u.s. access board accessibility for diagnostic medical equipment computed tomography / nuclear...
TRANSCRIPT

U.S. Access BoardAccessibility for Diagnostic Medical
Equipment
Computed Tomography / Nuclear Medicine
May 8, 2012John JaeckleGE HealthcareChief Regulatory Affairs StrategistMITA – Chair, CT GroupMITA - Co-Chair MI Dose Task ForceChair of IEC MT-30 – CT safety and performance standards.
Eduard ToerekPhilips HealthcareDirector, Quality & RegulatoryCT/NM Imaging SystemsMITA – Vice Chair, CT Group
May 8, 2012 1

United States Access BoardGoal has long been and continues to be to
ensure access to diagnostic equipment for all patients.
Prescription only devices, must be cleared by FDA
Clinical objective of a study is to acquire diagnostic data for all patients for the area of interest in the head and body that are within the capabilities of the system
Computer Tomography (CT)– X-Ray tube rotates around the patient. Multiple images taken
from different angles are combined to create detailed cross-sectional images.
Nuclear Medicine/Multi-Modality– Nuclear Imaging includes PET and SPECT, Multi-modalities
also exist for nuclear imaging which include combinations of PET/CT, PET/MR, or SPECT/CT
– PET/CT is primarily used to diagnose, stage and monitor cancerous growths and metastases, SPECT and SPECT/CT is primarily for cardiac studies with a growing presence in early cancer detection; both modalities are used in neurology applications
May 8, 2012 3
Patient are always assisted by trained staff during entire study – patient preparation for injections, entering the exam room, placement/positioning and removal from table, and exiting the exam room.

CT Systems
May 8, 2012
Tilting Gantry
4

Nuclear Medicine PET/CT Scanner
May 8, 2012 5

General Nuclear Medicine, SPECT/CT
May 8, 2012 6

General Nuclear Medicine / SPECT
General Nuclear Medicine accessible via:– Wheelchair– Seated– Standing– Gurney/bed


Clinical Use of Equipment Equipment cannot be used independently by patient
– Access must be through physician order or prescription (not used for routine, periodic, asymptomatic screening types of scans)
– Technologist always present for the study. Discusses examination with the patient, assesses ability of the patient to complete the study, assists in placement and positioning of the patient on the table and patient preparation for oral and IV injections of contrast material. Often comes into the scan room between series to check patient and reassure them.
Equipment designed to effectively image patients of all ages and sizes (up to table weight capacity/bore size)
Designed for virtually all situations including critical care, limited mobility patients, trauma/emergency room cases, unconscious & seriously ill patients
May 8, 2012 10

Technical Criteria
CT, PET, SPECT, PET/CT, SPECT/CT, PET/MR Scanners– M301 Supine, prone, or side-lying position– M305.2 Transfer Supports– M306 Communication, 2 methods: audible, visible or tactile
General Nuclear Medicine Scanners– M301 Lying, M302 Seated, M303 Wheelchair, M304 Standing– M305.2 Transfer Support– M305.3 Standing Support– M306 Communication, 2 methods: audible, visible or tactile
M307 Operable Parts– Does not apply
May 8, 2012 11

Typical Features of Current Systems Features of current design
– Long couch/table for patient to lay on during diagnostic scans– Patient transfer from gurney to couch is very common– Couch vertical motion for patient load and imaging– Wide variety of patient positioning pads and straps– Gantry tilt for patient positioning– Patient Lift compatibility– Intercom system between the patient and technologist– Window between scan control room and scan room– Ability to conduct scan in-room by technologist
May 8, 2012 12

Technical Considerations
Transfer Surface Height– Structural and drive components in base of table
Transfer Supports– Design standards require safety factors of x4 to x12 for patient
support– May impact clinical utility or broader access
May 8, 2012 13
Avoid requirements that would compromise the functionality, features, and clinical utility of the scanners.

Patient Lifts
May 8, 2012
Ref. Americans with Disabilities Act / Access to Medical Care for Individuals with Mobility Disabilities
14

Patient Transfer
May 8, 2012
Ref. Americans with Disabilities Act / Access to Medical Care for Individuals with Mobility Disabilities
15
Siting Requirements Large capital equipmentFixed installation (not portable)Room layout can require up to 400 sq. ft. or
moreScan room limitations, shielding requirementsADA requirements are considered during site
layout and planningOptional custom facility room layout could
incorporate patient lifts, accommodate patient mobility devices, etc.
May 8, 2012 16


Patient Communication
Intercom Window between
control & scan rooms
X-Ray On visual and audible indicators
Voice Commands Breathing
Lights/timers
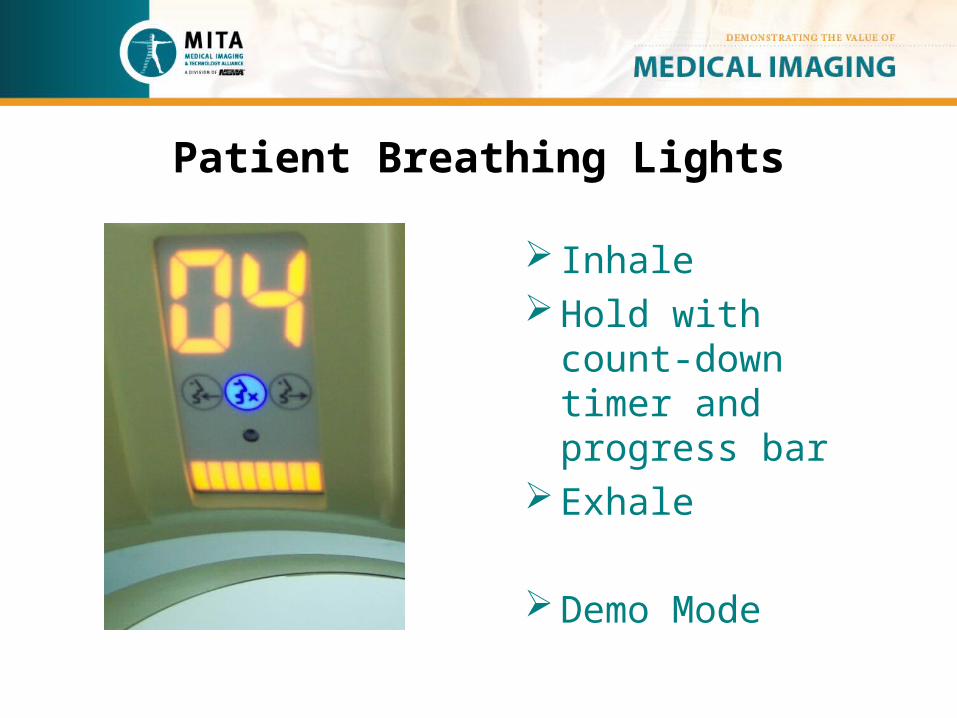
Patient Breathing Lights
InhaleHold with count-
down timer and progress bar
Exhale
Demo Mode

Training– Onsite training using customer installed equipment
• Patient handling & positioning
– Instructor-led classroom training at manufacturer’s training center
– RT Certification/registration training includes training modules on proper patient handling/transfer
– User facility based training in support of their required patient transfer protocols and procedures
May 8, 2012 20

Other Standards
Application of existing Standards (IEC, ISO, AAMI Usability/Human Factors standards)
AAPM TG66 Positional Accuracy Requirements 21 CFR 1020.30 General X-Ray & 1020.33
Computed Tomography Equipment IEC 60601-1-6 / 62366 Usability IEC 60601-2-44 Particular requirements for
the safety of X-Ray equipment for computed tomography
May 8, 2012 21

Transition Time for Design Changes
– Design changes require adherence to regulatory Design Controls and Verification & Validation (V&V)
– Design changes to subassemblies are typically multi-year projects, and even longer for complete system redesign
– Design changes incur significant up front investment which drives up the cost of re-designed medical equipment
May 8, 2012 22

Recommendations New requirements to be applicable to forward production
only, field retro-fit and refurb may not be feasible
Communication via 2 methods is supportable
Enhance site planning guides with ADA and Access Board considerations
Other technical criteria should be relaxed or exempted for large/complex fixed equipment, not used for ambulatory screening, requires healthcare professional assistance, and is a prescription only device NOT for independent use
May 8, 2012 23

Future Opportunities
As technology continues to advance, manufacturers continually incorporate features and capabilities to improve the patient experience & accessibility while optimizing and advancing the diagnostic capabilities of the equipment for all patients.
Feedback from clinicians is used as system design inputs for continuous improvements to products, services and accessories.
May 8, 2012 24

APPENDIX
U.S. Access BoardAccessibility for Diagnostic Medical Equipment

Step & Shoot Gated Aorta CTA of Renal Arteries of the kidney

General Nuclear Medicine / SPECT
May 8, 2012 27


Patient Lifts
May 8, 2012 29

Site Layout
May 8, 2012 30
Breathing Lights & Voice Commands
2-way intercom
Visual contact with patient

Patient Positioning Aids
May 8, 2012 31