urine microscopy cases - echo360
TRANSCRIPT

Urine Microscopy Cases
Mark A. Perazella, MDYale University School of Medicine
Case 1• 69 year old man presents to the ED with 1 week of 3‐4 episodes
of N/V per day, lower abdominal pain and 10 days of intermittent gross hematuria
• PMH: OA of hands and knees, mild COPD and GERD
• Medications: Aspirin, occ NSAID, albuterol inhaler, omeprazole
• Social Hx: 50 pack‐year smoking, no ETOH, no herbal remedies
• Examination: BP 150/89, P 87, afebrile
– H&N: pale conjunctiva, normal JVD, no bruit
– Chest: clear
– Heart: RRR, no rub or gallop
– Abd: soft, moderate to severe tenderness on lower abdomen, worst on RLQ, no rebound, no HSM, no bruit , no CVA tenderness
– Ext: no edema or rash
• Laboratory Results:
– Electrolytes: Na+=138, K+=4.1, HCO3=25, Cl‐=103
– BUN=29 mg/dl Cr=1.7 mg/dl
– Glucose=96 mg/dl
– Hb=10.1 mg/dl Plt=195 x1000/uL
– WBCs=6700 per mm3, Eosinophils=3%
– Urinalysis: SG‐1.012, pH‐6.0, Protein‐trace, Blood‐
2+, Glucose‐neg, Leukocyte esterase‐trace
– Urine Na+=25 mEq/L, FENa+=1.1%
Urine sediment
Case 1
• What is present on urine microscopy?
A. Dysmorphic RBCs
B. Yeast
C. Renal tubular epithelial (RTE) cells
D. Isomorphic RBCs
E. WBCs
Case 1
• What is present on urine microscopy?
A. Dysmorphic RBCs
B. Yeast
C. Renal tubular epithelial (RTE) cells
D. Isomorphic RBCs
E. WBCs

Case 1
• Based on the urine microscopy, what is the most likely diagnosis?
A. IgA nephropathy
B. Interstitial nephritis
C. Bladder cancer
D. Thin basement membrane disease
E. Acute pyelonephritis
Case 1
• Based on the urine microscopy, what is the most likely diagnosis?
A. IgA nephropathy
B. Interstitial nephritis
C. Bladder cancer
D. Thin basement membrane disease
E. Acute pyelonephritis
• Renal Ultrasound was
negative
• Renal CT scan was negative
• Fortunately, CT scan included
abdomen & pelvis
Case 1
•Bladder mass is noted on CT
scan (concerning for cancer)
• Cystoscopy/biopsy confirmed
bladder cancer
What if you saw this on urine microscopy?
Case 1a
• What is present on urine microscopy?
A. Dysmorphic RBCs
B. Yeast
C. RTE cells
D. Isomorphic RBCs
E. WBCs
Case 1a
• What is present on urine microscopy?
A. Dysmorphic RBCs
B. Yeast
C. RTE cells
D. Isomorphic RBCs
E. WBCs

Case 1a
• Based on the urine microscopy, what is the most likely diagnosis?
A. IgA nephropathy
B. Interstitial nephritis
C. Bladder cancer
D. Acute tubular necrosis
E. Acute pyelonephritis
Case 1a
• Based on the urine microscopy, what is the most likely diagnosis?
A. IgA nephropathy
B. Interstitial nephritis
C. Bladder cancer
D. Acute tubular necrosis
E. Acute pyelonephritis
Urine MicroscopyHematuria
• Visual exam of urine
– Gross hematuria
– Microscopic hematuria
– Isomorphic vs dysmorphic RBCs
• Dipstick testing for hematuria
– Very sensitive (+ with >2 RBCs/HPF)
– Not specific (+ with heme pigment)
• Definitions of hematuria
– 1 to > 10 RBC/HPF– ≥ 3 RBC/HPF on > 2 separate samples is diagnostic Dysmorphic Red Blood Cells
Acanthocytes (> 5% of RBCs)
‐ sensitivity (52%)
‐ specificity (98%)
Case 2• 48 year old man presents with several days of N/V, and
generalized weakness prompting ED visit. He admits to recently abusing cocaine and bath salts
• PMH: HIV+ , HTN, hyperlipidemia, hyperlipidemia, substance abuse, stage 3 CKD (baseline serum Cr=1.3‐1.6 mg/dl)
• Medications: elvitegravir/cobicistat/emtricitabine/tenofovir(Stribild), statin, oxycontin, neurontin, amlodipine, losartan
• Allergy: sulfa‐based medications
• Examination: BP‐148/88 P‐95 Afebrile
– H&N‐ pink conjunctiva, increased JVP
– Lungs‐ clear
– Heart‐ S1S2, no S3, rub or murmur
– Abdomen‐ benign with normal bowel sounds
– Extremities‐ trace edema
• Laboratory Results:
– Electrolytes: Na+=133 mEq/L, K+ =3.2 mEq/L,
HCO3‐ =15 mEq/L, Cl‐ =106 mEq/L, Alb 3.2 g/dl
– BUN=65 mg/dl Cr=4.7 mg/dl
– Hb=10.9 mg/dl Plt=135 x1000/uL
– WBC=15,500 per mm3, Eosinophils=5%
– Phosphorus 1.8 mg/dl Glucose 96 mg/dl
– Urinalysis: SG‐1.010, pH‐5.5, Protein‐1+, Glucose‐1+, Blood‐negative, Leukocyte esterase‐trace
– Urine Na +=98 mEq/L, FENa+=2.6%

Urine Sediment
• What is present on urine microscopy?
A. Dysmorphic RBCs
B. WBCs
C. Transitional epithelial cells
D. RTE cells
E. Oval fat bodies
Case 2
• What is present on urine microscopy?
A. Dysmorphic RBCs
B. WBCs
C. Transitional epithelial cells
D. RTE cells
E. Oval fat bodies
Case 2
• Based on the urine microscopy, what is the most likely diagnosis?
A. Thrombotic microangiopathy
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Postinfectious glomerulonephritis
E. Uroepithelial (ureteral) cancer
Case 2
• Based on the urine microscopy, what is the most likely diagnosis?
A. Thrombotic microangiopathy
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Postinfectious glomerulonephritis
E. Uroepithelial (ureteral) cancer
Case 2
Acute Tubular Apoptosis/Necrosis• luminal ectasia, loss of brush border
• tubular dropout, apoptotic figures

Urine MicroscopyCellular Elements
• Urine sediment exam
– RBCs (monomorphic vs dysmorpic)
– Epithelial cells • Squamous epithelial cells, transitional epithelial cells, renal tubular epithelial cells
– WBCs (eosinophils, PMNs, lymphocytes)
– Other cells/organisms• Malignant (lymphoid cells, uropeithelial cancer)
• Decoy cells (BK‐polyoma virus)
• Bacteria, Yeast, Mycobacterium, etc
Epithelial Cells• Squamous• Transitional• Renal Tubular
Renal Tubular Epithelial Cells
Case 3• 71 year old female presents with poor appetite, fatigue and
increased serum Cr that is noted noted on blood draw at office visit
• PMH: HTN, T2 DM, GERD, osteoarthritis, osteoporosis, COPD
• Medications: enalapril, amlodipine, glyburide, combivent inhaler, lansoprazole, calcium tablets, occasional tramadol and naproxen (for hip pain), no OTC or herbal products
• No allergies
• Examination: BP‐128/82 P‐94 T‐98.3
– H&N‐ pale conjunctiva, normal JVP
– Lungs‐ clear
– Heart‐ S1S2, no S3, or rub
– Abdomen‐ benign with normal BS, no flank tenderness
– Extremities‐ trace ankle edema, no rash
• Laboratory Results:
– Electrolytes: Na+=135, K+=5.1, HCO3=18, Cl‐=104
– BUN=59 mg/dl Cr=3.4 mg/dl
– Glucose=110 mg/dl Alb 3.4 g/dl
– Hb=10.1 mg/dl Plt=335 x1000/uL
– WBCs=12,000 per mm3, Eosinophils=1%
– Urinalysis: SG‐1.015, pH‐5.5, Protein‐1+, Blood‐
1+, Glucose‐neg, Leukocyte esterase‐2+
– Urine Na +=21 mEq/L, FENa+=0.95%
Urine Sediment

Case 3
• What is present on urine microscopy?
A. RTE cells
B. WBCs
C. RBCs
D. Transitional epithelial cells
Case 3
• What is present on urine microscopy?
A. RTE cells
B. WBCs
C. RBCs
D. Transitional epithelial cells
Urine Sediment Case 3
• What is present on urine microscopy?
A. Lipid cast
B. RTE cast
C. RBC cast
D. WBC cast
Case 3
• What is present on urine microscopy?
A. Lipid cast
B. RTE cast
C. RBC cast
D. WBC cast
Case 3
• Based on the urine microscopy, what is the most likely diagnosis?
A. Thrombotic microangiopathy
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Postinfectious glomerulonephritis

Case 3
• Based on the urine microscopy, what is the most likely diagnosis?
A. Thrombotic microangiopathy
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Postinfectious glomerulonephritis
Acute Interstitial Nephritis• Lymphocytes, plasma cells, eosinophils
• Interstitial edema with tubulitis
White Blood Cells White Blood Cells
White Blood Cells White Blood Cell Cast

White Blood Cell Casts
Case 4• 44 year old woman presents with malaise, anorexia, and lower
extremity swelling over the past 3‐4 weeks
• PMH: Obesity, T2 DM, osteoarthritis of knees, asthma
• Medications: glyburide, combivent inhaler, lansoprazole, calcium tablets, celecoxib, naproxen, no OTC or herbal products
• Allergies: PCN (rash)
• Examination: BP‐112/70 P‐97 T‐99.9
– H&N‐ pale conjunctiva, increased JVP
– Lungs‐ clear with dullness at bases
– Heart‐ S1S2, no S3, rub or 2/6 holosystolic murmur
– Abdomen‐ obese with normal BS, no flank tenderness
– Extremities‐ 3+ LE edema to the mid thighs, skin erythema with weeping blisters
• Laboratory Results:
– Electrolytes: Na+=134, K+=5.4, HCO3=16, Cl‐=105
– BUN=35 mg/dl Cr=1.4 mg/dl
– Glu=295 mg/dl
– Hb=10.9 mg/dl Plt=435 x1000/uL
– WBCs=9,300 per mm3, Eosinophils=4%
– Urinalysis: SG‐1.020, pH‐5.5, Protein‐3+, Blood‐1+,
Glucose‐1+, Leukocyte esterase‐trace
– Urine Na +=65 mEq/L, FENa+=2.4%
Urine Sediment
• What is present on urine microscopy?
A. RTE cell and fine granular cast
B. WBC and hyaline cast
C. OFB and fatty cast
D. RTE cell and hyaline cast
E. RTE cell and RBC cast
Case 4
• What is present on urine microscopy?
A. RTE cell and fine granular cast
B. WBC and hyaline cast
C. OFB and fatty cast
D. RTE cell and hyaline cast
E. RTE cell and RBC cast
Case 4
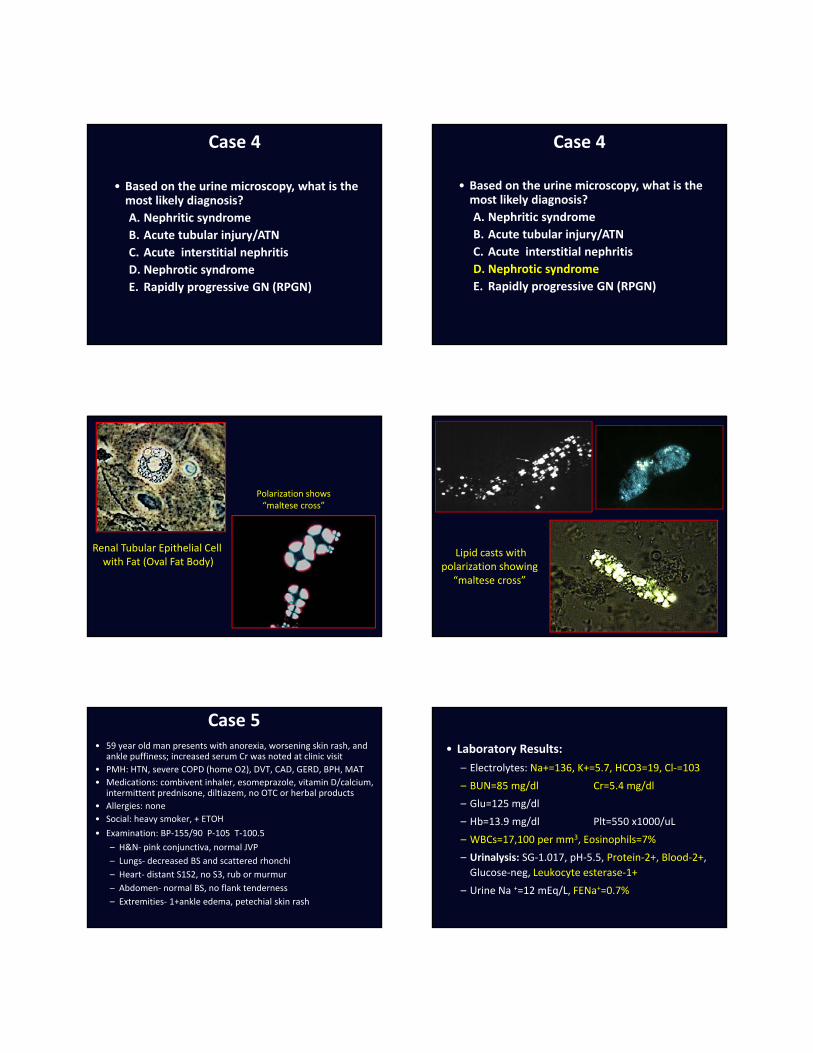
• Based on the urine microscopy, what is the most likely diagnosis?
A. Nephritic syndrome
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Nephrotic syndrome
E. Rapidly progressive GN (RPGN)
Case 4
• Based on the urine microscopy, what is the most likely diagnosis?
A. Nephritic syndrome
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Nephrotic syndrome
E. Rapidly progressive GN (RPGN)
Case 4
Renal Tubular Epithelial Cell with Fat (Oval Fat Body)
Polarization shows “maltese cross”
Lipid casts withpolarization showing
“maltese cross”
Case 5• 59 year old man presents with anorexia, worsening skin rash, and
ankle puffiness; increased serum Cr was noted at clinic visit
• PMH: HTN, severe COPD (home O2), DVT, CAD, GERD, BPH, MAT
• Medications: combivent inhaler, esomeprazole, vitamin D/calcium, intermittent prednisone, diltiazem, no OTC or herbal products
• Allergies: none
• Social: heavy smoker, + ETOH
• Examination: BP‐155/90 P‐105 T‐100.5
– H&N‐ pink conjunctiva, normal JVP
– Lungs‐ decreased BS and scattered rhonchi
– Heart‐ distant S1S2, no S3, rub or murmur
– Abdomen‐ normal BS, no flank tenderness
– Extremities‐ 1+ankle edema, petechial skin rash
• Laboratory Results:
– Electrolytes: Na+=136, K+=5.7, HCO3=19, Cl‐=103
– BUN=85 mg/dl Cr=5.4 mg/dl
– Glu=125 mg/dl
– Hb=13.9 mg/dl Plt=550 x1000/uL
– WBCs=17,100 per mm3, Eosinophils=7%
– Urinalysis: SG‐1.017, pH‐5.5, Protein‐2+, Blood‐2+,
Glucose‐neg, Leukocyte esterase‐1+
– Urine Na +=12 mEq/L, FENa+=0.7%

Urine Sediment
• What is present on urine microscopy?
A. RTE cell cast
B. WBC cast
C. RBC cast
D. Fatty cast
E. Hyaline cast
Case 5
• What is present on urine microscopy?
A. RTE cell cast
B. WBC cast
C. RBC cast
D. Fatty cast
E. Hyaline cast
Case 5
• Based on the urine microscopy, what is the most likely kidney lesion?
A. Proliferative glomerulonephritis
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Membranous glomerulonephritis
E. Nephrolithiasis with bilateral urinary obstruction
Case 5
• Based on the urine microscopy, what is the most likely kidney lesion?
A. Proliferative glomerulonephritis
B. Acute tubular injury/ATN
C. Acute interstitial nephritis
D. Membranous glomerulonephritis
E. Nephrolithiasis with bilateral urinary obstruction
Case 5
Proliferative (necrotizing) glomerulonephritis• Segmental necrosis• Cellular proliferation• Crescent formation

Urine MicroscopyCasts
• Urine sediment exam
– Cells found admixed with casts• RBCs (isomorphic vs dysmorphic)
• Renal tubular epithelial cells
• WBCs (PMNs, eosinophils, lymphocytes), OFBs
– Non‐cellular Casts• Hyaline, Broad, Waxy, other
– Cellular Casts• RBC casts
• WBC casts
• Renal tubular epithelial cell casts
• Granular casts (muddy brown, pigmented)Red Blood Cell Cast
Red Blood Cell Cast RBC Cast & Dysmorphic RBCs
Case 6• 85 year old woman presents with anorexia, diarrhea, fever, and
left leg pain present to the ED for evalaution
• PMH: HTN, COPD , CAD, peptic ulcer disease, osteoporosis, OA, and atrial fibrillation
• Medications: combivent inhaler, esomeprazole, vitamin D/calcium, warfarin, diltiazem, occasional ibuprofen, and furosemide
• Allergies: None
• Social: nonsmoker, ‐ ETOH
• Examination: BP‐105/68 P‐112 T‐100.5
– H&N‐ pale conjunctiva, normal JVP
– Lungs‐ decreased BS
– Heart‐ distant S1S2, irreg irreg rhythm, no S3, rub or murmur
– Abdomen‐ normal BS, no flank tenderness
– Extremities‐ trace ankle edema, erythema with blisters LLE
• Laboratory Results:
– Electrolytes: Na+=135, K+=5.3, HCO3=22, Cl‐=100
– BUN=65 mg/dl Cr=2.3 mg/dl
– Glu=285 mg/dl
– Hb=11.9 mg/dl Plt=250 x1000/uL
– WBCs=13,000 per mm3, Eosinophils=3%
– Urinalysis: SG‐1.018, pH‐5.5, Protein‐1+, Blood‐1+, Glucose‐1+, Leukocyte esterase‐trace
– Urine Na +=41 mEq/L, FENa+=1.7%

Urine Sediment
• What is present on urine microscopy?
A. RTE cell cast
B. WBC cast
C. Waxy cast
D. Hyaline cast
E. Fatty cast
Case 6
• What is present on urine microscopy?
A. RTE cell cast
B. WBC cast
C. Waxy cast
D. Hyaline cast
E. Fatty cast
Case 6
• Based on the urine microscopy, what is the most likely diagnosis?
A. Progressive CKD
B. Prerenal AKI
C. Acute tubular injury/ATN
D. Acute interstitial nephritis
E. Membranoproliferative GN
Case 6
• Based on the urine microscopy, what is the most likely diagnosis?
A. Progressive CKD
B. Prerenal AKI
C. Acute tubular injury/ATN
D. Acute interstitial nephritis
E. Membranoproliferative GN
Case 6
Prerenal AKI• No biopsy
AKI (serum Cr returned to baseline)resolved over 48 hours with IV fluids
and holding diuretics

Urine MicroscopyCasts
• Urine sediment exam
– Cells found admixed with casts• RBCs (isomorphic vs dysmorphic)
• Renal tubular epithelial cells
• WBCs (eosinophils), OFBs
– Non‐cellular Casts• Hyaline casts
• Broad, Waxy casts
– Cellular Casts• RBC casts
• WBC casts
• Renal tubular epithelial cell casts
• Granular casts (muddy brown, pigmented)
Hyaline Casts
Waxy Casts
Case 7• 75 year old man is brought to the ED by his daughter with altered
sensorium, fever/chills, productive cough, SOB and diarrhea; increased serum Cr was noted in the ED
• PMH: Lung cancer s/p lobectomy, COPD, HTN, CAD, GERD, & BPH
• Medications: combivent inhaler, lansoprazole, ASA, amlodipine, tamsulosin, s/p XRT and chemotherapy (8 weeks ago)
• Allergies: None
• Social: former smoker, ‐ ETOH
• Examination: BP‐98/54 P‐124 T‐101.5
– H&N‐ pale conjunctiva, normal JVP
– Lungs‐ decreased BS, crackles at L base, and scattered wheezes
– Heart‐ distant S1S2, no S3, rub or murmur
– Abdomen‐ normal BS, no flank tenderness
– Extremities‐ Trace ankle edema
• Laboratory Results:
– Electrolytes: Na+=133, K+=5.1, HCO3=16, Cl‐=100
– BUN=65 mg/dl
– Cr=2.4 mg/dl‐‐>3.3‐‐>4.1‐‐> 5.3
– Hb=8.9 mg/dl Plt=98 x1000/uL
– WBCs=21,000 per mm3, Eosinophils=3%
– Urinalysis: SG‐1.020, pH‐6.0, Protein‐1+, Blood‐
trace, LE‐trace
– Urine Na +=13 mEq/L, FENa+=0.65%
Urine Sediment

• What is present on urine microscopy?
A. RTE cells
B. WBCs
C. RBCs
D. Transitional epithelial cells
Case 7
• What is present on urine microscopy?
A. RTE cells
B. WBCs
C. RBCs
D. Transitional epithelial cells
Case 7
• What is present on urine microscopy?
A. Hyaline casts
B. Granular casts
C. RBC casts
D. WBC casts
E. Waxy casts
Case 7
• What is present on urine microscopy?
A. Hyaline casts
B. Granular casts
C. RBC casts
D. WBC casts
E. Waxy casts
Case 7
• Based on the urine microscopy, what is the most likely diagnosis?
A. Acute postinfectious GN
B. Acute tubular injury/ATN
C. Prerenal AKI
D. Acute interstitial nephritis
E. ANCA vasculitis (pulmonary renal syndrome)
Case 7

• Based on the urine microscopy, what is the most likely diagnosis?
A. Acute postinfectious GN
B. Acute tubular injury/ATN
C. Prerenal AKI
D. Acute interstitial nephritis
E. ANCA vasculitis (pulmonary renal syndrome)
Case 7
Acute Tubular Apoptosis/Necrosis• Luminal ectasia, loss of brush border
• Tubular dropout, apoptotic figures
Urine MicroscopyCasts
• Urine sediment exam
– Cells found admixed with casts• RBCs (isomorphic vs dysmorphic)
• Renal tubular epithelial cells
• WBCs (eosinophils), OFBs
– Non‐cellular Casts• Hyaline, Broad, Waxy, other casts
– Cellular Casts• RBC casts
• WBC casts
• Renal tubular epithelial cell casts
• Granular casts (muddy brown, pigmented)Renal Tubular Epithelial Cell Cast
Renal Tubular Epithelial Cell Cast Granular Casts

Case 8• 58 year old obese female presents with malaise,
weakness, and frequent “oily” stools for a few weeks
• PMH: HTN, T2‐DM, arthritis, CKD (baseline serum Cr=2.1 mg/dl), GERD, asthma, gout, hypothyroid
• Medications: diltiazem , singular, furosemide, pantoprazole, orlistat, allopurinol, colchicine prn, synthroid, bactrim for URI for past 7 days, no herbal products or NSAIDs
• Examination: BP‐130/80 P‐82 Afebrile– H&N‐mild conjunctival pallor, elevated JVP
– Lungs‐minimal bibasilar crackles
– Heart‐ S1S2, 1/6 SM, no rub
– Abdomen‐ obese, no flank pain
– Extremities‐ trace edema of ankles
• Laboratory Results:– Electrolytes: Na+‐136 mEq/L, K+‐4.8 mEq/L, HCO3‐‐26 mEq/L, Cl‐‐99 mEq/L
– BUN=52 mg/dl Cr=3.8 mg/dl ‐> 5.8
– Hb=10.2 mg/dl Plt=286 x1000/uL
– WBCs=17 per mm3
– Uric acid=10.6 mg/dl Ca++=8.7 mg/dl PO4=5.5 mg/dl
– Urinalysis: SG=1.018, pH=6.0, Protein‐trace, Blood‐negative, Glucose‐negative, Leukocyte esterase‐negative
– Urine Na += 71 mEq/L, FENa+=2.7%, Pro/Cr ratio=0.45
• Renal Ultrasound:– 10.4 and 10.7 cm kidneys
– Increased cortical echogenicity
Urine Sediment
• What crystals are present on urine microscopy?
A. Sulfonamide crystals
B. Calcium phosphate crystals
C. Calcium oxalate crystals
D. Uric acid crystals
E. Hippurate crystals
Case 8
• What crystals are present on urine microscopy?
A. Sulfonamide crystals
B. Calcium phosphate crystals
C. Calcium oxalate crystals
D. Uric acid crystals
E. Hippurate crystals
Case 8