uterine prolapse di wen m.d., ph.d., di wen m.d., ph.d., professor & chairman professor &...
TRANSCRIPT

Uterine ProlapseUterine Prolapse DI WEN DI WEN M.D., Ph.D., M.D., Ph.D.,
Professor & Chairman Professor & Chairman Department Of Obstetrics & GynecologyDepartment Of Obstetrics & Gynecology Renji Hospital Affiliated to SJTU School of MedicineRenji Hospital Affiliated to SJTU School of Medicine

Uterine Prolapse 2
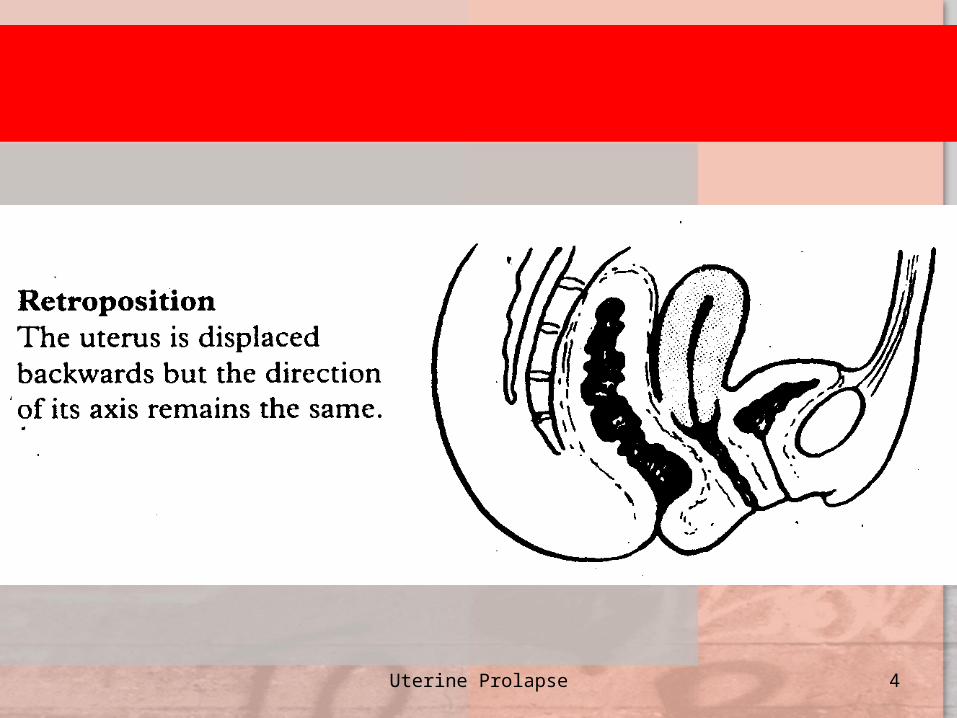
The uterus gradually The uterus gradually
descends in the axis of the descends in the axis of the
vagina taking the vaginal vagina taking the vaginal
wall with it. It may present wall with it. It may present
clinically at any level, but is clinically at any level, but is
usually classified as one of usually classified as one of
three degrees.three degrees.
DefinitionDefinition

Uterine Prolapse 3
Uterine Prolapse 4

Uterine Prolapse 5

Uterine Prolapse 6

Uterine Prolapse 7
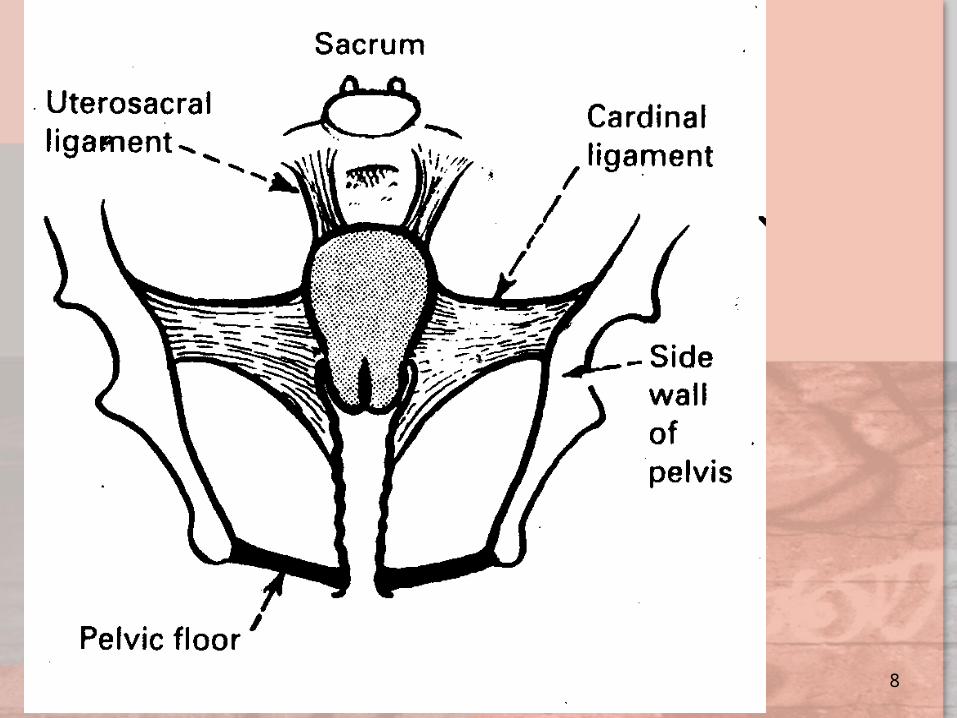
CausesCauses
1. The stretching of muscle and fibrous 1. The stretching of muscle and fibrous
tissuetissue
2. Increased intra-abdominal pressure2. Increased intra-abdominal pressure
3. A constitutional predisposition to 3. A constitutional predisposition to
stretching of the ligaments as a stretching of the ligaments as a
response presumably to years in the response presumably to years in the
erect positionerect position
Uterine Prolapse 8

Uterine Prolapse 9

Uterine Prolapse 10
• In recent years,the incidence of prolapsIn recent years,the incidence of prolapse is greatly reduced. The more liberal ue is greatly reduced. The more liberal use of caesarean section and the eliminase of caesarean section and the elimination of labours are probably the two motion of labours are probably the two most important factors. st important factors.
Uterine Prolapse 11
SymptomsSymptoms
• Something coming downSomething coming down• BackacheBackache• Increased frequency of micturitionIncreased frequency of micturition• A ‘bearing down’ sensationA ‘bearing down’ sensation• Stress incontinenceStress incontinence• Coital problemsCoital problems• Difficulty in voiding urineDifficulty in voiding urine

Uterine Prolapse 12

Uterine Prolapse 13

Uterine Prolapse 14

Uterine Prolapse 15

Uterine Prolapse 16

Uterine Prolapse 17

Uterine Prolapse 18
Degrees of uterine prolapseDegrees of uterine prolapse
First degreeFirst degree: cervix still inside vagina: cervix still inside vagina

Uterine Prolapse 19
Degrees of uterine prolapseDegrees of uterine prolapse• Second degreeSecond degree: the cervix appears outside : the cervix appears outside
the vulva. The cervical lips may become the vulva. The cervical lips may become congested and ulceratedcongested and ulcerated
Uterine Prolapse 20
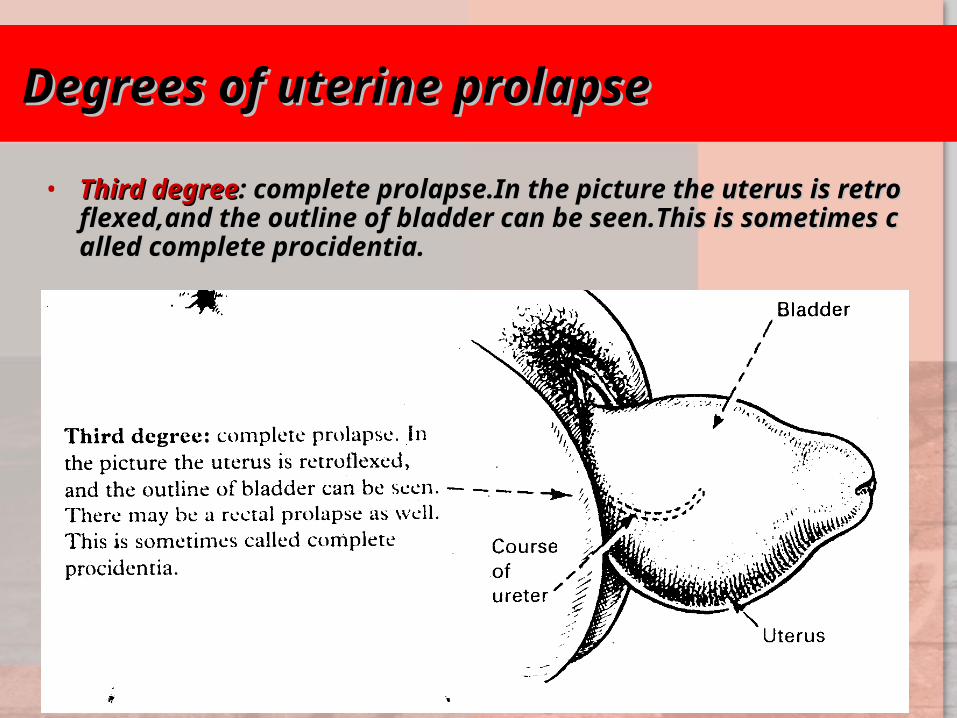
Degrees of uterine prolapseDegrees of uterine prolapse
• Third degreeThird degree: complete prolapse.In the picture the uterus is ret: complete prolapse.In the picture the uterus is retroflexed,and the outline of bladder can be seen.This is sometiroflexed,and the outline of bladder can be seen.This is sometimes called complete procidentia.mes called complete procidentia.

Uterine Prolapse 21
Diagnosis Diagnosis
• A pelvic examination reveals protrusion of the A pelvic examination reveals protrusion of the cervix into the lower part of the vagina (cervix into the lower part of the vagina (mild pmild prolapserolapse), past the vaginal introitus/opening (), past the vaginal introitus/opening (mmoderate prolapseoderate prolapse), or protrusion of the entire u), or protrusion of the entire uterus past the vaginal introitus/opening (terus past the vaginal introitus/opening (seversevere prolapsee prolapse).).

Uterine Prolapse 22
TreatmentTreatment
Pessary treatmentPessary treatment Indications:Patient prefers a pessary.Indications:Patient prefers a pessary. Pelvic surgery unaviodable risksPelvic surgery unaviodable risks Prolapse amenable to pessaryProlapse amenable to pessary The patient is not fit for surgeryThe patient is not fit for surgery Patient wishes to delay operationPatient wishes to delay operation

Uterine Prolapse 23
Uterine Prolapse 24

Uterine Prolapse 25

Uterine Prolapse 26

Uterine Prolapse 27
* Anterior colporrhaphy* Anterior colporrhaphy
(and repair of cystocele)(and repair of cystocele) * Posterior colpoperineorrhaphy* Posterior colpoperineorrhaphy (including repair of rectocele)(including repair of rectocele) * Manchester repair* Manchester repair * Vaginal hysterectomy* Vaginal hysterectomy
SurgerySurgery

Uterine Prolapse 28

Uterine Prolapse 29

Uterine Prolapse 30

Uterine Prolapse 31

Uterine Prolapse 32

Uterine Prolapse 33

DI WEN DI WEN M.D., Ph.D.M.D., Ph.D.
Professor & ChairmanProfessor & Chairman Department of Obstetrics & GynecologyDepartment of Obstetrics & Gynecology Renji Hospital Affiliated to SJTU School of MedicineRenji Hospital Affiliated to SJTU School of Medicine
Thanks for Your AttentionThanks for Your Attention

DI WEN DI WEN M.D., Ph.D.M.D., Ph.D.
Professor & ChairmanProfessor & Chairman Department of Obstetrics & GynecologyDepartment of Obstetrics & Gynecology Renji Hospital Affiliated to SJTU School of MedicineRenji Hospital Affiliated to SJTU School of Medicine
Thanks for Your AttentionThanks for Your Attention