use of a heart lung machine in cardiac surgery
TRANSCRIPT
February, 1961
Use of a Heart Lung Machine in Cardiac Surgery
Mary A. Costello, C.R.N.A.and Samuel Kaplan, M.D.*
Cincinnati, Ohio
Although surgical treatment forheart disease has been available formany years, definitive treatment ofintracardiac abnormalities requiredthe development of methods wherebythe heart chambers could be enteredand lesions treated under direct vision.The first step in this direction was theuse of general body hypothermiawhich reduces the tissue oxygen de-mand. When the body temperaturewas reduced to about 28-32° C, theblood flow through the heart could bearrested temporarily and some intra-cardiac lesions treated. The majordrawbacks of this method were: 1) thetime limits of the intracardiac pro-cedure (±8 minutes) 2) the ven-tricular chambers could not be enteredwithout excessive hazard. The suc-cessful development of heart lungmachines overcame these problems sothat the vast majority of cardiac ab-normalities are now accessible fordefinitive surgical treatment underdirect vision.
The function of these machines isto divert the venous blood from theinferior and superior vena cava to adevice which will oxygenate the blood
*From the Department of Surgery (Divisionof Anesthesia) and Pediatrics, College of Medi-cine, and Children's Hospital, Cincinnati.
Supported in part by Public Health Service,Grant No. H-2427, National Heart Institute.
Presented at the annual meeting, AmericanAssociation of Nurse Anesthetists, San Francisco,August 29, 1960.
and remove adequate amounts of car-bon dioxide. The arterialized bloodis then pumped into the systemic ar-terial system, usually via the femoralartery. Thus when the heart lungmachine is in operation the only bloodthat enters the heart is from the coro-nary sinus (into the right atrium)and from the bronchial vessels (intothe left atrium via the pulmonaryveins). The chambers of the heartcan now be opened (cardiotomy) tocorrect intracardiac defects under di-rect vision. These procedures areknown as open heart surgery duringtotal body perfusion (or cardiopul-monary bypass). The purpose of thispaper is to report the results of sur-gery in 100 consecutive patients inwhom the heart lung machine wasused for the treatment of congenitalheart disease during the last three andone-half years. The role of the anes-thetist as a part of the surgical teamwill be emphasized and the use ofmonitoring devices stressed.
METHODA. Anesthesia
The patients were premedicatedwith Nembutal®, Demerol® and atro-pine. The dose of these drugs variedaccording to the age and weight ofthe subjects. Adults received about100 mgms. Demerol®, 0.4 mgms. atro-pine and 100 mgms. Nembutal®. Thedosage schedule for infants and chil-dren was as described previously.'
19
J Am Assoc Nurs Anesth. 1961;29(1):19-28.
20
Originally, induction of anesthesiawas started with a small dose ofPentothal Sodium® intravenously(± 50 mgms. of a 2.5% solution)followed by a mixture of nitrousoxide, oxygen and ether using thehigh liter flow technique. To facilitateendotracheal intubation, transtrachealblock with 5% Cyclaine® was usedin adults.
In children, open drop ether wasgiven after Pentothal Sodium® induc-tion until anesthesia was deep enoughto permit the insertion of an endo-tracheal tube. More recently the anes-thetic agents used were a mixture ofFluothane2 , nitrous oxide and oxygen.When premedication was inadequatein children, a sleeping dose of Pento-thal Sodium® was given prior to theuse of nitrous oxide, oxygen andFluothane. Ether was added to thismixture prior to endotracheal intuba-tion in some children. The more re-cent anesthesia technique in adultsconsisted of induction with PentothalSodium® followed by the administra-tion of Fluothane, ether, nitrous oxide(flow of 2 liters per minute) and oxy-gen (3 liters per minute). Ether wasdiscontinued after endotracheal in-tubation was accomplished and anes-thesia was maintained with low per-centages of Fluothane, nitrous oxideand oxygen.
Ventilation was accomplished byaugmented respiration until the pleurawas entered. At that time Demerol®was given intravenously to abolishthe respiratory drive and ventilationwas continued using the "hand andbag" method. During the period oftotal body perfusion the lungs wereventilated with 100% oxygen. Anes-thetic gas mixtures were not addedto the heart lung machine. In themajority of instances supplemental
J. Am. A. Nurse Anesthetists
anesthesia during the period of cardio-pulmonary bypass was not necessary.However, a solution of 2.5% Pento-thal Sodium® was available at alltimes and was given into the heartlung machine when indicated. Whentotal body perfusion was discontinueda small percentage of Fluothane wasagain introduced and respirations con-trolled until the chest was air tight.Spontaneous respirations were thenre-established. Towards the end of theprocedure ventilation was assistedwith a mechanical respirator to ensurean inspiratory pressure of about10 cms. water.
Throughout the whole proceduregreat care was taken to maintain aclear airway to attempt to preventthe onset of acute or prolonged par-tial hypoxia. This was accomplishedby the optimal placement of the endo-tracheal tube, intermittent aspirationof tracheobronchial secretions and theprevention and treatment of broncho-spasm. After the chest incision wasclosed prophylactic tracheostomy wasperformed in those patients in whoma stormy postoperative course waspredicted. This included patients whohad severe pulmonary hypertension,recurrent or recent pneumonitis, orpoor risk subjects with severe cardiacmalformations. The presence of thetracheostomy tube allowed continuedassisted inspiration with a mechanicalrespirator and a method for adequateaspiration of tracheobronchial secre-tions in the immediate postoperativeperiod. In the majority of patientstracheostomy was not performed andthey were placed in an oxygen tentfor 2-3 days after surgery.
B. The Heart Lung MachineThe Clark bubble oxygenator and
pump was used in all patients. Detailsof the apparatus have been published
February, 1961
elsewhere.8 Venous blood was arteri-alized with oxygen bubbles of varyingsize. Small bubbles (10-50 micron)have a large surface and are extremelyefficient in oxygenating the blood.The flow of large bubbles (200-500microns) will remove excess carbondioxide. The oxygen gas flow was con-trolled by the arterial oxygen tensionand pH (see later). If the oxygentension fell below the desired levelthe flow of small bubbles was in-creased. If the pH fell (i. e. the bloodbecame acidotic) the flow of largebubbles was increased to remove morecarbon dioxide. The blood and gasmixture was then allowed to flow overteflon shreds covered with silicone(polymethylsiloxane). This materialcoalesced the excess gas. The arteri-alized blood then entered the pump-ing chamber which was electronicallycontrolled so that the flow rate wasknown at all times. The blood entereda monitoring chamber before it wasreturned to the patient. In the latterchamber the oxygen tension, pH andtemperature of the blood weremeasured.
The patients' venous blood wasbrought to the heart lung machinevia two catheters inserted into thesuperior and inferior vena cavae. Thearterialized blood was returnedthrough a cannula placed in the fe-moral artery with its tip facing prox-imally. Thus the blood flow in theaorta was retrograde during the periodof perfusion.
The left heart was decompressedin all patients by the insertion ofcannulae into the left atrium and leftventricle. The blood from thesechambers was aspirated and returnedto the heart lung machine. Duringcardiotomy intracardiac blood wasaspirated with hand suckers and re-turned to the oxygenator. In specific
patients the coronary circulation wascontrolled by occluding the ascendingaorta between the origin of the coro-nary arteries and the innominateartery. In these circumstances via-bility of the myocardium was pro-tected by stopping the heart beatwith coronary perfusion of potassiumcitrate in the earlier cases and localmyocardial hypothermia (± 170 C)in the later patients.
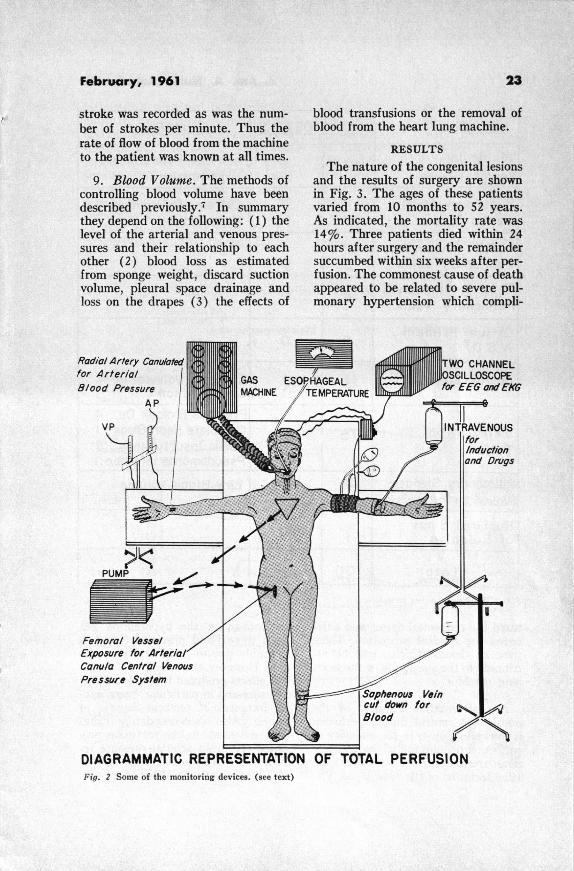
C. Monitoring Devices1. Systemic Blood Pressure. A
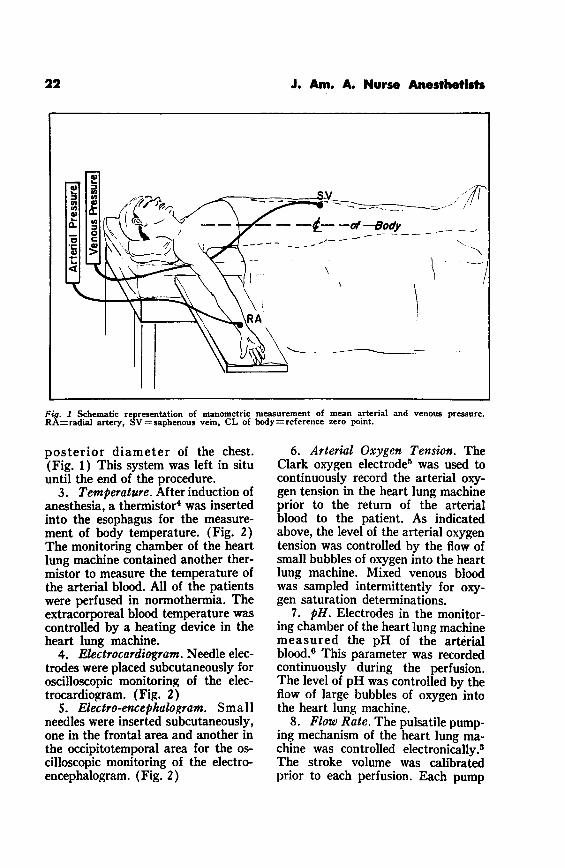
blood pressure cuff was attached to theupper arm of all patients. Ausculta-tory measurements were relied upononly at the beginning and the end ofthe procedure. In all patients priorto the preparation of the surgical fielda peripheral artery, either the radialat the wrist or the brachial at theantecubital fossa was cannulated forthe direct measurement of mean ar-terial pressure. The cannula was at-tached to a simple mercury mano-meter. The reference zero point ofthe manometer was the mid point ofthe anteroposterior diameter of thechest. (Fig. 1) Pulsations of themercury column synchronous with theheart beat ensured that the systemwas open. The cannula was left insitu until the end of the surgical pro-cedure and was removed only whenthe blood pressure could be measuredwithout difficulty using the ausculta-tory technique.
2. Venous Pressure. In the first 30patients of this series, mean venouspressure was measured from both thesuperior and inferior vena cava. Morerecently the venous pressure wasmeasured only from the inferior venacava after this vessel was cannulatedfrom the saphenous vein at the groin.The cannula was attached to a simplewater manometer and the referencezero was the mid point of the antero-
21
J. Am. A. Nurse Anesthetists
Fig. 1 Schematic representation of manometric measurement of mean arterial and venous pressure.RA=radial artery, SV=saphenous vein, CL of body=reference zero point.
posterior diameter of the chest.(Fig. 1) This system was left in situuntil the end of the procedure.
3. Temperature. After induction ofanesthesia, a thermistor4 was insertedinto the esophagus for the measure-ment of body temperature. (Fig. 2)The monitoring chamber of the heartlung machine contained another ther-mistor to measure the temperature ofthe arterial blood. All of the patientswere perfused in normothermia. Theextracorporeal blood temperature wascontrolled by a heating device in theheart lung machine.
4. Electrocardiogram. Needle elec-trodes were placed subcutaneously foroscilloscopic monitoring of the elec-trocardiogram. (Fig. 2)
5. Electro-encephalogram. Smallneedles were inserted subcutaneously,one in the frontal area and another inthe occipitotemporal area for the os-cilloscopic monitoring of the electro-encephalogram. (Fig. 2)
6. Arterial Oxygen Tension. TheClark oxygen electrode 5 was used tocontinuously record the arterial oxy-gen tension in the heart lung machineprior to the return of the arterialblood to the patient. As indicatedabove, the level of the arterial oxygentension was controlled by the flow ofsmall bubbles of oxygen into the heartlung machine. Mixed venous bloodwas sampled intermittently for oxy-gen saturation determinations.
7. pH. Electrodes in the monitor-ing chamber of the heart lung machinemeasured the pH of the arterialblood. 6 This parameter was recordedcontinuously during the perfusion.The level of pH was controlled by theflow of large bubbles of oxygen intothe heart lung machine.
8. Flow Rate. The pulsatile pump-ing mechanism of the heart lung ma-chine was controlled electronically. 3
The stroke volume was calibratedprior to each perfusion. Each pump
- -- -- -of--Body -
,-' -
^
22
February, 1961
stroke was recorded as was the num-ber of strokes per minute. Thus therate of flow of blood from the machineto the patient was known at all times.
9. Blood Volume. The methods ofcontrolling blood volume have beendescribed previously. 7 In summarythey depend on the following: (1) thelevel of the arterial and venous pres-sures and their relationship to eachother (2) blood loss as estimatedfrom sponge weight, discard suctionvolume, pleural space drainage andloss on the drapes (3) the effects of
Radial Artery Canulotedfor Arterial IBlood Pressure
Exposure for ArterialoCanula Central VenousPressure System
blood transfusions or the removal ofblood from the heart lung machine.
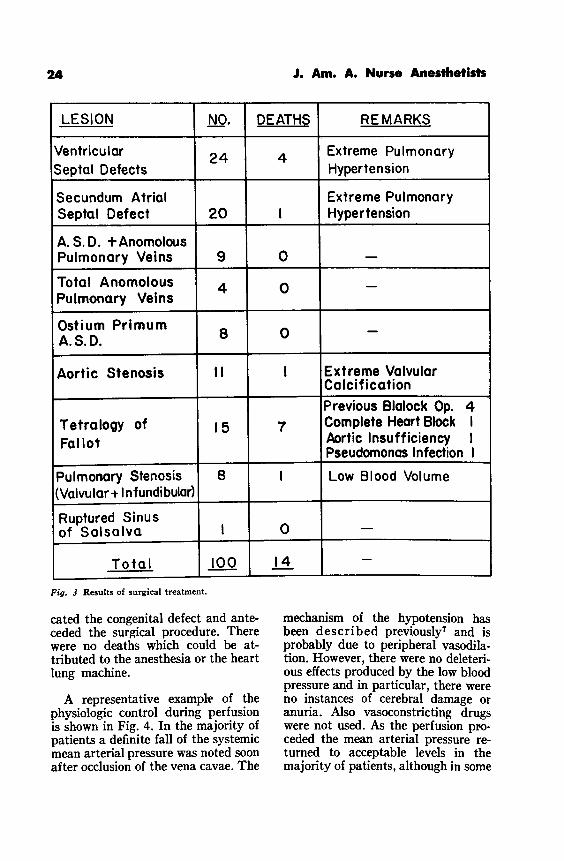
RESULTS
The nature of the congenital lesionsand the results of surgery are shownin Fig. 3. The ages of these patientsvaried from 10 months to 52 years.As indicated, the mortality rate was14%. Three patients died within 24hours after surgery and the remaindersuccumbed within six weeks after per-fusion. The commonest cause of deathappeared to be related to severe pul-monary hypertension which compli-
DIAGRAMMATIC REPRESENTATION OF TOTAL PERFUSIONFig. 2 Some of the monitoring devices. (see text)
J. Am. A. Nurse Anesthetists
LESION NO. DEATHS REMARKS
Ventricular 24 4 Extreme PulmonarySeptal Defects Hypertension
Secundum Atrial Extreme PulmonarySeptal Defect 20 I Hypertension
A. S.D. + AnomolousPulmonary Veins 9 0 -
Total Anomolous 4 0 -Pulmonary Veins
Ostium Primum 8 -A.S.D. 8
Aortic Stenosis II I Extreme ValvularCalcification
Previous Blalock Op. 4Tetralogy of 15 7 Complete Heart Block I
Follot Aortic Insufficiency IPseudomonos Infection I
Pulmonary Stenosis 8 I Low Blood Volume(Valvular + Infundibular)
Ruptured Sinusof Salsalva I 0 -
Total 100 14 -
Fig. 3 Results of surgical treatment.
cated the congenital defect and ante-ceded the surgical procedure. Therewere no deaths which could be at-tributed to the anesthesia or the heartlung machine.
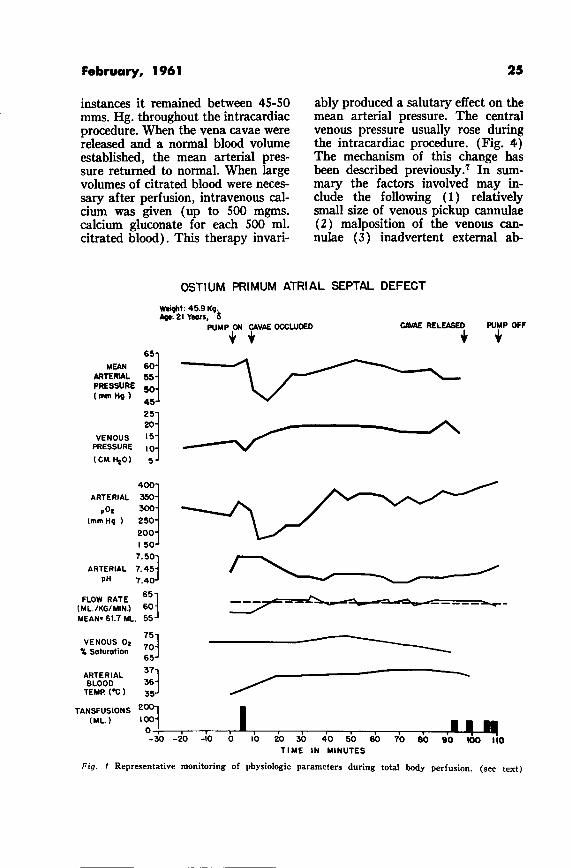
A representative example of thephysiologic control during perfusionis shown in Fig. 4. In the majority ofpatients a definite fall of the systemicmean arterial pressure was noted soonafter occlusion of the vena cavae. The
mechanism of the hypotension hasbeen described previously7 and isprobably due to peripheral vasodila-tion. However, there were no deleteri-ous effects produced by the low bloodpressure and in particular, there wereno instances of cerebral damage oranuria. Also vasoconstricting drugswere not used. As the perfusion pro-ceded the mean arterial pressure re-turned to acceptable levels in themajority of patients, although in some
24
February, 1961
instances it remained between 45-50mms. Hg. throughout the intracardiacprocedure. When the vena cavae werereleased and a normal blood volumeestablished, the mean arterial pres-sure returned to normal. When largevolumes of citrated blood were neces-sary after perfusion, intravenous cal-cium was given (up to 500 mgms.calcium gluconate for each 500 ml.citrated blood). This therapy invari-
ably produced a salutary effect on themean arterial pressure. The centralvenous pressure usually rose duringthe intracardiac procedure. (Fig. 4)The mechanism of this change hasbeen described previously. 7 In sum-mary the factors involved may in-clude the following (1) relativelysmall size of venous pickup cannulae(2) malposition of the venous can-nulae (3) inadvertent external ab-
OSTIUM PRIMUM ATRIAL SEPTAL DEFECT
MEANARTERIALPRESSURE(mm Hg)
VENOUSPRESSURE
(CM. H20)
65
60
45
15
5
Weight: 45.9 Kg.Age: 21 Yeors,
PUMP ON CAVAE OCCLUDED CAVAE RELEASED PUMP OFF
400
ARTERIAL 350
p02 300
(mm Hg ) 250
200
150
7.50
ARTERIAL 745
pH 7.4 0
FLOW RATE 65(ML./KG/MIN.) 60MEAN" 61.7 ML. 55
75
VENOUS 02 I. Saturation
65
ARTERIALBLOOD 36
TEMP ('C) 3
TANSFUSIONS2(ML.) I 1Ji I~ U.
0 '
-30 -20 -10 0 10 20 30 40 50 60 70 80 90 100 110TIME IN MINUTES
Fig. 4 Representative monitoring of physiologic parameters during total body perfusion. (see text)
25
I I
26
dominal pressure. In some patientsduskiness of the face was noted withan elevated superior vena caval pres-sure. This can be prevented by opti-mal placement of the superior venacava cannula to prevent partial ob-struction of blood flow through thisvessel. After excannulation of thevena cavae, the venous pressureusually returned to normal.
The oxygen tension of the arterialblood was maintained at relativelyhigh levels throughout the period ofperfusion. (normal ± 120 mms. Hg.)In the majority of patients the ar-terial oxygen tension was above 300mms. Hg. during most of the periodof cardiotomy. The relatively highoxygen tension was due to a smallvolume of oxygen dissolved in theplasma. Bubbles of oxygen were notnoted in the arterial blood and therewere no instances of oxygen embolism.
The pH of the arterial blood re-mained within normal limits duringthe period of perfusion. (Fig. 4) Con-trolled respiration prior to attach-ment of the patient to the heart lungmachine may result in acidosis fromcarbon dioxide accumulation or alka-losis from over-ventilation. These fac-tors were corrected by varying thevolume of large bubble flow into theoxygenator as indicated above. Ani-mal experiments in our laboratorieshave indicated that a significant me-tabolic acidosis does not occur duringcardiopulmonary bypass so thatchanges in pH are attributed to car-bon dioxide accumulation or loss.Postoperative respiratory acidosiscomparable to that reported in pa-tients undergoing thoracotomy forprocedures not involving perfusion,may occur but is mild and of shortduration. 8
The rate of flow of arterial bloodfrom the apparatus to the patient
J. Am. A. Nurse Anesthetists
varied according to the weight of thepatient. 8 In the example shown inFig. 4 the average flow rate was 2832ml. per minute (61.7 ml./KG/min.or 2.0 L/M 2 ). Because the saturationof the mixed venous blood remainedbetween 70-75%, it may be assumedthat the oxygen requirements of thetissues were supplied adequately.
Blood transfusions during perfu-sion were necessary in the majorityof cases. (Fig. 4) The indications forblood transfusion were one or moreof the following7 : (1) a low and fall-ing mean arterial and central venouspressure (2) "flutter" in the venouspickup line (3) inadequate venousinflow into the heart lung machinewhen mechanical factors such as kinksin the line or poor placement of thecannulae could be excluded (4) asudden accidental loss of blood (5) ifthe mean arterial pressure is not wellmaintained, although the central ven-ous pressure is normal, transfusioncould be considered.
Oscilloscopic visualization of theelectrocardiogram was found to beuseful throughout the whole proce-dure. On occasion impending hypoxiawas preceded by the development ofany arrhythmia, usually ventricularextrasystoles. Complete heart blockoccurred during cardiotomy in 4 pa-tients with ostium primum atrialseptal defect, 2 patients with tetral-ogy of Fallot and 2 patients withventricular septal defects. This com-plication was treated with large dosesof intravenous Isuprel® which re-verted the heart block to sinusrhythm in 5 instances. One patientsuccumbed to heart block 1 monthafter surgery. In 2 instances completeheart block has persisted. The fol-lowup period in these latter patients
February, 1961
is 3 years and 18 months. To datethe implantation of myocardial elec-trodes has not been necessary.
Although the electro-encephalogramwas visualized oscilloscopically in thisgroup of patients, its value has beendubious. It is believed that deteriora-tion or flattening of the waves of theelectro-encephalogram are late mani-festations of cerebral damage. Usuallythe other monitoring devices de-scribed above heralded the develop-ment of a complication which wasovercome prior to significant electro-encephalographic changes.
DISCUSSION
Laboratory experience with theheart machine in dogs indicated thatsuccessful total body perfusion de-pended in a great measure on theappreciation of physiologic changes
occurring during cardiopulmonary by-pass. This experience was transferredto the operating room where the abovementioned monitoring devices werefound to be essential in the successof the surgical procedure. We believethat these monitoring devices do notmake the operation more complex.In many instances they forewarnedthe operating room team of impend-ing complications which were notrecognized by clinical observation ofthe patient. These complications wereanticipated and controlled before theyappeared. The basic principles of totalbody perfusion depend on optimaloxygenation of blood, removal of ade-quate amount of carbon dioxide anda flow of blood to meet the metabolicrequirements of the body. Thereforeit is a fundamental requirement thatvariation of these parameters beknown at all times during total body
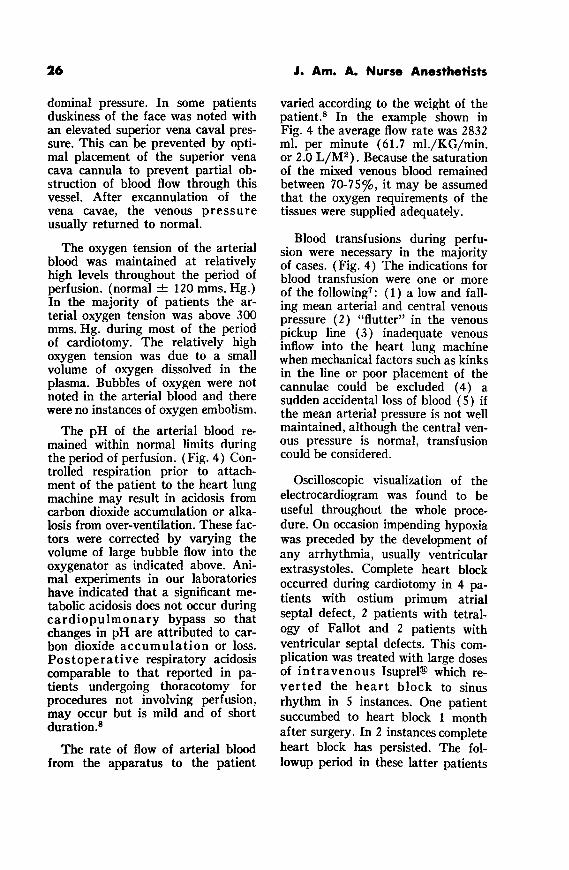
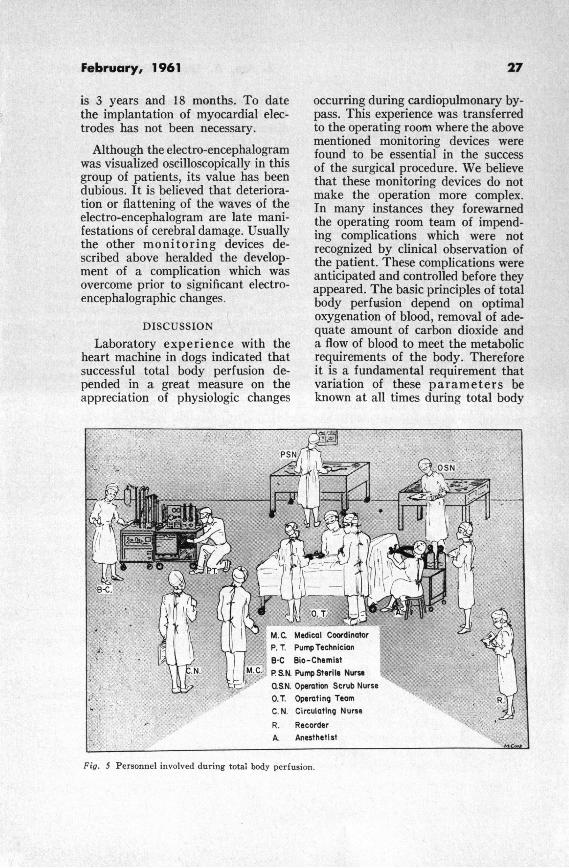
Fig. 5 Personnel involved during total body perfusion.
28
perfusion. This was accomplished bythe monitoring described above.
Fig. 5 represents the personnel ofour clinic during surgery with theheart lung machine. They consist ofthe following groups: (1) operatingsurgeon, assistants and scrub nurse(2) pump operator, biochemist andscrub nurse (3) anesthetist (4) re-corder (5) coordinator. The latterindividual acts as a liaison betweenthe other groups. It is his functionto advise the pump operating team ofchanges in the operative field whichwould influence perfusion techniquesin specific patients. Physiologicchanges related to anesthesia andblood volume are controlled and treat-ed by the coordinator. He also actsas the direct liaison between the sur-geon and the other groups. This sys-tem has allowed the surgeon to pro-ceed with the intracardiac procedurewithout being concerned with theminutia of physiologic and biochemi-cal detail of these major surgicalprocedures.
SUMMARY
(1) The results of surgery in 100consecutive patients in whom the
J. Am. A. Nurse Anesthetists
Clark heart lung machine was usedfor the treatment of congenital heartdisease is reported.
(2) The role of the anesthetist inthese procedures is emphasized.
(3) Monitoring devices to controlphysiologic and biochemical changesare stressed.
REFERENCES
1. Costello, M. A.: Anesthesia for ChildrenUndergoing Tonsillectomy. J. Am. A. NurseAnesthetists 17:25, 1949.
2. Costello, M. A.: Fluothane: A Clinical Evalu-ation. J. Am. A. Nurse Anesthetists 28:153,1960.
3. Clark, L. C.: Optimum Flow Rates in Per-fusion in Extracorporeal Circulation. Spring-field, Ill. Charles C Thomas, 1958.
4. Clark, L. C. and Trolander, H.: Thermometerfor Measuring Body Temperature in Hypo-thermia. J.A.M.A. 155:251, 1954.
5. Clark, L. C.: Monitor and Control of Bloodand Tissue Oxygen Tensions. Trans. Am. Soc.Artificial Internal Organs. 2:41, 1946.
6. Clark, L. C.; Kaplan, S.; Matthews, E. C.;Edwards, F. K. and Helmsworth, J. A.:Monitor and Control of Blood Oxygen Ten-sion and pH During Total Body Perfusion.J. Thoracic Surg. 36:488, 1958.
7. Kaplan, S.; Edwards, F. K.; Helmsworth,J. A. and Clark, L. C.: Blood Volume Duringand After Total Extracorporeal Circulation.A.M.A. Arch. Surg. 80:31, 1960.
8. Matthews, E. C.; Clark, L. C.; Edwards, F.K. ;Kaplan, S. and Helmsworth, J. A.: StudiesDuring the Immediate Postoperative PeriodFollowing Total Body Perfusion. A.M.A.Arch. Surg. 77:313, 1958.