using frameworks to measure and promote quality and ...€¦ · evolving the care model to achieve...
TRANSCRIPT

Using Frameworks to Measure and Promote Quality and Integrated Care
Richard Antonelli, MD, MS Medical Director of Integrated Care
Boston Children’s Hospital / Harvard Medical School Boston, USA
29 November 2016

Acknowledgements
• Federation for Children with Special Needs/ Family Voices • David K. Urion, MD, Director, Behavioral Neurology Clinics and Programs, Department of Neurology, Boston Children's Hospital • Menno Verhave, MD, Clinical Director, GI and Nutrition, BCH • Jennifer McCrave, RN, Senior Nurse, Ambulatory Child Neurology, BCH
• Lori Hartigan, RN, Senior Nurse, Ambulatory GI, BCH • Casey Fee, SM, Program Manager, Integrated Care, BCH • Hannah Rosenberg, MSc, Project Manager, Integrated Care, BCH
Funding Support • US Maternal and Child Health Bureau
– American Academy Pediatrics • Lucile Packard Foundation for Children’s Health • Harvard Pilgrim Health Care Foundation Quality Grants Program

Objectives
• Discuss a framework of care integration implementable at the level of the care delivery system
• Distinguish care integration from care coordination
• Discuss tools that measure and support continuous improvement of high value, person- and family-centered outcomes

Take Away Messages
• Build Capacity of Work Force
– Develop competencies to support integration
– Inter-professional education
• Implement Measures of Care Integration
• Implement Measures of Care Coordination
• Track Outcomes, Including Value
– Quality, Safety
– Cost
– Experience

Miguel
• 4 year old Hispanic boy
• Dx with asthma by PCP
• referred for “poor attention”
• ED visit 3 times in prior year for asthma
• no assessment/ intervention for
attention

One Family’s
Care Map
www.childrenshospital.org/care-coordination-curriculum/care-mapping
6

Health & Social Service Spending Combined
Source: EH Bradley et al. Health and social services expenditures: associations with health outcomes. BMJ Qual Saf; 2011;20:826-831.

Healthy, Preventive
Chronic
Complex
Matching Services to Complexity– Including Social, Medical, Behavioral
Children with complex needs --Neurodevelopmental (Autism, etc.) --Behavioral/Psychiatric --Hematology/ Oncology
• Sickle cell • Hemophilia
--Technology dependent --Multiple Chronic Conditions -- Social Risk Factors
Children with chronic conditions --Behavioral (ADHD, depression, anxiety, PTSD) --Asthma -- Obesity --Diabetes -- Social Risk Factors

Costs Across Population Reflect Prevalence, and Service Needs/ Utilization
Total Paid Amount
Re
lati
ve C
ost

Achieving Optimal Value
• Chronic Conditions
– Enhancing F/PCMH performance
– Enhance Subspecialty “Access”
• Collaborative Care Models
• More timely access to actionable information
• More timely access to appointments
• Virtual access to referring providers
• Virtual access to patients/ families
– Enhance Patient Self-Management Skills


Specialist or PCP comfortable with high risk patients as the medical home. Patient's specialists highly
connected and identified patient coordinator supports the patient and/or family, including social
and behavioral health needs.
Healthy, Preventive
Chronic
Complex
Evolving the Care Model to Achieve High Value
PCP as the medical home and specialist visits as needed. Most care
coordination is conducted by the patient and/or family.
PCP as the primary care medical home + the patient’s specialists. PCP care team support care coordination
with the patient and/or family.

Family Experience of CC Supporting BH Needs
27.7% 18.7%
74.7%
44.6%
28.9%
71.1%
16.3%
41.6% 47.0% 36.7%
18.7%
58.4%
13.9%
0.0%10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%
What has helped you, past or present, in gaining knowledge and understanding about your child's Mental Health needs?


Team Roles and Structure: One Model
Courtesy Heather Walter, MD

Care Coordination the set of activities in “the space between”- Visits, Providers,
Hospital Stays [Turchi RM, Antonelli RC et al. Patient- and Family-Centered Care Coordination: A Framework for Integrating Care
For Children and Youth Across Multiple Systems. Pediatrics. May 2014.
Integrated Care seamless provision of health care services, from the perspective of the patient
and family, across entire care continuum. It results from coordinating the efforts of all providers, irrespective of
institutional, departmental, or community-based organizational boundaries.
Care Integration for Children with Special Health Needs:
Improving Outcomes and Managing Costs. National Governors Association Center for Best Practices, 2012

Domains of Integrated Care
Align with “Triple Aim”– Better Health, Better Care, Less Cost Per Capita
• Person, Patient, Family, Caregiver Experience • Care Coordination
o Closing the Loop
o High Quality Handoffs
o Care Tracking
o Care Planning
• Utilization and Financial Outcomes o Admissions, readmissions, Emergency Dept utilization
• Provider Experience

A Qualitative Study of Families with Children Seeing Multiple Health Care Providers
Aim: Explore and define how families who have children with multiple care providers perceive care integration and assess how well their child’s care is integrated
Funded by Lucile Packard Foundation for Children’s Health

Families said that integrated care would involve:
• “A knowledgeable professional taking some responsibility for a holistic look at my kid.”
• “Help with prioritizing.”
• “To really know everyone on the team, to have good working relationships.”
• “Someone who clears the path for me.”

Authentic Outcome Measure of Patient/ Family Experience Pediatric Integrated Care Survey (PICS)

Pediatric Integrated Care Survey (PICS)
Validation of a Parent-Reported Experience Measure of Integrated Care, Pediatrics, in press • Family reported measure to inform Quality Improvement/interventions
• The PICS is:
– 19 validated experience questions + health care status/utilization & demographic questions
– Supplementary and topic specific modules – Spanish version is available
• Development funded by Lucile Packard Foundation for Children’s Health


Pediatric Integrated Care Survey (PICS)
23

CTM= Care Team Member

Domains of Integrated Care
Align with “Triple Aim”– Better Health, Better Care, Less Cost Per Capita
• Person, Patient, Family, Caregiver Experience
• Care Coordination o High Quality Handoffs o Closing the Loop
o Care Tracking
o Care Planning
• Utilization and Financial Outcomes o Admissions, readmissions, Emergency Dept utilization
• Provider Experience

26
Elements of a High Quality Information Exchange
• Purpose of the referral request from the view of PCP or other
entity. Family engaged in process of referral choice and goal setting
• Relevant information received by community organization or specialist, including clinical, behavioral/ social risk factors
• Management relationship specified (eg, limited number of consults, continued co-management, etc.)
• Care planning across team members

Domains of Integrated Care
Align with “Triple Aim”– Better Health, Better Care, Less Cost Per Capita
• Person, Patient, Family, Caregiver Experience
• Care Coordination o High Quality Handoffs
o Closing the Loop o Care Tracking
o Care Planning
• Utilization and Financial Outcomes o Admissions, readmissions, Emergency Dept utilization
• Provider Experience

28
Closing the Loop: Follow-Up Referrals
0%20%40%60%80%
100%
Jun Jul Aug Sep Oct Nov
FY2015 FY2016
Pe
rce
nt
of
Follo
w U
p N
ote
s C
om
mu
nic
ate
d
Communication of Follow Up Note to Ordering Provider and PCP
Communicated to PCP Communicated to Ordering Provider
4
47 46
70
53
30
0%
20%
40%
60%
80%
100%
0
10
20
30
40
50
60
70
80
Jun Jul Aug Sep Oct Nov
FY2015 FY2016
Nu
mb
er
of
Follo
w U
ps
Performance on Follow Up Referrals
Follow Ups Ordered
Follow Ups Completed
Percent of Follow UpsCompleted

Domains of Integrated Care
Align with “Triple Aim”– Better Health, Better Care, Less Cost Per Capita
• Person, Patient, Family, Caregiver Experience
• Care Coordination o Closing the Loop
o High Quality Handoffs
o Care Tracking
o Care Planning
• Utilization and Financial Outcomes o Admissions, readmissions, Emergency Dept utilization
• Provider Experience

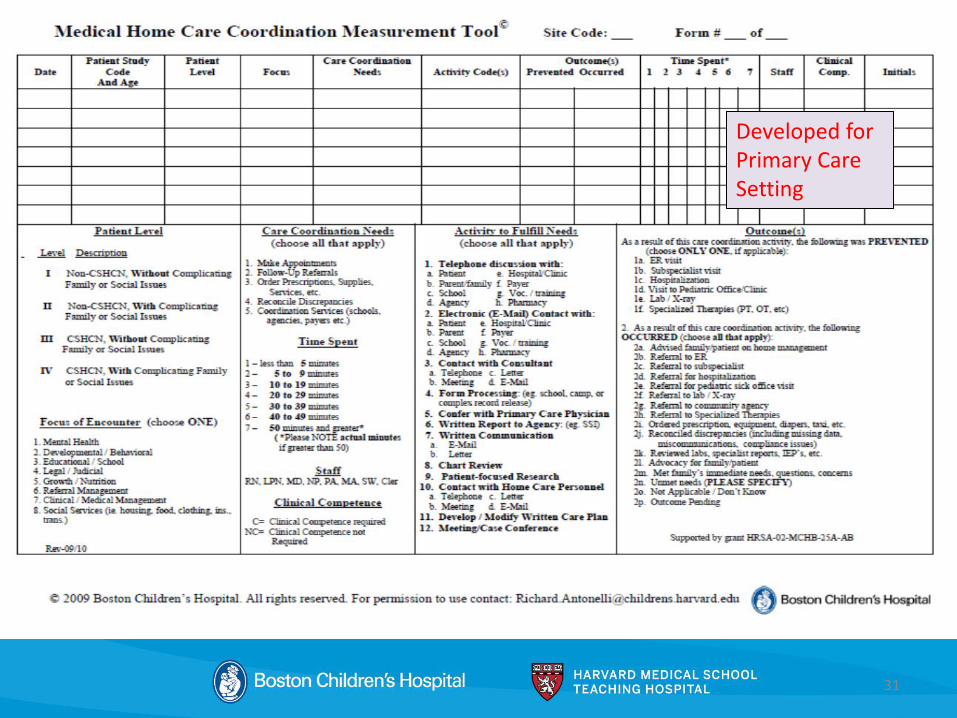
Care Coordination Tracking and Planning
Care Coordination Measurement Tool (CCMT)
• Captures Value of CC activities– For Both QI and Business Planning – Supports efforts of all disciplines doing CC
– Identify Gaps and Redundancies in Care (eg, vulnerable and underserved populations)
– Rationalization of workforce education and deployment-- functioning at “top of license or scope”
– More accurate reflection of true cost of care– enables sustainability of move from reactive to proactive care; fee-for-service to value-based care delivery
• Adapted to capture activities/ outcomes in diverse settings (adult, child) – Community Health Workers
– Social Workers
– Primary Care
– Subspecialty Care (behavioral, surgical, medical)
– Home Care
– Families
• Access BCH website: http://www.childrenshospital.org/care-coordination-curriculum/care-
coordination-measurement
31
Developed for Primary Care Setting

32
9%
11%
13%
16%
16%
21%
27%
54%
0% 10% 20% 30% 40% 50% 60%
Developed/modified clinical plan
Reconciled discrepancies
Education/anticipatory guidance
Scheduled clinic visit
Advocated for patient/family
Confer with provider (specialist)
Advised family on home management
Prescriptions/supplies ordered
Percent of Encounters
Outcomes Occurred
• Data represents care coordination encounters for patients with enteral tubes
Value Capture- Specialty Setting Boston Children’s Hospital
Division of Gastroenterology CCMT
7%
9%
10%
20%
47%
66%
0% 10% 20% 30% 40% 50% 60% 70%
Reconcile Discrepancies
Coordination of Services (Schools, Agencies, Payers)
Make Appointments
Education
Ordered Prescriptions/ Supplies/ Services
Clinical Management
Percent of Encounters
Care Coordination Needs
4%
5%
10%
12%
15%
20%
30%
0% 5% 10% 15% 20% 25% 30% 35%
Hospitalization
PCP Visit
Specialist/Clinic Visit
Urgent Clinic Visit
MD Phone Call
ED visit
Supply Problem
Percent of Encounters
Outcomes Prevented

Promising Early Financial Outcomes
• Integrated care model for patients with complex needs
• Reduced expense by 10%, primarily by shifting in-patient to ambulatory care
• Reduced 30 day, all cause readmissions from 22% to 13%
• Reduced Emergency Department usage

Funded by US Maternal and Child Health Bureau; co-created with National Family Voices

How To Sustain This?
• Altruism only goes so far…

Value-Based Payment Models for Medicaid Child Health Services
Payment model for all children except for those with Medical Complexity • Capitated Primary Care Payment (incorporating behavioral health) • CC Payment (risk adjusted per-patient-per-month) • Performance Incentive Bonus
Value-Based Payment for Children with Medical Complexity • Total Cost of Care-model evolving from shared savings to shared risk • CC Payment- risk adjusted per-patient-per-month
Other • Episode-based payment • Performance incentive/ shared savings- social determinants of health • Joint Accountability • Cross-subsidization
Value-Based Payment Models for Medicaid Child Health Services. Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, Bailit Health. (2016)

Take Away Messages
• Build Capacity of Work Force
– Develop competencies to support integration
– Inter-professional education
• Implement Measures of Care Integration
• Implement Measures of Care Coordination
• Track Outcomes, Including Value
– Quality, Safety
– Cost
– Experience

Contact
Medical Director of Integrated Care
Boston Children’s Hospital
Harvard Medical School

What’s Next in United States?




• Validation of a Parent-Reported Experience Measure of Integrated Care, Ziniel, S, Rosenberg, H, Bach, A, Singer, S, Antonelli, R, Pediatrics, in press
• Making Care Coordination a Critical Component of the Pediatric Health System: A Multidisciplinary Framework. Antonelli R, McAllister J, Popp J.. The Commonwealth Fund. May, 2009.
• MA Child Health Quality Coalition Care Coordination Framework. Funded by the Centers for Medicare and Medicaid Services (CMS) through grant funds issued pursuant to CHIPRA section 401(d). Contact: [email protected] www.masschildhealthquality.org/work/care-coordination/
• AAP Policy Statement: Patient- and Family-Centered Care Coordination: A Framework for Integrating Care For Children and Youth Across Multiple Systems. Pediatrics. May 2014.
• AHRQ Care Coordination Atlas (McDonald Nov 2010, June 2014) and companion document Care Coordination Accountability Measures for Primary Care (McDonald Jan 2012).
• Care Coordination Measurement Tool (CCMT). Care Coordination for Children and Youth with Special Health Care Needs: A Descriptive, Multisite Study of Activities, Personnel Costs, and Outcomes. Antonelli RC, Stille CJ, Antonelli DM. Pediatrics 2008; Providing a Medical Home : The Cost of Care Coordination Services in a Community-Based, General Pediatric Practice. Antonelli RC, Antonelli DM. Pediatrics 2004. www.childrenshospital.org/care-coordination-curriculum/care-coordination-measurement
• Achieving a Shared Plan of Care with Children and Youth with Special Health Care Needs. Jeanne W. McAllister/Lucile Packard Foundation for Children’s Health. May 2014. lpfch-cshcn.org/publications/research-reports/achieving-a-shared-plan-of-care-with-children-and-youth-with-special-health-care-needs/
• Care Coordination Curriculum and Care Mapping Tool User Guides: Antonelli, Browning, Hackett-Hunter, McAllister, Risko; Lind. Boston Children’s Hospital; funded thru Family Voices/MCHB HRSA grant. 2012. www.childrenshospital.org/care-coordination-curriculum
Select References