety and
reduces appetite
Data from Flint A, et al. J Clin Invest. 1998;101:515-520; Data from Larsson H, et al. Acta Physiol Scand. 1997;160:413-422
Data from Nauck MA, et al. Diabetologia. 1996;39:1546-1553; Data from Drucker DJ. Diabetes. 1998;47:159-169
Stomach:Helps regulate gastric
emptying
Liver:
Glucagon reduces
hepatic glucose output
Alpha cells: Glucose-dependent
postprandial
glucagon secretion
GLP-1 = glucagon-like peptide-1.

Characteristics of GLP-1 AgonistsExenatide, Liraglutide, Albiglutide, Dulaglutide
Mechanism Mimic prolonged action of GLP-1
Efficacy
Decrease A1C levels 0.5%–2.0%
(depends on entry of glucose into bloodstream from gut)
Dosing Once- or twice-daily injection, weekly *
Side effects Nausea, vomiting, weight loss
Main riskC-cell thyroid tumors**, long-term safety
unknown
Associated with Pancreatitis possible
Nathan DM, et al. Diabetes Care. 2008;31:173-175; Drucker DJ, et al. Lancet. 2006;368:1696- 1705.
Exenatide [package insert]. San Diego, CA; Amylin Pharmaceuticals; 2010.; Tanzeum (albiglutide) [prescribing information].
*Dosing depends on GLP-1 agonist
**With liraglutide, in rodents only
A1C = glycated hemoglobin; GLP-1 = glucagon-like peptide-1.
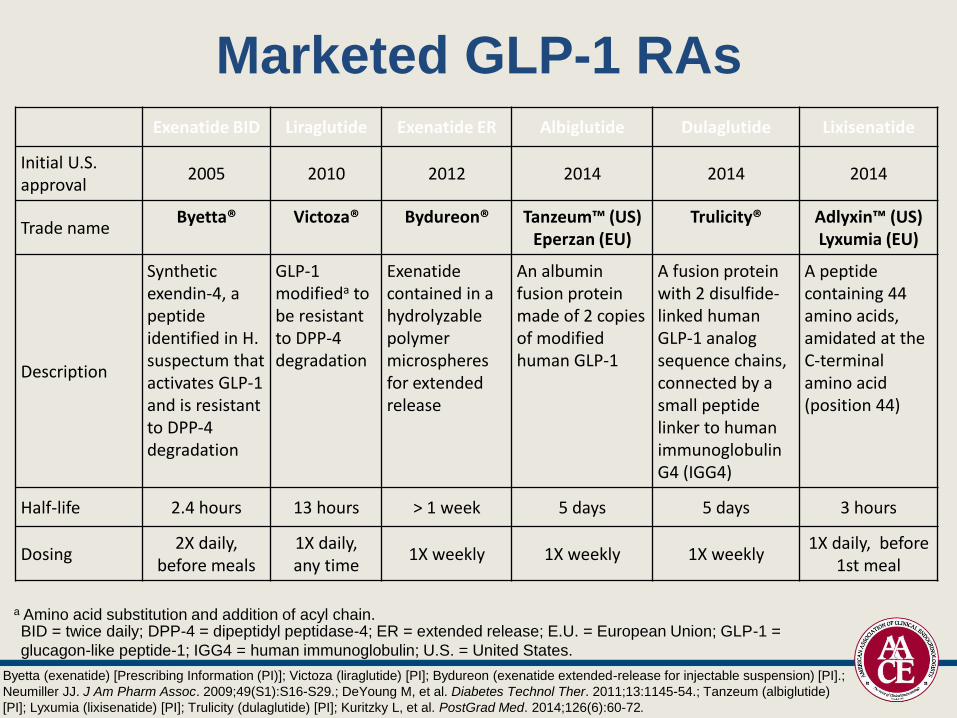
Marketed GLP-1 RAsExenatide BID Liraglutide Exenatide ER Albiglutide Dulaglutide Lixisenatide
Initial U.S. approval
2005 2010 2012 2014 2014 2014
Trade nameByetta® Victoza® Bydureon® Tanzeum™ (US)
Eperzan (EU)Trulicity® Adlyxin™ (US)
Lyxumia (EU)
Description
Synthetic exendin-4, a peptide identified in H. suspectum that activates GLP-1 and is resistant to DPP-4 degradation
GLP-1 modifieda to be resistant to DPP-4 degradation
Exenatide contained in a hydrolyzable polymer microspheres for extended release
An albumin fusion protein made of 2 copies of modified human GLP-1
A fusion protein with 2 disulfide-linked human GLP-1 analog sequence chains, connected by a small peptide linker to human immunoglobulin G4 (IGG4)
A peptide containing 44 amino acids, amidated at the C-terminal amino acid (position 44)
Half-life 2.4 hours 13 hours > 1 week 5 days 5 days 3 hours
Dosing2X daily,
before meals1X daily, any time
1X weekly 1X weekly 1X weekly1X daily, before
1st meal
a Amino acid substitution and addition of acyl chain.
Byetta (exenatide) [Prescribing Information (PI)]; Victoza (liraglutide) [PI]; Bydureon (exenatide extended-release for injectable suspension) [PI].;
Neumiller JJ. J Am Pharm Assoc. 2009;49(S1):S16-S29.; DeYoung M, et al. Diabetes Technol Ther. 2011;13:1145-54.; Tanzeum (albiglutide)
[PI]; Lyxumia (lixisenatide) [PI]; Trulicity (dulaglutide) [PI]; Kuritzky L, et al. PostGrad Med. 2014;126(6):60-72.
BID = twice daily; DPP-4 = dipeptidyl peptidase-4; ER = extended release; E.U. = European Union; GLP-1 =
glucagon-like peptide-1; IGG4 = human immunoglobulin; U.S. = United States.

GLP-1 Devices
• All GLP-1 RAs are available in pre-filled pens1
– Weekly GLP-1 RAs (exenatide ER, albiglutide, and dulaglutide) are available in single-dose pens
– Weekly GLP-1 RAs (exenatide BID, liraglutide, and lixisenatide) are available in multi-dose pens
• Various studies have examined patient preferences– Lixisenatide and liraglutide pens have higher patient satisfaction
compared to exenatide2
– Dulaglutide is the only weekly GLP-1 RA available in a ready-to-use formula that does not require reconstitution3
• New technology is being developed for an implantable, continuous subcutaneous delivery system for GLP-1 RAs4
1. MIMS. Diabetes Visual Guide. 2016. 2. Stauder U, et al. J Diabetes Sci Technol. 2014 Jan; 8(1): 123–131. 3. Amblee
A. Patient Prefer Adherence. 2016;10:975-82. 4. Diabetes in Control. Intarcia Platform Technology. 2015.
BID = twice daily; ER = extended release; GLP-1 = glucagon-like peptide-1 ; GLP-1 RA = glucagon-like peptide-1 receptor agonist.

Exenatide (Exendin-4)
– Synthetic version of salivary
protein found in the Gila
monster
– Approximately 50% identity
with human GLP-1
• Binds to known human
GLP-1 receptors on β cells
in vitro
• Resistant to DPP-4
inactivation
– Administered twice daily
Development of Exenatide: An Incretin Mimetic
Nielsen LL, et al. Regul Pept. 2004;117:77-88.
Fineman MS, et al. Diabetes Care. 2003;26:2370-2377.
DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1.

Liraglutide
• Injected SC once-daily
• Acylated GLP-1(C-16 fatty acid, palmitic acid, on position 26)
• Liraglutide is extensively bound to plasma protein (greater than 98%)
• 97% homology to GLP-1
• Endogenously metabolized without specific organ as major route of elimination
Victoza® [package insert]. Plainsboro, NJ: Novo Nordisk; 2016.
GLP-1 = glucagon-like peptide-1; SC = subcutaneously.

Albiglutide
• 30 mg SC QWK
• Increase to 50 mg SC QWK if needed
• Supplied as single-dose prefilled pen
Tanzeum® [package insert]. Wilmington, DE: GlaxoSmithKline LLC; 2016.
QWK = every week ; SC = subcutaneously.

Dulaglutide
• 0.75 mg SC QWK
• Increase to 1.5 mg SC QWK if needed
• Supplied as single-dose prefilled pen or prefilled syringe
Trulicity® [package insert]. Indianapolis, IN: Eli Lilly and Co.; 2015.
QWK = every week; SC = subcutaneously.

Nausea Declined Over Time with Liraglutide Monotherapy
Patients
(%)
0.
3.5
7.
10.5
14.
17.5
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Time (weeks)
Liraglutide 1.2 mg (n=251)
Liraglutide 1.8 mg (n=246)
Glimepiride 8 mg (n=248)Liraglutide Monotherapy vs SU
Liraglutide [package insert]. Princeton, NJ: Novo Nordisk Inc. 2010;
Garber A et al. Lancet. 2009;373:473-481.
SU = sulfonylurea.
Safety: Medullary Thyroid Cancer Risk
• All GLP-1 RAs are contraindicated in patients with a personal or family history of MTC or MEN2 because of the occurrence of c-cell tumors in rodents.
• The c-cell tumor risk in humans is unknown, because human relevance could not be determined in clinical trials.
• The value of routine calcitonin and/or ultrasound monitoring is uncertain.
• Patients with thyroid nodules or elevated serum calcitonin levels identified for other reasons should be sent to an endocrinologist.
• To monitor potential associations, report MTC to state cancer registry, regardless of treatment.
Victoza® PI 2013.; Bydureon® PI 2013.
Parks M, et al. N Eng J Med. 2010;362:774-777.
GLP-1 RA = glucagon-like peptide-1 receptor agonist; MEN2 = multiple endocrine neoplasia 2; MTC
= medullary thyroid cancer.

Safety: Renal Impairment
• Renal impairment affects the clearance of exenatide BID & ER, but not that of liraglutide, albiglutide or dulaglutide.
• Hypovolemia due to nausea and vomiting may worsen renal function.
• Renal impairment with GLP-1 RAs has been reported postmarketing, usually in association with nausea, vomiting, diarrhea, or dehydration.
Linnebjerg H, et al. Br J Clin Pharmacol. 2007;64:317-327.
Jacobsen L, et al. Br J Clin Parmacol. 2009;68:898-905.; Byetta® PI 2013.
BID = twice daily; ER = extended release; GLP-1 RA = glucagon-like peptide-1 receptor agonist.

Safety: Pancreatitis
• Pancreatitis has been reported with all incretin-based therapies, although no causal relationship has been established.
• Patients should know signs and symptoms of pancreatitis and stop taking incretin-based therapies if signs and symptoms occur.
• If pancreatitis is confirmed, therapy should not be restarted.
Ahmad SR, et al. N Engl J Med. 2008;358:1970-1971.; Garg R, et al. Diabetes Care. 2010;33:2349-2354.; Byetta® PI
2013.; Victoza® PI 2013.; Bydureon® PI 2013.; Januvia® PI 2013.; Onglyza® PI 2013.; Tradjenta® PI 2013.; Nesina® PI
2013.

DPP-4
Active GLP-1
Inactive GLP-1
Active GIP
Inactive GIP
• Increased insulin secretion
• Decreased glucagon release
Glucose control improved
DPP-4 inhibitor
Inhibition of DPP-4 Increases Active IncretinLevels, Enhancing Downstream Incretin Actions
Umpierrez et al. Endocrine Practice 2014

Characteristics of DPP-4 InhibitorsAlogliptin, Linagliptin, Saxagliptin, Sitagliptin
MechanismInhibit enzymatic degradation of GLP-1 and GIP; glucose-dependent
Efficacy Decrease A1C levels 0.6%–0.9%
Dosing Once daily
Side effects Headaches, nasopharyngitis
Main risk Viral infection; long-term safety unknown
Rosenstock J, et al. Curr Opin Endocrinol Diabetes Obes. 2007;14:98-107. Nathan DM, et al. Diabetes Care. 2008;31:173-175.
A1C = glycated hemoglobin; GIP = gastric inhibitory polypeptide; GLP-1 = glucagon-like peptide-1

Placebo-corrected Change From Baseline In A1C: Monotherapy
Comparative Efficacies of DPP-4s
-0.1
-0.3
-0.2
-0.4
-0.8
-0.5
-0.6
-0.7
-0.9
-1.0
-1.1
-1.2
ΔH
bA
1C
(%
)
Alogliptin1
12.5mg 25mg
7.9% 7.9%
Linagliptin2
5mg 5mg
8.1% 8.0%
Saxagliptin2
5mg 5mg
7-10% 8.0%
Sitagliptin2
100mg 100mg
8.0% 8.0%
Vildagliptin3
50mg BID 50mg
8.6% 8.4%
The current DPP-4s have comparative efficacy
1. DeFronzo R, et al. Diabetes Care 2008;31:2315-2317. 2. Linagliptin Prescribing Information. 3. Saxagliptin PrescribingInformation. 4. Sitagliptin Prescribing Information.5. Vildagliptin Summary of Product Characteristics.
-0.56
-0.59 -0.6
-0.7
-0.4
-0.6 -0.6
-0.8
-0.5
-0.7

Sodium Glucose Co-Transporter 2
Reabsorption of glucose is
mediated by SGLTs in
proximal convoluted tubule
– Independent of insulin
• SGLT2 and SGLT1
– located on luminal surface of
epithelial cells lining proximal
convoluted tubule
• SGLTs in other organs
– 2: liver
– 1: small intestine
Bays, H. Diabetes Therapy, 2013Chao EC, et al. Nat Rev Drug Discovery. 2010;9:551-559
90% glucose is reabsorbed in S1 by SGLT2
Low affinity, high capacity transporter
10% reabsorbed in S3 by SGLT1High affinity, low capacity transporter
S1 segment of proximal tubule:
SGLT2
S3 segment of proximal
tubule: SGLT1
90% reabsorption
10% reabsorption
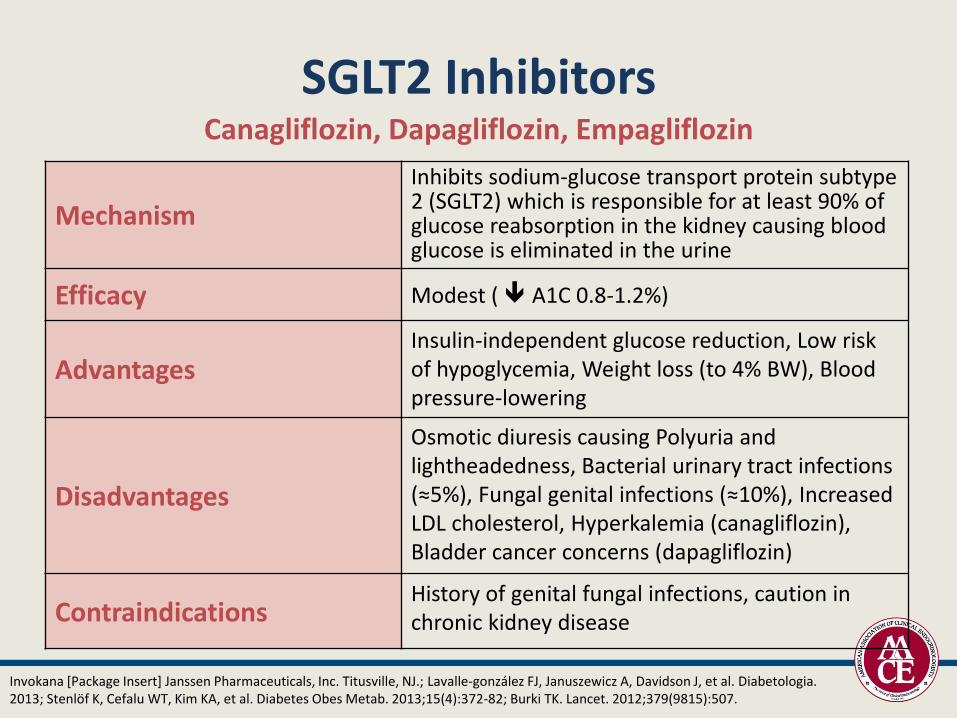
SGLT2 InhibitorsCanagliflozin, Dapagliflozin, Empagliflozin
Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ.; Lavalle-gonzález FJ, Januszewicz A, Davidson J, et al. Diabetologia. 2013; Stenlöf K, Cefalu WT, Kim KA, et al. Diabetes Obes Metab. 2013;15(4):372-82; Burki TK. Lancet. 2012;379(9815):507.
Mechanism
Inhibits sodium-glucose transport protein subtype 2 (SGLT2) which is responsible for at least 90% of glucose reabsorption in the kidney causing blood glucose is eliminated in the urine
Efficacy Modest ( A1C 0.8-1.2%)
AdvantagesInsulin-independent glucose reduction, Low risk of hypoglycemia, Weight loss (to 4% BW), Blood pressure-lowering
Disadvantages
Osmotic diuresis causing Polyuria and lightheadedness, Bacterial urinary tract infections (≈5%), Fungal genital infections (≈10%), Increased LDL cholesterol, Hyperkalemia (canagliflozin),Bladder cancer concerns (dapagliflozin)
ContraindicationsHistory of genital fungal infections, caution in chronic kidney disease

Efficacy of SGLT2 Inhibitors as Monotherapya
0.14
−0.23
0.08
−0.77 −0.77−0.66
−1.03
−0.89−0.78
-1.5
-1.0
-0.5
0.0
0.5
Δ A
1C
, %
a Phase 3 trials, BL A1C 7.8% to 8.1%, 24-26 weeks.
1. Stenlöf K, et al. Diabetes Obes Metab. 2013;15:372-382.2. Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224.3. Roden M, et al. Lancet Diabetes Endocrinol. 2013;1:208-219.
P<0.001 vs PBO for all
CANA1
PBO 100 300
DAPA2
PBO 5 10
EMPA3
PBO 10 25

Roden M et al. Lancet Diabetes Endocrinol. 2013;1:208-219.Stenlöf K et al. Diabetes Obes Metab. 2013;15:372-382.
Weight Effects with SGLT2 Inhibitorsa as Monotherapy
Ferrannini E et al. Diabetes Care. 2010;33:2217-2224.US FDA. Drugs@FDA. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA/.

SGLT2 Inhibitors Safety: Warnings and Precautions
• SGLT2 inhibitor use may be associated with hypotension, ketoacidosis, impaired renal function, hypoglycemia, and increased LDL-C
– Patients should be closely monitored, particularly those with a history of, or at risk for, these conditions
• Dapagliflozin should not be used in patients with a history of bladder cancer
• Canagliflozin may be associated with hyperkalemia and bone fracture
– Bone fracture risk should be considered before use, and potassium levels should be monitored during use
Empagliflozin/Jardiance®PI 2016.; Dapagliflozin/Farxiga® ® PI 2016.; Canagliflozin/Invokana® ® PI 2016.
LDL-C = low-density lipoprotein cholesterol; SGLT2 = sodium-glucose cotransporter-2

CVD Outcomes in ACCORD, ADVANCE, and VADT
ACCORD ADVANCE VADTIntensive Standard Intensive Standard Intensive Standard
Baseline 8.1% 8.1% 7.5% 7.5% 9.4% 9.4%
Final 6.4% 7.5% 6.4% 7.0% 6.9% 8.4%
CVD/year 2.1% 2.3% 2.0% 2.1% 3.8% 4.9%
The Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med 2008; 358:2545-255. Abraira, C, et al. J Diab Comp, 2003;314–322. Patel, A. et al. N Engl J Med, 2008;358:2560–2572.
ACCORD = The Action to Control Cardiovascular Risk in Diabetes study; ADVANCE = The Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation trial; CVD = cardiovascular disease; VADT = Veterans Affairs Diabetes Trial
Clear Findings from EMPA-REG• EMPA-REG studied a high-risk group of people
- Mean age 63 years
- Type 2 diabetes X 10 years; mean A1C 8.1%
- Proven CV disease with prior heart failure in 10%
- eGFR between 30-60 mL/min in 20%
- Cardioprotective Rx (statins 77%, ACEi 81%, ASA 83%)
- MACE event rate ~ 4%/year, CV death rate ~ 1.8%/year
• In 7,020 such people, empagliflozin (10 or 25 mg/day)- Clearly reduces CV death and heart failure hospitalization
- Starts to reduce these outcomes within 3 months
• There is no clear MI or stroke effect over 3 years of treatment- The “composite” outcome may not be relevant
- The effect on its 3 components appears heterogeneous
Zinman B et al. N Engl J Med 2015;373:2117-28. Supplement to: Zinman B et al. N Engl J Med 2015;373:1-66.
ASA = aspirin; ACEi = angiotensin-converting enzyme inhibitors; CV = cardiovascular; eFGR = estimated glomerular filtration
rate; MACE = Major Adverse Cardiac Events; MI = myocardial infarction.
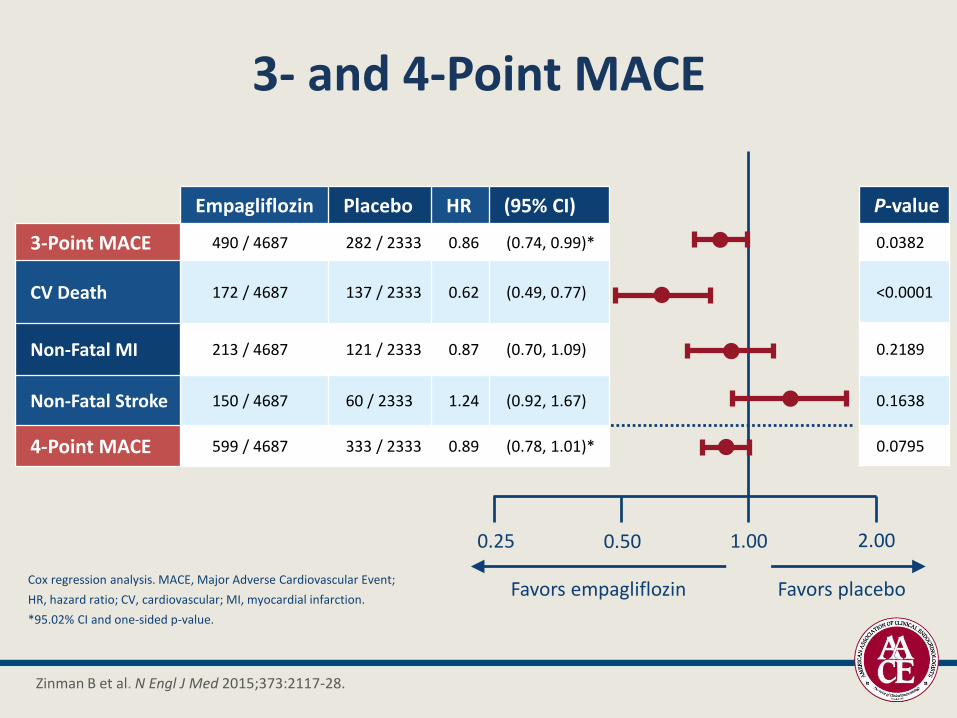
3- and 4-Point MACE
Empagliflozin Placebo HR (95% CI)
3-Point MACE 490 / 4687 282 / 2333 0.86 (0.74, 0.99)*
CV Death 172 / 4687 137 / 2333 0.62 (0.49, 0.77)
Non-Fatal MI 213 / 4687 121 / 2333 0.87 (0.70, 1.09)
Non-Fatal Stroke 150 / 4687 60 / 2333 1.24 (0.92, 1.67)
4-Point MACE 599 / 4687 333 / 2333 0.89 (0.78, 1.01)*
P-value
0.0382
<0.0001
0.2189
0.1638
0.0795
Cox regression analysis. MACE, Major Adverse Cardiovascular Event;
HR, hazard ratio; CV, cardiovascular; MI, myocardial infarction.
*95.02% CI and one-sided p-value.
0.25 0.50 1.00 2.00
Favors empagliflozin Favors placebo
Zinman B et al. N Engl J Med 2015;373:2117-28.

Empa-Reg: Reduction in All-Cause Mortality
HR 0.68(95% CI 0.57, 0.82)
p<0.0001
Zinman B et al. N Engl J Med 2015;373:2117-28.
46

Empa-Reg: Reduction in CHF admissions
Zinman B et al. N Engl J Med 2015;373:2117-28.

LEADER Trial: Primary Outcome
Placebo
Liraglutide
Pati
en
ts w
ith
an
eve
nt
(%)
Months since randomization
Hazard ratio, 0.87 (95% CI, 0.78–
0.97)
P<0.001 for noninferiority
P=0.01 for superiority
First occurrence of CV death, nonfatal myocardial infarction, or nonfatal stroke in
the time-to-event analysis in patients with type 2 diabetes and high CV risk.
Marso SP et al., NEJM 2016
CI = confidence interval; CV = cardiovascular; LEADER = Liraglutide Effect and Action in Diabetes: Evaluation of
cardiovascular outcome Results.

LEADER - Cardiovascular Death
Cumulative incidences were estimated with the Kaplan–Meier method,
and hazard ratios with Cox proportional-hazard regression model.
Data analyses are truncated at 54 months because <10% of patients
had an observation time beyond 54 months.
CI = confidence interval; HR = hazard ratio.
Marso SP et al. NEJM. 2016;375(4):311-322.