uropean medicines agency drug safety · pdf filefor the assessments and related documents...
TRANSCRIPT

EUROPEAN MEDICINESAGENCY DRUG SAFETYPRACTICES AND TOOLS
Henry Fitt, Kevin Blake, Xavier KurzPharmacovigilance & Risk ManagementEuropean Medicines Agency, London

Contents
• Eudravigilance & Signal Detection• EPITT• THIN• ENCePP

Background – Need To Further Strengthen Pharmacovigilance • 5% of all hospital admissions are for Adverse Drug Reactions (ADRs)
• 5% of all hospital patients suffer an ADR• ADRs are the 5th most common cause of hospital death
• Estimated 197,000 deaths per year in EU from ADRs
• EU societal cost of ADRs amounts to Euro 79 Billion per year
Source: Annex 2 of the Report on the impact assessment of strengthening and rationalising EU Pharmacovigilance COMMISSION OF THE EUROPEAN COMMUNITIES Sept 2008
Post authorisation safety monitoring
• Pre‐authorisation clinical trials are not of sufficient size to elucidate and characterise every adverse effect of a medicinal product
• Results cannot be assumed to be generalisable to patients who will use the product in a usual care setting
• Special populations such as the elderly are underrepresented in pre‐authorisation clinical trials
• Spontaneous reporting systems are an important source for safety monitoring in post‐authorisation “real‐life” setting

National Competent Authorities (NCAs)
Marketing Authorisation Holders
(MAHs)
ICSRs outside the EEAICSRs within the EEA
Data-Processing Network
Secure e-reporting of Individual Case Safety
Reports (ICSRs)
Signal Detection and Data Analysis for EMA/Member
States (MSs)ICSRs for all
medicines authorised in the EEA
EudraVigilance: A data processing network and management system for reporting and evaluating suspected ADRs in EEA
EudraVigilance
• An average of ~72,000 ICSRs reported monthly from Jan‐Jun 2011
• Total number of ICSRs approaching 5 million
• Approx. 8,000 users and >100,000 product presentations in EV Medicinal Product Dictionary
• Almost 24,000 queries performed in EV Data Analysis System (EVDAS) by National Competent Authorities (NCAs) (Jan‐Jun 2011)
• EudraVigilance now ranks within the 3 largest databases on adverse drug reactions in the world

EudraVigilance Reports per month
Number of ICSRs (excluding backlog) received per month in EV (2004 - 2011)
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
Jan 2
004
May 20
04Sep
2004
Jan 2
005
May 20
05Sep
2005
Jan 2
006
May 20
06Sep
2006
Jan 2
007
May 20
07Sep
2007
Jan 2
008
May 20
08Sep
2008
Jan 2
009
May 20
09Sep
2009
Jan 2
010
May 20
10Sep
2010
Jan 2
011
May 20
11Sep
2011
EVPM ICSR(s) EVCTM ICSR(s)
Signal Management (SM) definition and steps• SM – set of activities to determine whether there are new
risks associated with a medicinal product or whether risks have changed based on various data sources*
• Steps:• signal detection• signal validation and confirmation• prioritisation, analysis and assessment • recommendation for action
* ICSRs (EudraVigilance, national databases, company specific), data from active surveillance systems or studies, literature and other available

Signal Detection at the EMA
• Signal detection and Data analysis section within the Pharmacovigilance and Risk Management Sector of the Patient Health Protection Unit
• Focused on EudraVigilance data• In liaison with (Co)‐Rapps and PhVWP• Scope: ~ 600 Centrally Authorised Products (CAPs) plus
new MAA under evaluation at EMA• Periodic signal detection for centrally authorised
products based on reaction monitoring reports

Signal Detection at the EMAMain tool for signal detection is the electronic Reaction Monitoring Report (e‐RMR):
• A periodical formatted Excel file which contains ICSRs historically submitted in EudraVigilance + new data submitted during the period of interest;
• Tool that facilitate screening and filtering of large dataset to support signal detection activities;
• Facilitates review of signals of disproportionality reporting (SDR)
• Allows selection of cases of interest to view CIOMS forms.


1/3 - Structure of the e-RMR worksheet
Active su
bstan
ces
MedDRA Structure
SO
Cs
HLG
Ts
HLTs
SM
Qs (n
arrow)
PTs
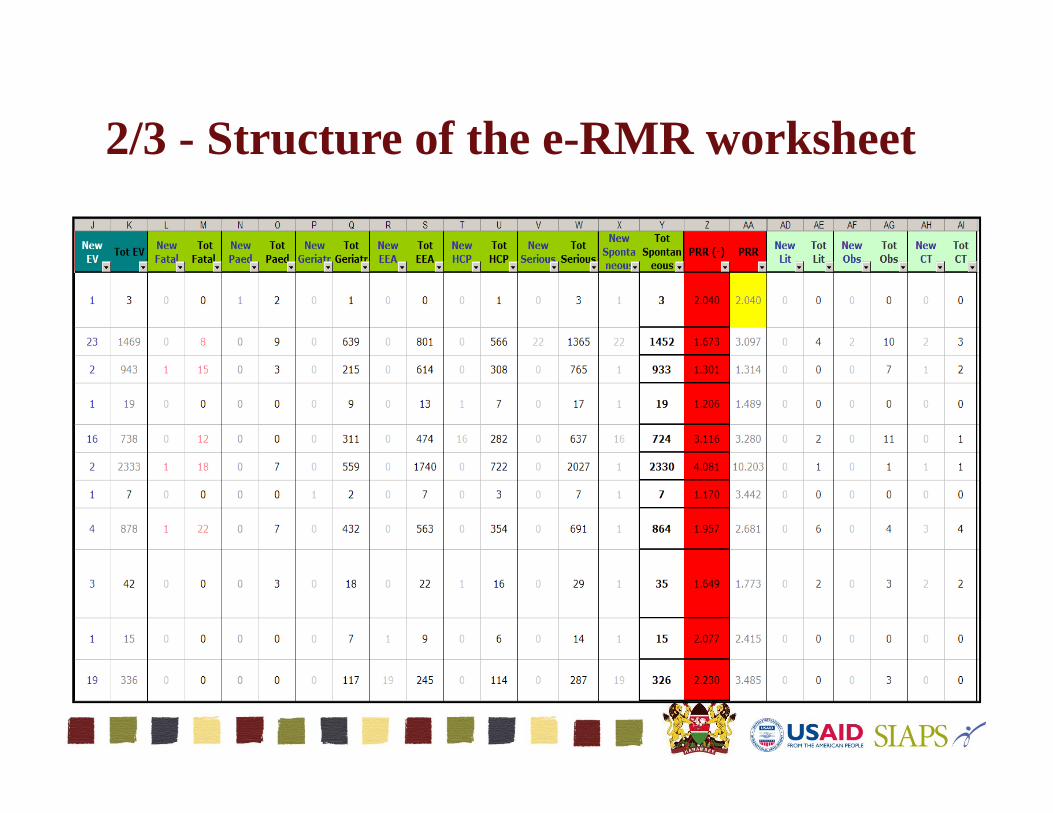
2/3 - Structure of the e-RMR worksheet
EV C
ases
Fatal cases
SPONTANEOUS
Paediatric cases
Geriatric cases
EEA cases
HCP cases
Serious cases
Total cases
PR
R(-)/
PR
R
OTHERS
Literature cases
Observational studies
CT cases

3/3 - Structure of the e-RMR worksheet
Operational columns
Med
DR
A P
T code
IME
DM
E
Ch
ang
es
SD
R (n
)

Key activities in screening the e-RMR
• Selection of a reference period• Prioritisation of ADRs for review based on several criteria
• Grouping/selection of paediatric/geriatric ADRs• Filtering by new literature reports received in EV• Filtering/selection of ADRs from studies/RCTs • Comparison of various ‘Totals’• Search at the level of the SOC/HLGT/HLT• Filtering by multi‐axial SMQs

Factors in signal detection
• Clinical judgment • Clinical relevance and potential impact on public health (e.g.
hepatic failure, agranulocytosis, serious allergic reactions, fatal medication errors)
• Number of reports >3, statistical threshold applied to screen for signals
• Check for expectedness against the latest approved or submitted product information
• Evaluation of the signal by the Rapporteur • Evaluation of the signal by a scientific committee (e.g. CHMP,
PhVWP)• Ongoing regulatory procedure relevant to the signal

Validation of activities
• Statistical methods can lead to earlier detection of safety signals – approx. 54% signals were detected earlier (mean time saved 2.45 years)
• 20% signals detected earlier by traditional methods• 26% not detected by statistical methods ‐ established
pharmacovigilance and PRR analysis are complementary
• Validation of Statistical Signal detection for CAPs in EudraVigilance• Drug Saf 2010; 33:(6):475‐487
New PV legislation• ADRs are big burden to patients and society• Signal Detection using spontaneous reporting systems is an
important source for safety monitoring in post authorisation “real‐life” setting.
• The main objective of the new pharmacovigilance legislation is to promote and protect public health by reducing the burden of ADRs and optimising the use of medicines
• There are opportunities for improved data collection and enhanced signal detection that should be considered carefully in order to further strengthen pharmacovigilance

EPITT (European Pharmacovigilance Issues Tracking Tool)
• Database facilitating the tracking and sharing of safety information related to the medicinal products / substances for human use, between the NCAs and the Agency (about 350 users within the European Economic Area)
• 4 “main modules” : Safety Issues, Safety Signals, PSURs (Periodic Safety Update Reports), RMPs (Risk Management Plans)

EPITT• Objectives:
• Tracking of Safety Issues and Signals independently of the marketing authorisation type (incl. PhVWP discussions, Rapid Alerts, PhVWP recommendations and SmPC wordings updates...),
• Tracking and monitoring of the PSUR cycles, timetable for the assessments and related documents (scope: Centrally Authorised Products + Work Sharing project),
• Tracking of the EU‐RMP Annexes 1 submitted by the Marketing Authorisation Holders, together with the implementation of the regulatory actions they require,
• Support to the European Incident Management Plan procedure.


The THIN database
• The Health Improvement Network Database at EMA• Collects all data from subset of General Practice computer systems.
• Population based data ‐ 5% UK population• Practices geographically representative of England and Wales
• Anonymised at source• Simple flat file structure• Regularly updated

Clinical Databases
• Designed for patient management
BUT
• Allow opportunities to do rapid analyses on wide range of pre‐existing clinical data. Hence very useful research tool.

Examples from EMA
• Investigation of dosages of Somatropin given to children in UK• Challenging because dose adjusted for body weight
• Rosiglitazone – Is it given even in presence of cardiac contraindications?• Complete GP data gives simple and powerful approach to this sort of question.

The European Network of Centres for Pharmacoepidemiology & Pharmacovigilance (ENCePP)The aim of ENCePP:• Bring together expertise in the fields of
pharmacovigilance & pharmacoepidemiology scattered across Europe.
• Further strengthen the post‐authorisation monitoring of medicinal products in Europe.
• Focus on academia and not‐for‐profit organisations.• Facilitate post authorisation studies: high quality
independent multi-centre

How does ENCePP work?
ENCePP Steering Group•16 members in total:• 6 elected: from network• 6 appointed:
• Heads of Medicines Agencies (HMA),
• Committee for Medicinal Products for Human Use (CHMP),
• Committee for Orphan Medicinal Products (COMP)
• CHMP’s Pharmacovigilance Working Party (PWP),
• CHMP’s Patient and Consumers Working Party (PCWP),
• International Society of Pharmacoepidemiology (ISPE),
• International Society of Pharmacovigilance (ISoP)• 3 members from EMA•2 observers:
• European Federation of the Pharmaceutical Industries & Associations (EFPIA)
• Int’l Regulatory Agency (to be appointed)

Who are the ENCePP partners?• Universities, hospitals;• Owners of healthcare databases and/or electronic registries;• Other public/non‐profit research centres specialised in PhV;• Existing European networks covering certain rare diseases,
therapeutic fields and adverse drug events of interest. • For‐profit organisations
• provided that they perform studies commissioned by third parties and their main focus is pharmacoepidemiology and pharmacovigilance research

Who are the ENCePP partners?
• 103 centres
• 14 networks
• 24 data sources
from 17 different European countries
(data as of 12 April 2012)

ENCePP guiding principles
Independence
Standards
Transparency
Stimulate consideration of
important study principles in design of studies
Registration of studies
Publication of protocols and results
Clear roles and responsibilities of
researcher & funder
Freedom to publish
Code of Conduct
Methodological Standards Checklist & Guide
E-Register of Studies (Code of Conduct)

ENCePP Studies
To reinforce the confidence
of the public, other researchers as well as regulators
that research done under the ENCePP “seal” is as far as possible free from biases and commercial, financial and personal influences.

For further information:
www.encepp.eu