update on devices for diastolic dysfunction: options for a no … on devices... · 2018-11-23 ·...
TRANSCRIPT

INTERVENTIONAL CARDIOLOGY (SR BAILEY, SECTION EDITOR)
Update on Devices for Diastolic Dysfunction: Options for a NoOption Condition?
Ahmit Gupta1 & Steven R. Bailey1
# Springer Science+Business Media, LLC, part of Springer Nature 2018
AbstractPurpose of Review This article provides an update on percutaneous devices to treat diastolic dysfunction, current clinicalexperience, and actively enrolling trials. We also discuss potential complications and limitations of devices.Recent Findings Exertional symptoms including exertional dyspnea and exercise intolerance are common features of heartfailure that are driven by left ventricular and left atrial non-compliance that results in pulmonary vascular congestion. Multiplestudies that have shown that reducing total body volume and intravascular pressure, using pharmacologic therapies, are associ-ated with improved outcomes among patients who have heart failure with reduced ejection fraction (HFrEF) (ejection fraction[EF] < 40%), but not heart failure with preserved ejection fraction (HFpEF) (EF > 55%).This is related to the fact that HFpEF isassociatedwith altered diastolic compliance but not volume overload, which presents as exertional increases in left atrial pressure.Exercise assessment of LA and pulmonary pressures are not commonly assessed today in the clinic or in the catheterizationlaboratory. As elevated left atrial pressure mediates these symptoms, selective reduction in left atrial pressure may provideimprovement in symptoms without complications of pharmacologic therapy such as diuresis and aggressive blood pressurereduction. Mechanical devices that aim to reduce left atrial pressure have been developed and evaluated in HFpEF and HFrEFpatients.Summary The current data from the small number of patients who have undergone treatment with left atrial decompressiondevices indicate that they have a high rate of success and may improve patient’s exercise capacity. Larger, controlled trials areunderway to better understand the role of these devices in patients with diastolic dysfunction.
Keywords Heart failure . Diastolic dysfunction . HFpEF . Left atrial pressure . Percutaneous device . Atrial septum
AbbreviationsLA Left atriumLV Left ventricleHFpEF Heart failure with preserved ejection fractionHFrEF Heart failure with reduced ejection fractionLVEF Left ventricular ejection fractionIASD The Inter Atrial Shunt Device
Introduction
The prevalence of heart failure with preserved ejection frac-tion (HFpEF) is estimated to represent 50% of all clinical heartfailure (HF) patients. Left ventricular diastolic dysfunctionresulting from abnormal relaxation and increased passive stiff-ness impairs diastolic reserve. While many patients withHFpEF may have normal resting pressures, they typically de-velop marked elevations in LA pressure followed by pulmo-nary vein hypertension with exercise due to the altered dia-stolic compliance. This is typically manifest as exertional dys-pnea. Therapies that aim to reduce total body volume andconsequently intravascular pressure have been associated withimproved outcomes among patients who have heart failurewith reduced ejection fraction (HFrEF) (ejection fraction[EF] < 40%), but not heart failure with preserved ejection frac-tion (HFpEF) (EF > 50%). Diuretics may be effective in bring-ing symptomatic relief but their use is frequently complicated
This article is part of the Topical Collection on Interventional Cardiology
* Steven R. [email protected]
Ahmit [email protected]
1 Janey andDolph BriscoeDivision of Cardiology, University of TexasHealth Sciences Center at San Antonio, Mail Code 7872, 7703 FloydCurl Drive, San Antonio, TX 78229, USA
Current Cardiology Reports (2018) 20:85 https://doi.org/10.1007/s11886-018-1027-2

by hypovolemia and azotemia as many patients are not vol-ume overloaded. In recent years, innovative devices in clinicaltrials have shown promise and this article is intended to reviewcurrent status of progress made.
Diastolic Heart Failure (HFpEF)
Heart failure is a clinical diagnosis and several criteria havebeen proposed to define HFpEF such as (a) clinical signs orsymptoms of heart failure, (b) evidence of preserved or normalleft ventricular ejection fraction (LVEF) (variably classified asEF > 40%, > 50%, or > 55%), and (c) evidence of left ventric-ular (LV) diastolic dysfunction by echocardiographic or car-diac catheterization criteria [1•]. The pathophysiologic basisof diastolic dysfunction is impaired LV relaxation (which pri-marily affects early diastole) and increased myocardial stiff-ness (which primarily affects late diastole). The pathophysio-logic basis of diastolic dysfunction is impaired active LV re-laxation (which primarily affects early diastole) and increasedmyocardial stiffness (which primarily affects late diastole).The rate and extent of the active relaxation influence LV re-laxation during the early filling phase. Both abnormalities leadto elevation of diastolic pressures which are transmitted even-tually to left atrium (LA) and pulmonary veins leading toexercise intolerance and dyspnea [2]. Both abnormalities leadto elevation of diastolic pressures which are transmitted even-tually to the left atrium (LA) and pulmonary veins leading toincreased pulmonary interstitial fluid, increased work ofbreathing, exercise intolerance, and dyspnea on exertion.
In the USA, the prevalence of heart failure (HF) cases isestimated to exceed 5.8 million patient with > 650,000 newHF cases diagnosed annually. Of these, based on communitystudies, nearly half of the patients have preserved ejectionfraction (HFpEF) [3]. HF is characterized by periodic exacer-bations that require treatment intensification most often in thehospital and is the single most frequent primary diagnosis atthe time of hospitalization in persons aged ≥ 65 years. Nearly1 million hospitalizations for HF occur each year, with rates ofhospitalization that continue to rise [4]. With aging populationand expected increasing prevalence of HF, there is unmet needfor exploring therapies to decrease morbidity and mortalityfrom HFpEF.
Role of Left Atrial Pressure
Hemodynamics obtained with invasive catheterization duringrest and exercise have shed more light on HFpEF patients, allof which demonstrate (1) marked increase in LA/pulmonarycapillary wedge pressure (PCWP) with increasing exerciseworkload compared to normal subjects even though corre-sponding measurements are comparable at rest, (2) rapid de-crease in PCWP within a few minutes of cessation of exercisewhich emphasizes that these patients are not hypervolemic,
and (3) volume sensitivity with as little as 600 ml intravenousfluid administration resulting inmarked increase in pulmonarywedge pressure which is a surrogate of LA pressure [5••].Higher peak PCWP corrected for workload during exercisehas been associated with reduced exercise capacity and worseoutcomes in the setting of HFpEF [6••, 7•]. In addition, intrin-sic LAmechanical dysfunction is associated with an increasedincidence of atrial fibrillation and is recognized as a driver ofpoor outcomes in HFpEF [8–10, 11••].
Strict control of LA pressure by invasive monitoring andphysician-directed self-management have been associatedwith significant improvement in NYHA class as well as witha major reduction in rehospitalizations and mortality at mid-term follow-up [12]. The closure of congenital atrial septaldefects in patients with diastolic dysfunction have been asso-ciated with a rise in LA pressures and decompensated HF[13].
None of the medical therapies other than diuretics havebeen able to show any decrease in morbidity, which them-selves have side effects due to decrease in intravascular vol-ume. Hence device-based therapies which can decrease LApressure selectively with exercise would seem to promise de-creasing morbidity with fewer side effects than medical ther-apy alone.
Rationale of Interatrial Septostomy
Left atrium is an elastic chamber receiving blood from pulmo-nary vein passively which modulates LV filling by acting asactive booster during atrial systole. The LA buffers pressureand flow coupling between the LV and the pulmonary circu-lation due to the cyclic nature of cardiac hemodynamics [14].At identical mean LA pressure in patients with heart failure,HFrEF patients had larger LA volumes while HFpEF patientshad higher LA peak pressures and higher LA stiffness. LAfunction has been related to mortality in HFpEF patients butnot in HFrEF patients [9].
LA pressure itself may be prognostically important. In pa-tients undergoing paravalvular leakage closure (n = 134) withinvasive LA pressure monitoring, the LA pressure post clo-sure was found to be related to mortality in over next 3 yearsof follow-up. Each 10% reduction in post procedural LA pres-sure was associated with a significant 9% decrease in risk ofdeath after adjustment for age, gender, and residual MR overthe next 3 years [15]. It has been reported that patients withLutembacher syndrome which is a combination of mitral ste-nosis and atrial septal defect (ASD) did better than patientswith mitral stenosis alone [16]. There have been case reportsof iatrogenic ASD made to decompress LV in case of fulmi-nant myocarditis with pulmonary hemorrhage which wasshown to decrease LA hypertension [17]. Also, in patientswith restrictive LV physiology who have ASD, case reportssuggest improved outcomes by closing them with fenestrated
85 Page 2 of 8 Curr Cardiol Rep (2018) 20:85

ASD closure devices [18]. In patients with severe pulmonaryhypertension and right ventricular dysfunction, creation ofinteratrial shunt already has been shown to improve symptomsand hemodynamics [19]. So, creation of unidirectional left toright shunt in patient with HFpEF should provide relief duringepisodes of acute elevation of LA pressure, reduce LA pres-sure overtime, improve functional class, and eventually re-duce rehospitalizations.
Computer simulation study performed with exercise-associated hemodynamics has shown the theoretical effectsof such a shunt (diameter up to 12 mm) on acute rest andexercise hemodynamic data (including changes in PCWP) inpatients with HFpEF. The interatrial shunt was predicted tolower PCWP acutely by ~ 3 mmHg under simulated restingconditions (from 10 to 7 mmHg) and by ~ 11 mmHg duringsimulated peak exercise (from 28 to 17 mmHg). Left ventric-ular cardiac output was predicted to decrease ~ 0.5 L/min atrest and ~ 1.3 L/min at peak exercise, with correspondingincreases in right ventricular cardiac output. The authors alsostudied effect on rest and exercise hemodynamics of varyingthe shunt diameter from 0 to 12 mm [20•]. As expected, shuntflow increases with increasing shunt size at rest and duringexercise [20•]. Under resting conditions, as shunt flow sizewas increased, there was a progressive decrease in PCWPand a lesser increase in RA pressure with corresponding in-crease in right ventricular cardiac output (CO) and a decreasein left ventricular CO [20•]. All of these effects reach a plateauat a shunt diameter of 8–9 mm. During exercise, the effectswere significantly more pronounced because of the larger LA-RA pressure gradient under this condition; however, the effecton shunt flow still plateaus at approximately 10 mm [20•].Direction of flow in shunt was left to right in all case scenariostested. Authors concluded that this approach may reduce thepropensity for heart failure exacerbations and allow patients toexercise longer, thus attaining higher heart rates and cardiacoutputs with the shunt compared with no shunt [20•].
There are multiple established techniques for creating largeinteratrial communication like percutaneous perforation, bal-loon dilation, and stent implantation. However, complicationsof these procedures include excessive desaturation, spontane-ous fenestration closure, stent occlusion or migration, difficul-ties in adjusting shunt size to achieve the desired hemodynam-ic effect, and the inability to remove or close the shunt [21].Now, there are three percutaneously deployed innovative de-vices which avoid these complications and are currently un-dergoing clinical trials. The trials of percutaneous device ther-apies are summarized in Table 1.
Inter Atrial Shunt Devices
The Inter Atrial Shunt Device (IASD) (Corvia Medical Inc.,Tewkesbury, MA, USA) (Fig. 1a) is a nitinol device (outerdiameter 19.4 mm) inserted percutaneously in the interatrial Ta
ble1
Current
HFpE
Fdevice
trials
Device
Manufacturer
Etio
logy
Title
1°endpoint
No.of
patients
Design
NCTnumber
IASD
CorviaMedical
HFp
EF
REDUCELAPH
FII
Cardiovascularmortalityor
non-fatal,ischem
icstroke
through
6months;2.Changein
baselin
eKCCRat6months
380
Tripleblindwith
sham
arm
NCT03088033
Vwave
V-W
aveLtd
Heartfailu
reRelieve
HF
Freedom
from
study-relatedmajor
adversecardiacandneurological
events(M
ACNE)at6months
Not
specified
Singlearm
with
draw
nNCT02511912
CORolla
CorAssist
Cadiovascular
Ltd.
HFp
EF
CORolla®
TAAforheartfailure
with
preservedejectio
nfractio
n(H
FpEF)
anddiastolic
dysfunction(D
D)
All-causemortalityandseriousadverse
events(SAEAs)at6months
10Single-arm
studydesign
includingwith
patientswith
isolated
HFpE
F,in
NYHA
f.Cl.III-IV
NCT02499601
Curr Cardiol Rep (2018) 20:85 Page 3 of 8 85
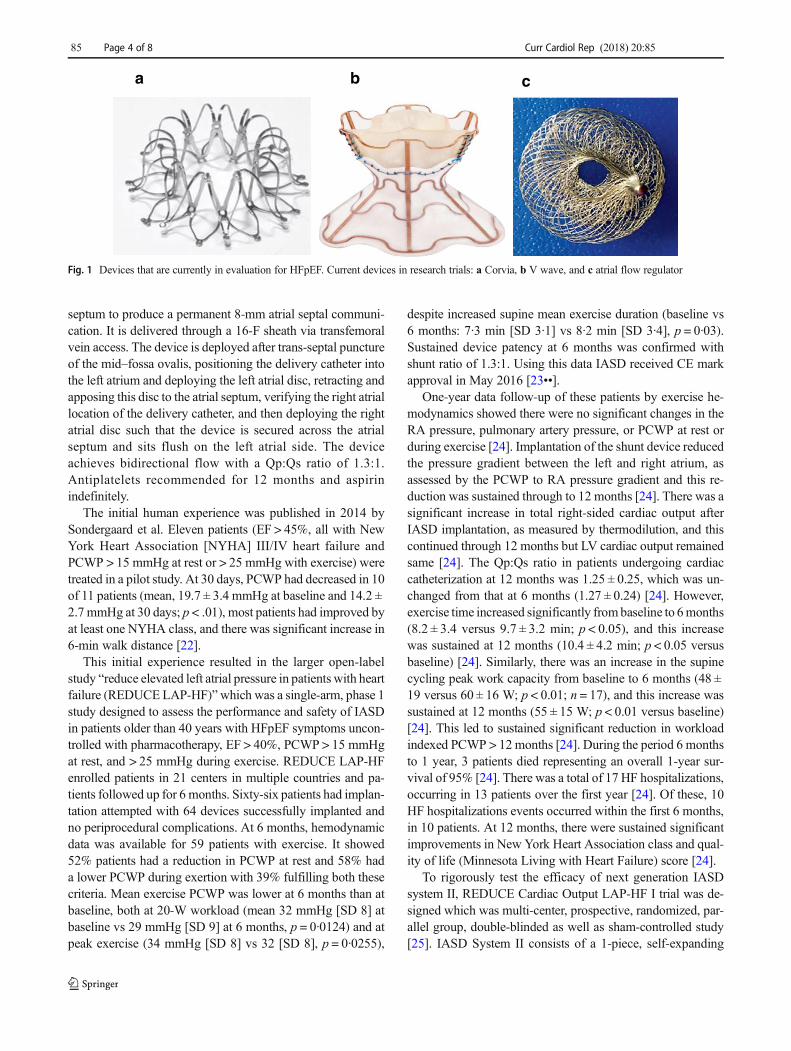
septum to produce a permanent 8-mm atrial septal communi-cation. It is delivered through a 16-F sheath via transfemoralvein access. The device is deployed after trans-septal punctureof the mid–fossa ovalis, positioning the delivery catheter intothe left atrium and deploying the left atrial disc, retracting andapposing this disc to the atrial septum, verifying the right atriallocation of the delivery catheter, and then deploying the rightatrial disc such that the device is secured across the atrialseptum and sits flush on the left atrial side. The deviceachieves bidirectional flow with a Qp:Qs ratio of 1.3:1.Antiplatelets recommended for 12 months and aspirinindefinitely.
The initial human experience was published in 2014 bySondergaard et al. Eleven patients (EF > 45%, all with NewYork Heart Association [NYHA] III/IV heart failure andPCWP > 15 mmHg at rest or > 25 mmHg with exercise) weretreated in a pilot study. At 30 days, PCWP had decreased in 10of 11 patients (mean, 19.7 ± 3.4 mmHg at baseline and 14.2 ±2.7 mmHg at 30 days; p < .01), most patients had improved byat least one NYHA class, and there was significant increase in6-min walk distance [22].
This initial experience resulted in the larger open-labelstudy “reduce elevated left atrial pressure in patients with heartfailure (REDUCELAP-HF)”which was a single-arm, phase 1study designed to assess the performance and safety of IASDin patients older than 40 years with HFpEF symptoms uncon-trolled with pharmacotherapy, EF > 40%, PCWP > 15 mmHgat rest, and > 25 mmHg during exercise. REDUCE LAP-HFenrolled patients in 21 centers in multiple countries and pa-tients followed up for 6 months. Sixty-six patients had implan-tation attempted with 64 devices successfully implanted andno periprocedural complications. At 6 months, hemodynamicdata was available for 59 patients with exercise. It showed52% patients had a reduction in PCWP at rest and 58% hada lower PCWP during exertion with 39% fulfilling both thesecriteria. Mean exercise PCWP was lower at 6 months than atbaseline, both at 20-W workload (mean 32 mmHg [SD 8] atbaseline vs 29 mmHg [SD 9] at 6 months, p = 0·0124) and atpeak exercise (34 mmHg [SD 8] vs 32 [SD 8], p = 0·0255),
despite increased supine mean exercise duration (baseline vs6 months: 7·3 min [SD 3·1] vs 8·2 min [SD 3·4], p = 0·03).Sustained device patency at 6 months was confirmed withshunt ratio of 1.3:1. Using this data IASD received CE markapproval in May 2016 [23••].
One-year data follow-up of these patients by exercise he-modynamics showed there were no significant changes in theRA pressure, pulmonary artery pressure, or PCWP at rest orduring exercise [24]. Implantation of the shunt device reducedthe pressure gradient between the left and right atrium, asassessed by the PCWP to RA pressure gradient and this re-duction was sustained through to 12 months [24]. There was asignificant increase in total right-sided cardiac output afterIASD implantation, as measured by thermodilution, and thiscontinued through 12 months but LV cardiac output remainedsame [24]. The Qp:Qs ratio in patients undergoing cardiaccatheterization at 12 months was 1.25 ± 0.25, which was un-changed from that at 6 months (1.27 ± 0.24) [24]. However,exercise time increased significantly frombaseline to 6months(8.2 ± 3.4 versus 9.7 ± 3.2 min; p < 0.05), and this increasewas sustained at 12 months (10.4 ± 4.2 min; p < 0.05 versusbaseline) [24]. Similarly, there was an increase in the supinecycling peak work capacity from baseline to 6 months (48 ±19 versus 60 ± 16 W; p < 0.01; n = 17), and this increase wassustained at 12 months (55 ± 15 W; p < 0.01 versus baseline)[24]. This led to sustained significant reduction in workloadindexed PCWP > 12months [24]. During the period 6 monthsto 1 year, 3 patients died representing an overall 1-year sur-vival of 95% [24]. There was a total of 17 HF hospitalizations,occurring in 13 patients over the first year [24]. Of these, 10HF hospitalizations events occurred within the first 6 months,in 10 patients. At 12 months, there were sustained significantimprovements in New York Heart Association class and qual-ity of life (Minnesota Living with Heart Failure) score [24].
To rigorously test the efficacy of next generation IASDsystem II, REDUCE Cardiac Output LAP-HF I trial was de-signed which was multi-center, prospective, randomized, par-allel group, double-blinded as well as sham-controlled study[25]. IASD System II consists of a 1-piece, self-expanding
cba
Fig. 1 Devices that are currently in evaluation for HFpEF. Current devices in research trials: a Corvia, b V wave, and c atrial flow regulator
85 Page 4 of 8 Curr Cardiol Rep (2018) 20:85

metal cage that has a double-disc design with an opening inthe center and is echogenic and radiopaque. Key inclusioncriteria included documented chronic symptomatic HF and(1) prior hospitalization for HF (or acute care facility/emergency room intensification of diuretic therapy) withinthe prior 12 months, or (2) elevated B-type natriuretic peptide(BNP) or N-terminal pro-BNP (NTproBNP) within the past6 months with defined criteria in patients > 40 years of agewith EF > 40%, no right ventricular dysfunction, no pulmo-nary hypertension(< 4 Woods unit), and elevated LA pressuredocumented invasively by end-expiratory PCWP during su-pine bike exercise ≥ 25 mmHg, and PCWP-RA pressure(RAP) gradient ≥ 5 mmHg [25].
Patients were randomized 1:1 ratio between device andsham-controlled arms. Both patients and physicians whofollowed them were blinded to treatment assignment and he-modynamic findings. Both treatment and control arm patientsunderwent femoral venous access after randomization.Patients randomized to the treatment arm underwent a trans-septal puncture and IASD System II implantation guided byfluoroscopy and intracardiac or transesophageal echocardiog-raphy whereas control arm underwent all procedures excepttrans-septal puncture. The primary effectiveness endpoint wasexercise PCWP at 1 month. The primary safety endpoint wasmajor adverse cardiac, cerebrovascular, and renal events(MACCRE) at 1 month.
Ninety patients were enrolled, of which 44 met criteria andwere randomized to the IASD (N = 22) and control (N = 22)groups. Mean age was 70 ± 9 years and 50% were female.Device was implanted successfully in 20/22 patients. At1 month, the IASD resulted in a greater reduction in PCWPcompared to sham-control (p = 0.028) meeting predefined pri-mary efficacy endpoint. Peak PCWP decreased by 3.5 ±6.4 mmHg in the treatment group vs. 0.5 ± 5.0 mmHg in thecontrol group (p = 0.14) which was similar as seen previouslyin REDUCE LAP-HF trial at 6 months and 12 months. Therewere no periprocedural complications and 1 MACCRE eventwith worsening renal function. No patient from treatment armwas admitted for HF during this period whereas 9.1% (2/22)patients in sham-control arm were admitted. The lowering ofPCWP during exercise and improvements in workload-corrected PCWP, exercise duration, and peak exercise work-load compared to sham control were numerically better in thetreatment group but the differences did not achieve statisticalsignificance, as the trial was not powered to demonstrate ef-fectiveness in these endpoints.
V Wave
The V wave device (V-Wave Ltd., Or Akiva, Israel), Fig. 1b,in the first generation consisted of an hourglass shaped, self-expanding nitinol frame that contains a tri-leaflet porcine peri-cardium tissue valve sutured inside which allowed
unidirectional flow from the LA to the right atrium if thepressure gradient exceeded 2 mmHg achieving a Qp:Qs of1.1–2:1. The valve prevents reverse shunting of blood andprevents paradoxical embolism. The stent is deployed underfluoroscopic and transesophageal echo guidance with a 14-French sheath so that the neck of the hourglass is placed acrossthe fossa ovalis and secured in place by its geometry with thewider entry funnel deployed in the left atrium and the widerexit funnel in the right atrium. The entry funnel and the centralneck are encapsulated with expanded polytetrafluoroethylene(ePTFE) to facilitate laminar flow and limit tissue ingrowthduring device healing. Three months of anticoagulation withcoumadin or DOAC is recommended by the device manufac-turer along with aspirin for life.
The Vwave device was evaluated in 10HFrEF patients in asingle center in Canada using the special access process toprove the concept. The patients averaged 62 years of ageand notably had an average LVEF of 25%, and NYHA classIII or greater symptoms; the average PCWP at cath was23 mmHg without right ventricular dysfunction. The averageNTproBNP at baseline was 2712 pg/mL. The patients wereevaluated at 3 months after the index procedure and in thissmall population, there was a reduction in NYHA class, im-proved their 6-min walk distance, and reported improvedquality of life (QoL) and physical function. Echo cardiogramsat 3 months showed a small decrease in LV volumes but im-portantly, there was a decrease in PCWP from 23 mmHg atbaseline to 17 mmHg at 3-month follow-up; p = 0.035.Neither the RAP (9 vs 8 mmHg) nor the mean pulmonaryartery pressure (29 vs 26 mmHg) showed a significant change[26].
At 1-year follow-up, resting shunt fraction had declinedfrom a mean of 1.2:1 to 1.1:1, with 14% of patients havingno interatrial flow. This occurred in conjunction with pannusthickening of the bioprosthetic leaflets and lumen loss, whichprompted the creation of a second-generation device with ex-tended ePTFE coating and without unidirectional valve andincluded a hood to prevent potential thromboemboli from op-posing the right atrial side of the implant. This version of thedevice has not shown late lumen loss at 6 months in animalstudies [26].
Cabau presented a larger series including of 22 patientsfrom the original single center and 16 additional patientsfrom the First in Man Multi-Center Feasibility Study per-formed in Israel and Italy [27]. The population included 30patients with reduced LVEF (26%) and eight with pre-served LVEF (50%). There was 100% implant success(38/38) but at 1 year, 5/36 (14%) of devices were occludedor stenotic. Stenosis conveyed a worse outcome. A furthersingle-arm prospective, nonrandomized, open-label, multi-center study of the device was planned in patients withboth HFrEF and HFpEF (NCT02511912) but was with-drawn in September 8, 2017.
Curr Cardiol Rep (2018) 20:85 Page 5 of 8 85

Atrial Flow Regulator
The atrial flow regulator (AFR) (Occlutech, Istanbul, Turkey),Fig. 1c, is a self-expandable double-disc wire mesh device con-structed from 0.004–0.0075-in. nitinol braided into two flatdiscs connected by a waist of 1–2 mm and central fenestrationwhich enables bidirectional flow. A welded ball connector lo-cated on the device’s proximal disc serves as an adapter toconnect the delivery system for deployment. After implanta-tion, the AFR conforms completely to the atrial septum leavingan interatrial communication with a preselected fixed diameter.The device is easy to handle, self-centers following deploy-ment, and is retrievable prior to release. The device is availablein 6, 8, and 10 mm fenestration diameters with a total devicediameter of 18, 24, and 30mm delivered via 10- to 12-F sheath.
The first clinical utilization of the device followed a com-passionate use approval from the US Food and DrugAdministration. The patient was a 54-year-old woman withsevere and irreversible pulmonary artery hypertension.Implantation was associated with immediate right-to-leftshunting and a corresponding decrease in arterial saturation(from 95 to 89%). She reported functional improvement at6 weeks [28•]. This experience was later extended to 12 pa-tients (mean age 28.3 ± 8.5 years) with severe irreversible pul-monary arterial hypertension [29]. All the patients were re-ceiving optimal doses of two oral pulmonary vasodilators ofwhich one belonged to endothelin receptor antagonists and theother belonged to phosphodiesterase-5 inhibitors. All proce-dures were successful without any major complications andantiplatelets were given to maintain patency of device. Allpatients had relief of syncope and 6-min walk distance im-proved significantly from 377.3 ± 33.2 to 423 ± 31.32 m.The cardiac index (2.36 ± 0.52 to 2.89 ± 0.56 L/min/m2) andsystemic oxygen transport (367.5 ± 75.5 to 428.0 ± 67.1 ml/min/m2) also showed a significant improvement [29]. Eventhough echocardiographic parameters of right ventricularfunction did not show significant change, inferior caval veincongestion and pericardial effusion were reduced due to im-provement in heart failure. The device was patent in all pa-tients at a median follow-up of 189 days (range 10–296 days)resulting in a significant reduction of oxygen saturations from98 ± 0.18 to 85.2 ± 62.86% after exercise [29]. Complete en-dothelialization of nitinol atrial septal occluders was demon-strated within a few months after implantation, permittingwithdrawal of antiplatelets after 6–12 months.
In patients with diastolic dysfunction and left to right atrialgradient, the shunt direction will be left to right and is expectedto get results similar to other interatrial septostomy devices withshunt ratio based on device size. An international clinical trialPRELIEVE to study AFR device is currently recruiting. It is anopen-label, nonrandomized trial including up to 30 patientswith symptomatic heart failure (HFpEF or HFrEF) and a heartfailure admission in the past 12 months (NCT03030274).
CoRolla
CoRolla (CorAssist Inc., Haifa, Israel) is an intraventriculardevice invented by Dr. Yair Field which is designed to beimplanted by minimally invasive transapical approach offpump. It is elastic self-expanding internal spring like devicewhich is based on mechanical principles of energy transferfrom systole to diastole. The device applies direct internalexpansion forces distributed on the left ventricle wall andseptum to directly improve diastolic function. The device im-proves filling performance and diastolic dynamics withoutneeding an external power source. Preclinical studies haveshowed safety over 24-month duration and first in humanimplantation was carried out in RAMBAM medical center,Haifa, Israel, in July 2017. There is registered clinical trialNCT01956526 which is an open-label study to evaluateCoRolla in HFpEF patients with NYHA III-IVand in patientswith Aortic stenosis who are undergoing aortic valve replace-ment as add on procedure. Primary aim of trial is to assesssafety over 12 months post procedure and assess for efficacyover 36 months with clinical and echocardiographicendpoints.
Long-term Considerations
Biggest concern for interatrial septostomy devices is an in-creased volume loading of right-sided circulation fromshunting causing pulmonary hypertension and leading to RVdysfunction. Such hemodynamic changes might affect otherorgans already compromised in HFpEF, such as the kidneys,with a subsequent negative impact on long-term outcome[30]. Although the literature from congenital heart diseasepatients suggest small shunts (< 1.3:1) are generally tolerablefor decades [28•], the adult heart failure phenotype, especiallywith hypertension, may be different. Reported experiencewith the IASD system in heart failure patients has revealednonsignificant increases in right atrial and ventricular volumesat 6 months after implantation, which did not progress at 12-month follow-up and have not been associated with depressedright ventricular function or pulmonary hypertension [24].
Another factor that may influence long-term outcome is theuse of anticoagulation: IASD implantation required 1-yeardual antiplatelet therapy, AFR required 6–12 months whereasV wave required warfarin or DOAC for 3 months followingimplantation. All devices require indefinite, low-dose aspirin.Additionally, because atrial arrhythmias are a common mani-festation of unrepaired congenital atrial septal defects and areobserved with greater frequency in the months after implanta-tion of other atrial septal devices [29], ongoing surveillance iswarranted post IASD implantation. As atrial arrhythmias arealso common in heart failure patients, it will be interesting tosee if the incidence of atrial arrhythmias in interatrialseptostomy devices is even higher or lower than anticipated.
85 Page 6 of 8 Curr Cardiol Rep (2018) 20:85

The anticoagulation required for atrial fibrillation or Flutterwhen concurrent with DAPT may also increase bleeding risk.
Recently, closure of PFO has been shown to be beneficialin long-term management of cryptogenic stoke likely due topreventing paradoxical embolism [31, 32]. It will be importantto follow the IASD patients long term to assess if incidence ofstrokes is found to be higher than general population andneeds to be included in any risk versus benefit discussion.
Sham-controlled trial for renal nerve denervation hasshown that invasive treatment trials for devices may be subjectto bias. Also, changing patient behavior due to study involve-ment, known as the “Hawthorne effect,” could have influ-enced the study results [32], possibly by increasing medica-tion compliance during follow-up. In view of these concerns,it is important that future randomized trials include an activesham procedure or blinded readers with larger sample size andfor longer duration to get definitive evidence of efficacy.
Conclusion
Diastolic heart failure patients still do not have effective phar-macological therapies other than managing underlying co-morbidities including hypertension, diabetes, and CKD.Innovative approaches to lower left atrial pressure with devicesor increase compliance of LVoffer options for this unmet need.Early clinical studies have provided evidence of efficacy of thesedevices with most robust evidence base for IASD. Ongoingclinical trials are needed to provide more evidence of efficacyas well as longevity of therapeutic effect for other devices.
Compliance with Ethical Standards
Conflict of Interest Ahmit Gupta and Steven R. Bailey declare that theyhave no conflict of interest.
Human and Animal Rights and Informed Consent This article does notcontain any studies with human or animal subjects performed by any ofthe authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major Importance
1.• Yancy CW, et al. ACCF/AHA guideline for the management ofheart failure. Circulation. 2013;128:e240–327. This publicationis the most recent consensus guidelines for the management ofheart failure of all types. This guideline was the first to summa-rize “Optimal Medical Therapy” for heart failure.
2. Brutsaert DL, Sys SU, Gillebert TC. Diastolic failure: pathophysiolo-gy and therapeutic implications. J Am Coll Cardiol. 1993;22:318–25.
3. Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S,Nkomo VT, et al. Systolic and diastolic heart failure in the commu-nity. JAMA. 2006;296:2209–16.
4. Roger VL. Epidemiology of heart failure. Circ Res. 2013;113:646–59.
5.•• Borlaug BA, Nishimura RA, Sorajja P, Lam CSP, Redfield MM.Exercise hemodynamics enhance diagnosis of early heart failurewith preserved ejection fraction. Circ Heart Fail. 2010;3:588–95.This trial was one of the first to demonstrate the importance ofexercise in diagnosing HFpEF in euvolemic patients. This setsthe stage for future therapeutic trials to utilized exercise hemo-dynamics in assessing pharmacologic therapy and devices.
6.•• Wolsk E, Kaye D, Borlaug BA, Burkhoff D, Kitzman D, Lam CS,et al. Resting and exercise hemodynamics in relation to 6-minutewalk test in patients with heart failure and preserved ejection frac-tion. Eur J Heart Fail. 2017; https://doi.org/10.1002/ejhf.976.Wolsk and colleagues demonstrate the relationship of the 6-min walk with exercise pulmonary capillary wedge pressure.This study reinforces the ability to use the 6-min walk time inpatients with HFpEF to assess the severity of disease.
7.• Dorfs S, Zeh W, Hochholzer W, Jander N, Kienzle RP, Pieske B, etal. Pulmonary capillary wedge pressure during exercise and long-term mortality in patients with suspected heart failure with pre-served ejection fraction. Eur Heart J. 2014;35:3103–12.This inves-tigation correlated symptoms and long-term outcome withworkload and exercise pulmonary capillary wedge pressure ina large patient population. It adds information about whyHFpEF pateints have such high mortality.
8. Freed BH, Shah SJ. Stepping out of the left ventricle’s shadow: timeto focus on the left atrium in heart failure with preserved ejectionfraction. Circ Cardiovasc Imaging. 2017;10:e006267.
9. Melenovsky V, Hwang SJ, Redfield MM, Zakeri R, Lin G, BorlaugBA. Left atrial remodeling and function in advanced heart failurewith preserved or reduced ejection fraction. Circ Heart Fail. 2015;8:295–303.
10. von Roeder M, Rommel KP, Kowallick JT, Blazek S, Besler C,Fengler K, et al. Influence of left atrial function on exercise capacityand left ventricular function in patients with heart failure and pre-served ejection fraction. Circ Cardiovasc Imaging. 2017;10:e005467.
11.•• Rossi A, Gheorghiade M, Triposkiadis F, Solomon SD, Pieske B,Butler J. Left atrium in heart failure with preserved ejection fraction:structure, function, and significance. Circ Heart Fail. 2014;7:1042–9. This review addresses the pathologic and hemodynamicchanges that occur in the left atrium as a consequence ofHFpEF. It also correlates these changes with the diagnosisand prognosis of this condition.
12. Ritzema J, Troughton R, Melton I, Crozier I, Doughty R, Krum H,et al. Hemodynamically Guided Home Self-Therapy in SevereHeart Failure Patients (HOMEOSTASIS) Study Group.Physician-directed patient self-management of left atrial pressurein advanced chronic heart failure. Circulation. 2010;121:1086–95.
13. Ewert P, Berger F, Nagdyman N, Kretschman O, Dittrich S, Abdul-Khaliq H, et al.Masked left ventricular restriction in elderly patientswith atrial septal defects: a contraindication for closure? CatheterCardiovasc Interv. 2001;52:177–80.
14. Braunwald E, Frahm CJ. Studies on starling’s law of the heart: IV.Observations on the hemodynamic functions of the left atrium inman. Circulation. 1961;24:633–42.
15. Maor E, Raphael CE, Panaich SS, Alkhouli M, Cabalka A, HaglerDJ, et al. Left atrial pressure and predictors of survival after percu-taneous mitral paravalvular leak closure. Catheter CardiovascInterv. 2017;90:861–9.
16. Sambhi MP, Zimmerman HA. Pathologic physiology ofLutembacher syndrome. Am J Cardiol. 1958;2:681–6.
Curr Cardiol Rep (2018) 20:85 Page 7 of 8 85

17. Johnston TA, Jaggers J, McGovern JJ, O’Laughlin MP. Bedsidetransseptal balloon dilation atrial septostomy for decompressionof the left heart during extracorporeal membrane oxygenation.CCI. 1999;46:197–9.
18. Peters B, Ewert P, Schubert S, Abdul-Khaliq H, Schmitt B,NagdymanN, et al. Self-fabricated fenestrated Amplatzer occludersfor transcatheter closure of atrial septal defect in patients with leftventricular restriction:midterm results. Clin Res Cardiol. 2006;95:88–92.
19. Kurzyna M, Dabrowski M, Bielecki D, Fijalkowska A, PruszczykP, Opolski G, et al. Atrial septostomy in treatment of end-stage rightheart failure in patients with pulmonary hypertension. Chest.2007;131:977–83.
20.• Kaye D, Shah SJ, Borlaug BA, Gustafsson F, Komtebedde J, KuboS, et al. Effects of an interatrial shunt on rest and exercise hemody-namics: results of a computer simulation in heart failure. J CardFail. 2014;20:212–21. This computer simulation modeled thepredicted effect of a small left to right interatrial shunt on leftatrial pressure and function. This supports percutaneous ther-apies to decompress the left atrial hypertension during exercise.
21. Sivaprakasam M, Kiesewetter C, Veldtman GR, Salmon AP,Vettukattil J. New technique for fenestration of the interatrial sep-tum. J Interv Cardiol. 2006;19:334–6.
22. Sondergaard L, Reddy V, Kaye D, Malek F, Walton A, Mates M, etal. Transcatheter treatment of heart failure with preserved or mildlyreduced ejection fraction using a novel interatrial implant to lowerleft atrial pressure. Eur J Heart Fail. 2014;16:796–801.
23.•• Hasenfuss G, Hayward C, Burkhoff D, Silvestry FE, McKenzie S,Gustafsson F, et al. investigators RL-Hs. A transcatheter intracardi-ac shunt device for heart failure with preserved ejection fraction(REDUCE LAP-HF): a multicentre, open-label, single-arm, phase1 trial. Lancet. 2016;387:1298–304. This First in Man trial dem-onstrated that an intracardiac shunt in HFpEF patients couldbe accomplished and improved functional status.
24. Kaye DM, Hasenfuss G, Neuzil P, Post MC, Doughty R, TrochuJN, et al. One-year outcomes after transcatheter insertion of aninteratrial shunt device for the management of heart failure withpreserved ejection fraction. Circ Heart Fail. 2016;9:e003662.
25. Ted Feldman, Laura Mauri, Rami Kahwash, Sheldon Litwin, MarkJ. Ricciardi, Pim van der Harst, et al. A transcatheter interatrialshunt device for the treatment of heart failure with preserved ejec-tion fraction (REDUCE LAP-HF I): a phase 2, randomized, sham-controlled trial. https://doi.org/10.1161/CIRCULATIONAHA.117.032094( final ref pending).
26. Stone GW R-CJ, Amat-Santos IJ, Ben Gal T, et al. Interatrialshunting for heart failure: the V-wave shunt. Presented at transcath-eter therapeutics (TCT); October 31. 2017; Denver, Colorado.
27. Cadeau, JC.Interatrial shunting for treating heart failure: early andlate results of the first in human experience with the V waveinteratrial shunt system. Presented at ACC 2018 March 12 2018.
28.• Patel MB, Samuel BP, Girgis RE, et al. Implantable atrial flowregulator for severe, irreversible pulmonary arterial hypertension.EuroIntervention. 2015;11:706–9. This case report demonstratesthe possible use of left atrial decompression in a patient withprior ASD closure devices. The AFR device ( Mia Medical,Istanbul, Turkey) was successfully deployed and improved thepatients symptoms.
29. Ramasamy R, Pavithran S, Sivakumar K, Vettukattil JJ. Atrialseptostomy with a predefined diameter using a novel occlutechatrial flow regulator improves symptoms and cardiac index in pa-tients with severe pulmonary arterial hypertension. CatheterCardiovasc Interv. 2017;90:1145–53.
30. Pellicori P, Cleland JG. Heart failure with preserved ejection frac-tion. Clin Med (Lond). 2014;14(Suppl 6):s22–8.
31. Sondergaard L, Kasner SE, Rhodes JF, et al. Patent foramen ovaleclosure or antiplatelet therapy for cryptogenic stroke. N Engl JMed.2017;377:1033–42.
32. Sedgwick P. The Hawthorne effect. BMJ. 2011;344:d8262.
85 Page 8 of 8 Curr Cardiol Rep (2018) 20:85