upper cervical spine fractures originally created by daniel gelb, md january 2006 updated by robert...
TRANSCRIPT
Upper Cervical Spine Fractures
Originally created by Daniel Gelb, MDJanuary 2006
Updated by Robert Morgan, MD; November 2010
Upper Cervical Spine Fractures
• Epidemiology
• Anatomy
• Imaging Characteristics
• Common Injuries
• Management Issues
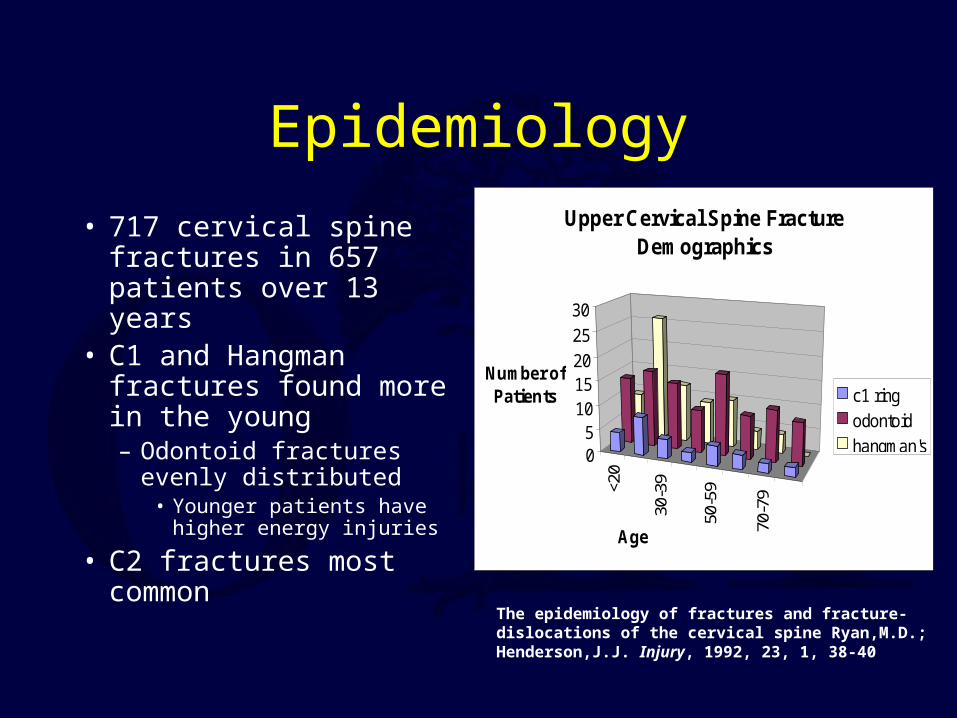
Epidemiology
• 717 cervical spine fractures in 657 patients over 13 years
• C1 and Hangman fractures found more in the young– Odontoid fractures evenly
distributed• Younger patients have higher
energy injuries
• C2 fractures most common
<20
30-3
9
50-5
9
70-7
9
05
1015202530
Number of Patients
Age
Upper Cervical Spine Fracture Demographics
c1 ringodontoidhangman's
The epidemiology of fractures and fracture-dislocations of the cervical spine Ryan,M.D.; Henderson,J.J. Injury, 1992, 23, 1, 38-40
Upper Cervical Anatomy

Upper Cervical Anatomy
• Biomechanically Specialized– Support of “large” Cranial mass– Large range of motion
• Flexion/extension
• Axial rotation
• Unique osteological characteristics
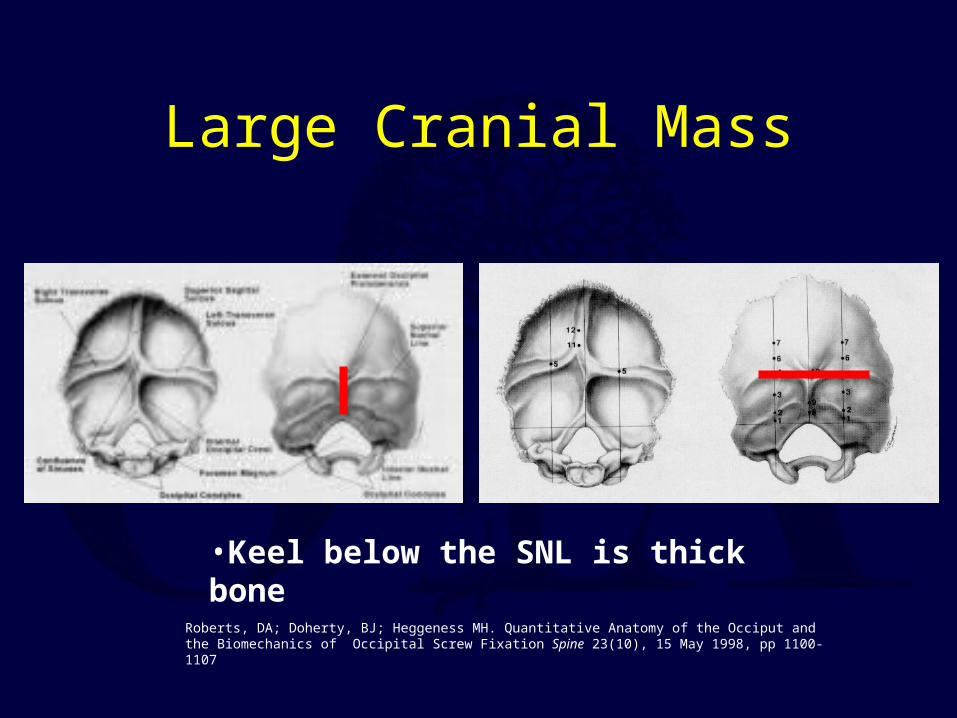
Large Cranial Mass
Roberts, DA; Doherty, BJ; Heggeness MH. Quantitative Anatomy of the Occiput and the Biomechanics of Occipital Screw Fixation Spine 23(10), 15 May 1998, pp 1100-1107
•Keel below the SNL is thick bone
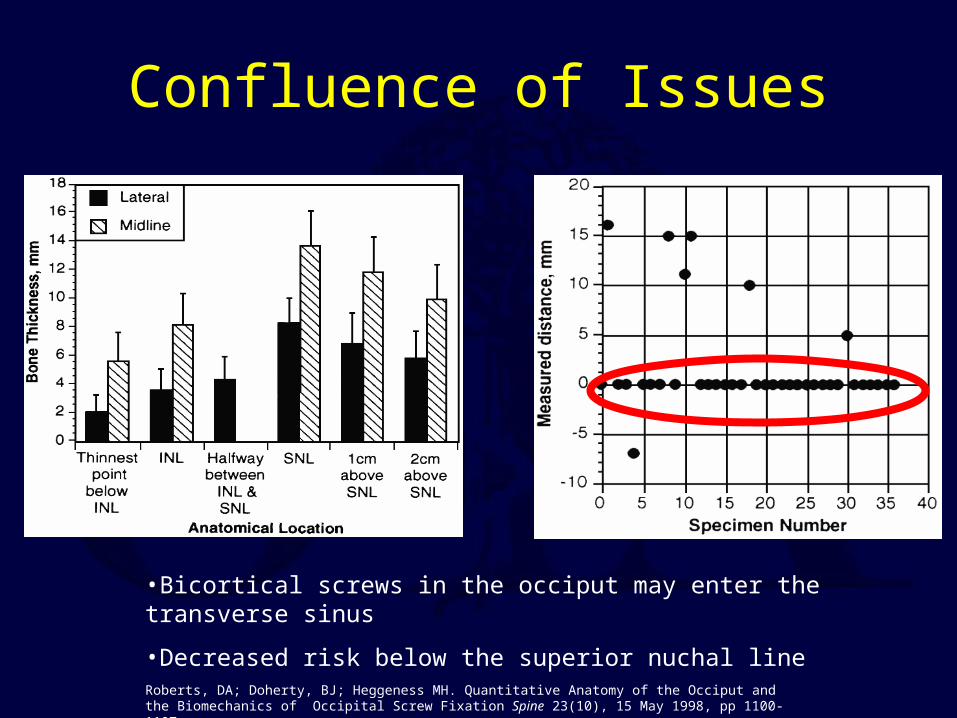
Confluence of Issues
Roberts, DA; Doherty, BJ; Heggeness MH. Quantitative Anatomy of the Occiput and the Biomechanics of Occipital Screw Fixation Spine 23(10), 15 May 1998, pp 1100-1107
•Bicortical screws in the occiput may enter the transverse sinus
•Decreased risk below the superior nuchal line
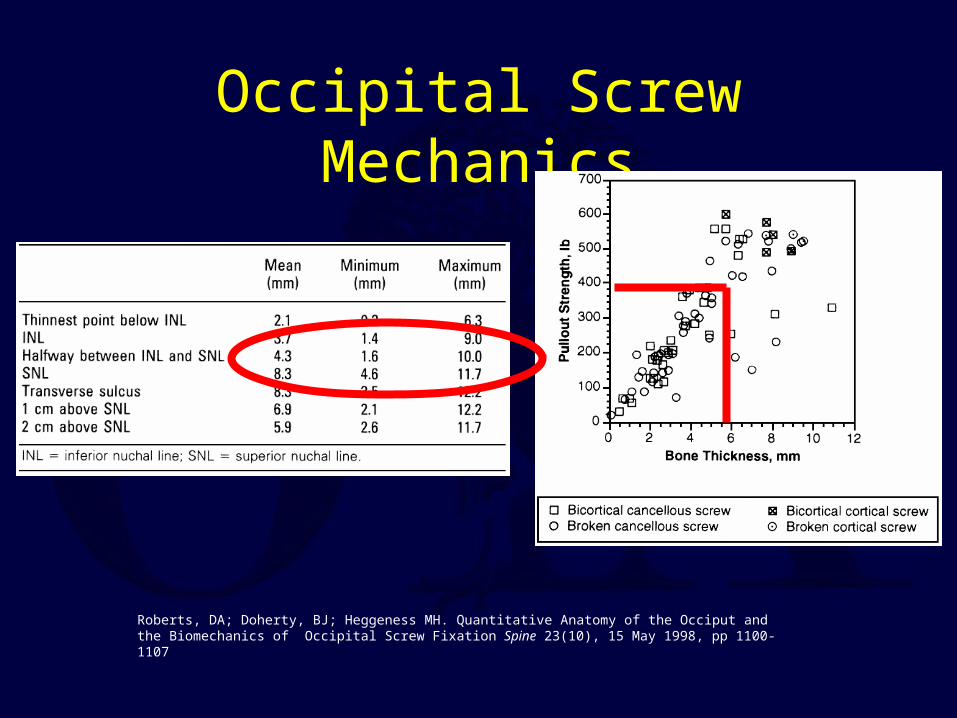
Occipital Screw Mechanics
Roberts, DA; Doherty, BJ; Heggeness MH. Quantitative Anatomy of the Occiput and the Biomechanics of Occipital Screw Fixation Spine 23(10), 15 May 1998, pp 1100-1107
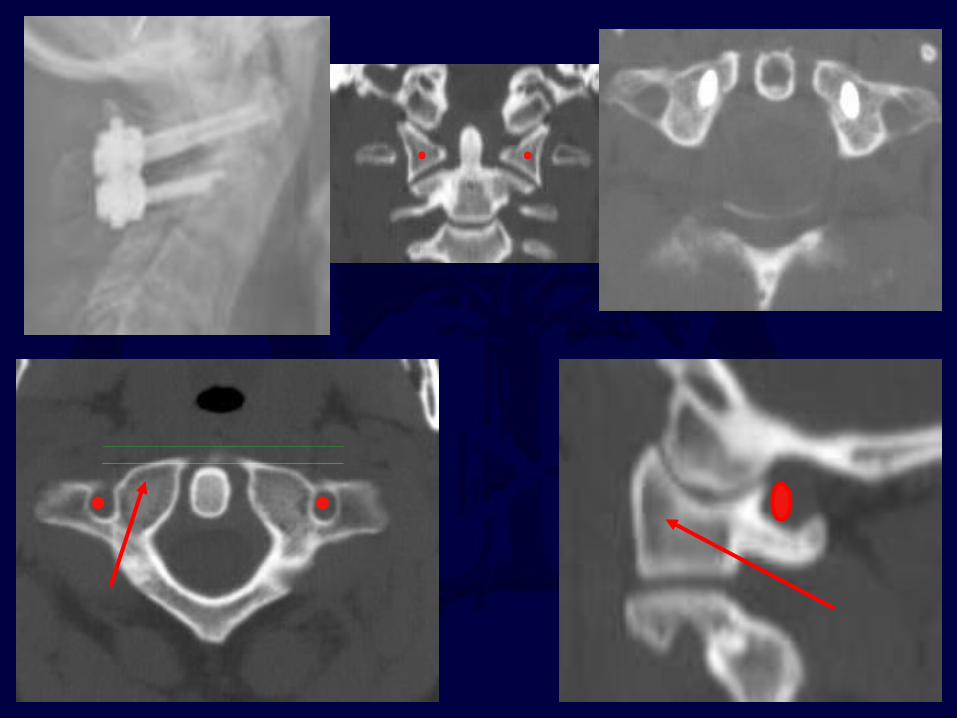
The course of the vertebral artery through C1 and C2 determines the possibility of placing
screws for fixation of fractures and dislocations
• C1 lateral mass screws
• C1-2 transarticular screws
• C2 pedicle/pars screws
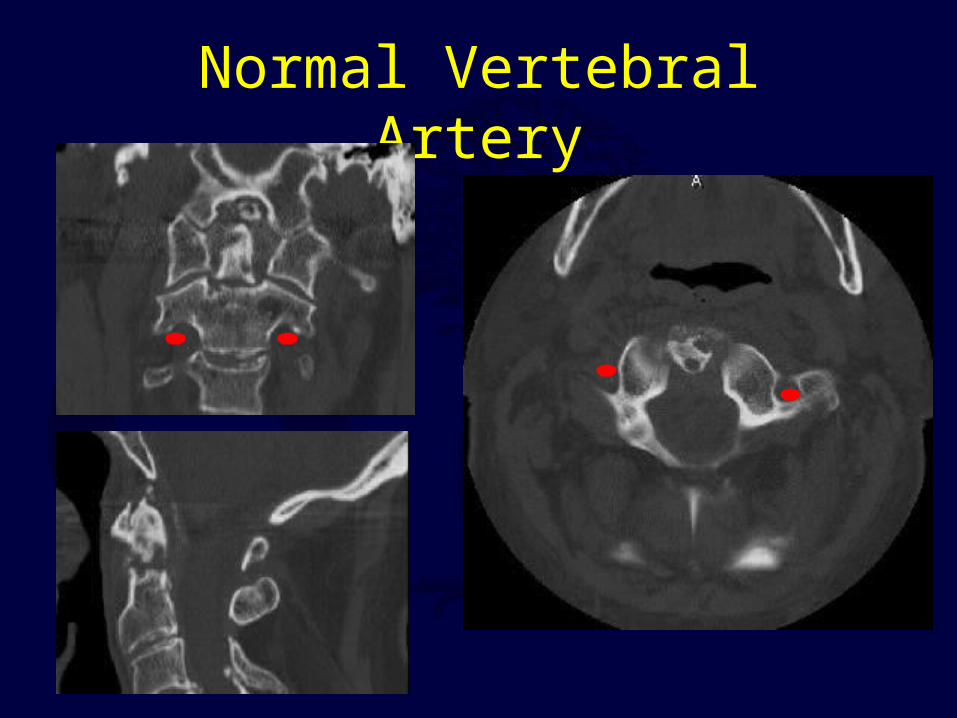
Normal Vertebral Artery
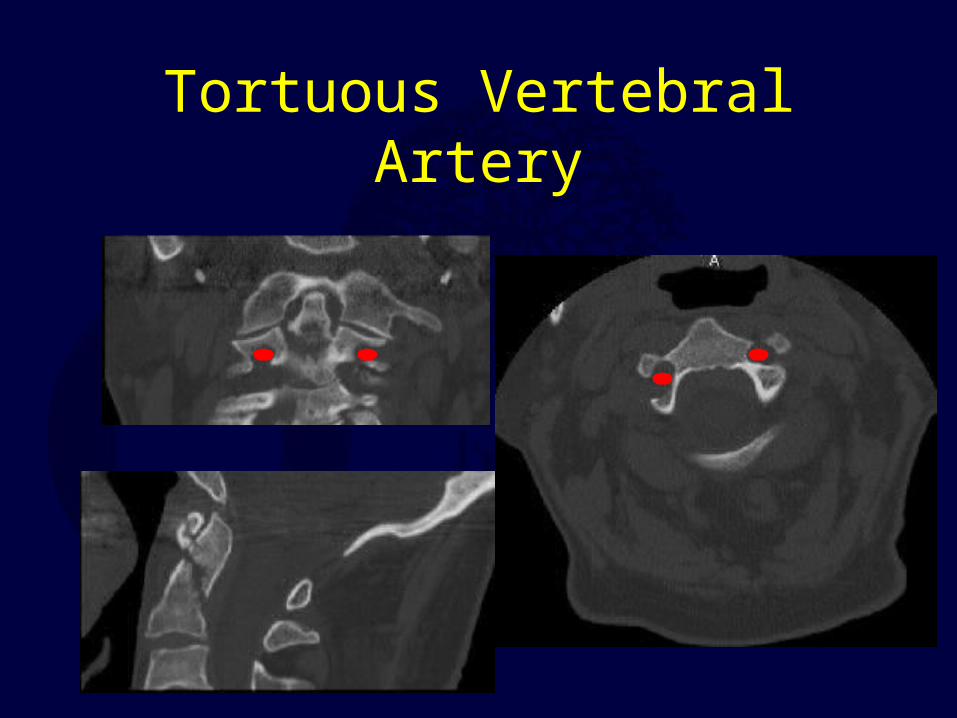
Tortuous Vertebral Artery
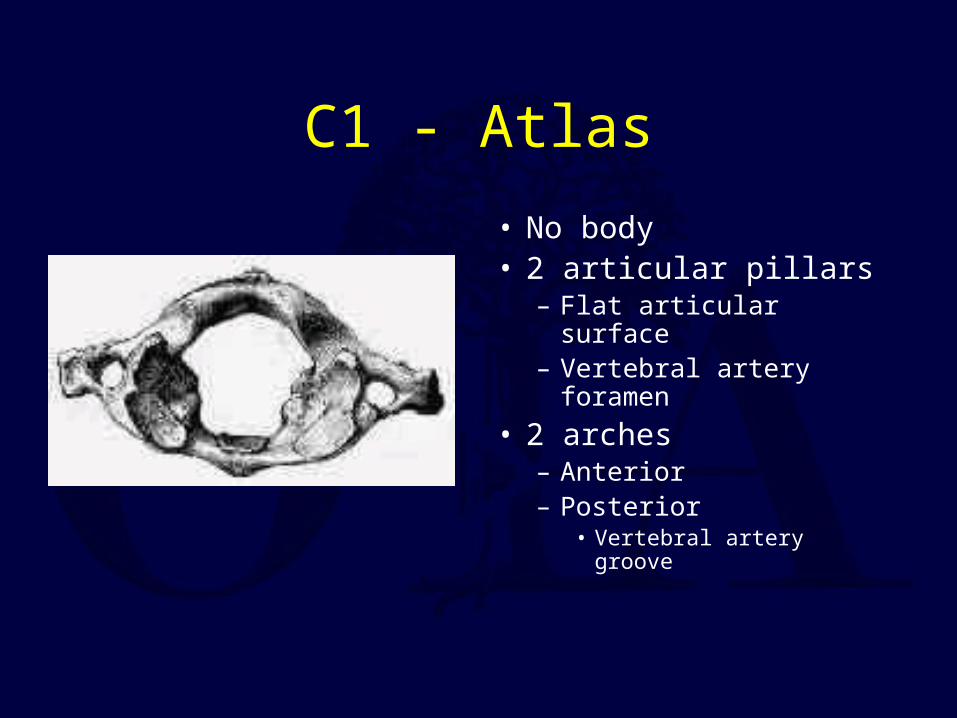
C1 - Atlas
• No body• 2 articular pillars
– Flat articular surface– Vertebral artery
foramen
• 2 arches– Anterior– Posterior
• Vertebral artery groove
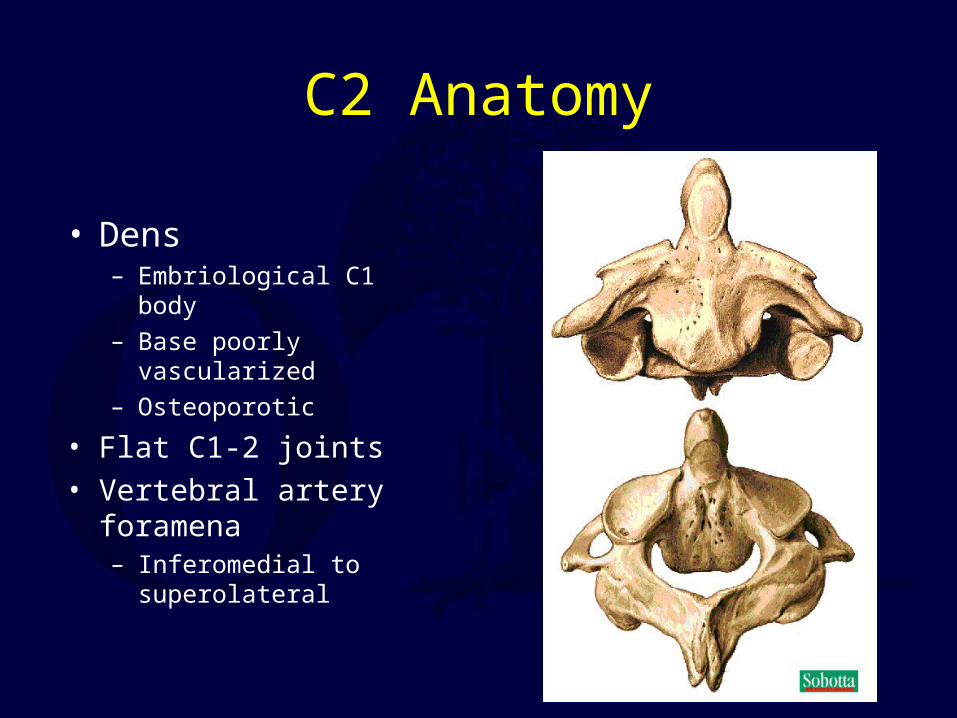
C2 Anatomy
• Dens– Embriological C1 body
– Base poorly vascularized
– Osteoporotic
• Flat C1-2 joints
• Vertebral artery foramena– Inferomedial to
superolateral
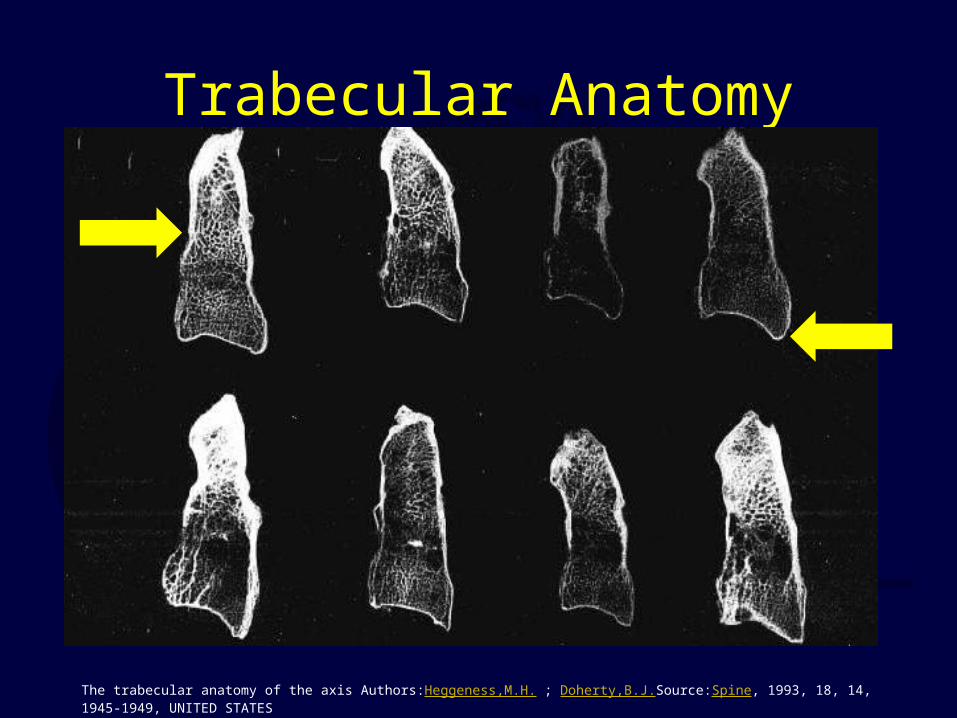
Trabecular Anatomy
The trabecular anatomy of the axis Authors:Heggeness,M.H. ; Doherty,B.J.Source:Spine, 1993, 18, 14, 1945-1949, UNITED STATES
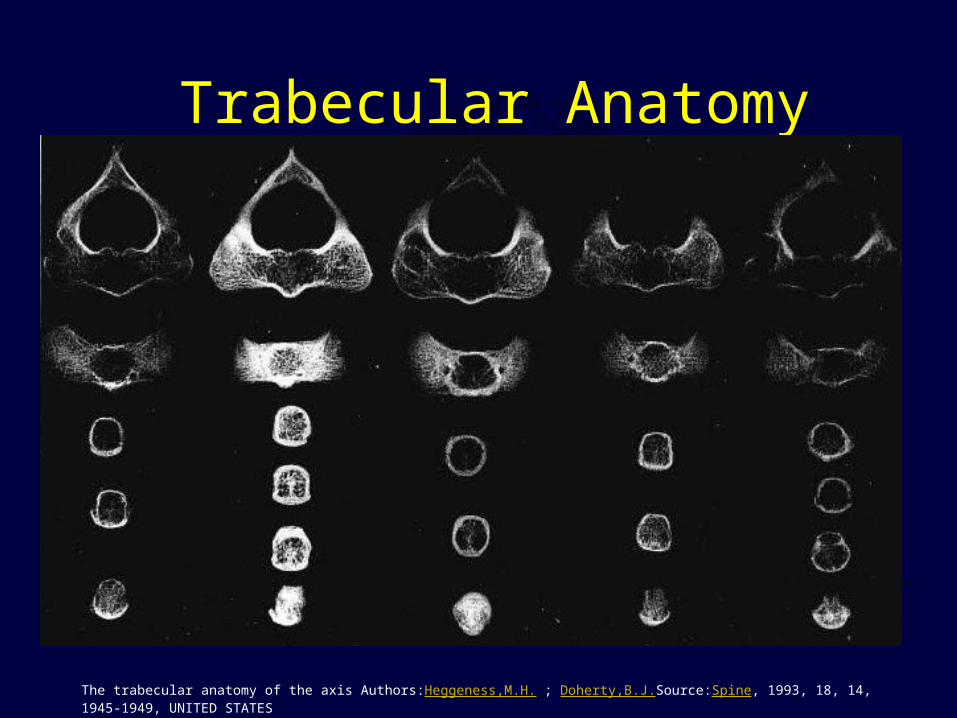
Trabecular Anatomy
The trabecular anatomy of the axis Authors:Heggeness,M.H. ; Doherty,B.J.Source:Spine, 1993, 18, 14, 1945-1949, UNITED STATES
Anatomy – The Ligaments
• Allow for the wide ROM of upper C-spine while maintaining stability
• Classified according to location with respect to vertebral canal– Internal:
• Tectorial membrane• Cruciate ligament – including transverse ligament• Alar and apical ligaments
– External• Anterior and posterior atlanto-occipital membranes• Anterior and posterior atlanto-axial membranes• Articular capsules and ligamentum nuchae
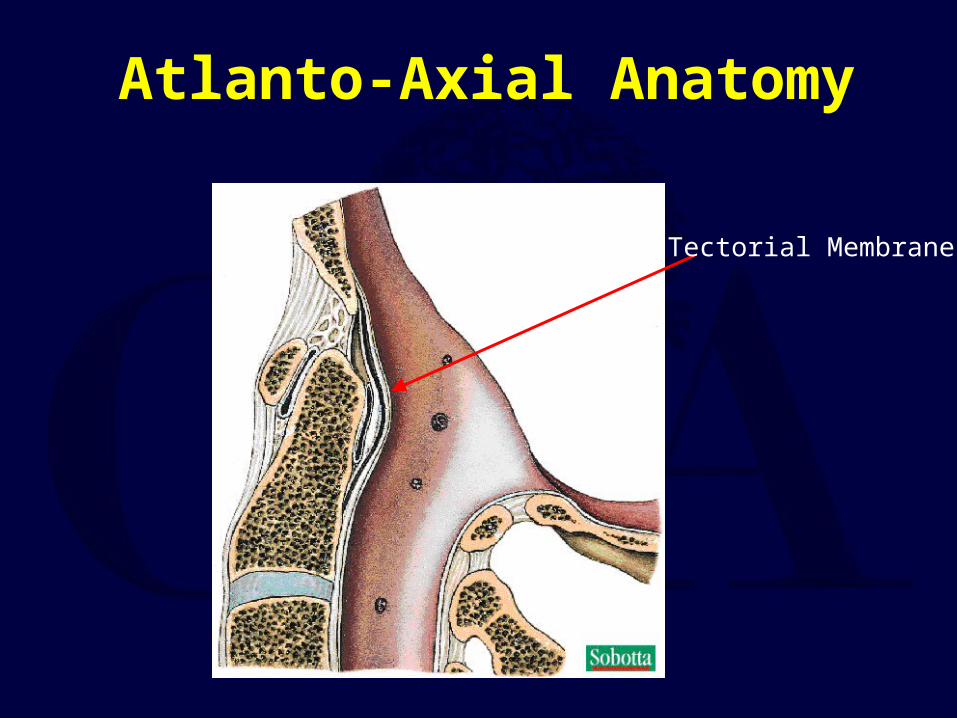
Atlanto-Axial Anatomy
Tectorial Membrane
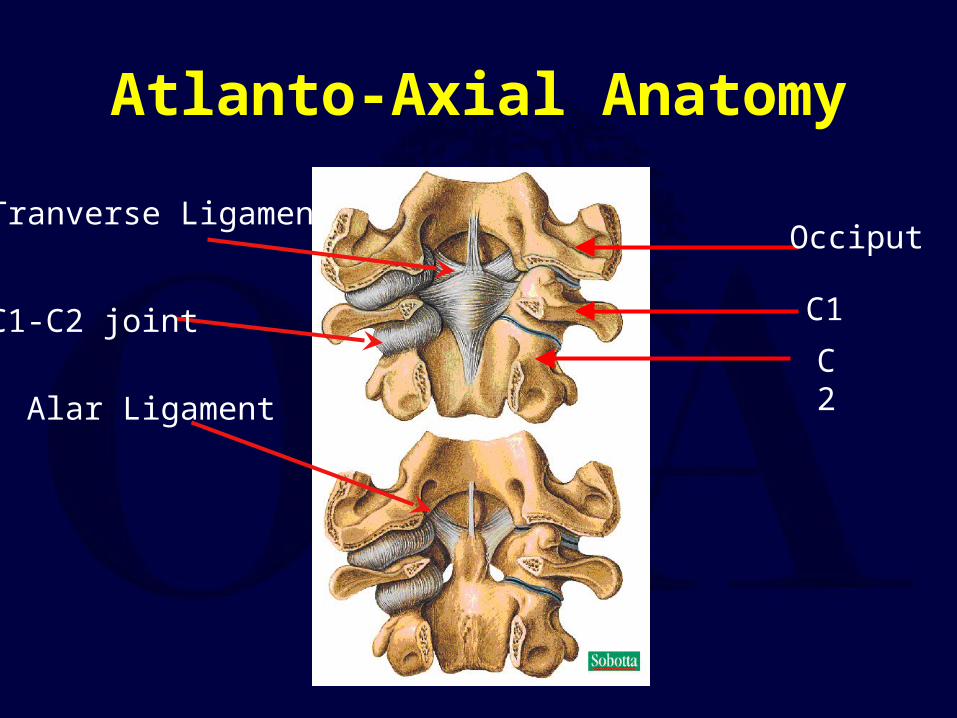
Atlanto-Axial Anatomy
Occiput
C1
C2
Tranverse Ligament
C1-C2 joint
Alar Ligament
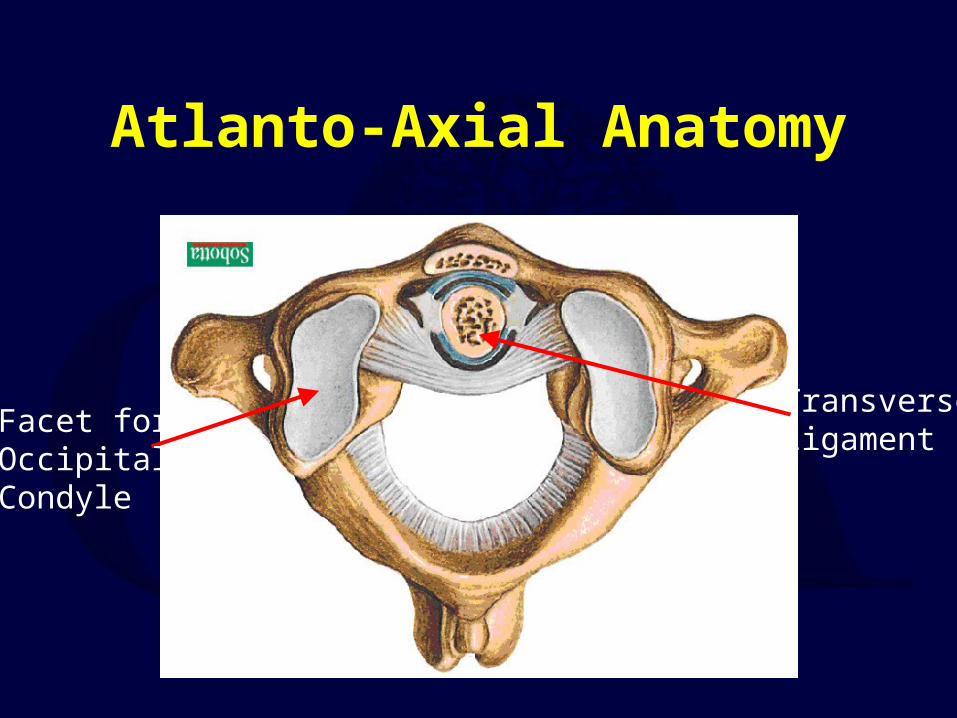
Atlanto-Axial Anatomy
TransverseLigament
Facet forOccipitalCondyle
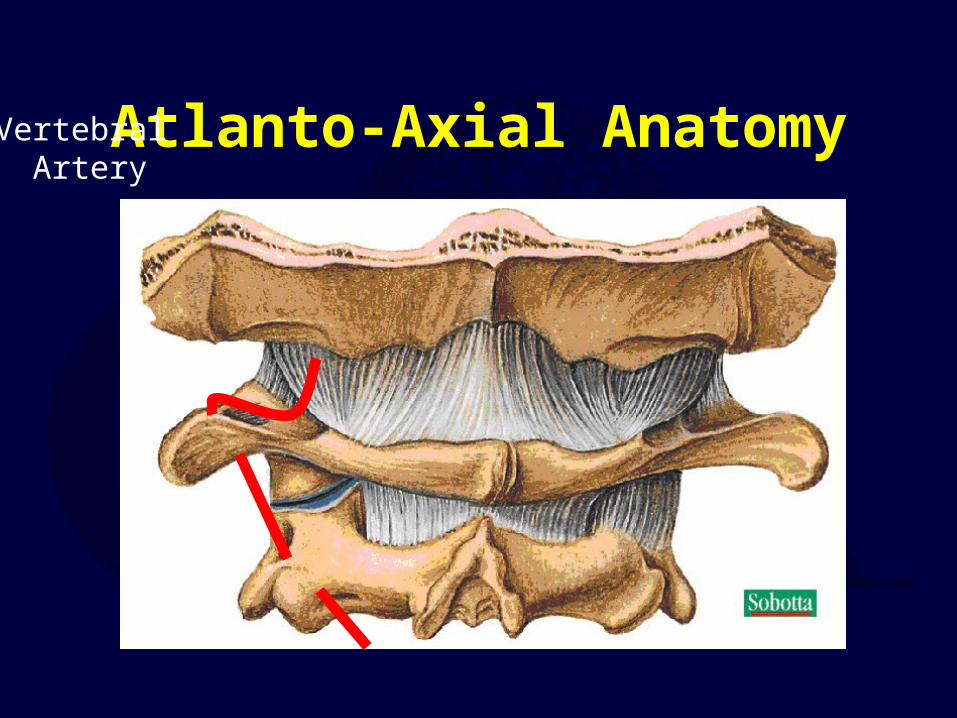
Atlanto-Axial AnatomyVertebral Artery
Radiographic Evaluation

Plain Radiographic EvaluationPlain Radiographic Evaluation
Lateral ViewPrevertebral Swelling
Soft Tissue Shadow<6mm at C2Concave/Flat
Pre-dental space < 3mm Atlanto-Occipital Joint CongruenceRadiographic Lines*
Open Mouth APDistractionC1-2 Symmetry
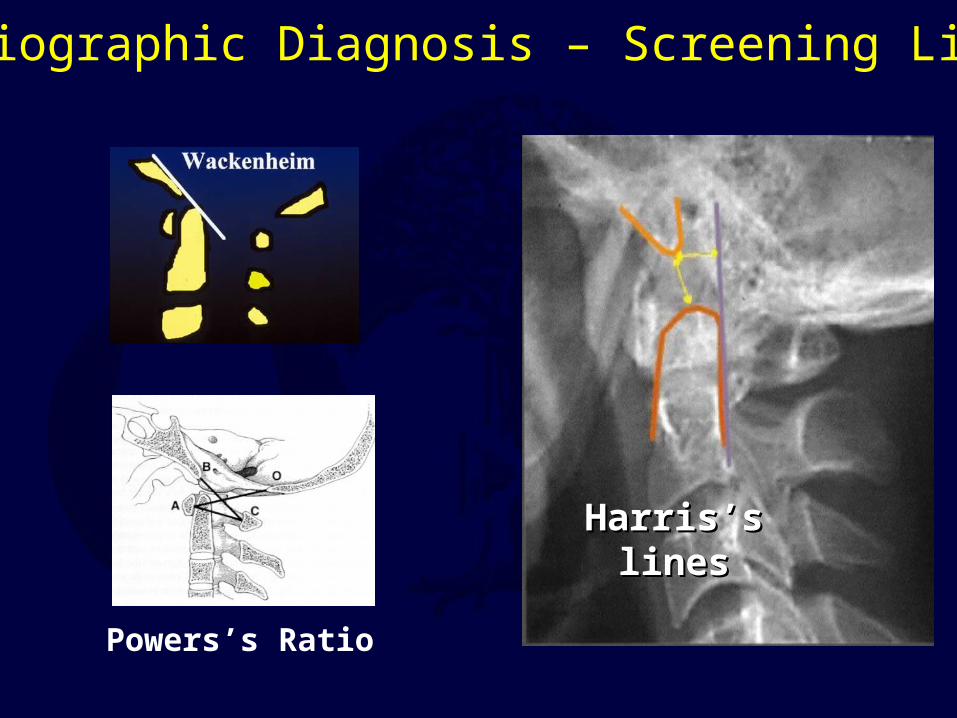
Radiographic Diagnosis – Screening Lines
Powers’s Ratio
Harris’s linesHarris’s lines
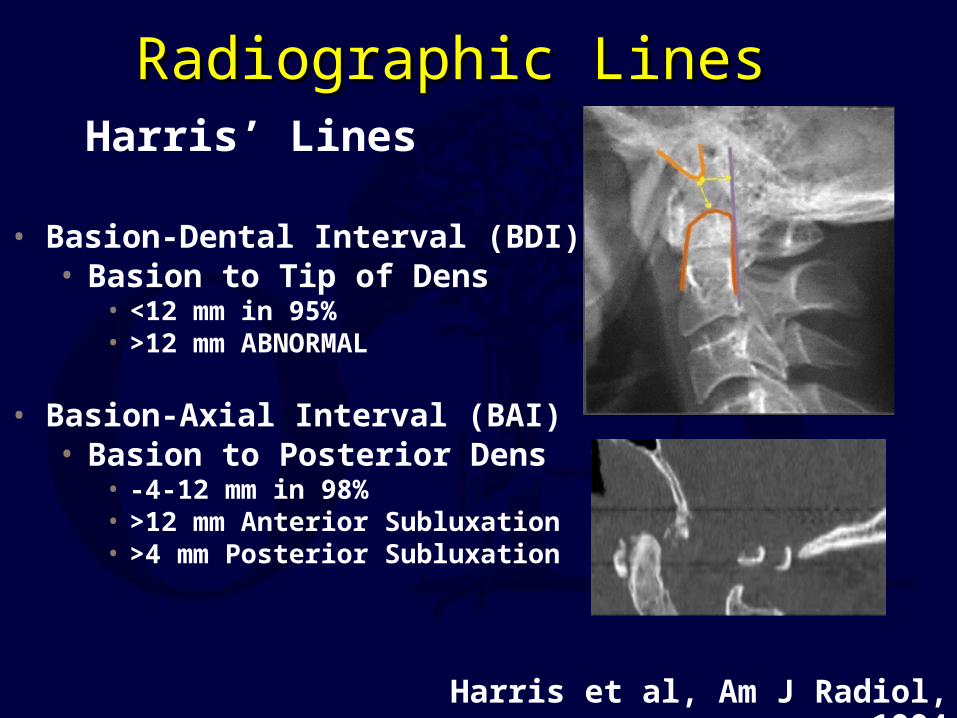
Radiographic LinesRadiographic Lines
Harris et al, Am J Radiol, 1994
• Basion-Dental Interval (BDI)• Basion to Tip of Dens
• <12 mm in 95% • >12 mm ABNORMAL
• Basion-Axial Interval (BAI)• Basion to Posterior Dens
• -4-12 mm in 98%• >12 mm Anterior Subluxation• >4 mm Posterior Subluxation
Harris’ Lines

Radiographic Lines
• BC/OA– >1 considered abnormal
• Limited Usefulness
• Positive only in Anterior Translational injuries
• False Negative with pure distraction
Powers et al, Neurosurg, 1979
Powers’ Ratio
Radiographic DiagnosisRadiographic Diagnosis
CT Scan
• Same rules as with plain films• Better visualization of cranio-
cervical junction• Subluxation• Focal hematomas• Occipital condyle fractures• Dens fractures

Radiographic DiagnosisMRI
Increased Signal Intensity in :
• C0-C1Joint• C1-2 Joint• Spinal Cord• Cranio-cervical
ligaments• Pre-vertebral
soft tissues
Warner et al, Emerg Radiol, 1996
Dickman et al, J Neurosurg, 1991
Upper Cervical Spine Fractures
• Common Injuries– Occipital Condyle
Fracture
– Craniocervical sprain?
– C1 ring injuries
– Odontoid Fracture
– Hangman’s Fracture
• Uncommon Injuries– Craniocervical
Dislocation
– Rotatory subluxation

Occipital Condyle FractureOccipital Condyle Fracture
Type I
Impaction Fracture
Type II
Extension of basilar skull
fracture
Type IIIALAR ligament Avulsion
Anderson ,SPINE 1988Tuli, NEUROSURGERY, 1997

Cranio-cervical Dislocation
• Antlanto-Occipital Joint
• Occipito-Cervical Joint
• Cranio-cervical Joint
• Atlanto-Axial Joint
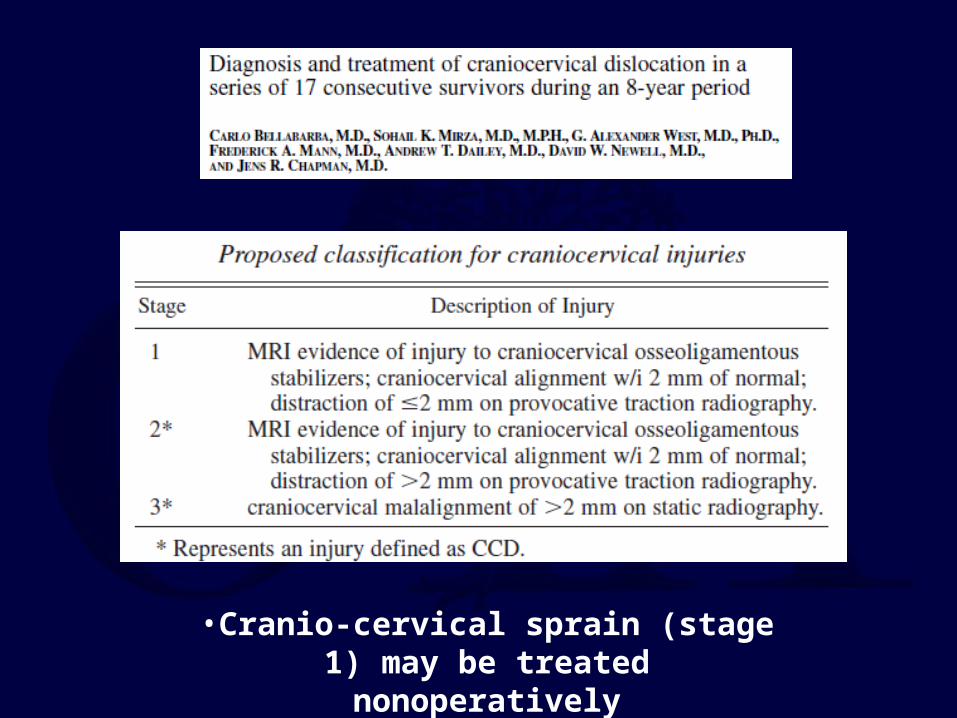
•Cranio-cervical sprain (stage 1) may be treated nonoperatively
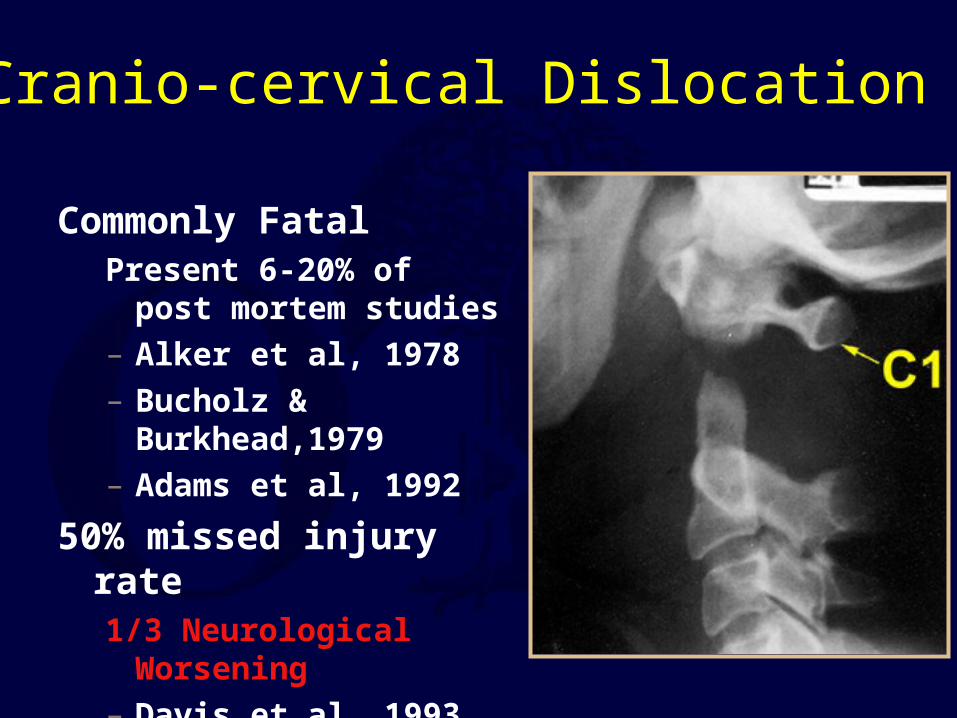
Cranio-cervical Dislocation
Commonly FatalPresent 6-20% of post
mortem studies
– Alker et al, 1978
– Bucholz & Burkhead,1979
– Adams et al, 1992
50% missed injury rate1/3 Neurological Worsening
– Davis et al, 1993

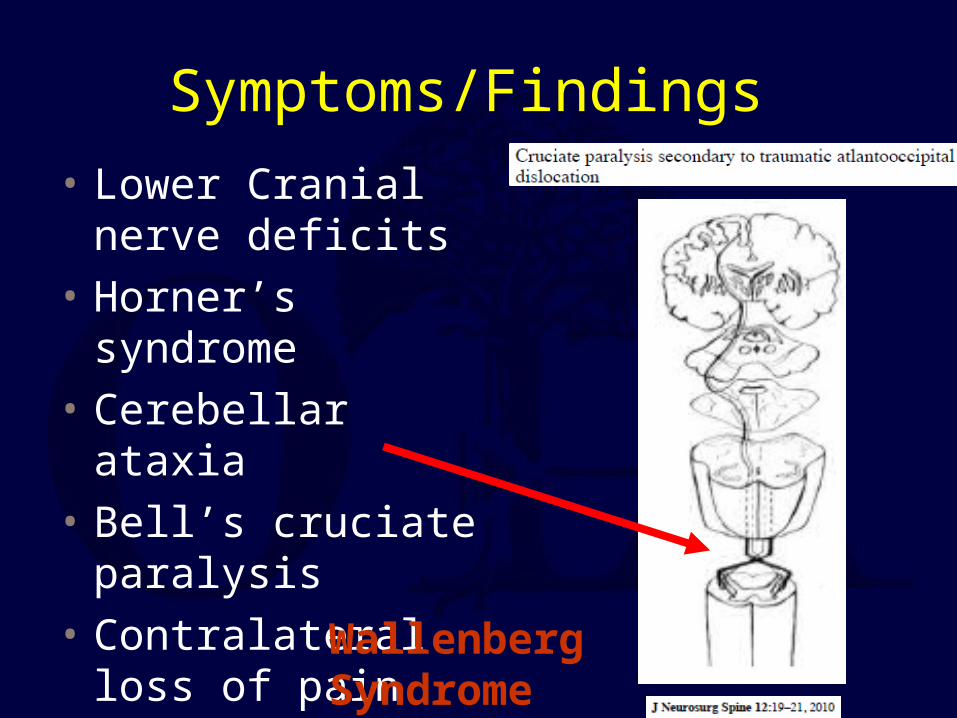
Symptoms/Findings
• Lower Cranial nerve deficits
• Horner’s syndrome
• Cerebellar ataxia
• Bell’s cruciate paralysis
• Contralateral loss of pain and temperature
Wallenberg Syndrome
www.med.yale.comwww.meddean.luc.edu
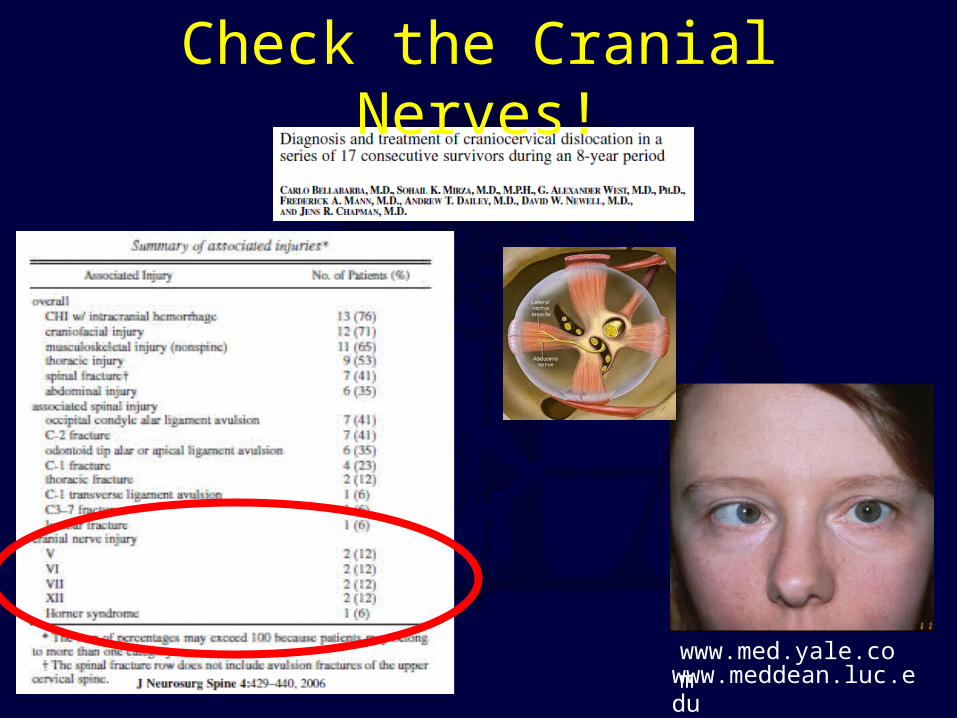
Check the Cranial Nerves!
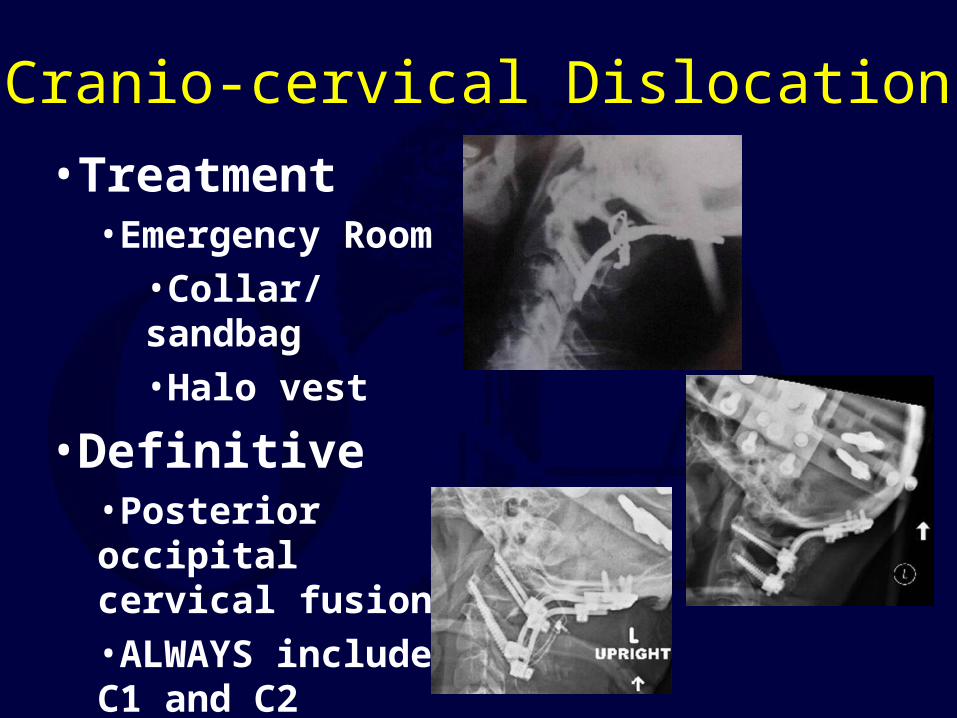
Cranio-cervical Dislocation
•Treatment•Emergency Room
•Collar/sandbag•Halo vest
•Definitive•Posterior occipital cervical fusion•ALWAYS include C1 and C2
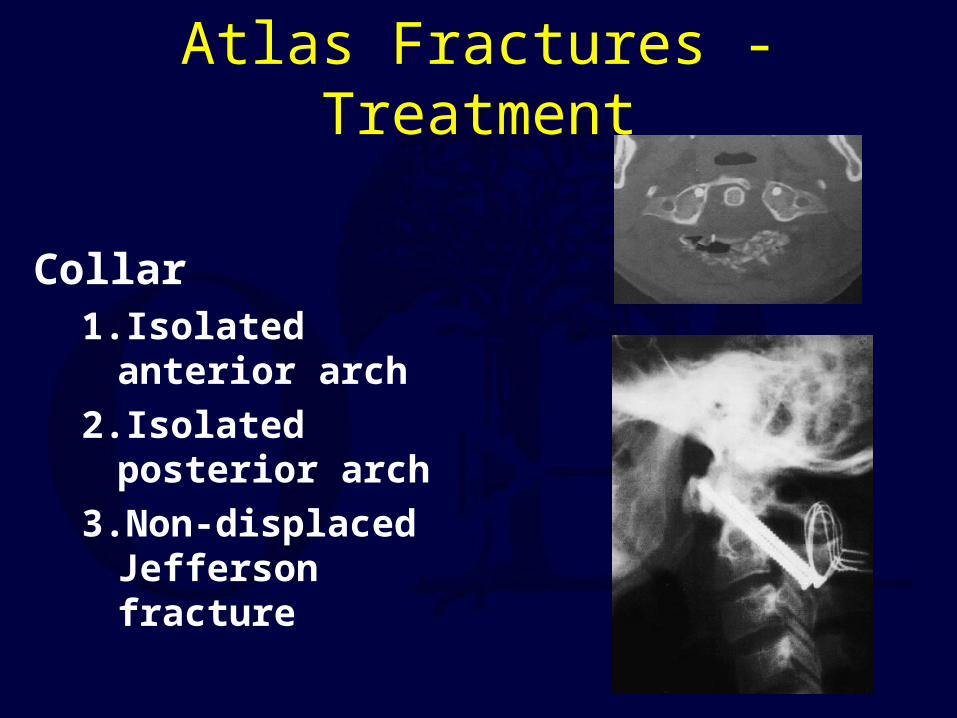
Atlas Fractures - Treatment
Collar1. Isolated anterior
arch
2. Isolated posterior arch
3.Non-displaced Jefferson fracture

Atlas Fractures - Treatment
Displaced <6.9 mm•Halo vest * 3 mos
Displaced >6.9 mm•Halo traction (reduction) * several weeks followed by halo vest•Immediate halo vest•Posterior C1-2 fusion (unable to tolerate halo)
After brace treatment complete confirm C1-2 stability
Flexion/extension films
C1-2 fusion for ADI > 5mm
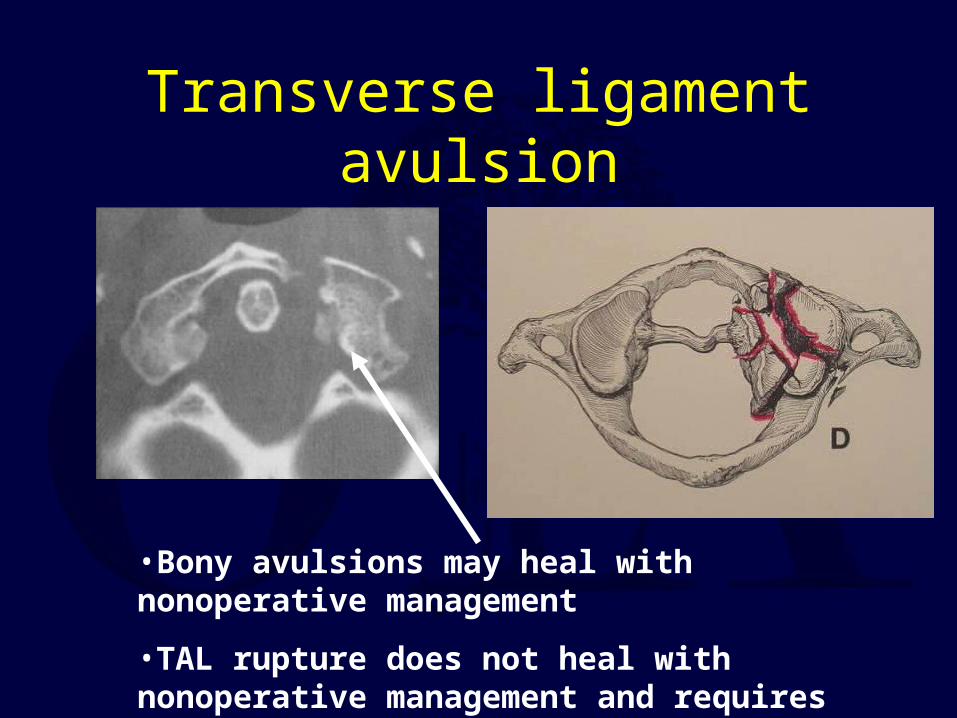
Transverse ligament avulsion
•Bony avulsions may heal with nonoperative management
•TAL rupture does not heal with nonoperative management and requires C1-C2 arthrodesis
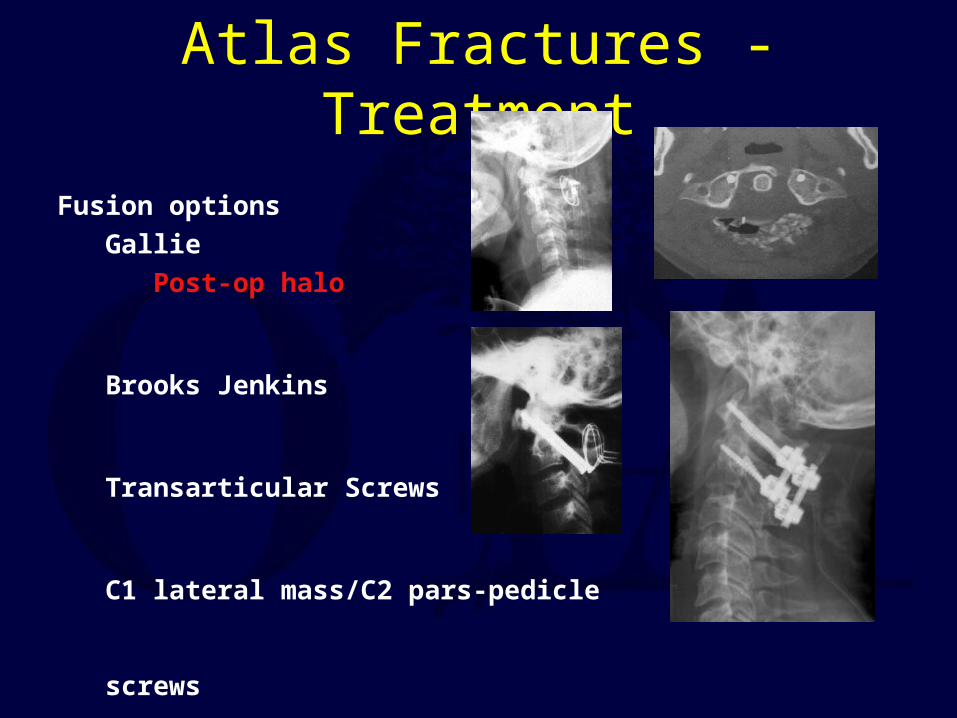
Fusion options
Gallie
Post-op halo
Brooks Jenkins
Transarticular Screws
C1 lateral mass/C2 pars-pedicle screws
Atlas Fractures - Treatment

Odontoid Fractures
Most common fracture of Axis (nearly 2/3 of all C2 Fxs)
10 – 20 % of all cervical fractures
Etiology Bimodal distribution
Young - high energy, multi-trauma
Elderly - low energy, isolated injury
(most common C-spine Fx elderly)
Elderly and the Odontoid• Platzer Studies
– Elderly increased pseudarthrosis rate( 12% v. 8%)
– Elderly tolerated pseudarthosis well(1/5)
– Elderly tolerated halo well– 10% mortality (4/41)– 22% complication rate
• Chapman studies– Elderly did not heal the
odontoid fracture (4/17)– Elderly tolerated halo well
(7/8)– 15% mortality (3/20)
• Harrop and Vaccaro– 9/10 “union”– 5/10 postop halo– 1/10 perioperative death
• Multiple series of high mortality rates
Anterior screw fixation of odontoid fractures comparing younger and elderly patientsAuthors:Platzer,P.; Thalhammer,G.; Ostermann,R.; Wieland,T.; Vecsei,V.; Gaebler,C.Source:Spine, 2007, 32, 16, 1714-1720, United States
Nonoperative management of odontoid fractures using a halothoracic vestAuthors:Platzer,P.; Thalhammer,G.; Sarahrudi,K.; Kovar,F.; Vekszler,G.; Vecsei,V.; Gaebler,C.Source:Neurosurgery, 2007, 61, 3, 522-9; discussion 529-30, United States
Posterior atlanto-axial arthrodesis for fixation of odontoid nonunionsAuthors:Platzer,P.; Vecsei,V.; Thalhammer,G.; Oberleitner,G.; Schurz,M.; Gaebler,C.Source:Spine, 2008, 33, 6, 624-630, United States
Type II odontoid fractures in the elderly: early failure of nonsurgical treatmentAuthors:Kuntz,C.,4th; Mirza,S.K. ; Jarell,A.D.; Chapman,J.R.; Shaffrey,C.I.; Newell,D.W.Source:Neurosurg.Focus., 2000, 8, 6, e7, United States
Efficacy of anterior odontoid screw fixation in elderly patients with Type II odontoid fracturesAuthors:Harrop,J.S. ; Przybylski,G.J.; Vaccaro,A.R.; Yalamanchili,K.Source:Neurosurg.Focus., 2000, 8, 6, e6, United States
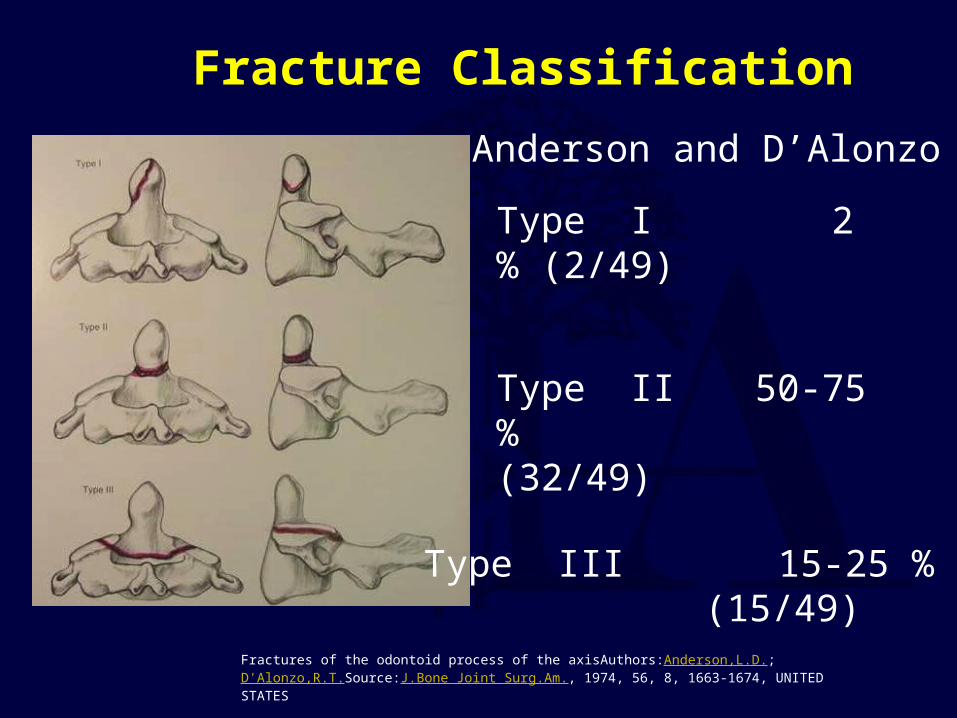
Fracture Classification
Anderson and D’Alonzo
Type I 2 % (2/49)
Type II 50-75 % (32/49)
Type III 15-25 % (15/49)
Fractures of the odontoid process of the axisAuthors:Anderson,L.D.; D'Alonzo,R.T.Source:J.Bone Joint Surg.Am., 1974, 56, 8, 1663-1674, UNITED STATES
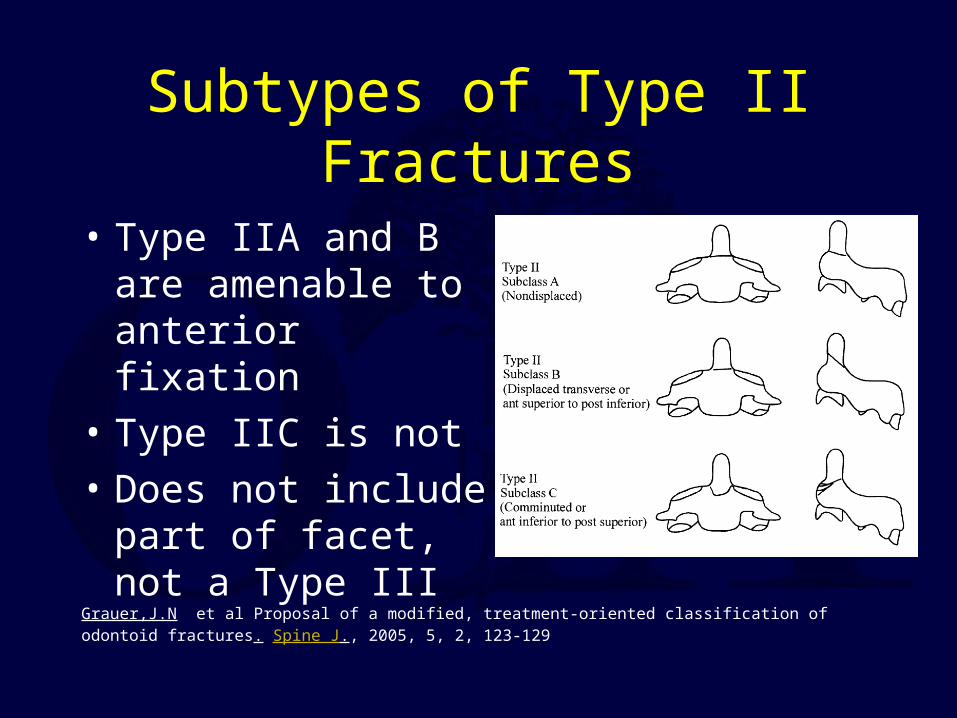
Subtypes of Type II Fractures
• Type IIA and B are amenable to anterior fixation
• Type IIC is not
• Does not include part of facet, not a Type III
Grauer,J.N et al Proposal of a modified, treatment-oriented classification of odontoid fractures. Spine J., 2005, 5, 2, 123-129
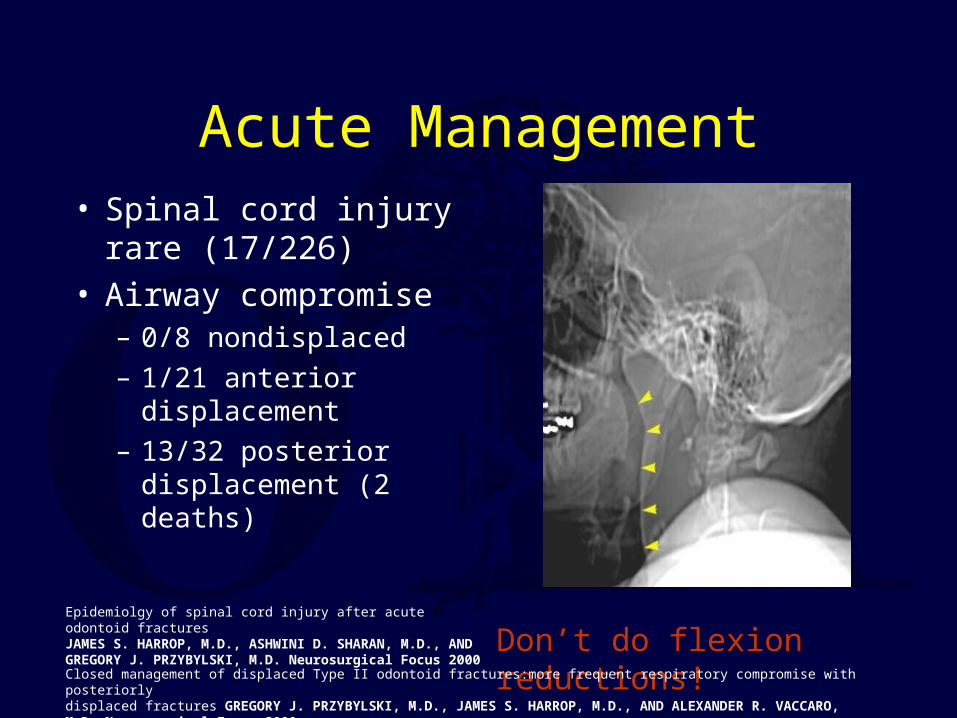
Acute Management• Spinal cord injury rare
(17/226)• Airway compromise
– 0/8 nondisplaced
– 1/21 anterior displacement
– 13/32 posterior displacement (2 deaths)
Don’t do flexion reductions!Closed management of displaced Type II odontoid fractures:more frequent respiratory compromise with posteriorlydisplaced fractures GREGORY J. PRZYBYLSKI, M.D., JAMES S. HARROP, M.D., AND ALEXANDER R. VACCARO, M.D. Neurosurgical Focus 2000
Epidemiolgy of spinal cord injury after acute odontoid fracturesJAMES S. HARROP, M.D., ASHWINI D. SHARAN, M.D., AND GREGORY J. PRZYBYLSKI, M.D. Neurosurgical Focus 2000
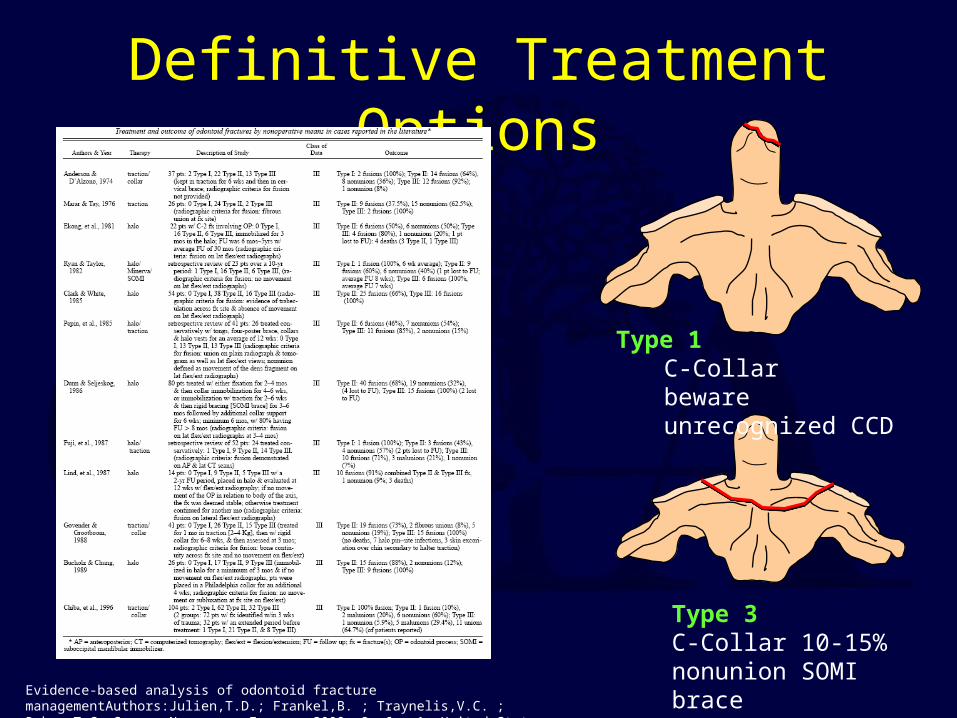
Definitive Treatment Options
Type 1C-Collarbeware unrecognized CCD
Type 3C-Collar 10-15% nonunion SOMI braceHalo Vest
Evidence-based analysis of odontoid fracture managementAuthors:Julien,T.D.; Frankel,B. ; Traynelis,V.C. ; Ryken,T.C. Source:Neurosurg.Focus., 2000, 8, 6, e1, United States
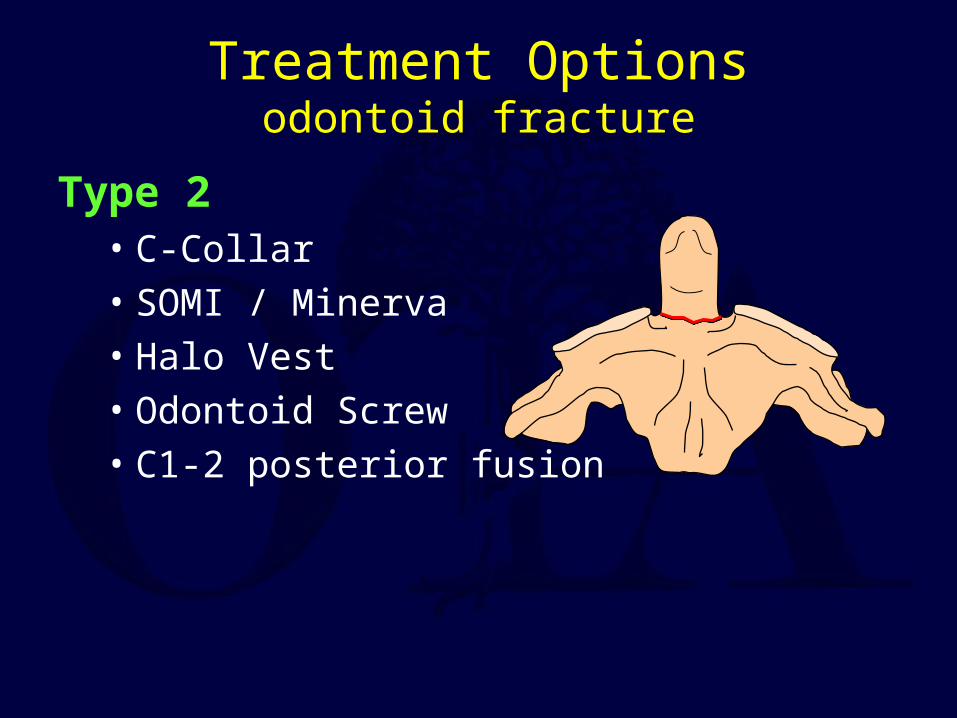
Treatment Optionsodontoid fracture
Type 2• C-Collar• SOMI / Minerva• Halo Vest• Odontoid Screw• C1-2 posterior fusion

Anterior Odontoid Screw FixationIndications
• Displaced Type II, Shallow Type III• Polytrauma patient• Unable to tolerate halo-vest• Early displacement despite halo-vest• (Reduces in extension)
Contraindications• Non-reducible odontoid fracture• (Reduces in flexion)• Body habitus (Barrel chest )• Associated TAL injury• Subacute injury (> 6 months)• Reverse oblique• (elderly)
Roy-Camille Classification
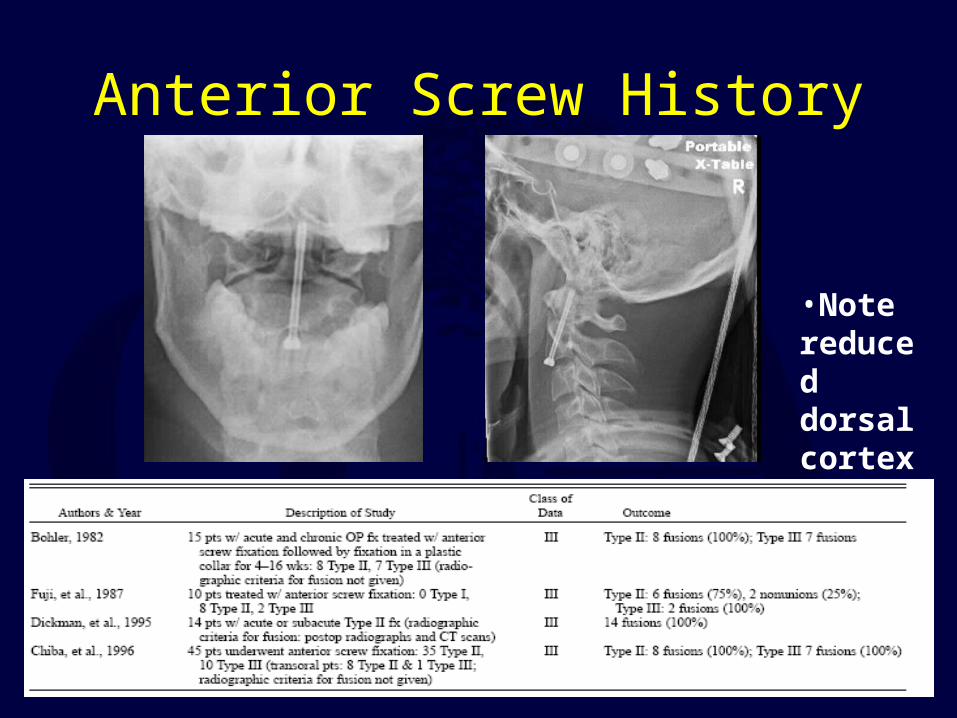
Anterior Screw History
•Note reduced dorsal cortex
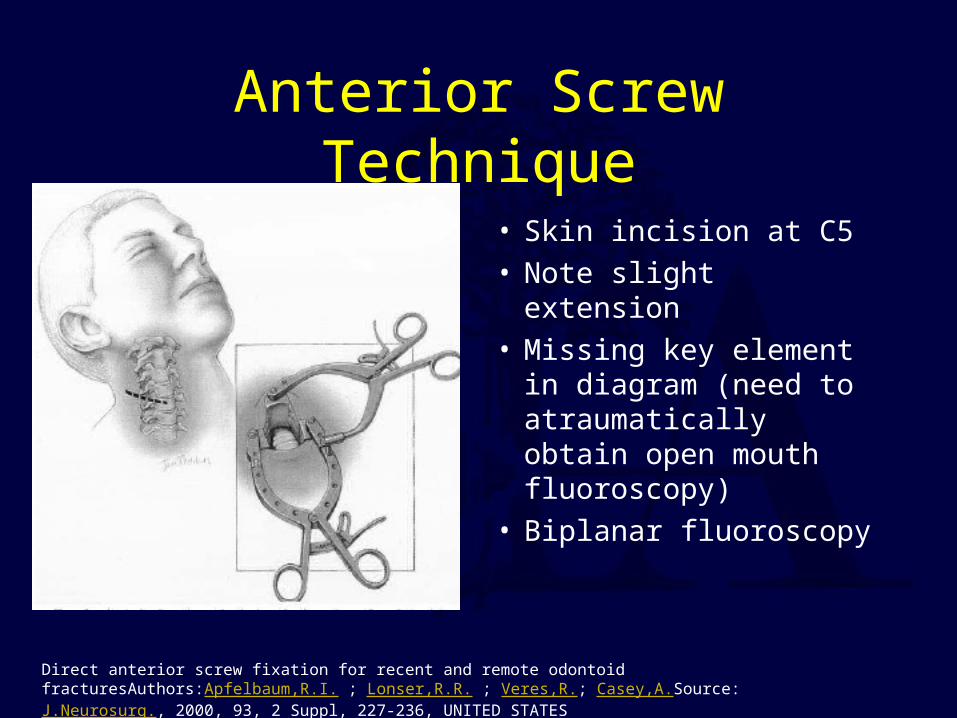
Anterior Screw Technique
• Skin incision at C5• Note slight extension• Missing key element
in diagram (need to atraumatically obtain open mouth fluoroscopy)
• Biplanar fluoroscopy
Direct anterior screw fixation for recent and remote odontoid fracturesAuthors:Apfelbaum,R.I. ; Lonser,R.R. ; Veres,R.; Casey,A.Source:J.Neurosurg., 2000, 93, 2 Suppl, 227-236, UNITED STATES

Anterior Screw Technique
• Need to enter body caudal portion of promontory
• Midline for single screw placement
Direct anterior screw fixation for recent and remote odontoid fracturesAuthors:Apfelbaum,R.I. ; Lonser,R.R. ; Veres,R.; Casey,A.Source:J.Neurosurg., 2000, 93, 2 Suppl, 227-236, UNITED STATES
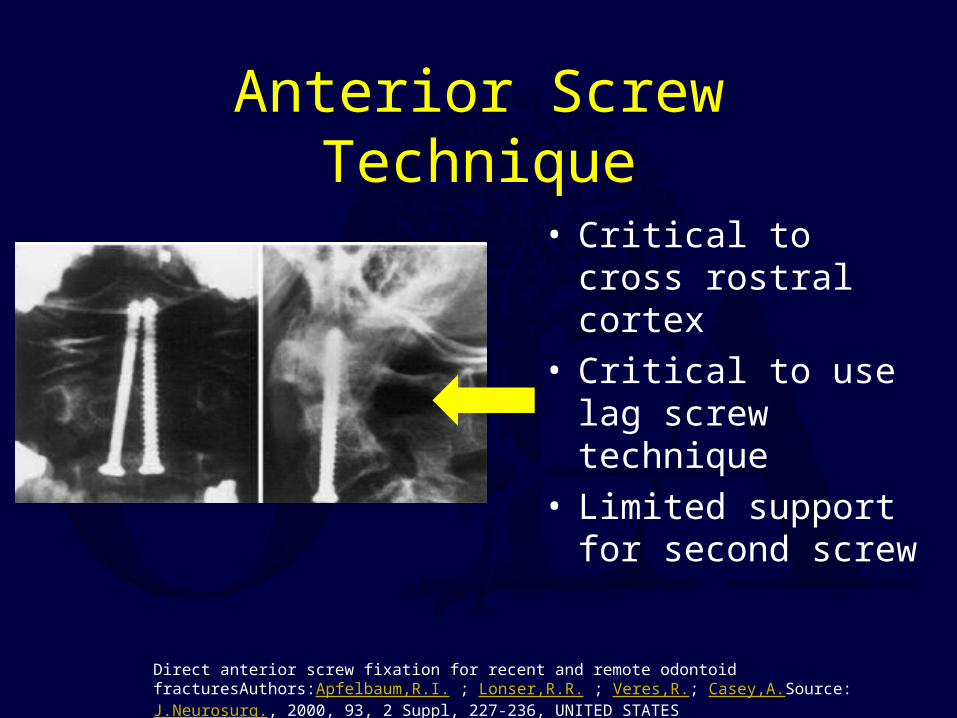
Anterior Screw Technique
• Critical to cross rostral cortex
• Critical to use lag screw technique
• Limited support for second screw
Direct anterior screw fixation for recent and remote odontoid fracturesAuthors:Apfelbaum,R.I. ; Lonser,R.R. ; Veres,R.; Casey,A.Source:J.Neurosurg., 2000, 93, 2 Suppl, 227-236, UNITED STATES
One or Two Screws?
• No significant difference biomechanically– Sasso– Graziano
• No difference clinically– Apfelbaum– Jenkins
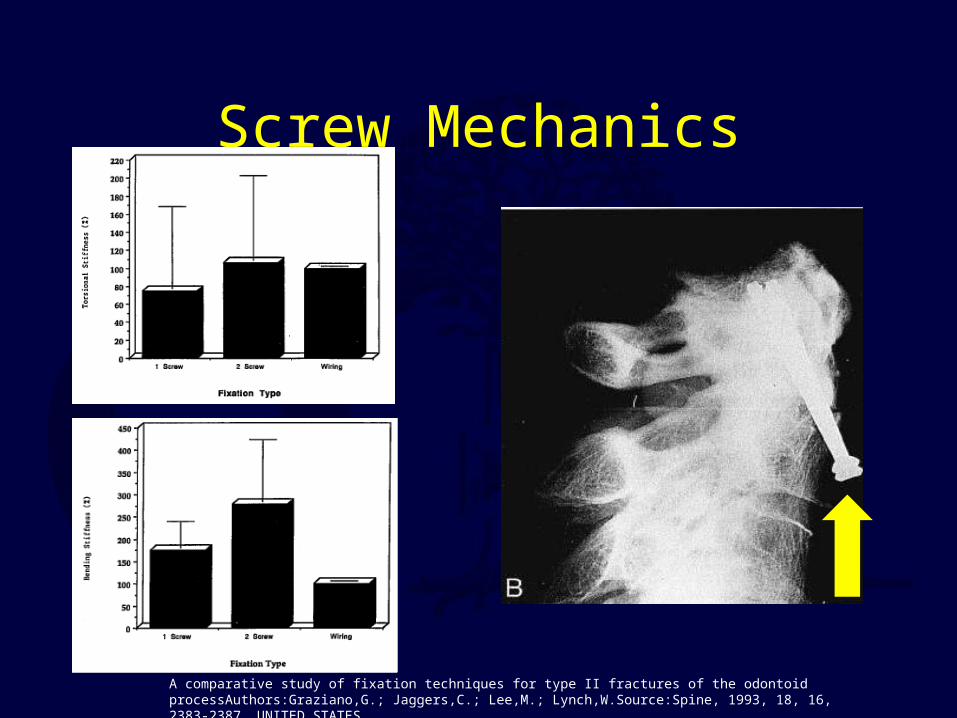
Screw Mechanics
A comparative study of fixation techniques for type II fractures of the odontoid processAuthors:Graziano,G.; Jaggers,C.; Lee,M.; Lynch,W.Source:Spine, 1993, 18, 16, 2383-2387, UNITED STATES
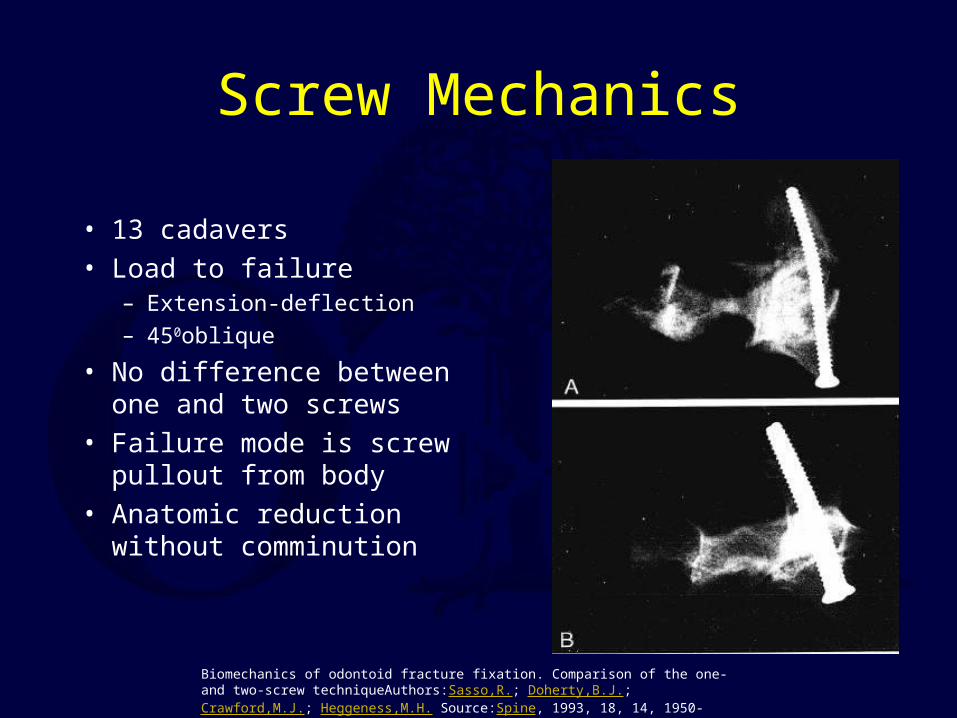
Screw Mechanics
• 13 cadavers• Load to failure
– Extension-deflection– 450oblique
• No difference between one and two screws
• Failure mode is screw pullout from body
• Anatomic reduction without comminution
Biomechanics of odontoid fracture fixation. Comparison of the one- and two-screw techniqueAuthors:Sasso,R.; Doherty,B.J.; Crawford,M.J.; Heggeness,M.H. Source:Spine, 1993, 18, 14, 1950-1953, UNITED STATES
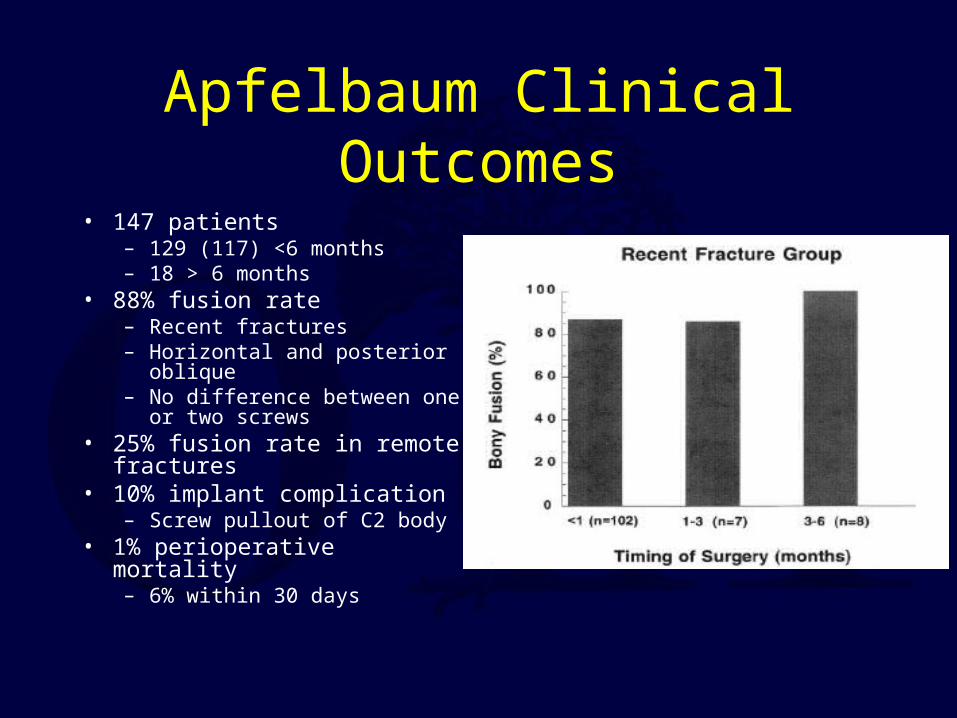
Apfelbaum Clinical Outcomes
• 147 patients– 129 (117) <6 months– 18 > 6 months
• 88% fusion rate– Recent fractures– Horizontal and posterior oblique– No difference between one or
two screws• 25% fusion rate in remote
fractures• 10% implant complication
– Screw pullout of C2 body• 1% perioperative mortality
– 6% within 30 days
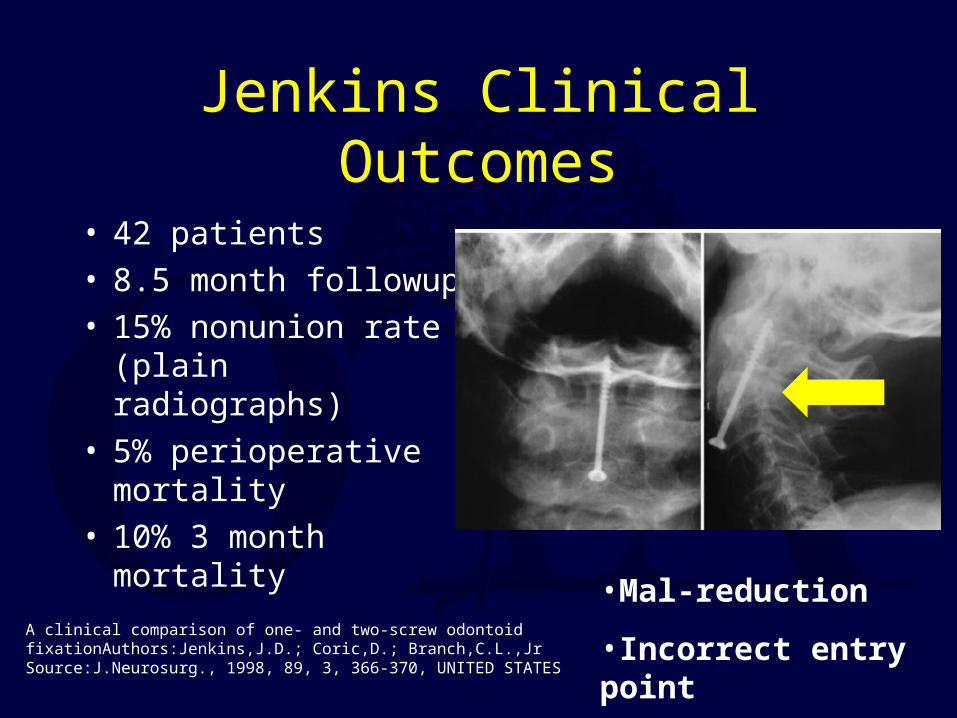
Jenkins Clinical Outcomes
• 42 patients• 8.5 month followup• 15% nonunion rate
(plain radiographs)• 5% perioperative
mortality• 10% 3 month
mortalityA clinical comparison of one- and two-screw odontoid fixationAuthors:Jenkins,J.D.; Coric,D.; Branch,C.L.,Jr Source:J.Neurosurg., 1998, 89, 3, 366-370, UNITED STATES
•Mal-reduction
•Incorrect entry point

Posterior Odontoid Stabilization

Posterior Odontoid Stabilization• Options
– Posterior wiring• Up to 25% pseudoarthrosis• Halo vest necessary (?) Dickman JNS 1996, Grob Spine 1992
– Transarticular screw fixation• Magerl and Steeman Cerv Spine 1987• Reilly et al, JSD 2003
– C1 lateral mass - C2 pars/pedicle/lamina screw
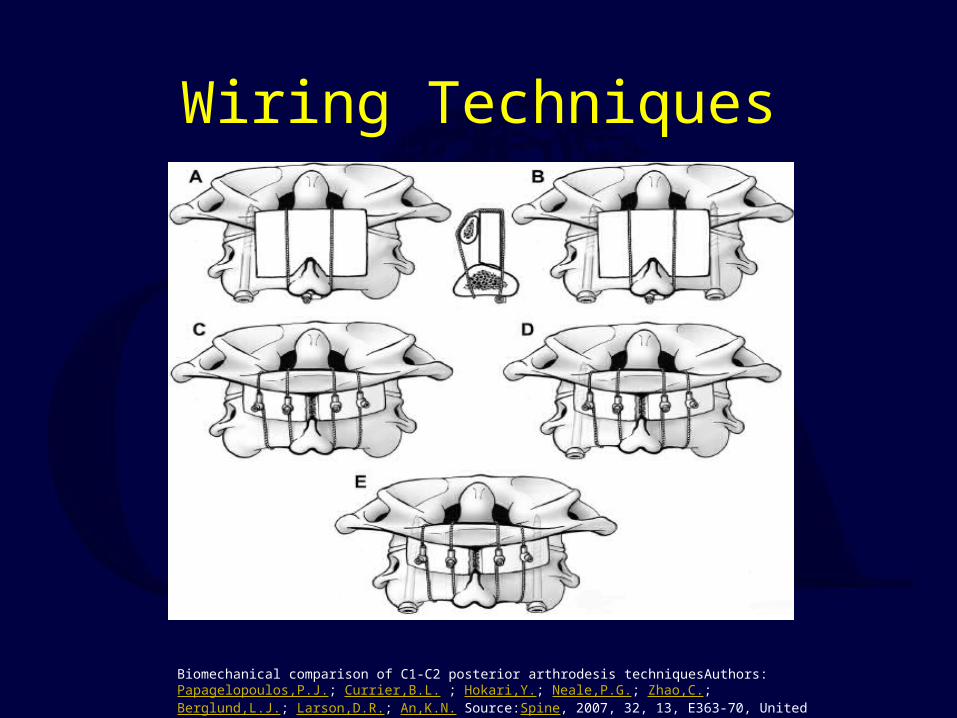
Wiring Techniques
Biomechanical comparison of C1-C2 posterior arthrodesis techniquesAuthors:Papagelopoulos,P.J.; Currier,B.L. ; Hokari,Y.; Neale,P.G.; Zhao,C.; Berglund,L.J.; Larson,D.R.; An,K.N. Source:Spine, 2007, 32, 13, E363-70, United States
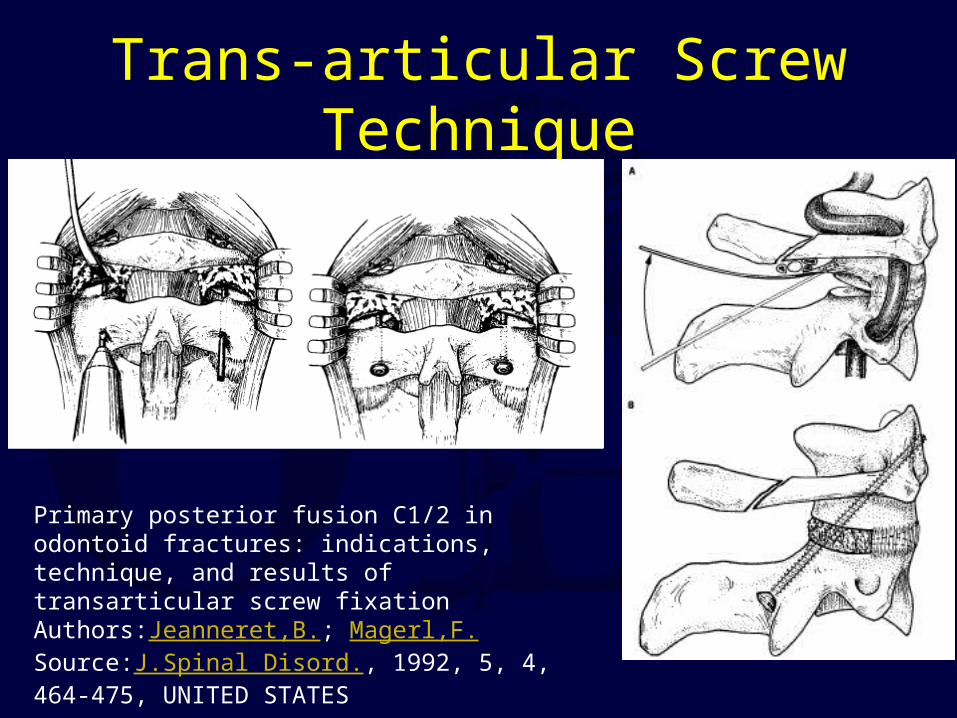
Trans-articular Screw Technique
Primary posterior fusion C1/2 in odontoid fractures: indications, technique, and results of transarticular screw fixation Authors:Jeanneret,B.; Magerl,F.Source:J.Spinal Disord., 1992, 5, 4, 464-475, UNITED STATES
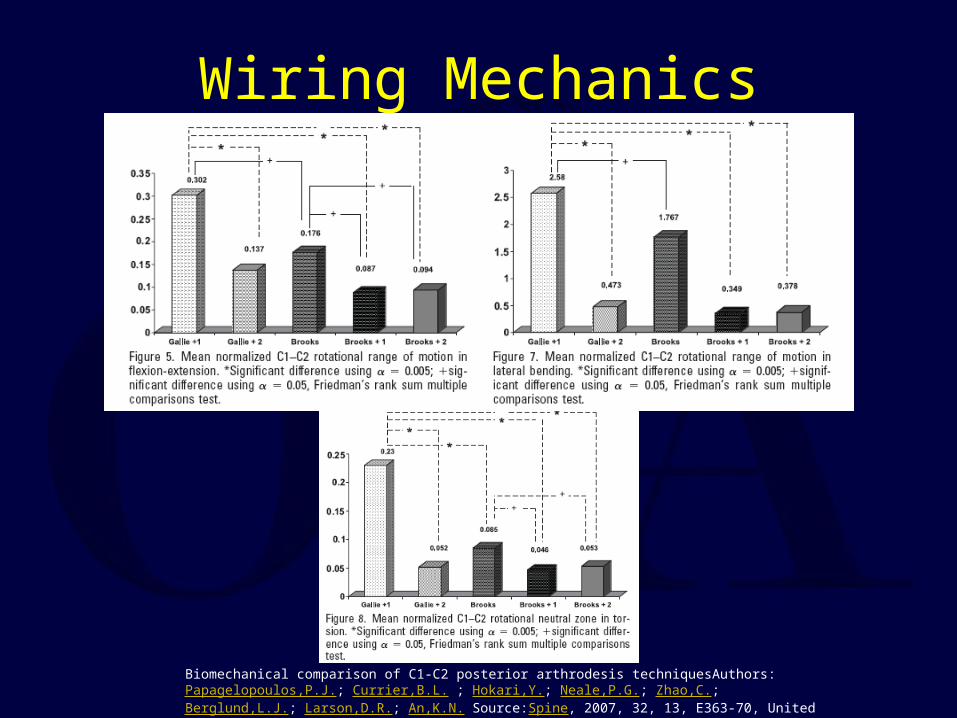
Wiring Mechanics
Biomechanical comparison of C1-C2 posterior arthrodesis techniquesAuthors:Papagelopoulos,P.J.; Currier,B.L. ; Hokari,Y.; Neale,P.G.; Zhao,C.; Berglund,L.J.; Larson,D.R.; An,K.N. Source:Spine, 2007, 32, 13, E363-70, United States

Posterior Wiring Outcomes

C1C2 Segmental Instrumentation
Posterior C1-C2 fusion with polyaxial screw and rod fixationAuthors:Harms,J.; Melcher,R.P.Source:Spine, 2001, 26, 22, 2467-2471, United States
..
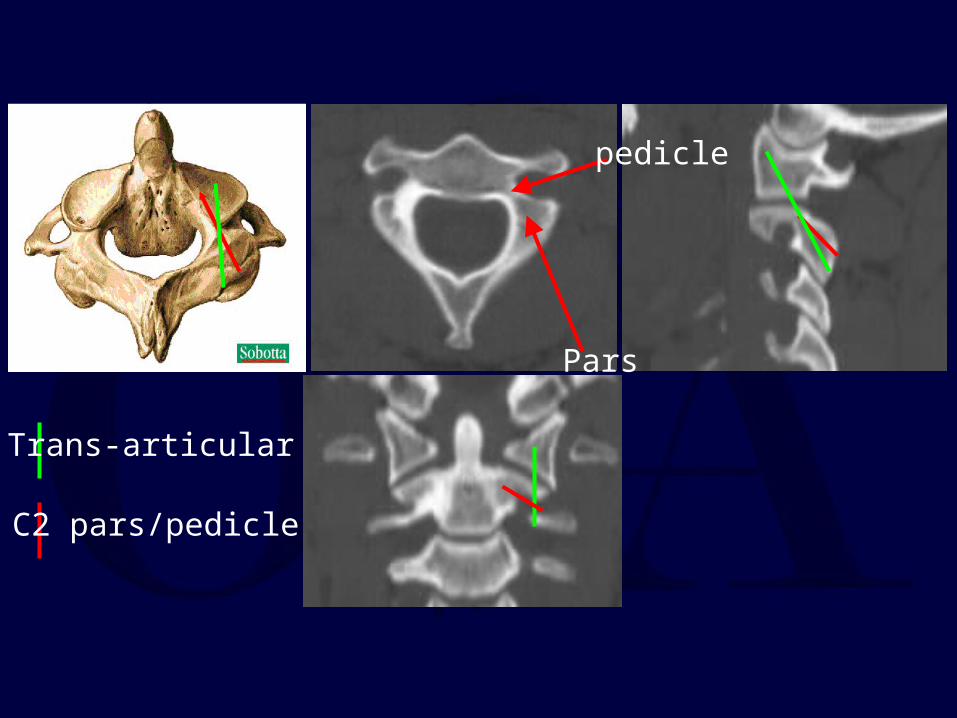
pedicle
Pars
Trans-articular
C2 pars/pedicle
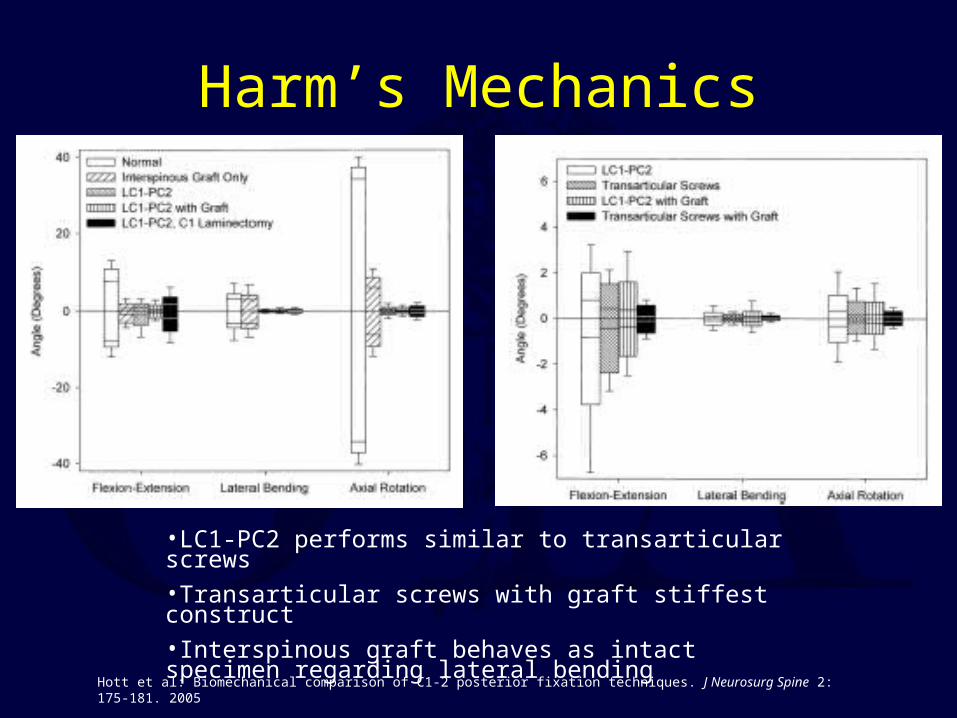
Harm’s Mechanics
Hott et al: Biomechanical comparison of C1-2 posterior fixation techniques. J Neurosurg Spine 2: 175-181. 2005
•LC1-PC2 performs similar to transarticular screws•Transarticular screws with graft stiffest construct•Interspinous graft behaves as intact specimen regarding lateral bending
Harm’s Outcomes
• 37 patients• 100% fusion• 1 wound infection
• 102 patients• 98% fusion rate• Navigation• Allograft/BMP• 2 dissection VA injury• 1 neuropathic pain (C2
root sacrifice)• 4 wound infections
Stabilization of the atlantoaxial complex via C-1 lateral mass and C-2 pedicle screw fixation in a multicenter clinical experience in 102 patients: modification of the Harms and Goel techniquesAuthors:Aryan,H.E.; Newman,C.B.; Nottmeier,E.W.; Acosta,F.L.,Jr; Wang,V.Y.; Ames,C.P.Source:J.Neurosurg.Spine, 2008, 8, 3, 222-229, United States
Posterior C1-C2 fusion with polyaxial screw and rod fixationAuthors:Harms,J.; Melcher,R.P.Source:Spine, 2001, 26, 22, 2467-2471, United States
Posterior Fusion Takehome
• Catastrophic failures reported for trans-articular screws alone• Trans-articular screws with wired bone graft is stiffest
construct– Requires intact C1 lamina– Requires reducible C1-2 facets– Requires favorable anatomy
• Gallie wiring is inadequate without two supplemental screws• No advantage of either wiring construct with two
transarticular screws• Harm’s technique is most flexible• Think about hooks?
Traumatic Spondylolisthesis Axis(Hangman’s Fracture)
Second most common fracture of axis25% of C2 injuries
Most common mechanism of injury is MVA
Hangman’s Fracture
Younger age group (Avg 38 yrs)
Usually due to hyperextension-axial compression forces (windshield strike)
Neurologic injury seen in only 5-10 % (acutely decompresses canal)
Traditional treatment has been Halo-vest
Collar adequate if < 6 mm displacedCoric et al JNS 1996
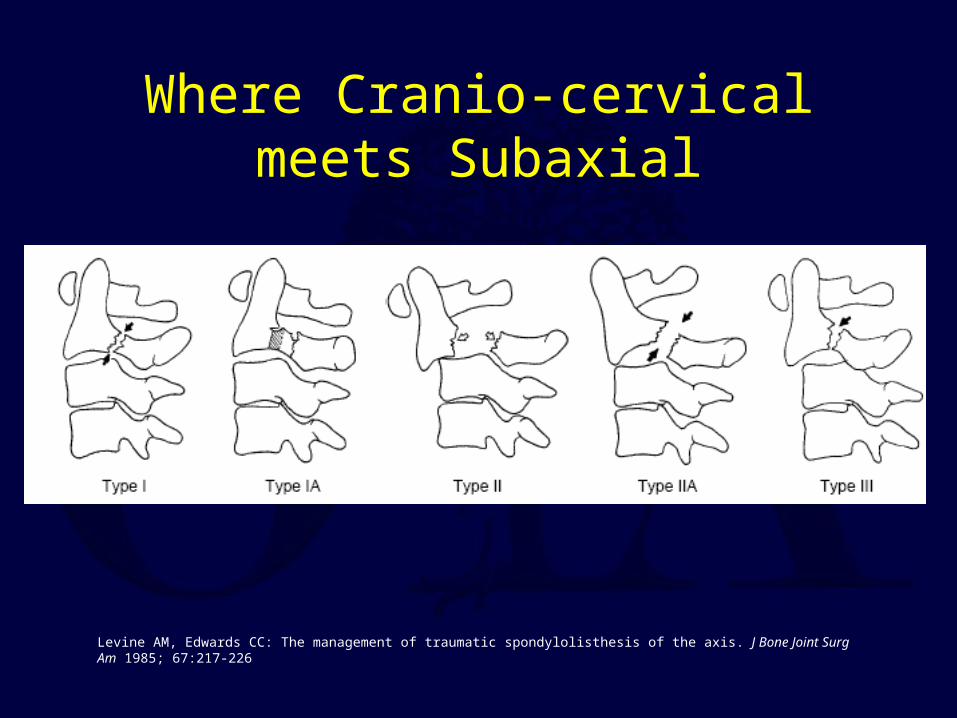
Where Cranio-cervical meets Subaxial
Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985; 67:217-226
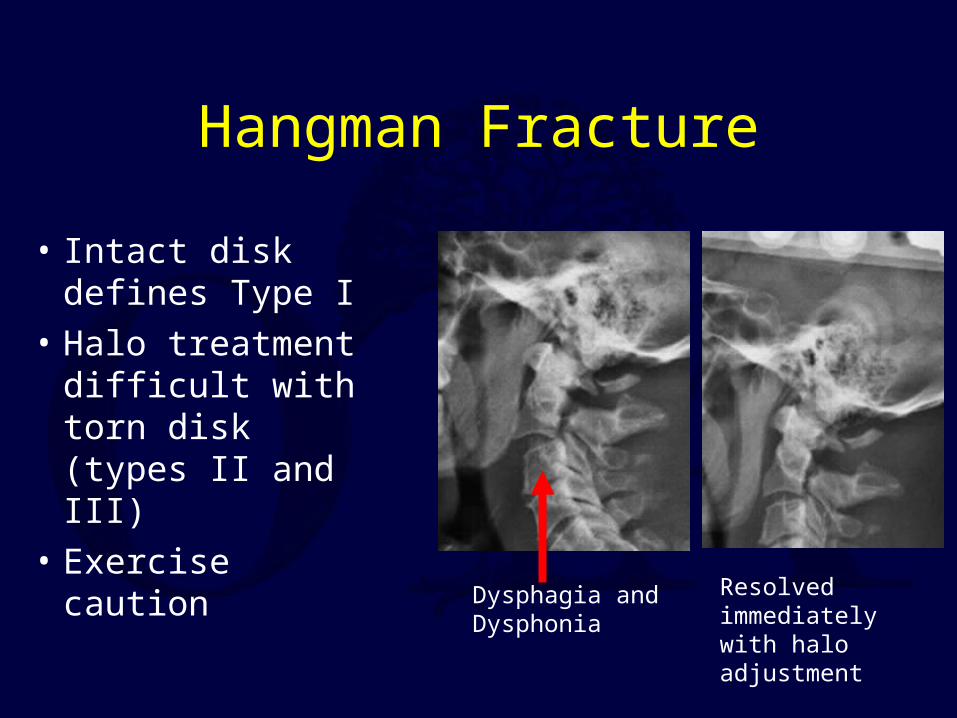
Hangman Fracture
Dysphagia and Dysphonia
Resolved immediately with halo adjustment
• Intact disk defines Type I
• Halo treatment difficult with torn disk (types II and III)
• Exercise caution
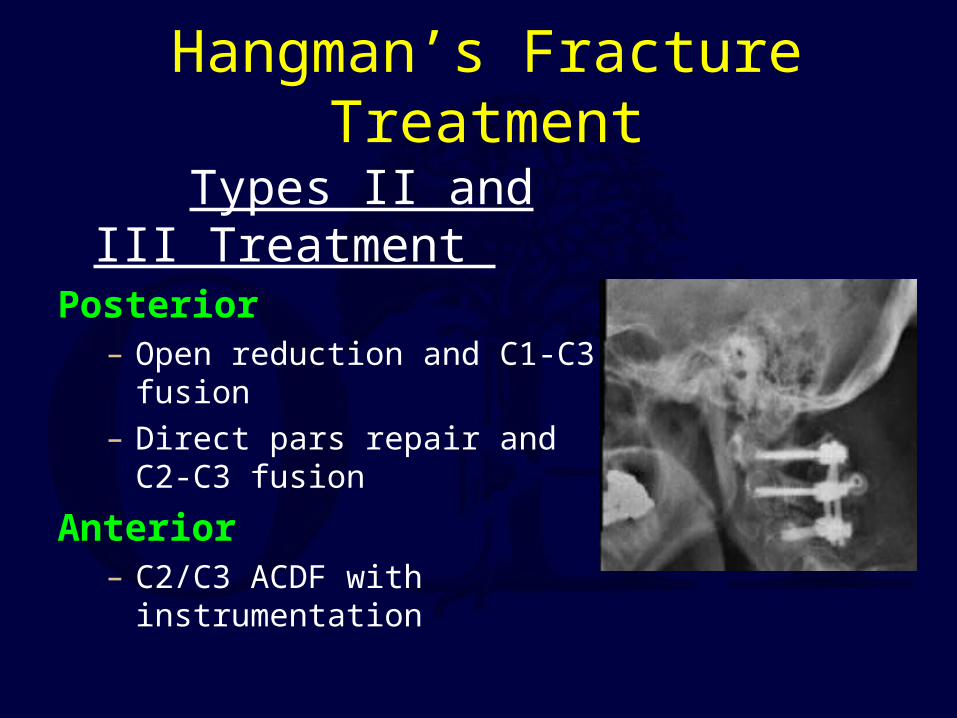
Hangman’s Fracture Treatment
Types II and III Treatment
Posterior – Open reduction and C1-C3 fusion
– Direct pars repair and C2-C3 fusion
Anterior– C2/C3 ACDF with instrumentation
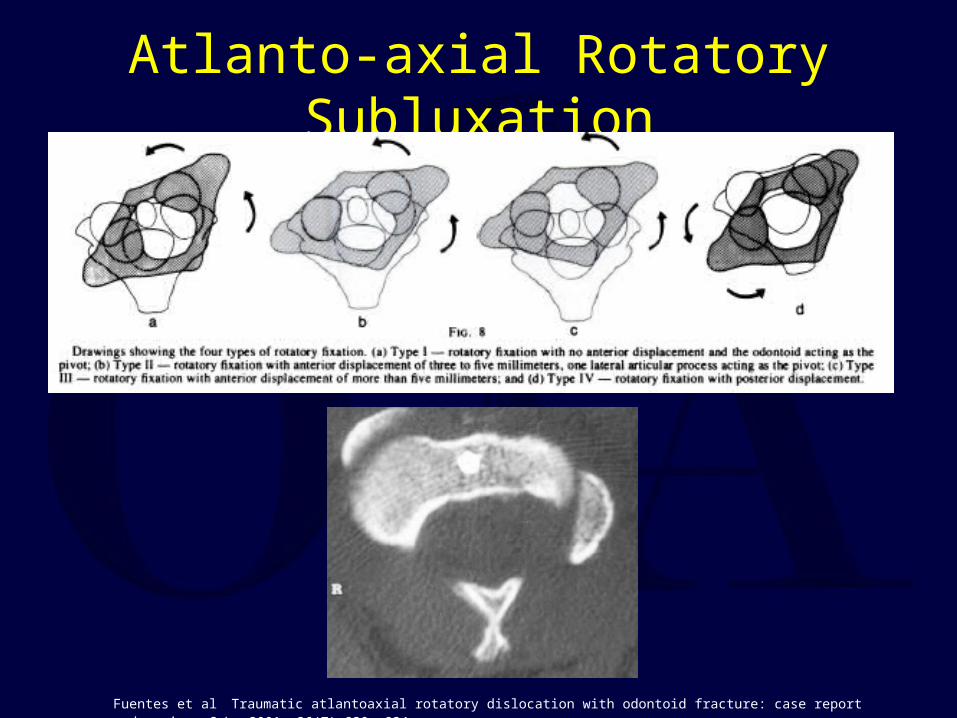
Atlanto-axial Rotatory Subluxation
Fuentes et al Traumatic atlantoaxial rotatory dislocation with odontoid fracture: case report and review. Spine 2001; 26(7) 830 -834
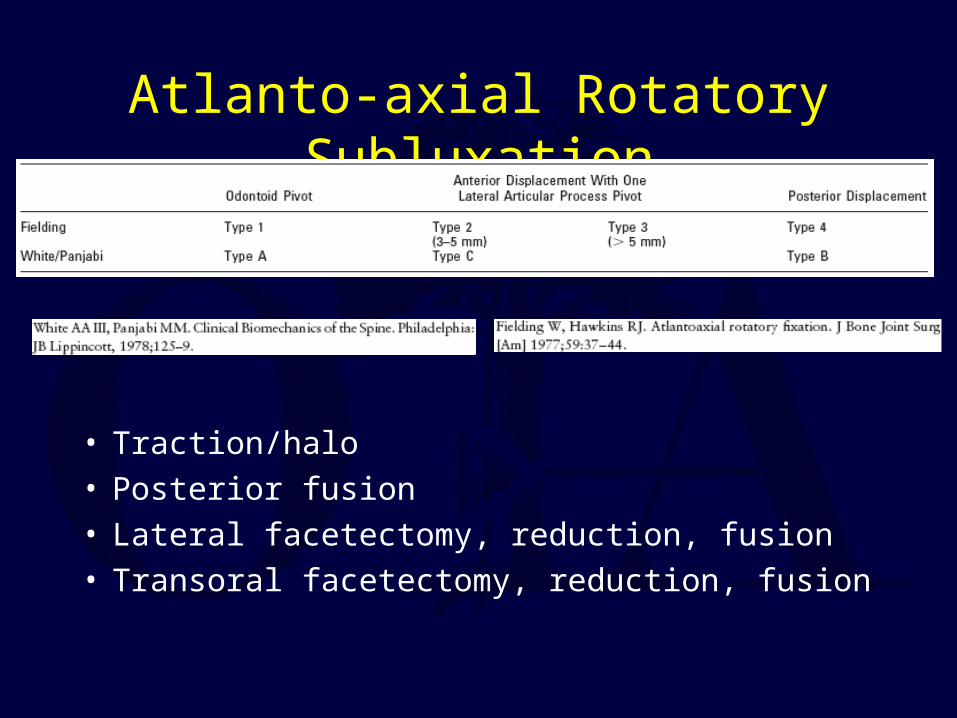
Atlanto-axial Rotatory Subluxation
• Traction/halo• Posterior fusion• Lateral facetectomy, reduction, fusion• Transoral facetectomy, reduction, fusion
Halo Immobilization
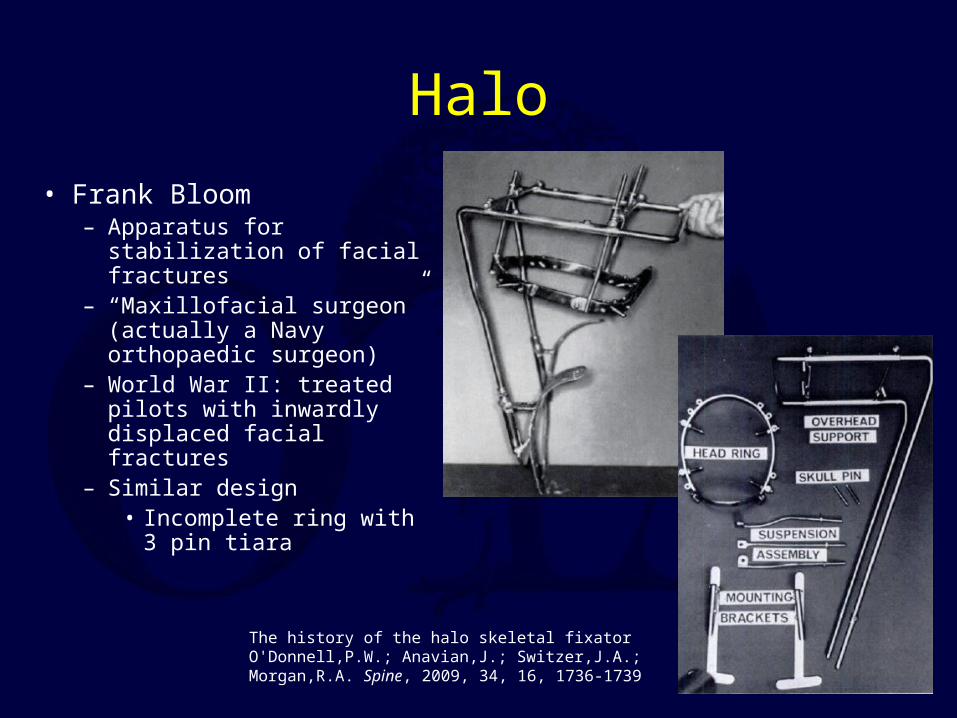
Halo
• Frank Bloom – Apparatus for stabilization
of facial fractures– “Maxillofacial surgeon”
(actually a Navy orthopaedic surgeon)
– World War II: treated pilots with inwardly displaced facial fractures
– Similar design • Incomplete ring with 3
pin tiara
The history of the halo skeletal fixator O'Donnell,P.W.; Anavian,J.; Switzer,J.A.; Morgan,R.A. Spine, 2009, 34, 16, 1736-1739
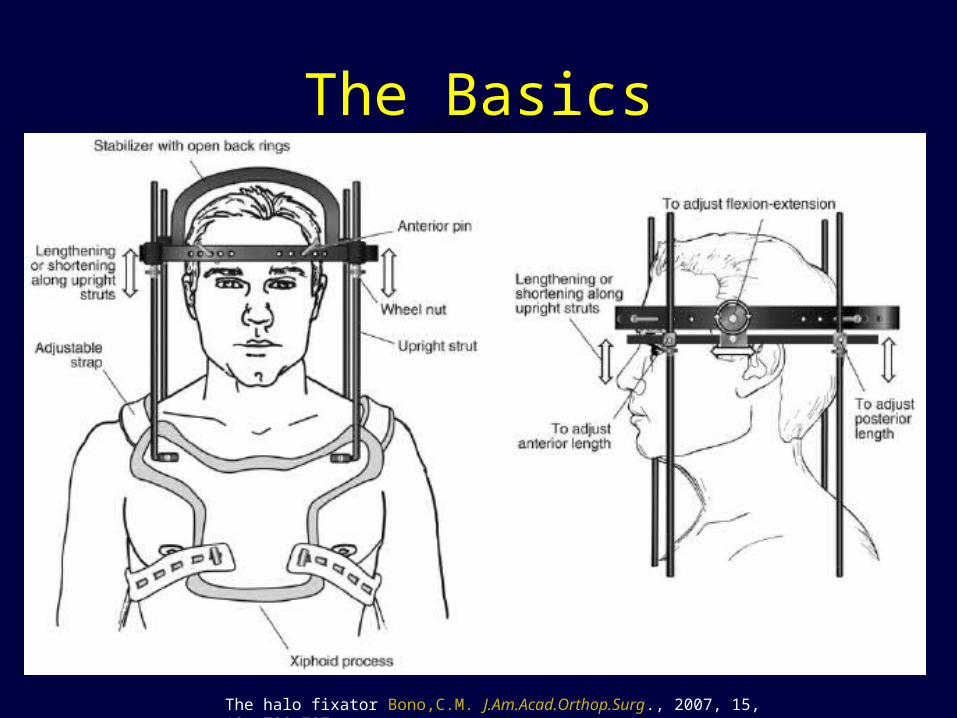
The Basics
The halo fixator Bono,C.M. J.Am.Acad.Orthop.Surg., 2007, 15, 12, 728-737

Pin Placement
The halo fixator Bono,C.M. J.Am.Acad.Orthop.Surg., 2007, 15, 12, 728-737
If you would like to volunteer as an author for the Resident Slide Project or recommend updates to any of the following slides, please send an e-mail to [email protected]
Halo in Elderly• Tashijan J. Trauma 2006
– 78 patients, age > 65yo
– Type II or III odontoid fractures
– Increased early morbidity and mortality
• Compared with treatment using operative fixation or rigid collar
• Van Middendorp JBJS 2009– 239 patients
– All ages in halo
– No increased risk of pneumonia or death in patients >65 years old Halo vest immobilization in the elderly: a death sentence? Majercik,S.;
Tashjian,R.Z.; Biffl,W.L.; Harrington,D.T.; Cioffi,W.G. J.Trauma, 2005, 59, 2, 350-6; discussion 356-8
Incidence of and risk factors for complications associated with halo-vest immobilization: a prospective, descriptive cohort study of 239 patients van Middendorp,J.J.; Slooff,W.B.; Nellestein,W.R.; Oner,F.C. J.Bone Joint Surg.Am., 2009, 91, 1, 71-79

E-mail OTA about
Questions/Comments
If you would like to volunteer as an author for the Resident Slide Project or recommend updates to any of the following slides, please send an e-mail to [email protected]
Thank You
•Return to •Spine•Index