updates on the pathogenesis iga nephropathy and iga ...€¦ · updates on the pathogenesis iga...
TRANSCRIPT

29th Annual Meeting of the Glomerular Disease Collaborative Network
Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP)
J. Charles Jennette, M.D.Brinkhous Distinguished Professor and Chair of Pathology and Laboratory Medicine
University of North Carolina at Chapel Hill
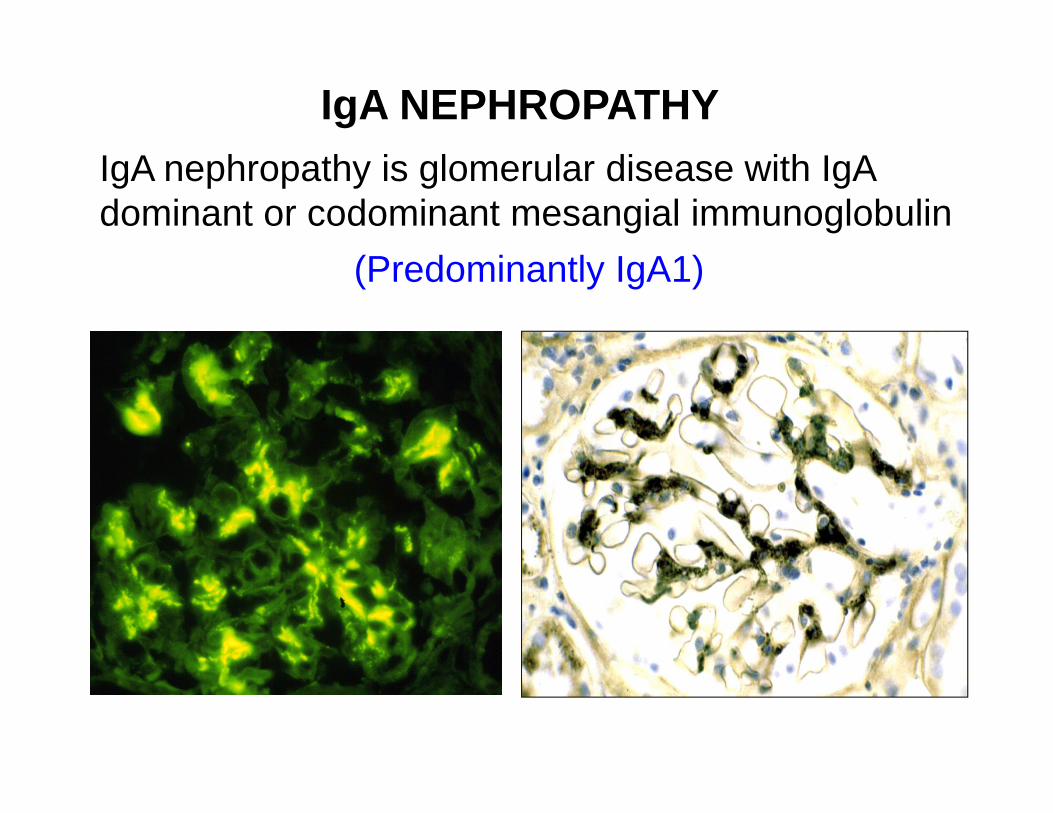
IgA NEPHROPATHYIgA nephropathy is glomerular disease with IgA dominant or codominant mesangial immunoglobulin
(Predominantly IgA1)

0
100
200
300
400
500
600
700
1‐9 10‐19 20‐29 30‐39 40‐49 50‐59 60‐69 70‐79 >79
Lupus IgA Nep
ANCA GN TBM Lesion
Fibrillary GN Post Infect GN
Anti‐GBM GN Hereditary Nep
Causes of Nephritis
Lupus GN
IgAN
ANCA GN
Frequency of Renal Biopsy Diagnoses vs Age at UNC from 1985-2007
Jennette JC, Falk RJ. NKF Primer on Kidney Disease, 6th Ed, 2014, Chapter 16:152-163
Anti-GBM GN

IgA Nephropathy
mesangial immune complex deposits

Focal thinning of the GBM
Mesangial dense deposits
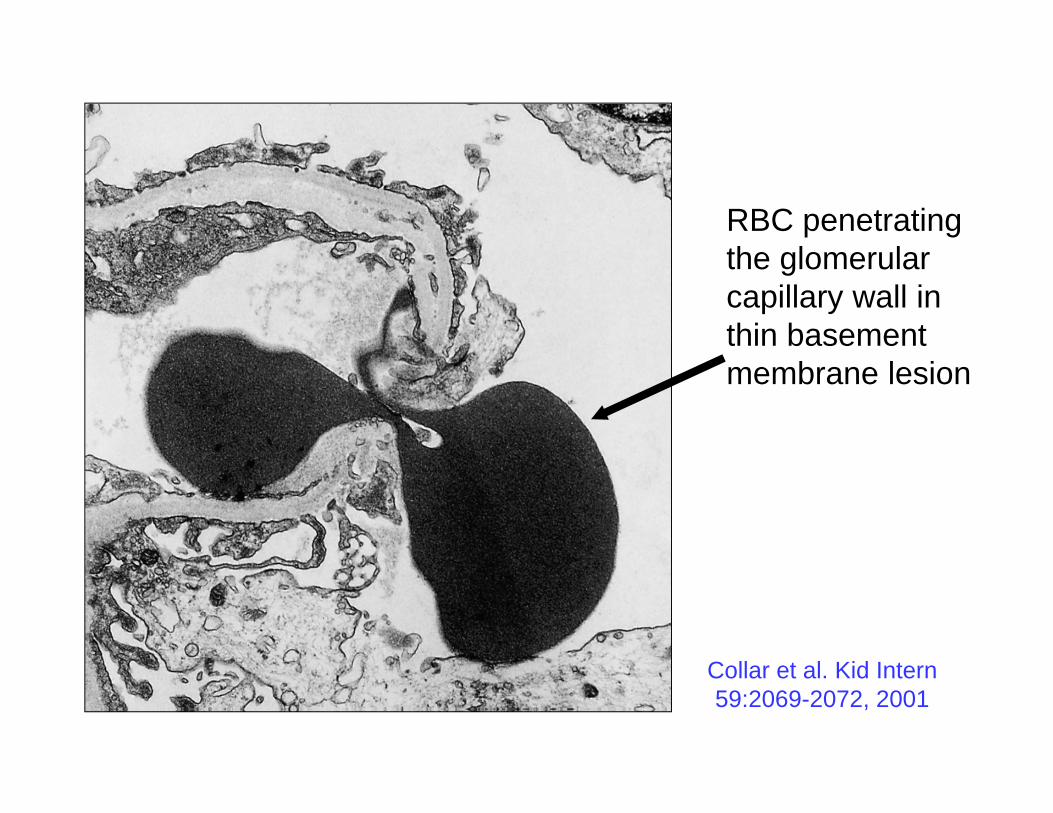
RBC penetrating the glomerular capillary wall in thin basement membrane lesion
Collar et al. Kid Intern 59:2069-2072, 2001

HistologicallyNormal
Glomeruli
Focal or DiffuseMesangioprolifertiveGlomerulonephritis
Focal or DiffuseProliferative or Necrotizing
Glomerulonephritis
Focal or DiffuseSclerosing
Glomerulonephritis
CrescenticGlomerulonephritis
Frequency in Biopsy Specimens
IgA Nephropathy

HistologicallyNormal
Glomeruli
Focal or DiffuseMesangioprolifertiveGlomerulonephritis
Focal or DiffuseProliferative or Necrotizing
Glomerulonephritis
Focal or DiffuseSclerosing
Glomerulonephritis
CrescenticGlomerulonephritis
IgA Nephropathy
AsymptomaticHem / Proteinuria
Mild to Moderate Nephritis Severe to
Rapidly progressive Nephritis
Chronic Nephritis

Analysis of the Oxford Data Using the ISN/RPS Classification Approach
J C Jennette, Y Hu, SL Hogan, S Troyanov, M Haas. Unpublished data

IgA NEPHROPATHY
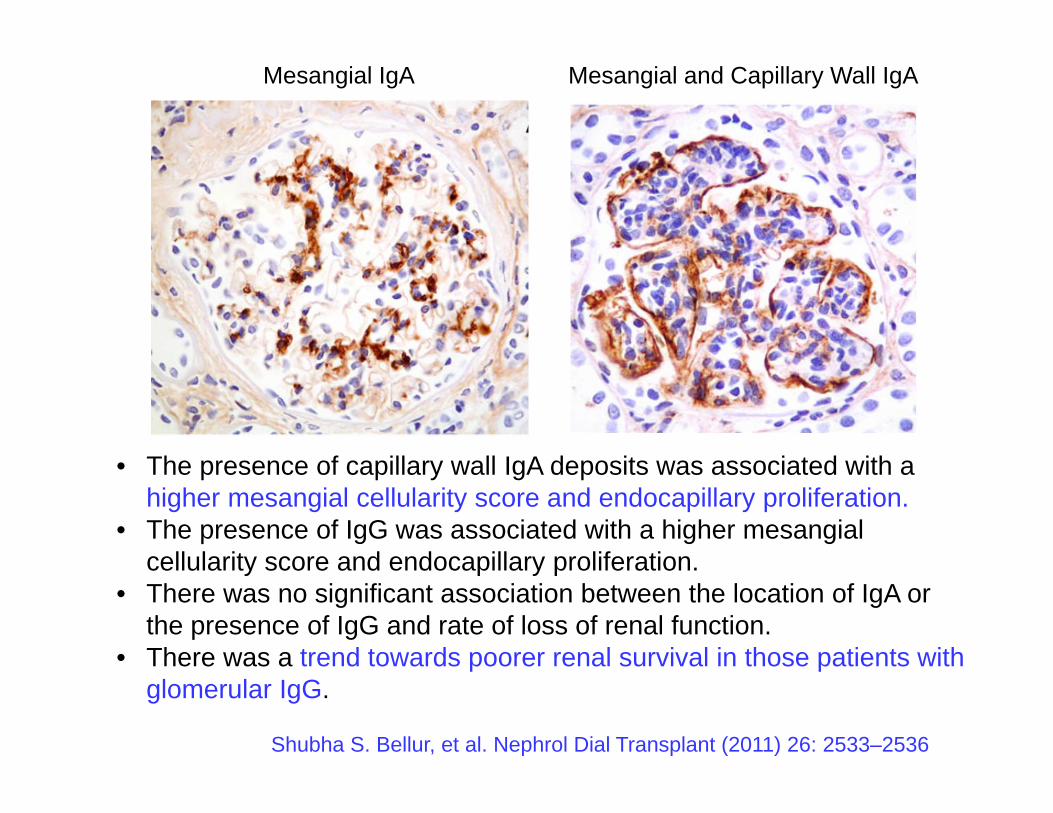
Mesangial IgA Mesangial and Capillary Wall IgA

0
510
1520
25
3035
4045
50
% IgA Nephropathy Specimens with Capillary Wall Electron Dense Deposits Relative to Histologic Phenotype
n=447
Mesangial IgA Mesangial and Capillary Wall IgA
Shubha S. Bellur, et al. Nephrol Dial Transplant (2011) 26: 2533–2536
• The presence of capillary wall IgA deposits was associated with a higher mesangial cellularity score and endocapillary proliferation.
• The presence of IgG was associated with a higher mesangial cellularity score and endocapillary proliferation.
• There was no significant association between the location of IgA or the presence of IgG and rate of loss of renal function.
• There was a trend towards poorer renal survival in those patients with glomerular IgG.

IgA nephropathy probably can be caused by multiple different etiologies and pathogenic processes:
1) abnormally glycosylated IgA
2) antibodies against abnormally glycosylated IgA
3) reduced clearance of circulating IgA complexes
4) increased affinity for or reduced clearance of IgA deposits from the glomerular mesangium
5) excessive IgA antibody production in response to mucosal antigen exposure
6) increased permeability of mucosa to antigen
7) combinations of these factors
Aberrant glycosylation of IgA1 may be caused by genetically determined aberrant mucosal immune responses to infections.
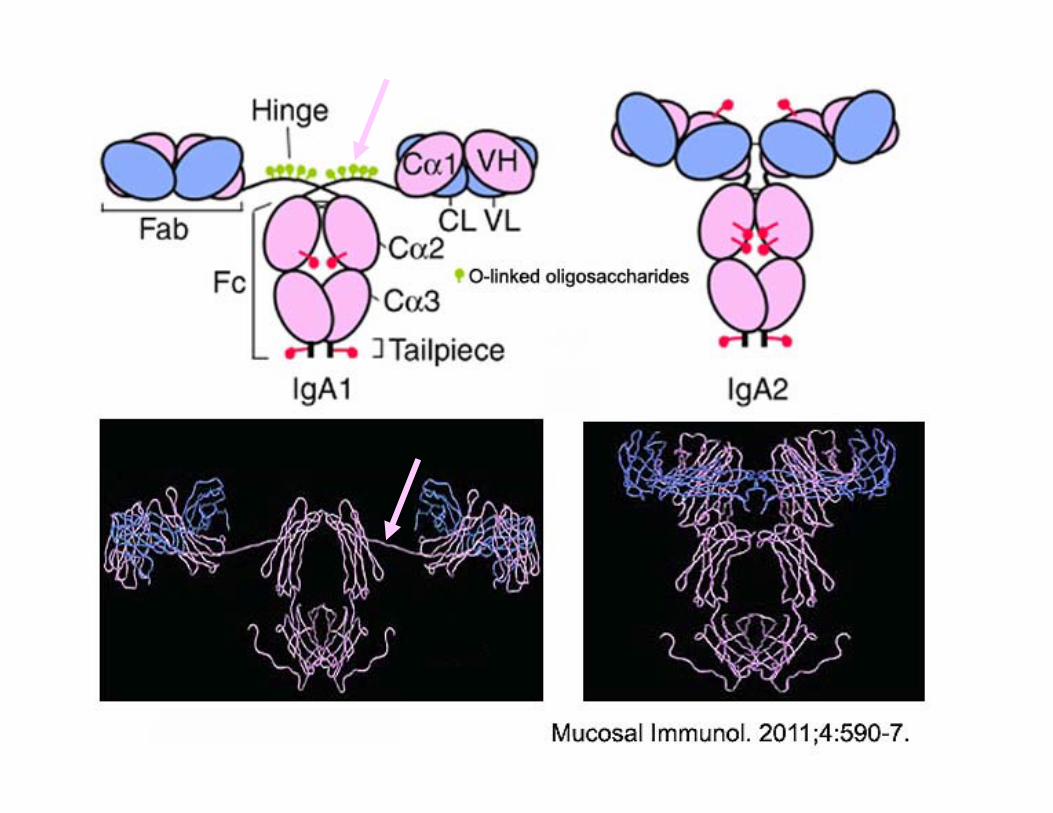

IgA1 but not IgA2 has a hinge region with 0-linked glycan chains. Each O-glycan chain is based on a core N-acetyl galactosamine unit (GalNAc) O-linked to serine or threonine. This can exist alone but usually carries galactose and sialic acid. Each IgA1 molecule can carry a mixture of chain types.
Ser/Thr-O-GalNAc
Ser/Thr-O-GalNAc--Galactose
Ser/Thr-O-GalNAc--Galactose-Sialic Acid
Ser/Thr-O-GalNAc----Galactose-Sialic Acid-
Sialic Acid
VL
CLVH
CH1
CH2
CH3
Hinge Region
IgA1
In IgA nephropathy and IgA vasculitis, serum IgA1 has reduced terminal sialation and galactosylation (X), resulting in increased
exposure of terminal GalNAc.

Patients with IgA nephropathy have increased serum galactose-deficient IgA1 levels. Moldoveanu Z, Wyatt RJ, et al. Kidney Int. 2007;71:1148-54.
A lectin that recognizes N-acetylgalactosamine was used in an ELISA to measure serum galactose-deficient IgA1. The diagnostic sensitivity 76.5%, with specificity 94%; the positive predictive value was 88.6% and the negative predictive value was 78.9%.

Abnormal IgA glycosylation in Henoch-Schonlein purpura restricted to patients with clinical nephritis. Allen AC, Willis FR, Beattie TJ, Feehally J. Nephrol Dial Transplant. 1998 Apr;13(4):930-4.
Children with HSP nephritis showed significantly higher IgA1-VV binding than children with HSP lacking renal involvement (P=0.004), children with post-streptococcal GN (P=0.002), or control children (P=0.005).
Adults with IgAN showed significantly higher IgA1-VV binding than adults with non-IgA glomerulonephritis or adult controls. There was no difference in IgA1-VV binding between adults with HSPN and IgAN.

Aberrant sialylation of serum IgA1 was associated with prognosis of patients with IgA nephropathy
Ding JX, et al. Clin Immunol. 2007;125:268-74.

Glycopeptides in higher mass range contain more sialic acids
Healthy Control
5 5 4
5 4 4
5 4 3
5 4 3
5 3 2 4 4 3
5 44 4
4 3
5 3 34 4 4
5 3GalNAcGalactoseSialic acid
1
1
11
m/z
1-2 sialic acids per glycopeptide
3-4 sialic acids per glycopeptide
IgA1 hinge glycopeptide characterization by quadrupole orthogonal acceleration time-of-flight MS & MS/MS tandem mass spectroscopy (Q-TOF LC-MS/MS)
Provided by Olivier Lardinois, PhD, UNC Kideny Center

Active IgAN
Healthy Control
Healthy Control treated with neuraminidase(=sialidase)
Quadrupole orthogonal acceleration time-of-flight tandem mass spectroscopy in MS & MS/MS modes
(Q‐TOF LC‐MS/MS)
Provided by Olivier Lardinois, PhD, UNC Kideny Center
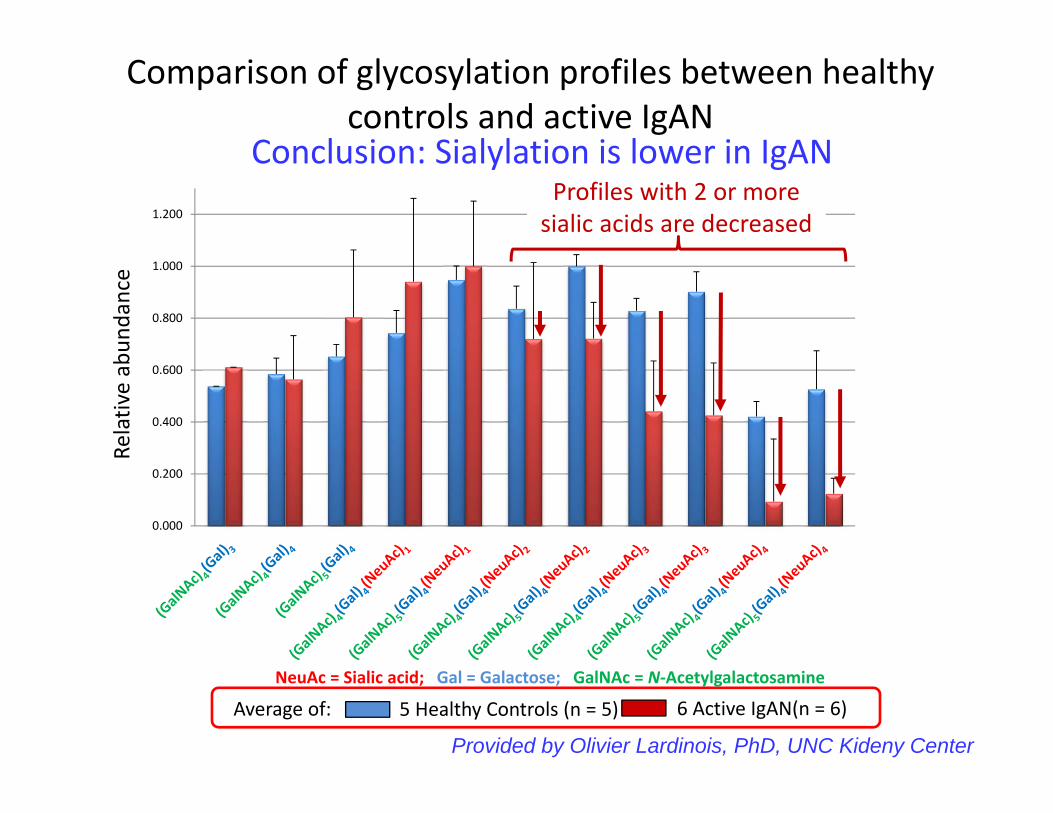
Relative abun
dance
0.000
0.200
0.400
0.600
0.800
1.000
1.200
5 Healthy Controls (n = 5)Average of: 6 Active IgAN(n = 6)
Comparison of glycosylation profiles between healthy controls and active IgAN
NeuAc = Sialic acid; Gal = Galactose; GalNAc = N‐Acetylgalactosamine
Conclusion: Sialylation is lower in IgANProfiles with 2 or more sialic acids are decreased
Provided by Olivier Lardinois, PhD, UNC Kideny Center

IgA1
IgG
Glycan-specific IgG antibodies may form immune complexes with aberrantly glycosylated IgA1
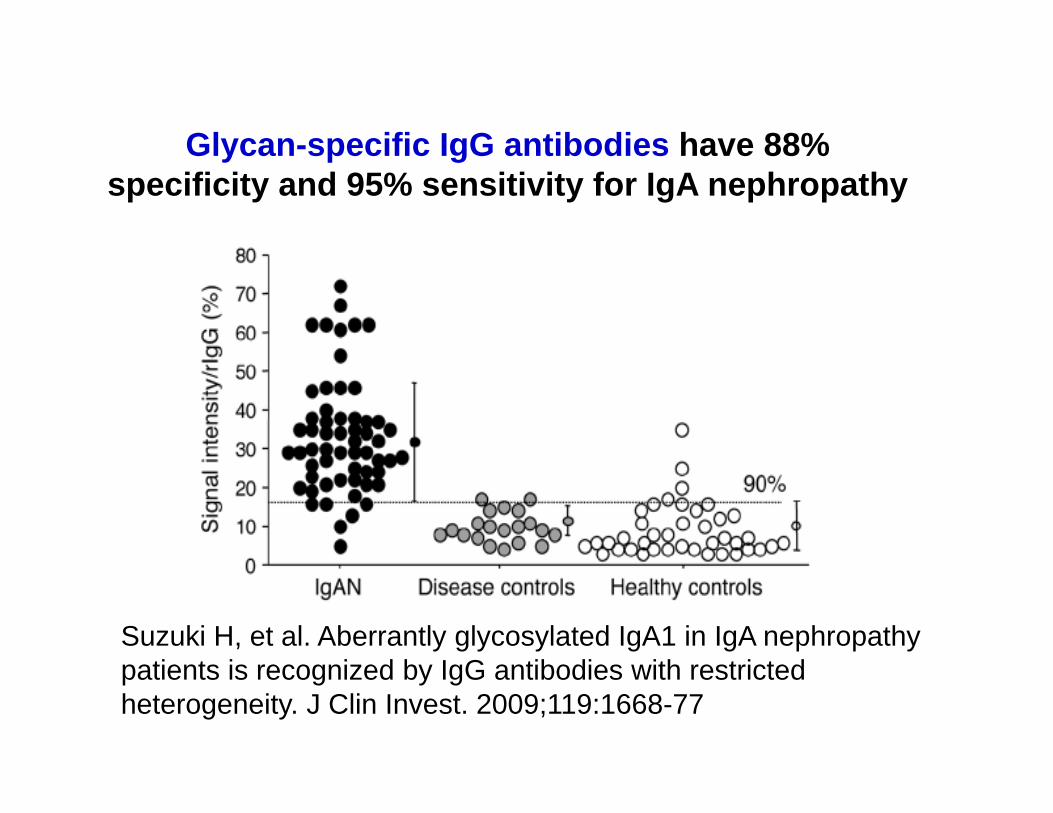
Glycan-specific IgG antibodies have 88% specificity and 95% sensitivity for IgA nephropathy
Suzuki H, et al. Aberrantly glycosylated IgA1 in IgA nephropathy patients is recognized by IgG antibodies with restricted heterogeneity. J Clin Invest. 2009;119:1668-77

Correlation between severityof hematuria/proteinuria and serum Gd-IgA1 or IgA/IgG-IC
Suzuki H, et al. Clin Exp Nephrol. 2014;18:770-7.
Hematuria 1+ to 4+
Hematuria 1+ to 4+
Proteinuria 1+ to 4+
Proteinuria 1+ to 4+
Serum Abnormal
IgA1 Glycosylation
Serum IgA-IgG Immune
Complexes

Abnormally glycosylated IgA1 molecules ( ), even in the absence of antigen, self aggregate or bind to antibodies directed against the abnormal glycosylation ( ) and localize in the glomerular mesangium where they activate complement by the lectin and alternative pathways..
Hypothesis: Glycan-specific IgG antibodies binding to abnormally gylcosylated IgA cause IgA nephropathy
Discovery of new risk loci for IgA nephropathy implicates genes involved in immunity against
intestinal pathogens.
Kiryluk K, et al. Nat Genet. 2014;46:1187-96.
• Genome-wide association study (GWAS) of IgA nephropathy in 20,612 individuals of European and East Asian ancestry.
• Multiple risk alleles, most associated with maintenance of the intestinal epithelial barrier and response to mucosal pathogens, including risk of inflammatory bowel disease.
• The risk alleles suggest host-intestinal pathogen interactions in establishing genetic susceptibility to IgAN.

IgA nephropathy probably can be caused by multiple different etiologies and pathogenic processes:
1) abnormally glycosylated IgA
2) antibodies against abnormally glycosylated IgA
3) reduced clearance of circulating IgA complexes
4) increased affinity for or reduced clearance of IgA deposits from the glomerular mesangium
5) excessive IgA antibody production in response to mucosal antigen exposure
6) increased permeability of mucosa to antigen
7) combinations of these factors
Aberrant glycosylation of IgA1 may be caused by genetically determined aberrant mucosal immune responses to infections.
