urine drug screening - amazon s3 · pdf fileexpert guidance statement 6: urine drug screening...
TRANSCRIPT

Urine Drug Screening (UDS)
Dr. Erica L. Weinberg
December 2017

Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
form or by any means – graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without
prior written permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or
omissions.

Conflict of Interest Disclosure
Presenter/Faculty: Dr. Erica L. Weinberg
Relationships with Commercial Interests:
Grants/research support: none
Speaker bureau/honoraria: Sea Courses
Consulting fees: none
Other: none

Potential for Conflict of Interest
• I have been Medical Inspector (MI)/Independent Opinion (IO) Provider at the
College of Physicians and Surgeons of Ontario (CPSO, ‘College’) –
frequently regarding opioid prescribing practices
• I have been a member of the National Faculty at the Michael G. Degroote
National Pain Centre since 2012
• I am one of the many authors on the Canadian Pain Society’s revised
consensus statement on the pharmacological management of chronic
neuropathic pain

Mitigating Potential Bias
• Information presented or recommendations made are
evidence/guideline/consensus-based
• I have completed the CPFC Mainpro+/Cert+ Declaration of Conflict of
Interest form evidencing compliance with Mainpro+/Cert+ requirements, a
requisite for this program to be given accredited status
• I will be discussing “off-label” uses of medications

The Guideline - Risk Mitigation
A baseline UDS may be useful for patients currently receiving
or being considered for a trial of opioids.
Clinicians may repeat UDS on an annual basis and more frequently if the patient is at elevated risk or
in the presence of any ADRBs.
When ordering a UDS, clinicians should ask patients about all medications/drugs recently
taken, and be aware of local resources to assist them in assessing for potential false
positive and false negative results.
Expert Guidance Statement 6: Urine Drug Screening
Available at http://nationalpaincentre.mcmaster.ca/guidelines.html

How Often Do You Think a UDS Should be Done?

How Often Do You Think a UDS Should be Done?
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Should You Do Random UDS?

Should You Do Random UDS?
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

What about collecting UDS at every visit,
but not necessarily testing every time?

UDS – Why Bother
• To improve patient care and communication
• To help verify self-report of medication history
• To encourage or reinforce healthy behavioural change, sometimes as a
requirement of continued treatment
• Everyone has a role to play in safe medication use
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Learning Objectives
After this session, participants will be able to:
• Develop a plan for urine drug screening (UDS)/urine drug testing (UDT) in
the office/clinic
• Interpret UDS results with more confidence
• Manage unexpected UDS results more effectively
Things to Know Before you Start
• You are not a police officer
• UDS is an imperfect tool, yet it can assist you in managing your patients
• The UDS test available to us is not performed up to forensic standards
• You must document your interpretation of the results and your subsequent
plan for action
• You must have standard operating procedures for UDS

Have Standard Operating Procedures
• Inform the patient of the routine nature of the test
– Is it part of your Opioid Treatment Agreement?
• Take a careful history of medication/drug use for the past week
– Consider asking, “What should I expect to see in the results?”
• Collect the urine sample in the your office/clinic, if possible
– Be consistent on what a patient can/cannot take into the washroom with them• E.g. Bulky clothing, bags …
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf

Have Standard Operating Procedures
• Ensure proper labelling
• What is the urine temperature – ensure it is checked within a few minutes
– Does the urine sample feel ‘body temperature’
– Have a protocol in place if it feels ‘cold’
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf

Have Standard Operating Procedures
If you are doing Point of Care (POC) Testing:
• Ensure you have read the instructions thoroughly
• Consider occasionally verifying your POC UDS results with a laboratory immune
assay (IA) UDS
If you are Delegating the Act of POC Testing:
• Be aware of your College’s equivalent of a “Delegation of Controlled Acts Policy”
and ensure that your staff are adequately trained
– E.g. evaluation of the delegate, quality assurance, supervision of the delegation, ongoing
monitoring and evaluation …

Know the Limits
of the Test You Are
Ordering/Performing

Types of UDS
Point of Care (POC)
Laboratory
Enzyme Immunoassay (EIA)
Immunoassay (IA)
Gas Chromatography/Mass Spectrometry
(GC/MS)
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf

POC UDS
Advantages
• Portable
• Immediate results
• Urine collected & tested
at clinician’s office/clinic
• Concurrently tests for
multiple drug classes
• Very responsive for
morphine and codeine
Disadvantages
• Cost of POC test kit/dipstick
• Less sensitive and specific than laboratory test
• Will NOT identify specific drugs or metabolites,
except for some exception
• Subjective nature of the qualitative assay
• Drug concentration in urine and assay’s
concentration cut-offs will affect detection
• More definitive testing may be required to
identify a specific drug or metabolite
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Laboratory IA UDS
Advantages
• Rapid turnaround time
• Less expensive than
GC/MS
• Detects drugs for a longer
time than GC/MS
– e.g. (5-7days vs. 1-2 days)
• Concurrently tests for
multiple drug classes
• Very responsive for
morphine and codeine
Disadvantages
• Does not, usually, differentiate between
various opioids
• Often misses synthetic and semisynthetic
opioids
• Cross reactivity: will show false positives
with poppy seeds, quinolone antibiotics …
• Drug concentration in urine and assay’s
concentration cut-offs will affect detection
• More definitive testing may be required to
identify a specific drug or metabolite
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Some Limitations to UDS by IA/EIA
• Cocaine is highly specific as the antibody reacts only to cocaine and its
principle metabolite
• Amphetamine/methamphetamine are highly cross reactive and detects other
sympathomimetic amines e.g. ephedrine and pseudoephedrine
• Opiate testing does not distinguish between morphine, heroin and codeine
• Opiate testing does not always detect semi-synthetics e.g. hydromorphone
• Oxycodone, methadone and buprenorphine need their own specific antibody
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf
Patients who are on fentanyl ONLY and show positive for opiates using standard
IA/EIA test are using other opioids which react with the standard IA/EIA testing

Opioids in CanadaNatural
(extracted from opium)
Semi-synthetic(derived from opium extracts)
Synthetic(man made)
Buprenorphine Fentanyl
Codeine Hydrocodone Loperamide
Morphine Hydromorphone Meperidine
Oxycodone Methadone
Tapentadol
Diamorphine (Heroin) Tramadol
Speak to your laboratory if you are not
sure what opioids their IA UDS
is directed towards

Laboratory GC/MS* UDS
Advantages
• More accurate for semi-
synthetic and synthetic opioids
• Identifies specific drugs
• Differentiates: codeine,
fentanyl, heroin, hydrocodone,
hydromorphone, morphine,
oxycodone …
• Doesn’t react to poppy seeds
• May also detect non-opioid
medications
Disadvantages
• More expensive
• Takes longer to get results
• Requires caution in interpretation
– e.g. codeine metabolized to morphine
*
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Some Limitations to UDS
• QUALITATIVE only
• CANNOT determine the amount and frequency of use, time of last use, route
of administration or the source of the drug
• Adherence
– Presence of a prescribed drug CANNOT distinguish whether the patient has been
taking the drug AS DIRECTED
• ‘Window’ of test detection varies for different drugs
• ‘Cut-off concentration’
– Important when interpreting a report of “no drug present”
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf

http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

UDS – Benzodiazepines (BNZ)
• Not all BNZ are equally detected
• Both IA and GC/MS have significant challenges in detection and clinical
interpretation
• In general, EIA/IA for BNZ:
– Is based on the diazepam antibody
– Shows reliably positive test for diazepam and alprazolam
– Does not usually detect clonazepam or lorazepam
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf

Possible Results of a UDS
What you expect IS present
What you expect ISN’T present
What you DIDN’T expect IS present

What To Do if You Find an
Unexpected UDS Result

General Approach to an Inconsistent UDS
• Take a careful Hx of medication/drug use in the past week and discuss
openly with the patient … WITHOUT being accusatory
– Remember there is the potential for false positive and false negative results
• Be aware of resources to assist you in assessing for potential false positive and false
negative results
– Give the patient an opportunity to address the report
• Check with the lab re potential error
– What kind of urine test was done?

General Approach to an Inconsistent UDS
• Interpret results in the context of the patient’s clinical presentation and
assessments
• Possibly ask the lab to re-run the sample with GC/MS if response still unclear
• Unexpected result does NOT necessarily diagnose:
– Abuse or addiction
– Physical dependence
– Diversion
https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf

Interpreting Unexpected UDS Results
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Interpreting Unexpected UDS Results
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Some Patients …
• May tamper with urine samples to hide aberrant behaviours by:
– Adding adulterants
– Diluting the sample
– Substituting another individuals sample for their own
– Ingesting excessive water or diuretics prior to giving a sample
• ValidationTests
– Performed to improve the reliability of urine sample results
– The laboratory may point out if a validation test seems “off”
• i.e. read the report

Validation Tests
Normal Characteristics of a Urine Specimen
Temperature 32-38o C
pH 4.5 – 8.0
Urine Creatinine >20 mg/dL
Specific Gravity >1.003

Interpreting Unexpected UDS Results
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Known Agents to Cause Interference in UDS Results

http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf


Case 1*: Spinal Stenosis
• 73 y.o. female
• 2 “failed” back surgeries in past (1999, 2006)
• Intolerant to NSAIDs/COXIB
• No personal and no family history of drug/alcohol use issues
• No personal history of mental health issues
*Case 1 courtesy of Dr. Joel Bordman

Case 1*: Spinal Stenosis
• Taking acetaminophen 650 mg qid on a regular basis
• Previously (>1 year) reported constipation with acetaminophen 300
mg/codeine 30 mg/caffeine 15 mg
• Still reporting significantly decreased QoL over last 6 months, despite
maximizing physical and psychological modalities
• You are considering a trial of oxycodone IR 5 mg prn
*Case 1 courtesy of Dr. Joel Bordman

Case 1*: Spinal Stenosis
• Taking acetaminophen 650 mg qid on a regular basis
• Previously (>1 year) reported constipation with aceta/codeine 30 mg/caffeine
• Still reporting significantly decreased QoL over last 6 months, despite
maximizing physical and psychological modalities
• You are considering a trial of oxycodone IR 5 mg prn
Would you consider a UDS as part of your
work up for a trial of opioid therapy?
*Case 1 courtesy of Dr. Joel Bordman

Case 1*: Spinal Stenosis
• Taking acetaminophen 650 mg qid on a regular basis
• Previously (>1 year) reported constipation with aceta/codeine 30 mg/caffeine
• Still reporting significantly decreased QoL over last 6 months, despite
maximizing physical and psychological modalities
• You are considering a trial of oxycodone IR 5 mg prn
UDS (IA) = + opiates, BNZ
*Case 1 courtesy of Dr. Joel Bordman

Case 1*: Spinal Stenosis
• Taking acetaminophen 650 mg qid on a regular basis
• Previously (>1 year) reported constipation with aceta/codeine 30 mg/caffeine
• Still reporting significantly decreased QoL over last 6 months, despite
maximizing physical and psychological modalities
• You are considering a trial of oxycodone IR 5 mg prn
Now what do you do?
UDS (IA) = + opiates, BNZ
*Case 1 courtesy of Dr. Joel Bordman

Case 1*: Spinal Stenosis
• Take a careful history of medication/drug use in the
past week and discuss openly with the patient
• Try not to be accusatory
• The patient explains that she occasionally takes her
sister’s diazepam 5 mg pills
• She also has been using left-over aceta /codeine/caffeine tabs
on a fairly regular basis
*Case 1 courtesy of Dr. Joel Bordman

Post-Operative Opioid Prescriptions
Prescription opioids often go unused after surgery, with few patients
planning to dispose of the unused pills
Researchers analyzed data from six studies that examined the oversupply of prescription opioids
after seven types of surgical procedures (e.g., obstetric, thoracic, urologic). Overall, roughly 800
adults received an opioid prescription after surgery. Among the findings:
• Some 67% to 92% of patients across the studies reported unused opioids.
• Up to 21% did not fill their opioid prescription, and up to 14% filled the prescription but did not
take any of the pills — most often because of adequate pain control.
• Three-quarters of patients stored their opioids in unlocked areas.
• Just 4–30% of patients intended to dispose of their unused pills.
• The researchers caution, "The combination of unused opioids, poor storage practices, and
lack of disposal sets the stage for the diversion of opioids for nonmedical use."
Bicket et al, JAMA Surg. Published online August 2, 2017. doi:10.1001/jamasurg.2017.0831

Sale of Non-Prescription Codeine Products
• Number of countries have already banned the sale of codeine products without
a prescription
– Belgium, Czech Republic, Finland, France, Greece, Iceland, India, Italy, Norway, Russia
and Sweden
– Manitoba = Feb 1, 2016
• Australia announced a ban on OTC sale of products beginning February 2018
• Health Canada announced a move to ban non-prescription (low dose) codeine
products
– Canadians had until November 8 to comment on Health Canada’s proposed regulations
OTC = over the counter; http://www.cbc.ca/news/politics/codeine-opiate-prescription-health-canada-juurlink-pharmacists-ban-sales-1.4284013

Case 1*: Spinal Stenosis
• A confirmatory UDS by GC/MS is positive for:
– Oxazepam
– Temazepam
– Diazepam
– Nordiazepam
– Codeine
– Morphine
Can you explain this?
*Case 1 courtesy of Dr. Joel Bordman

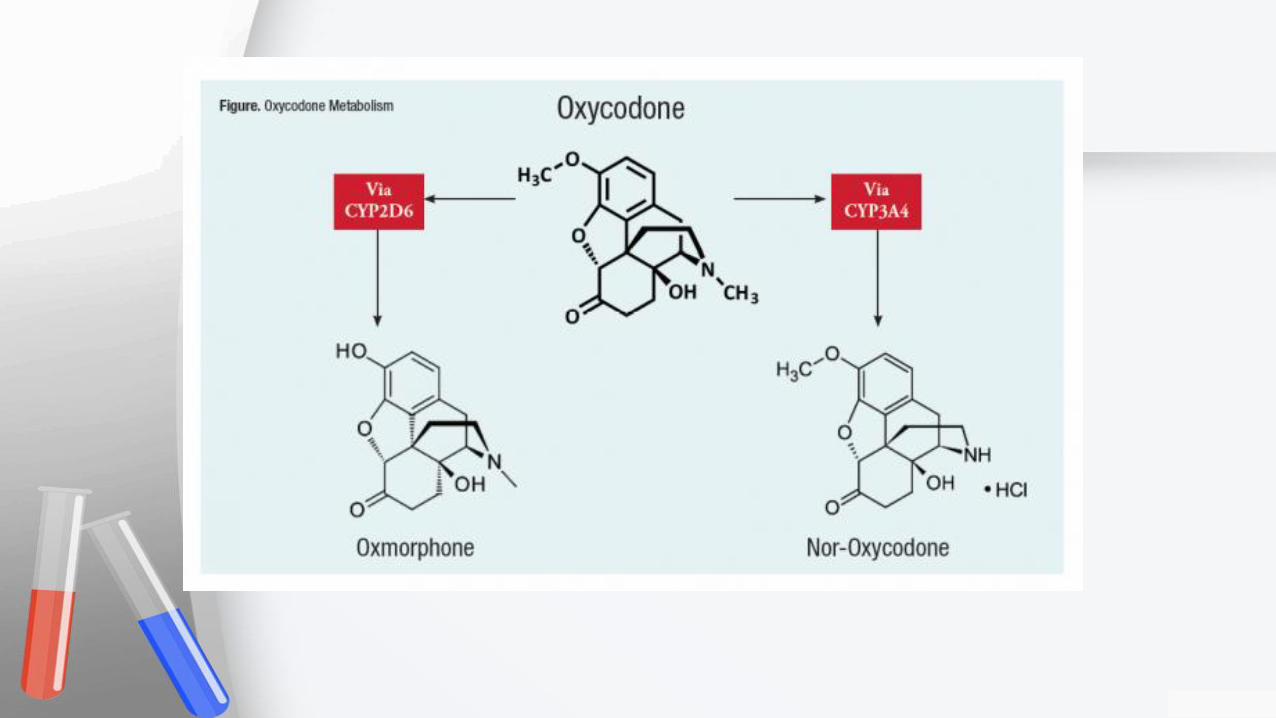
Codeine
metabolizes
to morphine

Diazepam
metabolizes to
nordiazepam,
temazepam and
oxazepam

Case 1*: Spinal Stenosis
• A confirmatory UDS by GC/MS is positive for:
– Oxazepam
– Temazepam
– Diazepam
– Nordiazepam
– Codeine
– Morphine
What would your approach
be now?
*Case 1 courtesy of Dr. Joel Bordman

“Well, yeah, laughter IS the best medicine –
But Xanax is a very close second.”

Case 1*: Spinal Stenosis
• Explore the reasons for BNZ use
• Consider non-BNZ treatments for symptoms
• Repeat UDS (3-4 wks) to ensure BNZ negative
• Educate re acceptable acetaminophen intake
WHY?
*Case 1 courtesy of Dr. Joel Bordman

https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf
Drug Urine Detection Time Frame
Methadone 4 - 5 days
Opiates 2 - 3 days
Cocaine/metabolites 2 - 4 days
Benzodiazepines 1 - 42 days
THC single use 2 - 3 days
THC habitual use Up to 12 weeks
Methamphetamine 3 - 5 days
Alcohol 6 - 24 hours

Case 2: Back Pain
• 40 y.o. male; previous lt knee injury; smokes cigarettes and MJ
• 2 month Hx of severe back pain
– CT: L4-5 herniation with encroachment
– MRI: as above with mass effect
• Tried acetaminophen, NSAIDs, PT, chiro with minimal effect

Case 2: Back Pain
• You are now considering a trial of aceta/codeine 30 mg/caffeine
• You elect to order a UDS
– Your office UDS protocol is that your administrative assistant collects and labels
the urine sample and arranges for it to be sent to the lab
• Which type of UDS do you order?
• Do you prescribe the aceta/codeine/caffeine on this visit?

Case 2: Back Pain
• Two (2) UDS (both GG/MS) arrive from the lab 1 week later
• You find no additional information from your administrative assistant and she
cannot remember any particulars
o 1st UDS positive for:
✓ BNZ, opiates, oxycodone, GBP and cotinine
o 2nd UDS positive for:
✓ THC, cotinine
What
might this
mean?

Interpreting Unexpected UDS Results
http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-UDS-QandA.pdf

Result

Case 3: Crush Injury to Hand
• 35 y.o. man
• Crush injury to right hand 2008 (surgery followed by infection …)
• On high dose oxycodone for years
• 1st UDS = October 2015
– UDS (IA) = opiates

Case 3: Crush Injury to Hand
• 35 y.o. man
• Crush injury to right hand 2008 (surgery followed by infection …)
• On high dose oxycodone for years
• 1st UDS = October 2015
– UDS (IA) = opiates
– UDS laboratory report clearly states that oxycodone is not determined by their assay

Case 3: Crush Injury to Hand
• 2011 note from ER: “suspected narcotic abuse”
• 2013 call from pharmacist re ‘polypharmacy; “away for work”
• 2014 polypharmacy; left pills in another city …
• 2015 BPI – 100% pain relief
• MD did not in, even with above
▪ Only after got a from ‘reliable’ source

Case 4: The Wandering Oxycodone
• 67 y.o. woman, long standing patient
• DM II, chronic pain, stress/anxiety
• On CR oxycodone for decades
June visit
– UDS (GC/MS) ordered Rx: CR OC 40 mg iii 5x/d + alprazolam bid
– 5 days later UDS report: alprazolam, lorazepam, lidocaine, diphenhydramine
Checked with pharmacy; pt 4 days late filling prescription

Checked with pharmacy; pt 4 days late filling prescription
http://www.prescribechangeallegany.org/assets/samhsa-toolkit_community.pdf


Case 4: The Wandering Oxycodone
• 67 y.o. woman
• DM II, chronic pain, stress/anxiety; long standing pt
• On CR oxycodone for decades
June visit
– UDS (GC/MS) ordered Rx: CR OC 40 mg iii 5x/d + alprazolam bid
– 5 days later UDS report: alprazolam, lorazepam, lidocaine, diphenhydramine
July visit
– UDS (GC/MS) ordered Rx: as above
– 6 days later UDS report: morphine, alprazolam, lorazepam, gabapentin,
diphenhydramine

Case 5: the Report?
• 25 y.o. woman; currently on hydromorphone (CR + IR) plus gabapentin
March
• UDS (IA) = opiates




Case 5: the Report?
• 25 y.o. woman; currently on hydromorphone (CR + IR) plus gabapentin
March
• UDS (IA) = opiates
“creatinine concentration and specific gravity are not consistent
with expected ranges for a normal urine”
May• UDS (GC/MS) = + morphine, codeine, hydromorphone, norhydrocodone,
diphenhydramine, pseudo/ephedrine, cotinine, lorazepam

http://mytopcare.org/prescribers/about-urine-drug-tests/

Pearls - UDS
• 2017 Guideline found only low/very low quality of evidence regarding
strategies to reduce the adverse impact of opioid prescribing
• Expert Guidance Statement 6: UDS ‘may be useful’
• Have a Standard Operating Procedure for UDS in your office/clinic
• Different UDS (POC, laboratory IA, laboratory GC/MS) have different
advantages, disadvantages and limitations

Pearls - UDS
• Always compare the UDS result to the actual patient chart/drugs prescribed
- Are the prescribed drugs/metabolites present?
- Are any prescribed drugs absent?
- Are there any unexpected drugs present?
- Read any comments listed by the laboratory
• If you encounter an inconsistent/unexpected UDS, your first action should be:
To take a careful history of medication/drug use in the past week and discuss
openly with the patient – without being accusatory
• Each type of inconsistent UDS result has a differential diagnosis and actions
for the clinician to take – documentation is key
Don’t rely on
your memory

Resources on UDS
• Ron Joe, College of BC: Urine Drug Testing
– https://www.cpsbc.ca/files/pdf/M-WS-101H-2014-09-13-P06-UDT.pdf
• Rxfiles
– http://www.rxfiles.ca/rxfiles/uploads/documents/Urine-Drug-Screening-
UDS-QandA.pdf
